Embed Size (px)
Citation preview

TRANSACTIONS OF THE ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENE (1993) 87, 201-206 201
Towards optimal regimens of parenteral quinine for young African children with cerebral malaria: the importance of unbound quinine concentration
Peter Winstanley 1a2,3, Charles Newton1>2, William Watkins ‘a3, Edward Mberu’, Steven Ward1>3, Peter Warnl,*, Isiah Mwangi’, Catherine Warui&, Geoffery Pasvo11>2, David Warrel11a2 and Kevin Marsh1>2 ‘Kenya Medical Research Institute, Kilifi Unit, P.O. Box 428, Kilifi, Kenya; ‘Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK; 3Department of Pharmacology and Therapeutics, University of Liverpool, Liverpool, UK
Abstract Young African children with severe malaria are given quinine using a regimen designed for Thai adults. We measured quinine in the blood, plasma and Dlasma water of young children in Kenva after ranid intravenous and intramuscular dosing, and- calculated the therapeutic-range of unbound qiinine. T&e peak plasma quinine concentration after rapid intravenous dosing was 12.3k3.7 mg/L (mea&SD), 43% higher than in adults given the same regimen previously; this was due to a smaller apparent volume of distribution in the children. The therapeutic range of unbound quinine was calculated as 0.2-2.0 mg/L. Simulations of un- bound quinine were made for the standard quinine regimen: unbound drug concentrations rose above the therapeutic range after each dose. The possible risks of quinine-induced visual impairment are discussed. Alternative, lower dose regimens for young African children with severe malaria are described.
Introduction The mortality of cerebral malaria in young children re-
mains 10-40% (WARRELL et al., 1990) and attempts to reduce this figure must include the early and optimal use of quinine. More than 90% of global malaria-related mor- tality occurs in young African children and yet there is no clear consensus on the use of quinine in this popula- tion. Currently used regimens are generally based on data derived from non-immune -adult populations (WHITE et al., 1982, 1983a, 1983b; PHILLIPS et al., 1986; WATTANACOON et al., 1986; DAVIS et al., 1988), but this is not ideal since quinine disposition probably varies with age (SABCHAREON et al., 1982; SHANN et al., 1985) and the chemosensitivity of Kenyan strains of Plasmodium falciparum to quinine is probably greater than that of strains in Thailand (SUBSAENG, 1986). We wanted to de- sign quinine regimens for children with severe malaria which would be practical for African hospitals, and yet achieve therapeutic quinine levels as rapidly as possible. We have addressed 3 areas: first, we have studied the dis- position of quinine in young children with severe malaria in sufficient detail to allow statistical comnarison with published data from adults; secondly, we have defined the drug’s approximate local therapeutic range; finally, since the concentration of the unbound fraction of qui- nidine, the optical isomer of quinine, falls at high pH (BRORS et al., 1984), and pH rises in stored samples of plasma, we have studied the effect of pH on the protein binding of quinine. Using computer simulations, based on compartmental models of our data, we have designed improved quinine regimens for young children.
Methods Clinical studies
Patients. Approval for the study was given by the Ethics Committee of the Kenva Medical Research In- stitute. Children with P. faliiparum parasitaemia ad- mitted to Kilifi District Hospital, Kenya, were given par- enteral quinine if they were unable to localize pain (i.e., had cerebral malaria), or were unable to drink and sit be- cause of impaired consciousness (‘prostrate’). Patients were excluded if written consent was refused, if quinine had already been given, or if systolic blood pressure was below 70 mm Hg. Hypoglycaemia was corrected and seizures. of >5 min duration were treated with in- travenous (i.v.) diazepam (0.3 mgikg). The stomach was emptied by nasogastric tube in most patients, and pyre- xia was treated with rectal paracetamol and tepid spong- ing.
Address for correspondence and offprint requests: Dr P. A. Winstanley, Department of Pharmacology and Therapeutics, University of Liverpool, P.O. Box 147, Liverpool, L69 3BX, UK.
Dosing and sampling. (i) Intravenous dose. Quinine di- hydrochloride (Paris Chemicals: 300 mg, 500 pL) was diluted 1:l (v/v) with normal saline; the calculated dose (4.0 mg of the salt/kg body weight, equivalent to 3.33 mgikg of the base) was transferred to a 10 mL syringe and further diluted to 8.0 mL with saline. This was then injected manually into the side arm of the drip over exactly 4.0 min, as described by DAVIS et al. (1988). Exactly 60 min after the start of the bolus dose, an i.v. infusion of quinine dihydrochloride (10 mgikg in 20 mL normal saline) was given by electronic infusion pump over 2 h. Thereafter, quinine (10 mgikg over 2 K) was eiven at 12 h intervals to a minimum of 4 such infusions: &al quinine sulphate (10 mg/kg) was given 12 h there: after. Blood for quinine estimation (200 yL) was drawn from an indwelling Teflon@ cannula after removal of dead space (1.0 mL; returned after withdrawal of sample). Samples were collected before dosing and at the following times after the start of the injection: 2, 4, 5, 6, 7, 8,9, 10, 12, 14, 16,30and45 min; 1,2, 3,4, 5, 7,9 and 13 h. Blood (200 yL) was also drawn before and upon completion of each subsequent i.v. infusion, and ?, 4, 5, and 12 h after the start of the last infusion. In addl- tlon, plasma (1.0 mL) was saved for measurement of total and unbound quinine at the following times: 4 and 60 min; 3, 7, 15, 27, 39 and 49 h. Plasma was saved for measurement of albumin (ALB) and al acid-glycoprotein (AAG) before the start of treatment, and AAG was also measured 48 h after the start of treatment.
(ii) Intramuscular dose. Quinine dihydrochloride (20 mg of the salt per kg) was divided equally between 2x5 mL syringes, and diluted 1:5 (v/v) with water for injec- tions. The two halves of the dose were given simulta- neously by deep intramuscular (i.m.) injection into both anterior thighs. Thereafter,, quinine (10 mgikg) was given 12 hourly (initially 1.m. into alternate anterior thighs, but by mouth as soon as possible). Blood (200 uL) was drawn from a Teflon@ cannula at the following &es: 0, 1, 2, 3, 4, 5, 10, 15, 30, 45, 60 and 90 mins; 2”, 4,6 and 12 h.
Assays. Blood for quinine estimation was taken into li- thium heparin tubes, aliquots were transferred to filter paper strips, the remainder was centrifuged (1000 g, 10 min), and plasma was stored at -70°C. Plasma water was obtained using the centrifugation dialysis method of MANSOR et al. (1991). Blood, plasma and unbound quinine concentrations were measured by high perfor- mance liquid chromatographv (HPLC) (MBERU et al., 1991). Plasma chloroq&e <ai mea&dd by enzyme: linked immunosorbent assav (SHENTON et al.. 1988). ALB and AAG were measuied by immunodiffusidn (NOR-Partigen@; Behringwerke, Germany).
Compartmental modelling and simulation. Data were fitted to open models using a non-linear regression pro-

202
gram (Topfit@; Schering, Germany); goodness of fit was determined bv the Aikake test, and the principle of parsi- mony was applied. Distribution half-time- (tt& was derived from data following the i.v. bolus dose, but an- other quinine dose was needed after 1 h, and ehmination half-time (t& was therefore derived from data collected 3-13 h after the first i.v. infusion. Because of the exten- sive change in kinetics over the 49 h sampling period simulations of ‘new’ regimens were based on models which used data from all 5 quinine doses.
Determination of unbound quinine in vitro by the microtest at 3 concentrations of al acid-glycoprotein
In previous work, the 99% inhibitory concentration (I&) of quinine against local strains of P. falciparum was found to be 0.89 mg/L (PASVOL et al., 1991) in children whose wean plasma AAG concentration was 2.21-0.8 g/L (unpublished data). However, conditions of parasite drug exposure in vitro differ considerably from those in vivo: diluted blood presents a changed ratio of free/bound drug to the parasitized erythrocyte because of the difference in AAG concentration. This can be over- come by determination of the unbound drug concentra- tion in vitro, at the I&.
AAG was added to whole blood taken from a healthy volunteer at 3 differing AAG concentrations; final plasma AAG concentration was measured in each. Blood was diluted (1: 10, v/v, with RPMI-1640iHEPEsibicarbonate) to simulate conditions in the microtest (RIECKMANN et al., 1978), but using final volumes of 1 mL rather than 50 uL to urovide masses of unbound QN above the limit of hete&on of the HPLC assay. Polypropylene tubes (Sterilin, UK) were dosed with quinine in ethanolic solu- tion, the solvent was evaporated under N2, and quinine was re-dissolved bv the addition of diluted blood to pro- duce the same co&entrations as used in the microtest. After reconstitution, tubes were incubated overnight (37”C, in an atmosphere of 3% CO?, 5% 02, 92% N2). Supernatant from each tube was dlalysed as described above, and unbound quinine in the filtrate was measured by HPLC.
Protein binding studies in vitro The effect of pH on the association constants (&) of
quinine for the individual proteins, AAG (human; Sigma, UK) and ALB (bovine, fraction V; British Drug Houses, UK), was studied by incubating the drug (l-10 mg/L) for 15 min in phosphate buffer (40 mM) at room temperature with AAG alone (0.5, 2.0, and 5.0 g/L) or ALB alone (29 g/L), pH was checked after the addition of the protein. Aliquots (100-300 pL) were dialysed in triplicate, as described above; the filtrate was assayed for quinine, the same day, by HPLC.
The effect of pH on the unbound fraction of quinine (fQNu) in a solution containing both AAG and ALB was studied by incubating the drug (1-316 mg/L) for 15 min in phosphate buffer (40 mM; pH 7.0 or 7.4) with ALB (30 g/L) and AAG [0.5, 2.0 and 5.0 g/L). Triplicate aliquots were handled as above.
Calculations and statistics K, was calculated for the equation K,= [Db]/[Du] [PI,
where rDhl=concentration of protein-bound drug, [Du]=co&ntration of free drug, grid [P]=protein co& centration.
First-dose kinetics after i.v. dosing were compared with those of DAVIS et al. (1988), and absorption half-life (tl/&,tJ after i.m. dosing was compared with the estima- &o&of WATTANAGOON et al. (1986) and WALLER et al. (1990) bv the Mann-Whitnev U test: the same test was ised to Compare first-dose &d final-hose kinetics in the present study. AAG concentrations in the present study were compared with those of SILAMUT et al. (1991) by Student’s t test, which was also used to assess the effect of AAG concentration on fQNu in the microtest.
Results Clinical studies
Patients. Twelve children (all with cerebral malaria) re- ceived i.v. quinine and 10 (6 with cerebral malaria and 4 prostrate) received i.m. quinine (Table 1); 2 children had
Table 1. Admission characteristics of children in the study”
Number Age (months)
Route of quinine administration Intravenous Intramuscular
12 10 36.4? 18.4 (7-77) 38.3i22.4 (l&82)
Blantyre coma SCO& 5 0 0 4 0 2 3 0 0 2 6 6 1 4 2 0 2 0
Haemoglobin (g%) 6.3k2.2 8.2i1.9 Parasite counf (Per lc 216 272 144 a77
(19 600-2 708 200) (9600-l 586 700)
“Mean *standard deviation (ranges in parentheses). bM~~~~~~ et al. (1989).
intercurrent septicaemia. There was no significant change in mean arterial pressure and no episode of hypo- glycaemia or arrhythmia in the 60 min after i.v. or i.m. quinine. Three children died (2 after i.v., and 1 after i:m., quinine, 1, 2 and 12 h after the start of treatment). Four children. all of whom had received i.v. auinine. had neurological sequelae (including athetosis, hiplegia and hemiparesis), and 3 of these had visual impairment. All the survivors cleared parasitaemia without recrude- scence. Plasma chloroquine was measured on admission in 13 of 22 patients and ranged from undetectable to 776 PgiL. Plasma albumin was 28.9’16.7 g/L (mean&SD); plasma AAG was 2.48kO.58 g/L (range 1.63-3.23) be- f$; treatment, and 2.1340.46 g/L (range 1.68-3.05) at
Quinine pharmacokinetics. (i) After i.v. injection, blood quinine concentrations followed a bi-exponential decline, and were best fitted to a 2 compartment model. Peak plasma concentrations ranged from 6.6 to 18.2 mg/L (12.2k2.9 mg/L), and were seen 4 min after the start of the injection in 7 children and 5 min after the start in the remaining 5. After the first quinine infusion, peak plasma concentrations ranged from 11.0 to 19.1 mg/L (13.8k3.1 mg/L). The plasma:blood concentration coef- ficient was 1.08. Derived (plasma) pharmacokinetic
Table 2. Pharmacokinetics of plasma quinine following intravenous injection of 4.0 mg/kg over 4 min, followed by intravenous infusion of 10 mgikg over 2 h
Patient no.
: 3
t a ha
0.19 0.30 0.05
v,b t c v,d Cl’ hz
0.22 0.29 15.1 15.9 0.46 0.47 0.42 0.43 nd nd nd nd
0.17 0.25 10.8 0.58 0.67 0.37 0.25 i7.0 0.35 0.32 0.07 0.16 10.5 0.31 0.36 0.52 0.26 22.0 0.34 0.31
i 0.18 0.08 0.23 0.18 10.9 . 3z
0.49 0.42 0.68 0.39 10 0.71 0.51 0.61 0.42
::. 0.05 0.31 oz7 13.4 nd o?o 0?6 Mean 0.24 0.27 16.4 0.45 0.45 SD 0.20 0.10 8.8 0.10 0.13
“Distribution half time (h). bApparent volume of the central compartment (L/kg); nd=not determined.
‘Elimination half time (h); nd=not determined. dTotal apparent volume of distribution (L/kg); nd=not deter- mined.
‘Clearance (mLimin/kg); nd=not determined.

203
of quinine against local strains of P. falciparum, in child- ren whose mean plasma AAG concentration was 2.2kO.8 g/L, was previously found to be 0.89 mg/L, the unbound quinine concentration in vitro at the IC99 was (0.2 mg/L.
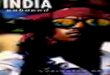
Fig. 1. Association constants (X 106imol) of o(t acid-glycoprotein (AAG) and albumin (ALB) for quinine (QN) at different pH. Closed triangles: [AAG]=O.5 g/L, [QN]=l.O mg/L; open squares [AAG]=2,0 g/L, [QN)=4.0 mg/L; open circles [AAG]=5.0 g/L, [QN]= 10.0 mg/L; closed squares: (ALB)=29,0 g/L, [QN]=lO,O mg/L. Means plus or minus I standard deviation are shown.
values after the first quinine dose are given in Table 2. fQNu did not vary significantly over time, and was 0.09*0.04 (66 estimations). Unbound quinine concen- trations ranged from 0.18 to 4.0 mg/L.
In 7 children it was possible to compare total apparent volume of distribution (I’d), plasma clearance (Cl) and elimination half-life (tt& between the first and fifth quinine doses. I’d rose during treatment from 0.45+0.01 to 1.54kO.60 L/kg (P=O.O02), Cl rose from 0.4820.14 to 1.38kO.49 mL/min/kg (P=O.O02), while tl/zz was not significantly different (13.8k6.5, vs. 11.311.8 h; P=O.48).
(ii) After i.m. injection, the data best fitted a one com- partment model. Quinine was detectable one minute after dosing; tl/Zabs ranged from 3.0 to 25.8 (8.717.8 min), achieving a maximum concentration (C,,,) in plasma of 15.7k3.1 mg/L at 1.6k1.7 h (range 0.25-6.0 h).
Therapeutic concentration of unbound quinine in vitro The plasma AAG concentration in undiluted blood
from a healthy subject was 0.7 g/L before addition of AAG (sample l), and was 0.9 (sample 2) and 1.6 g/L (sample 3) in samples to which AAG had been added. The fQNu in culture medium fell from 0.41+0.10, in medium containing blood sample 1, to 0.3 1 i 0.10 in me- dium containing sample 2 (P=O.O8) and 0.25 F0.03 in medium containing sample 3 (P=O.O02). Since the IC99
QUININE (mg/L)
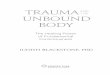
Fig. 2. Change in unbound fraction of quinine with variation of total quinine concentration, pH and concentration of at acid-glycoprotein (AAG). Albumin concentration=30 g/L in all experiments. Solid lines: [AAG]=O.5 g/L; closed circles: pH=7.4, open circles: pH=7,0; dashed lines: [AAG]=2,0 g/L; closed squares: pH=7.4, open squares: =7.0; dotted lines: [AAG]=5.0 g/L; closed triangles: pH=7.4, open triangles: pH=7,0. Means plus or minus 1 standard deviation are shown.
The effect of pH on plasma protein binding in vitro Quinine bound more avidly to AAG than to ALB (Fig.
1). Irrespective of protein concentration the relationship between pH and Ka for AAG was hyperbolic (Fig. l), being maximal at c. pH 7.4, falling to nadir at c. pH 7.0 and rising again by c. pH 6.8. No such relationship was seen with ALB. When incubated with AAG and ALB simultaneously, fQNu rose in an asymptotic manner which was influenced markedly by AAG concentration and, at low AAG concentration, also by pH (Fig. 2).
Simulation of improved dose regimens in vitro The aim of simulation was to derive regimens which
rapidly achieved unbound quinine concentrations within the therapeutic range, but which would be practical for clinical use. One i.m. and 2 i.v. regimens are described in Table 3, and their simulated unbound quinine profiles are contrasted with that of the standard regimen in Fig. 3.
Discussion Quinine is the only available drug consistently effec-
tive for life-threatening falciparum malaria in East Af- rica. Quinine is active against the pathogenic sequestered forms of P. falciparum and therapeutic concentrations should be achieved as early as possible. There has been considerable controversy over the merits of starting ther- apy with a loading dose of quinine, but the practice is now widely accepted. Proving a clinical advantage for loading doses is likely to remain impossible because of ethical and logistic difficulties, but some data are sugges- tive of an advantage (WHITE et al., 1983; PASVOL et al., 1991), and the concept is theoretically sound. In the management of young children with cerebral malaria the main questions are: what is the therapeutic range? and what regimen achieves concentrations within this range fastest? Given the high frequency of lactic acidosis in cerebral malaria, and the importance of plasma protein binding (particularly to the acute-phase protein AAG) in determining quinine disposition (SILAMUT et al., 1985, 1991; MANSOUR et al., 1990, 1991) and activity in vitro (B. C. Ellford & R. A. Pinchers,, personal communica- tion), a further question of practical importance is: does pH effect the protein binding of quinine?

204
-___--------------- 0 r-
0 12 24 36 42
3-f 4
2 J. - - - - - - - - - - - - - +Ly _
0 12 24 36 46 0 12 24 36 46
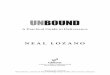
Fig. 3. Simulations of unbound quinine concentration vs. time curves with three intravenous and one intramuscular dosing regimen. The dashed lines represent the upper and lower limits of the therapeutic range as derived in the text; the dotted lines represent 95% confidence limits. Regimen 1: 20 mg/kg quinine dihydrochloride over 4 h Regimen 2: 15 mgikg over 2 h intravenously, followed by 10 mgikg over 2
intravenously, followed by 10 mgikg over 2 h, 8 hourly. h, 12 hourly. Regimen 3: 7.5 mgikg over 0.5 h intravenously,
followed immediately by 7.5 mgikg over 1.5 h and by 10 mgikg over 2 h, 12 hourly. Regimen 4: 15 mgikg intramuscularly (diluted 1:5 and given into both thighs), followed by 10 mgikg 12 hourly (into alternate thighs).
Table 3. Recommended quinine regimens
A. Intravenous administration (no burette) Loading
dosea 15
Maintenance ’ dosea Volumeb DurationC Frequencyd
10 10 2 12
B. Intravenous administration (burette available) Fast loading Continuation
dosea Volumee DurationC loadil;g5 dosea Volumeb 7.5 20 0.5
Maintenance doses size, volume, duration and frequency as in previous schedule (as.
Duration’ 1.5
C. Intramuscular administration Loading Maintenance
dosea dosea Frequencyd 15 10 12
All doses to be diluted 1:5 (v/v) with water for injections; loading dose to be given half into each anterior thigh; maintenance doses to be given into alternate thighs.
“Quinine dihydrochloride (mg of the salt per kg body weight). bDextrose (5% or 10%) or dextrose (4%) in saline (0.18%); volume (mL/kg) remaining in infusion bag (after wasting the balance) to which drug should be added.
‘Duration of infusion (h). dtime between doses (h). eTotal volume (mL) in burette or infusion pump.
Chemosensitivity testing of quinine in vitro is limited BOWMAN et al., 1985; DYSON et al., 1985), and becomes in the estimation of its therapeutic range mainly because a problem at total plasma quinine concentrations above of the unphysiologically low AAG concentration in cul- 10 mg/L. These data are not directly comparable with ture medium. The ICaa of total quinine against 60 iso- those from patients with malaria because of the disease- lates of P. falciparum from Kilifi was 0.89 mg/L (PASVOL induced rise in AAG concentration. However, if un- et al., 1991), but the closest possible estimate of desired bound quinine is assumed to be identically toxic in health drug concentrations in vivo is probably given by express- and malaria (a reasonable assumption), and if metabolites ing chemosensitivity in vitro as unbound drug concentra- are not incriminated in toxicity (there is no evidence that tion. Using the data on the fQNu in the microtest from they are), then an approximate threshold of toxicity can the present study, the mean 99% effective concentration be estimated. In health quinine is 20% unbound in the for unbound quinine in Kilifi district is about 0.2 mg/L. plasma (MIHALY et al., 1987), so that oculotoxicity is un- The unbound quinine level, above which serious, con- likely to occur at unbound quinine concentrations below centration-dependent toxicity becomes a risk, cannot be 2.0 mg/L. Combining the estimates of fQNu concentra- estimated with accuracy but can be approximated from overdose data. Oculotoxicity is the commonest serious
tions required for efficacy and toxicity gives an approxi-
problem after deliberate overdose (BATEMAN et al., 1985; mate thereapeutic range for the unbound drug of 0.2-2.0 mg/L .

205
In the present study, after i.v. administration of rela- tively low quinine doses (14 mgikg loading, and 12 hourly 10 mgikg maintenance doses), unbound quinine concentrations exceeded 0.2 mg/L throughout treatment in all but 2 patients (in whom &bound quinine concen- trations of 0.18 and 0.19 mrriL were measured 60 min after the bolus injection). &bound quinine concentra- tions exceeded 2 mg/L in only 5 of 66 samples. The fQNu in the present study (0.09+0.04) was higher than that reported by SILAMUT et al. (1991) in non-immune adults with cerebral malaria (0.055+0.024; P=O.O5) des- pite the fact that AAG concentrations in our study were higher (2.48kO.58 vs. 2.06kO.53 g/L; P=O.O5). How- ever, given the effect of pH on the binding of quinine to AAG (discussed below), and since SILAMUT et al. (1991) did not control pH during dialysis, their fQNu values may have been artefactually low, especially at lower AAG concentrations.
Whole plasma quinine concentrations in the present study were higher than those reported by DAVIS et al. (1988), who studied non-immune adults, and pharmaco- kinetic data differed. In the present study tl/Za (14.9k12.2 min) was longer than in adults (2.3k3.2 min; P=O.OOl), and Vd was smaller (0.45t0.13 vs 0.71kO.37 L/kg; P=O.O2). Values for tluz and the apparent volume of the central compartment (V,) did not differ between the populations (P=O.43 and 0.11 respectively). It is not clear why quinine disposition in children differed from that in adults, though it has been noted before, and may result from the higher concentrations of AAG seen in these children compared with those in adults.
The main aim of this study was the assessment and op- timization of quinine usage in African children; we have therefore used our data to simulate the performance of 4 regimens that have been considered practical. The ‘standard’ regimen for childhood cerebral malaria in much of Africa comprises a larger loading dose than in the present study (20 vs. 14 mgikg) plus maintenance doses every 8 h instead of every 12 h; unbound quinine concentrations certainly exceed those measured here, and are simulated in our 12 children in Fig. 3. Unbound quinine concentrations above the therapeutic range are simulated after every dose. No prediction can be made from this simulation of the risk of oculotoxicity from the ‘standard’ regimen, but current recommendations for the use of narenteral quinine in childhood cerebral malaria need td be reassessed. Blindness following treatment of cerebral malaria with quinine is almost invariably associ- ated with other neurological defects and probably results mainly from the disease rather than the drug. However, blindness due to, or exacerbated by, quinine is thought to occur in patients with malaria (RHEEDER & SIELING, 1991) and detailed studies into the causes of blindness in children who have recovered from cerebral malaria are now needed.
Clearly, the constraints on the use of quinine vary, and we have-therefore presented, in Table 3-(see also F&. 3), dose regimens which would be suitable for a varietv of settings-in Africa. This emphasis on practicality means that, although frequent small doses would produce less variation in concentration, 12 hourly dosing is preferable to reduce clinical work-load. Furthermore, neither infu- sion pumps nor burettes are routinely available in most hospitals; quinine is usually added to a residual volume of i.v. fluid in the bag after wastage of the excess. Regimen A in Table 3 takes account of this; in occasional units both burettes and infusion pumps are available making rapid loading doses practical, as set out in regimen B .
The i.m. administration of quinine has been reassessed in recent years, and it has been given undiluted into one site at 20 mg/kg (WATTANAGOON et al., 1986), diluted in water and given into one site at 10 mgikg (final concen- tration 60 mg/mL) (MANSOR et al., 1990), left undiluted but given into 2 sites (WALLER et al., 1990), and finally both diluted and given into 2 sites as we have done, at 20
mgikg (final concentration 120 mg/mL). The last regimen achieved a mean tl/Zabs of 8.7k7.8 min, which is faster than administration undiluted into either one site Inn.n&lr.n . . . . n-n.nn,\ IWInTTr%rrnr\nrr ^f -7 1986), or 2 sites-(37225 min;‘P=O.OOOl) (WALLER et al., 1990) and probably results from the greater surface area of the dose after injection. However, tl/Zabs after i.m. administration of diluted drug ranged from 3.0 to 25.8 min in this study and Cm, Fanged from 11.2 to 19.3 mg/L. WALLER et al. (1990) found similar variation in abiorption, with tl/zabs ;ang&g from 0.19 to 1.55 h, and Cmax ranging from 4 to 25.9 mg/L. None of the children in the present study was shocked (systolic pressure ranged from 82 to 140 mm HE and diastolic nressure from 0 to 70 mm Hg) and there was no correlation be- tween blood pressure or skin temperature and tl/tabs. Given the variation in its rate of gbsorption (whether diluted or not) and the risk of sensis (esneciallv when dis- posable needles are unavailable) i.;. idministration of quinine is preferable. However, in poorly equipped pe- ripheral health centres i.v. drug administration may be hazardous, and in such situations quinine should be given by the i.m. route as outlined in Table 3 (regimen C).
The unbound fraction of quinidine in normal serum falls as pH rises (BRORS et al., 1984); and since the pH of stored plasma is about 8.5 we were concerned that the same effect might be relevant to assay for unbound quinine. We have shown that the relationship between quinine-AAG binding and pH is hyperbolic; this is prob- ably due both to pH-induced conformation transition of AAG, as has been described for ALB (KREMER et al., 1988), and ionization of quinine (HENRY et al., 1981). Consequently, the pH of stored plasma is a potential source of artefact in unbound quinine assays; pH should be adjusted to lie within the range encountered in clinical practice. The clinical implications of these observations is difficult to assess. MACKICHAN (1989) has argued that, for drug displacement interactions to be clinically rele- vant, the displaced drug must have a low Vd, a narrow therapeutic range, and impaired elimination following the interaction, and quinine fulfills these criteria. How- ever, since quinine is g base it is more extensively ionized at low DH, and its ilonln1 octanol nartition falls from 1.875 to l&53 over the-&I gradient’7.4 to 7.0 (unpub- lished data), which would make it less available to cross membranes. Clinical studies looking for a relationship between arterial pH and quinine toxicity are needed, es- pecially in the setting of overdose.
We have demonstrated important differences in quinine disposition in cerebral malaria between children and adults, have estimated the therapeutic range of the unbound drug, and have designed improved treatment regimens. We now propose to test the predictive value of our simulations by clinical study. Acknowledgement$
We thank the director of the Kenya Medical Research In- stitute (KEMRI) for permission to publish these findings. Dr N. Peshu, Head of the Kilifi Unit, and Dr J. B. 0. Were, Director of the Clinical Research Centre, KEMRI, gave invaluable support. Thanks are also due to Prof. G. Tucker. Mr S. Szwandt and Drs G. Edwards, T. Eggelte,, D. L. Forster; F. J. Kirkham, E. Lin- dup, V. Marsh, C. Nevlll, C. Newbold, R. W. Snow and M. T. Winstanley. The study would not have been possible without the dedication of the nurses, technicians and other staff of the KEMRI Unit. P. A. W. is a Medical Research Council Training Fellow in Tropical Medicine, and has personal support from thi Royal Society; K. M. is a Wellcome Trust Senior Research Fel- low; C. R. J. C. N. holds an Advanced Training Fellowship from the Wellcome Trust. This study received financial support from the UNDlYWorld Bank/WHO programme for training and research in tropical medicine, and forms part of the KEMRdUniversity of OxfordiWellcome Trust research pro- gramme at Kilifi.
References Bateman, D. N., Blain, l’. G., Woodhouse, K. W., Rawlins,
M. D., Dyson, H., Heyworth, R., Prescott, L. F. & Proud- foot, A. T. (1985). Pharmacokinetics and clinical toxicity of

206
quinine overdosage: lack of efficacy of techniques intended to enhance elimination. Quarter& Journal of Medicine, 54, 12% 131.
Bowman, M. E., Brennan-Roper, S. M. & Henry, J. A. (1985). Complications of quinine poisoning. Lancet, i, 384-385.
Brors, O., Nilsen, O., Sager, G., Sandnes, D. & Jacobsen, S. (1984). Influence of pH and buffer type on drug binding in human serum. Clinical Phamacokinetics, 9,85-86.
Davis, T. M. E., White, N. J., Looareesuwan, S., Silamut, K. & Warrell, D. A. (1988). Quinine pharmacokinetics in cere- bral malaria: predicted plasma concentrations after rapid in- travenous loading using a two-compartment model. Transactions of the Royal Society of Tropical Medicine and Hy- giene, 82,542-547.
Dyson, E. H., Proudfoot, A. T., Presott, L. F. & Heyworth, R. (1985). Death and blindness due to overdose of quinine. British M’edicalJoumal, 291,31-33.
Henry, J. A., Dunlop, A. W., Mitchell, S., Turner, I’. & Adams, P. (1981). A model for the pH dependence of drug- protein binding. Journal of Pharmacy and Pharmacology, 33, 179-182.
Kremer, J. M. H., Wilting, J. & Janssen, L. H. M. (1988). Drug binding to human alpha-1-acid-glycoprotein in health and disease. Pharmaceutical Reviews, 40, 1-47.
MacKichan, J. (1989). Protein binding drug displacement inter- actions: fact or fiction? Clinical Pharmacokinetics, 16,65-73.
Mansor, S. M., Taylor, T. E., McGrath, C. S., Edwards, G., Ward, S. A., Wirima, J. J. & Molyneux, M. E. (1990). The safety and kinetics of intramuscular quinine in Malawian children with moderately severe falciparum malaria. Transac- tions of the Royal Society of Tropical Medicine and Hygiene, 84, 4X2-488.
Mansor, S. M., Molyneux, M. E., Taylor, T. E., Ward, S. A., Wirima, I. I. & Edwards, G. (1991). Effect of Plasmodium falciparum malaria infection onthe plasma concentration of alphat acid glycoprotein and the binding of quinine in Mala- wian children. British Journal of Clinical Pharmacology, 32, 317-323.
Mberu, E. K., Ward, S. A., Winstanley I’. A. & Watkins, W. M. (1991). Measurement of auinine in filter-paper absorbed blood by high performance liquid chromatography. Journal of Chromatography, 570,180-184.
Mihaly, G. W., Ching, M. S., Klein, M., Paull, J. & Small- wood, R. (1987). Differences in the binding of quinine and quinidine to plasma proteins. BritishJournal of Clinical Phar- macology, 24,769-774.
Molyneux, M. E., Taylor, T. E., Wirima, J. J. & Borgstein, J. (1989). Clinical features and prognostic indicators in paedia- tric cerebral malaria: a study of 131 comatose Malawian child- ren. QuarterlyJournal of Medicine, 71,441-459.
Pasvol, G., Newton, C. R. J. C., Winstanley, I’. A., Watkins, W. M., Peshu, N. M., Were, J. B. O., Marsh, K. & Warrell, D. A. (1991). Quinine treatment of severe falciparum malaria in African children; a randomized trial of three regimens. American Journal of Tropical Medicine and Hygiene, 45, 702- 711 _-.
Phillips, R. E., Looareesuwan, S., White, N., Silamut, K., Kietnun, S. & Warrell, D. A. (1986). Quinine uharmaco- kinetics in pregnant and’lactating women w&h falciparum ma-
laria. BritishJournal of Clinical Pharmacology, 21,677-683. Rheeder, I’. & Sieling, W. L. (1991). Acute persistent quinine-
induced blindness. South African Medical Journal, 79, 563- 564.
Rieckmann, K. H., Sax, L. J., Campbell,, G. H. & Mrema, J. E. (1978). Drug sensitivity of Plasmodtum falciparum: an in- vitro microtechnique. Lancet, ii, 22-23.
Sabchareon, A., Chongsuphajaisiddhi, T. & Attanath, I’. (1982). Serum quinine concentrations following the initial dose in children with falciparum malaria. Southeast Asian Journal of Tropical Medicine and Public Health, 13,556-562.
Shann, F., State, J. & Edstein, M. (1985). Pharmacokinetics of quinine in children.Joumal ofPediatrics, 106,506-510.
Shenton, F. C., Bots, M., Menon, A., Eggelte, T. A., de Wit, M. & Greenwood, B. M. (1988). An ELISA test for detecting chloroquine in urine. Transactions of the Royal Society of Tropical Medicine and Hygiene, 82,216-220.
Silamut, K., White, N. J., Looareesuwan, S. & Warrell, D. A. (1985). Binding of quinine to plasma proteins in falciparum malaria. American Journal of Tropical Medicine and Hygiene, 34,681-686.
Silamut, K., Molunto, I’., Ho, M., Davis, T. M. E. & White, N. J. (1991). Alphat acid glycoprotein (orosomucoid) and plasma protein binding of quinine in falciparum malaria. Brit- ishJouma1 of Clinical Pharmacology, 32, 311-317.
Subsaeng, L. (1986). Sensitivity to quinine and mefloquine of Plasmodium falciparum in Thailand. Bulletin of the World Health Organization, 64,759-765.
Wailer, D., Krishna, S., Craddock, C., Brewster, D., Jammeh, A., Kwiatkowski, D., Karbwang, J., Molunto, I’. & White, N. J. (1990). The pharmacokinetic properties of intramuscu- lar quinine in Gambian children with severe falciparum mala- ria. Transactions of the Royal Society of Tropical Medicine and Hygiene, 84,488-491.
Warrell, D. A., Molyneux, M. & Beales, I’. F., editors (1990). Severe and complicated malaria, 2nd edition. Transactions of the Royal Society of Tropical Medicine and Hygiene, 84, supple- ment 2.
Wattanagoon, Y., Phillips, R. E., Warrell, D. A., Silamut, K., Looareesuwan, S., Nagachinta, B. & Back, D. J. (1986). In- tramuscular loading dose of quinine for falciparum malaria: pharmacokinetics and toxicity. British Medical Journal, 293, 11-13.
White, N. J., Looareesuwan, S., Warrell, D. A., Warrell, M. J., Bunnag, D. & Harinasuta, T. (1982). Quinine pharmaco- kinetics and toxicity in cerebral and uncomplicated falcipa- rum malaria. AmericanJournal of Medicine, 73,564571.
White, N. J., Looareesuwan, S., Warrell, D. A., Warrell, M. J., Chanthavanich, I’., Bunnag, D. & Harinasuta, T. (1983a). Quinine loading dose in cerebral malaria. American Journal of Tropical Medicine and Hygiene, 32, l-5.
White, N. J., Chanthavanich, I’., Krishna, S., Bunch, C. & Si- lamut, K. (1983b). Quinine disposition kinetics. BritishJour- nal of Clinical Pharmacology, 16,399-403.
Received 3 November 1992; revised 14 December 1992; accepted for publication 15 December 1992