Embed Size (px)
Citation preview

Vol. 3, 19-24, January/February 1994 Cancer Epidemiology, Biomarkers & Prevention 19
Tobacco Smoking, Occupation, and p53 NuclearOverexpression in Early Stage Bladder Cancer”
Zuo-Feng Zhang,2 Alvaro S. Sarkis,Carlos Cordon-Cardo, Guido Dalbagni,Jonathan Melamed, Armen Aprikian, Daphna Pollack,Joel Sheinfeld, Harry W. Herr, William R. Fair,Vidor E. Reuter, and Cohn BeggDepartment of Epidemiology and Biostatistics [Z.-F.Z., D.P., C.B.[,
Urology Service, Department of Surgery [ASS., GD., A.A., 1.5., H.W.H.,
and W.R.F.[, and Department of Pathology [CC-C., J.M., V.E.R.[,Memorial Sloan-Kettering Cancer Center, New York, New York
Abstrad
Epidemiological studies show an increased risk ofbladder cancer associated with tobacco smoking andoccupational exposures. Certain carcinogens in tobaccoand occupational exposures cause DNA damage andmay produce specific mutations. TP53 is considered acommon target for carcinogenic agents, and mutationsof this gene are reported to be the most frequentnuclear abnormalities in human cancer. In order toinvestigate the relationship between tobacco smoking,occupations, and altered patterns of p53 expression, wehave analyzed a group of 1 09 incident patients withsuperficial transitional cell carcinoma of the bladder.We assessed p53 nuclear overexpression by the use ofanti-p53 antibody PAb1 801 and immunohistochemistry,and identified 45 of 109 patients (41 %) displayingp53-positive phenotype. We observed a significantassociation between the number of cigarettes smokedper day and p53 nuclear overexpression ( p = 0.02). Theodds ratios were 2.3 for those smoking 1-2 packs perday and 8.4 for smoking more than 2 packs per day.Similar estimates were obtained after controlling for age,sex, and race. Elevated odds ratios were also observedfor dye-/ink-related (odds ratio = 2.0; 95% Cl, 0.4-9.4)
and cooking-related occupations (1 .8, 0.6-5.0), althoughthose were not statistically significant. These datasupport the hypothesis that certain carcinogens derivedfrom cigarette smoking and occupations may induceTP53 mutations, which in turn are involved in earlysteps of bladder carcinogenesis.
Introdudion
Bladder cancer is one of the most common cancers, with219,000 new cases occurring annually worldwide (1). Therates are highest in developed countries, with 148,200 new
patients each year, making bladder tumors the sixth highestranking cancer in the developed world. Many epidemio-logical studies have been conducted to explore the etiologyof bladder cancer. Cigarette smoking has been considered asthe most important risk factor (2), contributing to half of thebladder cancers in men and one-third of those in women.The relative risks (or ORs)’ for smoking ranges between 2and 3. Two known human bladder carcinogens, 2-AN (2-Aminonaphthalene) and 4-ABP (4-Aminobiphenyl), and twosuspected human bladder carcinogens, o-toluidine and ani-line, are present in tobacco (2). Occupational exposureshave also been associated with bladder cancer. In the United
States, the population-attributable risks for occupational ex-posure have been estimated to be 21-25% for white males(3) and 1 1% for white females (4). Most occupational orchemical substances and their metabolites are excretedthrough the urinary tract and have direct contact with thebladder mucosa (5). The risk of bladder cancer has beenlinked to dyestuff production (6-1 2), rubber manufacturing(8, 1 0, 1 3-1 6), the chemical and plastics industry (8, 1 2-14,17-20), the textile and leather industry (8, 10, 16, 21, 22),printing (1 0, 23, 24), petroleum, automobile and gas stationwork (3, 14, 19, 25), the metal industry (3, 10, 1 5, 26), mm-ing (8, 1 5, 23, 24), pesticides (1 3, 1 7, 27), hairdressing (28),and cooking (29). Results from different studies are incon-sistent, which may be caused by statistical problems such aspower and selection biases in the studies, and by the fact thatvarious populations may have different patterns of occupa-tional exposures (9). Although the carcinogens associatedwith occupational exposures remain unclear, 2-AN, 4-ABP,and benzidine (associated with occupational exposures todyestuff, textiles, and rubber) are considered as human blad-der carcinogens. o-Toluidine (used in rubber manufactur-ing), 4,4’-methylenebis(2-chloroaniline) (used in poly-
urethane manufacturing) and n itroarornatics (productsof diesel fuel) may be associated with the risk of bladdercancer.
Certain carcinogens present in tobacco cause DNAdamage and may produce specific mutations. TPS3 is a corn-mon target for carcinogenic agents, and mutations at thislocus are reported to be the most frequent molecular ab-normalities in human cancer. Inactivation of TP53 can becaused by TP53 mutations, or by complexation with viraloncoproteins such as the papilloma E6 or with the productencoded by the MDM2 gene (p90 protein) (30). MutatedTP53 loses its function as a tumor suppressor gene and usu-ally leads to overexpression of the p53 protein. Comparedwith the wild-type protein, most mutant p53 products have
Received 4/1 6/93; revised 8/3/93; accepted 8/1 2/93.I Supported in part by Grant ES-06718 and CA-47538 from the National
Institutes of Health.2 To whom requests for reprints should be addressed, at the Department ofEpidemiology and Biostatistics, Memorial Sloan-Kettering Cancer Center,
1 275 York Avenue, Box 44, New York, NY 10021.
I The abbreviations used are: OR, odds ratio; 2-AN, 2.Aminonaphthalene;4-ABP, 4-Aminobiphenyl; IHC, immunohistochemical; H-E, hematoxylin-
eosin; CI, confidence interval.
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

20 Smoking and p53 Overexpression in Bladder Tumor
a prolonged half-life and are thus more likely to be detectedusing IHC assays (31). Identification of p53 nuclear over-
expression by IHC has been reported to correlate well withTPS3 mutations, as determined by DNA sequencing analysisin a variety of tumors (32). Mutations or overexpression ofp53 have been associated with previous exposure to ciga-mette smoking in lung (33-35), head and neck (36, 37), andesophageal cancers (38). It also has been associated withexposure to UV light in squamous cell carcinoma (39), af-latoxin exposure, and hepatitis B virus in hepatocellular car-cinornas. Jones et al. (40) first reported the association be-tween smoking and TP53 genotype abnormalities in bladdercancer. To our knowledge, theme is no such study correlatingboth cigarette smoking and occupation with p53 tmans-formed phenotypes in bladder cancer.
Recent reports reveal that p53 mutations occur corn-monly in bladder carcinomas. We previously reported that
p53 nuclear overexpression correlates well with loss of het-emozygosity in bladder cancer (41 ),and is associated with ahigh risk for disease progression in T� bladder carcinomas(42). We undertook the present study in order to investigatethe relationship between tobacco smoking, occupation, andp53 nuclear overexpression in a group of 1 09 incident pa-tients with superficial transitional cell carcinomas of thebladder.
Patients and Methods
We reviewed the medical charts ofconsecutive patients withbladder cancer seen at the Memorial Sloan-Kettering CancerCenter from 1 972 to 1980. Attention was restricted to in-cident cases with tmansumethral resection specimens diag-nosed as transitional cell carcinoma ofthe bladder at Ta, TIS,
or T1 stage (tumor, nodes, metastasis classification), and noprevious history of adjuvant therapy. H-E sections were me-viewed and the pathological diagnosis of bladder cancerwas made by a single pathologist (V. E. R.). We obtained atotal of 1 09 (88 males, 21 females) incident cases.
Information on smoking, drinking, occupational expo-sure, and family history of cancer was abstracted from thecharts. These data were systematically collected on admis-sion. Patients were interviewed by surgeons or physicianswith a standard admission history form. The questions in thestandard admission history form include “Tobacco-type, du-ration, & when stopped ifstopped”; “Alcohol-type, duration,& when stopped if stopped”; “Occupation; Dye or rubberindustry employment”; and “Family history of cancer or al-lied disease.” Among 109 patients, 108 (99%) had infor-mation on ever/never smoking. Fifty-eight of 66 cigarettesmokers (88%) had information on cigarettes per day butonly 56% of cigarette smokers had data on years of smoking.One hundred seven (98%) incident cases had data on ever!never drinking and 102 (95%) had information on familyhistory of cancer. Occupational titles were available for 107(98%) patients but 9 patients (8%) were recorded as “me-tired”. Although ours is not an interview study, we believethat the information on smoking, drinking, occupation, andfamily history of cancer collected from the Standard Admis-sion History Form at the Memorial Sloan-Kettering CancerCenter are comparable in terms of reliability with data col-lected by conventional interview studies.
Tissue sections from these tumors and five normal blad-der specimens were analyzed immunohistochernically foraltered patterns of p53 expression, using a standard avidin-biotin technique (43). Sections 5 pm were deparaffinizedand incubated in 1 0% normal horse serum for 30 mm, and
then incubated overnight at 4#{176}with a mouse monoclonalantibody PAb1 801 (Ab2, IgGl , Oncogene Science, Union-dale, NY) at a concentration of 200 ng/rnl. This antibodyrecognizes a denatumation-mesistant epitope located betweenamino acids 32 and 79, which is present in both wild-typeand mutant human p53 proteins (44). Depamaffinized tissuesections of a breast carcinoma known to contain mutant p53served as a positive control. As a negative control, we sub-stituted antibody PAb1 801 with a class-matched, nonspe-cific mouse monoclonal antibody (MIgS1 -kp-1 , Phammin-gen, San Diego, CA) at the same final concentration. Tissueswere incubated subsequently with biotmnylated horse anti-mouse secondary antibodies (Vector Laboratories, Inc., Bum-lingarne, CA) for 30 mm at a 1 :1 00 dilution, and then withavid i n-bioti n peroxidase complexes (Vector Laboratories,Inc.) at 1 :25 dilution for 30 mm. Diaminobenzidine (0.06%)was used as the chmomogen and 1 % modified Harris he-matoxylmn was used as the counterstain.
Two investigators (C. C. C. and V. E. R.)jointly reviewedthe slides in order to score IHC staining. To limit discrep-ancies, the pattern of p53 nuclear overexpression was clas-sified into four categories by estimating the percentage oftumor cell nuclear staining: (1 ) negative, (2) patchy (<20%),(3) heterogeneous (20-75%), and (4) homogeneous (>75%).There was no disagreement between two investigators byusing the four categories for this study. For statistical analy-sis, negative or patchy was considered as negative and het-emogeneous or homogeneous as positive. All specimenswere graded using a modification of the World Health Or-ganization classification and staged according to the tumor,nodes, metastasis classification. Researchers abstracted epi-demiological risk factors from the charts without knowledgeof the IHC results.
Association between p53 nuclear ovemexpression andexposure to risk factors, such as cigarette smoking and oc-cupations, were measured by the OR and its 95% CI. Theodds ratio for smoking is the odds of smoking in the p53-positive group divided by the odds of smoking in the p53-negative group. Smoking exposure was classified by ciga-mettes per day in four categories: non-smoking, 1-20cigarettes per day, 21-40 Cigarettes per day, and more than40 cigarettes per day. ORs and 95% CIs were estimated foreach of the smoking groups by comparing them with thenonsmoki ng group. The dose-response relationsh i p wasevaluated by a trend test. A multiple unconditional logisticregression method was used to estimate the adjusted OR
after controlling for potential confounders such as age, sex,and mace. Each ofthese factors was observed to be associated(not necessarily significantly) with both smoking and P53overexpression, satisfying the conditions for potential con-founding. In addition, it seems prudent to adjust for knownbladder cancer risk factors. The occupational data were firststudied on the basis of individual occupational titles. Pa-tients were subsequently divided into seven occupationalgroups: dye-/ink-related, cooking-related, chemical-related,exhaust-related, professional/busi ness-related, medical-related, and other occupations. ORs and 95% CIs were es-timated on the grouped basis.
ResultsTwenty-seven percent of the patients were aged less than 60years, 48% were between the ages of 60 and 69 years, and25% were aged 70 or older; 81 % were males and 94% werewhite.
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

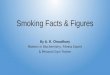
C
Fig. 1. PAB1 801 immunoreactivity in a 1, bladder carcinoma showing IHC
nuclear staining.
Cancer Epidemiology, Biomarkers & Prevention 21
p53 Nuclear Overexpression in Superficial Bladder Cancer.Five morphologically normal bladder specimens examinedshowed absenceofnuclearstaining in urothelial and stromalcells. Similarly, noneofthe normal mesenchyrnal cells in all1 09 superficial bladder tumors analyzed showed detectablep53 nuclear reactivity. However, 45 of 109 cases (41%)studied showed heterogeneous or homogeneous nuclearstaining for the anti-p53 PAb18O1 antibody. The positivestaining is illustrated in Fig. 1.
Cigarette Smoking and p53 Nuclear Overexpression.Seventy-seven patients (71 %) had been smokers during theirlifetime (“ever” smokers, at least one cigarette per day for aminimum of 1 year). Sixty-six patients (61 %) were cigarettesmokers and 1 1 (1 0%) were either pipe or cigar smokers.Among ever smokers, 45 of 77 patients (58%) smoked 1-20cigarettes per day, 27 (35%) smoked 21-40 per day, and 5(6%) smoked more than two packs per day.
Nuclear overexpression of the p53 protein was ob-served in 34 of 77 (44%) ever smokers but in only 10 of 31(32%) never smokers. This results in a crude OR of 1 .7 forthe association between smoking status and p53 nuclearoverexpression. The results show a clear trend in smokingexposure. A significant association was observed betweencigarettes per day (as a continous variable) and p53 over-expression (OR = 1 .03; p = 0.02). The ORs were 1 .2, 2.3,and 8.4 for those who smoked 1-20 cigarettes per day,21 -40 per day, and more than 40 per day respectively corn-pared to the non-smoking group (trend test: p = 0.03). Aftercontrolling for the potential confounding effects of age, sex,and race, these associations were little changed (Table 1).
Table 2 summarizes data from recent studies dealingwith a variety of smoking-related tumors and their associa-tion between smoking and TP53 mutations. It also includesresults we have obtained on the association between p53nuclear overexpression and smoking in 48 patients with pri-mary prostate cancers and 1 08 patients with primary softtissue sarcomas, two diseases believed to be unrelated tosmoking. In Table 2, second column, the prevalences ofp53 ovemexpression are presented. Table 2, third columncontains the relative risks of smoking for each of the can-cer sites. Table 2, fourth column contains the ORs reflect-ing the association between smoking and p53 overexpres-sion among cases (i.e., the measure studied in this article).
These studies show a strong correlation between all threeof the measures examined across cancer sites. That is, can-cers more strongly associated with smoking possess ahigher prevalence of p53 overexpression, and in turn ex-hibit a stronger association between smoking and p53nuclear overexpression. Our results categorize bladdercancer between cancers that are strongly associated withsmoking (lung, head and neck, and esophageal cancers),and those cancers that are probably not related to smoking(prostate cancers and soft tissue sarcomas).
Occupations and p53 Overexpression. Occupations wereanalyzed first at the individual basis but the frequencies aretoo sparse for meaningful interpretation (Table 3). Patientswere then divided into seven general occupational groupsaccording to their potential exposures. The variation inprevalence among the seven groups is easily explained by
chance ( p = 0.68). The firstfour categories have been linkedto bladder cancer in previous studies. When combined,these occupations show little association with p53 overex-pression, with an OR of 1 .2 (0.55, 2.65). However, the small
sample sizes and consequent low power indicate that wecannot rule out the possibility of occupational/p53 associa-tions for selected occupations, such as dye-related andcooking-related occupation with ORs of 2.0 and 1 .8 respec-tively, combining all other occupations as a control group.
Smoking, Occupational Exposure, and Age. Further exam i-nation ofthe data reveals that age may be a modifier for theassociation between smoking, occupational exposures, andp53 nuclear overexpression. The ORs for srnoking-p53 as-
sociation are 0.6 for younger patients (<60 years) and 2.4 forolder patients (�60 years). The ORs of p53 overexpressionwere 4.3 for dye-related occupations and 7.5 for cooking-related occupations for younger patients (<60 years), and 1 .5for dye-related and 0.4 for cooking-related occupations forolder patients (�60 years) in a stratified analysis (no statis-tically significant interaction). Because of the number ofassociations studied, these results must be viewed withcaution.
Finally, we studied other risk factors including alcoholconsumption and family history of cancer but found no ap-parent associations.
DiscussionThere are several potential limitations ofthis study. First, thesmall sample size limits our ability to reliably detect asso-ciations. This is especially true for occupational exposures,due to the large variety of occupations. However, at presentbiomarker studies are difficult and expensive to conduct,and in context our study has a larger sample size than almostall other published molecular epidemiology studies in can-cer (33-35, 37, 38, 40, 45-48). Second, information ab-stracted from medical charts may be less reliable than fromconventional interview studies. However, since the smokinginformation was collected by surgeons or physicians whointerview patients according to formatted questions onsmoking history on a Standard Admission History Form, thepotential misclassification problem is comparable with con-ventional interview or questionnaire studies. Third, the po-tential misclassification bias may affect the association ob-served. The smoking information was abstracted by a singleinvestigator (Z. F. Z.) without knowledge of the p53 status.Consequently, iftheme is misclassified data on smoking statusthe errors should occur to a similar degree in p53-positiveand p53-negative patients. It is well known that nondiffer-
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

22 Smoking and p53 Overexpression in Bladder Tumor
Table 1 p53 overexpression/smoking association
p53 overexpressionVariables -� ORCrudc 95% Cl
No (%) Yes (0/)
ORAd,uste,ia 95% CI
Smoking
No 21 (68) 10 (32) 1.0 1.0
Yes 43 (56) 34 (44) 1 .7 0.7-4.0 1 .7 0.6-4.7
Cigarette 37 (56) 29 (44) 1 .7 0.7-4.0 1 .7 0.6-4.5
Pipe/cigar 6 (55) 5 (45) 1 .8 0.4-7.1 2.0 0.4-1 0.0
Cigarettes per day”
No 21 (68) 10(32) 1.0 1.0
1-20 29 (64) 16 (36) 1.2 0.4-3.1 1.3 0.4-3.7
21-40 13(48) 14(52) 2.3 0.8-6.6 2.4 0.7-8.1
>40 1 (20) 4 (80) 8.4 0.8-85.2 12.6 1.1-147
Trend test p 0.03 p 0.03
a OR adjusted, odds ratio adjusted for age, sex and race.1� Median of cigarettes per day was assigned for smokers with missing data and for pipe/cigar smokers.
Table 2 p53 smoking association by tumor sites
Prevalence and 95% CI” - .. . Relative risk
Tumor site of TPS3 mutation,/ .. of smoking-cancer
overexpression
OR and 95% CI”.
(or p-value) of smoking-p53.
mutation/overexpression
Lung
Suzuki (33) NSC” 47, 29-65 7-15 (2) 5.3 (p = 0.01)
Miller (34) SC 70, 58-91 NA
NSC 23,0.1-46 NA
Kondo)35) 44,21-67 ll.Btp= 0.03)
Head/neck (5CC)
Field (37) SC 67, 56-78 3-10 (2) 16, 1.8-142
Esophagus
Hollstein (38) SC 41, 25-58 3-5 (2) 3.1, 0.7-1 3.1
Bladder (TCC(
Jones (40) TC 36, 26-47 2-3 t2) 1 .4, 0.6-3.5
Zhang’ TC 41, 32-51 1.7, 0.7-4.0
Soft Tissue Sarcoma
Zhang’ 27, 18-35 0.7 (58)-1.8 (59) 0.9, 0.2-2.9Prostate
Zhang’ AD 19, 8-30 0.9 (60-62)-1.8 (63,64) 0.7, 0.2-2.9
a 95% CIs of prevalence and odds ratios were estimated by the authors according to original data.i, NSC, no small cell; SC, small cell; TC, transitional cell; AD, adenocarcinoma; NA, no applicable.C Unpublished data.
ential misclassification ofthis nature attenuates observed as-
sociations toward the null. For the occupational informa-tion, there may be a misclassification bias from using theoccupational title/group to represent the occupational ex-posure. Finally, we took care to assemble an incident caseseries in a defined time period. Since no informed consentwas required, we were able to include all incident cases.Moreover, the use of incident cases eliminates the bias thatwould be induced in a prevalent sample due to the knownassociation between p53 status and survival (42).
In this study, five momphologically normal bladderspecimens and the normal mesenchyrnal cells in all super-ficial bladder tumors analyzed showed absence of nuclearstaining. These findings are consistent with the well-documented short half-life of the wild-type p53 protein,which is normally present at a very low steady-state level(31) and is thus undetectable immunohistochemically. Mu-tated p53 products have a half-life 4-20 times longer thanthe wild-type p53 protein (31). This results in the accumu-lation of mutated p53 in the nucleus, rendering it detectableby IHC analysis (49). Moreover, detection of pS3 nuclearoverexpression by IHC analysis highly correlates with mu-
tations on the gene, identified by sequencing analysis by ourprevious study and others (32, 41 , 46, 50-52).
There is compelling evidence that cancer arises via amulti-step process (53). It has become apparent that the lossof tumor-suppressor gene function is widespread and an im-portant step in the development of most malignancies (54).It is known that most carcinogens induce carcinogenicchanges as a result of direct interaction with DNA (55, 56),and specific carcinogens produce mutations in particulargenes (57). It has also been hypothesized that a commonbiochemical pathway for controlling cell growth is inter-rupted in variety of cancers. TP53 is a good marker sincealterations ofthis tumor suppressor gene seem to be involvedthe pathway in the majority of cancers. TP53 mutations forbladder cancer reveal multiple examples of most possiblebase substitutions, which makes bladder cancer a goodcandidate in exploring the association between TP53 mu-tations and environmental exposures, as well as genetic sus-ceptibility.
Increased prevalence (44%) of p53 nuclear overexpres-sion was found in smokers compared with 32% in patientswho had never smoked. Jones et al. (40) first reported that
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Table 3 Occupational title and p53 overexpression
Occupational titlep53
ORcrude 95% CI- +
2.0 0.4-9.4
1.8 0.6-5.0
0.4 0.1-1.5
1 1
0 1
1 1
1 0
0 1
3 4 (57%)
1 3
0 2
0 1
7 38 9 (53%)
0 1
1 0
1 1
2 2 t50%)
1 0
1 0
6 1
0 1
0 1
1 0
1 0
10 3(23%)
5 4
1 1
0 1
4 1
0 1
1 1
1 0
1 1
2 3
3 2
1 1
0 1
6 1
1 0
1 0
27 18(40%)
0 1
2 1
1 0
1 0
4 2 (33%)
0 1
1 1
1 0
2 0
5 3
0 1
9 6 (40%)
63 44
0.9 0.4-2.0
0.7 0.1-4.0
0.9 0.3-2.9
16 of 40 (40%) bladder tumors from smokers and 1 3 of 40(33%) tumors from lifetime nonsmokers showed p53 mu-tations detected by polymerase chain reaction-single strandconformational polymorphism. Their results on the associa-tion between smoking and p53 genotype abnormalities in
Cancer Epidemiology, Biomarkers & Prevention 23
Die/ink-related
Die and tool maker
Publisher
Textile worker
Shoe repairman
Banker
Total
Cooking-related
Restaurant worker
Baker
Candy maker
Homemaker
Total
Chemical-related
Chemist
Photographer
Clean/maintenance worker
Total
Exhaust-related
Airplane pilot
Bus driver
Engineer
Foreman
Mechanic
Machinist
Taxi driver
Total
Professional/Business-related
Business
Insurance
Judge
Lawyer
Librarian
Manager
Professor
Secretary
Salesman/woman
Self employed
Stock broker
Importer
Administrator
Executive
Security
Total
Medical-related
Dentist
Physician
Podiatrist
Radiologist
Total
All other
Accountant
Butcher
Economist
Farmer
Retired
Seamstress
Total
Total
bladder cancer are consistent with our findings based onp53 transformed phenotypes. In addition, we explored thepossible dose-response relationship between smoking andp53 nuclear overexpression. We identified a significant as-sociation between cigarettes per day and p53 nuclear over-
expression.The results of this study are also consistent with studies
of this topic in other cancers (Table 2). The medium-sizedassociation (1 .7) between smoking and p53 nuclear over-expression in a tumor and a medium-sized relative risk (2-3)for smoking, along with a medium prevalence of p53 over-expression (41 %),categorizes bladder cancer between can-cers for which the smoking risk is very strong (e.g., lung, headand neck) and those for which the smoking risk is minimalor zero (prostate, soft tissue sarcoma).
References1 . Parkin, 0. M., Laara, E., and Muir, C. S. Estimates of the worldwide fre-
1 .5 0.2-1 0.7 quency of sixteen major cancers in 1 980. Int. 1. Cancer, 4 1: 1 84-1 97, 1988.2. IARC Working Group. IARC monographs on the evaluation of the carci-nogenic risk ofchemicals to humans. Tobacco Smoking, p. 83. Lyon, France:
International Agency for Research on Cancer, 1986.
3. Silverman, 0. T., Levin, 1. I., Hoover, R. N., and Hartge, P. Occupationalrisks ofbladder cancer in the United States. I. White men. 1. NatI. Cancer Inst.,
81: 1472-1479, 1989.
4. Silverman, 0. T., Levin, L. I., and Hoover, R. N. Occupational risks of
bladder cancer among white women in the United States. Am. 1. Epidemiol.,132:453-461, 1990.
5. Matanoski, G. M., and Elliott, E. A. Bladder cancer epidemiology. Epide-
miol. Rev., 3: 203-229, 1981.
6. Rehn, L. Blasengeschwulste bei Fuchsin-Arbeitern. Arch. KIm. Chir., 50:588-600, 1895.
7. Boyko, R. W., Cartwright, R. A., and Glashan, R. W. Bladder cancer in dye
manufacturing workers. 1. Occup. Med., 27: 799-803, 1985.
8. Claude, J., Kunze, E., Frentzel-Beyme, R., et al. Life-style and occupationalrisk factors in cancer of the lower urinary tract. Am. 1. Epidemiol., 124: 578-
589, 1986.
9. LaVeccia, C., Negri, E., D’Avanzo, B., and Franceschi, S. Occupation andthe risk of bladder cancer. nt. 1. Epidemiol., 19: 264-268, 1990.
1 0. Vineis, P., and Magnani, C. Occupation and bladder cancer in males: a
case-control study. Int. 1. Cancer., 35: 599-606, 198S.
1 1 . Ward, E., Carpenter, A., Markowitz, S., Roberts, 0., and Halperin, W.Excess number of bladder cancers in workers exposed to ortho-toluidine and
aniline. 1. NatI. Cancer. Inst., 83: 501-506, 1991.
12. Meigs, 1. W., Marrett, L. D., Ulrich, F. U., and Flannery, I. T. Bladdertumor incidence among workers exposed to benzidine: a thirty-year follow-
up. 1. NatI. Cancer Inst., 76: 1-8, 1986.
1 3. Zahm, S. H., Hartge, P., and Hoover, R. The national bladder cancer
study: employment in the chemical industry. 1. NatI. Cancer Inst., 83: 501-506, 1991.
14. Howe, G. R., Burch, 1. 0., Miller, A. B., et al. Tobacco use, occupation,
coffee, various nutrients, and bladder cancer. 1. NaIl. Cancer Inst., 64: 701-
713, 1980.
1 5. Schifflers, E., Jamart, J., and Renard, V. Tobacco and occupation as risk
factors in bladder cancer: a case-control study in southern Belgium. Int. J.Cancer, 39:287-292, 1987.
16. Negri, E., Piolatto, G., Pira, E., Decarli, A., Kaldor, 1., and LaVecchia, C.
Cancer mortality in a Northern Italian cohort of rubber workers. Br. I. Ind.Med., 46: 624-628, 1989.
1 7. Kabat, G. C., Dieck, G. S., and Wynder, E. L. Bladder cancer in non-
smokers. Cancer, 57: 362-367, 1986.
18. Steenland, K., Burnett, C., and Osorio, A. M. A case-control study ofbladder cancer using city directories as a source of occupational data. Am.1. Epidemiol., 126: 247-257, 1987.
1 9. Schoenberg, 1. B., Stemhagen, A., Mogielnicki, A. P., Altman, R., Abe, T.,
and Mason, T. J. Case-control study of bladder cancer in New Jersey. I Oc-cupational exposures in white males. J. NatI. Cancer Inst., 72:973-981 , 1984.
20. Cole, P., Hoover, R., and Friedell, G. H. Occupation and cancer of thelower urinary tract. Cancer, 29: 1250-1260, 1972.
21 . Morrison, A. S., Ahlbom, A., Verhoek, W. G., Aoki, K., Leck, I., Ohno,Y., and Obata, K. Occupation and bladder cancer in Boston, USA, Manches-
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

24 Smoking and p53 Overexpression in Bladder Tumor
ter, UK, and Nagoya, Japan. 1. Epidemiol. Community Health, 39: 294-300,
1985.
22. Marrett, L. 0., Hartge, P., and Meigs, 1. W. Bladder cancer and occu-
pational exposure to leather. Br. J. Ind. Med., 43: 96-100, 1986.
23. Claude, J. C., Frentzel-Beyme, R. R., and Kunze, E. Occupation and risk
of cancer of the lower urinary tract among men. A case-control study. Int. 1.Cancer, 41: 371-379, 1988.
24. Brownson, R. C., Chang, 1. C., and Davis, 1. R. Occupation, smoking, and
alcohol in the epidemiology of bladder cancer. Am. 1. Public Health, 77:1298-1300, 1987.
25. Silverman, D. T., Hoover, R. N., Mason, T. J., and Swanson, G. M. Motorexhaust-related occupations and bladder cancer. Cancer Res., 46: 2113-
2116, 1986.
26. Smith, E. M., Miller, E. R., Woolson, R. F., and Brown, C. K. Bladder
cancer risk among auto and truck mechanics and chemically related occu-pations. Am. J. Public Health, 75: 881-883, 1985.
27. Blair, A., Grauman, D. 1., Lubin, J. H., and Fraumeni, 1. F. Lung cancerand other causes of death among licensed pesticide applicators. 1. NatI. Can-cer Inst., 71: 31-37, 1983.
28. Guberan, E., Raymond, L., and Sweetnam, P. M. Increased risk for male
bladder cancer among a cohort of male and female hairdressers from Geneva.Int. 1. Epidemiol., 14: 549-554, 1985.
29. Anton-Culver, H., Lee-Feldstein, A., and Taylor, T. H. Occupation andbladder cancer risk. Am. J. Epidemiol., 136: 89-94, 1992.
30. Vogelstein, B.. and Kinzler, K. p53 function and dysfunction. Cell, 70:
523-526, 1992.
31. Finlay,C.A., Hinds,P.W.,Tan,T.H.,Eliyahu,D.,Oren,M.,andLevine,A. 1. Activating mutations for transformation by p53 produce a gene product
that forms an hsc7O-p53 complex with an altered half-life. Mol. Cell. Biol.,8:531-539, 1988.
32. Marks, J. R., Davidoff, A. M., Kerns, B. 1.. Humphrey, P. A., Pence, J. C.,Dodge, R. K., Clarke-Pearson, 0. L., Iglehart, 1. D., Bast, R. C., Jr., and Ber-
chuck, A. Overexpression and mutation of p53 in epithelial ovarian cancer.CancerRes., 51:2979-2984, 1991.
33. Suzuki, H., Takahashi, T., Kuroishi, T., Suyama, M., Ariyoshi, Y., and
Ueda, R. p53 mutations in non-small cell lung cancer in Japan: associationbetween mutations and smoking. Cancer Res., 52: 734-736, 1992.
34. Miller, C. W., Simon, K., Aslo, A., Kok, K., Yokota, J., Buys, C. H., Terada,M., and Koeffler, H. P. p53 mutations in human lung tumors. Cancer Res., 52:1695-1698, 1992.
35. Kondo, K., Umemoto, A., Akimoto, S., Uyama, T., Hayashi, K., Ohnishi,Y., and Monden, Y. Mutations in the P53 tumour suppressor gene in primarylung cancer in Japan. Biochem. Biophys. Res. Commun., 183: 1 1 39-1 146,
1992.
36. Brachman, 0. G., Graves, D., Vokes, E., Beckett, M., Harad, 0., Montag,A., Dunphy, E., Mick, R., Yandell, 0., and Weichselbaum, R. R. Occurrenceof p53 gene deletions and human papilloma virus infection in human head
and neck cancer. Cancer Res., 52: 4832-4836, 1992.
37. Field, J. K., Spandidos, 0. A., Malliri, A., Gosney, 1. R., Yiagnisis, M., and
Stell, P. M. Elevated P53 expression correlateswith a history of heavy smokingin squamouscell carcinoma ofthe head and neck. Br. J. Cancer, 64:573-577,1991.
38. Hollstein, M. C., Pen, L., Mandard, A. M., Welsh, J. A., Montesano, R.,
Metcalf, R. A., Bak, M., and Harris, C. C. Genetic analysis of human esopha-geal tumors from two high incidence geographic areas: frequent p53 basesubstitutions and absence of ras mutations. Cancer Res., 51: 4102-4106,
1 991.
39. Brash, D. E., Rudolph, 1. A., Simon, 1. A., Lin, A., McKenna, G, J., Baden,
H. P., Halperin, A. J., and Ponten, J. A role for sunlight in skin cancer: UV-induced p53 mutations in squamous cell carcinoma. Proc. NatI. Acad. Sci.USA, 88: 10124-10128, 1991.
40. Spruck, C. H., III, Rideout, W. M., Ill, Olumi, A. F., Ohneseit, P. F., Yang,
A. S., Tsai, Y. Y., Nichols, P. W., Horn, T., Hermann, G. G., Steven, K., Ross,R. K., Yu, M. C., and Jones, P. A. Distinct pattern of p53 mutations in bladder
cancer: relationship to tobacco usage. Cancer Res., 53: 1162-1166, 1993.
41 . Dalbagni, G., Presti, U. C., Jr., Reuter, V. F., Zhang, Z. F., Sarkis, A., Fair,W. R., and Cordon-Cardo, C. Molecular genetic alterations of chromosome1 7 and p53 nuclear overexpression in human bladder cancer. Diagn. Mol.
Pathol., 2(1):4-13, 1993.
42. Sarkis, A. S., Dalbagni, G., Cordon-Cardo, C., Zhang, Z. F., Sheinfeld, 1.�Fair, W. R., Herr, H. W., and Reuter, V. E. Nuclear overexpression of p53
protein in transitional cell bladder carcinoma: a marker for disease progres-
sion. J. NatI. Cancer Inst., 85: 53-59, 1993.
43. Cordon-Cardo, C., Finstad, C. L., Bander, N. H., Old, L. J., and Melamed,
M. Immunoanatomic distribution of cystostructural and tissue-associated an-tigens in the human urinary tract. Am. J. Pathol., 126: 269-284, 1987.
44. Banks, 1., Matlashewski, G., and Crawford, 1. Isolation of human p53-
specific monoclonal antibodies and their use in the studies of human p53expression. Eur. 1. Biochem., 159: 529-534, 1986.
45. Scorsone, K. A., Zhou, Y., Butel, J. S., and Slagle, B. L. p53 Mutationscluster at codon 249 in Hepatitis B virus-positive hepatocellular carcinomasfrom China. Cancer Res., 52: 1635-1638, 1992.
46. Vahakangas, K. H., Samet, J. M., Metcalf, R. A., Welsh, 1. A., Bennett, W.P., Lane, 0. P., and Harris, C. C. Mutations of p53 and ras genes in radon-associated lung cancer from uranium miners. Lancet, 339: 576-580, 1992.
47. Ozturk, M., and collaborators. p53 mutation in hepatocellular carcinoma
after aflatoxin exposure. Lancet, 338: 1356-1359, 1991.
48. Taylor, I. A., SandIer, 0. P., Bboomfield, C. 0., Shore, D. L., Ball, E. D.,Neubauer, A., McIntyre, 0. R., and Liu, E. ras Oncogene activation and oc-
cupational exposure in acute myeloid leukemia. 1. NatI. Cancer Inst., 84:1626-1632, 1992.
49. Addison, C., Jenkins, 1. R., and Sturzbecher, H. W. The p53 nuclearlocalisation signal is structurally linked to a p34cdc2kinase motif. Oncogene,
5:423-426, 1990.
50. Iggo, R., Gatter, K., Lane, 0., and Harris, A. L. Increased expression ofmutantforms of p53 oncogene in primary lung cancer. Lancet, 335:675-679,
1990.
51 . Thor, A. D., Moore, D. H., II, Edgerton, S. M., Kawasaki, E. S., Riehsaus,E., Lynch, H. T., Marcus, J. N., Schwartz, L., Chen, L. C., Mayall, B. H., Smith,H. S. Accumulation of p53 tumor suppressor gene protein: an independentmarker of prognosis in breast cancers. J. NatI. Cancer Inst., 84: 845-855,
1992.
52. Sommer, S. S., Cunningham, J., McGovern, R. M., Saitoh, S., Schroeder,J. J., Wold, L. E., and Kovach, J. S. Pattern of p53 gene mutations in breast
cancers of women of the midwestern United States. 1. NatI. Cancer Inst., 84:246-252, 1992.
53. Fearon, E. R., and Vogelstein, B. A genetic model for colorectal tumor-
igenesis. Cell, 61: 759-767, 1990.
54. Levine, A. The role of p53 as a tumor suppressor in human cancers. Adv.
Oncology, 8: 2-9, 1992.
55. Mazur, M., and Glickman, B. Sequence specificity of mutations induced
by benzolalpyrene-7,8-diol-9,1 0-epoxide at endogenous aprt gene in CHOcells. Cell. Mol. Genet., 14: 393-400, 1988.
56. Wang, P., Bennett, R. A. 0., and Povirk, L. F. Melphalan-induced mu-
tagenesis in an SV4O-based shuttle vector: predominance of A’T-oT.A trans-versions. Cancer Res., 50: 7527-7531 , 1990.
57. Zarbl, H., Sukumar, S., Arthur, A. V., Martin-Zanca, 0., and Barbacid, M.
Direct mutagenesis of Ha-ras-1 oncogenes by N-nitroso-N-methylurea duringinitiation of mammary carcinogenesis in rats. Nature (Lond.), 3 15: 383-385,1985.
58. Serraino, 0., Franceschi, S., Talamini, R., Frustaci, S., and La Vecchia,C. Non-occupational risk factors for adult soft-tissue sarcoma in northern Italy.
Cancer Causes Control, 2: 1 57-1 64, 1991.
59. Zahm, S. H., Heineman, E. F., and Vaught, J. B. Soft tissue sarcoma andtobacco use: data from a prospective cohort study of United States veterans.
Cancer Causes Control, 3: 371-376, 1992.
60. Akiba, S., and Hirayama, T. Cigarette smoking and cancer mortality risk
in Japanese men and women-results from reanalysis of the six-prefecturecohort study data. Environ. Health Perspect., 87: 1 9-26, 1990.
61 . Doll, R., and Peto, R. Mortality in relation to smoking: 20 years’ obser-vations on male British doctors. Br. Med. J., 2: 1525-1536, 1976.
62. Cartensen, J. M., Pershagen, G., and Eklund, G. Mortality in relation to
cigarette and pipe smoking: 1 6 years’ observation of 25,000 Swedish men.1. Epidemiol. Community Health, 41: 166-172, 1987.
63. Hsing, A. W., McLaughlin, J. K., Schuman, L. M., Bjelke, E., Gridley, G.,Wacholder, S., Chien, H. T., and Blot, W. J. Diet, tobacco use, and fatalprostate cancer: results from the Lutheran brotherhood cohort study. CancerRes., 50: 6836-6840, 1990.
64. Hsing, A. W., McLaughlin, J. K., Hrubec, Z., Blot, W. J., and Fraumeni,J. F. J. Tobacco use and prostate cancer: 26-year follow-up of US veterans.
Am. J. Epidemiol., 133:437-441, 1991.
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1994;3:19-24. Cancer Epidemiol Biomarkers Prev Z F Zhang, A S Sarkis, C Cordon-Cardo, et al. in early stage bladder cancer.Tobacco smoking, occupation, and p53 nuclear overexpression
Updated version
http://cebp.aacrjournals.org/content/3/1/19
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/3/1/19To request permission to re-use all or part of this article, use this link
on July 21, 2021. © 1994 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from