Embed Size (px)
Citation preview

The Victorian Infant Hearing Screening Program
Dr Melinda BarkerVIHSP Co-director
Maternal & Child Health Conference, October 2011

The Victorian Infant Hearing Screening Program (VIHSP) - historyVIHSP - since 1992• High risk status ascertainment (1992 – present)
+ behavioural screening via distraction test at 7-9m (1992 – 2005)
VicNIC 2003 - 2005• Pre-discharge AABR screening of all babies in
NICU and associated SCNs
Program of research into HL in childhoodPublic Health Hearing Group, Murdoch Childrens Research Institute/Royal Children’s Hospital

VIHSP Newborn Hearing Screening State-wide Rollout
Phase & Year
Hospitals % of Vic births
1
2005 & 2006
Tertiary maternity hospitals + co-located private hosps + RCH NICU
30%
2
2008 & 2009
Public metro maternity hospitals 57%
3
2009 & 2010
Public and private regional maternity hospitals
78%
4
2010 & 2011
(Remaining) private metro hospitals 100%

Basic principles of screening
• a screening test is not diagnostic: it is designed to identify those who are AT HIGHER RISK
• all screening tests will have a certain number of false positives and false negatives
• important that a positive result on a screening test results in referral to diagnostic testing
• condition being screened for should be an important health problem

Why screen for hearing loss in newborns?
• one in every 1000 babies will be born with a permanent, moderate or greater hearing loss in both ears that can be identified at birth
• without NHS, PCHI is detected late• intervention by 6 months = better communication skills, including
spoken language• technology to screen neonates is quick, easy, painless• diagnosis, early int & support services are available• potential to relieve burden of disability caused by
• language delays and deficits• academic delays and disadvantages• social impairments• economic disadvantages

The VIHSP screening process
VIHSP screen #1
Pass result in both ears Refer result in 1 or 2 ears
VIHSP screen #2
Pass result in both ears Refer result in 1 or 2 ears
NFA
NFAReferral to audiology
by VIHSP Area Coordinator
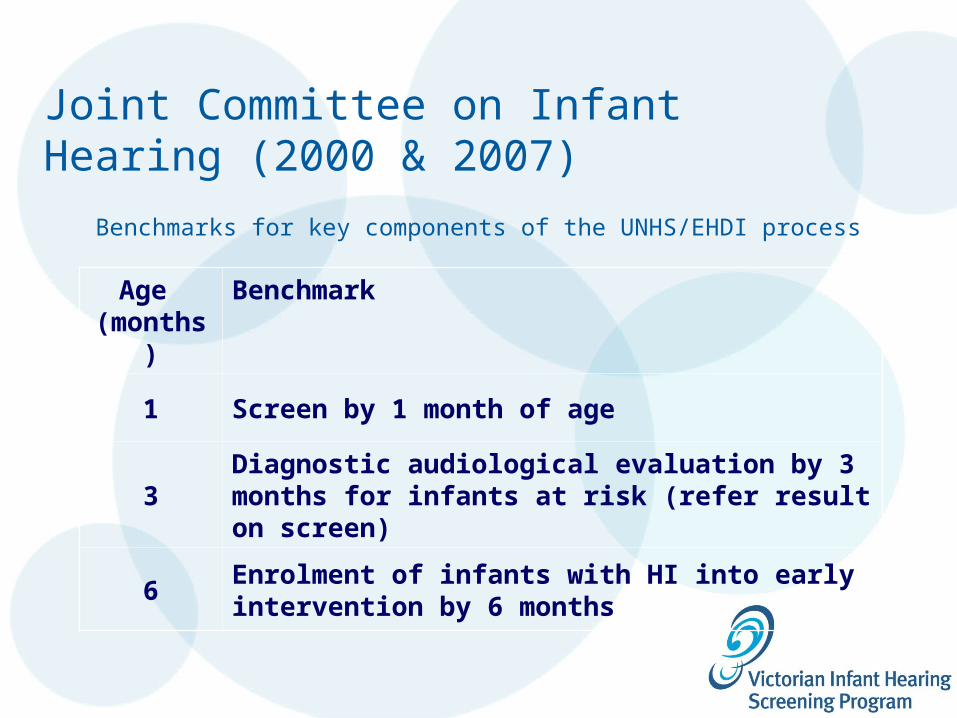
Joint Committee on Infant Hearing (2000 & 2007)
Benchmarks for key components of the UNHS/EHDI process
Age (months)
Benchmark
1 Screen by 1 month of age
3Diagnostic audiological evaluation by 3 months for infants at risk (refer result on screen)
6Enrolment of infants with HI into early intervention by 6 months

A hearing screen is one of the routine health checks babies have soon after birth. This is a quick and simple way to check the hearing of newborn infants.
Information brochure ‘Your baby’s hearing screen’ during one of the antenatal visits, in the pre-admission pack, or when the VIHSP screener visits after the baby is born.

Generally, the hearing screen will be done whilst the baby is still in hospital.
A hearing screener attends the hospital room and the screen is done at the bedside.
The hearing screener will explain the screen and will answer any questions parents might have.

If parents want their baby to have the hearing screen, they will be asked to sign a consent form.
The screen is not compulsory, however almost all parents choose to have their baby’s hearing screened.
The hearing screen is now the only routine hearing check that babies are offered.

The screen is quick and painless.
Most babies are not unsettled by the screen and most stay asleep in their cots whilst the screen is being
carried out.

The screener will put a sensor on the baby’s forehead, shoulder and neck. Two ear cups will be put over the baby’s ears and soft clicking sounds will be played to the baby.
As the baby hears those sounds, the sensors will send his/her responses to the screening machine.

We can do the hearing screen whilst the baby is being cuddled or breastfed.
The screener will give parents the results of the screen straight away.

A pass result means that the baby showed a clear response to the sounds played.
Hearing losses can develop at a later time; if parents have concerns about their baby’s hearing they can arrange to have another hearing check at an audiology clinic.
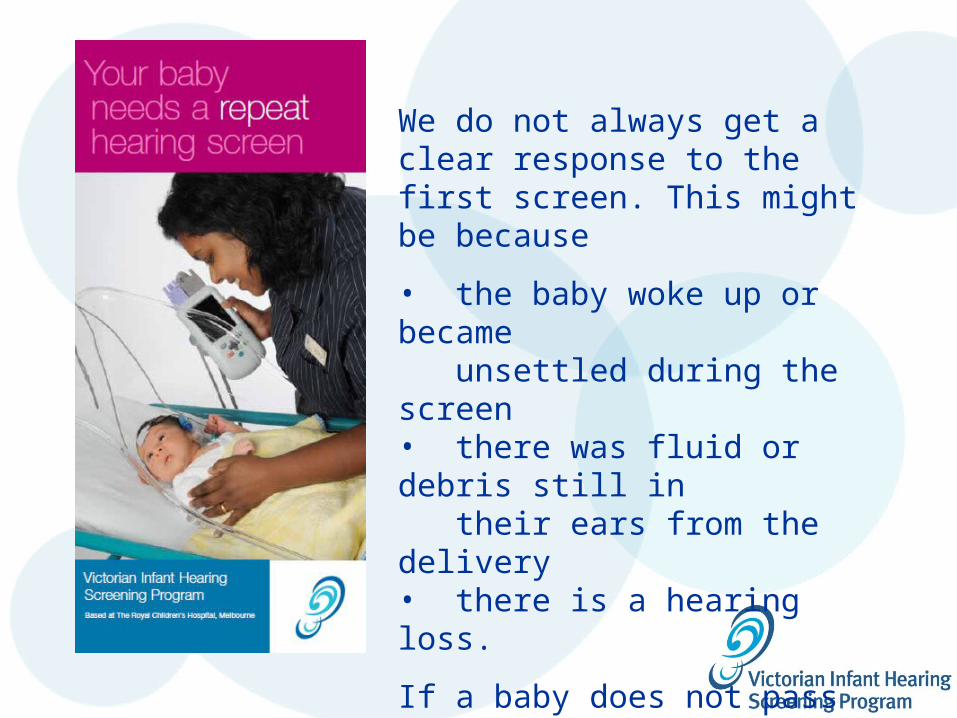
We do not always get a clear response to the first screen. This might be because
• the baby woke up or became unsettled during the screen• there was fluid or debris still in their ears from the delivery• there is a hearing loss.
If a baby does not pass their first screen, they have a repeat screen either before the baby goes home or as an outpatient.

A refer result means that, during two screens, we did not get a clear response from the baby to the sounds played.
This could be because:• the baby was unsettled during the screens• there is still fluid or another temporary blockage in his/her ears• the baby has a hearing loss.

The hearing screen does not diagnose a hearing loss.
A refer result does not always mean that the baby has a permanent hearing loss.
A refer result simply means that the baby needs to have a full hearing test at an audiology clinic.
If the baby needs to have a full hearing test, the VIHSP Area Coordinator at the hospital will arrange this appointment at the audiology centre of the parent’s choice.
What happens after a refer result?

Targeted surveillance: checking for risk factors
Hearing loss risk factors assessment via universal maternal and child health service.
Child Health Record used as the vehicle for targeted surveillance of infants at risk of progressive or acquired loss. Referral details recorded in CHR.

New Child Health Record
Birth Details page
Some risk factor information is recorded here

New CHR
In Birth Details sectionScreen Results Page 1
Screener records- Results (Pass or Refer)- Date of screen completion

New CHR
In Birth Details sectionScreen Results Page 2
Screener records- Result (Pass or Refer)- any risk factors present at time of screen

New CHR8m pageTargetted surveillance(risk factor follow up)

New VIHSP Referral Form

The VIHSP/MCH partnership VIHSP
recording of results of NHS referral coordination following NHS
MCH Following up on babies who have been referred Assisting to arrange screen for babies who missed it Risk factor ascertainment
Screened babies (passed screen): at 8m [“targetted surveillance”]
Language promotion Ongoing role in developmental surveillance

Why continue surveillance if a baby has passed the screen?
Hearing can change over time Risk factors can change over time
Therefore, Regardless of screen result, the MCH nurse
should review risk factors at the 6 -8 month visit and refer to audiology if any risk factors are present
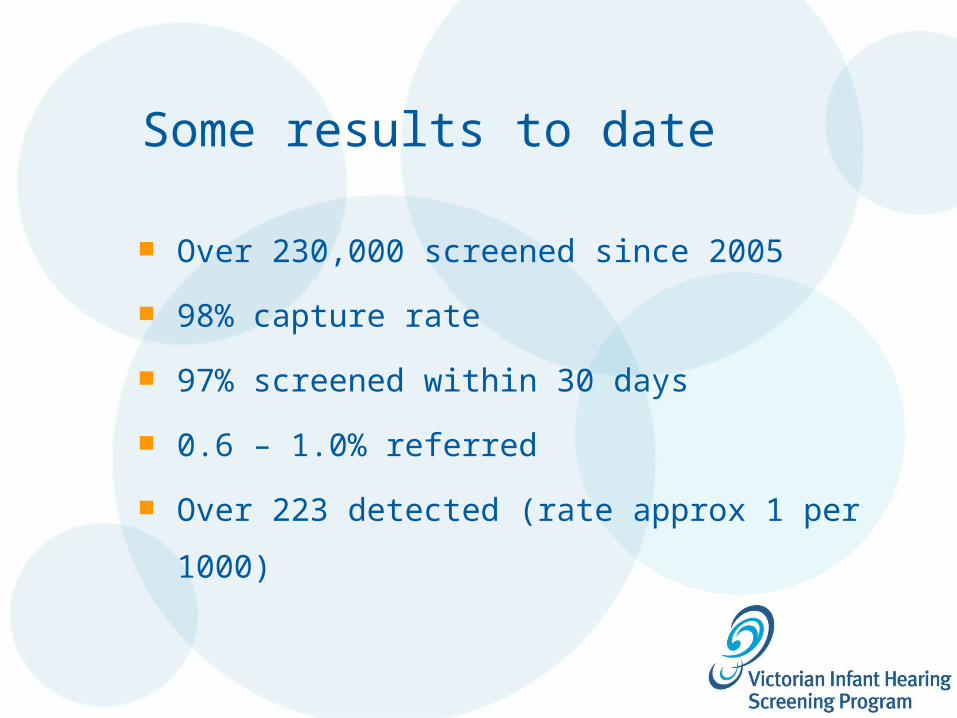
Some results to date
Over 230,000 screened since 2005
98% capture rate
97% screened within 30 days
0.6 – 1.0% referred
Over 223 detected (rate approx 1 per 1000)

Comparing Median Age at Diagnosis (in months) – Victoria
1.1
14.2
20.3
0
5
10
15
20
25
Pre-VIHSP (DOB 1989)
VIHSP Risk FactorScreening (DOB
1993)
VIHSP UNHS (DOB since Feb
2005)*

www.vihsp.org.au
Screen shot

New website LIVEhttp://infanthearing.vihsp.org.au

For more information:
The Victorian Infant Hearing Screening ProgramC/o Centre For Community Child Health
Royal Children’s HospitalFlemington Road Parkville, Vic 3052T: (03) 9345 4941F: (03) 9345 5049
E: [email protected] W: www.rch.org.au/vihsp