Embed Size (px)
Citation preview
Toxicology : Basic concepts and toxidromes
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Acute intoxications
Definition
Acute exposition to an overdose of drugs or substances not intended for human use
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
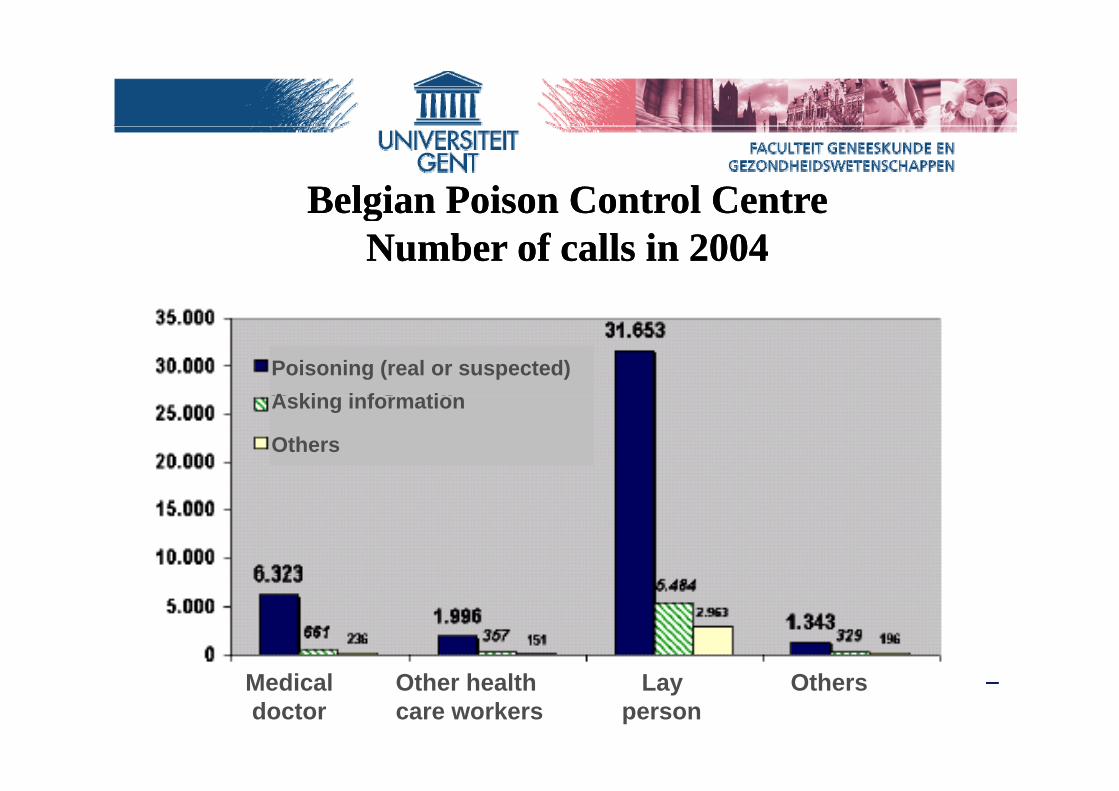
Belgian Poison Control Centre Belgian Poison Control Centre ggNumber of calls in 2004Number of calls in 2004
Poisoning (real or suspected)A ki i f tiAsking information
Others
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007Medical Other health Lay Othersdoctor care workers person
Types of acute poisoning
• Auto-intoxication• Accidental• Homicide, Münchhausen-syndrome• Bioterrorism• Alcohol and illicit drugsAlcohol and illicit drugs
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
I i i i h dIntoxications in the emergency department
Auto-intoxication = most frequentP i id l " f h l " i th t t f‣Parasuicidal : "cry for help" in the context ofa psychological crisisS i id l i t ti t di‣Suicidal : intention to die
diffi lt t di ti i h l hi t i l ti !difficult to distinguish always psychiatric evaluation!
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
NHSNational Institute forNational Institute for Clinical Excellence
Self-harmThe short-term physical and psycho-logical management and secondary prevention of self-harm in primary and p p ysecondary care
Developed by the National Collaborating Centre forMental Health
Types of acute poisoningTypes of acute poisoning
• Auto intoxication• Auto-intoxication• Accidental
‣ most frequently carbon monoxide‣ most frequently carbon monoxide‣ therapeutic mistakes (children / elderly patients)‣ errors
• Homicide, Münchhausen-syndrome• BioterrorismBioterrorism• Alcohol and illicit drugs
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007

Types of acute poisoning
• Auto-intoxication• Accidental• Homicide, Münchhausen-syndrome• Bioterrorism• Alcohol and illicit drugsAlcohol and illicit drugs
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Acute ethanol intoxication (1)
• Very frequent!
• Symptoms vary according to degree of intoxication with possible comaCaveat: interpretation of breath odour
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
A t th l i t i ti (2)Acute ethanol intoxication (2)
• Be aware of "hidden" clinical and metabolic disturbances:‣ hypoglycemia‣ head and neck trauma‣ head and neck trauma‣ Wernicke encephalopathy (thiamine deficiency)‣ acid-base disturbances
di th t i t ti l bl di‣ cardiomyopathy, gastro-intestinal bleeding‣ cardiac rhythm disturbances‣ infections (pneumonia, ...)‣ intake of ethylene glycol, methanol
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Interventions for preventing injuries in problem drinkersInterventions for preventing injuries in problem drinkersThe Cochrane Database of Systematic Reviews, 2005
Action with problem drinkers can cut risk of injury.Several different approaches were evaluated, the most common being brief counseling by health workers. The evidence from these studies suggests that action with problem drinkers is effective in reducing both injuries andproblem drinkers is effective in reducing both injuries andevents that lead to injury (such as falls, motor vehicle crashes and suicide attempts) However more research iscrashes, and suicide attempts). However, more research is needed to calculate the level of effectiveness accurately and to determine which type of program works best.
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Preventing acute intoxications
• "Child resistant" containersW i f t f th d f di ti• Warning of parents for the danger of medications for childrenL ibilit f i ti• Legibility of prescriptions
• Controlling medications and substances at home• Avoiding prescription of large quantities• …..
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
General approach in acute intoxication (1)
• Phases of intoxication : preclinical, toxic and resolution• Initial evaluation and treatment :• Initial evaluation and treatment :
‣ brief screening examination to identify immediate measures required to stabilize and prevent deterioration (vital signs,
)mental status, cardiac monitoring, ...)‣ supportive care, antidotes (glucose, thiamine, naloxone, ...)
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
General approach in acute intoxication (2)
• Diagnosis of intoxication :‣ history‣ physical examination‣ electrocardiography‣ X-rayy‣ toxicological screening / laboratory
• Evaluation of severity and predicting expected toxicity• Treatment
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Acute intoxication and physical examination (1)
• Mental status, vital signs and pupillary examination allow distinction between :‣ physiological excitation : e.g. by anticholinergic, sympatho-
mimetic or central hallucinogenic agents, drug withdrawal state‣ physiological depression : e.g. by cholinergics, sympathicolytics,
opiates, sedative-hypnotics or alcohols
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007

Acute intoxication and physical examination (2)Acute intoxication and physical examination (2)
‣ mixed physiological effects : e g polydrug overdoses certain‣ mixed physiological effects : e.g. polydrug overdoses, certain metabolic poisons (hypoglycemic agents, salicylates, cyanide, ...), membrane-active agents (e.g. antiarrhythmics, local anesthetics, ...), agents with multiple mechanisms of action (e g tricyclicagents with multiple mechanisms of action (e.g. tricyclic antidepressants)
• Other physical findings :• Other physical findings :odor, neuromuscular abnormalities, skin findings, temperature alterations, ...p
Toxic syndromes (toxidromes)
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
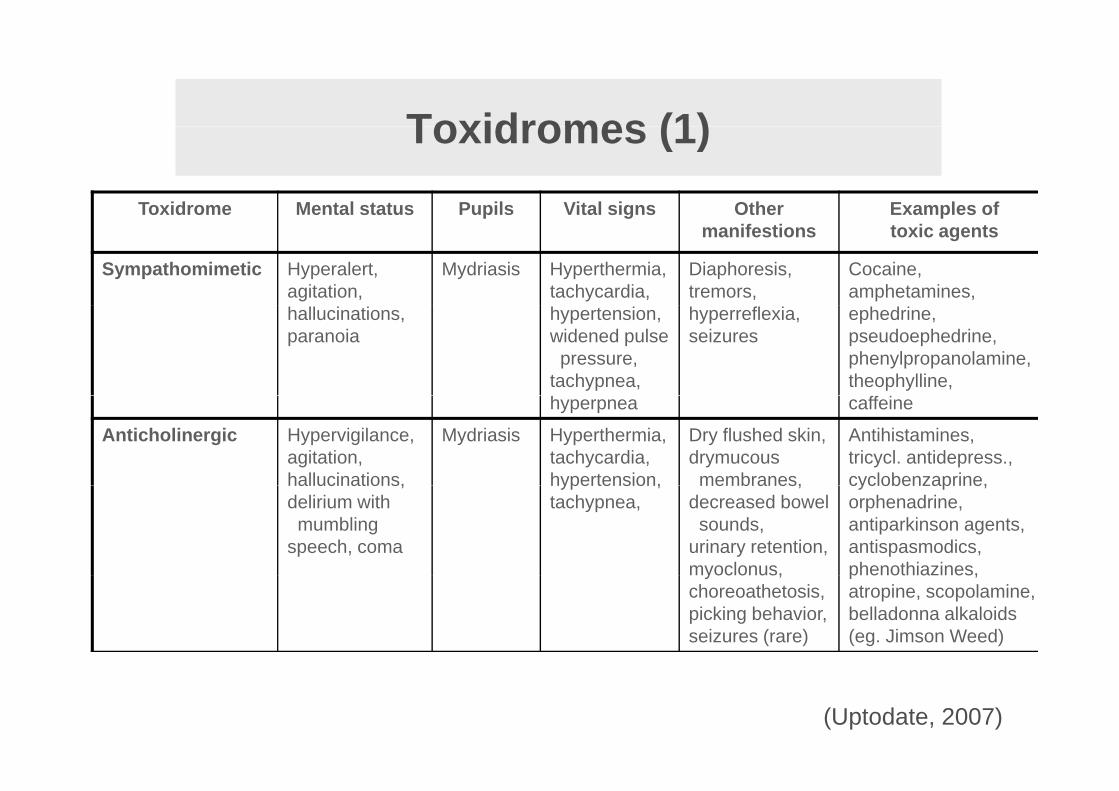
Toxidromes (1)Toxidromes (1)Toxidrome Mental status Pupils Vital signs Other Examples of p g
manifestionsp
toxic agents
Sympathomimetic Hyperalert,agitation,
Mydriasis Hyperthermia, tachycardia,
Diaphoresis, tremors,
Cocaine, amphetamines,
hallucinations, paranoia
hypertension, widened pulse pressure,
tachypnea,
hyperreflexia, seizures
ephedrine, pseudoephedrine, phenylpropanolamine, theophylline,
hyperpnea caffeine
Anticholinergic Hypervigilance, agitation, hallucinations,
Mydriasis Hyperthermia, tachycardia, hypertension,
Dry flushed skin, drymucousmembranes,
Antihistamines, tricycl. antidepress., cyclobenzaprine,hallucinations,
delirium withmumbling
speech, coma
hypertension, tachypnea,
membranes, decreased bowelsounds,
urinary retention, myoclonus,
cyclobenzaprine, orphenadrine, antiparkinson agents, antispasmodics, phenothiazines,myoclonus,
choreoathetosis, picking behavior, seizures (rare)
phenothiazines, atropine, scopolamine, belladonna alkaloids (eg. Jimson Weed)
(Uptodate, 2007)
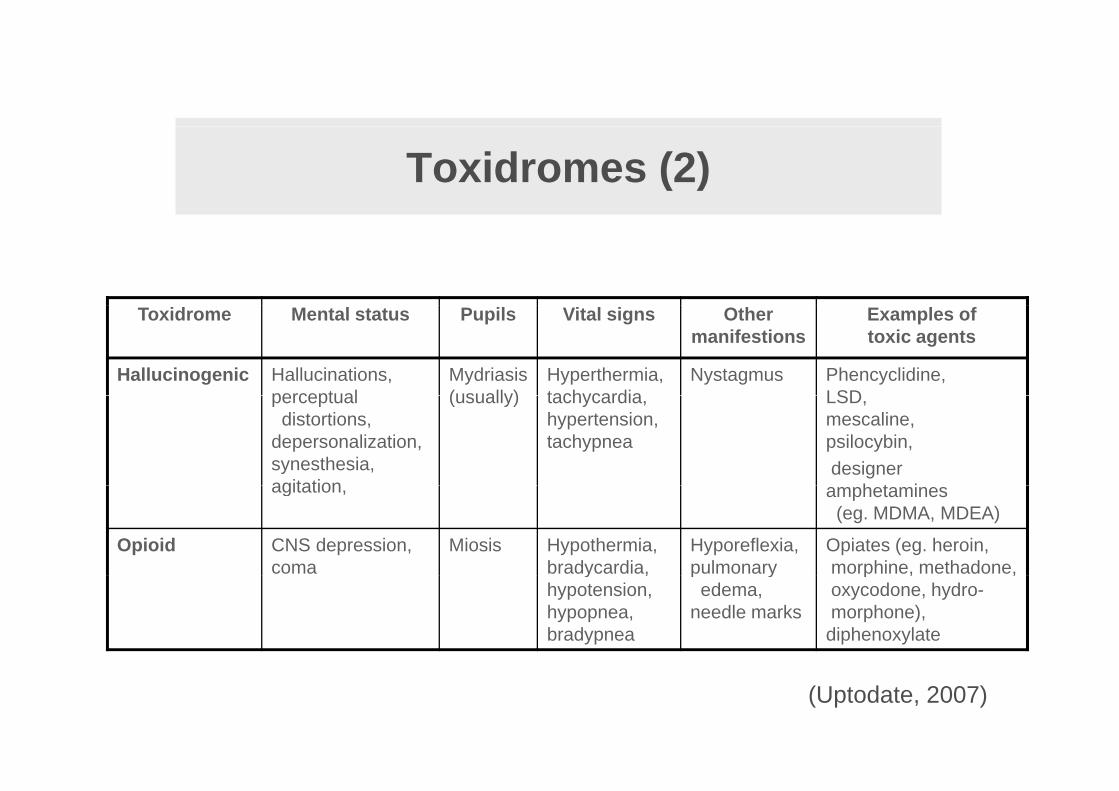
Toxidromes (2)
Toxidrome Mental status Pupils Vital signs Other manifestions
Examples of toxic agents
Hallucinogenic Hallucinations, perceptual
Mydriasis(usually)
Hyperthermia, tachycardia
Nystagmus Phencyclidine, LSDperceptual
distortions,depersonalization,synesthesia, agitation
(usually) tachycardia, hypertension, tachypnea
LSD,mescaline,psilocybin,designer
h t iagitation, amphetamines (eg. MDMA, MDEA)
Opioid CNS depression, coma
Miosis Hypothermia, bradycardia,
Hyporeflexia, pulmonary
Opiates (eg. heroin,morphine, methadone,y ,
hypotension, hypopnea, bradypnea
p yedema,
needle marks
p , ,oxycodone, hydro-morphone), diphenoxylate
(Uptodate, 2007)
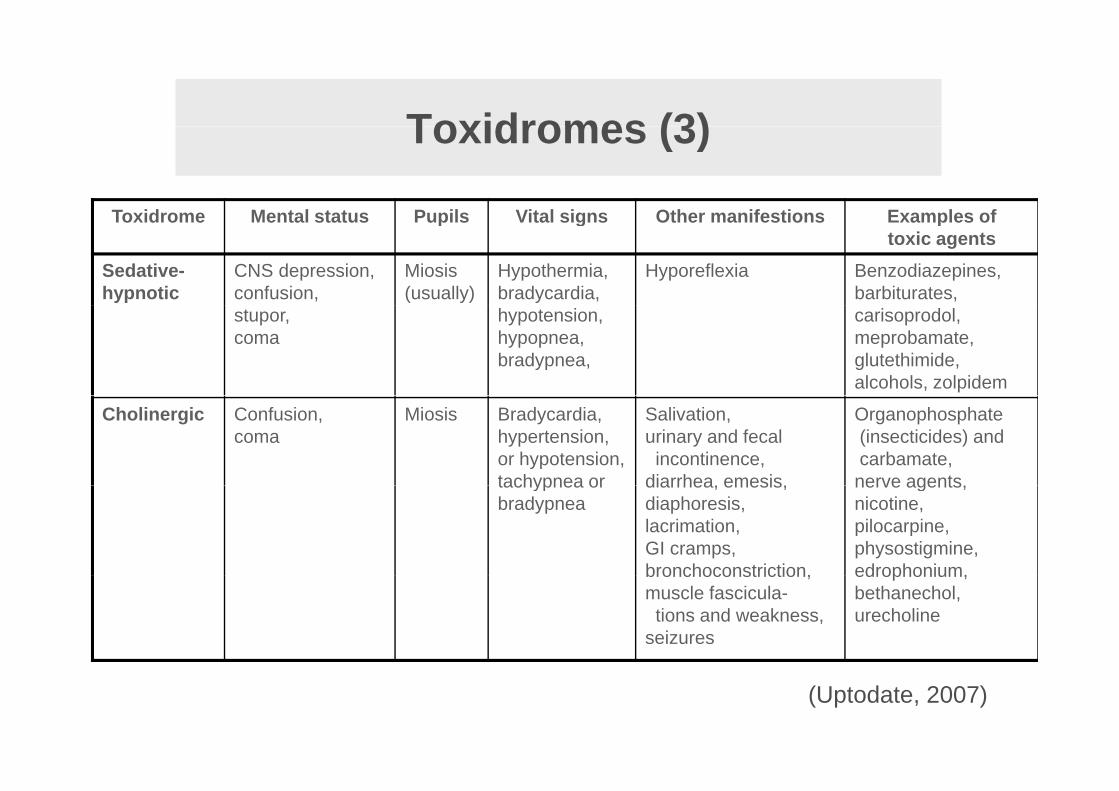
Toxidromes (3)Toxidromes (3)
Toxidrome Mental status Pupils Vital signs Other manifestions Examples ofToxidrome Mental status Pupils Vital signs Other manifestions Examples of toxic agents
Sedative-hypnotic
CNS depression, confusion,
Miosis (usually)
Hypothermia, bradycardia,
Hyporeflexia Benzodiazepines, barbiturates,
stupor,coma
hypotension, hypopnea, bradypnea,
carisoprodol, meprobamate, glutethimide, alcohols, zolpidem
Cholinergic Confusion,coma
Miosis Bradycardia, hypertension, or hypotension, tachypnea or
Salivation, urinary and fecalincontinence,
diarrhea emesis
Organophosphate(insecticides) andcarbamate, nerve agentstachypnea or
bradypneadiarrhea, emesis,diaphoresis,lacrimation, GI cramps,bronchoconstriction,
nerve agents,nicotine,pilocarpine,physostigmine,edrophonium,bronchoconstriction,
muscle fascicula-tions and weakness,
seizures
edrophonium,bethanechol,urecholine
(Uptodate, 2007)
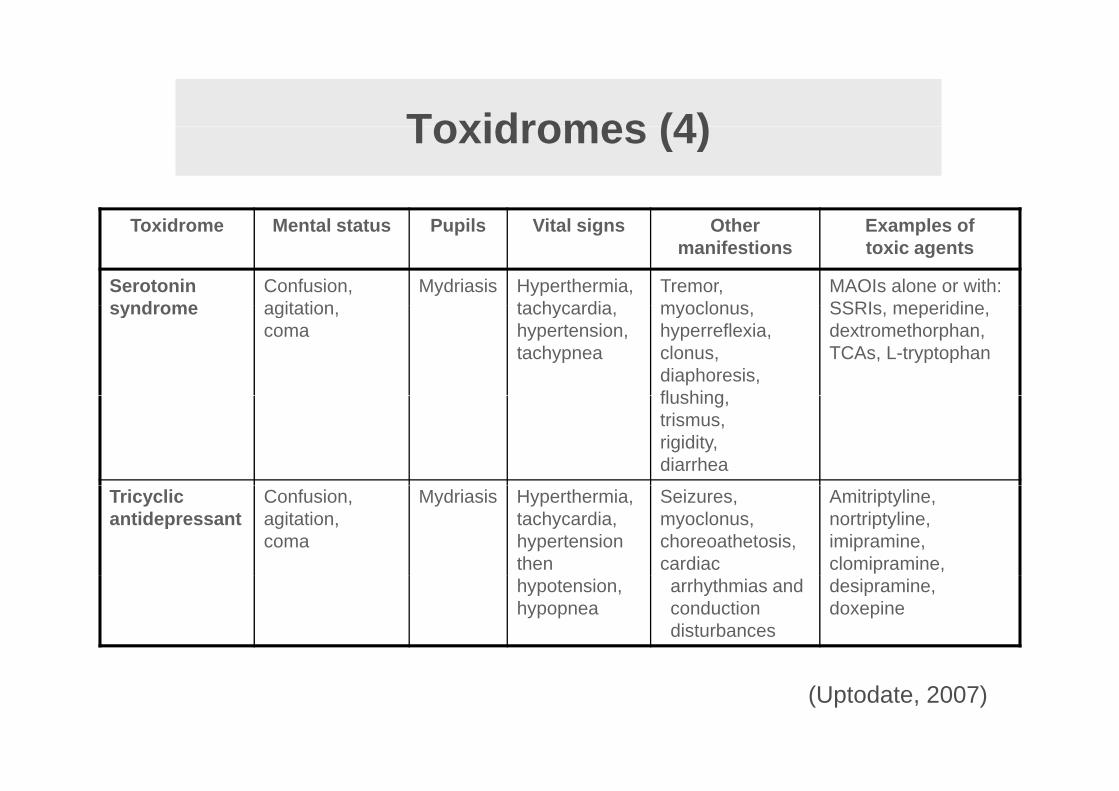
Toxidromes (4)Toxidromes (4)
Toxidrome Mental status Pupils Vital signs Other manifestions
Examples of toxic agents
Serotonin syndrome
Confusion, agitation
Mydriasis Hyperthermia, tachycardia
Tremor, myoclonus
MAOIs alone or with:SSRIs meperidinesyndrome agitation,
comatachycardia, hypertension, tachypnea
myoclonus, hyperreflexia, clonus, diaphoresis,flushing
SSRIs, meperidine,dextromethorphan,TCAs, L-tryptophan
flushing, trismus,rigidity,diarrhea
Tricyclic antidepressant
Confusion, agitation, coma
Mydriasis Hyperthermia, tachycardia, hypertensionthen
Seizures, myoclonus, choreoathetosis, cardiac
Amitriptyline,nortriptyline,imipramine,clomipramine,
hypotension, hypopnea
arrhythmias andconductiondisturbances
desipramine,doxepine
(Uptodate, 2007)
G l h i t i t i tiGeneral approach in acute intoxication
• Phases of intoxication : preclinical toxic and resolution• Phases of intoxication : preclinical, toxic and resolution• Initial evaluation and treatment
Di i f i t i ti• Diagnosis of intoxication :‣ history‣ physical examination‣ electrocardiography‣ X-ray‣ toxicological screening / laboratoryo co og ca sc ee g / abo a o y
• Evaluation of severity and predicting expected toxicity• Treatment
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
• Treatment

G l h i t i t i tiGeneral approach in acute intoxication
• Phases of intoxication : preclinical toxic and resolution• Phases of intoxication : preclinical, toxic and resolution• Initial evaluation and treatment
Di i f i t i ti• Diagnosis of intoxication :‣ history‣ physical examination‣ electrocardiography‣ X-ray‣ toxicological screening / laboratoryo co og ca sc ee g / abo a o y
• Evaluation of severity and predicting expected toxicity• Treatment
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
• Treatment
Toxicological investigationsToxicological investigations
• ScreeningScreening‣ e.g. acetaminophen and salicylates in cases of
auto-intoxication or uncertainty in history‣ immunoassay : fast, simple‣ qualitative screening (GC or MS) e.g. in cases of
severe toxicity or unexplained toxic symptomssevere toxicity or unexplained toxic symptoms
• Quantitative determination‣ e.g acetaminophen, carboxyhaemoglobin, methanol,
...
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007

Treatment of acute intoxications
1. Supportive therapy
2 Decontamination2. Decontamination
3. Antidotes
4. Enhanced elimination techniques
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007

D t i ti i t i t i tiDecontamination in acute intoxications
• For topical exposures :copious water / saline irrigation
• For oral ingestions :‣ activated charcoal‣ activated charcoal‣ syrup of ipecac, gastric lavage, whole bowel irrigation,
endoscopy, surgery, dilution, cathartics
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Problems with obtaining "evidence" for the utility ofProblems with obtaining evidence for the utility of gastro-intestinal decontamination in acute intoxication
• Large variability in intoxications (dose, time since ingestion, multiple substances, ...)
• Problem with reliability of the patient history
P bl f i f d t i i id l ti t• Problem of informed consent in suicidal patients
• Low mortality (1%)
(Smilkstein, 2002)
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Position statements : Gut decontamination
• Published in 1993 with updates in 2004-2005Published in 1993 with updates in 2004 2005
• The American Academy of Clinical Toxicology (AACT)(AACT)
• European Association of Poison Centers and Clinical Toxicology (EAPCCT)
http://www.clintox.org/Pos_Statements/Intro.html
Home» AACT Members Area
Click below for position statements on the following topics in PDF format:Ipecac Syrup
Single-Dose Activated
Charcoal
Multi-Dose
Activated Charcoal
Cathartics
Whole Bowel Irrigation
Gastric Lavage
Urine Alkalization
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Activated charcoalActivated charcoal
N t b b bl fi bl k• Not absorbable, fine black powder
• Adsorbs chemical substances in the pores within minutes of contactcontact
• Surface : 950 à 2000 m² per gramgram
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
A ti t d h lActivated charcoal
Adsorptive capacity varies according to g‣ molecular weight ‣ structure ‣ ionisation‣ ionisation‣ solubilityof the toxic substance
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
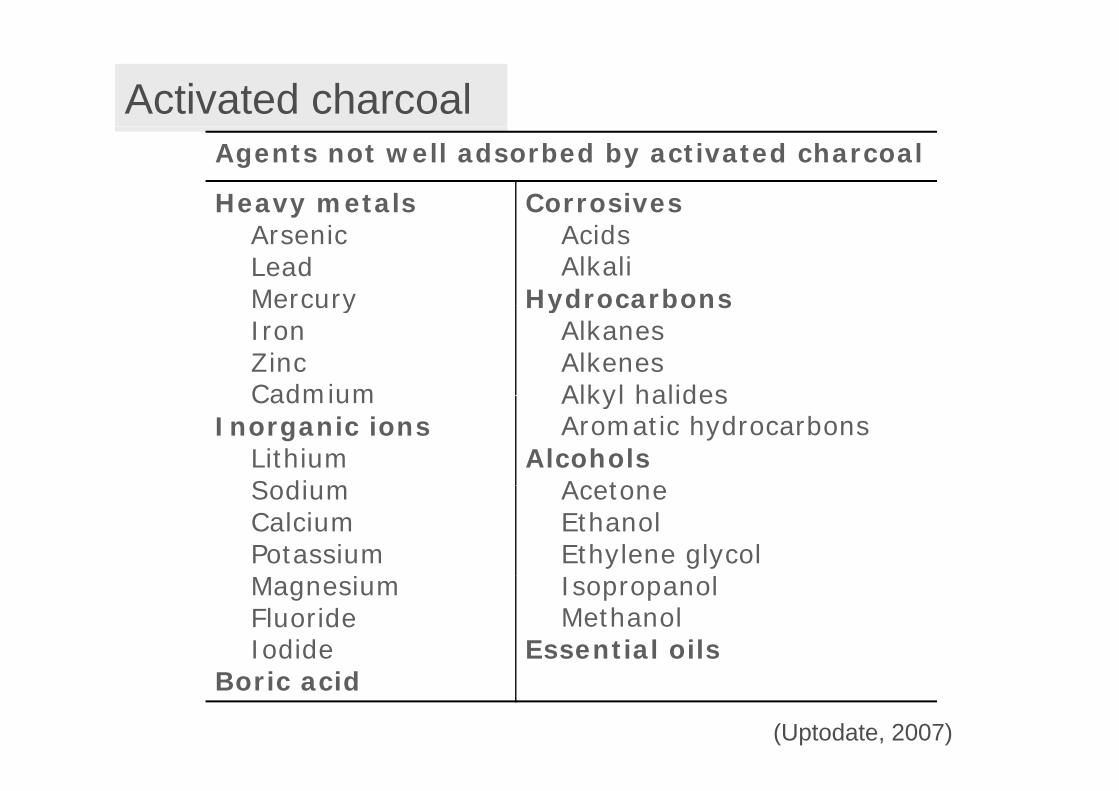
Activated charcoalAgents not well adsorbed by activated charcoal
Heavy metals CorrosivesyArsenicLeadMercury
AcidsAlkali
HydrocarbonsMercuryIronZincCadmium
HydrocarbonsAlkanesAlkenesAlkyl halidesCadmium
Inorganic ionsLithiumSodium
Alkyl halidesAromatic hydrocarbons
AlcoholsAcetoneSodium
CalciumPotassium
AcetoneEthanolEthylene glycol
lMagnesiumFluorideIodide
IsopropanolMethanol
Essential oilsBoric acid
(Uptodate, 2007)
I di ti f i l d ti t d h lIndications for single dose activated charcoal
• Volunteer studies suggest that activated charcoal is more likely to reduce poison absorption if it is administered within one hour of ingestionof ingestion.
• In the absence of satisfactorily designed clinical studies demonstrating benefit from its use, the administration of activated charcoal may be considered if a patient has ingested a potentially toxic amount of a poison up to one hour following ingestion.The potential for benefit after one ho r cannot be e cl ded• The potential for benefit after one hour cannot be excluded.
Position paper AACT/EAPCCT (Clinical Toxicology 2005; 43: 61-87)
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
C t i di ti f i l d ti t d h lContraindications for single dose activated charcoal
• The patient has an unprotected airway.
• Its use increases the risk and severity of aspiration (e.g. a hydrocarbon with a high aspiration potential)
• Patients who are at risk of gastrointestinal hemorrhage or per-f ti d t th l t di l ditiforation due to pathology, recent surgery or medical conditions.
• Presence of activated charcoal in the gastrointestinal tract may obscure endoscopic visualization but a corrosive is not aobscure endoscopic visualization, but a corrosive is not a contraindication when charcoal is used for co-ingested agents that are systemic toxins.
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
y

C li ti f i l d ti t d h l
M j it f d t t l t d t
Complications of single dose activated charcoal
Majority of adverse events not related to appropriate use :
•Aspiration pneumonitis
•Vomiting (5 – 15%)
•Corneal abrasions
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
D t i ti i t i t i tiDecontamination in acute intoxications
• For topical exposures :copious water / saline irrigation
• For oral ingestions :‣ activated charcoal‣ activated charcoal‣ syrup of ipecac, gastric lavage, whole bowel irrigation,
endoscopy, surgery, dilution, cathartics: see “Position Paper ACCT/EAPCCT”
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Gastrointestinal decontaminationGastrointestinal decontamination
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Treatment of acute intoxications
1. Supportive therapy
2 Decontamination2. Decontamination
3. Antidotes
4. Enhanced elimination techniques
Toxicology: Basic concepts and toxidromes – W. Buylaert and P. De Paepe - 25/08/2007
Poison control centre























![[Toxicology] toxicology introduction](https://img.pdfslide.net/doc/110x75/55c46616bb61ebb3478b4643/toxicology-toxicology-introduction.jpg)


