Embed Size (px)
Citation preview

ORIGINAL ARTICLE
The Spectrum of Apocrine Lesions of the BreastF. P. O’Malley, MB, FRCPC, and A. L. Bane, MB, MRCPath
Abstract: Apocrine change is seen in a wide spectrum of breastlesions, ranging from microscopic cysts to invasive carcinoma. Thisarticle reviews the range of apocrine lesions and discusses the clinicalsignificance of these lesions. Although apocrine change in manycases does not present any diagnostic difficulty, apocrine prolifera-tions demonstrating cytologic atypia can be particularly challenging.The histologic criteria that have been proposed to foster reproducibil-ity in categorizing such lesions are reviewed. This review attempts toclarify the terminology that has been applied to a range of benignlesions, including sclerosing adenosis and complex sclerosing le-sions, containing foci of apocrine change. Malignant apocrine le-sions, including both in situ and invasive carcinoma, are also dis-cussed.
Key Words: apocrine, breast, cysts, sclerosing adenosis, complexsclerosing lesion, ductal carcinoma in situ, molecular alterations
(Adv Anat Pathol 2004;11:1–9)
Apocrine change in the breast is seen in a broad spectrum oflesions, from microscopic cysts to invasive apocrine car-
cinoma. Most of the lesions are easy to interpret and presentlittle diagnostic difficulty. A minority of proliferative apocrinelesions, however, can present particular diagnostic challenges,especially if cytologic atypia is evident. Not only are some ofthese lesions difficult to categorize, but there is controversyregarding their risk associations for subsequent carcinoma de-velopment.1
The purpose of this review is to highlight the areas ofconsensus as well as the controversial areas and to clarify someof the confusing terminology and diagnostic criteria that havebeen applied to proliferative apocrine lesions. The literaturedealing with in situ and invasive malignant apocrine lesionsare also discussed.
GROSS APOCRINE CYSTIC FORMATIONGross (palpable) cystic change, a common occurrence in
premenopausal women, generally presents as a single cyst.
The electrolyte content of the cyst fluid is closely related to thenature of the cyst lining: cysts with a high potassium content(Na+/K+ ratio < 3) are usually lined by apocrine cells (type Icysts), whereas those with Na+/K+ > 3 are lined by flattenedepithelium (type II cysts). There was initial evidence to sug-gest that type I cysts had a higher likelihood of recurrence thancysts lined by flattened epithelium,2,3 but this has not been re-produced in studies with larger numbers of patients and longerfollow-up.4
Women with palpable cysts who have undergone aspi-ration, have been reported to have a slightly increased risk ofsubsequent carcinoma development.3,5–9 However, two of thelargest studies with long-term follow-up showed conflictingresults. Haagensen et al demonstrated a 3-fold increased rela-tive risk, which was further elevated in the presence of a posi-tive family history.10 Dupont and Page, in contrast, found thatwomen with gross cysts who did not have a family history ofbreast cancer had a relative risk of only 1.5.11 This study maynot be directly comparable to the study by Haagensen et al10
because gross cysts were defined on the basis of size (>1 cm)rather than on the basis of palpability. A more recent study byDixon et al reported follow-up data on over 1300 women whohad palpable cysts aspirated between 1981 and 1987.4 Overall,the incidence of breast cancer in women with palpable cystswas almost 3 times greater than that in the reference popula-tion. This increased incidence of breast cancer pertained toboth type I and type II cysts. Although the risk of developingbreast cancer was greatest within the first year after cyst aspi-ration, the risk remained elevated more than 5 years after as-piration of the cyst. The authors found a significant associationbetween increased risk and age at cyst aspiration. Womenyounger than 45 years had standardized incidence rates almost6 times greater than the reference population, whereas the rela-tive risk was only 1.7 in women older than 55 years. To explainthe significantly increased risk in younger women, the authorssuggest that the breast epithelium in these women may be moresusceptible to malignant transformation, given the increasedepithelial activity associated with cyst formation and thehigher circulating estrogen levels present in these premeno-pausal women. The findings from this study, if replicated byothers, may have implications for the management of youngwomen with palpable breast cysts. The current consensus,however, is that gross cysts are not associated with any signifi-cant increased risk of subsequent carcinoma development,
From the Department of Pathology and Laboratory Medicine, Mount SinaiHospital and University of Toronto, Toronto, Ontario, Canada.
Reprints: F. P. O’Malley, MB, FRCPC, Department of Pathology and Labo-ratory Medicine, Mount Sinai Hospital, 600 University Avenue, Toronto,Ontario M5G 1X5, Canada (e-mail: [email protected]).
Copyright © 2003 by Lippincott Williams & Wilkins
Adv Anat Pathol • Volume 11, Number 1, January 2004 1

therefore these women do not require any further follow-upthan would be offered routinely.12
PAPILLARY APOCRINE CHANGEMicroscopic cysts lined by a single layer of apocrine epi-
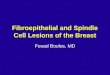
thelium are nonproliferative lesions that are not associatedwith any increased risk of subsequent carcinoma develop-ment.11,12 Microscopic cysts may also be lined by apocrineepithelium arranged in papillary formations that protrude intothe cyst lumen. One study categorized papillary formationsinto three groups—simple, complex, and highly complex—based on the length of the papillations and the tendency to formarches (Fig. 1).13 This study reported that although there was aslightly increased risk of subsequent carcinoma overall, mostof the elevated risk was related to the presence of atypical hy-perplasia in cases showing highly complex papillary apocrinechange (PAC). Only 1% of almost 3000 biopsies reviewedshowed highly complex PAC, yet, atypical hyperplasia waspresent in 20% of these cases.13 Thus, the finding of highlycomplex papillary apocrine change should prompt a thoroughsearch for the presence of concurrent atypical hyperplasia. Butit should also be noted that papillary apocrine change in theabsence of atypical hyperplasia in adjacent breast tissue is notassociated with any subsequent carcinoma risk.
BENIGN APOCRINE PROLIFERATIONSThe term “apocrine adenosis” has been applied to a
range of apocrine proliferations. This term was first used byEusebi et al to describe apocrine change in glands associatedwith two cases of adenomyoepithelioma,14 a lesion that hadpreviously been referred to as “adenomyoepitheliomatousadenosis.”15 “Apocrine adenosis” has subsequently been usedin several publications to describe apocrine change in a rangeof proliferative lesions.16–20 Simpson and Page used this termto describe apocrine change in deformed lobular units, scleros-ing adenosis, radial scars, and complex sclerosing lesions (Fig.2). In their study they reported these changes in 18.3% of con-sultation cases and in 3% of a consecutive series of benignbreast biopsies. In the consecutive series, the incidence ofatypical hyperplasia was statistically significantly greater incases with so-called apocrine adenosis than in those without.16
Further confusion has been added to the literature by theapplication of the term “apocrine adenosis” to a mass lesion.21
In this case report the authors concluded that apocrine adenosisrepresents a neoplastic process. This conclusion was based onthe finding of monoclonality in a single case that presentedclinically as a palpable mass that measured 4.3 cm in maxi-mum dimension. Thus, it was clearly different from the lesionsdescribed as “apocrine adenosis” by others,16,17,20 as high-lighted by Page and Simpson in a subsequent letter.22
Several studies have investigated the presence of mo-lecular markers in apocrine adenosis. However, these studiesare difficult to interpret because it is unclear which apocrine
lesions they investigated.18,23,24 Furthermore, HER2/neu pro-tein overexpression was reported in 10 of 18 (55.6%) suchcases in one study,23 but the authors reported lack ofHER2/neu amplification in all of these cases. Given thatHER2/neu protein overexpression is related to gene amplifica-tion in almost all cases,25,26 the lack of HER2/neu gene ampli-fication in this study calls into question the immunohistochem-ical results.23 On the other hand, a higher proliferation indexhas been consistently demonstrated in proliferative apocrinelesions than in apocrine change in cysts.18,24,27
Given the spectrum of nonproliferative and proliferativeapocrine lesions designated as “apocrine adenosis” and theconfusion that this has caused, it is preferable, as Eusebi et alhave proposed,28 to describe apocrine change in the specificunderlying lesion rather than to collapse different entities suchas sclerosing adenosis or radial scar into one diagnostic cat-egory based on the presence of apocrine change. Future stud-ies, using a more precise categorization of proliferative apo-crine lesions, may elucidate the conflicting results that have sofar been reported for the many lesions described as “apocrineadenosis”.
ATYPICAL APOCRINE PROLIFERATIONSThere is controversy regarding the criteria used to define
cytologic atypia and the clinical significance of atypia in apo-crine epithelium. This particularly applies to apocrine changein sclerosing lesions (Fig. 3). Much of this difficulty is relatedto the fact that normal apocrine cells are large and have promi-nent nucleoli. It is thus important to use normal apocrine mor-phology as the reference point when determining the presenceof cytologic atypia in apocrine proliferations. There are fewstudies assessing the clinical significance of atypia in apocrineproliferations. One study followed 51 patients with what theydescribed as “atypical apocrine metaplasia within sclerosinglesions.” The authors defined atypia as the presence of “promi-nent pleomorphic nucleoli” and an increased nuclear:cytoplas-mic ratio. These patients were followed for an average of 35months, and none of the women developed breast carcinoma.17
In contrast, Seidman et al20 reported a significantly increasedrisk of subsequent carcinoma development in atypical apo-crine proliferative lesions. Cytologic atypia was defined in thissetting as a 3-fold nuclear enlargement of the apocrine cellswith enlarged nucleoli. The authors coined the term “atypicalapocrine adenosis” for such lesions. They reported relativerisks of 5.5 overall (95% confidence interval 1.9 to 16), but inwomen older than 60 years of age the relative risk was 14 (95%confidence interval 4.1 to 48). It is likely that some of thesecases represented cancerization of sclerosing adenosis by duc-tal carcinoma in situ (DCIS) because the authors state that theycategorized lesions based on the presence/absence of atypia asdefined above and made no attempt to further separate cases ofnoninvasive apocrine carcinoma from cases demonstrating cy-tologic atypia. Also cases with a co-occurrence of atypical
F. P. O’Malley and A. L. Bane Adv Anat Pathol • Volume 11, Number 1, January 2004
2 © 2003 Lippincott Williams & Wilkins

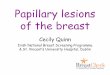
FIGURE 2. Apocrine change in a complex sclerosing lesion. A, The focus of apocrine change is indicated by the arrow. B, Highpower shows bland apocrine nuclei.
FIGURE 1. Papillary apocrine change. A, Simple papillary apocrine change. The papillary projections are rounded and protrudeinto the cyst space. B, Complex papillary apocrine change. The papillae are more elongated, and the tips tend to touch, formingirregular arches. C, Highly complex papillary apocrine change. The papillae are more irregular, and there is prominent formationof arches. D, High power shows that the cells lining all subcategories of papillary apocrine change exhibit the characteristicfeatures of benign apocrine change with the presence of a single, prominent, uniform nucleolus and abundant eosinophilicgranular cytoplasm.
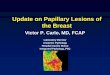
FIGURE 3. Benign apocrine proliferation in a radial scar. A, The medium-power view shows a portion of a radial scar containingcystically dilated ducts lined by apocrine cells. Focally there is a more solid proliferation of apocrine cells. B, At high power, themajority of the cells within the solid apocrine proliferation show the typical features of benign apocrine cells. An occasional cellshows approximately 3-fold nuclear enlargement.
Adv Anat Pathol • Volume 11, Number 1, January 2004 Apocrine Lesions of the Breast
© 2003 Lippincott Williams & Wilkins 3

ductal hyperplasia were not excluded. For these reasons therelative risks are most likely an overestimate of the risk asso-ciated with these so-called atypical apocrine proliferations.
The term “borderline” has been used to recognize agroup of atypical apocrine lesions that have some, but not all,of the features of DCIS. There are clinically validated criteriadescribed for nonapocrine lesions that can be used to separatesuch cases of atypical ductal hyperplasia from low-gradeDCIS.11,29 These criteria, however, are not readily applicableto apocrine lesions. Two groups have attempted to define cri-
teria to separate atypical apocrine lesions from minimal ex-amples of apocrine DCIS.30,31 O’Malley et al used cytologiccharacteristics (usual apocrine, borderline features, or “as inDCIS”) and extent criteria (<4 mm, 4–8 mm, and >8 mm) tohelp foster a more uniform categorization of proliferative apo-crine lesions that do not easily fall into the unequivocally be-nign or malignant categories.30 Lesions with usual apocrinecytology that measured <8 mm were called benign. Lesionswith cytologic features as in DCIS (irregular nuclear mem-brane, coarse chromatin, multiple, prominent nucleoli) were
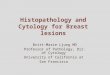
FIGURE 4. Complex sclerosing lesion with atypical apocrine proliferation bordering on ductal carcinoma in situ. A, The low-powerview shows marked expansion of spaces by a proliferation of apocrine cells. B, The cytologic atypia is demonstrated by nuclearenlargement and loss of a central nucleolus with replacement by smaller, multiple nucleoli. The nuclear borders are slightlyirregular. Apoptosis is evident.
FIGURE 5. Apocrine DCIS, Grade III/III. A, Medium power shows the marked heterogeneity that apocrine DCIS can demonstrate.B, High-power view of the nuclei in the middle portion of the duct shows overtly malignant features with marked nuclearpleomorphism, coarse chromatin, multiple, irregular nucleoli, and irregularity and thickening of the nuclear margins.
FIGURE 6. Invasive apocrine carcinoma. A, Medium power shows irregular tumor nests infiltrating the stroma. B, The malignantnuclei show prominent apocrine features.
F. P. O’Malley and A. L. Bane Adv Anat Pathol • Volume 11, Number 1, January 2004
4 © 2003 Lippincott Williams & Wilkins

diagnosed as apocrine DCIS. A “borderline” category was de-fined primarily by the cytologic features of nuclear enlarge-ment, the presence of slightly irregular nuclear membranes andmultiple, small nucleoli, and variability in nuclear size (Fig. 4).Marked nuclear enlargement was also considered atypical.Size was used as a secondary criterion such that lesions mea-suring between 4 and 8 mm required the borderline cytologicfeatures to be present in the majority of cells before being cat-egorized as “borderline DCIS.” Lesions greater than 8 mmwere assigned to the “borderline DCIS” category even if onlya minority of the cells demonstrated the borderline cytologicfeatures. This approach to classification has not, as yet, beenvalidated by clinical follow-up studies.
Tavassoli and Norris31 used cytologic atypia (defined asat least 3-fold nuclear enlargement) and nuclear stratificationor papillary tufting to define atypical apocrine lesions. Caseswith both cytologic atypia as defined above and stratificationwith papillary formations were described as atypical apocrinehyperplasia, and the term “atypical apocrine metaplasia” wasapplied to cases showing cytologic atypia only. The extent cri-terion of 2 mm was used to separate proliferative apocrine le-sions showing cytologic atypia and a cribriform architecturefrom apocrine DCIS. Although this study included some fol-low-up information, the majority of patients were treated bymastectomy, so the natural history of these atypical apocrineproliferations remains unclear.
The presence of necrosis has been reported as useful indistinguishing benign apocrine lesions from apocrine DCIS.31
In fact, these authors recommend caution in the diagnosis ofapocrine DCIS in the absence of necrosis. Others30,32 considerthat necrosis is not a prerequisite for a diagnosis of apocrineDCIS. Indeed, when necrosis is present, the nuclear gradetends to be high, and the diagnosis of DCIS in this setting is notdifficult.30
To summarize, cytologic atypia in a proliferative apo-crine lesion has been defined by several groups as 3-foldnuclear enlargement with nucleolar enlargement. Otherswould also accept the presence of multiple small nucleoli inapocrine cells showing variability in nuclear size as atypical.These cells usually lack coarse chromatin and demonstrateregular nuclear membranes in contrast to malignant apocrinecells. The studies that have attempted to define criteria foratypical apocrine lesions bordering on DCIS are limited by thelack of long-term clinical follow-up data. These criteria aresummarized in Table 1. Fortunately, these lesions are ex-tremely rare in clinical practice. When encountered, a conser-vative approach recommending clinical follow-up, is sug-gested.
APOCRINE DCISApocrine DCIS that presents the least diagnostic diffi-
culty is characterized by an extensive proliferation of apocrinecells showing marked nuclear pleomorphism with enlargednuclei, multiple prominent nucleoli, and irregular nuclearmembranes. This diagnosis is facilitated by the presence ofcomedo-type necrosis.
Although apocrine DCIS can also be diagnosed in caseswith lesser degrees of nuclear pleomorphism, the diagnosticchallenge in such cases is the accurate categorization of thenuclear grade.33 The participants of The Consensus Confer-ence on the Classification of Ductal Carcinoma In-Situ34 rec-ognized apocrine DCIS as a special variant, but they did notmake recommendations on the subclassification of apocrineDCIS. Some consider most apocrine DCIS lesions to be at leastintermediate grade.31 More recently, attempts have been madeto define criteria for low-grade apocrine DCIS.35 These au-thors used nuclear grade and the presence of extensive (com-edo-type) necrosis to stratify apocrine DCIS cases into low,
TABLE 1. Proposed Criteria to Separate Atypical Apocrine Proliferations From Low-Grade Apocrine DCIS
Atypical Apocrine Lesions Low-Grade Apocrine DCIS
Architecture • Often involve proliferative lesions including sclerosingadenosis, complex sclerosing lesion, or papilloma
• More Commonly involves areas of sclerosing adenosis,complex sclerosing lesion, or papilloma
• Nuclear stratification or tufting of epithelium may bepresent
• May exhibit the characteristic cribriform architecture oflow-grade nonapocrine DCIS
Cytology • 3-fold nuclear enlargement with nucleolar enlargement • Enlarged cells with enlarged, irregular nucleoli• Cells may contain multiple, smaller nucleoli, with
variability in nuclear size• Cells may contain multiple, smaller, irregular nucleoli
with variability in nuclear size• Slightly irregular nuclear membranes • Irregular nuclear membranes• Fine chromatin • Coarse chromatin• Necrosis is absent • Necrosis is absent
Extent • Usually of limited extent (<2–4 mm) • Usually larger (>4 mm)• Usually involves 1 lobular unit • Usually involves more than 2 lobular units and
intervening ducts
Source: References 16, 19, 29, 30.
Adv Anat Pathol • Volume 11, Number 1, January 2004 Apocrine Lesions of the Breast
© 2003 Lippincott Williams & Wilkins 5

intermediate, and high histologic grade. Apoptotic cells werenot taken into consideration. Low-grade DCIS was defined ascells with grade 1 or 2 nuclei and no evidence of necrosis.High-grade DCIS had grade 3 nuclei (characterized by the fre-quent presence of multiple nucleoli and coarse chromatin) aswell as extensive necrosis (Fig. 5). Intermediate-grade apo-crine DCIS included cases with grade 1 or 2 nuclei with necro-sis as well as cases with high-grade nuclei in the absence ofnecrosis. Almost 29% cases were classified as low histologicgrade, but only 1 case demonstrated low-grade nuclei. Tumorheterogeneity was evident, with all but 1 of the cases graded asintermediate or high grade demonstrating lower-grade foci inthe biopsy. This striking heterogeneity led the authors tospeculate that low-grade apocrine DCIS may be a precursor ofthe higher-grade lesions.
In summary, apocrine DCIS should be graded if pos-sible. Because of the marked heterogeneity of these lesions, thenuclear grade should be based on the foci showing the greatestdegree of nuclear pleomorphism. Although the majority ofapocrine DCIS lesions are associated with intraluminal necro-sis, the presence of necrosis is not a prerequisite for the diag-nosis of apocrine DCIS.
INVASIVE APOCRINE CARCINOMAThe incidence of pure apocrine carcinoma varies from
less than 0.3% to 4% (Fig. 6).36–38 The variability in incidenceis likely a result of the lack of well-defined diagnostic criteria.Rosen stipulates that the term should be reserved for “neo-plasms in which all or nearly all the epithelium has apocrinecytologic features.”39 In contrast, focal apocrine differentia-tion is quite common and has been reported in up to 60% ofcarcinomas of no special type (ductal, NST).40 Indeed, the in-cidence is as high as 72% when the apocrine phenotype isbased on the immunoexpression of the 15-kDa glycoprotein ofgross cystic disease (GCDFP).40–43 Areas of apocrine differ-entiation have also been reported in special type cancers in-cluding papillary44 and lobular carcinomas.45 The apocrinephenotype can be further corroborated by additional studiesincluding the presence of PAS-positive cytoplasmic granulesand the demonstration of empty vesicles and osmiophilic gran-ules at the ultrastructural level.37,41,46–49
Grossly, these tumors are indistinguishable from othermammary carcinomas and usually present as firm to hardmasses with infiltrating borders.39 Tumor size, means ofpresentation/detection, incidence of lymph node positivity,and tumor grade do not differ significantly from NST tu-mors.50–52 In the 2 reports that specify the laterality of disease,the left side predominates, a fact that should be interpretedwith caution because the cumulative number of invasive can-cers in these 2 reports is only 51.51,52 The frequency of bilat-erality in patients who have apocrine carcinoma is not signifi-cantly different from that of breast carcinomas in general.However, only 2 cases of bilateral apocrine carcinoma have
been reported, 1 synchronous53 and the other metachronous.54
In the case of synchronous apocrine carcinomas, the authorsdemonstrated the independent nature of these tumors by em-ploying a variety of immunohistochemical, cytogenetic, andmolecular genetic tests.53 Male apocrine breast cancer has alsobeen reported but presumably is rare.55
One study suggested that radiologically these tumorsmay present distinctive characteristics with a higher incidenceof “mixed form” diffusely scattered calcifications in tumorswith apocrine features.56 However Gilles et al, using strict his-tologic criteria, studied 16 invasive apocrine carcinomas andshowed that their mammographic presentation did not differfrom those of NST (ductal) carcinomas.57
Microscopically, apocrine carcinomas demonstrate thesame architectural growth pattern as other mammary carcino-mas of no special type, differing only in their cytologic appear-ance. The cells are characterized by the typical apocrine fea-tures of abundant eosinophilic granular cytoplasm and promi-nent and often multiple nucleoli.
The clinical significance of the apocrine phenotype hasbeen addressed by two studies.51,52 Both studies compared in-vasive apocrine carcinomas with NST tumors matched for im-portant prognostic parameters and time of diagnosis. No dif-ference in survival rates between the two groups was found ineither study, and the authors concluded that apocrine carci-noma is not clinically distinct from NST carcinomas.
Invasive carcinomas showing prominent apocrinechange have been reported to demonstrate a distinctive immu-nohistochemical profile. They are predominantly ER and PRnegative but strongly androgen receptor (AR) positive.58,59 Arecent study suggests that androgen immunopositivity is notrestricted to carcinomas showing apocrine differentiation.60 Inthis study, 87 of 145 (60%) invasive carcinomas of no specialtype (NST) were immunopositive for the androgen receptor(AR). The highest incidence of AR positivity was seen in thegrade I/III tumors (88%). There were 12 invasive tumorsshowing prominent apocrine differentiation in this series. All12 cases were poorly differentiated (grade III/III), and 9 ofthese were AR positive. Only 58% (7/12) showed theER−/PR−/AR+ immunphenotype. Thus, this study indicatesthat AR positivity may be common in all invasive carcinomasrather than being restricted to carcinomas showing prominentapocrine differentiation. Androgen receptor expression in in-vasive carcinomas requires further study to determine if thiscan be exploited therapeutically.
The incidence of HER2/neu protein overexpression orgene amplification in apocrine carcinomas has not been for-mally studied. Several other molecular markers have been as-sessed by immunohistochemistry in invasive carcinomasshowing apocrine differentiation. Moriya et al24 reported p53immunopositivity in 6 of 13 such cases (46.2%). The nuclearlocalization of p53 by IHC has been shown to correlatestrongly with inactivating mutations of the p53 gene. P21, a
F. P. O’Malley and A. L. Bane Adv Anat Pathol • Volume 11, Number 1, January 2004
6 © 2003 Lippincott Williams & Wilkins

member of the Cip/Kip family of cycle-dependent kinases anda downstream effector of the p53 gene, was shown to be ex-pressed in 8 of 13 invasive carcinomas with apocrine differen-tiation.24 Reduced immunohistochemical expression of p27,another Cip/Kip family member and p53-independent inhibi-tor of cell cycle progression that may be associated with poorsurvival, has been reported in both invasive carcinomas withapocrine differentiation and carcinomas of no special type.24,61
In summary, there is insufficient evidence to recognizethe apocrine phenotype as a special type carcinoma.
MOLECULAR STUDIES OF APOCRINE LESIONSThere are few molecular data available on proliferative
apocrine lesions. Two studies investigating loss of heterozy-gosity (LOH) at loci associated with invasive carcinoma failedto demonstrate allelic imbalances at these loci in apocrine hy-perplasias. However, a limited number of loci were investi-gated in these studies.62,63 A further study assessed LOH at 14polymorphic loci in 32 cases of fibrocystic changes. The au-thors detected LOH in 10 of 19 (53%) examples of apocrinemetaplasia. An additional 14 cases of apocrine metaplasia ad-jacent to carcinoma were also evaluated. The apocrine meta-plasia in 7 of these cases demonstrated LOH with at least 1marker, and the apocrine metaplasia and adjacent carcinoma inall 7 cases shared LOH at 1 or more loci.64
A study utilizing comparative genomic hybridization ina series of papillary apocrine hyperplasias, apocrine ductal car-cinoma in situ, and invasive apocrine carcinomas showed mo-lecular alterations in all three groups of lesions. Although thenumber of alterations was lower in the papillary apocrine hy-perplasias compared with the in situ and invasive apocrine le-sions, there was overlap in the pattern of genetic alterationsbetween the benign and malignant lesions. The most commonchanges reported in apocrine hyperplasia were gains of 2q,13q, and 1p and losses of 1p, 2p, 10q, 16q, 17q, and 22q. Ma-lignant apocrine lesions (both in situ and invasive) commonlyshowed gains of 1p, 1q, and 2q and losses of 1p, 12q, 16q, 17q,and 22q.65 These authors also demonstrated that invasive apo-crine carcinomas have areas of loss and gain in common withinvasive carcinomas of no special type but also harbor alter-ations not previously reported as playing a significant role inbreast tumorigenesis. These include losses at 2p, 9q, and 1qand gains at 2q, 3p, and 13q. Novel areas of loss and gain sug-gest a different genetic drive to the apocrine phenotype.
The findings of molecular alterations in benign prolif-erative apocrine lesions suggest that at least some of these le-sions may be clonal in nature. However, the significance ofmolecular alterations such as allelic imbalance or loss of het-erozygosity in the pathogenesis of proliferative apocrine le-sions or their associations with any increased risk of subse-quent carcinoma development are not clear. Long-term fol-low-up studies to fully elucidate the clinical significance ofsuch findings are required.
SUMMARYApocrine change in cysts is a particularly common find-
ing in the breast. There is a consensus that microscopic cystslined by apocrine cells are not associated with any increasedrisk of subsequent carcinoma development.11,12 In contrast,there has been much debate about the possible increased riskassociation with palpable cysts. This remains a controversialarea, but at present there are insufficient data to recommendany change to routine follow-up for women with palpablecysts.
Apocrine change is not uncommonly found in deformedlobular units as well as several proliferative lesions, includingsclerosing adenosis, papillomas, and complex sclerosing le-sions. Several recent publications have used the term “apo-crine adenosis” to describe all of these lesions. Given the con-fusion that this has caused, it is perhaps preferable to describeapocrine change in the specific underlying lesion rather than tocollapse different entities into one diagnostic category basedon the presence of apocrine change.
The majority of lesions in breast demonstrating apocrinechange do not present diagnostic challenges. However, apo-crine proliferations demonstrating cytologic atypia can be par-ticularly challenging. There has been an attempt in the litera-ture to define criteria that would help separate benign apocrinelesions from those that have malignant potential, but these cri-teria have not, as yet, been clinically validated. In clinical prac-tice, fortunately, such lesions are rare. It is hoped that the use ofstrict morphologic criteria in future molecular studies of pro-liferative apocrine lesions will further our understanding of thebiologic potential of these lesions. Clinical follow-up studiesare needed to determine their clinical significance.
Malignant apocrine lesions can also present diagnosticchallenges. Although apocrine ductal carcinoma in situ is usu-ally characterized by markedly pleomorphic nuclei and come-do necrosis, apocrine DCIS can also be recognized in the ab-sence of necrosis if the cytologic and extent criteria are ful-filled. Invasive carcinomas showing apocrine differentiationdo not differ clinically from carcinomas of no special typewhen matched for grade and stage.
ACKNOWLEDGMENTSThe authors thank Dr David Page, Vanderbilt University
Medical Center, Nashville, TN for his many helpful commentsduring preparation of this manuscript.
REFERENCES1. O’Malley. Non-invasive apocrine lesions of the breast. Current Diagnos-
tic Pathology. In press.2. Dixon JM, Lumsden AB, Miller WR. The relationship of cyst type to risk
factors for breast cancer and the subsequent development of breast cancerin patients with breast cystic disease. Eur J Cancer Clin Oncol. 1985;21:1047–1050.
3. Bruzzi P, Dogliotti L, Naldoni C, et al. Cohort study of association of riskof breast cancer with cyst type in women with gross cystic disease of thebreast. Br Med J. 1997;314:925–928.
Adv Anat Pathol • Volume 11, Number 1, January 2004 Apocrine Lesions of the Breast
© 2003 Lippincott Williams & Wilkins 7

4. Dixon JM, McDonald C, Miller WR. Risk of breast cancer in women withpalpable breast cysts: a prospective study. Lancet. 1999;353:1742–1745.
5. Devitt JE, To T, Miller AB. Risk of breast cancer in women with breastcysts. Can Med Assoc J. 1992;147:45–49.
6. Jones BM, Bradbeer JW. The presentation and progress of macroscopicbreast cysts. Br J Surg. 1980;67:669–671.
7. Haagensen CD. Diseases of the Breast. Philadelphia: WB Saunders, 1981.8. Roberts MM, Jones V, Elton RA, et al. Risk of breast cancer in women
with history of benign disease of the breast. Br Med J (Clin Res Ed). 1984;288:275–278.
9. Bundred NJ, West RR, Dowd JO, et al. Is there an increased risk of breastcancer in women who have had a breast cyst aspirated? Br J Cancer.1991;64:953–955.
10. Haagensen CD, Bodian CA. Haagensen DE Jr. Breast Cancer Risk andDetection. Philadelphia: WB Saunders, 1981.
11. Dupont WD, Page DL. Risk factors for breast cancer in women with pro-liferative breast disease. N Engl J Med. 1985;312:146–151.
12. Fitzgibbons PL, Henson DE, Hutter RV. Benign breast changes and therisk for subsequent breast cancer: an update of the 1985 consensus state-ment. Cancer Committee of the College of American Pathologists. [seecomments] Arch Pathol Lab Med. 1998;122:1053–1055.
13. Page DL, Dupont WD, Jensen RA. Papillary apocrine change of thebreast: associations with atypical hyperplasia and risk of breast cancer.Cancer Epidemiol Biomarkers Prev. 1996;5:29–32.
14. Eusebi V, Casadei GP, Bussolati G, et al. Adenomyoepithelioma of thebreast with a distinctive type of apocrine adenosis. Histopathology. 1987;11:305–315.
15. Kiaer H, Nielsen B, Paulsen S, et al. Adenomyoepithelial adenosis andlow-grade malignant adenomyoepithelioma of the breast. Virchows ArchA Pathol Anat Histopathol. 1984;405:55–67.
16. Simpson JF, Page DL, Dupont WD. Apocrine adenosis-a mimic of mam-mary carcinoma. Surg Pathol. 1990;3:289–299.
17. Carter DJ, Rosen PP. Atypical apocrine metaplasia in sclerosing lesions ofthe breast: a study of 51 patients. Mod Pathol. 1991;4:1–5.
18. Wells CA, McGregor GI, Makunura CN, et al. Apocrine adenosis: a pre-cursor of aggressive breast cancer. J Clin Pathol. 1995;48:737–742.
19. Raju U, Zarbo RJ, Kubus J, et al. The histologic spectrum of apocrinebrest proliferations: A comparative study of morphology and DNA con-tent by image analysis. Hum Pathol. 1993;24:173–181.
20. Seidman JD, Ashton M, Lefkowitz M. Atypical apocrine adenosis of thebreast: a clinicopathologic study of 37 patients with 8.7-year follow-up.Cancer. 1996;77:2529–2537.
21. Endoh Y, Tamura G, Kato N, et al. Apocrine adenosis of the breast: clonalevidence of neoplasia. Histopathology. 2001;38:221–224.
22. Page DL, Simpson JF. What is apocrine adenosis, anyway? Histopathol-ogy. 2001;39:433–434.
23. Selim AG, El-Ayat G, Wells CA. c-erbB2 oncoprotein expression, geneamplification, and chromosome 17 aneusomy in apocrine adenosis of thebreast. J Pathol. 2000;191:138–142.
24. Moriya T, Sakamoto K, Sasano H, et al. Immunohistochemical analysis ofKi-67, p53, p21, and p27 in benign and malignant apocrine lesions of thebreast: its correlation to histologic findings in 43 cases. Mod Pathol. 2000;13:13–18.
25. Slamon DJ, Godolphin W, Jones LA, et al. Studies of the HER-2/neuproto-oncogene in human breast and ovarian cancer. Science. 1989;244:707–712.
26. Press MF. Bernstein L, Thomas PA et al. HER-2/neu gene amplificationcharacterized by fluorescence in situ hybridization: poor prognosis innode-negative breast carcinomas. J Clin Oncol. 1997;15:2894–2904.
27. Selim AG, El-Ayat G, Wells CA. Expression of c-erbB2, p53, Bcl-2, Bax,c-myc and Ki-67 in apocrine metaplasia and apocrine change within scle-rosing adenosis of the breast. Virchows Arch. 2002;441:449–455.
28. Eusebi V, Damiani S, Losi L, et al. Apocrine differentiation in breastepithelium. Adv Anat Pathol. 1997;4:139–155.
29. Page DL, Rogers LW. Combined histologic and cytologic criteria for thediagnosis of mammary atypical ductal hyperplasia. Hum Pathol. 1992;23:1095–1097.
30. O’Malley FP, Page DL, Nelson EH, et al. Ductal carcinoma in situ of thebreast with apocrine cytology: definition of a borderline category. HumPathol. 1994;25:164–168.
31. Tavassoli FA, Norris HJ. Intraductal apocrine carcinoma: a clinicopatho-logic study of 37 cases. Mod Pathol. 1994;7:813–818.
32. Durham JR, Fechner RE. The histologic spectrum of apocrine lesions ofthe breast. Am J Clin Pathol. 2000;113(5 Suppl 1):S3–S18.
33. Scott MA, Lagios MD, Axelsson K, et al. Ductal carcinoma in situ of thebreast: reproducibility of histological subtype analysis [see comments].Hum Pathol. 1997;28:967–973.
34. The Consensus Conference Committee. Consensus conference on theclassification of ductal carcinoma in situ. [see comments]. Cancer. 1997;80:1798–1802.
35. Leal C, Henrique R, Monteiro P, et al. Apocrine ductal carcinoma in situof the breast: histologic classification and expression of biologic markers.Hum Pathol. 2001;32:487–493.
36. Azzopardi JG. Problems in Breast Pathology. Philadelphia: WB Saun-ders, 1979.
37. Mossler JA, Barton TK, Brinkhous AD, et al. Apocrine differentiation inhuman mammary carcinoma. Cancer. 1980;46:2463–2471.
38. Eusebi V, Betts C, Haagensen DE Jr, et al. Apocrine differentiation inlobular carcinoma of the breast: a morphologic, immunologic, and ultra-structural study. Hum Pathol. 1984;15:134–140.
39. Rosen PP. Rosen’s Breast Pathology. 2 ed. Philadelphia, PA: LippincottWilliams & Wilkins, 2001.
40. Haagensen CD. Diseases of the breast. 3 ed. Philadelphia: W.B. Saunders,1986.
41. Mazoujian G, Pinkus GS, Davis S, et al. Immunohistochemistry of a grosscystic disease fluid protein (GCDFP-15) of the breast. A marker of apo-crine epithelium and breast carcinomas with apocrine features. Am JPathol. 1983;110:105–112.
42. Eusebi V, Millis RR, Cattani MG, et al. Apocrine carcinoma of the breast.A morphologic and immunocytochemical study. Am J Pathol. 1986;123:532–541.
43. Wick MR, Lillemoe TJ, Copland GT, et al. Gross cystic disease fluidprotein-15 as a marker for breast cancer: immunohistochemical analysisof 690 human neoplasms and comparison with alpha-lactalbumin. HumPathol. 1989;20:281–287.
44. Papotti M, Eusebi V, Gugliotta P, et al. Immunohistochemical analysis ofbenign and malignant papillary lesions of the breast. Am J Surg Pathol.1983;7:451–461.
45. Eusebi V, Magalhaes F, Azzopardi JG. Pleomorphic lobular carcinoma ofthe breast: an aggressive tumor showing apocrine differentiation. HumPathol. 1992;23:655–662.
46. Pagani A, Sapino A, Eusebi V, et al. PIP/GCDFP-15 gene expression andapocrine differentiation in carcinomas of the breast. Virchows Arch. 1994;425:459–465.
47. Le D. V, Zangerle PF, Collette J et al. Immunohistochemistry of a com-ponent protein of the breast cystic disease fluid with mol. wt 15,000. EurJ Cancer Clin Oncol. 1985;21:715–725.
48. Miller WR, Shivas AA, Franchimont P, et al. Breast gross cystic diseaseprotein 15 in human breast cancer in culture. Eur J Cancer Clin Oncol.1988;24:223–228.
49. Ahmed A. Atlas of ultrastructure of human diseases. New York: ChurchillLivingstone, 1978.
50. Mossler JA, Barton TK, Brinkhous AD, et al. Apocrine differentiation inhuman mammary carcinoma. Cancer. 1980;46:2463–2471.
51. Abati AD, Kimmel M, Rosen PP. Apocrine mammary carcinoma. A clin-icopathologic study of 72 cases. Am J Clin Pathol. 1990;94:371–377.
52. d’Amore ES, Terrier-Lacombe MJ, Travagli JP, et al. Invasive apocrinecarcinoma of the breast: a long term follow-up study of 34 cases. BreastCancer Res Treat. 1988;12:37–44.
53. Schmitt FC, Soares R, Seruca R. Bilateral apocrine carcinoma of thebreast. Molecular and immunocytochemical evidence for two indepen-dent primary tumours. Virchows Arch. 1998;433:505–509.
54. Frable WJ, Kay S. Carcinoma of the breast. Histologic and clinical fea-tures of apocrine tumors. Cancer. 1968;21:756–763.
55. Bryant J. Male breast cancer: a case of apocrine carcinoma with psam-moma bodies. Hum Pathol. 1981;12:751–753.
56. Kopans DB, Nguyen PL, Koerner FC, et al. Mixed form, diffusely scat-tered calcifications in breast cancer with apocrine features. Radiology.1990;177:807–811.
57. Gilles R, Guinebretiere JM, Toussaint C, et al. Locally advanced breast
F. P. O’Malley and A. L. Bane Adv Anat Pathol • Volume 11, Number 1, January 2004
8 © 2003 Lippincott Williams & Wilkins

cancer: contrast-enhanced subtraction MR imaging of response to preop-erative chemotherapy. Radiology. 1994;191:633–638.
58. Gatalica Z. Immunohistochemical analysis of apocrine breast lesions.Consistent over-expression of androgen receptor accompanied by the lossof estrogen and progesterone receptors in apocrine metaplasia and apo-crine carcinoma in situ. Pathol Res Pract. 1997;193:753–758.
59. Sapp M, Malik A, Hanna W. Hormone receptor profile of apocrine lesionsof the breast. Breast J. 2003;9:335–336.
60. Moinfar F, Okcu M, Tsybrovskyy O, et al. Androgen receptors frequentlyare expressed in breast carcinomas: potential relevance to new therapeuticstrategies. Cancer. 2003;98:703–711.
61. Catzavelos C, Bhattacharya N, Ung YC, et al. Decreased levels of thecell-cycle inhibitor p27Kip1 protein: prognostic implications in primarybreast cancer. Nature Med. 1997;3:227–230.
62. Lakhani SR, Slack DN, Hamoudi R, et al. Detection of allelic imbalanceindicates that a proportion of mammary hyperplasia of usual type areclonal, neoplastic proliferations. Lab Invest. 1996;74:129–135.
63. Lininger RA, Zhuang Z, Man Y, et al. Loss of heterozygosity is detectedat chromosomes 1p35-36 (NB), 3p25 (VHL), 16p13 (TSC2/PKD1), and17p13 (TP53) in microdissected apocrine carcinomas of the breast. ModPathol. 1999;12:1083–1089.
64. Washington C, Dalbegue F, Abreo F, et al. Loss of heterozygosity in fi-brocystic change of the breast: genetic relationship between benign pro-liferative lesions and associated carcinomas. Am J Pathol 2000;157:323–329.
65. Jones C, Damiani S, Wells D, et al. Molecular cytogenetic comparison ofapocrine hyperplasia and apocrine carcinoma of the breast. Am J Pathol.2001;158:207–214.
Adv Anat Pathol • Volume 11, Number 1, January 2004 Apocrine Lesions of the Breast
© 2003 Lippincott Williams & Wilkins 9