Embed Size (px)
Citation preview

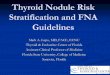
0 100 200 300 400
Trainee - PD
Trainee - US
Specialist - PD
Specialist - US
FNA approach
Cycle I Cycle II
Thyroid ultrasound and fine needle aspiration in one-stop surgical outpatient clinic: a 3-year audit
Introduction: Thyroid swelling is a common referral which constitutes more than 500 attendances to our specialist outpatient clinic ever year. Despite the majority of thyroid nodules are benign, there is an increasing trend of thyroid cancer in Hong Kong. Fine needle aspiration (FNA) is a simple, inexpensive and safe procedure for the detection of potentially malignant thyroid nodules. The reported sensitivity and specificity rates of thyroid FNA are 65-98% and 72-100% respectively. In order to find out the best surgical candidate, it is necessary to have an accurate thyroid FNA under palpation or ultrasound guidance. A one-stop thyroid ultrasound FNA clinic can increase efficiency of thyroid nodule management.
Objective: To evaluate the performance of fine needle aspiration of thyroid nodules in the surgical outpatient clinic
Methodology: All patients with thyroid FNA performed during their outpatient clinic visit from January 2009 to December 2011 were recruited. FNA was performed according to the American Thyroid Association Guideline. The decision on palpation directed or ultrasound guided approach was made by the attending surgeon. Trainees in rotational basis were also allowed to perform these procedures under supervision after adequate training. The thyroid FNA cytology was reported according to the Bethesda system. A comprehensive protocol for tracing FNA result and repeating biopsy were applied for non-diagnostic result.
Results: 851 FNAs were performed (494 in the first cycle and 357 in the second cycle). Majority (80%) were female patients with mean age of 53 years old. 487 (57%) patients had benign cytology and 17(2%) patients had suspicious or malignant FNA cytology in this study. The demographic data of the two cycles are shown in the following table:
Conclusion: Ultrasound scan of the neck and FNA are the essential investigations for thyroid nodules. We demonstrate that the use of ultrasound guidance for thyroid FNA decrease the non-diagnostic rate significantly. Patients with suspicious or malignant thyroid nodules are benefit from one-stop thyroid ultrasound FNA clinic being picked up and operated in a timely fashion.
DKK Tsui, KK Yau, CN Tang. Department of Surgery, Pamela Youde Nethersole Eastern Hospital.
0
100
200
300
400
500
600
700
1983
19
84
1985
19
86
1987
19
88
1989
19
90
1991
19
92
1993
19
94
1995
19
96
1997
19
98
1999
20
00
2001
20
02
2003
20
04
2005
20
06
2007
20
08
2009
Incidence of Thyroid Cancer in Hong Kong (Data Source: Hong Kong Cancer Registry, Hospital Authority)
Male Female Total 0
100
200
300
400
500
600
700
800
2009 2010 2011
Outpatient attendance for Thyroid Swelling (Data source: Clinical Data Analysis and Reporting System)
Male Female
In order to improve quality of thyroid nodule management, an additional portable ultrasound machine was installed in the clinic. Trainees were encouraged to use USG for guided FNA. FNA performance was distributed to team members regularly. Individual feedback and remedial sessions were given to the poor performers. The second cycle was started in January 2011 after implementation of these changes. The results of the two cycles were compared. Chi-square test was used for categoric data and t-test was used for continuous data. A P value of <0.05 was considered statistically significant.
PD – Palpation directed US – USG guidance
Cycle I = 2009 – 2010, Cycle II = 2011
Trainee (n=452)
Specialist (n=399)
P value
Approach: - palpation directed - USG guided
351 101
104 295
<0.001 *
Overall non-diagnostic no. (rate)
130 (29%) 62 (16%) 0.001 *
Non-diagnostic rate - by palpation directed - by USG guidance
31% 23%
15% 16%
0.002 * 0.101
Palpation directed (n=455)
USG guided (n=396)
P value
No. of FNA performed - by trainee - by specialist
351 104
101 295
<0.001 *
Overall non-diagnostic no. (rate)
123 (27%) 69 (17%) 0.001 *
Non-diagnostic no. - by trainee - by specialist
30% 15%
23% 16%
0.131 0.96
The performance of trainee versus specialist is shown below:
The performance of palpation directed versus USG guided FNA is shown below:
A sample slide of FNA result distributed to team members
FNAC record book: results were traced regularly Algorithm for management of thyroid nodule
* P < 0.05 * P < 0.05
Discussion: Trainees pay an important role in the management of thyroid nodules as they have performed almost half of the FNA in the outpatient clinic. As new trainees will be rotated to our team on half year basis, training on FNA techniques and performance review should be regularly employed. Ideally, on-site cytolopathological support will increase the yield of FNA and decrease non-diagnostic aspirate. However, this service is not available in our centre. The use of ultrasound guidance for FNA will improve the diagnostic accuracy. Trainees are encouraged to use them whenever possible. In the first cycle, trainees did not performed USG guided FNA because only one ultrasound machine was available in the outpatient clinic. With the implementation of a new portable ultrasound machine in the second cycle, trainee started to perform ultrasound guided aspirations. The non-diagnostic rate of trainee improved significantly on the second cycle as 70% of the FNA were performed under USG guidance. Although majority of thyroid nodules are benign, an improvement in FNA diagnostic accuracy will decrease the need for diagnostic lobectomy. More operation time can be left for management of suspicious and malignant thyroid nodules.
USG guided FNA with portable USG machine
References: 1. Gharib H, Goellner JR. Fine-needle aspiration biopsy of the thyroid: an appraisal. Ann Intern Med. 1993; 118: 282-9. 2. Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2009; 19: 1167-1299. 3. Cibas ES, Ali SZ. The Bethesda System for Reporting Thyroid Cytopathology. Am J Clin Pathol 2009; 132: 658-65. 4. Hag IAE, Kollur SM, Chiedozi LC. The role of FNA in the initial management of thyroid lesions: 7-year experience in a district general hospital. Cytopathology 2003; 14: 126-30. 5. Bohacek L, Milas M, Mitchell J, et al. Diagnostic Accuracy of Surgeon-Performed Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules. Ann Surg Oncol 2012; 19: 45-51.
First Cycle (N=494)
Second Cycle (N=357)
P value
No. of female patients (percentage) 396 (80%) 290 (81%) 0.697
Mean age of patients (years) 53.6 52.7 0.379
No. of FNA performed by trainee (proportion) No. of FNA performed by specialist
252 (51%) 242
200 (56%) 157
0.148
Approach: - USG guided - Palpation directed
146 (30%) 348
250 (70%) 107
<0.001 *
Mean size of thyroid nodule (cm) 2.5 2.2 <0.001 *
FNA Cytology Result Bethesda System (with proportion)
First Cycle (N=494)
Second Cycle (N=357)
P value
Benign - Class II
269 (54%) 218 (61%)
0.105
Indeterminate IIIA- Follicular lesion / atypia IIIB- Follicular Neoplasm
(18%) 77 12
(19%) 64 2
Suspicious or Malignant IV - Suspicious V - Malignant
(2%) 2 8
(2%) 3 4
Non-diagnostic – Class I 126 (26%) 66 (18%) Non-diagnostic FNA rate - by Trainee - by Specialist
33% 18%
24% 12%
0.029 * 0.127
The performance of FNA is shown in the following table:
* P < 0.05
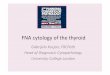
0
50
100
150
200
250
300
I II IIIA IIIB IV V
FNA Cytology Class
Cycle I Cycle II
I – Non-diagnostic II – Benign IIIA – Follicular lesion / atypia IIIB – Follicular neoplasm IV – Suspicious V - Malignant
* P < 0.05