Embed Size (px)
Citation preview
Title Slideoption 1 – blue background
Migraine Treatment Patterns and Opioid Use
Among Chronic and Episodic Migraine
Patients Identified by a Clinician-
Administered Semi-Structured Diagnostic
Interview
2018 CADTH Yu, et al 3
Justin S. Yu;1 Jelena M. Pavlovic;2 Stephen D. Silberstein;3 Michael L. Reed;4 Steve H.
Kawahara;5 Robert P. Cowan;6 Firas Dabbous;7 Karen L. Campbell;1 Riya Pulicharam;5
Hema N. Viswanathan;1 Richard B. Lipton8
1Allergan plc, Irvine, CA, USA2Montefiore Medical Center, Bronx, NY, USA
3Jefferson Headache Center, Philadelphia, PA, USA4Vedanta Research, Chapel Hill, NC, USA
5DaVita Medical Group; El Segundo, CA, USA6Stanford University School of Medicine, Stanford, CA, USA
7Independent Consultant, La Jolla, CA, USA8Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY, US
Presentation: Tuesday April 17, 10.30 to 11.45amPresentations must be taken to the SPEAKER READY Room the day before the presentationPresentations will be either 15 minutes including time for questionsComputer will run with 1024 by 768 resolution and 32 bit color, equipped with USB portsAdvise if presentation includes sound and/or video
PRESENTER’S DISCLOSURE
I have the following relevant financial relationships to disclose:
• Employed by Allergan plc
• Holds stock in Allergan plc
2018 CADTH Yu, et al 4
DISCLOSURES FOR ALL AUTHORS
This study was sponsored by Allergan plc, Dublin, Ireland. Writing and editorial assistance was provided to the authors by Lee B. Hohaia, PharmD of CHC (West Chester, PA, USA) and funded by Allergan plc, Dublin, Ireland. All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Financial arrangements of the authors with companies whose products may be related to the present report are listed below, as declared by the authors.
Justin Yu, MS, PharmD, is an employee of Allergan plc and receives stock or stock options. Jelena M. Pavlovic, MD, PhD has received honoraria from Allergan and the American Headache Society. Dr. Stephen Silberstein, as a consultant and/or advisory panel member,receives honoraria from Alder Biopharmaceuticals; Allergan, Inc.; Amgen; Avanir Pharmaceuticals, Inc.; eNeura; ElectroCore Medical, LLC; Labrys Biologics; Medscape, LLC; Medtronic, Inc.; Neuralieve; NINDS; Pfizer, Inc.; and Teva Pharmaceuticals. His employer receives research support from Allergan, Inc.; Amgen; Cumberland Pharmaceuticals, Inc.; ElectroCore Medical, Inc.; Labrys Biologics; Eli Lilly and Company; Merz Pharmaceuticals; and Troy Healthcare. Michael L. Reed, PhD, is Managing Director of Vedanta Research, which has received research funding from Allergan, Amgen, Dr. Reddy’s Laboratories, Eli Lilly GlaxoSmithKline, Merck & Co., Inc., and Novartis, via grants to the National Headache Foundation. Vedanta Research has received funding directly from Allergan for work on the CaMEO Study. Steve Kawahara, PharmD, in the past 12 months, has served as a consultant to Allergan and is a full-time employee of the DaVita Medical Group. Robert P. Cowan, MD and Firas Dabbous, PhD have no financial disclosures to report. Karen Campbell, PharmD, is a full-time employee of Allergan plc and owns stock in the company. Riya Pulicharam, MD, in the past 12 months, has served as a consultant and received consulting fees from DaVita medical Group. Hema Viswanathan B.Pharm, PhD is an employee of Allergan and holds stock, stock options, patent or other intellectual property in Allergan plc. Dr Lipton, MD, serves on the editorial board of Neurology and as senior advisor to Headache. He has received research support from the NIH. He also receives support from the Migraine Research Foundation and the National Headache Foundation. He has reviewed for the NIA and NINDS, serves as consultant, advisory board member, or has received honoraria from: Alder, Allergan, Amgen, Autonomic Technologies, Avanir, Boston Scientific, Dr. Reddy’s, Electrocore, Eli Lilly, eNeura Therapeutics, GlaxoSmithKlein, Merck, Novartis, Teva, Vedanta. He receives royalties from Wolff’s Headache, 8th Edition, Oxford Press University, 2009 and Informa. He holds stock options in eNeura Therapeutics and Biohaven.
2018 CADTH Yu, et al 5
INTRODUCTION
• Migraine is a leading cause of disability1 and affects approximately
12% of individuals in the United States2
− Affected individuals report reduced productivity, missed days from
work/school, and decreased health-related quality of life3,4
• Multiple treatment options exist for both acute and preventive
treatment of migraine
− Opioids have been used for acute treatment of migraine in people with
chronic migraine (CM; ≥15 headache days/month) and in people with
episodic migraine (EM; <15 headache day/month)
− Opioids are not recommended for regular use due to the risks of
medication overuse, tolerance, dependence, and opioid hyperalgesia5
2018 CADTH Yu, et al 6
1. Vos T et al. Lancet 2016;388(10053):1545-1602.
2. Buse DC et al. Headache 2012;52:1456-1470.
3. Lipton RB et al. Headache. 2001;41(7):646-657.
4. Blumenfeld AM et al. Cephalalgia. 2010;31(3):301-315.
5. Marmura MJ et al. Headache 2015;55:3-20.
OBJECTIVE
2018 CADTH Yu, et al 7
To describe migraine treatment patterns and opioid use in chronic migraine and episodic migraine patients using health claims data
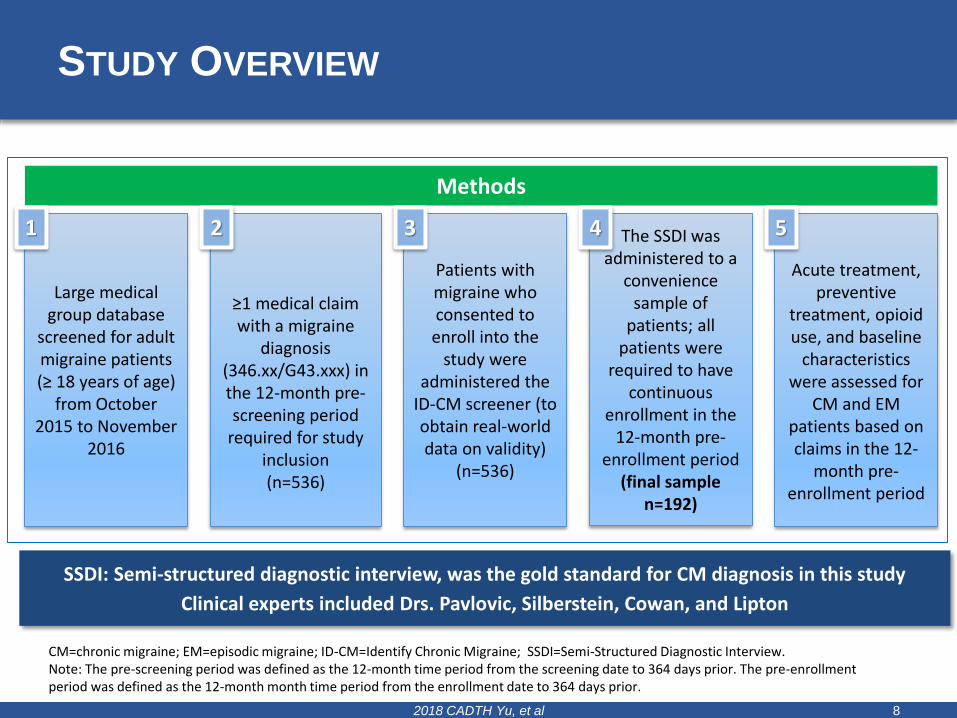
STUDY OVERVIEW
2018 CADTH Yu, et al 8
SSDI: Semi-structured diagnostic interview, was the gold standard for CM diagnosis in this study
Clinical experts included Drs. Pavlovic, Silberstein, Cowan, and Lipton
CM=chronic migraine; EM=episodic migraine; ID-CM=Identify Chronic Migraine; SSDI=Semi-Structured Diagnostic Interview.Note: The pre-screening period was defined as the 12-month time period from the screening date to 364 days prior. The pre-enrollment period was defined as the 12-month month time period from the enrollment date to 364 days prior.
Methods
Large medical group database
screened for adult migraine patients (≥ 18 years of age)
from October 2015 to November
2016
≥1 medical claim with a migraine
diagnosis (346.xx/G43.xxx) in the 12-month pre-screening period
required for study inclusion(n=536)
Patients with migraine who consented to enroll into the
study were administered the
ID-CM screener (to obtain real-world data on validity)
(n=536)
The SSDI was administered to a
convenience sample of
patients; all patients were
required to have continuous
enrollment in the 12-month pre-
enrollment period(final sample
n=192)
Acute treatment, preventive
treatment, opioid use, and baseline
characteristics were assessed for
CM and EM patients based on claims in the 12-
month pre-enrollment period
51 2 3 4
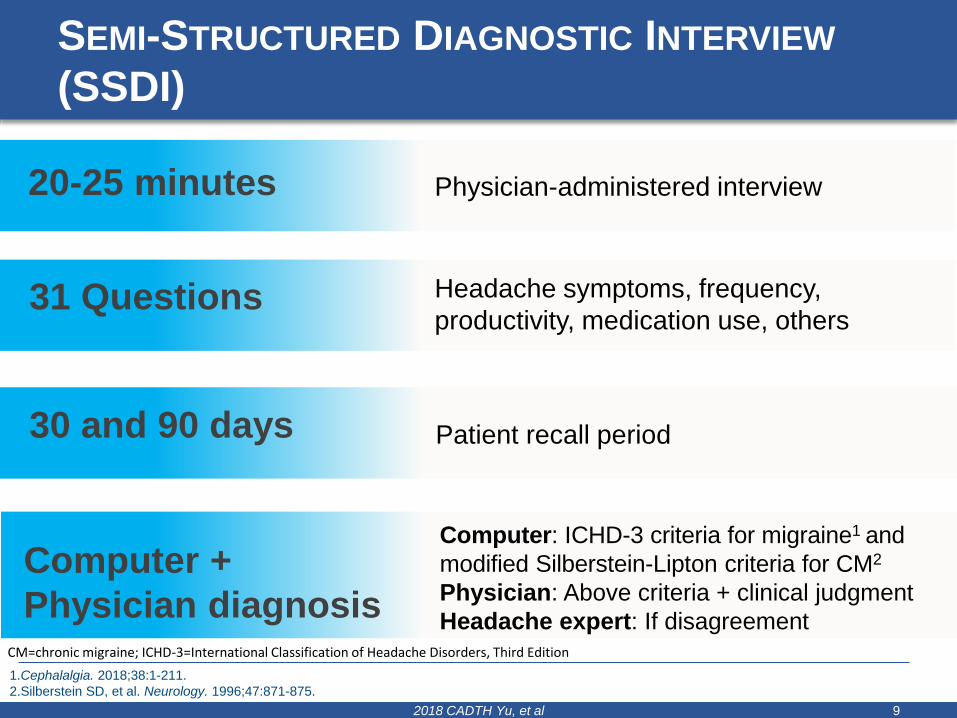
SEMI-STRUCTURED DIAGNOSTIC INTERVIEW
(SSDI)
2018 CADTH Yu, et al 9
20-25 minutes Physician-administered interview
31 Questions Headache symptoms, frequency,
productivity, medication use, others
30 and 90 days Patient recall period
Computer +
Physician diagnosis
Computer: ICHD-3 criteria for migraine1 and
modified Silberstein-Lipton criteria for CM2
Physician: Above criteria + clinical judgment
Headache expert: If disagreementCM=chronic migraine; ICHD-3=International Classification of Headache Disorders, Third Edition
1.Cephalalgia. 2018;38:1-211.
2.Silberstein SD, et al. Neurology. 1996;47:871-875.
ASSESSMENTS
• Assessments for CM and EM patients based on pharmacy and
medical claims data collected in the 12-month period from the
enrollment date to 364 days prior to enrollment (i.e., pre-enrollment
period) included
− Baseline characteristics
− Acute treatments for migraine
− Preventive treatments for migraine
− Opioids (pharmacy claims only)
• All variables were assessed using descriptive analyses
2018 CADTH Yu, et al 10
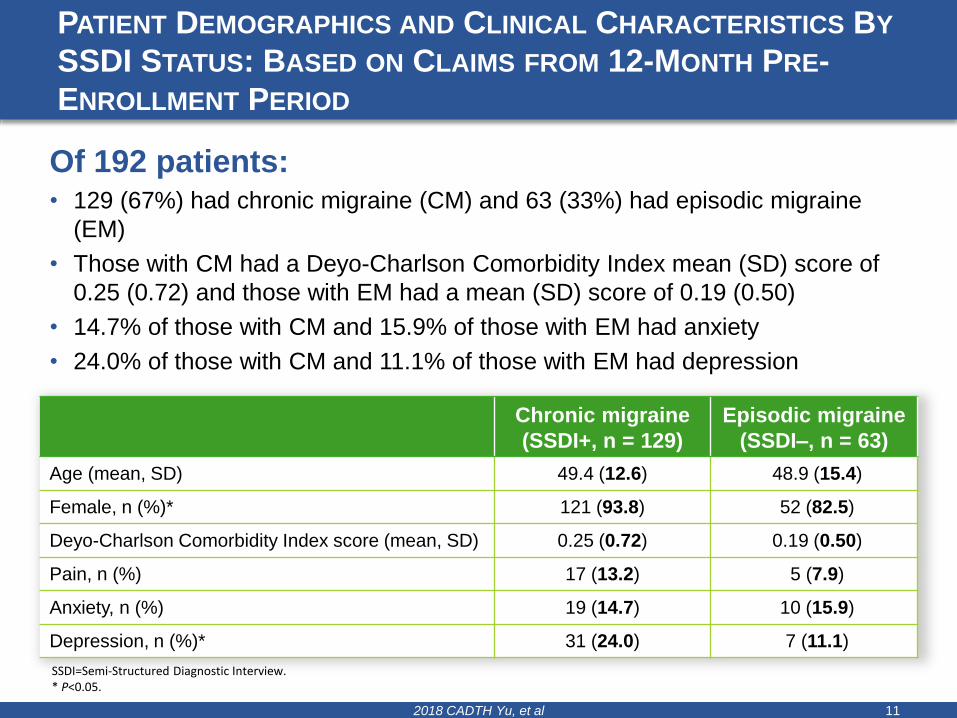
PATIENT DEMOGRAPHICS AND CLINICAL CHARACTERISTICS BY
SSDI STATUS: BASED ON CLAIMS FROM 12-MONTH PRE-
ENROLLMENT PERIOD
2018 CADTH Yu, et al 11
Chronic migraine
(SSDI+, n = 129)
Episodic migraine
(SSDI–, n = 63)
Age (mean, SD) 49.4 (12.6) 48.9 (15.4)
Female, n (%)* 121 (93.8) 52 (82.5)
Deyo-Charlson Comorbidity Index score (mean, SD) 0.25 (0.72) 0.19 (0.50)
Pain, n (%) 17 (13.2) 5 (7.9)
Anxiety, n (%) 19 (14.7) 10 (15.9)
Depression, n (%)* 31 (24.0) 7 (11.1)
SSDI=Semi-Structured Diagnostic Interview.* P<0.05.
Of 192 patients: • 129 (67%) had chronic migraine (CM) and 63 (33%) had episodic migraine
(EM)
• Those with CM had a Deyo-Charlson Comorbidity Index mean (SD) score of
0.25 (0.72) and those with EM had a mean (SD) score of 0.19 (0.50)
• 14.7% of those with CM and 15.9% of those with EM had anxiety
• 24.0% of those with CM and 11.1% of those with EM had depression
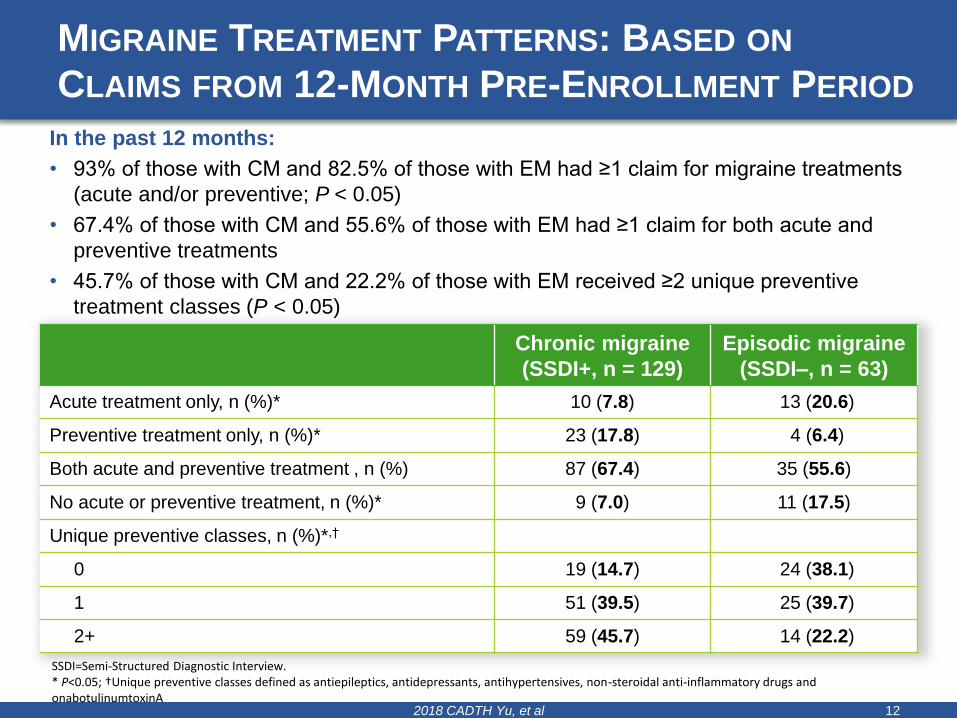
MIGRAINE TREATMENT PATTERNS: BASED ON
CLAIMS FROM 12-MONTH PRE-ENROLLMENT PERIOD
2018 CADTH Yu, et al 12
Chronic migraine
(SSDI+, n = 129)
Episodic migraine
(SSDI–, n = 63)
Acute treatment only, n (%)* 10 (7.8) 13 (20.6)
Preventive treatment only, n (%)* 23 (17.8) 4 (6.4)
Both acute and preventive treatment , n (%) 87 (67.4) 35 (55.6)
No acute or preventive treatment, n (%)* 9 (7.0) 11 (17.5)
Unique preventive classes, n (%)*,†
0 19 (14.7) 24 (38.1)
1 51 (39.5) 25 (39.7)
2+ 59 (45.7) 14 (22.2)
SSDI=Semi-Structured Diagnostic Interview.* P<0.05; †Unique preventive classes defined as antiepileptics, antidepressants, antihypertensives, non-steroidal anti-inflammatory drugs and onabotulinumtoxinA
In the past 12 months:
• 93% of those with CM and 82.5% of those with EM had ≥1 claim for migraine treatments
(acute and/or preventive; P < 0.05)
• 67.4% of those with CM and 55.6% of those with EM had ≥1 claim for both acute and
preventive treatments
• 45.7% of those with CM and 22.2% of those with EM received ≥2 unique preventive
treatment classes (P < 0.05)
OPIOID TREATMENT PATTERNS: BASED ON CLAIMS
FROM 12-MONTH PRE-ENROLLMENT PERIOD
2018 CADTH Yu, et al 13
Chronic migraine
(SSDI+, n = 129)
Episodic migraine
(SSDI–, n = 63)
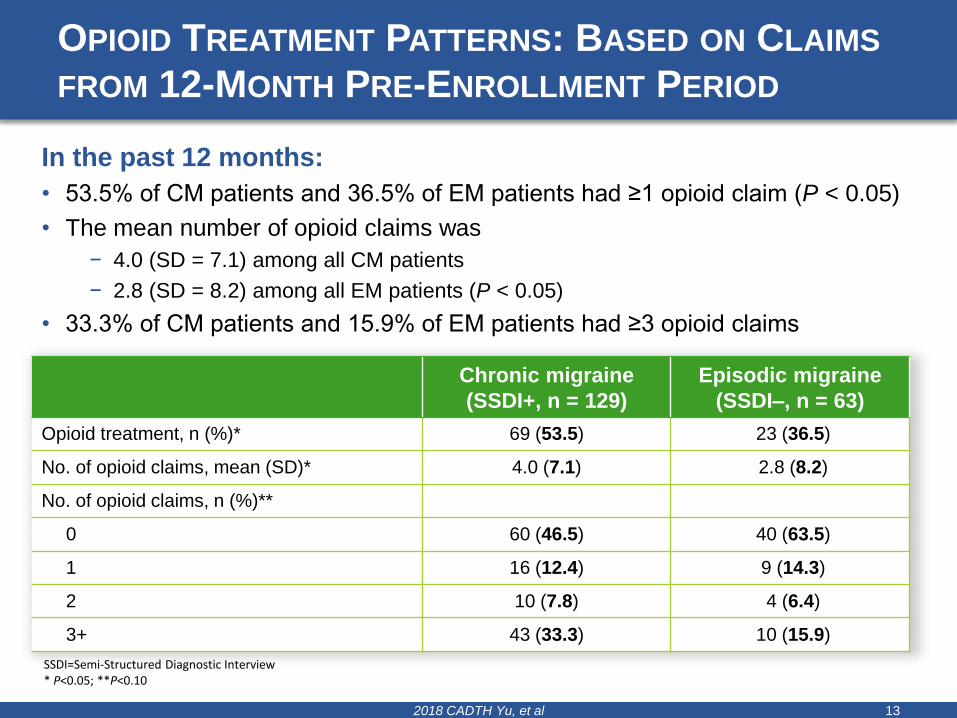
Opioid treatment, n (%)* 69 (53.5) 23 (36.5)
No. of opioid claims, mean (SD)* 4.0 (7.1) 2.8 (8.2)
No. of opioid claims, n (%)**
0 60 (46.5) 40 (63.5)
1 16 (12.4) 9 (14.3)
2 10 (7.8) 4 (6.4)
3+ 43 (33.3) 10 (15.9)
SSDI=Semi-Structured Diagnostic Interview* P<0.05; **P<0.10
In the past 12 months:
• 53.5% of CM patients and 36.5% of EM patients had ≥1 opioid claim (P < 0.05)
• The mean number of opioid claims was
− 4.0 (SD = 7.1) among all CM patients
− 2.8 (SD = 8.2) among all EM patients (P < 0.05)
• 33.3% of CM patients and 15.9% of EM patients had ≥3 opioid claims
LIMITATIONS
• The lists of acute and preventive medications for migraine were
based on Level A and B evidence1-3 from United States clinical
practice guidelines and clinical expert opinion
− Other medications, including over-the-counter mediations used for the
treatment of migraine, were not included
• Only pharmacy claims were evaluated to assess opioid use
• The analysis was limited to patients with a diagnosis of migraine in
the 12-month pre-screening period who were likely seeking medical
care
2018 CADTH Yu, et al 14
1. Marmura MJ et al. Headache 2015;55:3-20.
2. Silberstein et al., Neurology 2012;78:1337-1345.
3. Holland S et al., Neurology 2012;78:1346-1353.
CONCLUSIONS
• Approximately two-thirds of patients with chronic migraine (CM) had
prescriptions for both acute treatments for migraine and medications
that can be used for prevention of migraine in the past year
• More than half of patients with CM and about a third of patients with
episodic migraine (EM) also received an opioid prescription in the
same time period
• Given the prevalence of opioid use in migraine patients, especially
those with CM, results suggest that improved management of
treatment is needed to optimize care
2018 CADTH Yu, et al 15
2018 CADTH Yu, et al 16
QUESTIONS?

The Prescription Side of the Opioid Crisis:-
Supporting NB Prescribers and Clinicians in Appropriate Use, Monitoring and Patient
Management
Dr. Heidi Liston, NB Department of HealthStephanie Smith, CADTH
Dr. Pam Jarrett, Horizon Health Network and NB Department of Health
APRIL 17, 2018 2018 CADTH Symposium, Halifax
PMPs have tended to be “reactive” focusing on
identifying the worst cases at the point of dispensing
Paradigm shift
• Focus on prevention and the
prescriber
• Focus on new patients
• Evidenced-based and guideline
supported prescribing of new
patients
• Appropriate management of
patients on long-term opioids to
avoid individuals being “cut-off”
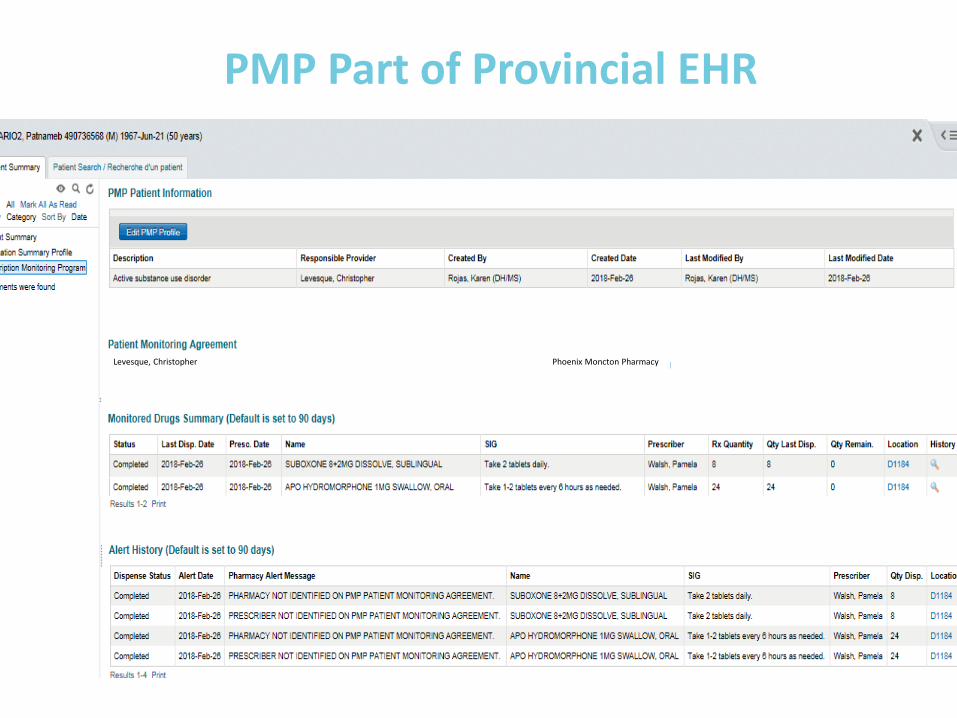
PMP Part of Provincial EHR
Levesque, Christopher Phoenix Moncton Pharmacy
“While someday computerization of medicine will surely be that long-awaited ‘disruptive innovation,’ today it’s often just plain disruptive: of the doctor-patient relationship, of clinicians professional interactions and work flow, and of the way we measure and try to improve things,” Robert Wachter
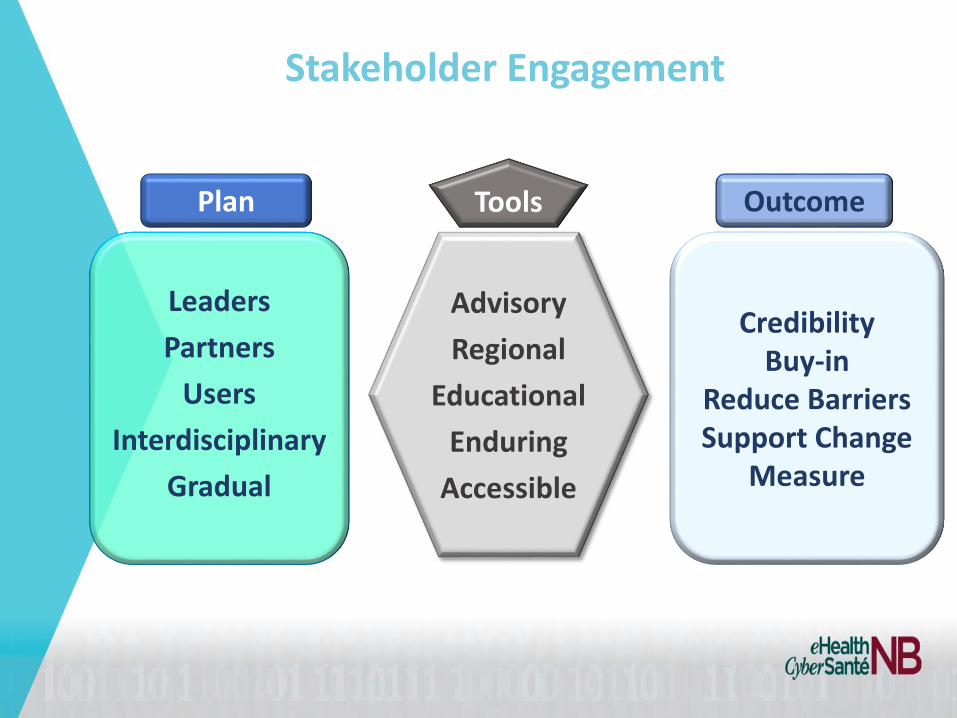
CredibilityBuy-in
Reduce BarriersSupport Change
Measure
Advisory
Regional
Educational
Enduring
Accessible
Leaders
Partners
Users
Interdisciplinary
Gradual
Plan OutcomeTools
Stakeholder Engagement
A national campaign to help reduce opioids over-
prescribing
Choosing Wisely New Brunswick

Information Available on the Electronic Health Record (EHR):
Patient demographicinformation
Medication summary profile and Prescription Monitoring Program
Laboratorytest results
Diagnosticimaging reports
Specific cardiologyreports
Hospitalvisit history
Patient demographicinformation
Medication summary profile and Prescription Monitoring Program
Laboratorytest results
Engagement To Date
• Since 2016– Hosted 15 face to face and virtual meetings with
stakeholders groups across disciplines
– Partnered on 6 panels at professional body AGMs
– Presented directly to Association Boards, Regulatory Councils, Practice Groups
– Additional outreach: Grand Rounds, Harm Reduction events, Pain sessions
Knowledge Mobilization &
Implementation Support
24
Knowledge Mobilization &
Implementation Support
25
• Presentations, Education
• Exhibits / Booths
• Conference abstracts
• News Articles (e.g., InfoNursing)
•
• Moving Forward?
How did this help?
• eHealthNB• Real time access to ALL prescription information
(Opioids and Non-Opioids)
• Intervention is educational and patient focused
• Everyone has a role to play in Opioid crisis
• Educational Sessions • Very good attendance
• Educational opportunity
• Forum for discussion when otherwise difficult to create this forum
What Else Did We Learn?
• Doctors appreciate the information being provided
• Physicians want to be part of the solution
• Lack of community resources to assist the primary care provider to help patient with opioid addiction
• More opportunities to work together to learn better ways to help patients with pain management and thus opioid prescriptions
• Managing patient expectations of pain control is also important
• We are on the RIGHT TRACK!
Where To From Here?
• Broader range of education required to ALL health care professionals (prescribers and non-prescribers)
• Who should lead this educational drive?
• Emphasis on alternatives such as Non-Opioid treatment of pain
• Role of eConsult
Clinical Indications for Initiating
Opioidsfor Pain Management in Ontario, Canada
A population-based retrospective cohort study
Sachin Pasricha, Queen’s University School of MedicineDr. Mina Tadrous, U of T Lesile Dan School of PharmacyWayne Khuu, Institute for Clinical Evaluative SciencesDr. David Juurlink, Sunnybrook Health Sciences CentreDr. Muhammad Mamdani, Li Ka Shing Centre for Healthcare Analytics and TrainingDr. Michael Paterson, Institute for Clinical Evaluative SciencesDr. Tara Gomes, St. Michael’s Hospital
Ontario Drug Policy Research Network
Disclosures
• Studentship Funding from Ontario Drug
Policy Research Network, Ontario Ministry
of Health and Long-term Care
Opioid-related deathsRoad trauma
Addiction Healthcare
costs
Side Effects
Psychosocial
effects
Inequity
Opioids
Opioid-related deathsRoad trauma
Addiction Healthcare
costs
Side Effects
Psychosocial
effects
Inequity
Opioids
Pain Management
Opioid-related deathsRoad trauma
Addiction Healthcare
costs
Side Effects
Psychosocial
effects
Inequity
Opioids
Back Pain
Surgery
Opioids
Clinical Indications for
which People Initiate
Opioids for Pain
Management
Opioids
Clinical Indications for
which People Initiate
Opioids for Pain
Management
Primary
Care
Private
Insurance
Musculoskeletal
Pain
TOTAL POPULATION?
(Narcotics Monitoring System)
Opioids
Clinical Indications for
which People Initiate
Opioids for Pain
Management
TOTAL POPULATION?
(Narcotics Monitoring System)
Methods Results Discussion
Clinical Indications for
which People Initiate
Opioids for Pain
Management
Purpose
Appropriateness – Dose, duration,
type, indication
Alternatives
Guidelines by Clinical Indication
Resource Allocation
Purpose Methods Results Discussion
Narcotics Monitoring System (NMS)
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
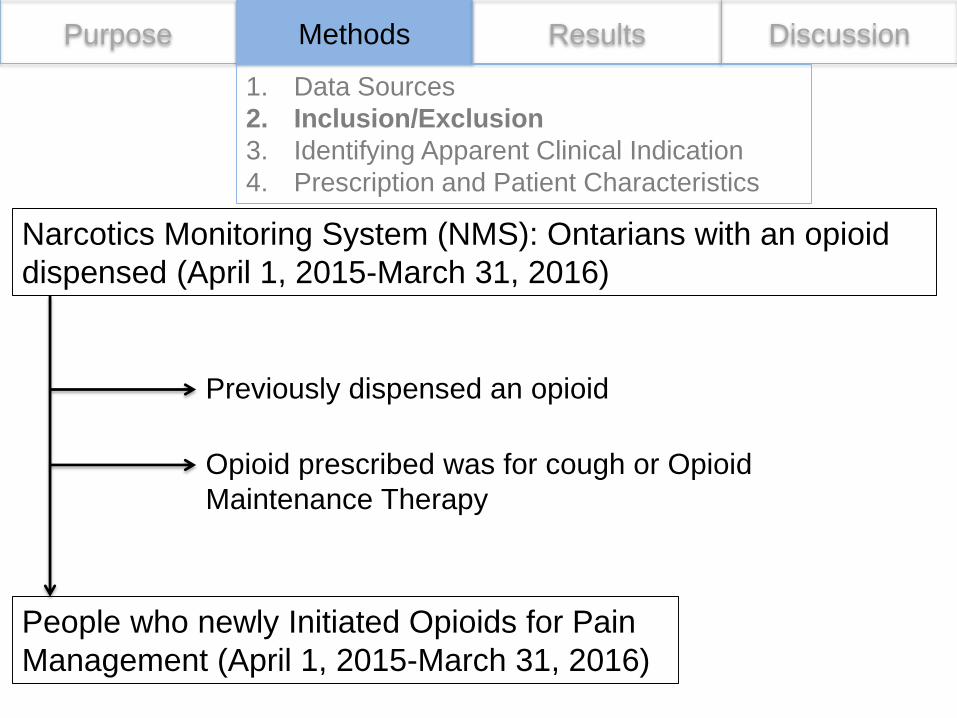
Purpose Methods Results Discussion
Narcotics Monitoring System (NMS): Ontarians with an opioid
dispensed (April 1, 2015-March 31, 2016)
Previously dispensed an opioid
Opioid prescribed was for cough or Opioid
Maintenance Therapy
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
People who newly Initiated Opioids for Pain
Management (April 1, 2015-March 31, 2016)
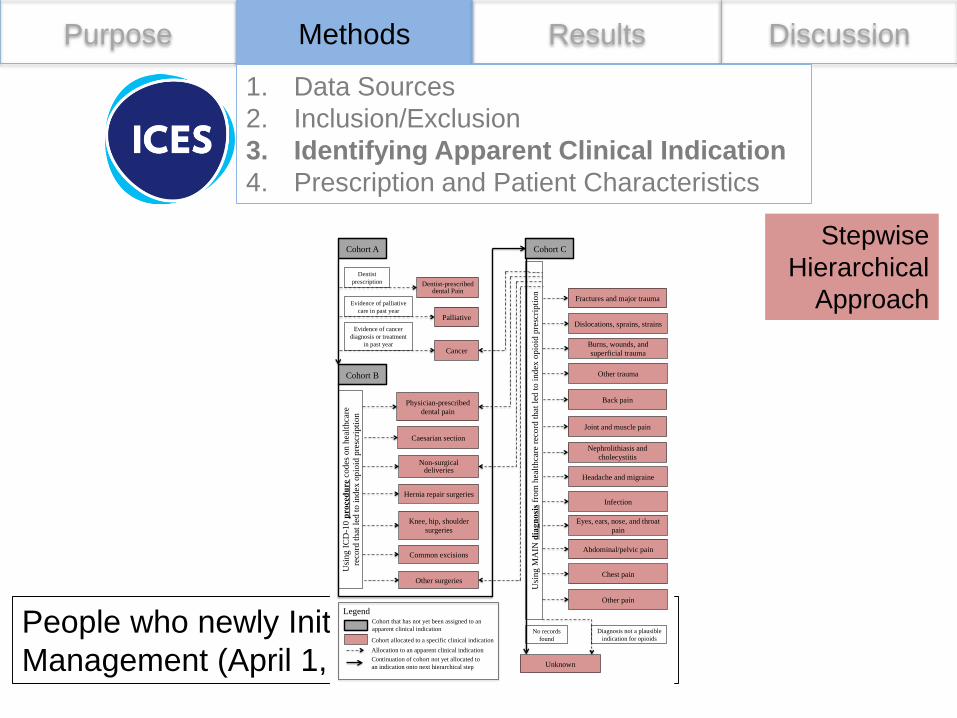
Purpose Methods Results Discussion
Stepwise
Hierarchical
Approach
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
People who newly Initiated Opioids for Pain
Management (April 1, 2015-March 31, 2016)
Cohort A
Palliative
Cancer
Usi
ng
MA
IN diagnosis
fro
m h
ealt
hca
re r
eco
rd t
hat
led
to
in
dex
opio
id p
resc
ripti
on
Physician-prescribed
dental pain
Non-surgical deliveries
Hernia repair surgeries
Dentist
prescription
Evidence of palliative
care in past year
Cohort B
Caesarian section
Usi
ng
IC
D-1
0 procedure
co
des
on
hea
lth
care
reco
rd t
hat
led
to
in
dex
op
ioid
pre
scri
pti
on
Knee, hip, shoulder
surgeries
Common excisions
Other surgeries
Dentist-prescribed dental Pain
Evidence of cancer
diagnosis or treatment
in past year
Cohort C
Unknown
No records
found
Diagnosis not a plausible
indication for opioids
Fractures and major trauma
Dislocations, sprains, strains
Burns, wounds, and
superficial trauma
Other trauma
Back pain
Joint and muscle pain
Nephrolithiasis and
cholecystitis
Headache and migraine
Infection
Eyes, ears, nose, and throat
pain
Abdominal/pelvic pain
Chest pain
Other pain
Legend
Allocation to an apparent clinical indication
Continuation of cohort not yet allocated to
an indication onto next hierarchical step
Cohort that has not yet been assigned to an
apparent clinical indication
Cohort allocated to a specific clinical indication
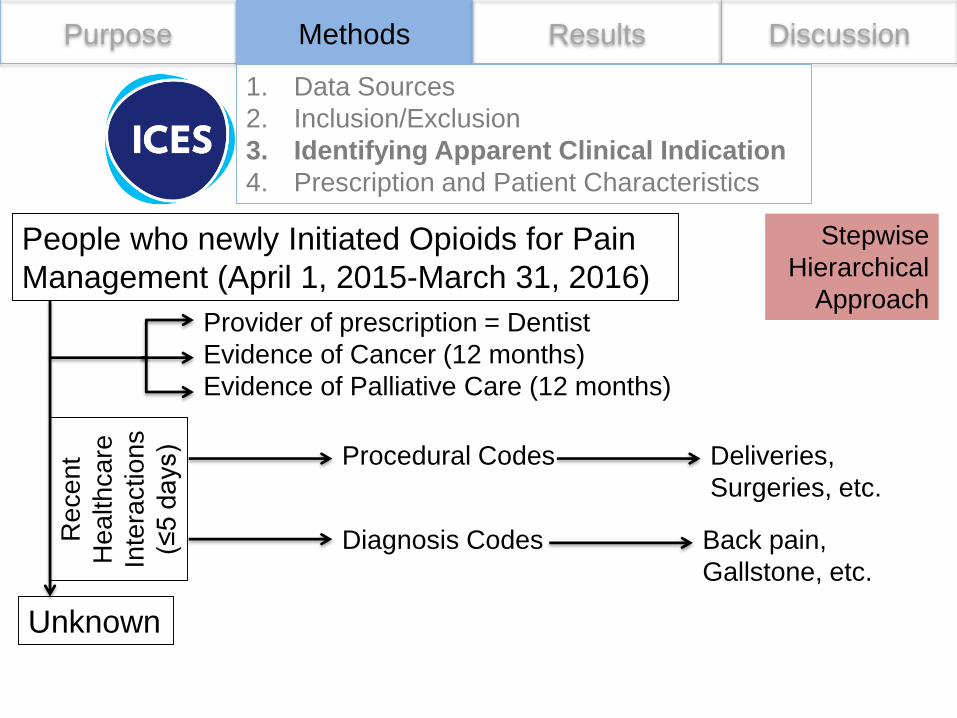
Purpose Methods Results Discussion
People who newly Initiated Opioids for Pain
Management (April 1, 2015-March 31, 2016)
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
Stepwise
Hierarchical
ApproachProvider of prescription = Dentist
Evidence of Cancer (12 months)
Evidence of Palliative Care (12 months)
Re
ce
nt
He
alth
ca
re
Inte
ractions
(≤5
da
ys) Procedural Codes
Unknown
Diagnosis Codes
Deliveries,
Surgeries, etc.
Back pain,
Gallstone, etc.
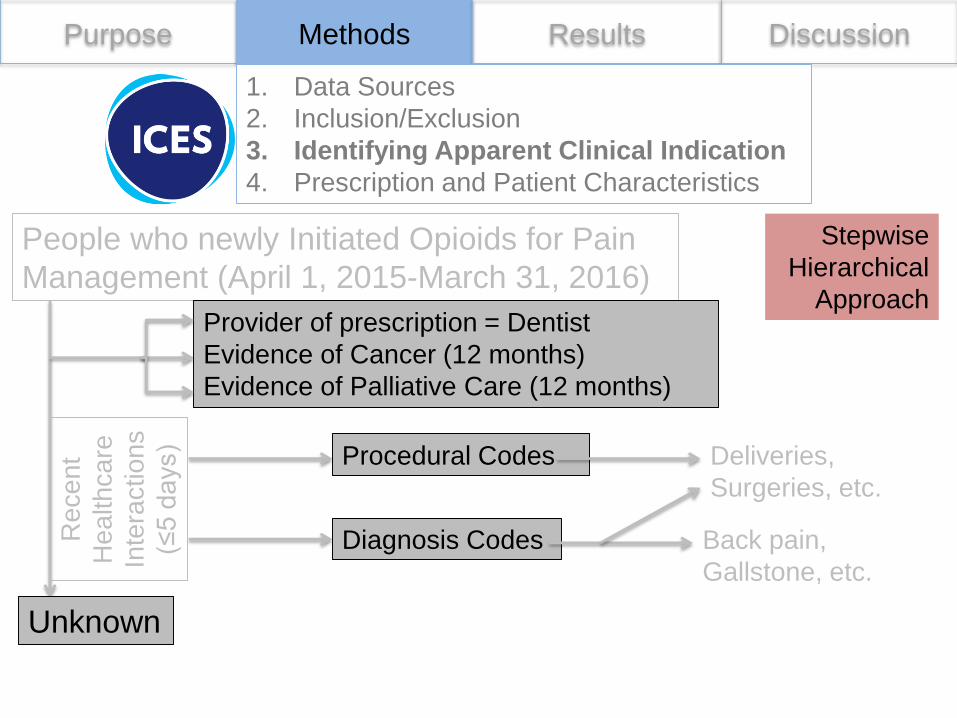
Purpose Methods Results Discussion
People who newly Initiated Opioids for Pain
Management (April 1, 2015-March 31, 2016)
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
Stepwise
Hierarchical
ApproachProvider of prescription = Dentist
Evidence of Cancer (12 months)
Evidence of Palliative Care (12 months)
Re
ce
nt
He
alth
ca
re
Inte
ractions
(≤5
da
ys) Procedural Codes
Unknown
Diagnosis Codes
Deliveries,
Surgeries, etc.
Back pain,
Gallstone, etc.
Purpose Discussion
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
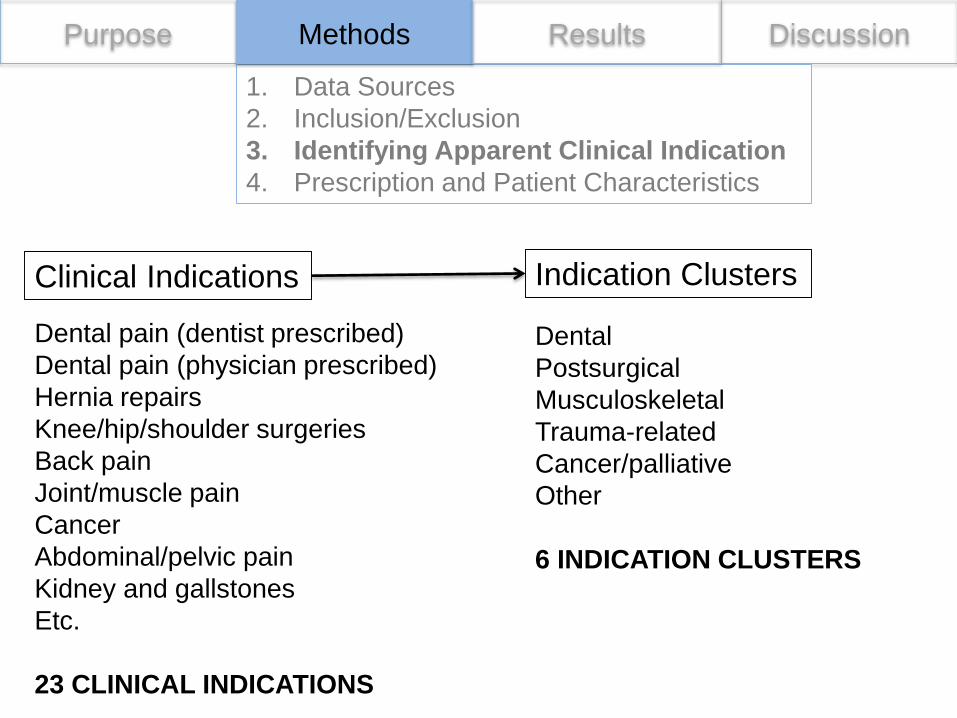
Clinical Indications Indication Clusters
Methods Results
Dental pain (dentist prescribed)
Dental pain (physician prescribed)
Hernia repairs
Knee/hip/shoulder surgeries
Back pain
Joint/muscle pain
Cancer
Abdominal/pelvic pain
Kidney and gallstones
Etc.
23 CLINICAL INDICATIONS
Dental
Postsurgical
Musculoskeletal
Trauma-related
Cancer/palliative
Other
6 INDICATION CLUSTERS

Purpose Discussion
1. Data Sources
2. Inclusion/Exclusion
3. Identifying Apparent Clinical Indication
4. Prescription and Patient Characteristics
Indication Clusters
Daily Dose
Duration
Opioid formulation
Patient Characteristics
Methods Results
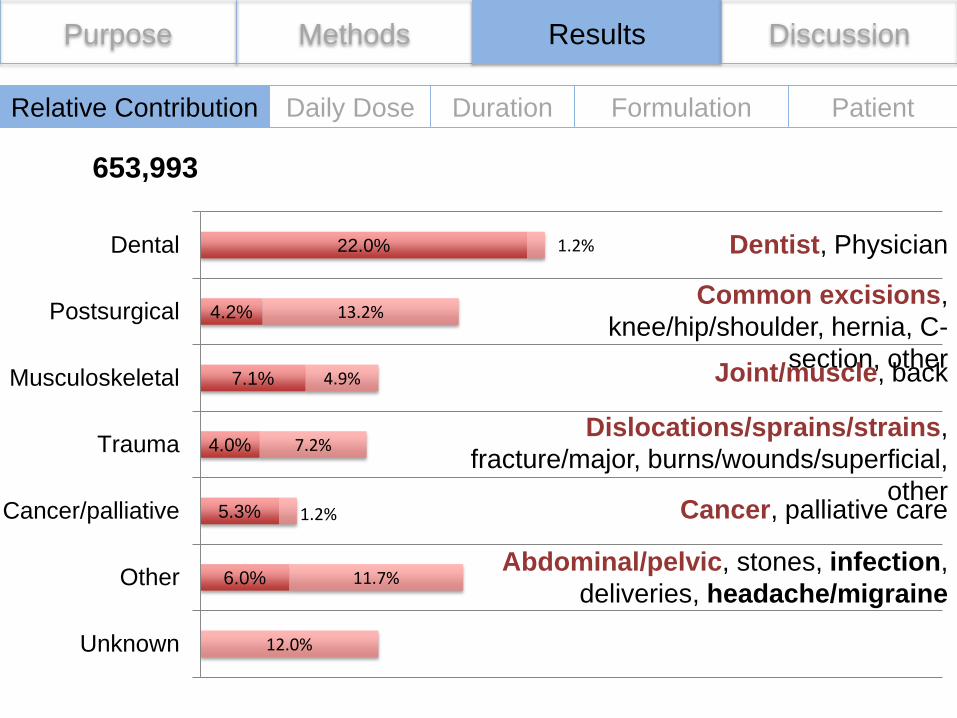
Relative contribution
Clinical Indications
Purpose Methods Results Discussion
6.0%
5.3%
4.0%
7.1%
4.2%
22.0%
12.0%
11.7%
1.2%
7.2%
4.9%
13.2%
1.2%
Unknown
Other
Cancer/palliative
Trauma
Musculoskeletal
Postsurgical
Dental
653,993
Dentist, Physician
Common excisions,
knee/hip/shoulder, hernia, C-
section, other Joint/muscle, back
Dislocations/sprains/strains,
fracture/major, burns/wounds/superficial,
otherCancer, palliative care
Abdominal/pelvic, stones, infection,
deliveries, headache/migraine
Relative Contribution Daily Dose Duration Formulation Patient
Purpose Methods Results Discussion
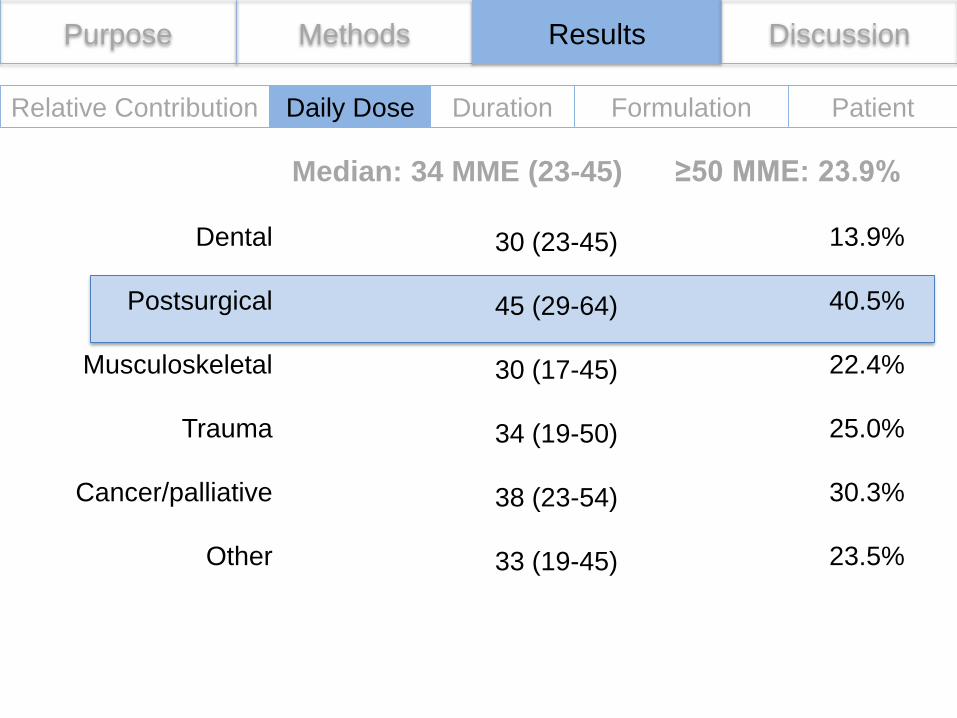
Median: 34 MME (23-45) ≥50 MME: 23.9%
Dental
Postsurgical
Musculoskeletal
Trauma
Cancer/palliative
Other
30 (23-45)
45 (29-64)
30 (17-45)
34 (19-50)
38 (23-54)
33 (19-45)
13.9%
40.5%
22.4%
25.0%
30.3%
23.5%
Relative Contribution Daily Dose Duration Formulation Patient
Purpose Methods Results Discussion
Relative Contribution Daily Dose Duration Formulation Patient
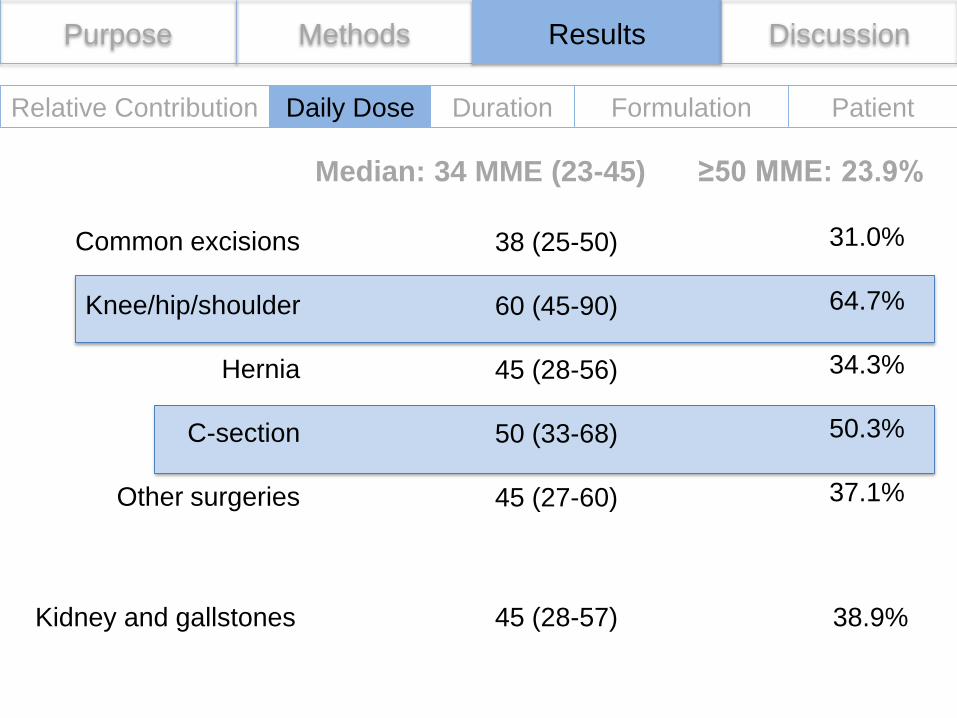
Median: 34 MME (23-45) ≥50 MME: 23.9%
38 (25-50)
60 (45-90)
45 (28-56)
50 (33-68)
45 (27-60)
31.0%
64.7%
34.3%
50.3%
37.1%
Common excisions
Knee/hip/shoulder
Hernia
C-section
Other surgeries
Kidney and gallstones 45 (28-57) 38.9%
Purpose Methods Results Discussion
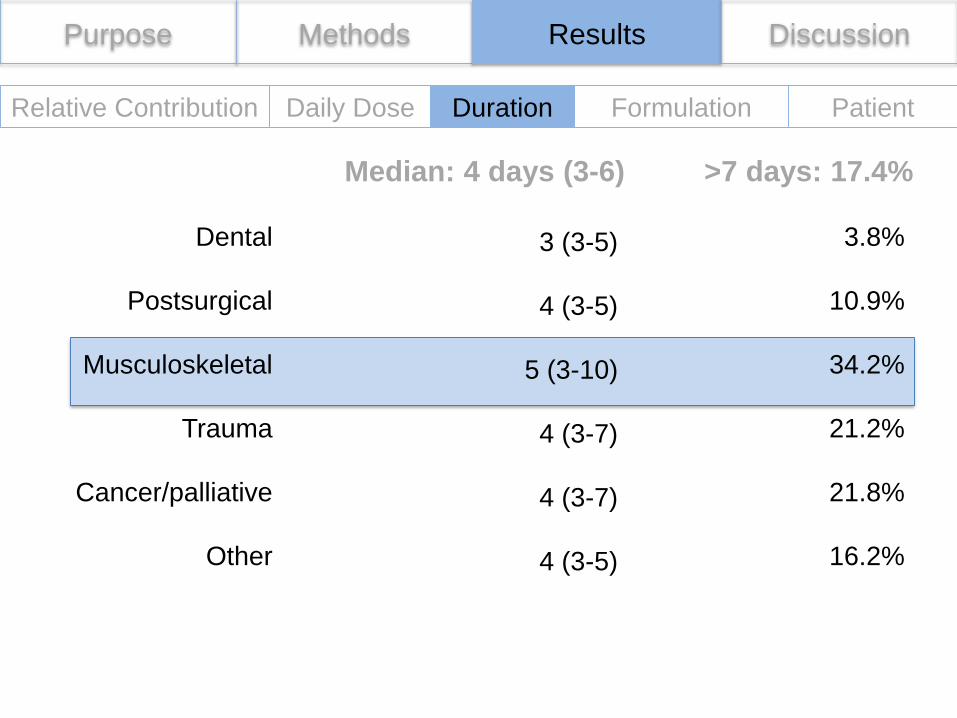
Relative Contribution Daily Dose Duration Formulation Patient
Median: 4 days (3-6) >7 days: 17.4%
Dental
Postsurgical
Musculoskeletal
Trauma
Cancer/palliative
Other
3 (3-5)
4 (3-5)
5 (3-10)
4 (3-7)
4 (3-7)
4 (3-5)
3.8%
10.9%
34.2%
21.2%
21.8%
16.2%
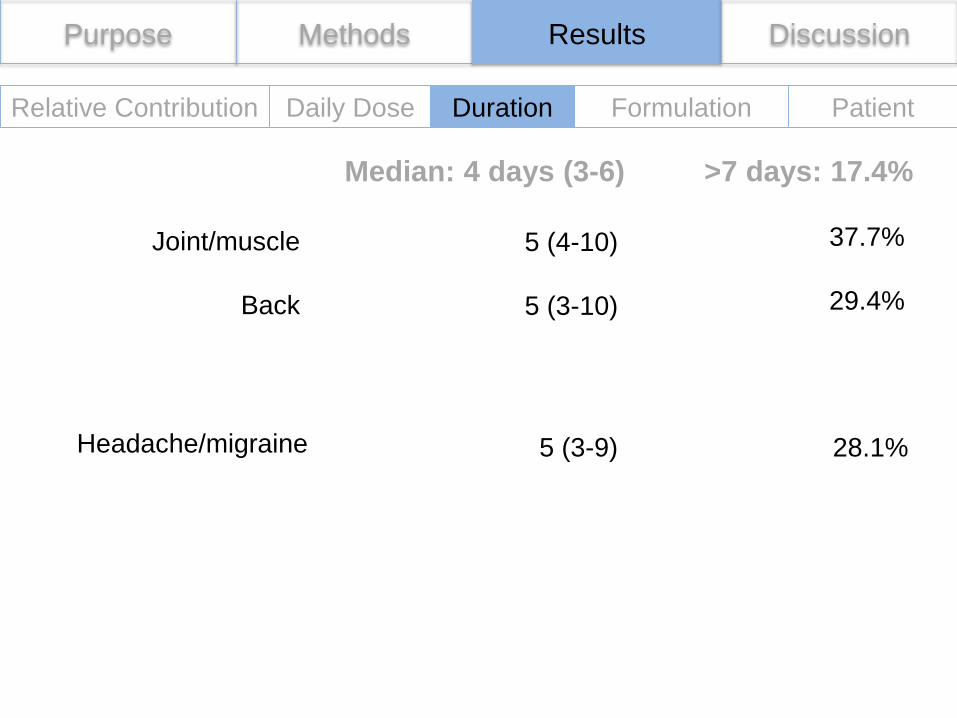
Purpose Methods Results Discussion
Relative Contribution Formulation Patient
5 (4-10)
5 (3-10)
37.7%
29.4%
Joint/muscle
Back
Headache/migraine 5 (3-9) 28.1%
Daily Dose Duration
Median: 4 days (3-6) >7 days: 17.4%
Purpose Methods Results Discussion
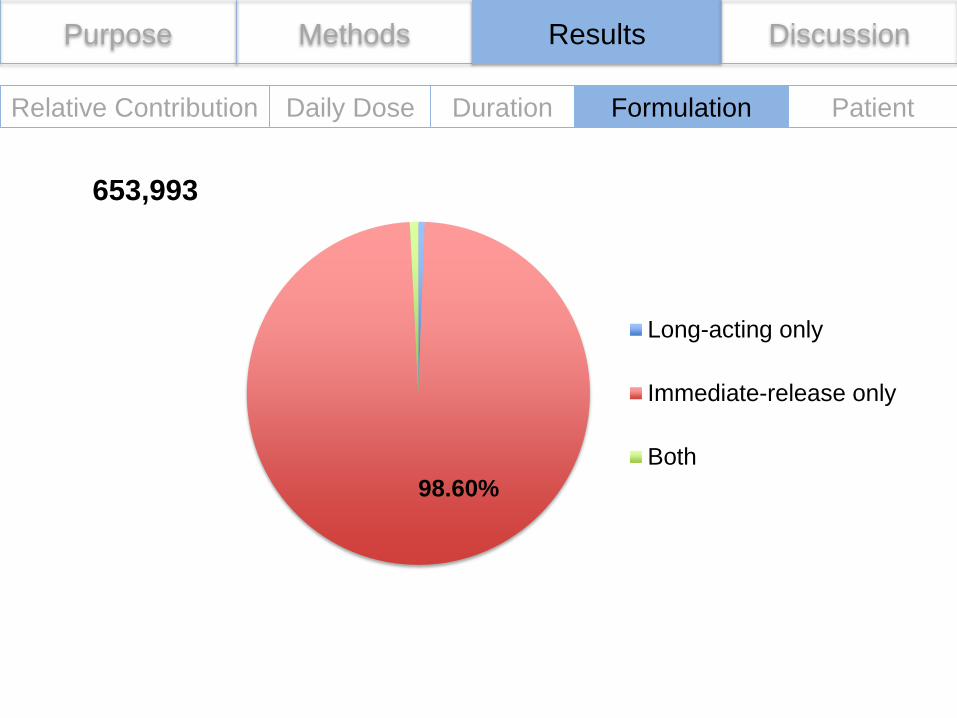
Relative Contribution Daily Dose Duration Formulation Patient
98.60%
Long-acting only
Immediate-release only
Both
653,993
Purpose Methods Results Discussion
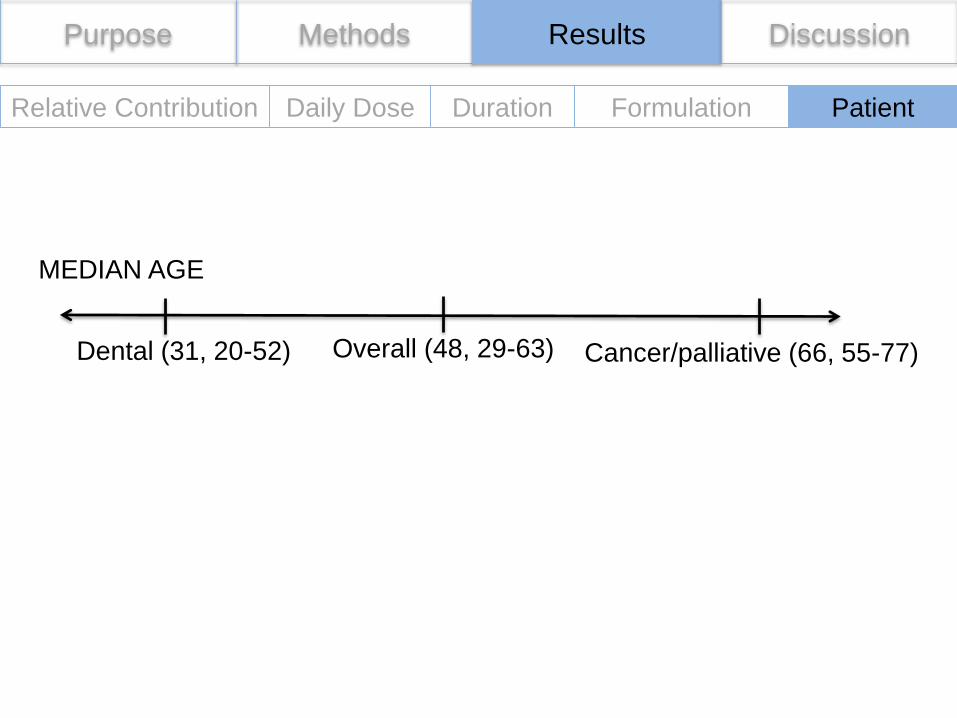
Relative Contribution Daily Dose Duration Formulation Patient
Overall (48, 29-63)Dental (31, 20-52) Cancer/palliative (66, 55-77)
MEDIAN AGE
Opioids
Clinical Indications for
which People Initiate
Opioids for Pain
Management
Purpose Methods Results Discussion
Purpose Methods Results Discussion
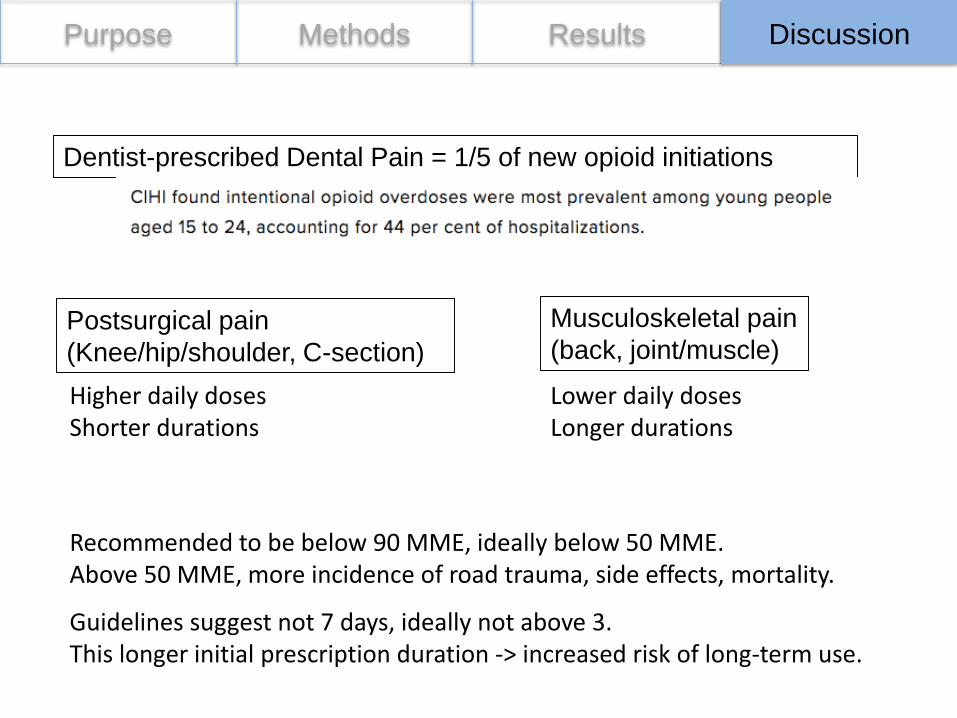
Dentist-prescribed Dental Pain = 1/5 of new opioid initiations
Postsurgical pain
(Knee/hip/shoulder, C-section)
Musculoskeletal pain
(back, joint/muscle)
Recommended to be below 90 MME, ideally below 50 MME.Above 50 MME, more incidence of road trauma, side effects, mortality.
Guidelines suggest not 7 days, ideally not above 3.This longer initial prescription duration -> increased risk of long-term use.
Higher daily dosesShorter durations
Lower daily dosesLonger durations
Purpose Methods Results Discussion
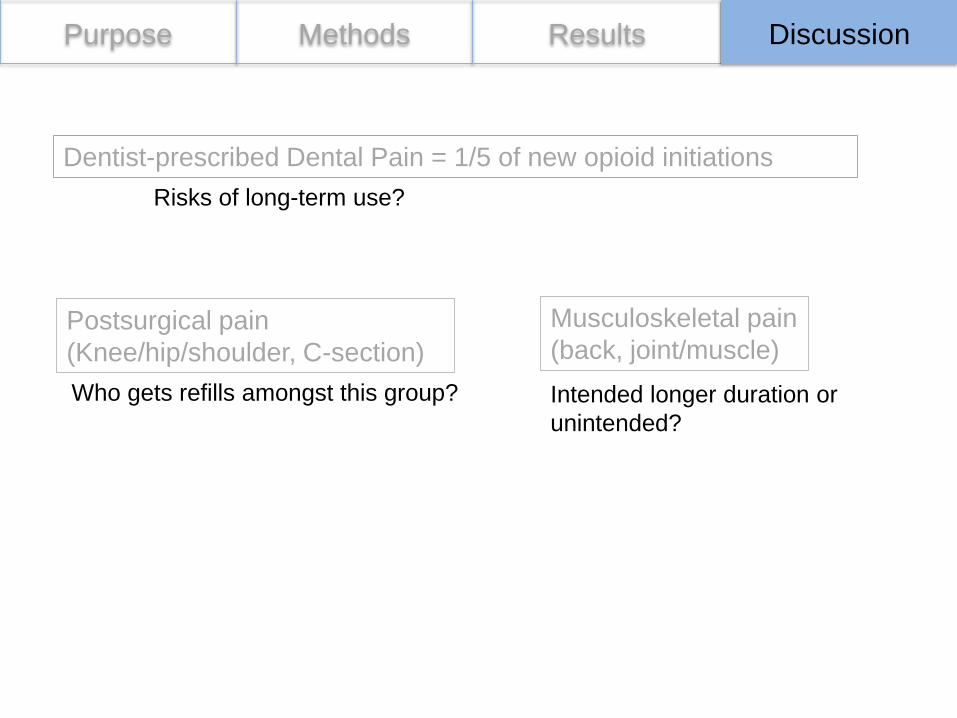
Risks of long-term use?
Who gets refills amongst this group? Intended longer duration or
unintended?
Dentist-prescribed Dental Pain = 1/5 of new opioid initiations
Postsurgical pain
(Knee/hip/shoulder, C-section)
Musculoskeletal pain
(back, joint/muscle)
Purpose Methods Results Discussion
Limitations
1. Certainty of stepwise hierarchical approach
2. Unknown (78,481, 12.0%)
3. Multiple pain indications
Appropriateness – Dose, duration, length, indication
Alternatives
Guidelines by Clinical Indication
Clinical Indications for
which People Initiate
Opioids for Pain
Management
Resource Allocation
Manuscript Coming Soon …
• Accepted to PAIN
References
• https://upload.wikimedia.org/wikipedia/en/c/c8/Trileptal_tablets.jpg
• https://www.canada.ca/en/public-health/services/publications/healthy-living/apparent-opioid-related-deaths-report-2016-2017-december.html
• https://www.publicdomainpictures.net/en/view-image.php?image=174447&picture=&jazyk=DE
• https://www.ncbi.nlm.nih.gov/pubmed/18443635
• https://c1.staticflickr.com/5/4566/24328746088_5f7c130180_b.jpg
• https://vimeo.com/167689608
• https://www.marketwatch.com/story/how-much-the-opioid-epidemic-costs-the-us-2017-10-27
• https://www.cnbc.com/2018/02/12/economic-cost-of-the-opioid-crisis-1-trillion-and-growing-faster.html
• https://www.vox.com/science-and-health/2017/11/20/16679688/white-house-opioid-epidemic-cost
• https://globalnews.ca/news/3743705/canadas-opioid-crisis-is-burdening-the-health-care-system-report-warns/
• https://www.cihi.ca/en/opioid-crisis-having-significant-impact-on-canadas-health-care-system
• https://commons.wikimedia.org/wiki/File:Medicon_cough.svg
• http://www.choosingwisely.org/patient-resources/treating-migraine-headaches/
BACK DECK
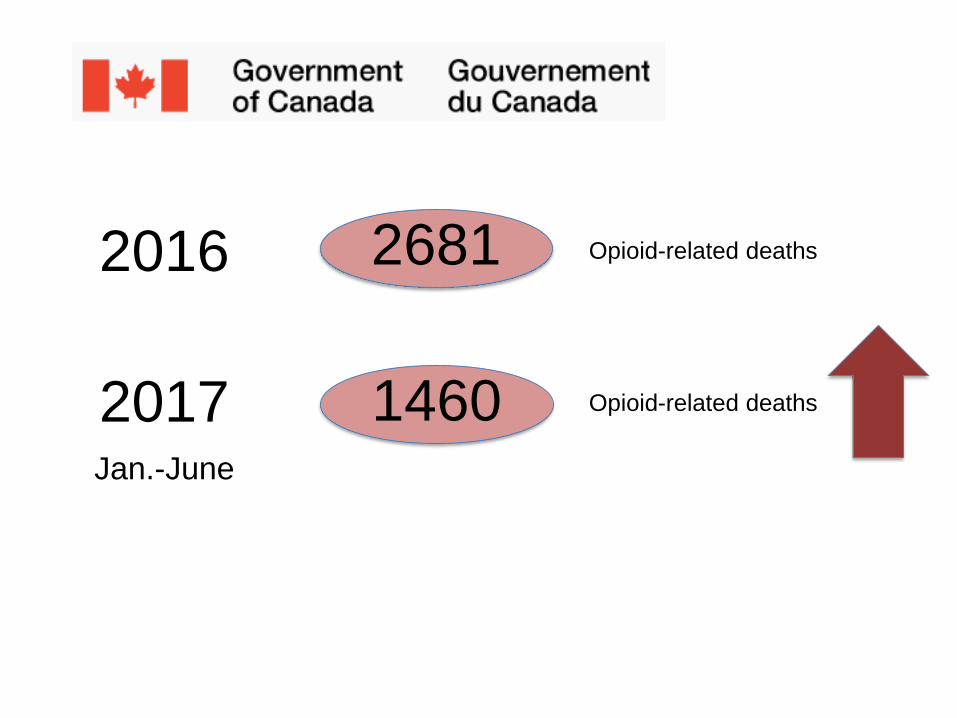
2016
2017Jan.-June
Opioid-related deaths
Opioid-related deaths
2681
1460
Purpose Discussion
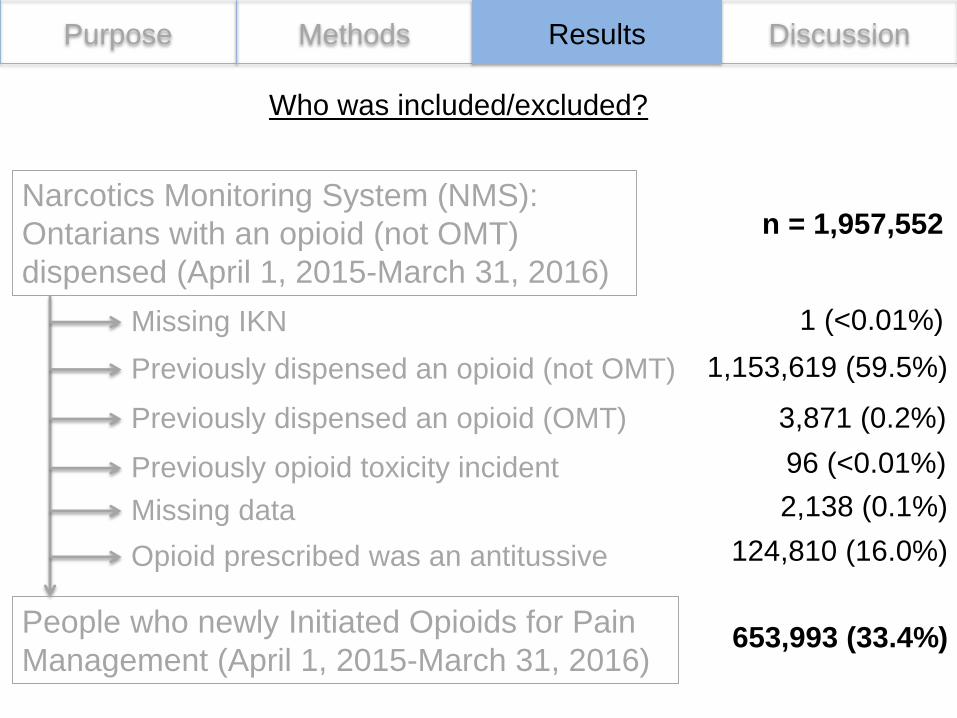
Narcotics Monitoring System (NMS):
Ontarians with an opioid (not OMT)
dispensed (April 1, 2015-March 31, 2016)
Missing IKN
Previously dispensed an opioid (not OMT)
Previously dispensed an opioid (OMT)
Previously opioid toxicity incident
Missing data
Opioid prescribed was an antitussive
People who newly Initiated Opioids for Pain
Management (April 1, 2015-March 31, 2016)
Methods Results
Who was included/excluded?
n = 1,957,552
1 (<0.01%)
1,153,619 (59.5%)
3,871 (0.2%)
96 (<0.01%)
2,138 (0.1%)
124,810 (16.0%)
653,993 (33.4%)
Purpose Methods Results Discussion
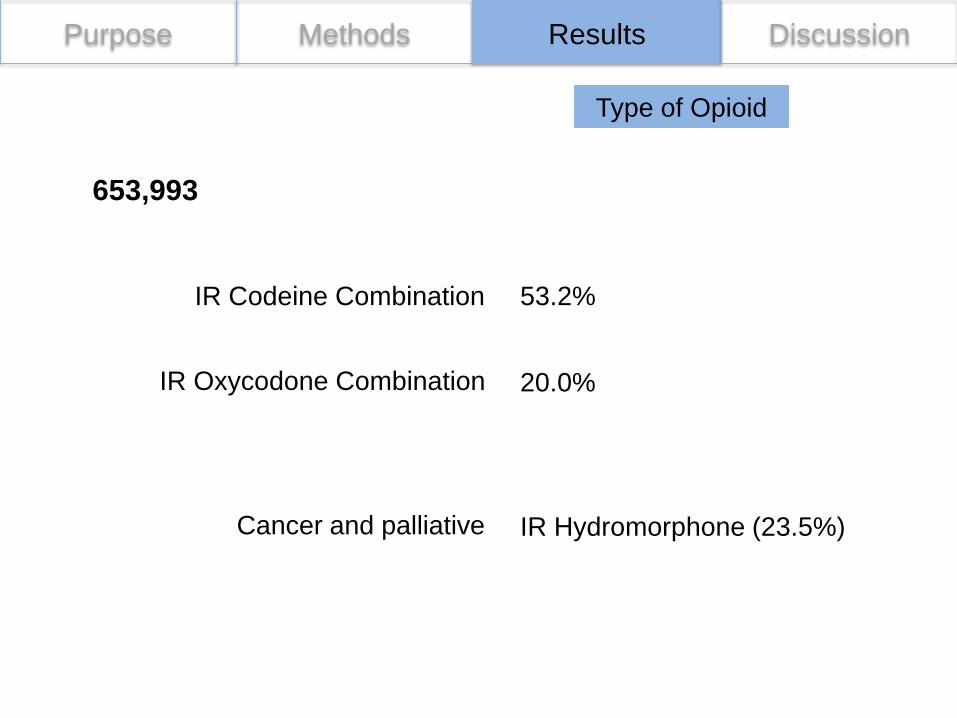
Type of Opioid
IR Codeine Combination
653,993
IR Oxycodone Combination 20.0%
Cancer and palliative IR Hydromorphone (23.5%)
53.2%
Purpose Methods Results Discussion
Other Limitations
1. July 2012 onwards
2. Inter-province travel (lag period for health system access)
For more information
Acknowledgements• For the SALOME and NAOMI trials
– The participants– Frontline workers at the Crosstown clinic– Research team– Partners, past and present:
• Providence Health Care, Providence Health Care Research Institute, St. Paul’s Hospital Foundation
• Vancouver Coastal Health• Canadian Institutes of Health Research• InnerChange foundation• Michael Smith Foundation for Health Research• University of British Columbia• Center for Health Evaluation and Outcomes Science• Canada Research Chairs Program• BC Ministry of Health
• For the economic analysis
– Dr. Bohdan Nosyk for his work developing the initial model and protocol for the study.• Email: [email protected]
School of Population and Public Health





























