Embed Size (px)
Citation preview
Thyroid Malignancy
• 39 y/o female from Bicol• C/C: anterior neck mass
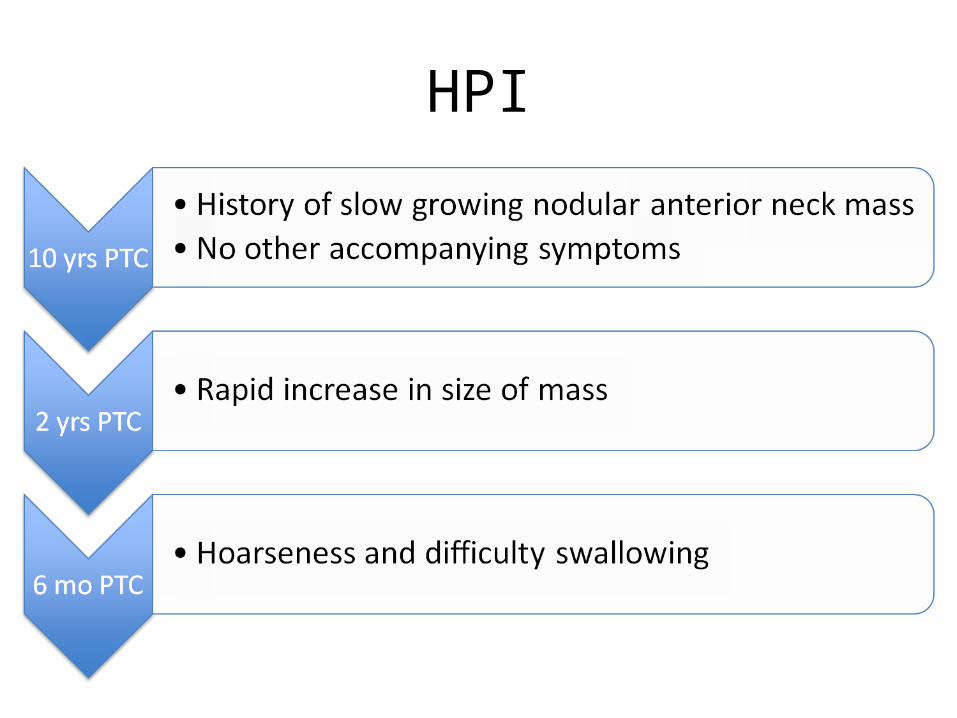
HPI
ROS
• No fever, weight loss and tremors• No chest pain and easy fatigability• No abdominal pain
• Past medical and family history both unremarkable
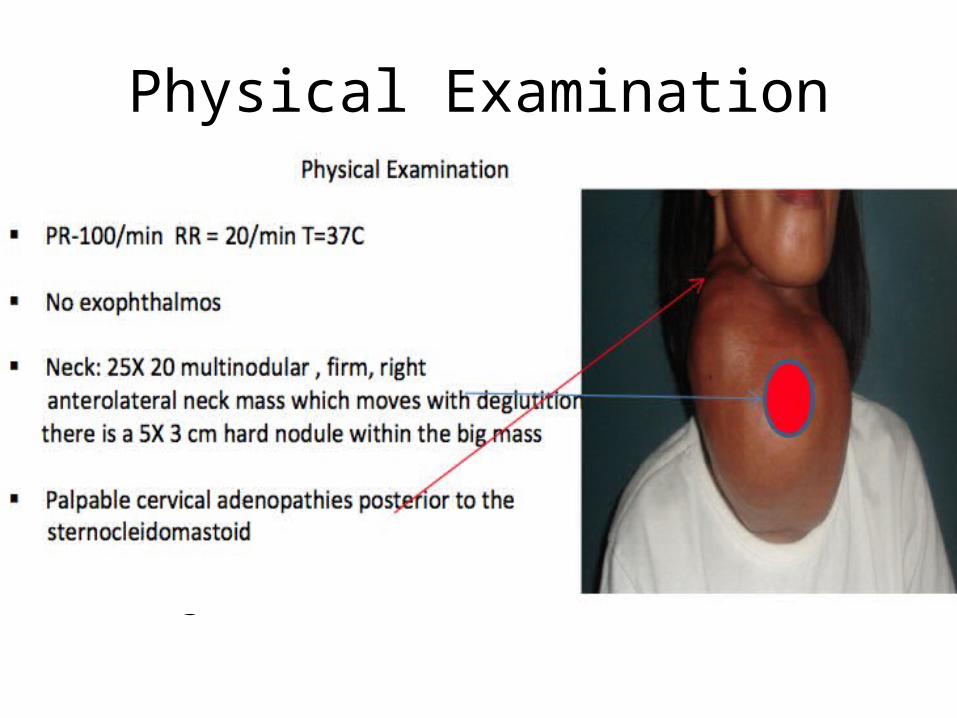
Physical Examination
• PR = 100/minRR = 20/minTemperature = 37 °C
• No exophthalmos• Neck:– 12x10 cm multilobulated firm mass on the left
neck, moves with deglutition
What is your clinical impression?What are the differential diagnosis?
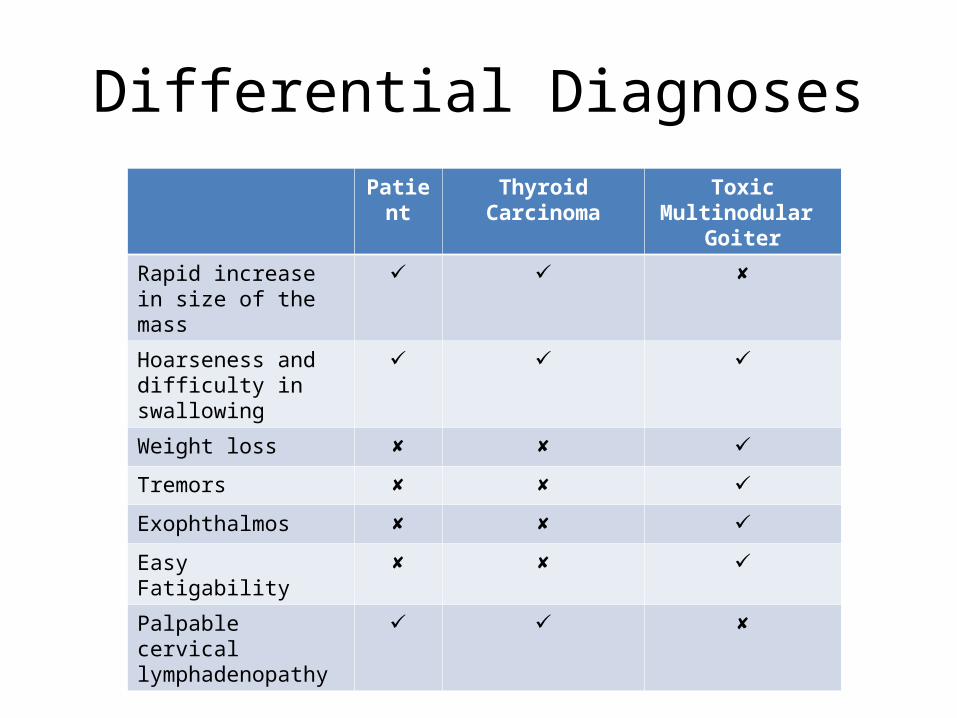
Differential DiagnosesPatient Thyroid Carcinoma Toxic Multinodular
Goiter
Rapid increase in size of the mass
Hoarseness and difficulty in swallowing
Weight loss
Tremors
Exophthalmos
Easy Fatigability
Palpable cervical lymphadenopathy
Thyroid cancer
• Most common malignancy of the endocrine system
• Accounts for less than 1% of all malignancies• Common among chinese males & filipino
females
Risk factors for thyroid carcinoma in patients with thyroid nodule
• History of head & neck irradiation• Age <20 or > 70 y/o• Increased nodule size (>4cm)• New or enlarging neck mass• Male gender
• Family history of thyroid cancer or MEN 2
• Vocal cord paralysis, hoarse voice• Nodule fixed to adjacent structures• Suspected lymph node involvement• Iodine deficiency (follicular)
Clinical features:
• Lump in the neck• Gradually enlarging mass• Firm or hard• Rapidly growing: soft or fluctuant• May be painful• May present with hoarseness, dysphagia,
dysphonia, dyspnea• Rare: hyperthyroidism
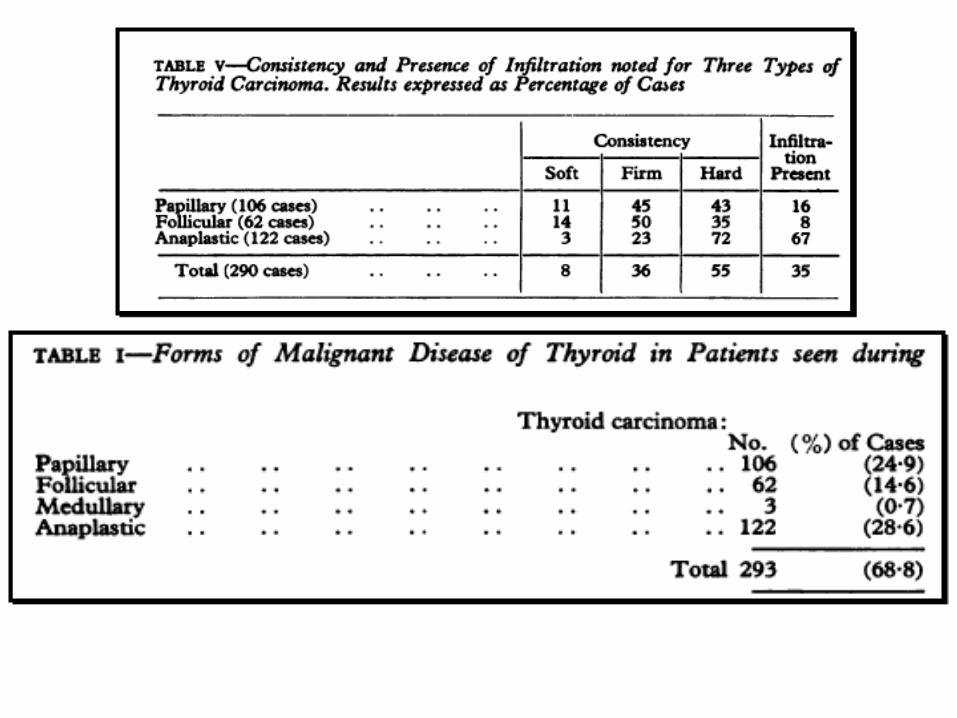
Papillary Carcinoma
• 80-85%• Predominant: children & individuals exposed to
external radiation• 2:1 F:M ratio• Mean age: 30-40 y/o• S/Sx: slow growing painless mass– Dysphagia, dyspnea, dsyphonia– Lymph nodes metastases (common)– Distal mets uncommon (lungs, bone, liver, brain)

• Characteristic cellular patterns: Orphan Annie nuclei
• Psamomma bodies• Multifocality (85%)• Prognosis: excellent (95% 10 yr survival rate)
Diagnosis• discovered when a hard nodule is found in
multinodular goiter• when enlarged cervical lymph nodes are
detected• when there are unidentified metastatic lesions
elsewhere in the body• Other clinical signs that could indicate papillary
thyroid are: – fixation to the trachea, stony hardness, damage to
recurrent laryngeal or cervical sympathetic nerves.
Follicular Carcinoma
• Second most common (10%) • Iodine deficient areas• 3:1 F:M ratio• Mean age: 50 y/o• Usually solitary (rapid size increase & goiter)• s/sx: pain & cervical lymphadenopathy
uncommon initial presentation
• 1%: hyperfunctioning - thyrotoxicosis• Solitary & encapsulated• Prognosis: mortality 15% at 10 yrs, 30% at 20
yrs
Hurthle Cell CA
• 3-5%• Variant of follicular CA• Vascular or capsular invasion• Multifocal & bilateral• Metastasize to local & distant sites• Higher mortality rate
Medullary CA
• 5%• From parafollicular or C cells • 1.5:1 F:M ratio• Mean age: 50-60 y/o• 70-80% are sporadic• 20-30% familial autosomal dominant
syndromes
• s/sx:neck mass w/ cervical lymphadenopathy - local pain - dysphagia, dyspnea or dysphonia• 2-4%: Cushing’s syndrome• Unilateral (sporadic); multicentric (familial)• Presence of amyloid• Prognosis: related to disease stage
Anaplastic CA
• 1%• F>M• Mean age: 65 y/o • s/sx: rapidly enlarging, long standing neck
mass, painful- dysphonia, dysphagia, dyspnea
• Tumor: large, hard, poorly circumscribed & fixed
• Palpable lymph nodes• Metastatic spread• Prognosis: one of the most aggressive, few
survive beyond 6 months
Lymphoma
• <1%• Most: Non-Hodgkin’s B-cell type• 2-3xF>M• Age: 62 y/o• Patients with chronic lymphocytic thyroiditis• Prognosis: overall 5 yr survival rate: 50%
2. What work ups are needed, if any?
Evaluation of a Thyroid Nodule• History
– Risk factors for thyroid cancer• History of thyroid irradiation, especially in infancy or childhood• Age < 20 yr• Male sex• Family history of thyroid cancer or multiple endocrine neoplasia• A solitary nodule• Dysphagia• Dysphonia• Increasing size (particularly rapid growth or growth while receiving thyroid
suppression treatment)• Physical Examination
– Signs that suggest thyroid cancer• stony hard consistency or fixation to surrounding structures• cervical lymphadenopathy• hoarseness due to recurrent laryngeal nerve paralysis
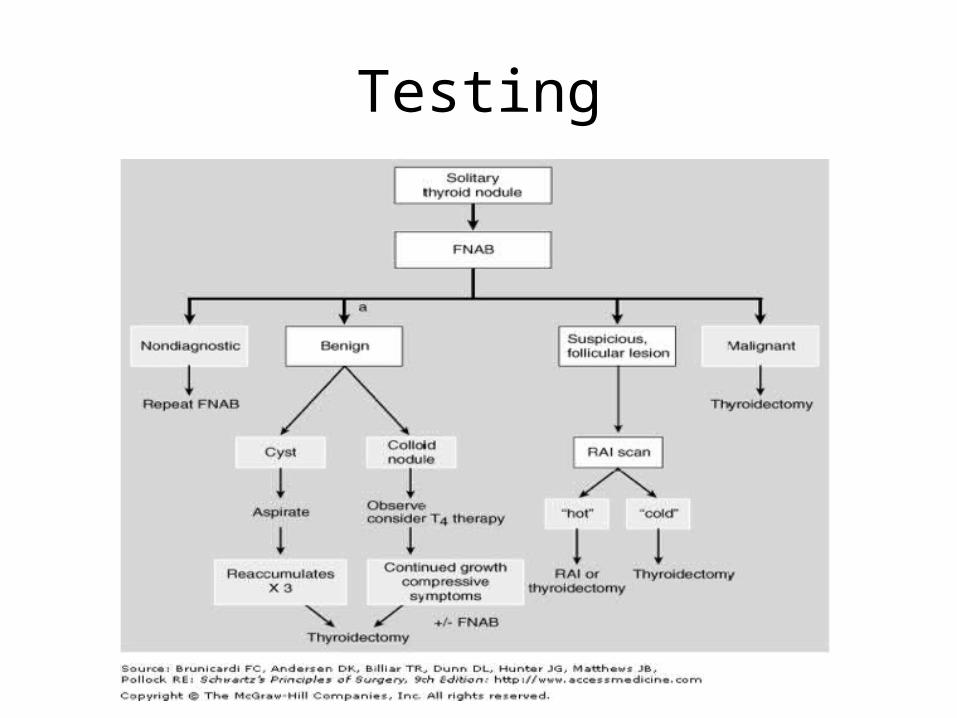
Testing
Testing
• Fine-Needle Aspiration Biopsy (FNAB)– Cornerstone in the evaluation of solitary thyroid
nodules and also dominant nodules within multinodular goiters
– Currently considered to be the best first-line diagnostic procedure in the evaluation of the thyroid nodule
Fine-Needle Aspiration Biopsy
• Advantages:– Safe– Cost-effective– Minimally invasive– Leads to better selection of patients for surgery
than any other test (Rojeski, 1985)– Halved the number of patients requiring
thyroidectomy (Mazzaferri, 1993)– Double the yield of cancer in those who do
undergo thyroidectomy (Mazzaferri, 1993)
Fine-Needle Aspiration Biopsy
• Four Categories of Cytologic Diagnosis– Benign (Negative) – 69%– Suspicious (Indeterminate) – 10%– Malignant (Positive) – 4%– Unsatisfactory (Nondiagnostic) – 17%
Reference: Gharib, H. (2008). Fine-Needle Aspiration Biopsy of the Thyroid Gland. Thyroid Disease Manager.
Fine-Needle Aspiration Biopsy• Limitations
– Skill of the aspirator– Expertise of the cytologist– Difficulty in distinguishing some benign cellular adenomas from
their malignant counterparts (follicular and Hurthle cell)
• Sensitivity: 65 – 98% (avg. 83%)• Specificity: 72 – 100% (avg. 92%)• Positive Predictive Value: 50 – 96% (avg. 75%)• False-negative Rates: 1.5 – 11.5% (avg. < 5%)• False-positive Rates: 0 – 8% (avg. 3%)
Reference: Gharib, H. (2008). Fine-Needle Aspiration Biopsy of the Thyroid Gland. Thyroid Disease Manager.
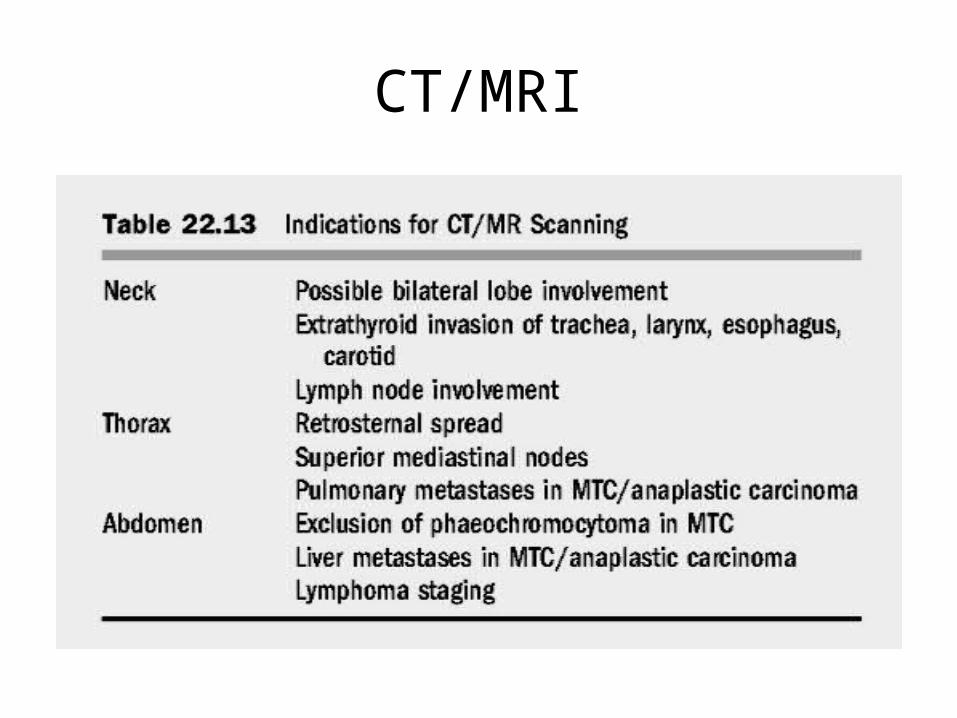
CT/MRI
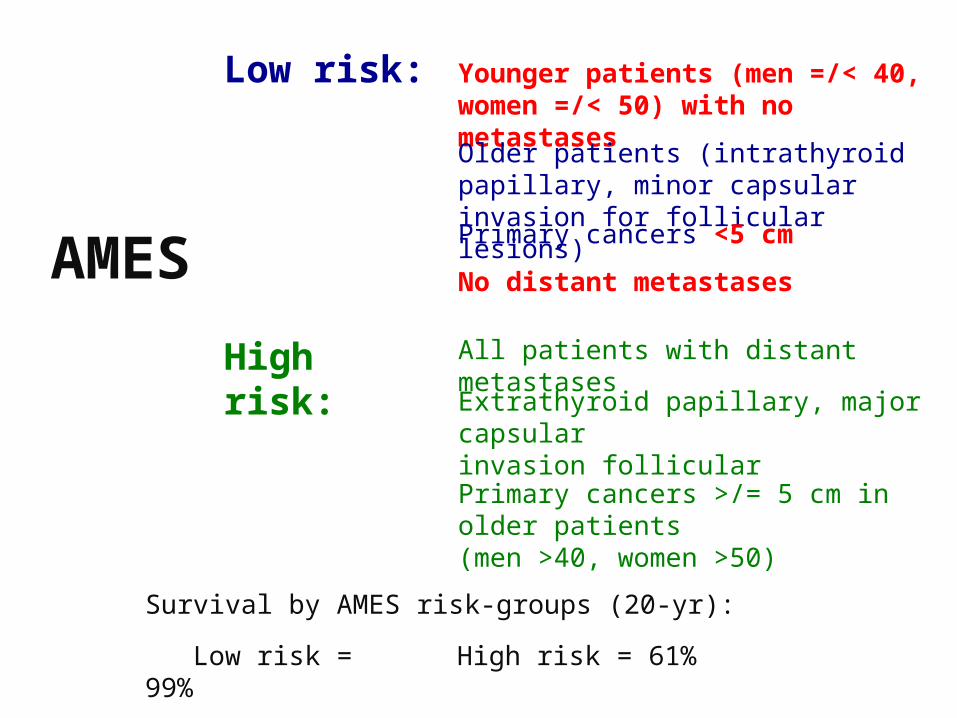
AMES
Low risk: Younger patients (men =/< 40, women =/< 50) with no metastases
Older patients (intrathyroid papillary, minor capsular invasion for follicular lesions)
Primary cancers <5 cm
No distant metastases
High risk: All patients with distant metastases
Extrathyroid papillary, major capsularinvasion follicular
Primary cancers >/= 5 cm in older patients(men >40, women >50)
Survival by AMES risk-groups (20-yr):
Low risk = 99% High risk = 61%
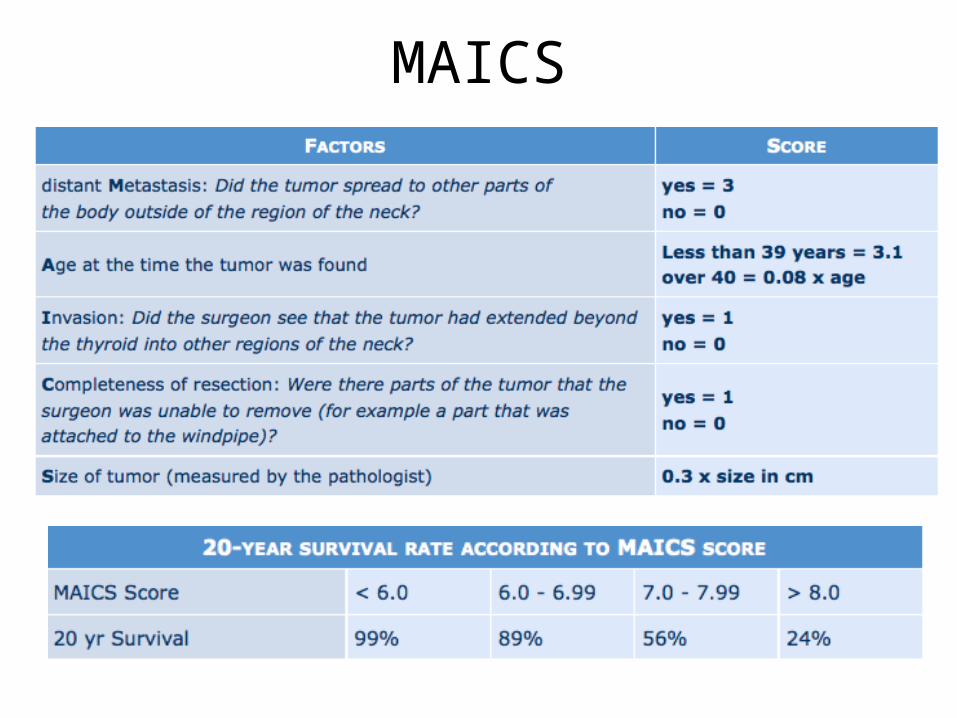
MAICS

AMES
Surgical Treatment: Papillary CA
High risk or bilateral tumors: Total or near - total thyroidectomy
Minimal Papillary Thyroid TumorUnilateral lobectomy and isthmusectomy
•Enables the use of RAI for detecting and treating residual thyroid tissue and metastatic disease. •Makes serum Tg level a more sensitive marker of recurrent or persistent disease•Eliminates contralateral occult cancer as sites of recurrence•Reduces risk of recurrence•Increases survival•Decreases 1% risk of progression to ATC•Reduces need for reoperative surgery
Total Thyroidectomy
•Lower complication rate•Recurrence is unusual (5%)•Excellent prognosis
Unilateral Lobectomy
Why Thyroidectomy?
• Recurrence rates are lowered and survival is improved when a patient underwent thyroidectomy
• Diminished survival was noted in patients with low-risk disease
Total Thyroidectomy
• Enables the use of RAI for detecting and treating residual thyroid tissue and metastatic disease.
• Makes serum Tg level a more sensitive marker of recurrent or persistent disease
• Eliminates contralateral occult cancer as sites of recurrence
• Reduces risk of recurrence• Increases survival• Decreases 1% risk of progression to ATC• Reduces need for reoperative surgery
1) 30%-87.5% of papillary carcinomas involve opposite lobe (Hirabayashi, 1961, Russell, 1983)
2) 7%-10% develop recurrence in the contralateral lobe (Soh, 1996)
3) Lower recurrence rates, some studies show increased survival (Mazzaferri, 1991)
4) Facilitates earlier detection and tx for recurrent or metastatic carcinoma with RAI (Soh, 1996)
5) Residual WDTC has the potential to dedifferentiate to ATC
Rationale for total thyroidectomy
Indications for total thyroidectomy
1) Patients older than 40 years with papillary or follicular carcinoma
2) Anyone with a thyroid nodule with a history of irradiation
3) Patients with bilateral disease
Rationale for subtotal thyroidectomy
1) Lower incidence of complications Hypoparathyroidism (1%-29%) (Schroder, 1993) Recurrent laryngeal nerve injury (1%-2%) (Schroder,
1993) Superior laryngeal nerve injury
2) Long term prognosis is not improved by total thyroidectomy (Grant, 1988)
Complications
• Injury to RLN, Superior Laryngeal Nerve• Transient hypocalcemia (50%)• Permanent hypoparathyroidism (<2%)• Postoperative hematoma• Bilateral vocal cord dysfunction
Postoperative Management of Differentiated Thyroid Cancer
• Thyroid Hormone– After thyroidectomy, should placed on
thyroxine to ensure that the patient remains euthyroid
– serves as a replacement therapy and also suppresses TSH
– reduces growth stimulus to possible residual cancer cells
– reduces recurrence rates (papillary ca)– risk of tumor recurrence must be balanced
with the side effects associated with prolonged TSH suppression, including osteopenia and cardiac problems, particularly in older patients
Postoperative Management of Differentiated Thyroid Cancer
• Thyroglobulin Measurement– levels in patients who have undergone total
thyroidectomy should be below 2 ng/mL when the patient is taking T4, and below 5 ng/mL when the patient is hypothyroid
– level above 5ng/mL is highly suggestive of metastatic disease or persistent normal thyroid tissue. In this situation, radioiodine scan should be performed.
– Measure serum levels every 6 months, and then annually if the patient is clinically disease free
– Level >30 ng/ml is abnormal– High-risk patients should also have an
ultrasound of the neck and CT or MRI scan of the neck and mediastinum for early detection of any persistent or recurrent disease.
Postoperative Management of Differentiated Thyroid Cancer
• Radioiodine Therapy– I-131 whole body scan to detect residual normal thyroid tissue
&/or metastatic disease– Metastatic differentiated thyroid carcinoma can be
detected and treated by radioactive iodine in about 75 % of patients.
– Administration Scan at 4-6 weeks postoperatively repeat scan at 6-12 months after ablation repeat scan at 1 year then... every 2 years thereafter
• External Beam Radiotherapy and Chemotherapy– External beam radiotherapy is required
occasionally to control unresectable locally invasive or recurrent disease
– It also is of value for the treatment and control of pain from bony metastases when there is no appreciable radioiodine uptake.