Embed Size (px)
Citation preview

Nephrol Dial Transplant (2011) 0 1ndash5
doi 101093ndtgfr422
Exceptional Case
Thrombotic microangiopathy mimicking membranoproliferativeglomerulonephritis
Damien Brackman1 Lisa Sartz2 Sabine Leh3 Ann-Charlotte Kristoffersson2 Anna Bjerre4Ramesh Tati2 Veronique Fremeaux-Bacchi5 and Diana Karpman2
1Department of Pediatrics Haukeland University Hospital Bergen Norway 2Department of Pediatrics Clinical Sciences Lund LundUniversity Lund Sweden 3Department of Pathology Haukeland University Hospital Bergen Norway 4Department of PediatricsOslo University Hospital Oslo Norway and 5Assistance Publique-Hopitaux de Paris Department of Immunology Hopital EuropeenGeorges-Pompidou Paris France
Correspondence and offprint requests to Diana Karpman E-mail dianakarpmanmedluse
AbstractA 4-year-old boy presented with proteinuria and developedprogressive renal failure over 6 years In the patientrsquos familyfive individuals were affected with atypical haemolytic urae-mic syndrome (aHUS) but not the patient Renal biopsies (n5 3) showed glomerular basement membrane thickeningwith double contours endothelial swelling and deposits ofC3 and C1q Electron microscopy revealed mesangial andsubendothelial electron-dense deposits Complement muta-tions in membrane cofactor protein (Y155D) and C3(R713W and G1094R) were detected in all affected familymembers The patient also had transient autoantibodies tofactor H The findings suggest that aHUS and glomerulop-athy resembling membranoproliferative glomerulonephritismay have a common molecular background
Keywords complement C3 haemolytic uraemic syndromemembranoproliferative glomerulonephritis eculizumab
Background
Haemolytic uraemic syndrome is defined as non-immunemicroangiopathic haemolytic anaemia thrombocytopoeniaand renal failure A subtype termed atypical haemolyticuraemic syndrome (aHUS) is associated with activation ofthe alternative pathway of complement [1] Mutations havebeen identified in complement regulators factor H (CFH)factor I membrane cofactor protein (MCP) and complementfactors C3 [2] and factor B Deletions were found in factorH-related proteins 1 and 3 often associated with anti-factorH antibodies In addition mutations have been found inthrombomodulin (mutations reviewed in ref 1)
Membranoproliferative glomerulonephritis (MPGN) is adistinct renal disease presenting with haematuria proteinuriahypertension and impaired renal function MPGN is subclas-sified based on the localization of immune deposits consistingof IgG andor C3 [3] MPGN Types I and III are considered tobe immune complex-mediated diseases whereas Type II also
known as dense deposit disease is associated with comple-ment activation via the alternative pathway [3]
Both aHUS and MPGN can thus be associated withactivation of the alternative pathway of complement Cer-tain cases have been described in which individuals presentwith a combined clinical picture of aHUS and MPGN TypeI [4] indicating that these conditions may have a commonmolecular background
Case report
A 4-year-old boy was investigated at the Department ofPaediatrics Section of Paediatric Nephrology of the Hau-keland University Hospital in Bergen He is referred to asPatient III1 He was asymptomatic at the time of primaryinvestigation and had not previously exhibited any signs orsymptoms of renal disease but underwent a medical exami-nation because his younger sister had an episode of aHUSThe initial examination revealed a clinically healthy childwith normal blood pressure Urinalysis revealed protein-uria microscopic haematuria and casts Blood and urinetests are summarized in supplementary Table 1
Complement levels taken when the patient was firstexamined showed normal levels (supplementary Table 2)Ultrasound of the kidneys showed mildly increased paren-chymal echogenicity A renal biopsy was performed Theresults are presented in Table 1 and Figure 1AndashC Thebiopsy showed glomerular basement membrane (GBM)thickening with double contours mesangial cell prolifera-tion endothelial cell swelling and deposits of C3 IgG andIgM Electron microscopy revealed subendothelial and me-sangial electron-dense deposits as well as mesangial cellinterposition and podocyte foot effacement The patientwas treated with an angiotensin-converting enzyme inhib-itor and an angiotensin receptor blocker and remainedasymptomatic
At the age of 6 his creatinine levels started to rise and heexhibited increased proteinuria He underwent a second
The Author 2011 Published by Oxford University Press on behalf of ERA-EDTA All rights reservedFor Permissions please e-mail journalspermissionsoupcom
NDT Advance Access published August 1 2011 at G
irls University on A
ugust 10 2011ndtoxfordjournalsorg
Dow
nloaded from
renal biopsy (Table 1 Figure 1D) As in the first biopsythickening of the GBM with double contours and narrow-ing or occlusion of glomerular capillaries were noted Inaddition mild tubular atrophy and interstitial fibrosis weredemonstrated Blood samples were repeatedly assessedduring symptom-free periods and during infections but nolaboratory parameters indicated HUS
At the age of 65 years the patient developed hyperten-sion and by the age of 8 years he was being treated withfour antihypertensive medications He was stable on thistreatment until just before he turned 10 when his creatinineand proteinuria increased and glomerular filtration rate de-creased (supplementary Table 1) He underwent a third renalbiopsy at 10 years (Figure 1EndashG) The biopsy showed globalsclerosis of 1217 glomeruli and the remaining glomeruliexhibited mesangial expansion due to increased matrix andcells Endothelial cells were swollen and glomerular capil-laries were thickened or occluded One thrombus was notedin a capillary (Figure 1E) GBMs were thickened with doublecontours Arterioles and smaller arteries showed media hy-pertrophy Immunohistochemistry showed as in previousbiopsies labelling with C3 and C1q (Figure 1F) Electronmicroscopy showed electron-dense precipitations in capil-lary lumina mesangial cell interposition and podocyte footprocess effacement (Figure 1G)
Currently at the age of 10 years the patientrsquos clinicalcondition has deteriorated with decreased renal functionand increased blood pressure refractory to treatment witha combination of five antihypertensive medications Thelaboratory values for the first time indicate ongoing hae-molysis (undetectable haptoglobin elevated lactic dehy-drogenase elevated reticulocyte counts and reducedhaemoglobin) The direct antiglobulin test is negative Pro-teinuria has decreased and platelet counts remain normalTreatment with regular infusions of eculizumab (human-ized monoclonal anti-C5 antibody Alexion) was initiatedin January 2011 The initial dose was 600 mg intravenouslyonce a week for 4 weeks followed by 600 mg every otherweek
The family history is indicative of hereditary aHUS Theindex patient has two sisters currently 6 and 4 years old The6-year-old sister (Patient III2 in Figure 2) developed HUSfollowing a respiratory tract infection at the age of 5 monthsbut did not require dialysis and recovered with mild protei-nuria The father of Patients III1 and III2 developed HUS atthe age of 10 years (Patient II2) He too did not requiredialysis and recovered with no recurrences Patient II2 hada brother 2 years older that developed HUS at 4 months agefollowing a vaccination (Patient II1) Upon hospitalizationhe exhibited bloody diarrhoea Hospital records indicate hae-molytic anaemia and thrombocytopenia and the patient suc-cumbed within 48 h Post-mortem examination of kidneytissue showed acute thrombotic microangiopathy with swol-len endothelial cells and capillary thrombi (Figure 1H) Pa-tient II4 is a younger brother of Patients II1 and II2 Hedeveloped transient anaemia and jaundice at the age of 10months followed by HUS and proteinuria at 2 years of ageThere have been no recurrences since Patient II4rsquos daughterPatient III7 currently 6 years old has had eight episodes ofHUS since she was 4 months old Six episodes of HUSoccurred by the age of 21 months at which time regularT
able
1P
atho
logi
cal
find
ings
inpa
tien
tII
I1a
Lig
htm
icro
scop
ygl
omer
ular
path
olog
yIm
mun
ohis
toch
emis
try
Ele
ctro
nm
icro
scop
yF
igur
e
Bio
psy
Age
(yrs
)
GB
Mth
icke
ning
and
doub
leco
ntou
rsb
Mes
angi
alce
llpr
olif
erat
ion
Lob
ulat
ion
Mic
roth
rom
biE
ndot
heli
alce
llsw
elli
ngC
3cC
1qIg
GIg
M
1st
biop
sy4
11
111
111
1
11
Mes
angi
alan
dsu
bend
othe
lial
ED
D
mes
angi
alce
llin
terp
osit
ion
Pod
ocyt
efo
otpr
oces
sef
face
men
t
1AndashC
2nd
biop
sy6
11
11
11
1
M
esan
gial
cell
inte
rpos
itio
nP
odoc
yte
foot
proc
ess
effa
cem
ent
1D
3rd
biop
sy10
11
1
111
111
1
1E
lect
ron-
dens
epr
ecip
itat
esin
capi
llar
ylu
min
aM
esan
gial
cell
inte
rpos
itio
nP
odoc
yte
foot
proc
ess
effa
cem
ent
1EndashG
a ED
D
elec
tron
-den
sede
posi
ts
bT
ram
-tra
cks
c Gra
nula
rde
posi
tion
alon
ggl
omer
ular
capi
llar
yw
alls
2 D Brackman et al
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
plasma infusions were instituted after which she has sufferedtwo recurrences in 2 years Interestingly the parents of Pa-tients II1 II2 and II4 are cousins (Individuals I1 and I2 inFigure 2) They are unaffected but the paternal grandfather of
Patients II1 II2 and II4 had recurrent bouts of jaundice withno liver disease Complement levels of Patients II2 II4 III1III2 and III7 are presented in supplementary Table 2 Com-plement levels were not available from Patient II1
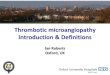
Fig 1 Pathological findings in Patients III1 and II1 (AndashC) Patient III1 first renal biopsy taken at the age of 4 years (A) Glomerulus with slight mesangialexpansion and thickened capillary walls with double contours (Periodic acid-Schiff staining) (B) Immunohistochemical staining for C3 (anti-C3 from DakoGlostrup Denmark) showing marked labelling of capillary walls (A and B original magnification 3400) (C) Ultrastructure showing a capillary withelectron-dense deposits (arrowheads) in subendothelial position and effacement of podocyte foot processes (arrow) Inset shows mesangial cell interpositionScale bar represents 1 lm (C) and 2 lm (C inset) (D) Patient III1 second renal biopsy at age 6 years Hypercellular glomerulus with thickened GBMs andnarrowed glomerular capillaries (inset) One sclerosing glomerulus with collapsed glomerular tuft segmental sclerosis and thickening of Bowmanrsquos capsuleis visible (arrow) A group of tubules with reduced diameter and thickened basement membrane (arrowhead) indicating tubular atrophy (original magni-fication 3200 inset 31000) (EndashG) Patient III1 third renal biopsy at age 10 years Panel E shows thickening of the GBM occluded capillaries (arrowhead)and one thrombus in a glomerular capillary (see arrow) Panel F shows C1q labelling of capillary walls (anti-C1q from Dako) Panel G ultrastructure showingelectron-dense precipitations in capillary lumina (arrowheads) and duplication of the GBM (arrow) Activated endothelial cells contain many organellesEffaced podocyte foot processes (scale bar 2 lm) (H) Patient II1 post-mortem renal tissue Glomerulus with intracapillary thrombi and swollen endothelialcells (trichrome stain thrombi are red erythrocytes yellow) E F and H original magnification 3400
Thrombotic microangiopathy mimicking MPGN 3
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
DNA sequencing was carried out as described in thesupplementary methods Patients II1 II2 II4 III1 III2and III7 carry a previously described MCP mutation(Y155D) [5] and two C3 mutations R713W (in Exon 17)and G1094R (in Exon 26) R713W has been previouslydescribed [2] whereas G1094R is a novel mutationsituated one amino acid from a described mutation atposition D1093N [2] These C3 mutations were presum-ably localized on the same allele due to the common patternof inheritance and they were not found in DNA from100 healthy controls In addition Patient III1 has a hetero-zygous deletion of CFHR13 and autoantibodies to CFHwere detected upon debut of disease but not 5 yearslater The MCP mutation was found in two unaffectedfamily members and the C3 mutations were found in oneunaffected family member The mutations and their pre-sumed functional consequences are presented in Figure 2and Table 2 as well as the supplementary results anddiscussion
Discussion
In this report we describe a child with progressive renal fail-ure and pathology exhibiting a membranoproliferative pattern
Other family members presented with features of aHUS Allaffected family members were found to share complementmutations in C3 and MCP This study suggests that differingclinical and pathological phenotypes of aHUS may have acommon molecular basis Thrombotic microangiopathy canthus develop even in the absence of clinical HUS
Patient III1 did not exhibit clinical signs of aHUSalthough haemolysis without thrombocytopenia was de-tected 6 years after debut of disease His biopsies showeda membranoproliferative pattern including C3 positivityThese findings are compatible with chronic thrombotic mi-croangiopathy except for the presence of subendothelialelectron-dense deposits Electron-dense deposits are a pecu-liar feature in this patient usually not observed in thromboticmicroangiopathy and making the distinction from MPGNType I difficult Furthermore strong C1q labelling is notfound in thrombotic microangiopathy but usually associatedwith systematic lupus erythematosis C1q nephropathy [7] orMPGN Type I but the weak IgG staining suggests that therenal deposits were probably not mediated by immune com-plexes The finding of membranoproliferative features is inline with other studies suggesting that there might be a con-tinuous spectrum of morphological changes from thromboticmicroangiopathy to MPGN [8ndash10] This group of disorderscould also encompass the more recently described C3
Table 2 Molecular characteristics of genetic alterations in patientsa
Complement protein Mutation or deletion Codon Protein Phenotype Reference
MCP Y155D 565 TgtG Tyr155Asp Reduced cell-surface expression of MCPNo detectable C3b- or C4b-binding activityand negligible cofactor activity
[5]
C3 G1094R 3346 GgtC Gly1116Arg Adjacent mutation (D1093N) showedreduced binding to MCP and to alesser degree CFH
[2]
C3 R713W 2203 CgtT Arg735Trp No documented abnormality NormalC3 binding to CFB CFH MCPand soluble CR1
[2]
CFHR13 DCFHR13b Associated with the presence ofanti-CFH antibodies
[6]
aCFB factor B CFH factor H MCP membrane cofactor proteinCD46 CR1 complement receptor 1 CFHR factor H-related protein All geneticalterations including DCFHR13 were heterozygousbThis deletion has also been detected in the healthy population
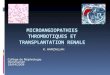
Fig 2 Pedigree of the investigated family CFH ab anti-factor H (CFH) antibodies The affected individuals in two generations are marked in filledboxes and circles Mutations C3 G1094R 1 R713W and MCP Y155D DCFHR13 heterozygous deletion of CFHR1 and CFHR3 Serum anti-CFHantibodies detected in Patient III1 at debut but not 5 years later Patients III2 and III7 were tested and did not have serum anti-CFH antibodies
4 D Brackman et al
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
glomerulopathy with isolated C3 deposits [11] However thestrong C1q labelling in the patientrsquos biopsies is not compatiblewith this diagnosis
The presence of complement activation due to mutationsin C3 and MCP enabled the pathological features toprogress even in the absence of overt HUS The clinicaland pathological features overlap with MPGN Type Iindicating that aHUS and MPGN may share a commonmolecular background We thus conclude that this patientexhibited an unusual presentation of chronic thromboticmicroangiopathy mimicking MPGN Type I
Supplementary data
Supplementary data are available online at httpndtoxfordjournalsorg
Acknowledgements This study was supported by grants from The SwedishResearch Council (K2010-65X-14008-10-3 to DK) Torsten and RagnarSoderberg Foundation The fund for Renal Research Crown PrincessLovisarsquos Society for Child Care Konung Gustaf Vs 80-aringrsfond FannyEkdahlrsquos Foundation (all to DK) DK is the recipient of a clinicalndashexperimental research fellowship from the Royal Swedish Academy ofSciences The Queen Silvia Jubilee Fond to LS French Agence Nationalede la Recherche (R09097DS) Programme Hospitalier de Recherche Clin-ique (AOM05130P051065) and French Association for Information andResearch on Genetic Renal Diseases (AIRG) to VF-B A preliminaryversion of the manuscript appeared in the PhD thesis of Dr LS
The authors would like to thank Dr Marie-Agnes Dragon-Durey HopitalEuropeen Georges-Pompidou Service drsquoImmunologie Biologique Parisfor analysis of anti-CFH antibodies in Patient III1 and Professor MartinOlsson Department of Transfusion Medicine Lund University for controlsamples
Transparency declaration VF-B was consultant for and gave lecturesfor Alexion Pharmaceuticals during 2010 DK was the national coordi-nator in Sweden of the multi-center trial of Eculizumab (Alexion Pharma-ceuticals) in patients with atypical hemolytic uremic syndrome
Conflict of interest statement None declared
References
1 Noris M Remuzzi G Atypical hemolytic-uremic syndrome N EnglJ Med 2009 361 1676ndash1687
2 Fremeaux-Bacchi V Miller EC Liszewski MK et al Mutations incomplement C3 predispose to development of atypical hemolytic ure-mic syndrome Blood 2008 112 4948ndash4952
3 Licht C Fremeaux-Bacchi V Hereditary and acquired complementdysregulation in membranoproliferative glomerulonephritis ThrombHaemost 2009 101 271ndash278
4 Vaziri-Sani F Holmberg L Sjoholm AG et al Phenotypic expressionof factor H mutations in patients with atypical hemolytic uremic syn-drome Kidney Int 2006 69 981ndash988
5 Fremeaux-Bacchi V Moulton EA Kavanagh D et al Genetic and func-tional analyses of membrane cofactor protein (CD46) mutations in atyp-ical hemolytic uremic syndrome J Am Soc Nephrol 2006 172017ndash2025
6 Zipfel PF Edey M Heinen S et al Deletion of complement factor H-related genes CFHR1 and CFHR3 is associated with atypical hemo-lytic uremic syndrome PLoS Genet 2007 3 e41
7 Pickering MC Cook HT Translational mini-review series on comple-ment factor H renal diseases associated with complement factor Hnovel insights from humans and animals Clin Exp Immunol 2008151 210ndash230
8 Servais A Fremeaux-Bacchi V Lequintrec M et al Primary glomer-ulonephritis with isolated C3 deposits a new entity which sharescommon genetic risk factors with haemolytic uraemic syndromeJournal of medical genetics 2007 44 193ndash199
9 Skerka C Licht C Mengel M et al Autoimmune forms of thromboticmicroangiopathy and membranoproliferative glomerulonephritis In-dications for a disease spectrum and common pathogenic principlesMol Immunol 2009 46 2801ndash2807
10 Fakhouri F Fremeaux-Bacchi V Noel LH et al C3 glomerulopathy anew classification Nat Rev Nephrol 2010 6 494ndash499
11 Vizjak A Ferluga D Rozic M et al Pathology clinical presentations andoutcomes of C1q nephropathy J Am Soc Nephrol 2008 19 2237ndash2244
Received for publication 20611 Accepted in revised form 20611
Thrombotic microangiopathy mimicking MPGN 5
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from

renal biopsy (Table 1 Figure 1D) As in the first biopsythickening of the GBM with double contours and narrow-ing or occlusion of glomerular capillaries were noted Inaddition mild tubular atrophy and interstitial fibrosis weredemonstrated Blood samples were repeatedly assessedduring symptom-free periods and during infections but nolaboratory parameters indicated HUS
At the age of 65 years the patient developed hyperten-sion and by the age of 8 years he was being treated withfour antihypertensive medications He was stable on thistreatment until just before he turned 10 when his creatinineand proteinuria increased and glomerular filtration rate de-creased (supplementary Table 1) He underwent a third renalbiopsy at 10 years (Figure 1EndashG) The biopsy showed globalsclerosis of 1217 glomeruli and the remaining glomeruliexhibited mesangial expansion due to increased matrix andcells Endothelial cells were swollen and glomerular capil-laries were thickened or occluded One thrombus was notedin a capillary (Figure 1E) GBMs were thickened with doublecontours Arterioles and smaller arteries showed media hy-pertrophy Immunohistochemistry showed as in previousbiopsies labelling with C3 and C1q (Figure 1F) Electronmicroscopy showed electron-dense precipitations in capil-lary lumina mesangial cell interposition and podocyte footprocess effacement (Figure 1G)
Currently at the age of 10 years the patientrsquos clinicalcondition has deteriorated with decreased renal functionand increased blood pressure refractory to treatment witha combination of five antihypertensive medications Thelaboratory values for the first time indicate ongoing hae-molysis (undetectable haptoglobin elevated lactic dehy-drogenase elevated reticulocyte counts and reducedhaemoglobin) The direct antiglobulin test is negative Pro-teinuria has decreased and platelet counts remain normalTreatment with regular infusions of eculizumab (human-ized monoclonal anti-C5 antibody Alexion) was initiatedin January 2011 The initial dose was 600 mg intravenouslyonce a week for 4 weeks followed by 600 mg every otherweek
The family history is indicative of hereditary aHUS Theindex patient has two sisters currently 6 and 4 years old The6-year-old sister (Patient III2 in Figure 2) developed HUSfollowing a respiratory tract infection at the age of 5 monthsbut did not require dialysis and recovered with mild protei-nuria The father of Patients III1 and III2 developed HUS atthe age of 10 years (Patient II2) He too did not requiredialysis and recovered with no recurrences Patient II2 hada brother 2 years older that developed HUS at 4 months agefollowing a vaccination (Patient II1) Upon hospitalizationhe exhibited bloody diarrhoea Hospital records indicate hae-molytic anaemia and thrombocytopenia and the patient suc-cumbed within 48 h Post-mortem examination of kidneytissue showed acute thrombotic microangiopathy with swol-len endothelial cells and capillary thrombi (Figure 1H) Pa-tient II4 is a younger brother of Patients II1 and II2 Hedeveloped transient anaemia and jaundice at the age of 10months followed by HUS and proteinuria at 2 years of ageThere have been no recurrences since Patient II4rsquos daughterPatient III7 currently 6 years old has had eight episodes ofHUS since she was 4 months old Six episodes of HUSoccurred by the age of 21 months at which time regularT
able
1P
atho
logi
cal
find
ings
inpa
tien
tII
I1a
Lig
htm
icro
scop
ygl
omer
ular
path
olog
yIm
mun
ohis
toch
emis
try
Ele
ctro
nm
icro
scop
yF
igur
e
Bio
psy
Age
(yrs
)
GB
Mth
icke
ning
and
doub
leco
ntou
rsb
Mes
angi
alce
llpr
olif
erat
ion
Lob
ulat
ion
Mic
roth
rom
biE
ndot
heli
alce
llsw
elli
ngC
3cC
1qIg
GIg
M
1st
biop
sy4
11
111
111
1
11
Mes
angi
alan
dsu
bend
othe
lial
ED
D
mes
angi
alce
llin
terp
osit
ion
Pod
ocyt
efo
otpr
oces
sef
face
men
t
1AndashC
2nd
biop
sy6
11
11
11
1
M
esan
gial
cell
inte
rpos
itio
nP
odoc
yte
foot
proc
ess
effa
cem
ent
1D
3rd
biop
sy10
11
1
111
111
1
1E
lect
ron-
dens
epr
ecip
itat
esin
capi
llar
ylu
min
aM
esan
gial
cell
inte
rpos
itio
nP
odoc
yte
foot
proc
ess
effa
cem
ent
1EndashG
a ED
D
elec
tron
-den
sede
posi
ts
bT
ram
-tra
cks
c Gra
nula
rde
posi
tion
alon
ggl
omer
ular
capi
llar
yw
alls
2 D Brackman et al
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
plasma infusions were instituted after which she has sufferedtwo recurrences in 2 years Interestingly the parents of Pa-tients II1 II2 and II4 are cousins (Individuals I1 and I2 inFigure 2) They are unaffected but the paternal grandfather of
Patients II1 II2 and II4 had recurrent bouts of jaundice withno liver disease Complement levels of Patients II2 II4 III1III2 and III7 are presented in supplementary Table 2 Com-plement levels were not available from Patient II1
Fig 1 Pathological findings in Patients III1 and II1 (AndashC) Patient III1 first renal biopsy taken at the age of 4 years (A) Glomerulus with slight mesangialexpansion and thickened capillary walls with double contours (Periodic acid-Schiff staining) (B) Immunohistochemical staining for C3 (anti-C3 from DakoGlostrup Denmark) showing marked labelling of capillary walls (A and B original magnification 3400) (C) Ultrastructure showing a capillary withelectron-dense deposits (arrowheads) in subendothelial position and effacement of podocyte foot processes (arrow) Inset shows mesangial cell interpositionScale bar represents 1 lm (C) and 2 lm (C inset) (D) Patient III1 second renal biopsy at age 6 years Hypercellular glomerulus with thickened GBMs andnarrowed glomerular capillaries (inset) One sclerosing glomerulus with collapsed glomerular tuft segmental sclerosis and thickening of Bowmanrsquos capsuleis visible (arrow) A group of tubules with reduced diameter and thickened basement membrane (arrowhead) indicating tubular atrophy (original magni-fication 3200 inset 31000) (EndashG) Patient III1 third renal biopsy at age 10 years Panel E shows thickening of the GBM occluded capillaries (arrowhead)and one thrombus in a glomerular capillary (see arrow) Panel F shows C1q labelling of capillary walls (anti-C1q from Dako) Panel G ultrastructure showingelectron-dense precipitations in capillary lumina (arrowheads) and duplication of the GBM (arrow) Activated endothelial cells contain many organellesEffaced podocyte foot processes (scale bar 2 lm) (H) Patient II1 post-mortem renal tissue Glomerulus with intracapillary thrombi and swollen endothelialcells (trichrome stain thrombi are red erythrocytes yellow) E F and H original magnification 3400
Thrombotic microangiopathy mimicking MPGN 3
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
DNA sequencing was carried out as described in thesupplementary methods Patients II1 II2 II4 III1 III2and III7 carry a previously described MCP mutation(Y155D) [5] and two C3 mutations R713W (in Exon 17)and G1094R (in Exon 26) R713W has been previouslydescribed [2] whereas G1094R is a novel mutationsituated one amino acid from a described mutation atposition D1093N [2] These C3 mutations were presum-ably localized on the same allele due to the common patternof inheritance and they were not found in DNA from100 healthy controls In addition Patient III1 has a hetero-zygous deletion of CFHR13 and autoantibodies to CFHwere detected upon debut of disease but not 5 yearslater The MCP mutation was found in two unaffectedfamily members and the C3 mutations were found in oneunaffected family member The mutations and their pre-sumed functional consequences are presented in Figure 2and Table 2 as well as the supplementary results anddiscussion
Discussion
In this report we describe a child with progressive renal fail-ure and pathology exhibiting a membranoproliferative pattern
Other family members presented with features of aHUS Allaffected family members were found to share complementmutations in C3 and MCP This study suggests that differingclinical and pathological phenotypes of aHUS may have acommon molecular basis Thrombotic microangiopathy canthus develop even in the absence of clinical HUS
Patient III1 did not exhibit clinical signs of aHUSalthough haemolysis without thrombocytopenia was de-tected 6 years after debut of disease His biopsies showeda membranoproliferative pattern including C3 positivityThese findings are compatible with chronic thrombotic mi-croangiopathy except for the presence of subendothelialelectron-dense deposits Electron-dense deposits are a pecu-liar feature in this patient usually not observed in thromboticmicroangiopathy and making the distinction from MPGNType I difficult Furthermore strong C1q labelling is notfound in thrombotic microangiopathy but usually associatedwith systematic lupus erythematosis C1q nephropathy [7] orMPGN Type I but the weak IgG staining suggests that therenal deposits were probably not mediated by immune com-plexes The finding of membranoproliferative features is inline with other studies suggesting that there might be a con-tinuous spectrum of morphological changes from thromboticmicroangiopathy to MPGN [8ndash10] This group of disorderscould also encompass the more recently described C3
Table 2 Molecular characteristics of genetic alterations in patientsa
Complement protein Mutation or deletion Codon Protein Phenotype Reference
MCP Y155D 565 TgtG Tyr155Asp Reduced cell-surface expression of MCPNo detectable C3b- or C4b-binding activityand negligible cofactor activity
[5]
C3 G1094R 3346 GgtC Gly1116Arg Adjacent mutation (D1093N) showedreduced binding to MCP and to alesser degree CFH
[2]
C3 R713W 2203 CgtT Arg735Trp No documented abnormality NormalC3 binding to CFB CFH MCPand soluble CR1
[2]
CFHR13 DCFHR13b Associated with the presence ofanti-CFH antibodies
[6]
aCFB factor B CFH factor H MCP membrane cofactor proteinCD46 CR1 complement receptor 1 CFHR factor H-related protein All geneticalterations including DCFHR13 were heterozygousbThis deletion has also been detected in the healthy population
Fig 2 Pedigree of the investigated family CFH ab anti-factor H (CFH) antibodies The affected individuals in two generations are marked in filledboxes and circles Mutations C3 G1094R 1 R713W and MCP Y155D DCFHR13 heterozygous deletion of CFHR1 and CFHR3 Serum anti-CFHantibodies detected in Patient III1 at debut but not 5 years later Patients III2 and III7 were tested and did not have serum anti-CFH antibodies
4 D Brackman et al
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
glomerulopathy with isolated C3 deposits [11] However thestrong C1q labelling in the patientrsquos biopsies is not compatiblewith this diagnosis
The presence of complement activation due to mutationsin C3 and MCP enabled the pathological features toprogress even in the absence of overt HUS The clinicaland pathological features overlap with MPGN Type Iindicating that aHUS and MPGN may share a commonmolecular background We thus conclude that this patientexhibited an unusual presentation of chronic thromboticmicroangiopathy mimicking MPGN Type I
Supplementary data
Supplementary data are available online at httpndtoxfordjournalsorg
Acknowledgements This study was supported by grants from The SwedishResearch Council (K2010-65X-14008-10-3 to DK) Torsten and RagnarSoderberg Foundation The fund for Renal Research Crown PrincessLovisarsquos Society for Child Care Konung Gustaf Vs 80-aringrsfond FannyEkdahlrsquos Foundation (all to DK) DK is the recipient of a clinicalndashexperimental research fellowship from the Royal Swedish Academy ofSciences The Queen Silvia Jubilee Fond to LS French Agence Nationalede la Recherche (R09097DS) Programme Hospitalier de Recherche Clin-ique (AOM05130P051065) and French Association for Information andResearch on Genetic Renal Diseases (AIRG) to VF-B A preliminaryversion of the manuscript appeared in the PhD thesis of Dr LS
The authors would like to thank Dr Marie-Agnes Dragon-Durey HopitalEuropeen Georges-Pompidou Service drsquoImmunologie Biologique Parisfor analysis of anti-CFH antibodies in Patient III1 and Professor MartinOlsson Department of Transfusion Medicine Lund University for controlsamples
Transparency declaration VF-B was consultant for and gave lecturesfor Alexion Pharmaceuticals during 2010 DK was the national coordi-nator in Sweden of the multi-center trial of Eculizumab (Alexion Pharma-ceuticals) in patients with atypical hemolytic uremic syndrome
Conflict of interest statement None declared
References
1 Noris M Remuzzi G Atypical hemolytic-uremic syndrome N EnglJ Med 2009 361 1676ndash1687
2 Fremeaux-Bacchi V Miller EC Liszewski MK et al Mutations incomplement C3 predispose to development of atypical hemolytic ure-mic syndrome Blood 2008 112 4948ndash4952
3 Licht C Fremeaux-Bacchi V Hereditary and acquired complementdysregulation in membranoproliferative glomerulonephritis ThrombHaemost 2009 101 271ndash278
4 Vaziri-Sani F Holmberg L Sjoholm AG et al Phenotypic expressionof factor H mutations in patients with atypical hemolytic uremic syn-drome Kidney Int 2006 69 981ndash988
5 Fremeaux-Bacchi V Moulton EA Kavanagh D et al Genetic and func-tional analyses of membrane cofactor protein (CD46) mutations in atyp-ical hemolytic uremic syndrome J Am Soc Nephrol 2006 172017ndash2025
6 Zipfel PF Edey M Heinen S et al Deletion of complement factor H-related genes CFHR1 and CFHR3 is associated with atypical hemo-lytic uremic syndrome PLoS Genet 2007 3 e41
7 Pickering MC Cook HT Translational mini-review series on comple-ment factor H renal diseases associated with complement factor Hnovel insights from humans and animals Clin Exp Immunol 2008151 210ndash230
8 Servais A Fremeaux-Bacchi V Lequintrec M et al Primary glomer-ulonephritis with isolated C3 deposits a new entity which sharescommon genetic risk factors with haemolytic uraemic syndromeJournal of medical genetics 2007 44 193ndash199
9 Skerka C Licht C Mengel M et al Autoimmune forms of thromboticmicroangiopathy and membranoproliferative glomerulonephritis In-dications for a disease spectrum and common pathogenic principlesMol Immunol 2009 46 2801ndash2807
10 Fakhouri F Fremeaux-Bacchi V Noel LH et al C3 glomerulopathy anew classification Nat Rev Nephrol 2010 6 494ndash499
11 Vizjak A Ferluga D Rozic M et al Pathology clinical presentations andoutcomes of C1q nephropathy J Am Soc Nephrol 2008 19 2237ndash2244
Received for publication 20611 Accepted in revised form 20611
Thrombotic microangiopathy mimicking MPGN 5
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from

plasma infusions were instituted after which she has sufferedtwo recurrences in 2 years Interestingly the parents of Pa-tients II1 II2 and II4 are cousins (Individuals I1 and I2 inFigure 2) They are unaffected but the paternal grandfather of
Patients II1 II2 and II4 had recurrent bouts of jaundice withno liver disease Complement levels of Patients II2 II4 III1III2 and III7 are presented in supplementary Table 2 Com-plement levels were not available from Patient II1
Fig 1 Pathological findings in Patients III1 and II1 (AndashC) Patient III1 first renal biopsy taken at the age of 4 years (A) Glomerulus with slight mesangialexpansion and thickened capillary walls with double contours (Periodic acid-Schiff staining) (B) Immunohistochemical staining for C3 (anti-C3 from DakoGlostrup Denmark) showing marked labelling of capillary walls (A and B original magnification 3400) (C) Ultrastructure showing a capillary withelectron-dense deposits (arrowheads) in subendothelial position and effacement of podocyte foot processes (arrow) Inset shows mesangial cell interpositionScale bar represents 1 lm (C) and 2 lm (C inset) (D) Patient III1 second renal biopsy at age 6 years Hypercellular glomerulus with thickened GBMs andnarrowed glomerular capillaries (inset) One sclerosing glomerulus with collapsed glomerular tuft segmental sclerosis and thickening of Bowmanrsquos capsuleis visible (arrow) A group of tubules with reduced diameter and thickened basement membrane (arrowhead) indicating tubular atrophy (original magni-fication 3200 inset 31000) (EndashG) Patient III1 third renal biopsy at age 10 years Panel E shows thickening of the GBM occluded capillaries (arrowhead)and one thrombus in a glomerular capillary (see arrow) Panel F shows C1q labelling of capillary walls (anti-C1q from Dako) Panel G ultrastructure showingelectron-dense precipitations in capillary lumina (arrowheads) and duplication of the GBM (arrow) Activated endothelial cells contain many organellesEffaced podocyte foot processes (scale bar 2 lm) (H) Patient II1 post-mortem renal tissue Glomerulus with intracapillary thrombi and swollen endothelialcells (trichrome stain thrombi are red erythrocytes yellow) E F and H original magnification 3400
Thrombotic microangiopathy mimicking MPGN 3
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
DNA sequencing was carried out as described in thesupplementary methods Patients II1 II2 II4 III1 III2and III7 carry a previously described MCP mutation(Y155D) [5] and two C3 mutations R713W (in Exon 17)and G1094R (in Exon 26) R713W has been previouslydescribed [2] whereas G1094R is a novel mutationsituated one amino acid from a described mutation atposition D1093N [2] These C3 mutations were presum-ably localized on the same allele due to the common patternof inheritance and they were not found in DNA from100 healthy controls In addition Patient III1 has a hetero-zygous deletion of CFHR13 and autoantibodies to CFHwere detected upon debut of disease but not 5 yearslater The MCP mutation was found in two unaffectedfamily members and the C3 mutations were found in oneunaffected family member The mutations and their pre-sumed functional consequences are presented in Figure 2and Table 2 as well as the supplementary results anddiscussion
Discussion
In this report we describe a child with progressive renal fail-ure and pathology exhibiting a membranoproliferative pattern
Other family members presented with features of aHUS Allaffected family members were found to share complementmutations in C3 and MCP This study suggests that differingclinical and pathological phenotypes of aHUS may have acommon molecular basis Thrombotic microangiopathy canthus develop even in the absence of clinical HUS
Patient III1 did not exhibit clinical signs of aHUSalthough haemolysis without thrombocytopenia was de-tected 6 years after debut of disease His biopsies showeda membranoproliferative pattern including C3 positivityThese findings are compatible with chronic thrombotic mi-croangiopathy except for the presence of subendothelialelectron-dense deposits Electron-dense deposits are a pecu-liar feature in this patient usually not observed in thromboticmicroangiopathy and making the distinction from MPGNType I difficult Furthermore strong C1q labelling is notfound in thrombotic microangiopathy but usually associatedwith systematic lupus erythematosis C1q nephropathy [7] orMPGN Type I but the weak IgG staining suggests that therenal deposits were probably not mediated by immune com-plexes The finding of membranoproliferative features is inline with other studies suggesting that there might be a con-tinuous spectrum of morphological changes from thromboticmicroangiopathy to MPGN [8ndash10] This group of disorderscould also encompass the more recently described C3
Table 2 Molecular characteristics of genetic alterations in patientsa
Complement protein Mutation or deletion Codon Protein Phenotype Reference
MCP Y155D 565 TgtG Tyr155Asp Reduced cell-surface expression of MCPNo detectable C3b- or C4b-binding activityand negligible cofactor activity
[5]
C3 G1094R 3346 GgtC Gly1116Arg Adjacent mutation (D1093N) showedreduced binding to MCP and to alesser degree CFH
[2]
C3 R713W 2203 CgtT Arg735Trp No documented abnormality NormalC3 binding to CFB CFH MCPand soluble CR1
[2]
CFHR13 DCFHR13b Associated with the presence ofanti-CFH antibodies
[6]
aCFB factor B CFH factor H MCP membrane cofactor proteinCD46 CR1 complement receptor 1 CFHR factor H-related protein All geneticalterations including DCFHR13 were heterozygousbThis deletion has also been detected in the healthy population
Fig 2 Pedigree of the investigated family CFH ab anti-factor H (CFH) antibodies The affected individuals in two generations are marked in filledboxes and circles Mutations C3 G1094R 1 R713W and MCP Y155D DCFHR13 heterozygous deletion of CFHR1 and CFHR3 Serum anti-CFHantibodies detected in Patient III1 at debut but not 5 years later Patients III2 and III7 were tested and did not have serum anti-CFH antibodies
4 D Brackman et al
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
glomerulopathy with isolated C3 deposits [11] However thestrong C1q labelling in the patientrsquos biopsies is not compatiblewith this diagnosis
The presence of complement activation due to mutationsin C3 and MCP enabled the pathological features toprogress even in the absence of overt HUS The clinicaland pathological features overlap with MPGN Type Iindicating that aHUS and MPGN may share a commonmolecular background We thus conclude that this patientexhibited an unusual presentation of chronic thromboticmicroangiopathy mimicking MPGN Type I
Supplementary data
Supplementary data are available online at httpndtoxfordjournalsorg
Acknowledgements This study was supported by grants from The SwedishResearch Council (K2010-65X-14008-10-3 to DK) Torsten and RagnarSoderberg Foundation The fund for Renal Research Crown PrincessLovisarsquos Society for Child Care Konung Gustaf Vs 80-aringrsfond FannyEkdahlrsquos Foundation (all to DK) DK is the recipient of a clinicalndashexperimental research fellowship from the Royal Swedish Academy ofSciences The Queen Silvia Jubilee Fond to LS French Agence Nationalede la Recherche (R09097DS) Programme Hospitalier de Recherche Clin-ique (AOM05130P051065) and French Association for Information andResearch on Genetic Renal Diseases (AIRG) to VF-B A preliminaryversion of the manuscript appeared in the PhD thesis of Dr LS
The authors would like to thank Dr Marie-Agnes Dragon-Durey HopitalEuropeen Georges-Pompidou Service drsquoImmunologie Biologique Parisfor analysis of anti-CFH antibodies in Patient III1 and Professor MartinOlsson Department of Transfusion Medicine Lund University for controlsamples
Transparency declaration VF-B was consultant for and gave lecturesfor Alexion Pharmaceuticals during 2010 DK was the national coordi-nator in Sweden of the multi-center trial of Eculizumab (Alexion Pharma-ceuticals) in patients with atypical hemolytic uremic syndrome
Conflict of interest statement None declared
References
1 Noris M Remuzzi G Atypical hemolytic-uremic syndrome N EnglJ Med 2009 361 1676ndash1687
2 Fremeaux-Bacchi V Miller EC Liszewski MK et al Mutations incomplement C3 predispose to development of atypical hemolytic ure-mic syndrome Blood 2008 112 4948ndash4952
3 Licht C Fremeaux-Bacchi V Hereditary and acquired complementdysregulation in membranoproliferative glomerulonephritis ThrombHaemost 2009 101 271ndash278
4 Vaziri-Sani F Holmberg L Sjoholm AG et al Phenotypic expressionof factor H mutations in patients with atypical hemolytic uremic syn-drome Kidney Int 2006 69 981ndash988
5 Fremeaux-Bacchi V Moulton EA Kavanagh D et al Genetic and func-tional analyses of membrane cofactor protein (CD46) mutations in atyp-ical hemolytic uremic syndrome J Am Soc Nephrol 2006 172017ndash2025
6 Zipfel PF Edey M Heinen S et al Deletion of complement factor H-related genes CFHR1 and CFHR3 is associated with atypical hemo-lytic uremic syndrome PLoS Genet 2007 3 e41
7 Pickering MC Cook HT Translational mini-review series on comple-ment factor H renal diseases associated with complement factor Hnovel insights from humans and animals Clin Exp Immunol 2008151 210ndash230
8 Servais A Fremeaux-Bacchi V Lequintrec M et al Primary glomer-ulonephritis with isolated C3 deposits a new entity which sharescommon genetic risk factors with haemolytic uraemic syndromeJournal of medical genetics 2007 44 193ndash199
9 Skerka C Licht C Mengel M et al Autoimmune forms of thromboticmicroangiopathy and membranoproliferative glomerulonephritis In-dications for a disease spectrum and common pathogenic principlesMol Immunol 2009 46 2801ndash2807
10 Fakhouri F Fremeaux-Bacchi V Noel LH et al C3 glomerulopathy anew classification Nat Rev Nephrol 2010 6 494ndash499
11 Vizjak A Ferluga D Rozic M et al Pathology clinical presentations andoutcomes of C1q nephropathy J Am Soc Nephrol 2008 19 2237ndash2244
Received for publication 20611 Accepted in revised form 20611
Thrombotic microangiopathy mimicking MPGN 5
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from

DNA sequencing was carried out as described in thesupplementary methods Patients II1 II2 II4 III1 III2and III7 carry a previously described MCP mutation(Y155D) [5] and two C3 mutations R713W (in Exon 17)and G1094R (in Exon 26) R713W has been previouslydescribed [2] whereas G1094R is a novel mutationsituated one amino acid from a described mutation atposition D1093N [2] These C3 mutations were presum-ably localized on the same allele due to the common patternof inheritance and they were not found in DNA from100 healthy controls In addition Patient III1 has a hetero-zygous deletion of CFHR13 and autoantibodies to CFHwere detected upon debut of disease but not 5 yearslater The MCP mutation was found in two unaffectedfamily members and the C3 mutations were found in oneunaffected family member The mutations and their pre-sumed functional consequences are presented in Figure 2and Table 2 as well as the supplementary results anddiscussion
Discussion
In this report we describe a child with progressive renal fail-ure and pathology exhibiting a membranoproliferative pattern
Other family members presented with features of aHUS Allaffected family members were found to share complementmutations in C3 and MCP This study suggests that differingclinical and pathological phenotypes of aHUS may have acommon molecular basis Thrombotic microangiopathy canthus develop even in the absence of clinical HUS
Patient III1 did not exhibit clinical signs of aHUSalthough haemolysis without thrombocytopenia was de-tected 6 years after debut of disease His biopsies showeda membranoproliferative pattern including C3 positivityThese findings are compatible with chronic thrombotic mi-croangiopathy except for the presence of subendothelialelectron-dense deposits Electron-dense deposits are a pecu-liar feature in this patient usually not observed in thromboticmicroangiopathy and making the distinction from MPGNType I difficult Furthermore strong C1q labelling is notfound in thrombotic microangiopathy but usually associatedwith systematic lupus erythematosis C1q nephropathy [7] orMPGN Type I but the weak IgG staining suggests that therenal deposits were probably not mediated by immune com-plexes The finding of membranoproliferative features is inline with other studies suggesting that there might be a con-tinuous spectrum of morphological changes from thromboticmicroangiopathy to MPGN [8ndash10] This group of disorderscould also encompass the more recently described C3
Table 2 Molecular characteristics of genetic alterations in patientsa
Complement protein Mutation or deletion Codon Protein Phenotype Reference
MCP Y155D 565 TgtG Tyr155Asp Reduced cell-surface expression of MCPNo detectable C3b- or C4b-binding activityand negligible cofactor activity
[5]
C3 G1094R 3346 GgtC Gly1116Arg Adjacent mutation (D1093N) showedreduced binding to MCP and to alesser degree CFH
[2]
C3 R713W 2203 CgtT Arg735Trp No documented abnormality NormalC3 binding to CFB CFH MCPand soluble CR1
[2]
CFHR13 DCFHR13b Associated with the presence ofanti-CFH antibodies
[6]
aCFB factor B CFH factor H MCP membrane cofactor proteinCD46 CR1 complement receptor 1 CFHR factor H-related protein All geneticalterations including DCFHR13 were heterozygousbThis deletion has also been detected in the healthy population
Fig 2 Pedigree of the investigated family CFH ab anti-factor H (CFH) antibodies The affected individuals in two generations are marked in filledboxes and circles Mutations C3 G1094R 1 R713W and MCP Y155D DCFHR13 heterozygous deletion of CFHR1 and CFHR3 Serum anti-CFHantibodies detected in Patient III1 at debut but not 5 years later Patients III2 and III7 were tested and did not have serum anti-CFH antibodies
4 D Brackman et al
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from
glomerulopathy with isolated C3 deposits [11] However thestrong C1q labelling in the patientrsquos biopsies is not compatiblewith this diagnosis
The presence of complement activation due to mutationsin C3 and MCP enabled the pathological features toprogress even in the absence of overt HUS The clinicaland pathological features overlap with MPGN Type Iindicating that aHUS and MPGN may share a commonmolecular background We thus conclude that this patientexhibited an unusual presentation of chronic thromboticmicroangiopathy mimicking MPGN Type I
Supplementary data
Supplementary data are available online at httpndtoxfordjournalsorg
Acknowledgements This study was supported by grants from The SwedishResearch Council (K2010-65X-14008-10-3 to DK) Torsten and RagnarSoderberg Foundation The fund for Renal Research Crown PrincessLovisarsquos Society for Child Care Konung Gustaf Vs 80-aringrsfond FannyEkdahlrsquos Foundation (all to DK) DK is the recipient of a clinicalndashexperimental research fellowship from the Royal Swedish Academy ofSciences The Queen Silvia Jubilee Fond to LS French Agence Nationalede la Recherche (R09097DS) Programme Hospitalier de Recherche Clin-ique (AOM05130P051065) and French Association for Information andResearch on Genetic Renal Diseases (AIRG) to VF-B A preliminaryversion of the manuscript appeared in the PhD thesis of Dr LS
The authors would like to thank Dr Marie-Agnes Dragon-Durey HopitalEuropeen Georges-Pompidou Service drsquoImmunologie Biologique Parisfor analysis of anti-CFH antibodies in Patient III1 and Professor MartinOlsson Department of Transfusion Medicine Lund University for controlsamples
Transparency declaration VF-B was consultant for and gave lecturesfor Alexion Pharmaceuticals during 2010 DK was the national coordi-nator in Sweden of the multi-center trial of Eculizumab (Alexion Pharma-ceuticals) in patients with atypical hemolytic uremic syndrome
Conflict of interest statement None declared
References
1 Noris M Remuzzi G Atypical hemolytic-uremic syndrome N EnglJ Med 2009 361 1676ndash1687
2 Fremeaux-Bacchi V Miller EC Liszewski MK et al Mutations incomplement C3 predispose to development of atypical hemolytic ure-mic syndrome Blood 2008 112 4948ndash4952
3 Licht C Fremeaux-Bacchi V Hereditary and acquired complementdysregulation in membranoproliferative glomerulonephritis ThrombHaemost 2009 101 271ndash278
4 Vaziri-Sani F Holmberg L Sjoholm AG et al Phenotypic expressionof factor H mutations in patients with atypical hemolytic uremic syn-drome Kidney Int 2006 69 981ndash988
5 Fremeaux-Bacchi V Moulton EA Kavanagh D et al Genetic and func-tional analyses of membrane cofactor protein (CD46) mutations in atyp-ical hemolytic uremic syndrome J Am Soc Nephrol 2006 172017ndash2025
6 Zipfel PF Edey M Heinen S et al Deletion of complement factor H-related genes CFHR1 and CFHR3 is associated with atypical hemo-lytic uremic syndrome PLoS Genet 2007 3 e41
7 Pickering MC Cook HT Translational mini-review series on comple-ment factor H renal diseases associated with complement factor Hnovel insights from humans and animals Clin Exp Immunol 2008151 210ndash230
8 Servais A Fremeaux-Bacchi V Lequintrec M et al Primary glomer-ulonephritis with isolated C3 deposits a new entity which sharescommon genetic risk factors with haemolytic uraemic syndromeJournal of medical genetics 2007 44 193ndash199
9 Skerka C Licht C Mengel M et al Autoimmune forms of thromboticmicroangiopathy and membranoproliferative glomerulonephritis In-dications for a disease spectrum and common pathogenic principlesMol Immunol 2009 46 2801ndash2807
10 Fakhouri F Fremeaux-Bacchi V Noel LH et al C3 glomerulopathy anew classification Nat Rev Nephrol 2010 6 494ndash499
11 Vizjak A Ferluga D Rozic M et al Pathology clinical presentations andoutcomes of C1q nephropathy J Am Soc Nephrol 2008 19 2237ndash2244
Received for publication 20611 Accepted in revised form 20611
Thrombotic microangiopathy mimicking MPGN 5
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from

glomerulopathy with isolated C3 deposits [11] However thestrong C1q labelling in the patientrsquos biopsies is not compatiblewith this diagnosis
The presence of complement activation due to mutationsin C3 and MCP enabled the pathological features toprogress even in the absence of overt HUS The clinicaland pathological features overlap with MPGN Type Iindicating that aHUS and MPGN may share a commonmolecular background We thus conclude that this patientexhibited an unusual presentation of chronic thromboticmicroangiopathy mimicking MPGN Type I
Supplementary data
Supplementary data are available online at httpndtoxfordjournalsorg
Acknowledgements This study was supported by grants from The SwedishResearch Council (K2010-65X-14008-10-3 to DK) Torsten and RagnarSoderberg Foundation The fund for Renal Research Crown PrincessLovisarsquos Society for Child Care Konung Gustaf Vs 80-aringrsfond FannyEkdahlrsquos Foundation (all to DK) DK is the recipient of a clinicalndashexperimental research fellowship from the Royal Swedish Academy ofSciences The Queen Silvia Jubilee Fond to LS French Agence Nationalede la Recherche (R09097DS) Programme Hospitalier de Recherche Clin-ique (AOM05130P051065) and French Association for Information andResearch on Genetic Renal Diseases (AIRG) to VF-B A preliminaryversion of the manuscript appeared in the PhD thesis of Dr LS
The authors would like to thank Dr Marie-Agnes Dragon-Durey HopitalEuropeen Georges-Pompidou Service drsquoImmunologie Biologique Parisfor analysis of anti-CFH antibodies in Patient III1 and Professor MartinOlsson Department of Transfusion Medicine Lund University for controlsamples
Transparency declaration VF-B was consultant for and gave lecturesfor Alexion Pharmaceuticals during 2010 DK was the national coordi-nator in Sweden of the multi-center trial of Eculizumab (Alexion Pharma-ceuticals) in patients with atypical hemolytic uremic syndrome
Conflict of interest statement None declared
References
1 Noris M Remuzzi G Atypical hemolytic-uremic syndrome N EnglJ Med 2009 361 1676ndash1687
2 Fremeaux-Bacchi V Miller EC Liszewski MK et al Mutations incomplement C3 predispose to development of atypical hemolytic ure-mic syndrome Blood 2008 112 4948ndash4952
3 Licht C Fremeaux-Bacchi V Hereditary and acquired complementdysregulation in membranoproliferative glomerulonephritis ThrombHaemost 2009 101 271ndash278
4 Vaziri-Sani F Holmberg L Sjoholm AG et al Phenotypic expressionof factor H mutations in patients with atypical hemolytic uremic syn-drome Kidney Int 2006 69 981ndash988
5 Fremeaux-Bacchi V Moulton EA Kavanagh D et al Genetic and func-tional analyses of membrane cofactor protein (CD46) mutations in atyp-ical hemolytic uremic syndrome J Am Soc Nephrol 2006 172017ndash2025
6 Zipfel PF Edey M Heinen S et al Deletion of complement factor H-related genes CFHR1 and CFHR3 is associated with atypical hemo-lytic uremic syndrome PLoS Genet 2007 3 e41
7 Pickering MC Cook HT Translational mini-review series on comple-ment factor H renal diseases associated with complement factor Hnovel insights from humans and animals Clin Exp Immunol 2008151 210ndash230
8 Servais A Fremeaux-Bacchi V Lequintrec M et al Primary glomer-ulonephritis with isolated C3 deposits a new entity which sharescommon genetic risk factors with haemolytic uraemic syndromeJournal of medical genetics 2007 44 193ndash199
9 Skerka C Licht C Mengel M et al Autoimmune forms of thromboticmicroangiopathy and membranoproliferative glomerulonephritis In-dications for a disease spectrum and common pathogenic principlesMol Immunol 2009 46 2801ndash2807
10 Fakhouri F Fremeaux-Bacchi V Noel LH et al C3 glomerulopathy anew classification Nat Rev Nephrol 2010 6 494ndash499
11 Vizjak A Ferluga D Rozic M et al Pathology clinical presentations andoutcomes of C1q nephropathy J Am Soc Nephrol 2008 19 2237ndash2244
Received for publication 20611 Accepted in revised form 20611
Thrombotic microangiopathy mimicking MPGN 5
at Girls U
niversity on August 10 2011
ndtoxfordjournalsorgD
ownloaded from