Embed Size (px)
Citation preview

Thrombocytopenia in SGA Neonates
Israel Neonatology Association Robert Christensen, MD

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

Meberg A, Halvorsen S, Orstavik I. Transitory thrombocytopenia in small for dates infants, possibly related to maternal smoking. Lancet 1977:11;303-304
• 23 neonates weighing <10th % who, with no other explanation, had one or more platelet count <100,000/µL in the first days after birth.• Counts typically increased to >150,000/µL by DOL 15.• None had pathological bleeding. • Authors speculated that this variety of thrombocytopenia was the result of placental insufficiency-induced chronic hypoxia in utero.
Shuper A, Mimouni F, Merlob P, Zaizov R, Reisner SH. Thrombocytopenia in small for gestational age infants. Acta Paediatr Scand 1983:72;139-140
•14 SGA with one or more platelet count <100,000/µL in first week, and no other explanation for the thrombocytopenia. •Bone marrow aspirates on two where thrombocytopenia persisted more than 2 weeks. Erythroid hyperplasia and few megakaryocytes in both. •Elevated NRBCs at birth were common.•Postulated (as had Meberg et al.) that the condition was due to reduced platelet production associated with chronic intrauterine hypoxia.

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

Martha C. Sola-Visner and Matthew A. Saxonhouse
Chapter 11: Placental Insufficiency and Chronic Intrauterine Hypoxia
•Thrombocytopenia is common in SGA (? Incidence).•Mild to moderate thrombocytopenia (50 - 100K).•Nadir (low point) not defined.•Duration 2 weeks, sometimes longer (?).•Pathogenesis ? involves chronic intrauterine hypoxia. (Lower circulating megakarycytopoietic progenitors. Lower marrow megakaryocytes progenitors, n=3).•Best treatment and Outcome ?

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

O R I G I N A L A R T I C L E
Thrombocytopenia in late preterm and term neonates after perinatal asphyxiaRobert D. Christensen, Vickie L. Baer and Hassan M. Yaish
Transfusion. January 2015;55:187-196.

Aims: 1) Identify a group of thrombocytopenic SGA neonates where the thrombocytopenia was not a readily apparent variety (Sepsis, ECMO, DIC, NAIT). 2) In that group (termed the “thrombocytopenia of SGA”) to identify the incidence, nadir, severity, and duration of the thrombocytopenia, to determine whether it was more closely associated with preeclampsia vs. SGA status, to assess the responsible mechanisms, and to describe the outcomes.
Thrombocytopenia Among Small for Gestational Age Infants
RD Christensen, VL Baer, E Henry, GL Snow, A Butler, and MC Sola-Visner
Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

NICU admissions during the 9-year period studied (n = 24,036)
SGA (birth weight <10th %) (n = 3,964)
Thrombocytopenic (≥ 2 counts <150,000/µL) (n = 905)
31.5%
Had ≥2 platelet counts obtained during the first week (n = 2,891)
Not SGA (birth weight >10th %) (n = 20,072)
Thrombocytopenic (≥ 2 counts <150,000/µL) (n = 287)
10.0%
Not SGA, matched 1:1 with SGA infants (n=2,891)
Included as “Thrombocytopenia of SGA” (n = 803)
Excluded from further analysis (n=102) ● ECMO (n=28)* ● Aneuploidy (n=30)* ● Early onset bacterial sepsis (n=6) ● Congenital marrow failure syndrome (n=4) ● CMV (n=6) ● Alloimmune (n=2) ● DIC (n=8) ● Multiple malformation syndromes (n=18)*Three had ECMO and also trisomy 21

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?


Only moderate severity, nadir 4 days, ½ have a count >150,000 by 13-15 days

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?


Thrombocytopenia does not appear to be associated with PIH, but with SGA status.


Thrombocytopenia may be more severe with more severe growth (weight) restriction.

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?


MVP is similar to thrombocytopenias due to reduced platelet production (high MVP with accelerated platelet destruction).
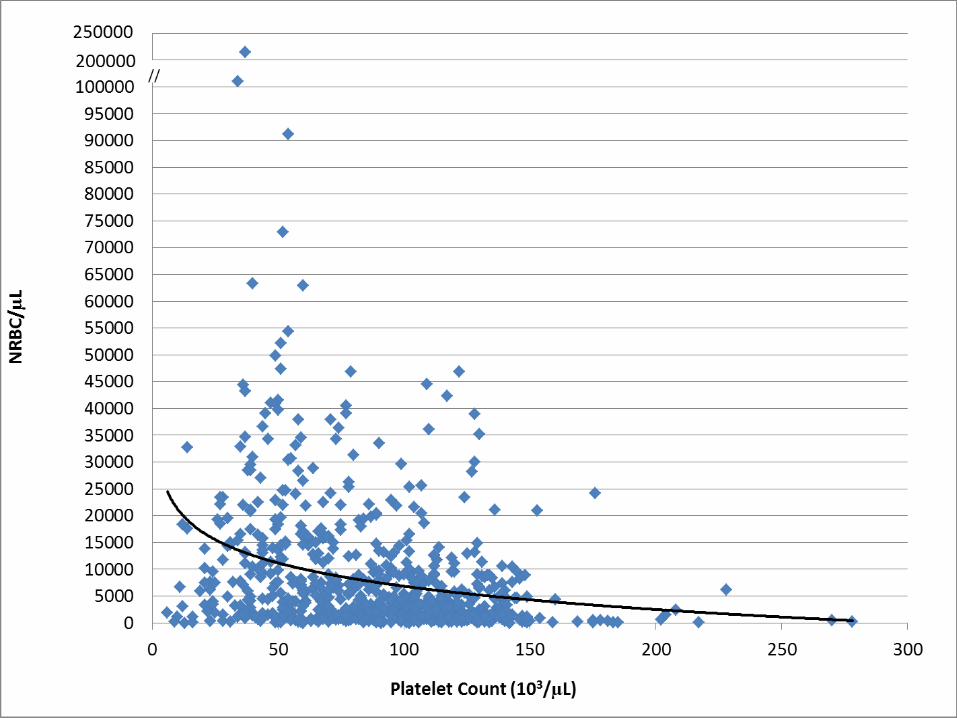

Similar to thrombocytopenia of perinatal asphyxia, may be associated with intrauterine hypoxia.


Response to transfusion is similar to thrombocytopenia from reduced platelet production (poor response with accelerated platelet destruction).

Thrombocytopenia of SGA is likely the kinetic result of reduced platelet production, resulting from intrauterine hypoxia.
Tpo deficiency? (3 of 3 cases)

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

Footnotes:•All thrombocytopenic SGA neonates with DIC who died had bleeding problems at the time of death, predominantly pulmonary hemorrhage.
•None of those with trisomy 18 or 13 who died had bleeding problems.
OUTCOME - DEATHSGroup Number Mortality Rate
SGA No Thrombocytopenia 1986 2%
SGA Thrombocytopenia 905 9% (p<0.0001 vs no thrombocytopenia)
•Thrombocytopenia with known cause (ECMO, DIC, EOS)
102 65% (p<0.0001 vs all other groups)
•The “Thrombocytopenia of SGA”
803 2%

•Ten SGA neonates had severe (<50K) thrombocytopenia that persisted for at least four weeks for which platelet transfusions were being administered.
•These 10 received 4 to 33 platelet transfusions. All but three transfusions were prophylactic for platelet counts in the range of 50,000 to 75,000/µL but with no signs of bleeding.
•Nine of these 10 were severely SGA (<1st % at birth).
OUTCOME – SEVERE PERSISTENT THROMBOCYTOPENIA

Birth weight (g)
SGA (%)
Gestational age @ birth (wks/days)
Maternal preeclampsia/
eclampsia/ HELLP
Lowest platelet count between four and six weeks (/µL)
Number platelet transfusions received
Outcome
350 <1st 24/0 No 48,000 21 Died at 6 months in NICU
406 <1st 22/6 HELLP 30,000 33 Died at home at 7 months
420 <1st 24/5 HELLP 23,000 31 Died at home at 17 months
470 <1st 26/5 Eclampsia 40,000 8 Lived480 <1st 23/6 Preeclampsia 38,000 11 Lived510 <1st 26/4 Preeclampsia 36,000 8 Lived565 <1st 27/0 HELLP 47,000 10 Lived
580 <1st 27/1 No 10,000 16 Lived
663 <1st
29/2 No 37,000 4 Lived
Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

Romiplostim ● Analog of thrombopoietin● Developed by Amgen under the trade name Nplate● FDA approved 2008 for long-term treatment for chronic ITP in adults who have not responded to other treatments.● The wholesale cost of romiplostim if administered weekly (adults) is about $55,000 per year.● IV or sub Q use only

Eltrombopag ● Small molecule agonist of the Thrombopoietin receptor ● Discovered as a result of research collaboration between GlaxoSmithKline and Ligand Pharmaceuticals.●FDA approved in 2008 for adults with ITP refractory to other treatments●Oral preparation only
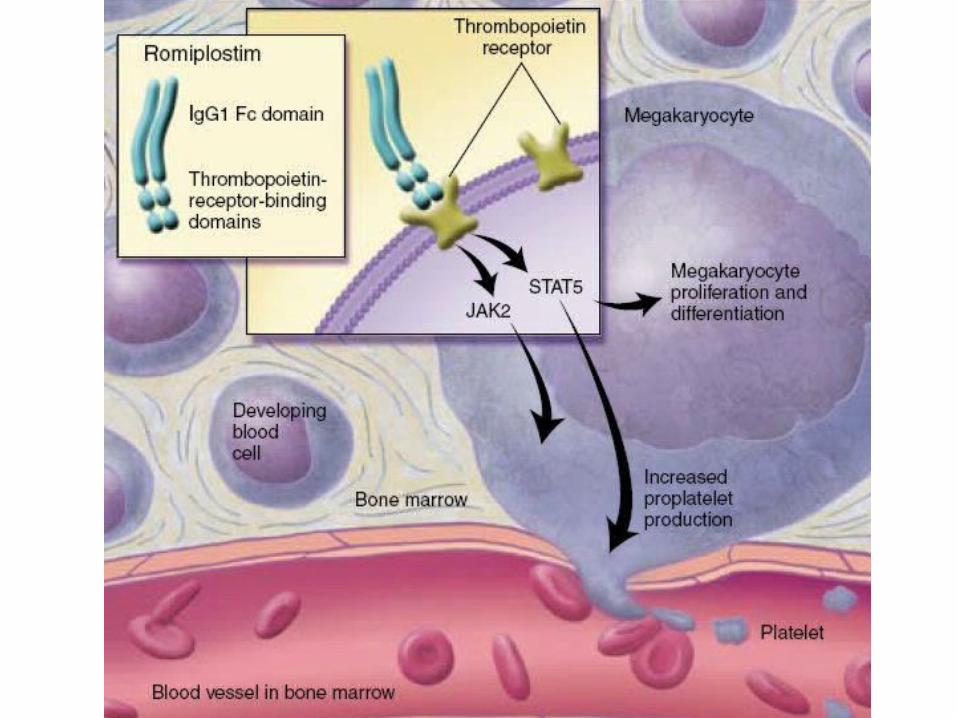
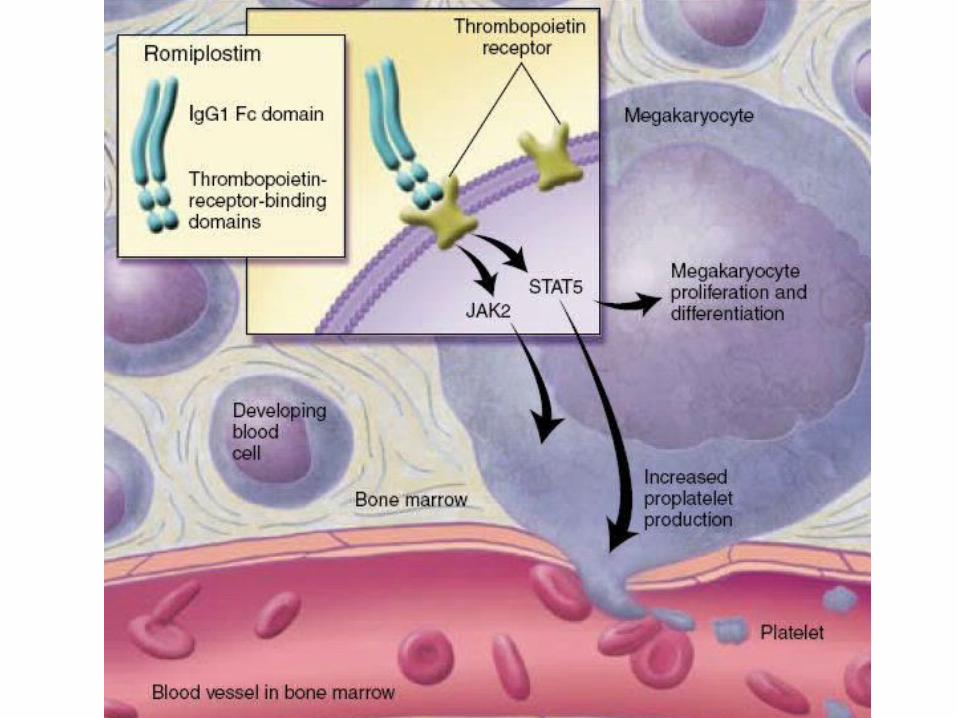

TPO-RECEPTOR AGONISTS1) Not rapid-acting (10 days)2) If severe persistent thrombocytopenia
could be predicted in the first days after birth, would TPO-receptor agonists have advantages over platelet transfusion?
3) Cost of one apheresis pl transfusion $1300

Predicted probability of platelet count < 50 @ 2 weeks
Gender……………………. Male 30%Gestation Age (weeks rounded down)…………… 23 Lowest Platelet Count in First 7 Days………………. 40
Calculate the odds that severe thrombo-cytopenia will persist beyond 2 wks

Outline1.Early reports2.What we DON’T know3.Nine-years of SGA neonates in the Intermountain
Healthcare NICUs4.Sorting out those with a recognized cause of
thrombocytopenia from those with “the Thrombocytopenia of SGA”
5.Incidence, Nadir, Duration6.Association with preeclampsia?7.Kinetic cause & Value of platelet transfusions8.Outcomes9.Are any candidates for Romiplostim?

Take-Home Messages1. 1/3 of SGA neonates will have early thrombocytopenia.2. 10% of these will have a “readily apparent” cause
(ECMO, DIC, EOS; high mortality rate…65%).3. 90% will have the “thrombocytopenia of SGA”.4. Low point = day 4.5. Typically increase to >150,000 by 2 weeks.6. Should not need platelet transfusions.7. Most severe (<1%) are likely to have lower counts and
longer durations.8. Can’t predict which will be severe and prolonged. 9. If still <50K, and receiving pl transfusions at 1 week,
should we measure serum TPO and talk about studying Romiplostim?

Thrombocytopenia in SGA Neonates
Thanks for your Kind Attention