-
8/14/2019 TORCH Screening: Time for Abolition?
1/4
TORCH screening: time for abolition?W . L. Lim and D. A.
Wong
AbstractThe acronym TORCH (toxoplasma, rubella, cytomegalovirus,
herpes simplex virus) was intro-duced to highlight a group of
agents which cause congenital and perinatal infections.
TORCHscreening is now widely requested by clinicians investigating
suspected cases of congenital an dperinatal infection. There is
concern that such requests ar e inappropriate and requests fo r
inves-tigation should be targeted more specifically. The prevalence
of TORCH infect ions in HongKong are examined in this study.
Toxoplasmosis is a rare infection in Hong Kong with aseropositivity
rate of only 2.4% amo ng wom en of child-bearing age; 87.5% of
women of child-bearing age are already seropositive for
cytomegalovirus (CM V) and therefore m ost cases ofcongenital CM V
infection are l ikely to result from maternal reinfection which
carries a muchlower risk of severe congenital abnormalities.
Congenital rubella infections still occur each yearin small num
bers. N eonatal herpes simplex virus (HSV ) infection is very rare
inHong Kon g. It isapparent that requests fo r TORC H screening has
been over-ordered and clinicians should beencouraged to send ap pro
priate specimens for spec ific tests depending on the clinical fe
atures ofth e individua l case.K e y w o r d s : TORCH;
Seroprevalence; Con genital infections
IntroductionTh e acronym TORCH was int roduced in 1971 byNahmias
et al. to highlight a group of agents whichaffect th e foetus an d
newborn, namely Toxoplasmagondii, rubella virus, cytomegalovirus
(CMV), an dherpes simplex virus (HSV).1 These ag ents often
pro-vide a similar clinical picture which include one ormore of the
following clinical signs: low birth weight,prematur i ty , purpura
, jaundice , anaemia , micro-c e p h a l y / h y d r o c e p h a l
y , c e r e b r a l ca lc i f i ca t ion ,c h o r io r e t i n i t
i s , c a t a r a c t s , m i c r oph t ha l mi a , a ndpneumonitis
. TORCH screening is now widely re-ques ted by c l in ic i ans
inves t iga t ing infant s andpr e gna n t wome n fo r c onge n i t
a l , pe r i na t a l a n dneonatal infections. There is concern
among micro-biologists that such requests are often inappropr ia
tean d that resources would be better utilized if requestsfor
investigation were targeted mo re specifically2. W edecided to
conduct a study in order to assess thefrequency of congenital TORCH
infections in HongKong.
Virus U nit , Queen Mary Hospital , Pokfulam , Hong KongW . L.
Lim, MRCP ath, FRCPAD. A. W ong , MB , ChB, M ScCorrespondence to:
Dr D . A. W ong
Patients and specimensAll requests fo r toxoplasma serology,
whether as par tof th e TORCH screen or otherwise, were docume
nted,as were al l requests for CMV antibody status for theperiod
from 1 July 1992 to the 30 June 1993. All re-quests for toxoplasma
serology were initially testedfor specific IgG by indirect immu
nofluorescence an dpaired sera were requested to detect rising
antibodytitre. Those wit h a titre of 80 or greater were tested
forthe presence of specific IgM by immunofluorescence.Th e
seroprevalence rate fo r women of child-bearingag e were compiled
from TORCH requests taken fromwomen who presented with ma ternal il
lness, intrau-terine growth retardation, abortion, prema ture ru
ptureof membrane (PROM) and foetal distress. Sera fo rCM V antibody
status were first screened for the pres-ence of CMV antibodies by
complement fixation tests.Those which were negative by com plement
fixationtest were retested by enzyme-linked immunosorbentassay
(ELISA) (Behring) for the presence of specificIgG. All requests for
CMV cul ture fo r urine, salivaand throat swabs collected from
neonates less th an 14days old were documented over the same
period.Diagnosis o f rubella infection was made when thereis a r is
ing ant ibo dy t i t re de tec te d by h aem ag-glu tina tion
inhibition tests and tha t specific IgMantibody is detectable by
ELISA (Abott an d Pasteur).
306
-
8/14/2019 TORCH Screening: Time for Abolition?
2/4
Lim & Wong: TORCH screening 307
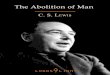
Table 1. Toxoplasma serology requests (1 July 1992 to 30 June
1993).Clinical presentation No. PosIUGR/SGA/LBWlUD/AbortionNeonatal
symptomsPrematurityPROM/leakage/foetal distress/preterm
labourMaternal fever and illnessPostnatal symptomsBone marrow
transplantAML/NHL/other haematological conditionsHIV+veOthers/no
details availableTotalWomen of child-bearing age
IUGR Intrauterine growth retardationSG A Small for gestational
ageLB W Low birth weightIUD Intrauterine deathPROM Premature
rupture of membraneAML Acute myeloid leukaemiaNHL Non Hodgkin's
lymphoma
31024 54931437933
20613741
162237
2086667
6810320
1122
15137216
1.933.262.022.092.5305.331.454.879.255.483.452.40
Herpes simplex virus infection is diagnosed by virusisolation. A
search was carried out on our positiverecord files for the years
1986 to 1992 for cases ofconfirmed congenital rubella an d neonatal
herpessimplex virus infection.
were sy mp tom atic adults. 1,303 (62.5%) were requestsfor TORCH
screening of which only 29 (2.22%) sam-ples had IgG antibody
against toxoplasma, none ofwhich ha d current infection. The
seropositivity rateamong women of child-bearing age was 2.4%.
ResultsToxoplasmosisFor the period from 1 July 1992 to 30 June
1993, theVirus Unit received requests fo r toxoplasma
antibodytesting from 2,086 patients (Table 1). Only 72 (3.45%)were
positive for IgG antibody against toxoplasmawhich is indicative of
past infection. IgM antibodieswere dem onstrated in only two
patients both of whom
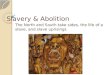
Table 2. Requests for CMV isolation from neonates lessthan 14
days of age (1 July 1992 to 30 June1993).
Clinical presentation Total no. PosIUGR/SGA/LBWNeonatal
symptomsPrematurityPROM/leakage/foetal distress/preterm
labourOthers/no details available
16623 113416
165
2411
2Total 712 10
Cytomegalovirus i n f e c t i o nFor the period from 1 July 1992
to 30 Jun e 1993, therewere 953 requests for CMV serology of which
887(93.1%) ha d demonstrable CMV antibodies, whichshows that Hong
Kong has a high prevalence of CMVinfection. 161 out of 184 (87.5%)
specimens taken fromwome n of child-bearing age (16-40 years) were
posi-tive for CMV antibodies. Over th e same period, urine,saliva
or throat swabs specimens were received from712 neonates less than
14 days old for CMV isolation(Table 2). Only 10 (1.4%) were
positive for CMV bythe CMV DEAFF test. Ho w many, if any, of
theseinfants had cytomegalic inclusion disease was notknown.
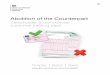
Serological testing for CMV antibodies usingcomplement-fixation
tests were carried out on sevenof these infants (Table 3), only in
one case (patient4)was a significan t rise in CMV antibody titre
demon-strated.RubellaA small num ber of infan ts with congen ital
rubellasyndrome are born each year (Table 4). For the periodfrom 1
July 1992 to 30 June 1993, of the 4,145 reque stsfor rubella
antibody testing by haemagglutination-
-
8/14/2019 TORCH Screening: Time for Abolition?
3/4
308 J Hong Kong Med Assoc Vol. 46, No. 4, December 1994
Table 3. Serological results (by complement-fixationtests for
CMV antibodies ) and clinical cond itionof the 10 neonates who we
re excreting CMV intheir urine within 14 days of birth.
CMV antibody titresPatient 1st titre 2nd titre Clinical
condition12345678910
10
-
8/14/2019 TORCH Screening: Time for Abolition?
4/4
Lim & Wong: TORCH screening 309
t h a t 90% of nulliparous women and 93% of multipa-rous women
of child-bearing age were positive ofrubella antibody.7 This showed
tha t despite the im-p l e m e n t a t i o n of selective rubella
vaccination inpr imary six school girls in 1978 and the extension
ofimmunization to postpartum women who are foundto be seronegative
while attending antenatal clinics,asizable percentage of women of
child-bearingag e werestill susceptible to rubella infection.
Therefore it is ofutmost importance that all women are
immunizedagainst rubella. A ll suspected contacts with rubella,or
any clinical symptoms of rubella infection in preg-nancy should be
investigated by rubella serology.From our data, neonatal herpes is
not an importantproblem in Hong Kong. Neonatal herpes is best
diag-nosed by the virus culture of specimens taken fromaffected
sites such as vesicle fluid, saliva, mouth swabsand CSF rather than
by serology.2To conclude, with th e exception of rubella,
TORCHagents are not as common a cause of congenital infec-tion in
Hong Kong as in other developed countries.W e feel that th e test
had been over-ordered. The con-cept of a common presentation of
congenital infection(TORCH syndrome) and a common investigativep a
t h w a y (TORCH screening) should be actively dis-couraged.
Instead, clinicians should be encouraged tosend specimens fo r
specific tests depending on theclinical features of individual
cases. For example,cataracts and cardiac lesions are common in
congeni-ta l rubella but not with any other TORCH agent:cerebral
calcification is extremely rare in rubella and
is only widely distributed in toxoplasmosis: deafnessis
associated only with rubella and CMV infect ion.Thus appropriate
samples such as urine, saliva andvesicle f lu id should be cultured
for CMV and HSV inthe case of suspected congenital CMV or HSV
infec-tion. Neonatal sera are useful for the diagnosis ofcongenital
rubella and toxoplasma infection, but oflittle value in the
diagnosis of neonatal CMV an dHSV infections.
References1. N a h m i a s A J, Josey W E , Naib Z M , Freeman M
G ,Fernandez RJ, Wheeler JH . Perinatal risk associatedwith
maternal herpes simplex infection. Am J OhstetGynecol 1971; 110:
825-37.2. Public Health Laboratory Service. TORCH
screeningreassessed. London: PHLS, 1990.3. Ludlam G B, Wong KK,
Elaine Field C. Toxoplasmaantibodies in sera from Hong Kong. J Hyg
Camb 1969;67: 739-41.4. Hal l S. Congenital toxoplasmosis. BMJ
1992; 305: 291-7.5. Fowler KB , Stagno S, Pass RF, Britt NJ, Boll
TJ , A lfo rdCA. The outcome of congenital cytomegalovirus
infec-tion to mate rna l an t i body status. N Engl J Med 1992;326:
663-7.6. Stagno S, Whitley RJ . Herpes infec t ions of
pregnancy,
part I: cytomegalovirusand Epstein-Barr virus infec-tions. N
Engl J Med 1985; 313: 1270-4.7. Lim WL. Seroimmunity to measles,
mumps, rubel laand poliomyelitis in Hong Kong. Hong KongJ Paed i a
t r1992; 1: 34-40.