Embed Size (px)
Citation preview

The Oncology Care Model, Care Delivery & Payment Reform:
A Riddle Wrapped in Risk, Culture, & Opportunity
perspec'ves of two frustrated, op'mis'c, one liberal -‐ one conserva've, red state oncologists facing
High Noon





Market Trends
• ACA model = Value, not volume • Buy and bill, ASP + X% is eroding, Part B DemonstraJon threats • ProliferaJon of treatment pathways/preauthorizaJons • Desire for quality reporJng (PQRS, NCQA, QOPI) • IncenJves for EHR use, meaningful use • Payer interest in bundled payments/episodes of care • Accountable Care OrganizaJons and networks • Oncology-‐specific paJent centered medical homes • MACRA legislaJon: APMs & MIPs

Oncology AlternaJve Payment Explored
2009 UHC episodes pilot Eliminates % drug mark-‐up -‐ drug margin paid in advance. Total spend reduced 11% annual
2010 Aetna-‐Texas Oncology Oncology Medical Home demo – saves 12% annual
2012 COME HOME $19M CMMI grant to demonstrate value of OMH
2012 Oncology ACO BapJst-‐AMS-‐Florida Blue shared savings
2014 RCCA-‐Horizon Blue Cross Breast Cancer episodes bundled pricing
2014 Anthem Cancer Care Quality Program
$350 per treatment paJent per month for pathway compliance + care coordinaJon
2014 Aetna OMH Program Enhanced generic drug fees; shared savings
2014 MD Anderson – UHC Bundled prices for head & neck cancers. All care for one year. May add lung, prostate
2015 CMMI Comprehensive Care for Joint Replacement
MANDATORY in 75 markets: joint replacement bundled pricing. All costs 90 days post surgery
2016 CMMI Oncology Care Model Enhanced services to Medicare Beneficiaries undergoing chemotherapy

New Reimbursement Methodologies from MACRA
• MIPS incenJvizes quality over volume – Meaningful Use – Clinical PracJce Improvement AcJvity – PQRS – Resource Use
• APMs aims to increase accountability for both quality and total cost of care
– OCM – ASCO’s PCOP model – COME HOME Medical Home Project – ACOs

OCM Launch
• OCM launched July 1, 2016
– 196 parJcipaJng pracJces naJonally represenJng some 3,200 oncologists, average pracJce size 17 oncologists
– Plus 17 commercial payors
• Medicare’s interpretaJon of OCM is that it is the soluJon to higher quality of care at lower cost
• Commercial payers are already trying their own models and many are parJcipaJng in OCM (Anthem, Aetna, some Blues Plans)

Two New Sources of Revenue
• $160PMPM • Care management and compliance
MEOS Payments
• Percent of savings • Percent depends on quality measures
Performance-‐Based Payments
(PBP)

OCM – Oncology Care Model
§ Medicare’s new alternaJve payment model for oncology which aims to provide higher quality, coordinated cancer care, at the same or lower cost to Medicare.
§ The program includes a monthly episode payment (MEOS) for providing enhanced services to Medicare beneficiaries receiving treatment for a cancer diagnosis.
§ The enhanced services must include 24/7 access, paJent navigaJon, documented care plan, and clinical pathways.
§ There is also a shared savings component for pracJces that meet certain quality and performance measures while reducing the overall cost of care.
§ CMS will be monitoring pracJce performance through onsite audits and interviews with providers, staff, paJents and caregivers.
§ PracJce must report claims and quality data measures through the CMS OCM Data Registry.

OCM Basics • Goal: achieve beoer health, improved care, and smarter spending
for individuals with cancer who receive chemotherapy through appropriately aligned financial incenJves
• Eligibility: physician pracJces that provide care for oncology paJents undergoing chemotherapy for cancer (both independent medical group pracJces and hospital-‐affiliated pracJces)
• Term: 5-‐year program commencing July 1, 2016 (“Start Date”) • Par2cipa2on: 196 parJcipaJng pracJces and 17 parJcipaJng
health plans. Represents over 3,200 oncologists. Average OCM pracJce size = 17 oncologists

OCM Basics § Objec2ve: reduce the total cost of care during a 6-‐month
“Episode” to an amount below the pracJce’s “Target Price” § Episode: commences with the iniJaJon of chemotherapy, either
infused/injected (Part B) or oral (Part D) § Compensa2on: (i) Monthly Enhanced Oncology Services
payment (“MEOS”) of $160 x 6 plus (ii) performance-‐based payment (“PBP”) = actual expenditures/claims against Target Price (OCM payments are in addiJon to regular Medicare fee-‐for-‐service reimbursement)
§ Enhanced Services: see OCM PracJce Redesign AcJviJes

OCM Basics • Risk Arrangement: 1-‐sided risk to June 30, 2018; opJon to assume 2-‐sided
risk thereater; 2-‐sided risk model qualifies OCM as an APM under MACRA • OCM Discount: DeducJon from “Benchmark Price” to determine Target
Price: 4.0% 1-‐sided risk; 2.75% 2-‐sided risk • Prac2ce Redesign Ac2vi2es: OCM ParJcipants must implement the 6
PracJce Redesign AcJviJes • Clinical Data and Quality Measures: 12 OCM quality measures reported
quarterly through OCM Data Registry • Monitoring: parJcipants subject to lots of monitoring by CMS, including
on-‐site inspecJons

PracJce Redesign AcJviJes 1. PaJent access 24/7 to clinician who has real Jme access to
paJent’s medical record 2. AoestaJon and use of ONC-‐cerJfied EMR 3. UJlize data for ConJnuous Quality Improvement (CQI) 4. Provide core funcJons of paJent navigaJon 5. Document care plan in accordance with IOM 6. Chemotherapy treatment consistent with naJonally
recognized clinical guidelines
15

The Issue in a Nutshell…
How can a community oncology prac1ce transform to adapt to OCM? Dilemma:
Every aspect of the market is rapidly trending toward value-‐based APMs – most oncology groups prac2ce technically and culturally only, with structures to treat pa2ents in a Fee-‐for-‐Service (FFS) environment.

How do Oncologists Currently Technically Operate in a FFS Environment?
• Decentralized PaJent Intake
• Decentralized Phone Banks • Decentralized Symptom Management • Limited (within the pracJce) Psychosocial Support Mechanisms • Scheduling Driven by Individual Physician Templates • Limited Survivorship Structure • Standard PalliaJve Care/Hospice Processes

How do Oncologists Technically Operate in a FFS Environment? – Cont.
• Physicians trained and focused on fixing all problems in the exam room. Team-‐based care not the typical MO in the clinic
• “Regimen du jour” • Clinical focus -‐ treaJng disease, not healing lives • Nursing focus -‐ solve the immediate issue, not the bigger problem –
chemo room triage • Satellite clinic staff focused on “ownership of their paJents” • Limited coordinaJon with the paJent post ER visit or hospital stay • Limited paJent educaJon about what to expect from beginning to end
of their journey

Making the Necessary Changes…
Embark on a path to transform pracJce from the very tradiJonal approaches in treaJng paJents to healing lives and improving value – Becoming a Medical Home –
It is not just for Primary Care…

Medical Home Purpose
• Improved access to healthcare
• Increased paJent saJsfacJon • Improved medical outcomes
• Efficient delivery of care
• Reduced costs

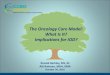
Large ReducJons in Avoidable HospitalizaJons
Are Possible
[VALUE] 2.567
2.067 1.604
1.273 1.119 0.969
0
0.5
1
1.5
2
2.5
3
2004 2005 2006 2007 2008 20009 2010
ER e
valu
atio
ns p
er p
atie
nt p
er
year
Year
Average emergency room (ER) evaluations at Delaware County Memorial Hospital of the Drexel Hill office population per
chemotherapy patient per year, 2004-2010
Source: Sprandio JD. “Oncology patient-centered medical home and accountable cancer care.” Community Oncology, December 2010

Sources of OMH-‐OCM Cost Savings Source % Cost Reduc2on
Drug pathways compliance 1.0% to 3.0%
Avoidable ER uJlizaJon 0.6% to 1.1%
Avoidable hospital admissions 4.0% to 7.0%
DiagnosJcs (imaging, lab) 0.2% to 0.5%
End-‐of-‐life care management 0.9% to 1.9%
Total potenJal savings 6.7% to 13.5%
(1) John D. Sprandio, MD, Consultants in Medical Oncology & Hematology. Oncology Pa2ent Centered Medical Home ® Analysis of OPCMH savings conducted by third party actuary 2010. (2) How Oncologists are Bending the Cost Curve. Oncology Times. January 10, 2013. (3) Changing Physician Incen1ves for Affordable, Quality Cancer Care: Results of an Episode Payment Model. Newcomer et. Al. Journal Oncology Prac2ce. July 8, 2014.
About 2/3 of
the savings comes
from avoidable
hospital events.

$2,700
$4,189
$3,656
Spending on Drugs, Imaging, and Hospitals Varies by More Than 60%
$- $5,000
$10,000 $15,000 $20,000 $25,000 $30,000
Quartile 1 Practices Quartile 2 Practices Quartile 3 Practices Quartile 4 Practices
Spending Per Medicare Beneficiary During Chemotherapy Episodes on Chemotherapy, Imaging, and Inpatient
Admissions, 2012
Chemotherapy Imaging Inpatient
Source: Clouagh, Patel, Riley, Rajkumar, Conway, Bach. "Wide VariaJon in Payments for Medicare Beneficiary Oncology Services Suggests Room for PracJce-‐Level Improvement." Health Affairs, April 2015

What is an Oncology Medical Home?
A Medical Home, also referred as a PaJent-‐Centered Medical Home (PCMH), is a team-‐based healthcare delivery model led by a physician. The model provides comprehensive and con2nuous medical care to pa2ents, with the goal of obtaining maximized health outcomes.

COME HOME Program (Community Oncology MEdical HOME)
• Barbara McAneny, M.D., InnovaJve Oncology Business SoluJons (IOBS)
• Name of the $19.8M CMMI grant • 7 U.S. pracJces • PaJents managed under OMH
structure – Centralized, protocol-‐driven triage nurses – Expanded office hours, 24/7 clinical staff access – Treatment pathway development and compliance – Laboratory/Molecular diagnosJcs efficiency
McAneny, J. Managed Care, 2013, SP41-42

ImplemenJng OMH Model Changing a pracJce technically and culturally
• Dedicated triage nurses, centralized phones • Scripted triage pathways • Expanded hours and dedicated triage clinic Jme • Navigators/Nurse educators • Coordinated emergency/hospital management • Treatment pathways • PaJent portal and communicaJon • Clinical trials support • Psychosocial distress evaluaJon • Survivorship clinic

Oncology Medical Home (OMH)
Commission on Cancer (CoC) Accredita2on Pilot Program

ParJcipaJng PracJces
1
2
3
4
56
8
7
9
10
1. Aus2n Cancer Centers 2. Center for Cancer and Blood Disorders 3. Dayton Physicians Network 4. New England Cancer Specialists 5. New Mexico Cancer Center 6. Northwest Georgia Oncology Centers 7. Space Coast Cancer Center 8. Hematology Oncology Associates of Central
New York 9. Oncology Hematology Associates
of Springfield 10. Oncology Hematology Care

OMH Key Points
• Much of the value gained from the OMH infrastructures comes through refinement of day-‐to-‐day paJent care processes resulJng in superior outcomes
• An OMH infrastructure gives the best opportunity for sustaining contracted bundled payments with risk sharing/shared savings, which are the anJcipated APMs in the near future

Aetna OMH Shared Savings Pilot
• Three pracJces, strong infrastructure support – Numerous pracJces now engaged in similar model
• Enhanced data sharing, benchmark data for shared cost savings
• Medical PaJent Management fee: – Reimbursement set up through TransiJon of Care
and S code billing
• Prior authorizaJon relief
• Quality metrics

Elements of Quality Measures ResulJng in Shared Savings
• ER visits (and costs)
• HospitalizaJon rates (and costs)
• Chemotherapy costs
• Adherence to evidence-‐based treatment guidelines (including treatment exceeding lines of therapy and documentaJon of off-‐pathways reasons)
• Cancer staging, performance status, pain assessment
• End-‐of-‐life metrics (ACP documentaJon, hospice enrollment, hospice length of stay)
• PaJent saJsfacJon

Medical Home Concluding Thoughts • Administra2ve burdens conJnue to adversely impact
oncology prac2ces • The costs of cancer care are unsustainable • MACRA – we now have law that will drive how we get paid
in the near future • For oncology to remain viable going forward, successful
management of the financial risks associated with APMs can be achieved by incorpora2ng OMH processes
• Prac2ce transforma2on is essen2al to prepare for APMs

Summary: FoundaJon for Success with AlternaJve Payment Models
• Triage pathways
• Centralized phone triage
• Expanded hours on weekend
• Dedicated schedule of paJent triage Jmes
• Treatment pathways
Beeer Care for Pa2ents
Lower Spending for Payers
Financially Viable Physician Prac2ces

OCM: Several other elements that are needed for opJmizaJon
• Know your QRUR • Episode clean periods – 0-‐60 days, 60+ days • Mail order drugs could cost your pracJce hundreds of thousands of dollars to do 90 day supply. • Learning about cancer episodes -‐ high variance = opportunity to show in savings. • Should you take 2 sided risk? – Think Reinsurance


Some Pricing Model ObservaJons • If the paJent had chemo <2 months before the episode started, your price goes up
11.4%. If the paJent had chemo 2 months-‐2 years before the episode started, your price drops by 21.5%.
• Dual eligibles get 25% higher prices. • PaJents with Part D coverage and the LICS get 17.9% higher prices even if they
have no Part D drugs during their episode. • PaJents who become eligible for Medicare during the prior year add 13.7% to
their prices. • For each comorbidity in the prior calendar year’s data, your price goes up about
12%. • PaJents enrolled in clinical trials where that fact is noted on claims get 25.5%
higher prices. • PaJents who have a single dose of radiaJon during the episode get 61.5% higher
prices. • Prices are 25%-‐70% higher if surgery occurs during episode.

Care Management Services
§ Chronic Care Management (CCM) § TransiJonal Care Management (TCM) § AccreditaJon Programs (QOPI, OMH)

Chronic Care Management (CCM)
§ TradiJonal and Advantage MCR paJents § 20 minutes of non-‐face to face contact with paJents/month § Two or more chronic condiJons to qualify § Care Plan – (all points within OCM) § CerJfied EMR § PaJent’s must sign a consent for parJcipaJon § Physician must discuss with the paJent and document discussion in their
medical record § PaJent’s enrolled in OCM will not be in CCM (can not parJcipate in both at the
same Jme)

TransiJonal Care Management (TCM)
§ Services furnished to paJents following discharge from an inpaJent hospital sezng.
§ Must contact paJent within 2 business days of discharge to schedule follow up visit, review discharge instrucJons, follow up on pending tesJng, provide educaJon and assess any needs prior to scheduled visit.
§ High complexity medical condiJon – follow up visit must occur within 7 days of discharge
§ Moderate complexity medical condiJon – follow up visit must occur within 14 days of discharge

AccreditaJon Programs • Commission on Cancer -‐ Oncology Medical Home Accredited (CoC OMH)
– Recognized by the CoC as promoJng high quality cancer care through our efforts around paJent engagement, expanded access, evidence-‐based care, comprehensive team-‐based care, and conJnuous quality improvement efforts. A key goal is to reduce ER visits/hospital admissions and ulJmately overall costs. Part of the accreditaJon process is an on-‐site visit by the CoC to audit and review compliance with these standards.
• American Society of Clinical Oncology (ASCO) – Quality Oncology PracJce IniJaJve CerJficaJon (QOPI)
– To be compliant with the American Society of Clinical Oncology (ASCO) Quality Oncology PracJce IniJaJve (QOPI) CerJficaJon Safety Standards around such things as chemotherapy administraJon, treatment planning, paJent consent and educaJon, monitoring and assessment, policy and procedures, and more. PracJces must also pass an on-‐site compliance audit and review.

A Pathway Through the Bundle Jungle Polite B, Jeff Ward, John Cox, Ray Page, et. al., JOP, June 2016
• Bundled payments transfer of risks from payer to provider
– Probability Risk: Out of provider’s direct control
• Random or unpredictable events
• Drug pricing
• Other doctor’s acJons
– Technical Risks:
• Drug/Regimen choices – Treatment Pathways
• Ancillary services
• Choosing Wisely Campaign
• PaJent triage Pathways

What you should be doing now to prepare for the 2019 MACRA Composite Score
• OpJmized your quality reporJng for PQRS, EHR IncenJve program, and Value Modifier
• Understand your Quality and Resource Use Report (QRUR) • Share, compare, and develop pracJce performance benchmarks
with like-‐minded groups (QCCA, NCCA, Oncology Circle, USON) • Make sure your pracJce data is accurate, Physician Compare • Maximize ICD-‐10 coding to the highest level of specificity, including
all comorbid problems • OpJmize your GPO, EHR and Pathways vendors pla|orms for OCM
data management

Summary: Components of Comprehensive Medical Oncology Payment Reform
1. ASCO’s PCOP payment model as an APM
2. The Quality Oncology Practice Initiative (QOPI)
3. ASCO’s “Choose Wisely” benchmarks
4. ASCO deemed Oncology Treatment Pathways
5. ASCO’s Value-Based Pathways
6. Care Coordination/Patient-Centered Medical Oncology Home
7. CancerLinQ – Data mgmt/rapid learning

• A new Texan…… – Different poliJcs but much fascinaJon with / agreement about care delivery

HHS Goal:
By 2018, 50% of all Medicare payments based on alterna've models

Template on which to Transform Oncology: CMMI’s Oncology Care Model
• CMS / CMMI Pilots – “Specialty Specific Payment Models”
• Oncology Care Model is “blended” approach focused on principles of ‘pracJce transformaJon’ derived from oncology medical homes – easily understood (at least on high level!)
• Centers for Medicare Medicaid InnovaJon (CMMI) / CMS – This provides benchmarks the ‘insJtuJon can understand’ – a contract – – An external authoritarian mover
• A model to follow – improves care short term / prepares for future change
• Whether a parJcipant or not – may be useful to transform clinics around same principles

Six OCM PracJce Requirements
1. PaJent access 24/7 to clinician who has real Jme access to pracJce’s medical record
2. AoestaJon and use of ONC-‐cerJfied EMR 3. UJlize data for ConJnuous Quality Improvement
(CQI) 4. Provide core funcJons of paJent navigaJon 5. Document care plan in accordance with IOM 6. Chemotherapy treatment consistent with
naJonally recognized clinical guidelines

UTSW / Parkland • 8 workgroups – with representaJves from across the
pracJce
• Workgroups organized around the core pracJce requirements
• Huge component is IT work….
• HUGE Culture issues

Our problems -‐-‐-‐-‐ (Opportunity)
– Accurate ID of paJents aoributed to model (Epic!!) – Deal with documentaJon / communicaJon of paJent calls / disposiJon
– Common triage scripts – Treatment plan (+ ongoing work d/t CoC requirements of treatment summary)
– PracJce reported measures

Our problems -‐-‐-‐-‐ (Opportunity) (2) – Two insJtuJons / One pracJce
• Employ of APPs – appropriate billing – ImplementaJon of Pathways (again across two insJtuJons / separate Epics)
– Structural organizaJon • Academic departments • Hospital departments – pracJce doesn’t control nursing / clerical / pharmacy / psychosocial supports
• Building accountability

Think beyond OCM a bit of preaching….
• Strategy / framework / a way of thought • … to relate OCM parJcipaJon into a higher order of goals…. A larger context

Porter • Our purpose in caring for paJents – to provide value
• Value classically = outcome / cost • Financial success is the result of delivering value – not an end in itself
• Path to success is to organize care delivery to improve paJent value

“Pa2ent” Value • Defined as a parameter for a paJent’s condiJon over the full cycle of care
• Outcomes inclusive of the full set of health results for the paJent (see ICHOM – InternaJonal ConsorJum for Health Outcomes Measurement)
• Costs are total care cost for the paJent’s condiJon – Most powerful lever at reducing costs is improving outcomes
• *** Yet we don’t know outcomes & don’t know costs

Porters’ Stratagem • Re-‐organize care around paJents condiJon in an environment that is
integrated • Measure outcomes and costs for every paJent • Pay providers differently – APM toward global payments • Integrate mulJ-‐site care delivery systems (aoack silos) • Expand geographic Reach – work together – leverage volume – drives
excellence • Enable IT pla|orms around measurement

High Noon
• Harken to the 1952 film with Gary Cooper / Grace Kelly…….

High Noon • Global payment for care of a defined populaJon of paJents to a
“System” (requires size and organizaJon) • System constructs prioriJes / Reflected in how it divides money • Requires knizng of providers across specialJes / sites of care in a
highly accountable (to whom?) system • Central focus on measuring / reporJng ‘quality’ ‘efficiency’ ‘access’
metrics • Emphasis on all aspects of the triple aim: safe, effecJve, Jmely
care for paJents; beoer health for populaJons; reduced per-‐capita costs
• Posit: Engine for change -‐ of structure / culture -‐ is risk • Our soul? (Gary Cooper)
• Physicians (&only) will be key to success for any ‘system’ (Resurgence of Physician Leadership?)

• QuesJons / Comments ???