Embed Size (px)
Citation preview

Thrombocytopenia in neonates
Adapted from a presentation by Bronwyn Waddell, MS 4
NICU Sub-internship
9-17-04

Definition
Thrombocytopenia < 150,000/µL (150 x 109/L)– Rare in general population (<1%); 22% in NICU– Many healthy newborns b/w 100,000 - 150,000/µL.– Average platelet counts lower in preterm infants
• Reflects increase during gestation, from 187,000 to 274,000/µL at 15 and 40 weeks
– Severe reductions (<50,000/µL) and/or persistent thrombocytopenia can result in bleeding.
– Severe and/or persistent thrombocytopenia requires evaluation, even in an asymptomatic infant.

Evaluation of the thrombocytopenic neonate
Based on recognizing typical patterns– 1) Immune– 2) Infectious– 3) Genetic– 4) Drug-induced– 5) Disseminated intravascular coagulation– 6) Placental insufficiency – 7) Miscellaneous

Algorithm in Evaluation
Does thrombocytopenia fit pattern of pathophysiologic process? (Table 1)– Proceed to confirmatory testing
Further evaluation is indicated if– It does not fit one of these patterns– The dx is not confirmed by appropriate
testing– It is more severe/prolonged than fits dx– It does not respond to appropriate tx

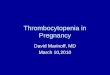
Category Subtype Severity Onset Resolution Mechanism
Immune
Alloimmune
Autoimmune
Severe
Moderate
Early
Early
Days - wks
Wks - mos
Incr. consumption
Infection
Bacterial
Viral
Fungal
Variable
Variable
Severe
Variable
Early
Late
1-7 days
Variable
2-7 days
Mixed
Genetic
disorder
Chromosomal
Bone marrow failures
Familial TCP
Moderate
Severe
Mild-mod
Early
Early
Early
Days - wks
Variable
Never
Decreased
production
Drugs Mod-severe
Late 8 days (med)
Variable
DIC Severe Variable Variable Inc consump
PIH/
IUGR
Mild-mod Early 7-10 days Dec prodxn
NEC Mod-sev Late 7-10 days Inc consump

Evaluation in early thrombocytopenia:
Mild to Moderate
Neonate with early thrombocytopenia (<72 hrs)– First distinguish b/w mild-mod and severe
• Mild (100-150 x 109/L) or moderate (50-100 x 109/L).
• PIH and IUGR are common causes of early thrombocytopenia among premature infants
• Generally, resolves spontaneously by day 7-10 of life
• Other labs include PT, PTT, D-dimers, cx

Evaluation in early severe thrombocytopenia
Severe/prolonged should trigger evaluation for other disease processes– Well-appearing infant: most common cause in
immediate post-natal period is immune thrombocytopenia from anti-plt Ab across placenta
– Ill-appearing infant: consider other causes• Sepsis, DIC (freq post severe perinatal asphyxia)• Viral infections and congenital toxoplasmosis
If tests fail to confirm dx, base further w/u on PE, response to plt transfusion, and mechanistic eval

Physical Examination Dysmorphic features suggestive of
chromosomal disorders provide dx clues:– Trisomy 21, 13, 18, Turner, Noonan
syndrome, DiGeorge/velocardiofacial syndrome
– HSM, abd masses (renal v thrombosis), forearm/thumb abnormalities (TAR/Fanconi’s)
– Decreased pronation/supination of forearm (congenital amegakaryocytic TCP w/proximal radial-ulnar synostosis)

Increased destruction Immune thrombocytopenia (0.3%)
– Neonatal alloimmune thrombocytopenia (NAIT) • Mom forms IgG class antiplatelet Ab against the "foreign" antigen (dad’s)
• Clinical features: mom asx, baby may have petechiae, ecchymosis• Labs: plts (often < 10,000/µL), antigen testing of parents’ plts,
mother's serum for antiplatelet alloantibody• Management: well, term infants transfused if plt <20,000/µL or if bld
– Transfusion threshold higher (<50,000/µL) in preterm/term infants who are ill or have risk factors.
• Initial evaluation: head CT to r/o hemorrhage (10-20%)• Adequate plt counts maintained during 1st 72-96 hrs (highest bld risk)• Tx with high-dose intravenous gamma-globulin (IVIG) may be effective

Increased Destruction:Immune Thrombocytopenia
Autoimmune thrombocytopenia:– Mediated by maternal Ab that react with maternal and infant platelets. – Occurs in maternal autoimmune disorders, including ITP and SLE– Dx apparent from mother's PMH and maternal thrombocytopenia– Mothers of infants with unexplained neonatal thrombocytopenia
autoimmune disorder?– Healthy women w/o hx of autoimmune d/o sometimes develop gestational
thrombocytopenia that usually is mild, transient, and benign. Clinical features: Petechiae, bruising, and bleeding.
– 90% infants have moderately severe thrombocytopenia in range of 20,000 to 50,000/µL
– Risk in infant correlates with severity of ITP in the mother:• Mother s/p splenectomy, plts < 50 in preg, or older sibling w/neonatal affects
– Plts decrease sharply during the several days after birth; nadir at 2-5 days Management: transfusion, IVIG, or prednisone for severe TCP or clinical bleeding
– Plt trx may not be as effective as in NAIT: autoAb usually react w/donor platelets

Drug related thrombocytopenia
Drug-related thrombocytopenia:– Mechanism is accelerated plt destruction caused by drug-
dependent Abs. – BM suppression may occur post chemo to mom or newborn
infant – Maternal thrombocytopenia post drug exposure mediated by IgG
Infant's platelet count should be monitored if exposed to quinidine, penicillins, digoxin, and antiepileptic drugs; indomethacin, heparin-induced thrombocytopenia less common
Management — If drug-associated thrombocytopenia is suspected, the offending agent should be withdrawn. – Transfusions should be given for low platelet counts
(<20,000/µL) or for bleeding. – If an immune-mediated condition is suspected, IVIG can be used
while awaiting confirmation.

Peripheral Consumption Hypersplenism: thrombocytopenia may be associated with an enlarged
spleen.– Underlying disorders: hemolytic anemia, congenital hepatitis, congenital
viral infection, and portal vein thrombosis – Management: Dx and tx of underlying cause.
• Plt transfusions PRN. Splenectomy if bleeding uncontrollable. Kasabach-Merritt: DIC, hemangiomas (kaposiform
hemangioendotheliomas)– shortened platelet survival caused by sequestration of plts in AVM.– Lesions noted at birth in approximately 50 % of patients
• Trunk (including retroperitoneum), arms and shoulder, lower extremity, and cervicofacial
– Severe thrombocytopenia, hypofibrinogenemia, elevated fibrin degradation products, and fragmentation of red blood cells
– Management: resolution of hemangioma, support hemostasis w/trx– Tx: prednisone, interferon alpha, surgery, embolization, vincristine,
cyclophosphamide, actinomycin D

Peripheral Consumption Disseminated intravascular coagulationthrombosis and hemorrhage.
– Complication of underlying illness, typically sepsis, asphyxia, MAS, severe RDS. – Dx suggested by associated illness, clinical presentation, and presence of
microangiopathic changes on the peripheral blood smear. – Confirming labs: prolonged PT and PTT, decreased fibrinogen, increased D-dimer– Tx: directed at the underlying cause of DIC: platelets and FFP to maintain plt
>50,000/µL and PT time within physiologic range. Fibrinogen concentration is maintained >100 mg/dL with infusion of cryoprecipitate.
Infection: bacterial, viral, and fungal organisms. – Bacterial mechanisms for thrombocytopenia include DIC, endothelial damage,
antibody-mediated, and platelet aggregation caused by adherence of bacterial products to platelet membranes.
• Decreased plt production due to injury to megakaryocytes in BM also possible– Viral: congenital rubella and cytomegalovirus.
• Mechanisms include platelet aggregation, loss of sialic acid from the platelet membrane caused by viral neuraminidase, and megakaryocyte degeneration.
• Splenomegaly and reticuloendothelial hyperactivity may play a role.
Management: tx underlying infection, platelet transfusions if associated bld

Peripheral Consumption Necrotizing enterocolitis: GI necrosis in 2-10% of infants <1500 g.
– thrombocytopenia from platelet destruction– In early stages, declining plts correlate with necrotic bowel and worsening
disease. – Levels of cytokines, including platelet activating factor (PAF), are increased
in premature infants with NEC and correlate w/ disease severity– Intestinal damage and inflammatory cell recruitment result from a cascade
of cellular events that may be mediated at least in part by PAF
Thrombosis: low plts often accompanies thrombosis in newborns. – Patients should be evaluated for a thromboembolic disorder if
thrombocytopenia cannot be explained by other conditions.

Decreased platelet production Often associated with genetic disorders: result in isolated thrombocytopenia or
syndrome
Thrombocytopenia-absent radius syndrome: severe thrombocytopenia and bilateral absent radii; thumbs are always present– Also hypoplasia or absence of the ulna, or abnormal or absent humerus. – Congenital heart disease, usually ASD or TOF, occurs in 1/3 of pts– plt <10,000 - 30,000/µL at birth-1st postnatal week in 59 %– Mortality is significant in neonate and early infancy, primarily due to ICH.
• If pt survives this period, spontaneous resolution usually occurs after 1st year
– Tx: supportive with platelet transfusions given when needed. Fanconi anemia: thrombocytopenia from FA is rare in the neonatal
period. – Pancytopenia typically diagnosed at six to nine years old – Condition recognized in newborn by characteristic congenital malformations in
60-70%:• Hypopigmented spots, abnormality of thumbs, microcephaly, café-au-lait spots, and
urogenital abnormalities; short stature of prenatal onset

Our DNCC Guidelines for platelet transfusion
Transfuse 10-15 mL/kg leukoreduced, irradiated platelets over 0.5-1 hour for:– Infants w/o signs of acute bld, but plt <20,000– Infant w/hemorrhage and plt <50,000– Consider w/bld and plt <100,000, esp ICH risk– Consider trx at predetermined value (20-100)
depending on infant’s status (d/w attending)

Transfusion precautions
Neonates should receive 10-15 ml/kg of CMV-safe (CMV Ab-) or leukoreduced plts– Increases count by >50 x 109
Neonates are at increased risk for transfusion-associated GVHD– Irradiated bld products for immunodeficiency,
intrauterine or exchange transfusions, or blood trx from relative or HLA-selected donor

Conclusion: Neonatal Thrombocytopenia
Common in NICU (sick and premature) Differentiate and tx based on severity Recognition of etiology based on typical
patterns associated with specific pathophysiologic processes
Work up and treat per algorithm and current clinical guidelines– Pursue immune etiology in infant
w/persistent thrombocytopenia

Sources/References Sola M. Evaluation and treatment of severe and prolonged
thrombocytopenia in neonates. Clin Perinatol; 2004:31(1) Saxonhouse M, Sola M. Platelet function in term and preterm
neonates. Clin Perinatol 2004;31(1) Andrew et al. A randomized, controlled trial of platelet transfusions in
thrombocytopenic premature infants. J Pediatr 1993;123:285-91. Murray NA. Evaluation and treatment of thrombocytopenia in the
neonatal intensive care unit. Acta Paediatr Suppl 2002;91:74-81. Sola, MC, Del Vecchio, A, Rimsza, LM. Evaluation and treatment of
thrombocytopenia in the neonatal intensive care unit. Clin Perinatol 2000; 27:655.
Jones, KL. Smith's Recognizable Patterns of Human Malformations, 5th ed. WB Saunders, Philadelphia 1997
Tomer et al. Autologous platelet kinetics in patients with severe thrombocytopenia. J Lab Clin Med 1991;118:546-54.
UpToDate Version 12.1: search term neonatal thrombocytopenia


![Senator(Joyce(Waddell The(Waddell Weekly(BulletinJan 16, 2016 · Senator Joyce Waddell's January 28, 2016, Newsletter Jyrita Moore (Sen. Joyce Waddell) [Waddelljla@ncleg.net]](https://img.pdfslide.net/doc/110x75/5f9c9a61763bb112073295e2/senatorjoycewaddell-thewaddell-weekly-jan-16-2016-senator-joyce-waddells.jpg)