Embed Size (px)
Citation preview

Thromboprophylaxis for PlacentalComplications: Perspectives in 2015
Nadine Sauvé, MDCanadian Society of Internal MedicineOctober 2015
No conflict of interest to declare

Objectives• After the conference, the participant will be able to:
• Use appropriate thrombophilia work-up for women at risk of placental complications.
• Identify women that could benefit from thromboprophylaxis to prevent placental complications.

Synopsis• Pathophysiology
• Thrombophilia screening
• Pre-eclampsia, late intrauterine fetal death, intrauterine growth restriction/small for gestational age, placental abruption• Role for LMWH? Role for ASA?
• Early recurrent pregnancy loss• Role for LMWH? Role for ASA?
• Conclusion: • Guidelines• What I am doing at present…
Pathophysiology
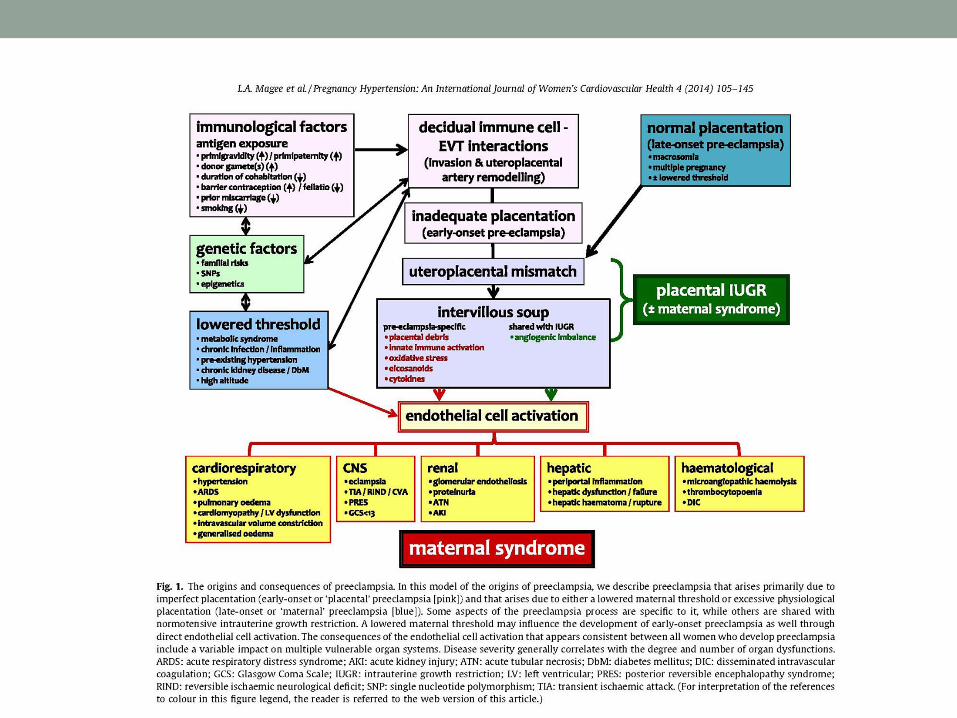

Pathophysiology• ASA and LMWH: antithrombotics, mitigation of
trophoblastic apoptosis.• LMWH: complement inhibitors.
• Before initiating these mesures, we must eliminate all other causes:• Maternal anatomy• Chromosomal• Fetal malformation • Infection in utero• Fetomaternal hemorrhage• Platelet alloimmunisation, erythroblastosis fetalis (Rh-negative)• Metabolic disorders (diabetes, thyroid dysfunction, etc.)• Other

Thrombophilias


Screening for thrombophilia• Prospective and retrospective studies: ACCP 2012
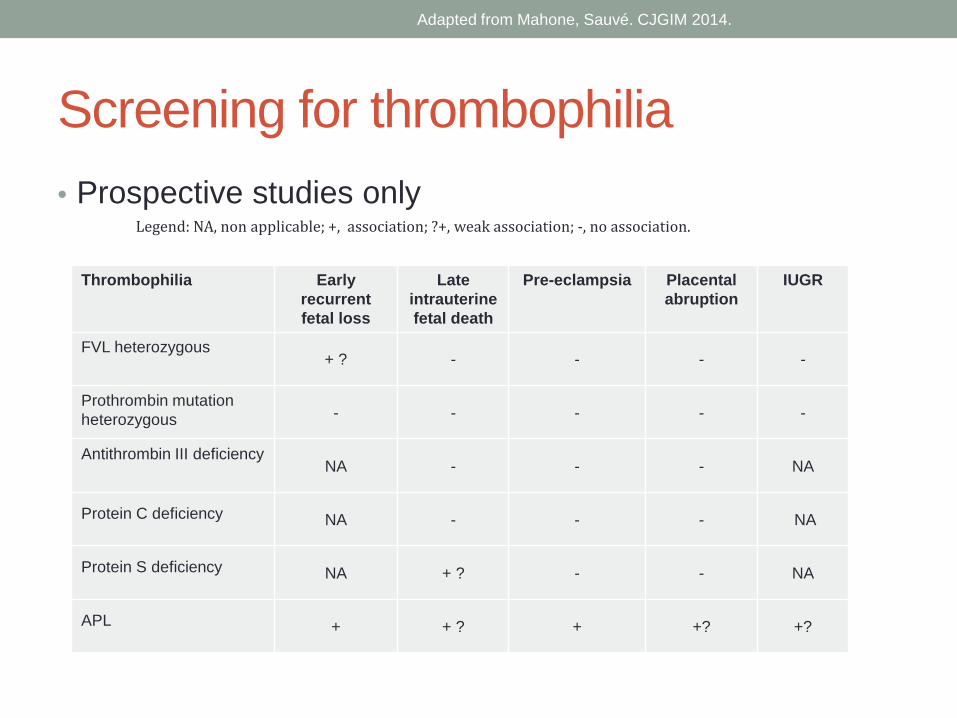
Screening for thrombophilia• Prospective studies only
Thrombophilia Earlyrecurrent fetal loss
Late intrauterine fetal death
Pre-eclampsia Placental abruption
IUGR
FVL heterozygous+ ? - - - -
Prothrombin mutation heterozygous - - - - -
Antithrombin III deficiencyNA - - - NA
Protein C deficiency NA - - - NA
Protein S deficiency NA + ? - - NA
APL + + ? + +? +?
Legend: NA, non applicable; +, association; ?+, weak association; -, no association.
Adapted from Mahone, Sauvé. CJGIM 2014.
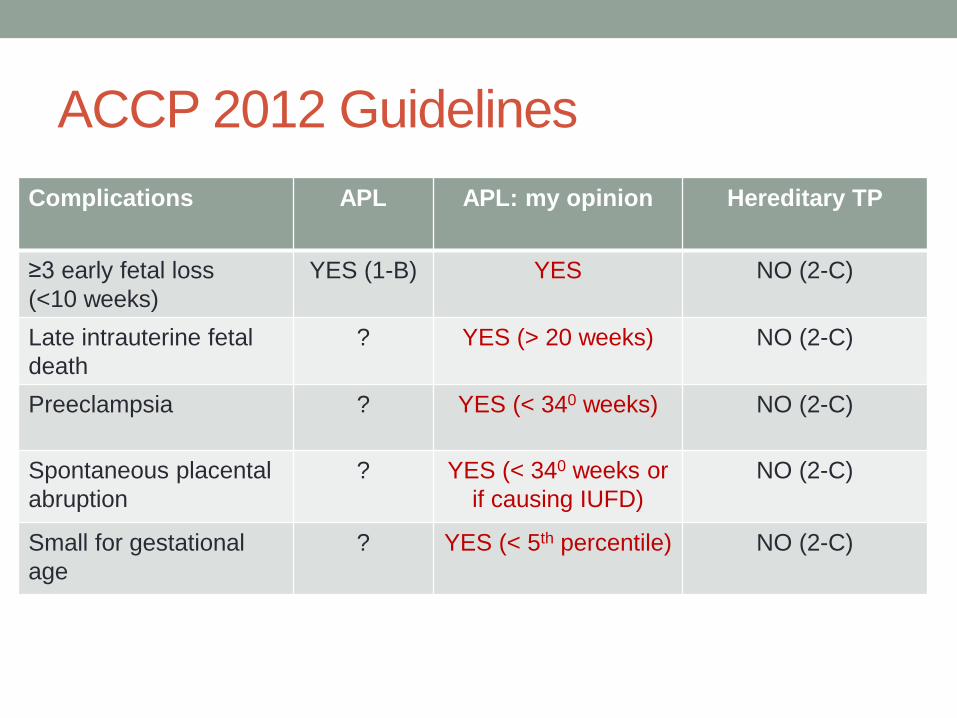
ACCP 2012 GuidelinesComplications APL APL: my opinion Hereditary TP
≥3 early fetal loss(<10 weeks)
YES (1-B) YES NO (2-C)
Late intrauterine fetal death
? YES (> 20 weeks) NO (2-C)
Preeclampsia ? YES (< 340 weeks) NO (2-C)
Spontaneous placentalabruption
? YES (< 340 weeks or if causing IUFD)
NO (2-C)
Small for gestational age
? YES (< 5th percentile) NO (2-C)

Placental complications






Placental complications (excluding recurrent early fetal loss)
• Pre-eclampsia (PE)• Late intrauterine fetal death (IUFD)• Placental abruption• Intrauterine growth restriction (IUGR) or Small for
gestational age (SGA)
• Prevalence: 1/6 pregnancies
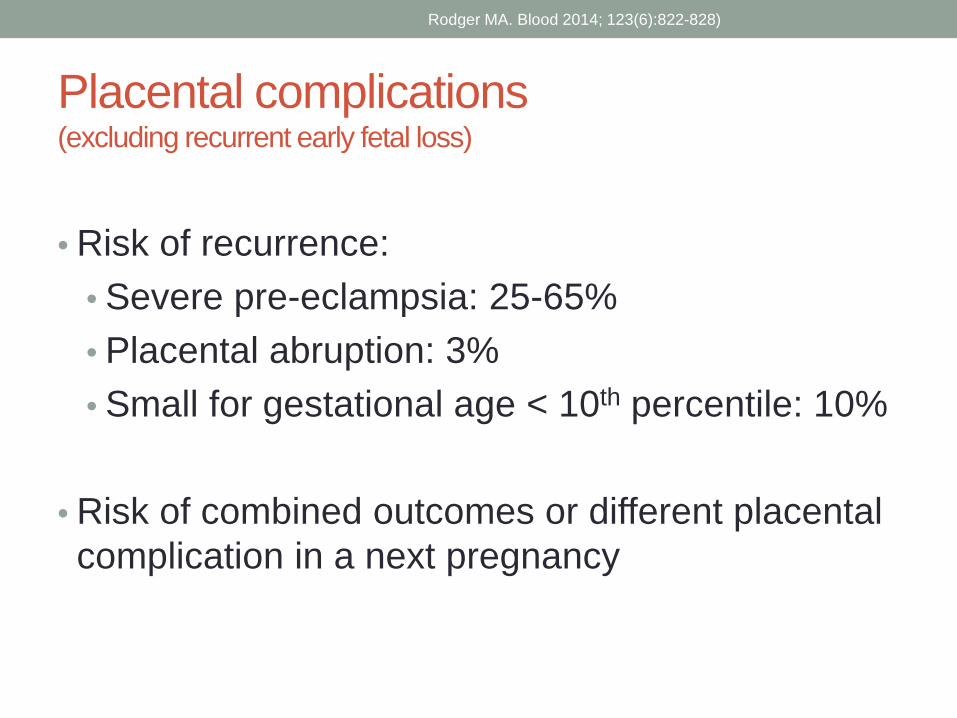
Placental complications (excluding recurrent early fetal loss)
• Risk of recurrence:• Severe pre-eclampsia: 25-65%• Placental abruption: 3%• Small for gestational age < 10th percentile: 10%
• Risk of combined outcomes or different placental complication in a next pregnancy
Rodger MA. Blood 2014; 123(6):822-828)

Approved preventive treatments• PE: ASA (1-A)
• PARIS1: ↓ PE 10%, ↓ births < 34 weeks 10%, ↓ serious complications 10%
• Roberge2: • ASA <16 weeks: ↓ RR PE 53%, severe PE 82%,
perinatal mortality 59%, prematurity 65%, IUGR 54%
• ASA >16 weeks: ↓ PE 22%, ↓ prematurity 10%
• PE: Calcium 1g / d if daily intake is insufficient (<600 mg/j) (1-A)
1. Askie et al. Lancet 2007;369(9575):1791-1798.2. Roberge et al. Ultras Obstet Gynecol 2013;41:491-499.

Cochrane 2012
• 10 studies (n=1139) of which 9 compared heparin (alone, with ASA or with dipyridamole) to placebo
• Quality: average to good
• Very heterogeneous; those not included in Rodger: • Patients with nephropathy (Kincaid-Smith)• Patients with ongoing IUGR or PE (Yu x2)• Biomarkers/placental morphology/abnormal Doppler < 24 weeks
(Kingdom)
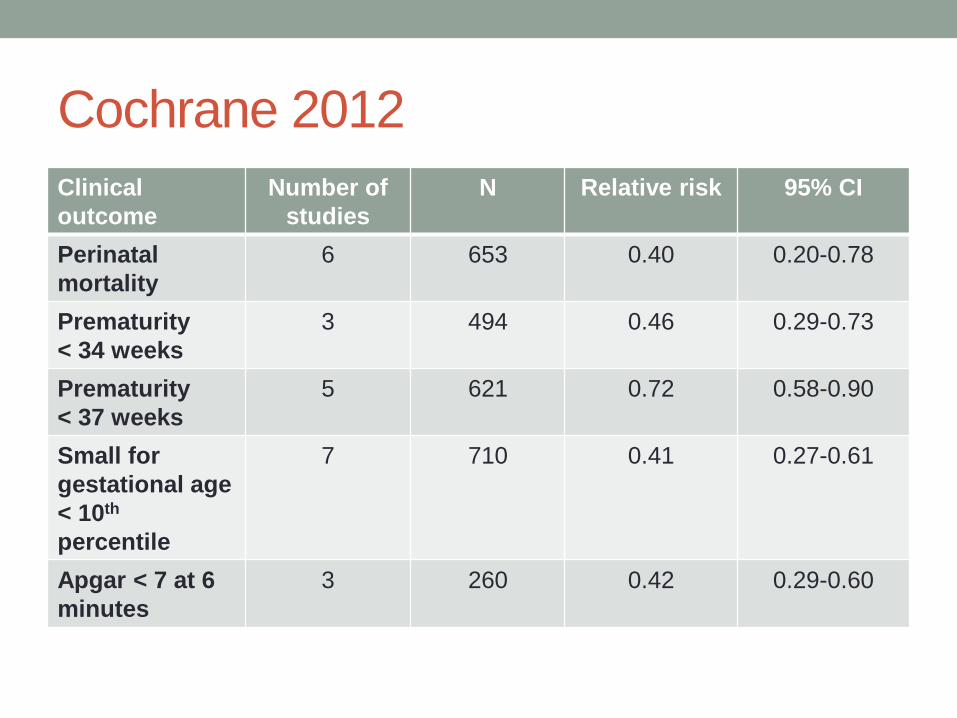
Cochrane 2012Clinical outcome
Number of studies
N Relative risk 95% CI
Perinatal mortality
6 653 0.40 0.20-0.78
Prematurity < 34 weeks
3 494 0.46 0.29-0.73
Prematurity< 37 weeks
5 621 0.72 0.58-0.90
Small for gestational age < 10th
percentile
7 710 0.41 0.27-0.61
Apgar < 7 at 6 minutes
3 260 0.42 0.29-0.60

Rodger MA.Blood 2014;123(6): 822-828
• 6 randomized controlled trials (RCT) n=854• Does not include TIPPS
• More than 40% come from a single centre (Gris, Nîmes).• Inclusion criteria:
• Pre-eclampsia: 70% (68% of these severe or early, so 32% non-severe).
• Placental abruption: 45%• Small for gestational age < 10th percentile: 37%• Intrauterine fetal death > 12 weeks: 27%
• 25% with thrombophilia• With ASA: 52%

StudiesCentre/ quality
# Inclusion criteria Thrombo-philias
Interventions Outcomes NNT
Mello et al. 2005 16
Single/ Poor
80 PE and ACE genotype GG
Excluded Dalteparin 5000 U vs. no Dalteparin
PE, SGA < 10th perc.7.3% vs. 28.2 %
5
Rey et al. 2009
+/-Multi/ average
116 Severe PE < 34 6 weeks (52%), SGA < 5th perc.
(18%), placentalabruption (14%), IUFD >
12 weeks (15%)
Excluded Dalteparin 5000 U +/- ASA vs. +/-
ASA(ASA used >80%)
PE, SGA <5th perc., placental abruption ,
stillbirth5.5% vs. 23.6%
5
NOH-AP2010
Single/ average
160 Placental abruption (44% with PE)
Allowed (16% +)
Enoxaparin 40 mg +/- ASA (19%) vs.
+/- ASA (41%)
PE, SGA <5th perc., placental abruption,
stillbirth12% vs. 31.3%
5
NOH-PE 2011
Single/ average
224 Severe PE60% > 34 weeks 40% < 34 weeks
17% HELLP
Allowed (14% +)
Enoxaparin 40 mg + ASA vs. ASA
PE, SGA <5th perc., placental abruption,
stillbirth8.9% vs. 25 %
7
FRUIT-RCT 2012
Multi/ good
139 Before 340 weeks:Severe PE (77%) and/or SGA< 10th perc. (68%)
Inclusion criteria
Dalteparin 5000 U + ASA vs. ASA
PE 18.6% vs. 21.7%
PE < 34 weeks0% vs. 8.7% 12
HAPPY2012
Multi/ very good
135 IUFD > 15 weeks (36%), PE (30%), SGA < 10th
perc. (21%), placentalabruption (4%)
Allowed(10% +)
Nadroparine 3800 IU vs. no
Nadroparine
PE, LBW <10th perc., placental abruption,
IUFD >15 weeks21% vs. 18%
Halted early for
futility

Rodger MA et al. Blood 2014;123(6):822-828)
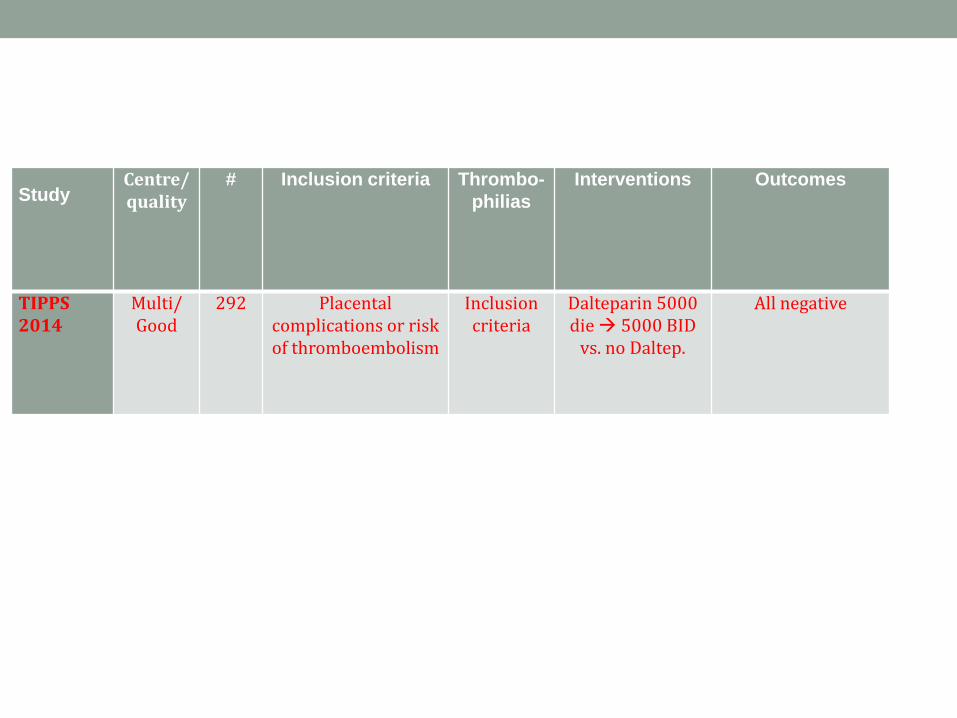
StudyCentre/ quality
# Inclusion criteria Thrombo-philias
Interventions Outcomes
TIPPS2014
Multi/ Good
292 Placental complications or risk of thromboembolism
Inclusion criteria
Dalteparin 5000 die 5000 BID
vs. no Daltep.
All negative
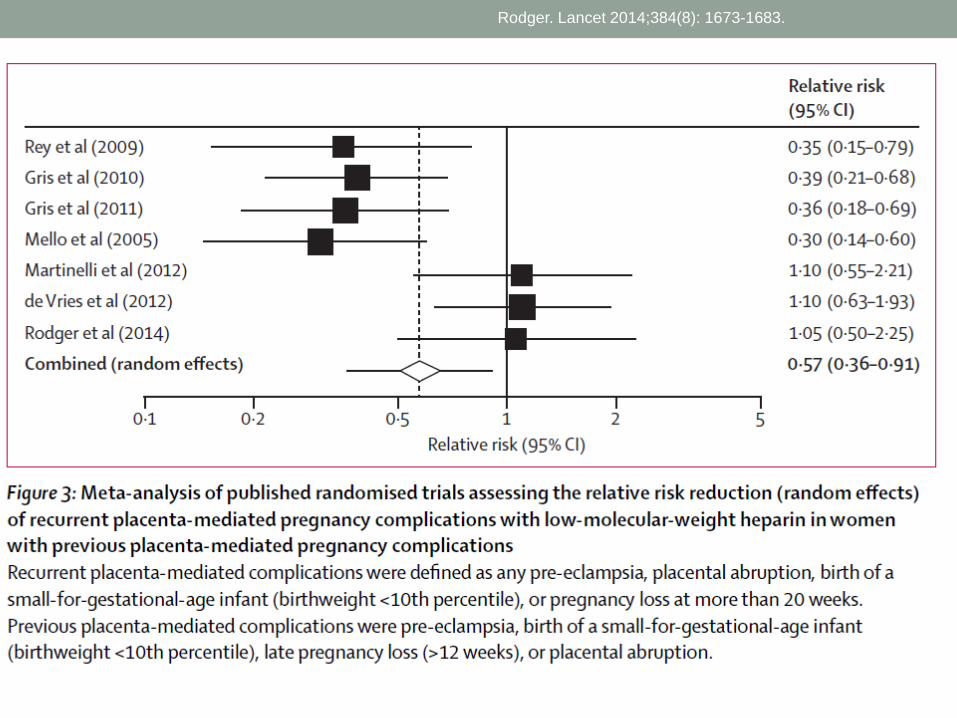
Rodger. Lancet 2014;384(8): 1673-1683.
AN EXTRA WORD ON LATE INTRAUTERINE FETAL DEATH…

Late intrauterine fetal death > 10 weeks
• Theory: • At around 10 weeks, the placenta takes over from the yolk sac to ensure embryonic infusion.
• If pathophysiology is placental inflammation/thrombosis, it will occur > 10 weeks.

Late IUFD > 10 weeks• 1 RCT: Gris, Blood 2004; 103:3695-3699.
• NOH: Nîmes Obstetricians and Haematologists studies• N=160 (184 eligibles:174 accepted, 12 spontaneous abortions T1)• Heterozygous Factor V Leiden or prothrombin gene mutation or
protein S deficiency• 1 intrauterine fetal death > 10 weeks
• N=96 60% (10-16 weeks)• N= 50 31% (16-22 weeks)• N= 14 9% (> 22 weeks)
• Exclusion: any etiology (infection, congenital defect or maternal anatomic anomaly, APL, chromosomal anomaly, PE, trauma, diabetes, thyroid, ITP, platelet alloimmunisation, etc.)
• ASA 100 mg vs. Enoxaparine 40 mg s/c from 8 weeks

Live births: 23 (29%) vs. 69 (86%) ↓ small for gestational age in Enoxaparine group (3043g vs. 2742g)
Gris et al. Blood 2004; 103:3695-99.

Conclusion: late intrauterine fetal death
Author Gestational age
% TP Number of patients
Outcomes specific to sub-group
Rey > 12 weeks 0 % 17 Unknown
Martinelli(HAPPY)
> 15 weeks 10% 49 Unknown
Gris 2004 > 10 weeks 100% 160 Questionable
Various studies: recurrent fetal loss
> 10 weeks Majority without
thrombophilia
? Unknown

Conclusion: placental complicationsOutcomes Relative risk CI 95%
Severe composite 0.37 0.25-0.55
Non-severe composite 0.80 0.44-1.46
Severe PE 0.16 0.07-0.36
Non-severe PE 0.46 0.28-0.75
Delivery <34 weeks 0.45 0.30-0.69
Delivery <37 weeks 0.77 0.62-0.96
Fetal death > 20 weeks 0.41 0.17-1.02
Fetal death < 20 weeks 0.89 0.50-1.6
Rodger MA. Blood 2014 et Lancet 2014.

Conclusions: placental complications• HAPPY (Martinelli) negative because …
• Majority (36%) included in fetal deaths > 15 weeks?• Inclusion of non-severe PE? (severity unknown in 38% of PE, early
onset not in inclusion criteria) • Stopped early?• 37% previous normal pregnancies?
• TIPPS (Rodger) negative because…• Inclusion criteria large/heterogeneous and often low risk

Recurrent early fetal loss



Prevalence
• 1 early fetal loss: 15%• 2 early fetal loss: 3-5%• 3 early fetal loss: 1-2%
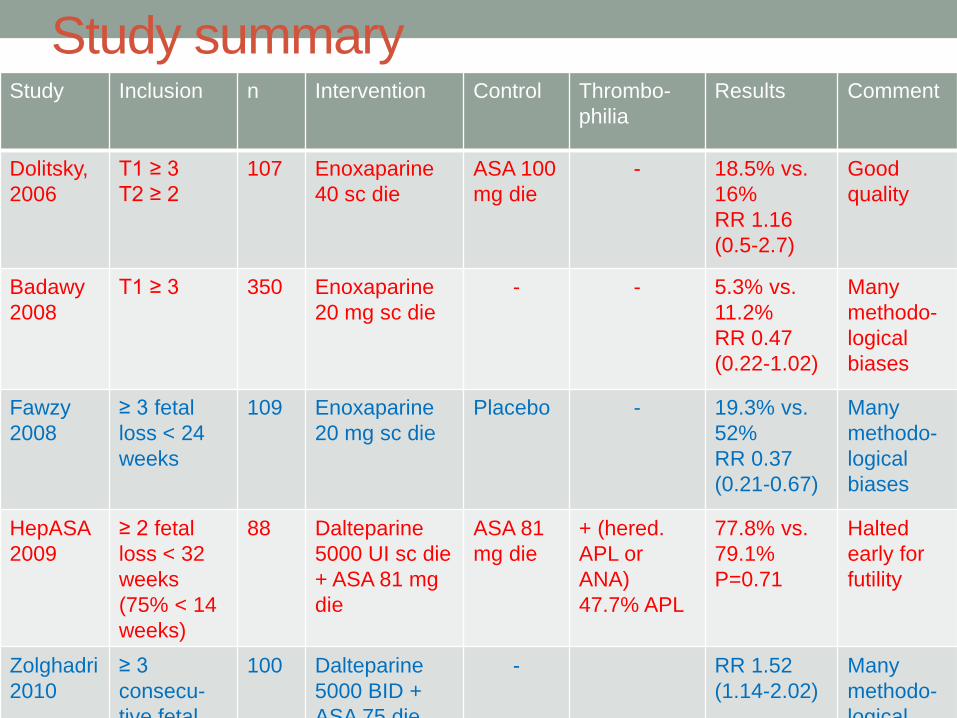
Study summaryStudy Inclusion n Intervention Control Thrombo-
philiaResults Comment
Dolitsky, 2006
T1 ≥ 3T2 ≥ 2
107 Enoxaparine40 sc die
ASA 100 mg die
- 18.5% vs. 16%RR 1.16 (0.5-2.7)
Good quality
Badawy2008
T1 ≥ 3 350 Enoxaparine20 mg sc die
- - 5.3% vs. 11.2%RR 0.47 (0.22-1.02)
Many methodo-logical biases
Fawzy2008
≥ 3 fetalloss < 24 weeks
109 Enoxaparine20 mg sc die
Placebo - 19.3% vs. 52%RR 0.37(0.21-0.67)
Many methodo-logical biases
HepASA2009
≥ 2 fetalloss < 32 weeks(75% < 14weeks)
88 Dalteparine5000 UI sc die + ASA 81 mg die
ASA 81 mg die
+ (hered. APL or ANA)47.7% APL
77.8% vs. 79.1%P=0.71
Halted early for futility
Zolghadri2010
≥ 3 consecu-tive fetal
100 Dalteparine5000 BID + ASA 75 die
- RR 1.52 (1.14-2.02)
Many methodo-logical

Study Inclusion n Intervention Control Thrombo-philia
Results Comment
Kaandorp,ALIFE 2010
≥ 2 FD before 20 weeks (60% ≥3) (30% late*)
299 Nadroparin 2850 mg s/c die + ASA 80mg
ASA 80 mg (n=99) or placebo (n=103)
+/-*12% -17% TP hereditairy
* No difference
LMWH 27.8% vs. ASA 37.4% vs. Placebo 30.1% RR 0.92 (0.60-1.43)
Good quality.Halted for futility.
Clark, SPIN 2010
≥ 2 FD before 24 weeks (43% ≥3)
294 Enoxaparin 40 mg sc die + ASA 75mg
- -3.5% hered. TP, 2.4% APL
22.4% vs. 20.7% RR 1.08 (0.69-1.69)
Good quality.
HABENOX 2011
≥ 3 FD T1≥ 2 FD T2≥ 1 FD T3 + 1 FD T1
207 Enoxaparine 40 mg sc die +/-ASA 80 mg die
ASA 80 mg die
+/-(25% APL)
65% vs. 71% vs. 61%P= 0.45
Good quality.Halted early.
Giancotti2012
≥ 2 FD < 12 weeks
124 Enoxaparine 40 mg sc die ORASA ad 32 weeks and Enox.40 die
ASA 100 mg die (63%)
+/-(35% with TP)
RR Enox1.39 (1.08-1.78)RR ASA/ Enox 1.54 (1.23-1.94)
High risk of bias.
TIPPS2014
≥ 3 FD <10≥ 2 FD10-16≥ 1 FD >16
129 Dalteparine 5000 die->BID
- + Nonsignificanttotal andsubgroup
Very hetero-geneousinclusion.

Conclusion
• Still very heterogeneous inclusion criteria• Early and late• With and without TP• Antiphopholipid antibody syndrome and hereditary thrombophilias
• It doesn’t look good…

Secondary effects

Secondary effects?• FRUIT:
• Cutaneous allergy, pruritis pain, edema: 11.4%• Need to change LMWH type: 2.9%• Hematoma: 1.4%• Major bleeding, thrombocytopenia, osteoporotic fracture: n=0
• TIPPS:• Major bleeding : 2.1% vs. 1.4% p=1.0• Minor bleeding : 19.6% vs. 9.2%• No heparin-induced thrombocytopenia, change in bone density or
fracture.• Does not cross the placenta• May interfere with neuraxial analgesia • Cost (patient/society)• Inconvenient for patient (daily injections)

Guidelines

ACCP 2012 guidelinesAPLS Hereditary TP Without
hereditary TP≥ 3 early fetalloss< 10 weeks
ASA + UH or LMWH (1-B)
NO (2-C) ?
1-2 early fetal loss
? ? NO (1-B)
Pre-eclampsia ? NO (2-C) ?
IUFD > 10 weeks ? NO (2-C) ?
Abruptio placentae
? NO (2-C) ?
SGA < 10th
percentile? NO (2-C) ?
UH: Unfractionated heparin

Guidelines• SOGJ 2014 for high-risk patients:
• 1. The following are recommended for prevention of preeclampsia: low-dose aspirin (I-A; High/Strong) and calcium supplementation (of at least 1 g/d) for women with low calcium intake (I-A; High/Strong).
• 2. Aspirin should be: taken in a low dose (75–162 mg/d) (III-B; Very low/Strong), administered at bedtime (I-B; Moderate/Strong), initiated after diagnosis of pregnancy but before 16 weeks’ gestation (I-B; Low/Weak), and considered for continuation until delivery (I-C; Very low/Weak).
• 3. Prophylactic doses of LMWH may be discussed in women with previous placental complications (including preeclampsia) to prevent the recurrence of ‘severe’ or early-onset preeclampsia, preterm delivery, and/or SGA infants (I-B; Moderate/Weak).

Guidelines• ACOG 2014:
• ASA 60-80 mg daily beginning at the end of first trimester for women having had:• Early-onset PE with delivery < 34 weeks• or• PE in more than one pregnancy
• No mention of LMWH, calcium

What I do…

Conclusion
• I do not look for hereditary TP with any placental complication• Recurrent early fetal loss WITH thrombophilia: I wait for proof
(consequences on insurance, familial screening)
• I look for APLA in all cases; ASA + LMWH antepartum + 6 weeks post-partum (expert recommendation…)
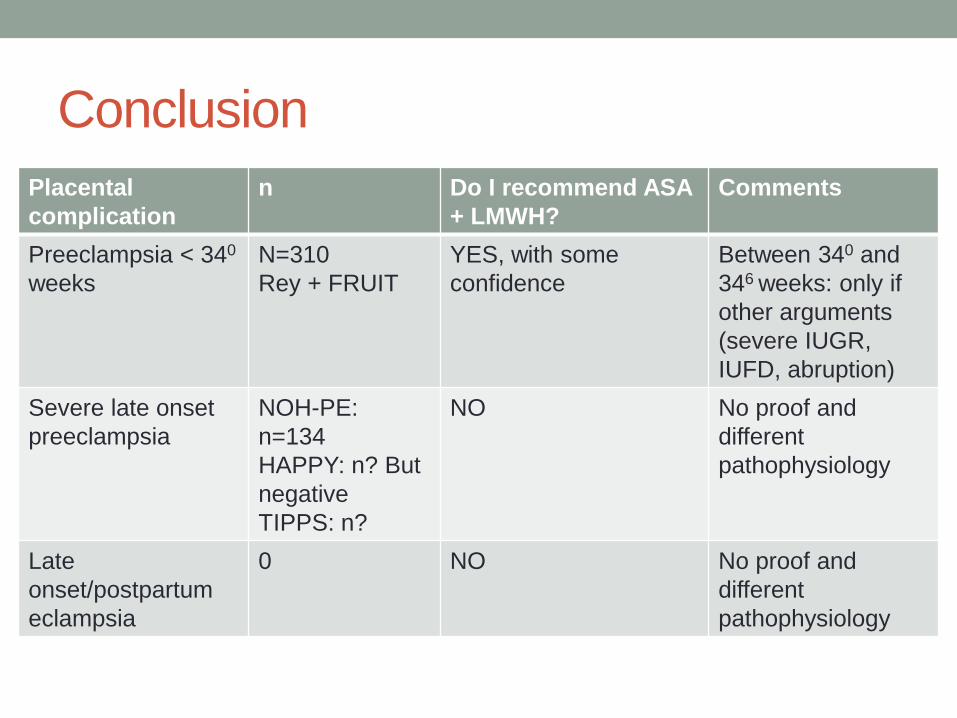
ConclusionPlacentalcomplication
n Do I recommend ASA + LMWH?
Comments
Preeclampsia < 340
weeksN=310Rey + FRUIT
YES, with some confidence
Between 340 and 346 weeks: only if other arguments (severe IUGR, IUFD, abruption)
Severe late onset preeclampsia
NOH-PE: n=134HAPPY: n? But negativeTIPPS: n?
NO No proof and different pathophysiology
Late onset/postpartumeclampsia
0 NO No proof and different pathophysiology
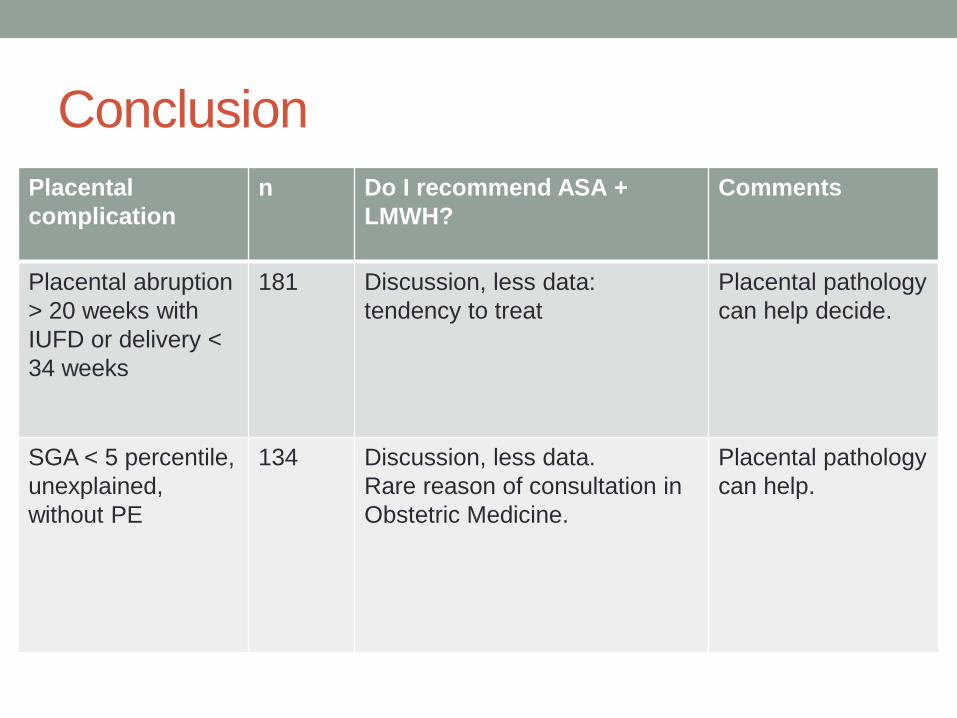
ConclusionPlacentalcomplication
n Do I recommend ASA + LMWH?
Comments
Placental abruption > 20 weeks with IUFD or delivery < 34 weeks
181 Discussion, less data: tendency to treat
Placental pathology can help decide.
SGA < 5 percentile, unexplained, without PE
134 Discussion, less data.Rare reason of consultation in Obstetric Medicine.
Placental pathology can help.

ConclusionPlacentalcomplication
n Do I recommend ASA + LMWH?
Comments
Unexplained IUFD > 20 weeks
N unknown in Rey and HAPPY
Discussion, tendency to treat especially if placental pathology compatible.
No specific data for this subgroup
1-2 IUFD 10-20 weeks
N unknown in Rey, HAPPY, multiples studies on recurrent fetal loss
Mostly NO, but case by case
No specific data for this subgroup
3 early fetal loss < 10 weeks without TP or TP status unknown
N unknown NO, with confidence
3 early fetal loss with hereditary TP
N unknown Mostly NO Higher consideration according to thromboembolic risk

Conclusion• If we can prevent something, it is mostly PE, regardless of
index placental complication
• Prevention of PE +/- important: prevention of complications more important (prematurity, maternal and fetal/neonatal complications) • Rodger’s meta-analysis shows reduction of severe outcomes when
severe index complications• Cochrane shows that we also diminish some of these outcomes
including perinatal mortality, prematurity, IUGR, Apgar ↓

QUESTIONS?



Early recurrent fetal loss• Middeldorp S. Thrombosis Research 2011;127
Supp.3:S105-109.

APL Screening
HereditaryTP
screening
ASA LMWH
≥ 3 fetaldeaths <10 weeks
YES NO YES NO
PE <34 0-6/7 YES NO YES YES
Late PE NO NO YES NO
Late eclampsia
NO NO YES NO
Fetal death > 12-20 weeks
YES? NO Mostly NO
Fetal death > 20 weeks
YES NO Mostly YES
Abruptio placentae
YES NO
LBW <5th OUI NON





























