Embed Size (px)
Citation preview

Hansen AR1*, Stanton T2, Hong MH3, Cohen EEW4, Mehanna H5, Chisamore M6, Turner D7, Yadavilli S7, Bell K7, Baccan C7, Leone R8, Chen H7, Zhou H7, Ellis C7, Ballas M7, Hoos A7, Rischin D9
1Princess Margaret Cancer Centre, Toronto, ON, Canada; 2St Joseph Health Cancer Center, Santa Rosa, CA, USA; 3Division of Medical Oncology, Department of Internal Medicine, Yonsei Cancer Center, Severance Hospital, Yonsei University College of Medicine, Yonsei University Health System, Seoul, Korea; 4Moores Cancer Center at University of California San Diego, CA, USA; 5Institute of Head and Neck Studies and Education, University of Birmingham, Birmingham, UK; 6Merck & Co., Inc., Kenilworth, NJ, USA; 7GlaxoSmithKline, Collegeville, PA, USA; 8GlaxoSmithKline, Stockley Park, Middlesex, UK; 9Peter MacCallum Cancer Centre and the University of Melbourne, Melbourne, Australia
INDUCE-3: A Randomized, Double-blind, Adaptive, Phase II/III Study of GSK3359609, an Inducible T-cell Co-stimulator Agonist Antibody, Plus Pembrolizumab Versus Placebo Plus Pembrolizumab for First-line Treatment of PD-L1–Positive Recurrent/Metastatic Head and Neck Squamous Cell CarcinomaPoster No. 252
Presented at the American Society for Clinical Oncology (ASCO) Congress, Virtual Scientific Program, May 29–31, 2020
AbbreviationsAE, adverse event; APC, antigen-presenting cell; CNS, central nervous system; CPS, combined positive score; CR, complete response; CTLA-4, cytotoxic T-lymphocyte–associated protein-4; CXCR5, C-X-C motif chemokine receptor 5; DCR, disease control rate; DoR, duration of response; ECOG PS, Eastern Cooperative Oncology Group Performance Status; EORTC QLQ-H&N35, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire – Head and Neck 35-Item Module; HNSCC, head and neck squamous cell carcinoma; HPV, human papilloma virus; HRQoL, health-related quality of life; ICOS, inducible T-cell co-stimulator; ICOS-L, ICOS ligand; IFN-γ, interferon gamma; IHC, immunohistochemistry; iPFS, immune-based PFS; ir, immune-related; iRECIST, immune-based Response Evaluation Criteria in Solid Tumors; IV, intravenous; MHC, major histocompatibility complex; MLR, mixed lymphocyte reaction; ORR, overall response rate; OS, overall survival; PD, progressive disease; PD-1, programmed cell death protein 1; PD-L1/L2, programmed death ligand 1/2; PFS, progression-free survival; PK, pharmacokinetics; PR, partial response; PRO, patient-reported outcome; PROMIS-PF-8c, Patient-Reported Outcomes Measurement Information System-Physical Function-Short Form; Q3/6/12W, every 3/6/12 weeks; RECIST, Response Evaluation Criteria in Solid Tumors; R/M, recurrent/metastatic; SD, stable disease; TCR, T-cell receptor.
DisclosuresINDUCE-3 study (NCT04128696; EudraCT 2019-002263-99) is funded by GSK and in collaboration with Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. ARH has had advisory/consultancy roles for Genentech/Roche, Merck, GSK, Bristol-Myers Squibb (BMS), Novartis, Boston Biomedical, and Boehringer Ingelheim; reports honoraria from Merck, AstraZeneca (AZ)/MedImmune, Pfizer, GSK/Novartis, and BMS; and reports research funding from Karyopharm Therapeutics, Merck, BMS, Boehringer Ingelheim, GSK, Novartis, Roche/Genentech, and Janssen. TS has received travel/accommodations/expenses from BMS and received honoraria from BMS, Ipsen, Axess Oncology, and Intellisphere. MHH has had advisory/consultancy roles for AZ, Merck, Roche, and Yuhan; holds stocks/shares in GI Cell and GI Biome; has received honoraria from AZ, Merck, and Roche; and received research funding from Yuhan. EEWC has had advisory/consultancy roles for ALX Oncology, Ascendis Pharma, Bayer, BioLineRx, BMS, Debiopharm Group, Dynavax Technologies, MSD, Merck, Regeneron, and Sanofi. HM is an employee of the Warwickshire Head and Neck Clinic; both he and an immediate family member have held leadership roles at Warwickshire Head and Neck Clinic; has had speaker bureau roles at MSD, Sanofi Pasteur, and Merck; has received travel/accommodations/expenses from Sanofi Pasteur, MSD, and Merck; holds stocks/shares in Warwickshire Head and Neck Clinic; has received honoraria and research funding from AZ; and has received research funding for his institution from GSK, MSD, Sanofi Pasteur, and Silence Therapeutics. MC is an employee of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, and holds stocks/shares in Merck & Co., Inc., Kenilworth, NJ, USA. DT, RL, HZ, and CE are employees of and holds stocks/shares in GSK. SY is an employee of, holds stocks/shares in, and holds patents/royalties/other intellectual property (IP) in GSK. KB is an employee of GSK and an immediate family member is an employee of Humana Pharmacy and holds stocks/shares in CVS. CB is an employee of GSK and a former employee of BMS and PARAXEL; has received travel/accommodations/expenses from BMS, PAREXEL, and GSK; and holds stocks/shares in BMS and GSK. HC is an employee of, holds stocks/shares in, and has received travel/accommodations/expenses from GSK. MB is an employee of, holds stocks/shares in, holds patents/royalties/IP in, has received travel/accommodations/expenses from, has received research funding from, and has held leadership roles at GSK; holds stocks/shares in BMS; and holds patents/royalties/IP in AZ. AH is an employee of, holds stocks/shares in and patents/royalties/IP in GSK, has had leadership roles at and owns stocks/shares in Imugene, and is a board member at Sabin Institute and Cancer Research Institute. DR reports travel/accommodations/expenses from Merck and reports research funding from Genentech/Roche, Merck, Regeneron, BMS, and GSK.
AcknowledgmentsEditorial support (in the form of writing assistance, assembling tables and figures, collating author comments, grammatical editing, and referencing) was provided by Victoria Hunter, MSc, and Becky Salisbury, PhD, at Fishawack Indicia Ltd, UK, and was funded by GlaxoSmithKline (GSK).
References1. Burtness B, et al. Lancet 2019;394:1915–28.2. Kok VC. Front Oncol 2020 Feb 28;10:268. 3. Hutloff A, et al. Nature 1999;397:263–6.4. Mak T, et al. Nature Immunol 2003;4:765–72.5. Mayes P, et al. Nat Rev Drug Disc 2018;17:509–27.6. Cavalieri S, et al. Cancer Treat Rev 2018;65:78–86.7. Brett S, et al. ESMO 2018 poster presentation: Abstract 1840P.8. Rischin D, et al. Ann Oncol 2019;30:v454–5.9. Angevin E, et al. J Clin Oncol 2020;38:(suppl;abstr 6517).10. Chen C, et al. Contemp Clin Trials 2018;64:238–42.
Please find the online version of this poster by scanning the QR code or via http://tago.ca/ASCO_13
Copies of this poster obtained through Quick Response (QR) Code are for personal use only and may not be reproduced
without permission from ASCO® and the author of this poster
Background INDUCE-3: An adaptive trial designed to evaluate if adding GSK3359609 to pembrolizumab as first-line treatment improves outcomes of patients with PD-L1–positive R/M HNSCC
Unmet need• Although outcomes in patients with R/M HNSCC have been
improved with first-line treatment with immunotherapies such as the PD-1 inhibitor pembrolizumab,1 there remains an unmet need for new treatment options as not all patients derive benefit due to inherent or emerging resistance to immune checkpoint blockade.2
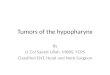
ICOS as a target in HNSCC• ICOS is a co-stimulatory receptor that promotes T-cell
proliferation and survival, making it a promising target for immunotherapy.3,4
• GSK3359609 is an ICOS agonist antibody with low/no T-cell–depleting effects via antibody-dependent cellular toxicity.5
• HNSCC has elevated expression of immune checkpoint modulators, including PD-1 and ICOS, and OS rates are higher in patients with HNSCC tumors that have high ICOS expression and/or are HPV+ compared with those that are HPV− or have low ICOS expression.6,7
Rationale for ICOS and PD-1 combination• Combining immunomodulatory agents targeting different components
of the cancer immunity cycle may generate more effective immune responses and overcome possible escape mechanisms.6
• Co-stimulators such as ICOS agonists may enhance the adaptive immune response and potentiate the antitumor activity of immunomodulatory and anticancer therapies.
– GSK3359609 has demonstrated antitumor activity in combination with PD-1 blockade in nonclinical models.8
This trial (NCT04128696) is
• In the HNSCC expansion cohort of the INDUCE-1 first-in-human study, GSK3359609 monotherapy and combination therapy with pembrolizumab had a manageable safety profile and showed evidence of single-agent activity in patients with PD-1/L1–experienced HNSCC.7 Follow-up data (below) are being presented by Angevin et al in Poster No. 178; GSK3359609 continues to show a promising signal in combination with pembrolizumab in PD-1/L1–naïve patients with HNSCC, with an ORR of 24%, durable responses (≥6 months), a median PFS of 4.2 months, and median OS of 13.1 months.9
Primary endpoints• OS by PD-L1 status
• PFS per RECIST v1.1 in PD-L1 CPS ≥1 population
Secondary endpointsKey secondary endpoints• iPFS in PD-L1 CPS ≥1 population• HRQoL assessments by PD-L1 status: time to deterioration in
EORTC QLQ-H&N35 pain domain and PROMIS-PF-8c physical functionOther secondary endpoints• PFS per RECIST v1.1 and iPFS in PD-L1 CPS ≥20 population• OS rate at 12 months and 24 months by PD-L1 status• ORR, DCR, and DoR per RECIST v1.1 by PD-L1 status• Frequency and severity of AEs• Dose modifications
!
Utilizing a 2-in-1 adaptive Phase II/III design,10 with the option to seamlessly expand the initial Phase II study into a Phase III study, without changing eligibility criteria, endpoints, or randomization scheme.
Adaptive decision analysis will inform if the study remains as a Phase II or Phase III design.
Up to
600 patientsPhase II/III
2 3Double-blindRandomized
Key inclusion criteria
• Age ≥18 years with R/M HNSCC consideredincurable by local therapies and no prior systemic therapy for R/M HNSCC
• Primary tumor of oral cavity, oropharynx, hypopharynx, or larynx
• Measurable disease • ECOG PS 0–1 • PD-L1 IHC CPS ≥1 and known HPV status(oropharyngeal cancer)
Key exclusion criteria
• Prior therapy with anti–PD-1/L1/L2 and/or anti-ICOS–directed agent
• Prior therapy ≤30 days or major surgery ≤28 days prior to randomization
• CNS metastases, active autoimmune disease, or immune deficiency
• Other invasive malignancy within 3 years
Exploratory endpoints • ORR, DoR, and DCR per iRECIST• PFS2 (time from randomization to 2nd objective
disease progression/death) per RECIST v1.1• PK analysis• Tumor- and blood-based biomarker analysis• Immunogenicity of GSK3359609• Symptomatic AEs measured by FACT GP5• HRQoL assessments• Germline genetic evaluations
Stratification factors:• PD-L1 status (CPS ≥20
vs CPS ≤1 to <20)• HPV status in oropharynx
sites (+ vs –/unknown)vs non-oropharynx sites
Day 1 Treatment end≤2 years or 35 cycles,
or until disease progression, death, or unacceptable toxicity
Arm 1
GSK3359609 (24 mg) + pembrolizumab(200 mg), IV Q3W
Arm 2
Placebo + pembrolizumab(200 mg), IV Q3W
SCREENING
Disease assessments Q6Wfrom Weeks 9 through 51
then Q12W thereafterPRO assessments Day 1,
Q3W to Week 21, then Q6W
TREATMENT≤35 cycles
Adaptivedecision
No treatment crossover permitted
Remain as Phase II
Expand to Phase III (N=600)
Ran
dom
izat
ion
(1:1
)Screening &stratification
R/M HNSCC
Consideredincurable bylocal therapies
T-cell priming/periphery Local antigen re-challenge Memory effector T cell
TCR
MHCCD28
CD80/CD86CD80/CD86
Maturation
MHC
CTLA-4
APC
Activation SurvivalProliferation
CD40LCXCR5 Granzyme B
T cell
TCR
ICOS
IFN-γ/othercytokines
ICOS-L
1.00
0.75
0.50
0.25
0.00
2000Days
600040000
OS
HPV+ & ICOShigh
HPV+ & ICOSlow
P=0.0023
HPV− & ICOShigh
HPV− & ICOSlow
HPV+ ICOShigh
HPV+ ICOSlow
HPV− ICOShigh
HPV− ICOSlow
4 (7)2 (5)
21 (11)19 (9)
0 (0)0 (0)8 (4)1 (0)
0 (0)0 (0)1 (1)0 (0)
60 (100)38 (100)198 (100)222 (100)
Number at risk: n (%)
50
0
−50
−100
irPD
irPR
irCRirPRirCR irSD irPD
Max
imum
cha
nge
from
ba
selin
e in
sum
of l
esio
ndi
amet
ers
(%)
Australia
Republic of KoreaUSA
Active sites
Canada Russian Federation
Trial status• INDUCE-3 is currently active and recruiting globally
25,000
20,000
15,000
10,000
5000
0
P=0.0036P=0.0090P=0.0009
**
Control
ICOS agonist
ICOS agonist +
pembrolizumabPembrolizumab
2 x control
IFN
-γ (p
g/m
L)***
ICOS agonist/anti–PD-1 combination enhances activity of anti–PD-1: MLR assay (IFN-g production)
*For questions, please contact the presenting author: [email protected]










![· ed b iariti the (Audit I Auc iced is co ecog in Dndit 10dif )irect ecog 'omm uth01 urop ecog ablic )rres] ecog: Isure 3rmit udit( ecog I a re](https://img.pdfslide.net/doc/110x75/5c605dfc09d3f20a6c8b635f/-ed-b-iariti-the-audit-i-auc-iced-is-co-ecog-in-dndit-10dif-irect-ecog-omm.jpg)