Embed Size (px)
Citation preview

THE TOOTH-COLOURED INLAY/ONLAY RESTORATIONS- A REVIEW
M Abdul Razak. The Tooth-Coloured /nlay/OnlayRestorations, Annals Dent Univ Malaya /998; 5: /7-23
ABSTRACTMuch interest has been generated in tooth-co louredinlays/onlays especially with patient's concern for estheticappearance and the dentist's appreciation for additionalstrength of the restored tooth, together with bonding. Manytypes of tooth-coloured inlay/onlay restorations are availablebut none have undergone extensive and long term research.The different types of inlay/onlay restorations together withsteps in their preparation are presented in this paper.
Keywords: Tooth-coloured inlay/onlay restorations
INTRODUCTIONCurrently, a dentist is provided with many options forrestoring a posterior tooth, depending on the clinicalsituation, esthetic requirements, patient's ability to pay andother factors.
These options include (Table I):AmalgamGoldApatiteCeramicsComposites
A recent study (I) has shown that mercury, which isreleased by amalgam fillings in monkeys has induced anincrease in mercury- and antibiotic-resistant bacteria in theoral and intestinal floras. This has drawn widespread public-ity in the United States. The Swedish National Board ofHealth and Welfare in August 1992 recommended its gov-ernment to reduce the use of amalgam by July 1995, espe-cially in teenagers and children. The Austrian Ministry forHealth has submitted a recommendation that amalgam fillingsnot be used in pregnant women and by 1995 not be used inchildren under 14 years of age (2). An increasing awarenessof the risk of mercury to health and the environment has ledsome patients to reject amalgam as a restorative material.While gold inlays and onlays have excellent durability andbiocompatibility, they can be considered unsuitable by manypatients for esthetic reasons.
At present, the use of direct posterior compositesremains restricted. Even though wear resistance can beachieved with the fine particle hybrid composites suitable forocclusal stress-bearing restorations, restoring posterior teethwith sufficient marginal integrity can still be difficult.Despite the application of the acid etch technique, microleak-age does still occur in Class II cavities because of shrinkagestresses during polymerization. The marginal integrity can beimproved by use of light-curing with the incremental tech-nique. However, this needs considerable clinical effort. Mostresearchers therefore agree that direct posterior composite
Abdul Aziz Abdul Razak
Associate ProfessorDepartment of Conservative DentistryFaculty of DentistryUniversity of Malaya50603 Kuala LumpurMalaysia
restorations should be restricted to occlusal and small two orthree surface cavities (3-5).
The patient's concern for an esthetic appearance and thedentist's appreciation of the additional strength of therestored tooth, and from acid etching and bonding, havegenerated much interest in the tooth-co loured inlays andonlays. Many researchers and clinicians have the opinion thatesthetic inlays and onlays are suitable as an alternativerestoration for moderately broken down posterior teeth (6-9).
The cavity design principle for the tooth-colouredrestorations differ from that of gold inlay/onlay preparationswhere all axial walls should be flared between 10° to IS°,without any bevels. The increased taper of the axial wallsallows easier placement and removal of the restoration dur-ing the try-in stage, but the taper should not be exaggeratedso as to unnecessarily remove additional tooth structure. Allinternal line angles should be rounded to reduce stress-bear-ing areas and there should be no undercuts. Even if there areundercuts within the dentine, this can be blocked out with aglass-ionomer cement prior to the final preparation andimpression. Alternatively, it can be blocked out in the labo-ratory, on the die, prior to the fabrication of the restoration.During the seating procedure, this space will be filled andbonded with the composite resin cementing agent, restoringcuspal stiffness and strength to the entire tooth. This strength-ening effect is caused by the dual bonding of the compositeresin to the tooth enamel and to the etched inlay restoration,thus not only providing support for the compromised cuspsbut also effectively sealing the margins.
All margins for onlays or large inlays should be cham-fered or butt-joined. The minimum isthmus width required is2.0 mm, while the minimum depth from the opposing sup-porting cusp is 1.5 mm and the wall thickness should be aminimum of 1.0 mm of material for adequate strength.
TYPES OF TOOTH-COLOURED INLAYS/ONLAYS.There are many types of tooth-coloured inlay/onlay restora-tions available at present but none has been the focus ofsignificant long term research. However, most of thesematerials have been used in dentistry for some otherpurposes.
1. APATITEIn 1986, casting of apatite, which is similar in nature to thecomposition of enamel was developed and called Cerapearl
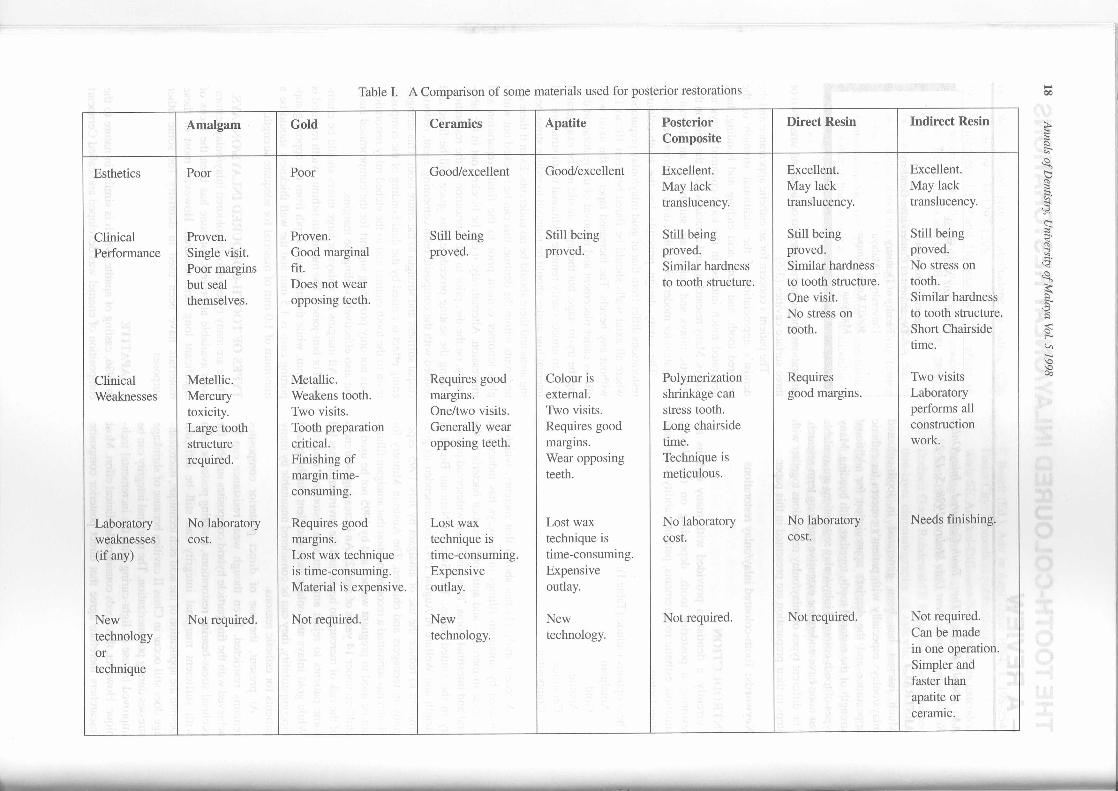
Table I. A Comparison of some materials used for posterior restorations
Amalgam Gold Ceramics Apatite Posterior Direct Resin Indirect ResinComposite
Esthetics Poor Poor Good/excellent Good/excellent Excellent. Excellent. Excellent.May lack May lack May lacktranslucency. translucency. translucency.
Clinical Proven. Proven. Still being Still being Still being Still being Still being
Performance Single visit. Good marginal proved. proved. proved. proved. proved.Poor margins fit. Similar hardness Similar hardness No stress onbut seal Does not wear to tooth structure. to tooth structure. tooth.themselves. opposing teeth. One visit. Similar hardness
No stress on to tooth structure.tooth. Short Chairs ide
time.
Clinical Metellic. Metallic. Requires good Colour is Polymerization Requires Two visits
Weaknesses Mercury Weakens tooth. margins. external. shrinkage can good margins. Laboratorytoxicity. Two visits. One/two visits. Two visits. stress tooth. performs allLarge tooth Tooth preparation Generally wear Requires good Long chairside constructionstructure critical. opposing teeth. margms. time. work.required. Finishing of Wear opposing Technique is
margin time- teeth. meticulous.consuming.
Laboratory No laboratory Requires good Lost wax Lost wax No laboratory No laboratory Needs finishing.
weaknesses cost. margms. technique is technique is cost. cost.(if any) Lost wax technique time-consuming. time-consuming.
is time-consuming. Expensive ExpensiveMaterial is expensive. outlay. outlay.
New Not required. Not required. New New Not required. Not required. Not required.
technology technology. technology. Can be made
or in one operation.
technique Simpler andfaster thanapatite orceralll1c.
(Kyocera International Inc.) (10). The technique is similar tothat of cast ceramics. Like cast ceramic, cast apatite is nottooth coloured and therefore needs pigments to be fired ontothe surface of the restoration. Being a new material, not muchliterature has been reported on this system.
2. CERAMICSCurrent full-ceramic systems for inlay/onlay restorations canbe class)fied according to the manner of production of therestorations which would be vacuum-fired, cast, pressed orCAD-CAM produced.
(i) Vacuum· fired CeramicsCeramic inlays has been used since the early 1900s. (11, 12).However the new concept in fired ceramic inlay is the bond-ing of acid-etched porcelain restorations into acid-etchedtooth preparations. Although this technique is relatively new,considerable clinical experience has been gained of theporcelain veneer technique. It has not been well 'acceptedbecause of the problem of poor fitting margins.
The various steps in the preparation are: an impressionis made of the tooth preparation; a die is made from diestone; an impression of the die is made by the technician; arefractory investment is poured into the impression; sever-al bakes of low-fusing porcelain are fired into the refracto-ry die in increments until the correct tooth anatomy isformed; the inlay is then removed from the refractory die andfitted onto the stone die by selective grinding and alterations;the margins are finished before the rest of the refractoryinvestment is sandblasted away after staining and glazing;the inlay is then etched with a form of hydrofluoric acid,silanated and ultimately cemented into the acid-etched toothwith dual-curing composite resin cement.
(ii) Cast CeramicsThe first cast ceramic restorative material introduced wasthat of Dicor, introduced by Dentsply International anddeveloped by Dow Coming (13). Apart from inlays/onlays,this system has also been used for making crowns, laminateveneers, all-ceramic fixed partial dentures and cores forceramic crowns.
This technique has some similarities to that of the castgold procedure, whereby, a wax-pattern is made on a die,invested and then removed. Molten ceramic is then cast intothe mould; the inlay is allowed to mature in the oven andthen a surface sealer containing pigments is fired on theinlay.
Durable and esthetic restorations have been achievedwith cast ceramic inlays (14). The adhesive bonding ofenamel, composite and the ceramic inlay is achieved byconditioning and silanation of the fit surfaces of the inlay,together with acid etching of the enamel. The disadvantageof this system is that since its surface colour is only surface-stained, any grinding of the restoration will leave an opaquewhite area; an additional appointment is necessary to fit andadjust the contact area, anatomic form and occlusion prior tostaining; once it is stained, the surface cannot be remodifiedwithout affecting the esthetics.
The tooth-coloured inlay/onlay restorations - A review 19
(Hi) Pressed CeramicsA new material of the all-ceramic type is the IPS Empress(Ivoclar- Vivadent) which not cast but pressure-pressed andinjection moulded. It is a unique leucite-reinforced ceramic.This system uses high- temperature pressing of a precer-ammed glass ceramic with hydrostatic pressure in a vacuumunit. Restorations are waxed, sprued and invested in a spe-cial flask system. The pressed-ceramic restoration is tried onthe die and adjusted for contact and occlusion before beingfinished with microfine rotary diamonds.
Different types of ceramic ingots can be used in either theshaded or layered technique by pressing these materials in aspecial furnace to fill the invested mould. The pressed-ceramic material is somewhat translucent, so that the color ofthe underlying tooth structure can be transmitted through it.The ceramic pellets are therefore available in 7 differentdentinal shades. External staining can be done either bypainting with shade porcelain onto the base-coloured restora-tion or layering of the Empress anatomic coping for occlusaltranslucency and individual characterizations. The finalrestoration can be very esthetic and fit quite well. They canbe bonded easily into the preparations and finished rapidlyand provide nearly optimum esthetic results and wear char-acteristics.
IPS Empress has many advantages and its success can beattributed to the many different characteristics that make it anesthetic and precise material. It is reasonably easy to handle,has natural colours, optimum fit, good strength and an abra-sion factor similar to that of enamel (15).
(iv) CAD/CAM CeramicsIt was Mormann, Brandestini and Lutz (1987)(16) whodeveloped a computer aided milling system to make ceram-ic reconstructions. An example of a system, the Cerec 2,allows inlays/onlays, veneers and partial crowns to be pro-duced from ceramic materials, chairside, in one appoint-ment, without having to incur any laboratory costs or the con-struction of temporary restorations.
The cavity preparation is stereogrammetrically scannedimmediately after the preparation has been made. The minia-turized video camera in the scanning head allows the cavitypreparation to be seen at a higher magnification on the com-puter's screen. As soon as the dentist starts the measuring pro-cedure, the computer calculates the parameters necessary todetermine the third dimension. The registered data can besaved in the graphic system. The dentist supplies the addi-tional information necessary to define and construct theinlay. The computer uses the data points of the inlay seen onthe video screen to calculate its outline. Using this informa-tion, a microprocessor controls the production of the ceram-ic inlay in a miniaturized milling machine. The restoration iscut, using both a milling disc and a cylindrical diamondinstrument, from a preformed ceramic block within 4 to 8minutes with a diamond disc powered by a water turbine.
The restoration's occlusal morphology can be pro-grammed. The resulting fit (marginal width opening) of theinlays produced with the Cerec 1 system, for example,before cementation has been measured to be between 0.0 um
20 Annals of Dentistry, University of Malaya Vol. 5 1998
to 250 um (17) and did not show any dye penetrationafter fatigue stress and had good morphologic marginqualities (18, 19).
Cast ceramic inlays, whether laboratory-made orcomputer aided, are time-consuming and very expensive tomake.
(v) Reinforced Conventional PorcelainWhen large amount of tooth substances are lost, fabricationof a conventional porcelain restoration is somewhat difficult.Variation in porcelain thicknesses on different tooth surfacesresults in differences in sintering shrinkage deformation andpoor marginal adaptation.
Traditionally, an even layer of porcelain is created bybuilding up the cavity preparation with a base. However,some of these base materials such as glass ionomer cementare too weak for extremely large core builtups.
To overcome this problem, an impression of the unevencavity preparation is made and a cast with dies poured. A baseof one of the reinforced aluminous ceramic cores is first builtup in the large cavity preparation which will support the sur-face layers of porcelain in the subsequent firings and preventshrinkage.
One system that is reportedly stronger and more stablethan conventional porcelain is Hi-Ceram (Vident). A strongerglass-refilled ceramic system (In-Ceram, Vident) will effec-tively support large amounts of porcelain. These core mate-
rials are built as the base to the conventional ceramic and arestable, so that with subsequent firings, the uneven thicknessof the porcelain and the repeated firing process do not resultin distortion of the overlying ceramic.
4. COMPOSITE RESINIn comparison to the direct composite restorations, compos-ite inlays are characterized by improved physical andmechanical properties which are achieved by curing theinlays with different techniques after modelling (Table II &III).
In the inlay technique, polymerization shrinkage of thecomposite restorative occurs before bonding to tooth struc-ture (20). Any shrinkage that occurs is restricted to the smallfilm thickness of the composite material used for cementa-tion. This has led to the considerable improvement of themarginal integrity of the restoration. Tests on inlays made ofmodem fine particle hybrid composite showed that suchinlays are at least equal to ceramic inlays with respect toesthetics, marginal integrity, abrasion resistance and adhesionto calcified tissues (21, 22).
Composite inlays are less expensive to produce com-pared to ceramic and gold inlays. Since the technique is sim-ple and uncomplicated, this allows the composite inlay to bemade quickly with less effort and in cases where' the directimmediate inlays are made, this obviates the need for a tem-porary restoration.
Table II. Examples of some composite inlay materials.
MATERIALS TYPE OFMATERIAL
TYPE OFSYSTEMRECOMMENDED
METHOD OFCURING
belleGlass Hybrid
Brilliant Hybrid
ClearFil CR Hybrid
Concept Microfill
Conquest Hybrid
Dentacolor Microfill
EOS Microfill
Heliomolar Microfill
Herculite XRV Lab Hybrid
Marathon Microfill
P50 Hybrid
Prisma TPH Hybrid
Targis Ceramic-reinforced
Tetric Hybrid
True Vitality Hybrid
Visio-Gem Microfill
Indirect
DirectlIndirect
Indirect
Indirect
Indirect
indirect
Direct/Lndirect
Direct
Indirect
Direct
Direct
Direct/Indirect
Indirect
Direct
Direct/Indirect
Indirect
Light+Heat+Pressure
Light + Heat
Light + Heat
Heat + Pressure
Light+ Vacuum+Heat
W Light
Light + Heat
Light + Heat
Light + Heat
Light + Heat
Light + Heat
Light + Heat
Heat+ Vacuum+Pressure
Light + Heat
Light + Heat
Light + Vacuum
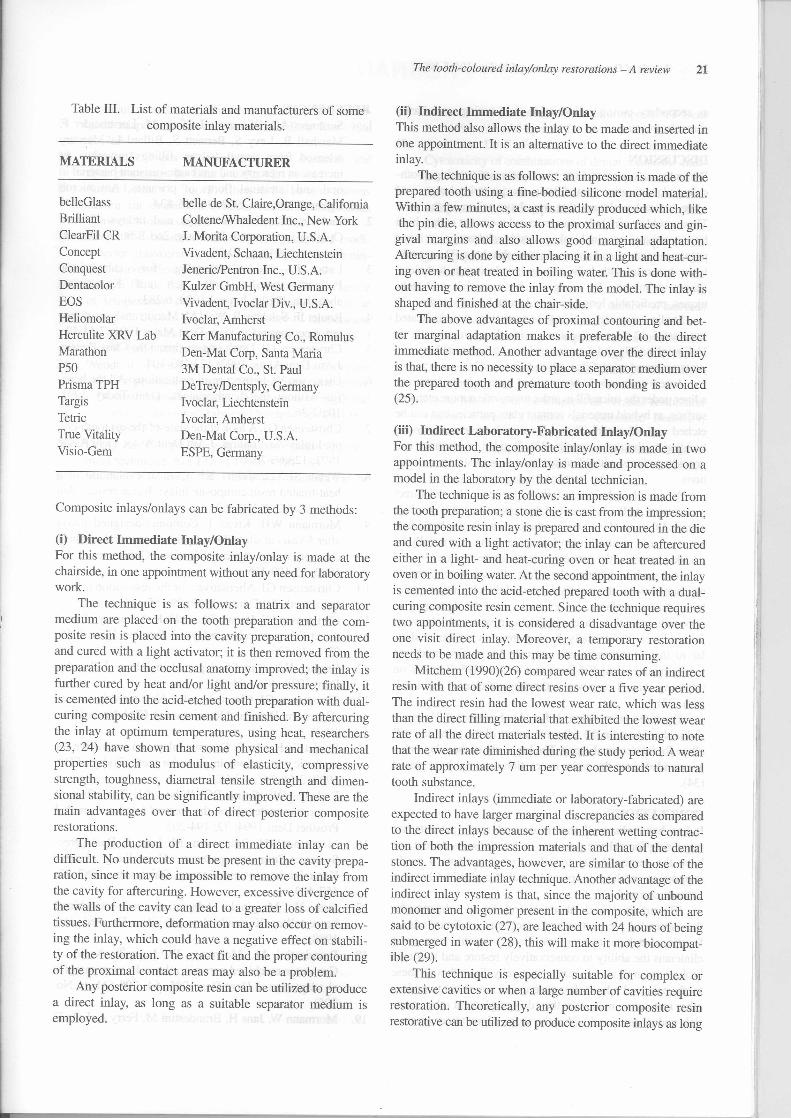
Composite inlays/onlays can be fabricated by 3 methods:
Table III. List of materials and manufacturers of somecomposite inlay materials.
(i) Direct Immediate Inlay/OnlayFor this method, the composite inlay/onlay is made at thechairside, in one appointment without any need for laboratorywork.
The technique is as follows: a matrix and separatormedium are placed on the tooth preparation and the com-posite resin is placed into the cavity preparation, contouredand cured with a light activator; it is then removed from thepreparation and the occlusal anatomy improved; the inlay isfurther cured by heat and/or light and/or pressure; finally, itis cemented into the acid-etched tooth preparation with dual-curing composite resin cement and finished. By aftercuringthe inlay at optimum temperatures, using heat, researchers(23, 24) have shown that some physical and mechanicalproperties such as modulus of elasticity, compressivestrength, toughness, diametral tensile strength and dimen-sional stability, can be significantly improved. These are themain advantages over that of direct posterior compositerestorations.
The production of a direct immediate inlay can bedifficult. No undercuts must be present in the cavity prepa-ration, since it may be impossible to remove the inlay fromthe cavity for aftercuring. However, excessive divergence ofthe walls of the cavity can lead to a greater loss of calcifiedtissues. Furthermore, deformation may also occur on remov-ing the inlay, which could have a negative effect on stabili-ty of the restoration. The exact fit and the proper contouringof the proximal contact areas may also be a problem.
Any posterior composite resin can be utilized to producea direct inlay, as long as a suitable separator medium isemployed.
MATERIALS
belleGlassBrilliantClearFil CRConceptConquestDentacolorEOSHeliomolarHerculite XRV LabMarathonP50Prisma TPHTargisTetricTrue VitalityVisio-Gem
MANUFACTURER
belle de St. Claire,Orange, CalifomiaColtenelWhaledent Inc., New York1. Morita Corporation, U.S.A.Vivadent, Schaan, LiechtensteinJeneric/Pentron Inc., U.S.A.Kulzer GmbH, West GermanyVivadent, Ivoclar Div., U.S.A.Ivoclar, AmherstKerr Manufacturing Co., RomulusDen-Mat Corp, Santa Maria3M Dental Co., St. PaulDeTrey/Dentsply, GermanyIvoclar, LiechtensteinIvoclar, AmherstDen-Mat Corp., U.S.A.ESPE, Germany
The tooth-coloured inlay/onlay restorations - A review 21
(ii) Indirect Immediate Inlay/OnlayThis method also allows the inlay to be made and inserted inone appointment. It is an alternative to the direct immediateinlay.
The technique is as follows: an impression is made of theprepared tooth using a fine-bodied silicone model material.Within a few minutes, a cast is readily produced which, likethe pin die, allows access to the proximal surfaces and gin-
gival margins and also allows good marginal adaptation.Aftercuring is done by either placing it in a light and heat-cur-ing oven or heat treated in boiling water. This is done with-out having to remove the inlay from the model. The inlay isshaped and finished at the chair-side.
The above advantages of proximal contouring and bet-ter marginal adaptation makes it preferable to the directimmediate method. Another advantage over the direct inlayis that, there is no necessity to place a separator medium overthe prepared tooth and premature tooth bonding is avoided(25).
(iii) Indirect Laboratory-Fabricated Inlay/OnlayFor this method, the composite inlay/onlay is made in twoappointments. The inlay/onlay is made and processed on amodel in the laboratory by the dental technician.
The technique is as follows: an impression is made fromthe tooth preparation; a stone die is cast from the impression;the composite resin inlay is prepared and contoured in the dieand cured with a light activator; the inlay can be aftercuredeither in a light- and heat-curing oven or heat treated in anoven or in boiling water. At the second appointment, the inlayis cemented into the acid-etched prepared tooth with a dual-curing composite resin cement. Since the technique requirestwo appointments, it is considered a disadvantage over theone visit direct inlay. Moreover, a temporary restorationneeds to be made and this may be time consuming.
Mitchem (I 990)(26) compared wear rates of an indirectresin with that of some direct resins over a five year period.The indirect resin had the lowest wear rate, which was lessthan the direct filling material that exhibited the lowest wearrate of all the direct materials tested. It is interesting to notethat the wear rate diminished during the study period. A wearrate of approximately 7 um per year corresponds to naturaltooth substance.
Indirect inlays (immediate or laboratory-fabricated) areexpected to have larger marginal discrepancies as comparedto the direct inlays because of the inherent wetting contrac-tion of both the impression materials and that of the dentalstones. The advantages, however, are similar to those of theindirect immediate inlay technique. Another advantage of theindirect inlay system is that, since the majority of unboundmonomer and oligomer present in the composite, which aresaid to be cytotoxic (27), are leached with 24 hours of beingsubmerged in water (28), this will make it more biocompat-ible (29).
This technique is especially suitable for complex orextensive cavities or when a large number of cavities requirerestoration. Theoretically, any posterior composite resinrestorative can be utilized to produce composite inlays as long
REFERENCES1. Summers AO, Wiremwn 1, Vimy M, Lorscheider F,
Marshall B, Levy S, Bennett S, Billard L. Mercuryreleased from dental 'silver' fillings provokes anincrease in mercury and antibiotic-resistant bacterial inoral and intestinal floras of primates. AntimicrobAgents Chemoter 1993; 38:825-834lackson RD. Esthetic inlays and onlays. CurrentOpinion in Cosmetic Dentistry. 2nd Edition, CurrentScience. 1994; pp. 30-39.Lutz F. Indikationskatalog furFullungsmaterialien, die sich aufabstutzen. Phillip lournal 1990; 6:283.Roulet IF, Salchow B, Wald M. Margin analysis of pos-terior composites in vivo. Dent Mater 1991; 7:44-49.Christensen, OJ. Don't underestimate the Class IT resin.1 Am Dent Assoc 1992; 123:103-104.Dickerson W. Indirect resin restorations: All the bene-fits without the disadvantages. Dent Today 1991;10:32-36.Christensen OJ. A look at the state-of-the-art tooth-col-ored inlays and onlays. 1 Am Dent Assoc Dent Assoc1992; 123:66-70.Wendt SL, Leinfelder KF. Clinical evaluation of aheat-treated resin composite inlay: 3-year results. Am1 Dent 1992; 5:258-262.Mormann WH, Krejci 1. Computer-designed inlaysafter 5 years in situ: Clinical performance and scanningelectron microscopic evaluation. Quintessence Int1992; 23:109-115.
10. Christensen 01. Alternatives for the restoration of pos-terior teeth. Int Dent 1. 1989; 39:155-161.
11. Christensen 01, Brown TA, Babb R. Accuracy of fit ofdirect-firing porcelain inlays. 1 Prosthet Dent 1969;22(1):46-53.
12. Brinker HA. Simplified porcelain inlays. 1 ProsthetDent 1978; 40(1):44-50.
13. Christensen 01, Christensen RP. New esthetic crowns(Cerestore, Dicor and Renaissance). CRA News 1986;10(3): I -2.
14. Roulet IF, Herder S. Ceramic inlays: an alternative foraesthetic restorations in posterior teeth. Todays FDA1990; 2(6): 1 C,4C-6C.
15. Ratledge DK, Smith BO, Wilson RF. The effect ofrestorative materials on the wear of human enamel. 1Prosthet Dent 1994; 72: 194-203.
16. Mormann WH, Brandestini M, Lutz F. Das Cerec-System: Computer gestutzte Herstellung direkterKeramikinlays in einer Sitzung. Quintessenz 1987; 38:457-469.
17. lans H. Marginale Adaptation von maschinellhergestellten Keramikinlays in vitro. Dr med dent1988.
18. Brandestini M, Mormann W, Lutz F, Krejci 1.Computer machined ceramic inlays: In-vitro margin-al adaptation. 1 Dent Res 1985; 64: 208 (Abstr. No.305)
19. Mormann W, lans H, Brandestini M, Ferry A, Lutz F.
22 Annals of Dentistry. University of Malaya Vol. 5 1998
as secondary curing and suitable dual-curing resin-basedcements are used.
DISCUSSIONPresently, many clinicians avoid or restrict using tooth-coloured restorative materials in the posterior because ofsome internal problems that may have arisen in the past.These problems include interproximal recurrent caries, highbite sensitivity, marginal leakage and breakdown, poor inter-proximal contacts and polymerization shrinkage. These prob-lems do occur with bulk composite placement technique(direct technique). By using suitable materials and tech-niques, predictable long-term results can be achieved.
Studies on posterior bonded restorations have indicatedsuccessful 12-year restorations with direct resin such asHeliomolar (30) and 8-year results with indirect, heat andpressure-cured microfills such as Concept (31).
A new technique is being tested using a hybrid resin ora liner under the microfill in order to provide a more etchablesurface, as hybrid materials contain glass particles that can beetched and silanated. This will provide micro mechanicalbonding to the resin cement (32). Bonded restorations canprovide patients with ideal functional and esthetic restora-tions.
As in all techniques, failure do occur. In the directrestorations, bulk placement of the composites may result ineventual failure. However in indirect restorations, bond fail-ure is often a result of microleakage and this can usually beavoided by using the proper cementation technique.
In a study comparing the effect of restorative materialson enamel wear, the results supported the claim that porce-lain occlusal surfaces, for example, may be damaging toopposing enamel surfaces. Empress crowns and inlays aresaid to be enamel friendly, having abrasion resistance simi-lar to that of natural tooth enamel. An in-vitro study onamalgam and enamel showed that wear of IPS Empress onopposing enamel cusp was in the range of enamel and amal-gam (33).
Fracture of restorations is found to be minimal. Howeverif this should occur, the adhesive nature of the materials willallow for intracoronal repair. The longevity of the inlay/onlayis extended since the entire restoration need not be replaced(34).
CONCLUSIONSIt has been observed that more and more patients arerequesting for esthetic posterior restorations. As dentist, wehave the responsibility to offer to our patients a tooth-supportive method to provide esthetic results that ourpatients demand.
This article reviews laboratory and clinical techniques forthe successful preparation and placement of direct/indirectfunctional esthetic restorations. These materials have givenclinicians the ability to conservatively restore and reinforcebroken-down tooth structure esthetically. Even though thesetooth- coloured inlay/onlay systems are not meant to replaceother restorative materials; they do complement other mate-rials and systems and widen the scope of treatment given.
2.
3.
4.
5.
6.
7.
8.
9.
zahnfarbeneKomposites
Computer-machined adhesive porcelain inlays: mar-ginal adaptation after fatigue stress. J Dent Res 1986;65:763.
20. Ruyter E. Types of resin-based inlay materials andtheir properties. Int Dent J 1992; 42: 139-144.
21. Krejci I, Reich T, Lutz F, Albertoni M. In-vitro testver-fahren zur evaluation dentaler restaurationssysteme.Schweiz Monastsschr 1990; 100:953-960.
22. Krejci I. Evaluation von AP.H-komposits und modi-fizierter glasskeramik als adhesive MOD- molarenin-lays. Unveroffentlicht, Universitat Zurich 1991.
23. Bausch JR, de Lange C, Davidson CL. The influenceof temperature on some physical properties of deLange C, Davidson CL. The influence of temperatureon some physical properties of dental composites. JOral Rehabil 1981; 8:309- 317 .
24. Wendt SL. The effect of heat used as a secondary cureupon the physical properties of three composite resins.I. Diametral tensile strength, compressive strength andmarginal dimensional stability. Quintessence Int 1987;18(4):265-271.
25. Donly KJ. Composite resin inlays: A single appoint-ment technique. Am J Dent 1990; 3:181-184.
26. Mitchem JC, Gronas DG. The use of dentures for the
The tooth-coloured inlaylonlay restorations - A review 23
evaluation of the abrasive wear of composites. J DentRes 1990: 69: 126 Special Issue Abstr. No. 142.
27. Anderson DAF, Ferracane JL, Zimmermann ER.Cytotoxicity of combinations of dental composite com-ponents. J Dent Res 1987; 66:133 Abstr. No. 214.
28. Ferracane JL, Condon JR. Rate of elusion of leachablecomponents from composite. Dent Mater 1990; 6:282-287.
29. Titus HW, Chan DCN. A comparison of gingival mar-ginal gap formation in composite inlays using three dif-ferent fabrication techniques. Texas Dent J 1992; 3: 13-16.
30. Belvedere P. Heliomolar: over a decade of successwith Heliomolar, Signature, Spring 1995: 14- 17.
31. Jackson R. Concept and Empress - an interview withDr. Ronald Jackson. Signature, Spring 1995: 6-13.
32. Dickerson WG. Improving the Concept restoration.Dent Today 1995,14:103-104.
33. Goulet MK. Use of the Empress all-ceramic restorationsystem. Current Opinion on Cosmetic Dentistry,Philadelphia 1997: 64-68.
34. Shannon A. Indirect posterior restorations: steps toclinical success. Current Opinion in CosmeticDentistry, Philadelphia 1997; 4: 40-44.