Embed Size (px)
Citation preview

6/19/2014
1
To VBAC or Not To VBAC:
What Does the Evidence Say
Angela Wilson-Liverman, MSN, CNM, FACNM
Assistant Professor of OBGYN
Vanderbilt University School of Medicine
Objectives
• Attendees will describe data regarding safety
of TOLAC based on a patient's individual
history
• Attendees will describe evidence-based
counseling for patients regarding TOLAC.
• Attendees will utilize a VBAC calculator to
estimate the likelihood of successful VBAC
Conflicts of Interest
• I have no conflicts to disclose ☺☺☺☺
6/19/2014
2
“The Decision”
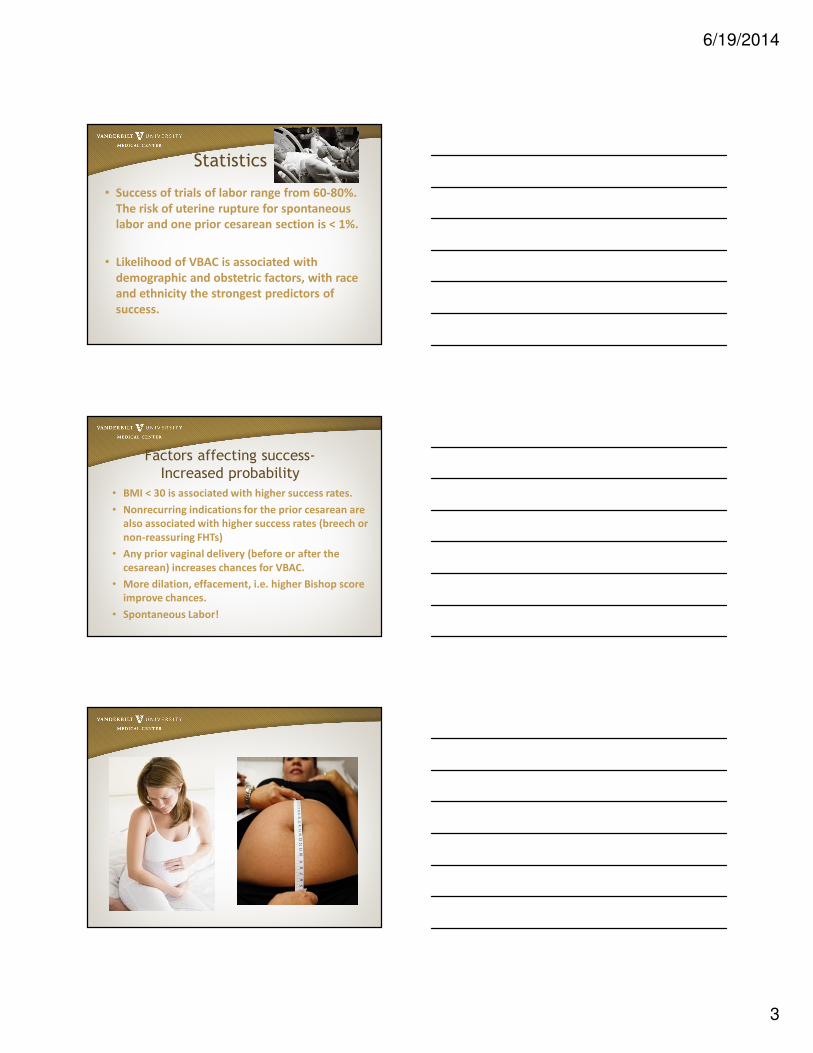
Statistics
Statistics• Cesarean delivery rates in America rose to 32
percent in 2007 from 21 percent in 1996.
• Since 1996 one-third of hospitals and one-
half of physicians no longer offer trial of labor
after cesarean (TOLAC).
• The repeat cesarean delivery rate for low-risk
women rose to 89 percent by 2003.
6/19/2014
3
Statistics
• Success of trials of labor range from 60-80%.
The risk of uterine rupture for spontaneous
labor and one prior cesarean section is < 1%.
• Likelihood of VBAC is associated with
demographic and obstetric factors, with race
and ethnicity the strongest predictors of
success.
Factors affecting success-
Increased probability
• BMI < 30 is associated with higher success rates.
• Nonrecurring indications for the prior cesarean are
also associated with higher success rates (breech or
non-reassuring FHTs)
• Any prior vaginal delivery (before or after the
cesarean) increases chances for VBAC.
• More dilation, effacement, i.e. higher Bishop score
improve chances.
• Spontaneous Labor!
6/19/2014
4
Factors affecting success
Decreased probability• Latina and African-American women have
lower rates of VBAC than non-hispanic white
women.
• Increasing maternal age, being single, and
having less than 12 years of education are also
associated with lower rates of VBAC.
• Induction or augmentation lower the rate of
VBAC.
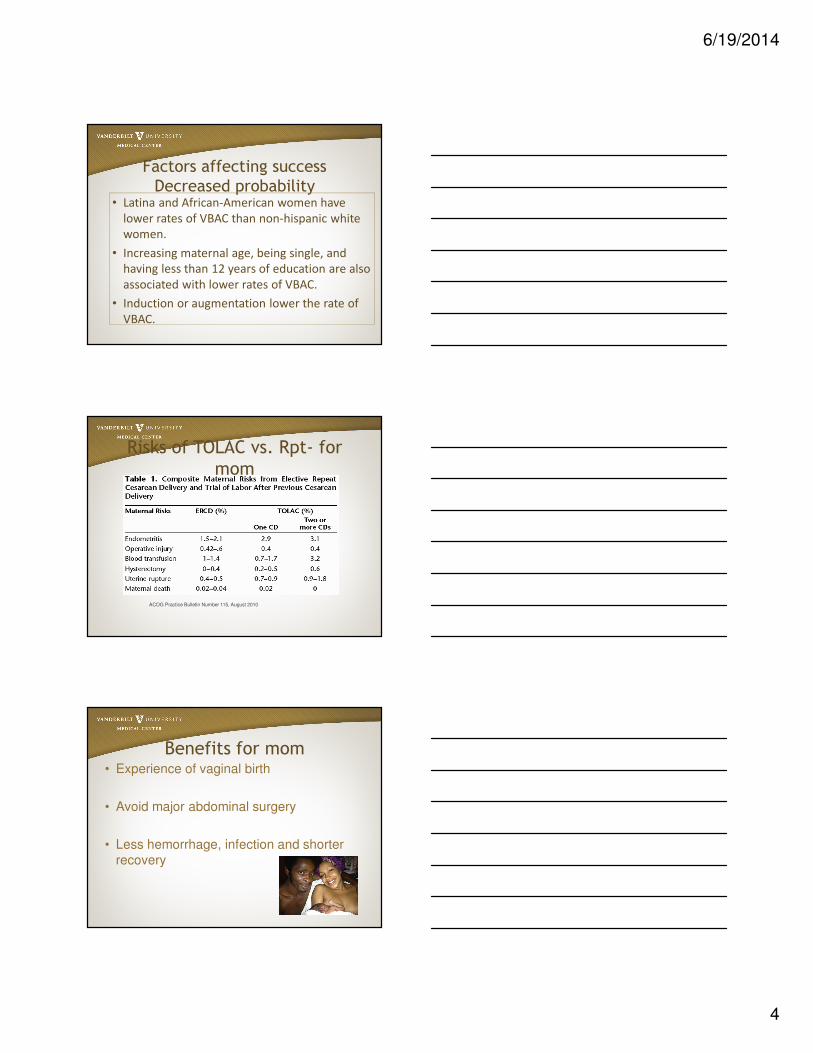
Risks of TOLAC vs. Rpt- for
mom
ACOG Practice Bulletin Number 115, August 2010
Benefits for mom• Experience of vaginal birth
• Avoid major abdominal surgery
• Less hemorrhage, infection and shorter recovery
6/19/2014
5
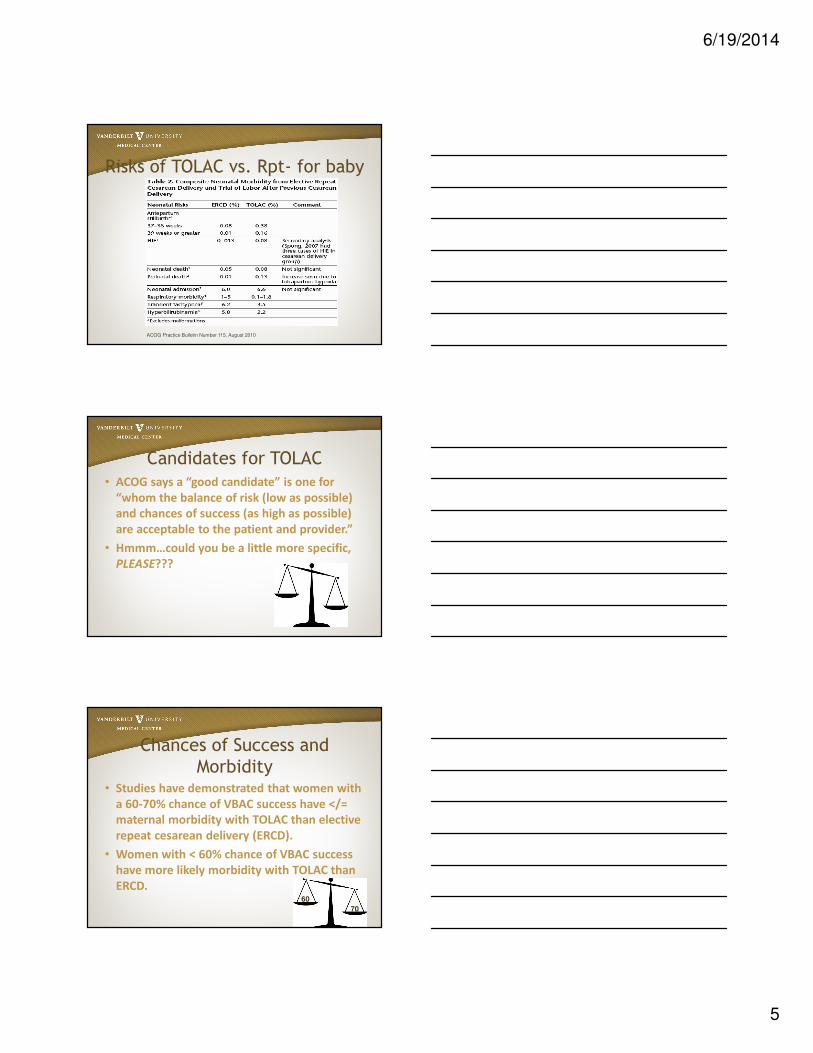
Risks of TOLAC vs. Rpt- for baby
ACOG Practice Bulletin Number 115, August 2010
Candidates for TOLAC
• ACOG says a “good candidate” is one for
“whom the balance of risk (low as possible)
and chances of success (as high as possible)
are acceptable to the patient and provider.”
• Hmmm…could you be a little more specific,
PLEASE???
Chances of Success and
Morbidity• Studies have demonstrated that women with
a 60-70% chance of VBAC success have </=
maternal morbidity with TOLAC than elective
repeat cesarean delivery (ERCD).
• Women with < 60% chance of VBAC success
have more likely morbidity with TOLAC than
ERCD.60
70
6/19/2014
6
One Prior Cesarean
• Most women with one prior cesarean with a
low transverse incision are candidates for and
should be counseled about VBAC and offered
TOLAC
• The risk of uterine rupture with one prior
cesarean section and spontaneous labor is
0.5-0.7% (1/150-1/200).
2 or more prior Cesareans• Studies differ with regards to risk of
uterine rupture with greater than one prior uterine incision.
• Rupture risks vary from 0.9-1.8%.
• Maternal morbidity increased
• Similar likelihood of success
• Reasonable to consider as candidates
for TOLAC although data is limited!
Estimated Fetal Weight
• If the EFW is greater than 4000g, likelihood of
VBAC success is lower, especially in women
who had a prior cesarean for dystocia with a
smaller baby.
6/19/2014
7
Incision Type
• Prior classical uterine incision not
recommended for TOLAC (~5% rupture risk)
• Prior low vertical- similar risk to low
transverse incision
• Unknown- No significant increase in TOLAC
risk. Scar type can often be inferred from
indication. With high suspicion (very preterm
delivery, e.g.) recommend repeat cesarean.
Twin Gestation• VBAC outcomes and success similar to
singleton gestations.
• May be considered for TOLAC per ACOG.
Labor Management TOLAC
• Is Induction or Augmentation OK?
– One study of > 20,000 women found an
increased rupture rate of 0.77% for induced (no
prostaglandins) vs. 0.52% for spontaneous
labors. Prostaglandins increased the rate to
2.24%. (Lydon-Rochelle M., et al 2001)
– Another of > 33,000 women found rates of 0.4%
for spontaneous, 0.9% for augmented and 1.1%
for oxytocin-induced. (Grobman WA., et al 2007)

6/19/2014
8
Pitocin and TOLAC• Induction or Augmentation have been shown to
increase risk
• Induction beginning with an unripe cervix decreases
likelihood of success
• Patients need counseling when pitocin is considered
or added; “this essentially doubles your rupture risk
from 1/200 to 1/100 (0.5 to 1%)
Misoprostol and TOLAC
• Multiple small studies have shown increased
risk…don’t use it!
Fetal Monitoring and TOLAC
• Often the first indicator of evolving uterine
rupture is changes in the fetal heart rate
tracing (i.e. before pain, bleeding, loss of
fetal station)
• Continuous EFM recommended!
6/19/2014
9
Foreboding EFM
Foreboding EFM
Interdelivery Interval
• Several studies have shown significantly
increased risk of uterine rupture with short
(< 18 months) interdelivery intervals
• As high as 6% rupture risk
• Believed to be related to scar
healing/integrity
6/19/2014
10
Counseling Your Patient• Early and Often!
• First prenatal visit history to obtain:
– Complete OB history
– Years of pregnancies, type of deliveries, reason
for C-Section(s), babies’ weights, complications
during pregnancy or delivery
– Request Operative Report
– Solicit TOLAC interest from patient
– Future fertility plans (family size, religious
objections)
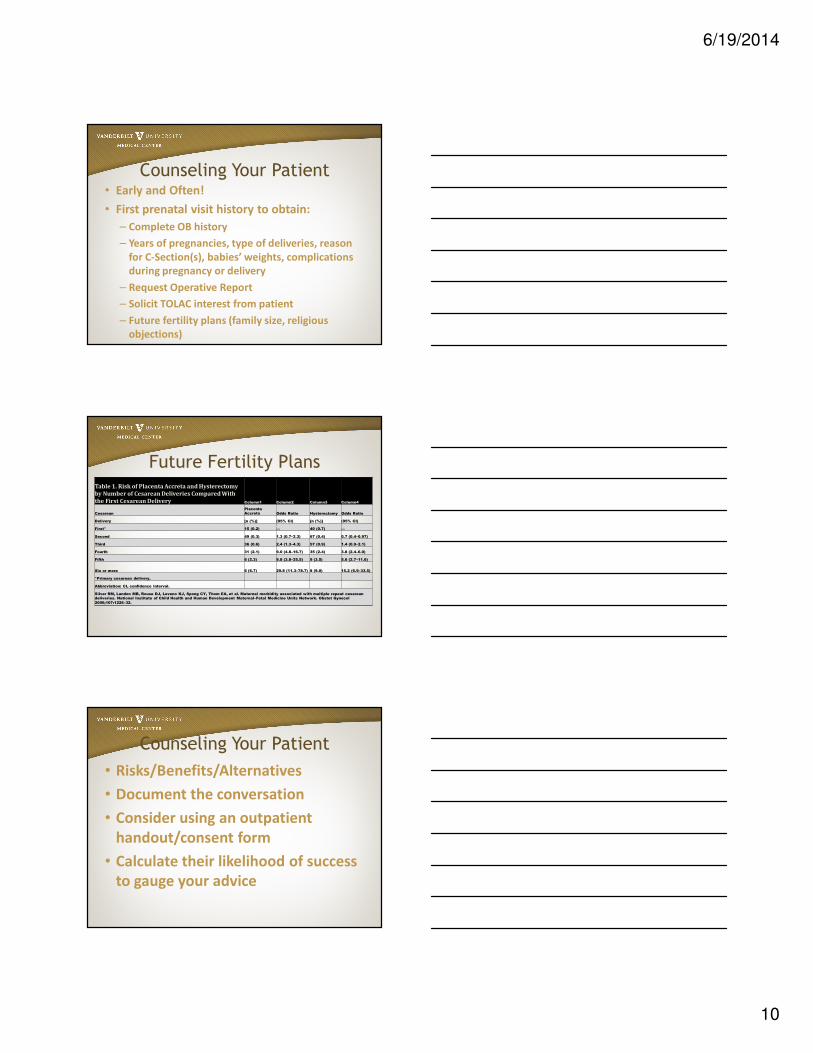
Future Fertility PlansTable 1. Risk of Placenta Accreta and Hysterectomy
by Number of Cesarean Deliveries Compared With
the First Cesarean Delivery Column1 Column2 Column3 Column4
Cesarean
Placenta
Accreta Odds Ratio Hysterectomy Odds Ratio
Delivery [n (%)] (95% CI) [n (%)] (95% CI)
First* 15 (0.2) — 40 (0.7) —
Second 49 (0.3) 1.3 (0.7–2.3) 67 (0.4) 0.7 (0.4–0.97)
Third 36 (0.6) 2.4 (1.3–4.3) 57 (0.9) 1.4 (0.9–2.1)
Fourth 31 (2.1) 9.0 (4.8–16.7) 35 (2.4) 3.8 (2.4–6.0)
Fifth 6 (2.3) 9.8 (3.8–25.5) 9 (3.5) 5.6 (2.7–11.6)
Six or more 6 (6.7) 29.8 (11.3–78.7) 8 (9.0) 15.2 (6.9–33.5)
*Primary cesarean delivery.
Abbreviation: CI, confidence interval.
Silver RM, Landon MB, Rouse DJ, Leveno KJ, Spong CY, Thom EA, et al. Maternal morbidity associated with multiple repeat cesarean
deliveries. National Institute of Child Health and Human Development Maternal–Fetal Medicine Units Network. Obstet Gynecol
2006;107:1226–32.
Counseling Your Patient
• Risks/Benefits/Alternatives
• Document the conversation
• Consider using an outpatient
handout/consent form
• Calculate their likelihood of success
to gauge your advice
6/19/2014
11
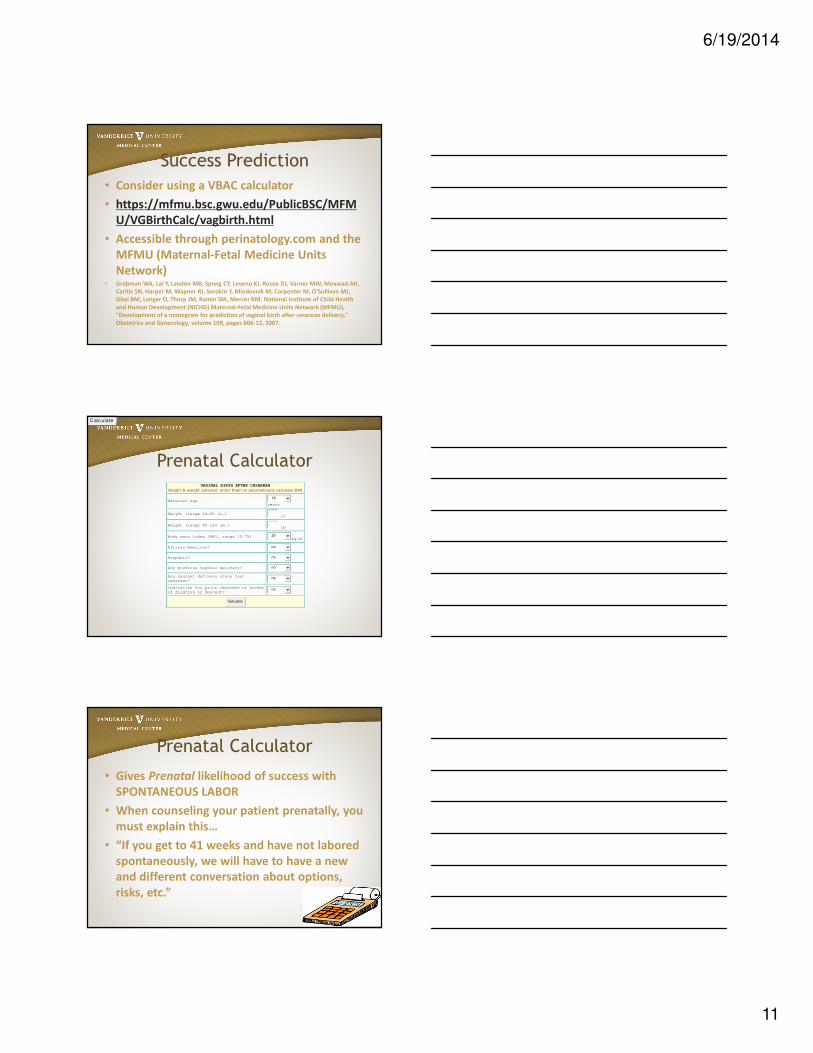
Success Prediction
• Consider using a VBAC calculator
• https://mfmu.bsc.gwu.edu/PublicBSC/MFM
U/VGBirthCalc/vagbirth.html
• Accessible through perinatology.com and the
MFMU (Maternal-Fetal Medicine Units
Network)• Grobman WA, Lai Y, Landon MB, Spong CY, Leveno KJ, Rouse DJ, Varner MW, Moawad AH,
Caritis SN, Harper M, Wapner RJ, Sorokin Y, Miodovnik M, Carpenter M, O'Sullivan MJ,
Sibai BM, Langer O, Thorp JM, Ramin SM, Mercer BM; National Institute of Child Health
and Human Development (NICHD) Maternal-Fetal Medicine Units Network (MFMU),
"Development of a nomogram for prediction of vaginal birth after cesarean delivery,"
Obstetrics and Gynecology, volume 109, pages 806-12, 2007.
Prenatal CalculatorVAGINAL BIRTH AFTER CESAREAN
Height & weight optional; enter them to automatically calculate BMI
Maternal age 18
years
Height (range 54-80 in.) in
Weight (range 80-310 lb.) lb
Body mass index (BMI, range 15-75) 25kg/m
2
African-American? no
Hispanic? no
Any previous vaginal delivery? no
Any vaginal delivery since last
cesarean? no
Indication for prior cesarean of arrest
of dilation or descent? no
Calculate
1825nononononoC alc ulate1825nononononoC alc ulate
Prenatal Calculator
• Gives Prenatal likelihood of success with
SPONTANEOUS LABOR
• When counseling your patient prenatally, you
must explain this…
• “If you get to 41 weeks and have not labored
spontaneously, we will have to have a new
and different conversation about options,
risks, etc.”
6/19/2014
12
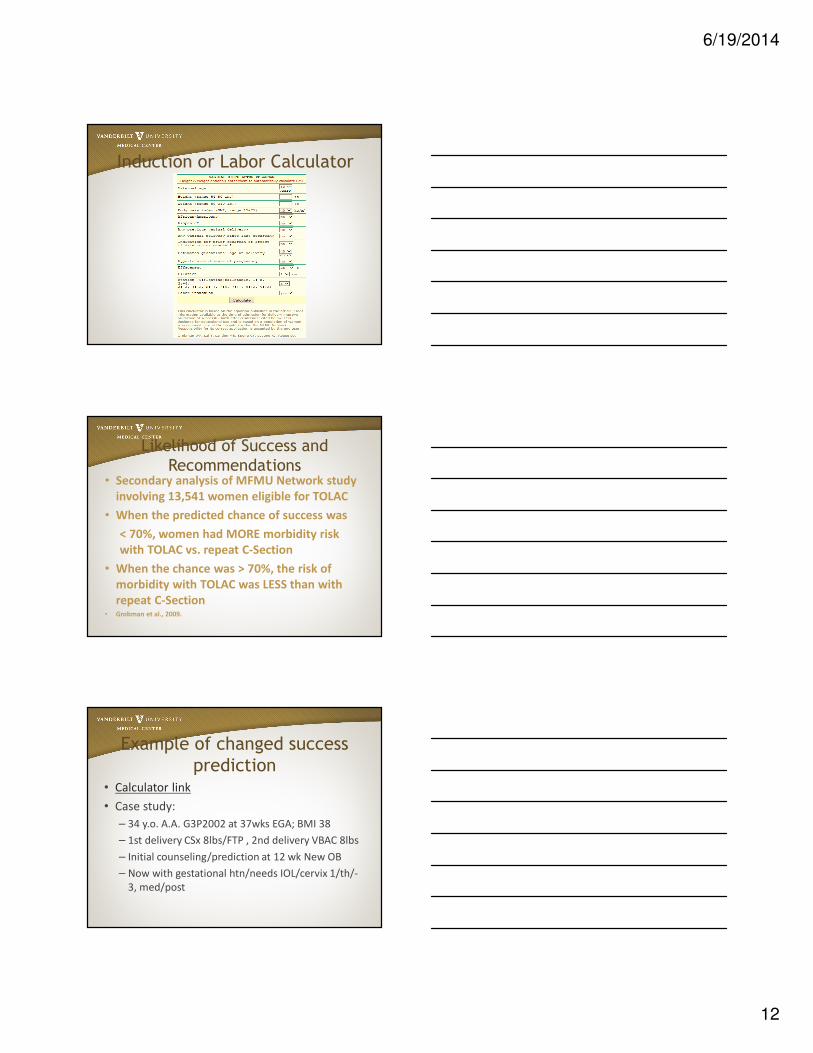
Induction or Labor Calculator
Likelihood of Success and
Recommendations• Secondary analysis of MFMU Network study
involving 13,541 women eligible for TOLAC
• When the predicted chance of success was
< 70%, women had MORE morbidity risk
with TOLAC vs. repeat C-Section
• When the chance was > 70%, the risk of
morbidity with TOLAC was LESS than with
repeat C-Section • Grobman et al., 2009.
Example of changed success
prediction• Calculator link
• Case study:
– 34 y.o. A.A. G3P2002 at 37wks EGA; BMI 38
– 1st delivery CSx 8lbs/FTP , 2nd delivery VBAC 8lbs
– Initial counseling/prediction at 12 wk New OB
– Now with gestational htn/needs IOL/cervix 1/th/-
3, med/post
6/19/2014
13
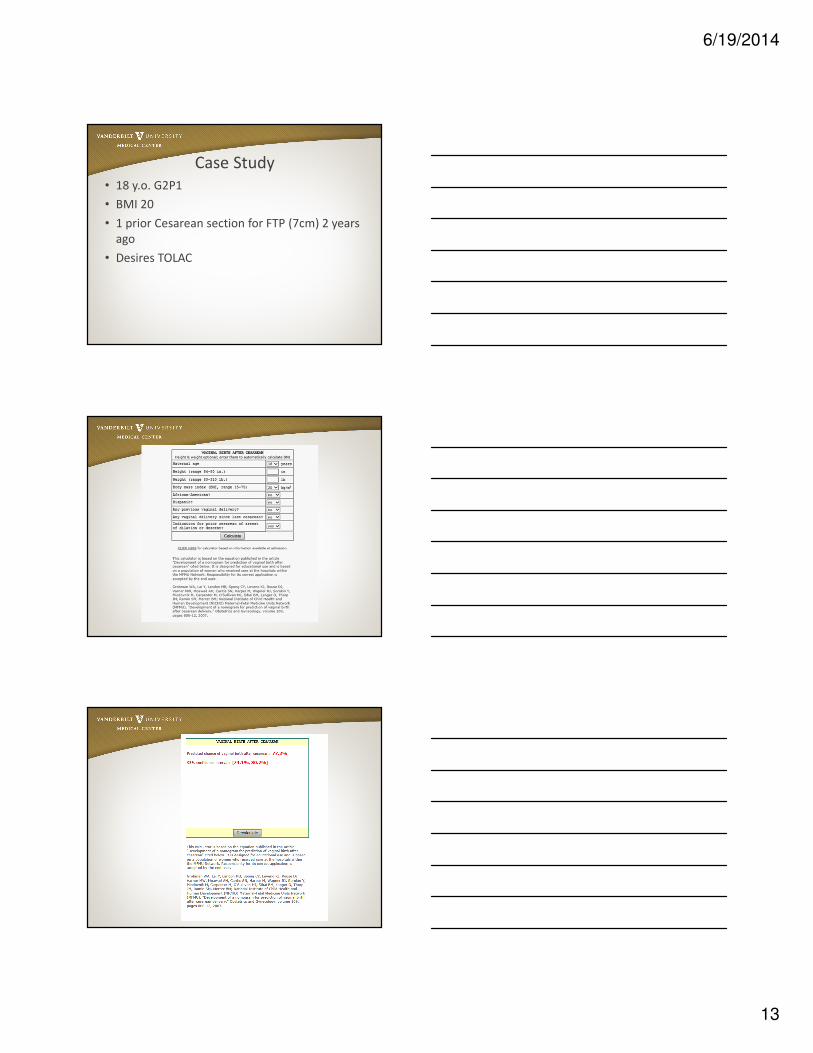
Case Study
• 18 y.o. G2P1
• BMI 20
• 1 prior Cesarean section for FTP (7cm) 2 years
ago
• Desires TOLAC
6/19/2014
14
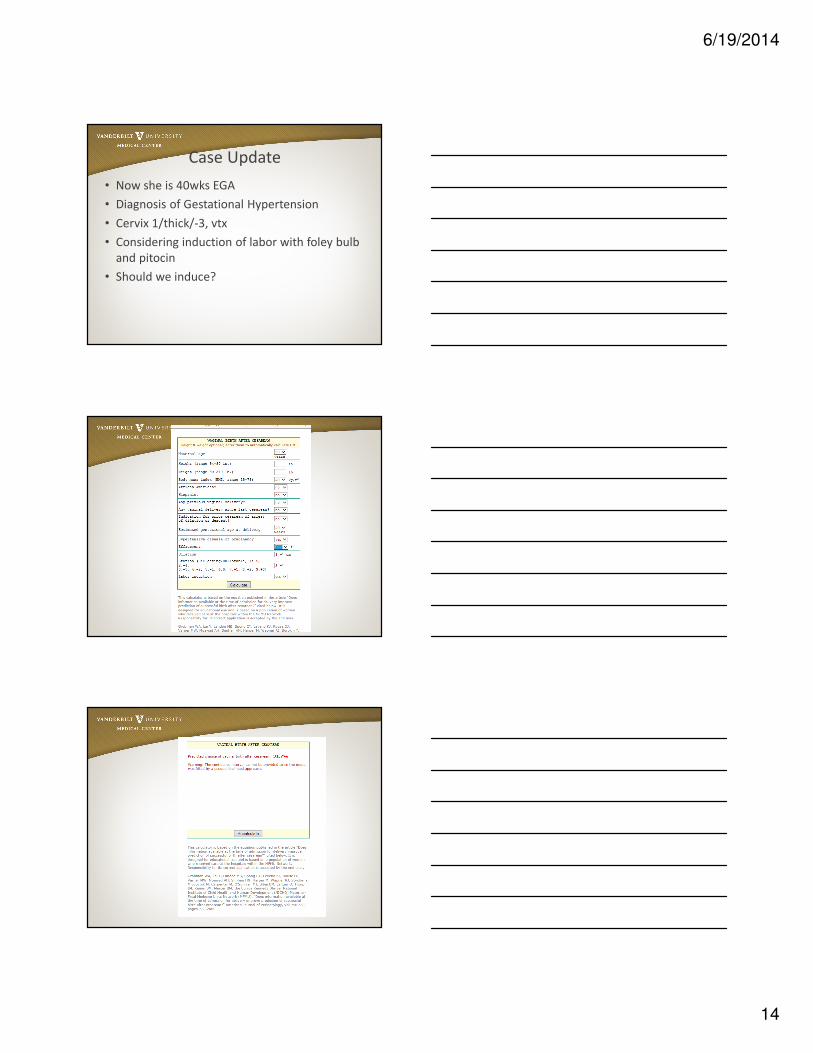
Case Update
• Now she is 40wks EGA
• Diagnosis of Gestational Hypertension
• Cervix 1/thick/-3, vtx
• Considering induction of labor with foley bulb
and pitocin
• Should we induce?
6/19/2014
15
Case 2
• 30 y.o G3P2002 Latina
• BMI 34
• h/o 1 SVD 2008, 8lb15oz female
And 1 CSx 2011, 7lb 11oz Male (breech)
Should she have a TOLAC?
6/19/2014
16
References• Grobman, WA, Lai Y, Landon MB, Spong CY, Leveno KJ, Rouse DJ, et al. Can a
prediction model for vaginal birth after cesarean also predict the probability of
morbidity related to a trial of labor? Am J Obstet Gynecol 2009; 200(1):56.e1-
56.e6.
• Grobman WA, Gilbert S, landon MB, Spong CY, Leveno KJ, Rouse DJ, et al.
Outcomes of induction of labor after one prior cesarean. Obstet Gynecol 2007;
109:262-9.
• Guise, JM, Denman MA, Emeis C, Marshall N, Walker M, Fu R, et al. Vaginal birth
after cesarean: New insights on maternal and neonatal outcomes. Obstet Gynecol
2010;115(6):1267-78.
• Landon, MB, Spong CY, Thom E, Hauth JC, Bloom SL, Varner MW, et al. Risk of
uterine rupture with a trial of labor in women with multiple and single prior
cesarean delivery. National Institute of Child Health and Human Development
Maternal-Fetal Medicine Units Network. Obstet Gynecol 2006; 108(1):12-20.
.
References• National Institutes of Health. NIH Consensus Development Conference: vaginal
birth after cesarean: new insights. Consensus Development Conference
statement. Bethesda (MD):NIH;2010. Retrieved from
http://consensus.nih.gov/2010/images/vbac/vbac_statement.pdf
• Tahseen, S., & Griffiths, M. Vaginal birth after two caesarean sections (VBAC-2)-a
systematic review with meta-analysis of success rate and adverse outcomes of
VBAC-2 versus VBAC-1 and repeat (third) caesarean sections. BJOG 2010;117:5-19.
• Vaginal birth after previous cesarean delivery, Practice Bulletin Number 115.
American College of Obstetricians and Gynecologists. Obstet Gynecol
2010;116:450-63.





























