Embed Size (px)
Citation preview
ผศผศ..นพนพ..กวีวรรณกวีวรรณ ลิ้มประยูรลิ้มประยูร
ออ..นพนพ..เฉลิมไทยเฉลิมไทย เอกศิลปเอกศิลป
พพ..ออ..นพนพ..ดุสิตดุสิต สถาวรสถาวร
TPRC Annual Meeting 2008Mar 26-26, 2008

เด็กชาย อายุ 10 เดอืนCC: ถายเหลว ซึมลง มา 3 วัน PI: ครั้งนี้ ถายเหลว 3 วัน ซึม กินไดนอย ไปรักษา รพ. ชุมชนใกลบาน แต
อาการไมดีขึ้น มารดาจึงพามาตรวจซ้ํา ประวัติการเจบ็ปวยในอดีต
Primary immune deficiency (T-cell dysfunction?)Recurrent pneumonia, chronic otitis mediaSevere gastroesopharyngeal refluxPharyngeal incoordinationDelayed development
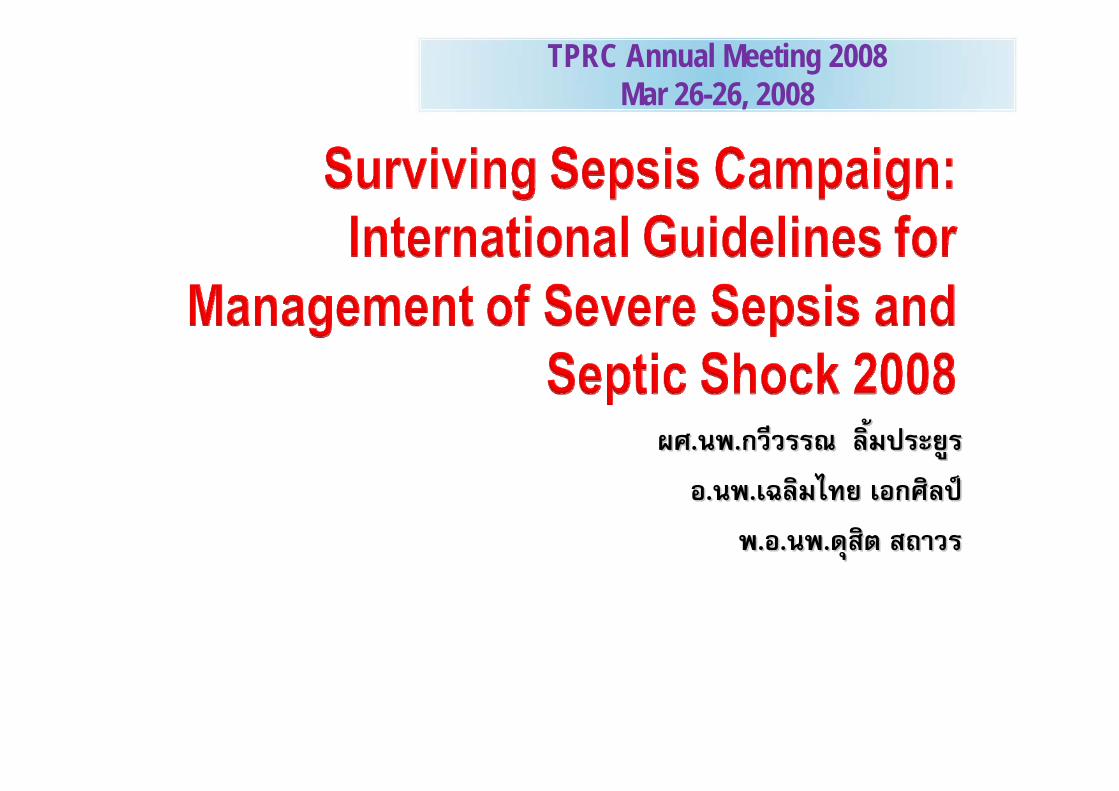
ประวัติเพิ่มเติมเพิ่ง discharge จากโรงพยาบาลเมื่อ 2 สัปดาหกอน โดยเคยนอน รพ.
นาน 1 เดือน ดวยปญหา ดังตอไปนี้•severe pneumonia with ARDS•septic shock & DIC
ผลการตรวจพิเศษเพิ่มเตมิ ไดแก • UGI study: Pharyngeal incoordination and severe
GE reflux • Serum IgG, IgA, IgM: Normal for age• Anti HIV - negative• CD count: CD3 85%, CD4 18.4%, CD8 58.7%,
CD4/CD8 0.3, CD19 11%, CD16/56 3.1% • DHR test: Normal (neutrophil oxidative burst assay) • T-cell proliferation essay: Normal
PH • บุตรคนเดียว คลอดปกติ ที ่รพ.ชุมชน
• น้ําหนักแรกคลอด 2,500 g• ดูดนมแมเฉพาะ อาย ุ1 เดือนแรก หลังจากนั้นใชนมผสม• วัคซีนไมครบ

PH• อายุ 1 เดือน admit ที ่รพ.จังหวัด
Dx: Pneumonia, anemia and thrombocytopenia (R/O ITP) on prednisolone ½ tab OD
• อายุ 1 ½ เดือน admit ที่ รพ.จังหวัด ครั้งที่สอง Dx: Acute Bronchitis and ITP on prednisolone
• อายุ 3 เดือน admit ที่ รพ.จังหวัด ครั้งที่สามDx: Severe thrombocytopenia on prednisolone

PH• อาย ุ5 เดือน admit ที่ รพ.จังหวัด และ refer ไป รพ.ศูนย
Dx : Acute gastroenteritis with moderate dehydration Metabolic acidosisPneumonia with ARDSAcute otitis mediaPersistent thrombogytopenia (peripheral destruction proved by bone marrow exam) Mucocutaneous candidiasis

PE: (at ER 2300 hr)V/S: T 38.3ºC, HR 100/ min, RR 40/min, BP 60/30 mm Hg BW 5 kg
GA: Lethargy, dyspnea, capillary refill > 3 sec. with cutis mamorata
Lung: Subcostal retraction, poor air entry, rhonchi both lungsHeart: Normal S1 S2 , nomurmurAbd: Liver 3 cm below right costal margin, spleen not palpable
active bowel soundNeurological: Stiffness of neck, Brudzinski’s sign - negative

Treatment at the ER: •Endotracheal intubation•Investigation
• CBC, ABGs, electrolyte, LFTs, blood C&S •0.9 % NaCl 50 ml IV drip 10 min x 2 dose•Ceftriaxone 350 mg IV stat•Repeated assessment
• BP 70/30 mm Hg delayed capillary refill•Start dopamine at 10 and increase to 15 mcg/kg/min•Give 7.5% NaHCO3 8.5 ml dilute IV drip 5 min•Repeated assessment
• BP 90/60 mmHg – transfer to PICU

Initial Lab:•CBC:
• Hb 10.6 g/ dl, Hct 33% • WBC 43,580/mm3 N 84% L 7%, M 4% Band 5 % • Platelets 196,000/mm3
•Blood glucose 180 mg/dl•LFTs:
• Total protein 5.8 g/dl, alb 2.98 g/dl, glob 2.83 g/dl, • Total bilirubin 0.23 mg/dl, direct bil. 0.1 mg/dl, AST 17
•BUN 35 mg/dl, Cr 0.96 mg/dl•Electrolytes: Na 120, K 2.0, CI 111, CO2 4.0 (mEq/L)•ABGs: pH 6.82, PaCO2 21.4, PaO2 385.9, HCO3 3.3, BE -27.5•Serum iCa : 1.62 mmol/L (1.18-1.30 mmol/L)

Minimal LLL infiltration
Initial CXR at PICU

Treatment at PICU (2400 hr )• Ventilator setting
• PCV A/C mode • FiO2 0.3, Ti 0.5 sec, PIP 17 cm H2O, PEEP 5 cm H2O,
Rate 50/min• 0.9% NaCl 50 ml IV dirp 10 min • Meropenam IV• Retained urine catheter• Tracheal suction C/S• Stool exam and C/S

Hospital Course:•at 0200-0300 hr
BP 71/30 - 69/29 mm Hg, PR 85-90 /minAdd adrenaline IV drip 0.1 → 0.15 → 0.2 mg/kg/min
•at 0400 hrBP 73/34 - 77/28 mm HgAdd hydrocortisone 1 mg/kg/dose IV drip q 8 hr
•at 0600 hrBP 76/28 - 89/27 - 99/36 mmHg PR 90 – 112Urine 7.5 ml/kg/hr (2400-0600)Serum Electrolyte: Na 131 K 1.73 CI 108 HCO3-ABG pH 7.05 PaCO2 24.7 PaO2 315.6 HCO3 7.1 BE -21.5Add norepinephrine IV drip at 0.4 mcg/kg/min Start KCI IV infusion

• 0800 hrCoagulation profile: • PT 16.4 sec (11.3-14.6), INR 1.3• aPTT 86.9 sec (27.4-34.1 sec)• TT 5.6 (4.7-6.5 sec)

• 1100 hrBP 92/36 – 85/50 mmHg PR 136 – 146Good capillary refillNo differences between proximal & distal pulseABGs: pH 7.317, PaCO2 20, PaO2 174, HCO3 13

Day 2
•Right foot : absence of dorsalis pedis pulse with cool skin, rapid progress to discoloration of skin

Investigation• Echocardiography:
• No vegetation, ejection fraction 26%• Serum protein C: 73 % (69.1-134.1%)• Anti-thrombin III: 68 % (71-115%)• Serum protein S: 24.9% (63-135%)• Anti-factor Xa: 0.13

Treatment•Low molecular weight heparin (LMWH) 0.01 ml/kg/dose
Q 12 hr (targeted anti factor Xa at 0.3-0.7 units/ml)•FFP IV drip OD•Coumadin after LMW heparin

Summary of Hospital Course•Day 7
Extubation•Day 38
BK amputation•Day 45
Discharge Home

HemodynamicHemodynamic support support in in
septic shockseptic shockกวีวรรณกวีวรรณ ลิ้มประยูรลิ้มประยูร
หนวยโรคระบบหายใจและเวชบําบัดวิกฤตหนวยโรคระบบหายใจและเวชบําบัดวิกฤต
ภาควิชากุมารเวชศาสตรภาควิชากุมารเวชศาสตร
คณะคณะแพทยศาสตรศิแพทยศาสตรศิริราชพยาบาลริราชพยาบาล

Respiratory failure Shock
Cardiopulmonary failure
Cardiopulmonary arrest
Progression of Respiratory Failure and Shock
Progression of Respiratory Progression of Respiratory Failure and ShockFailure and Shock
Various Conditions

HemodynamicsHemodynamics
MyocardialContractility
Stroke Volume Preload
Cardiac Output Afterload
Blood Pressure Heart Rate
Systemic Vascular Resistance
Textbook of Pediatric Advanced Life Support, 1988Textbook of Pediatric Advanced Life Support, 1988
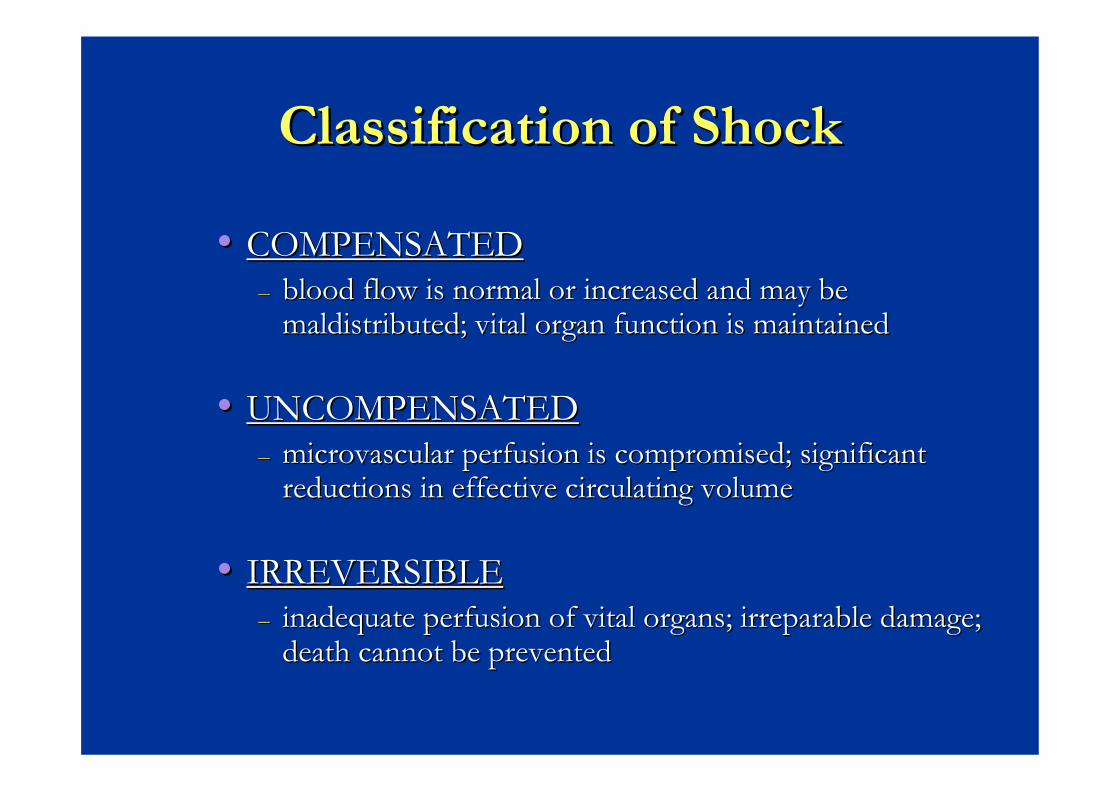
Classification of ShockClassification of Shock
•• COMPENSATEDCOMPENSATED–– blood flow is normal or increased and may be blood flow is normal or increased and may be
maldistributedmaldistributed; vital organ function is maintained; vital organ function is maintained
•• UNCOMPENSATEDUNCOMPENSATED–– microvascularmicrovascular perfusion is compromised; significant perfusion is compromised; significant
reductions in effective circulating volumereductions in effective circulating volume
•• IRREVERSIBLEIRREVERSIBLE–– inadequate perfusion of vital organs; irreparable damage; inadequate perfusion of vital organs; irreparable damage;
death cannot be preventeddeath cannot be prevented
SEPTIC SHOCK: SEPTIC SHOCK: ““WARM SHOCKWARM SHOCK””
Early, compensated, Early, compensated, hyperdynamichyperdynamic statestateClinical signsClinical signs
•• Warm extremities with bounding pulses, tachycardia, Warm extremities with bounding pulses, tachycardia, tachypneatachypnea, confusion, confusion
Physiologic parametersPhysiologic parameters•• widened pulse pressure, increased cardiac widened pulse pressure, increased cardiac ouptutouptut and mixed and mixed
venous saturation, decreased systemic vascular resistancevenous saturation, decreased systemic vascular resistanceBiochemical evidence:Biochemical evidence:
•• HypocarbiaHypocarbia, elevated lactate, hyperglycemia, elevated lactate, hyperglycemia
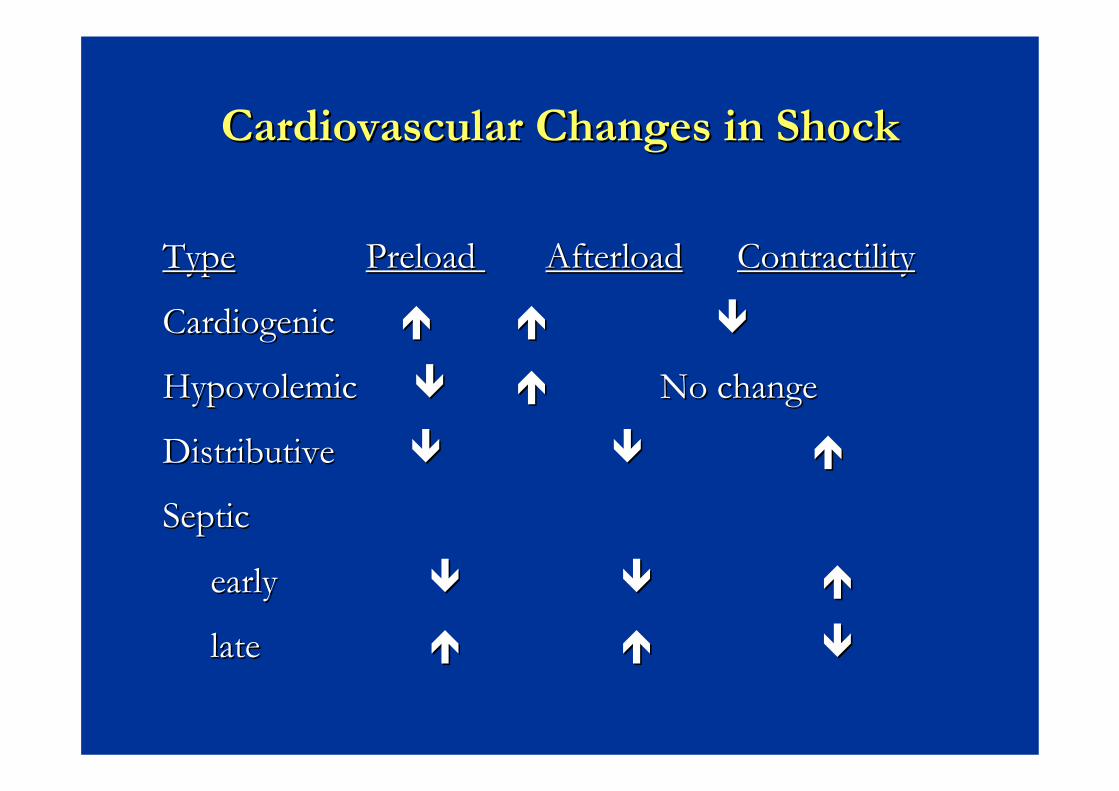
Cardiovascular Changes in ShockCardiovascular Changes in Shock
TypeType Preload Preload AfterloadAfterload ContractilityContractility
CardiogenicCardiogenic
HypovolemicHypovolemic No changeNo change
Distributive Distributive
SepticSeptic
early early
late late

Cardiovascular functionCardiovascular function
Cardiac OutputCardiac OutputClinical AssessmentClinical Assessment
peripheral perfusion, temperature, capillary refill, urine peripheral perfusion, temperature, capillary refill, urine output, output, mentationmentation, acid, acid--base statusbase status
CO = HR x SVCO = HR x SVHR responds the quickestHR responds the quickestSV is a function of three variablesSV is a function of three variables
preload, preload, afterloadafterload, and myocardial contractility, and myocardial contractilityA noncompliant heart cannot increase SVA noncompliant heart cannot increase SV

EvaluationEvaluationEarly Signs of ShockEarly Signs of Shock
sinus tachycardiasinus tachycardiadelayed capillary refilldelayed capillary refillfussy, irritablefussy, irritable
Late Signs of ShockLate Signs of Shockbradycardiabradycardiaaltered mental status (lethargy, coma)altered mental status (lethargy, coma)hypotoniahypotonia, decreased , decreased DTRDTR’’ssKussmalKussmal’’ss breathingbreathinghypotension is a very late sign hypotension is a very late sign Lower limit of SBP = 70 + (2 x age in years)Lower limit of SBP = 70 + (2 x age in years)

Cardiovascular AssessmentCardiovascular AssessmentHeart RateHeart Rate
Too high: 180 Too high: 180 bpmbpm for for infants, 160 infants, 160 bpmbpm for for children >1year oldchildren >1year old
Blood PressureBlood PressureLower limit of SBP = Lower limit of SBP = 70 + (2 x age in years)70 + (2 x age in years)
Peripheral PulsesPeripheral PulsesPresent/AbsentPresent/AbsentStrength (diminished, Strength (diminished, normal, bounding)normal, bounding)
Skin PerfusionSkin PerfusionCapillary refill timeCapillary refill timeTemperatureTemperatureColorColorMottlingMottling
CNS PerfusionCNS PerfusionRecognition of Recognition of parentsparentsReaction to painReaction to painMuscle toneMuscle tonePupil sizePupil size
Renal PerfusionRenal PerfusionUOP >1cc/kg/hrUOP >1cc/kg/hr

TreatmentTreatment
Airway managementAirway managementAlways provide supplemental oxygenAlways provide supplemental oxygenEndotrachealEndotracheal intubation and controlled intubation and controlled ventilation is suggested if respiratory failure or ventilation is suggested if respiratory failure or airway compromise is likelyairway compromise is likely
elective is safer and less difficultelective is safer and less difficultdecrease negative decrease negative intrathoracicintrathoracic pressure pressure improved oxygenation and Oimproved oxygenation and O22 delivery and decreased delivery and decreased OO22 consumptionconsumptioncan hyperventilate if necessarycan hyperventilate if necessary

TreatmentTreatment
CirculationCirculationBased on presumed etiology Based on presumed etiology Rapid restoration of intravascular volumeRapid restoration of intravascular volume
PIVPIV--if unstable you have 60if unstable you have 60--90 seconds90 secondsI.O. if less than 6I.O. if less than 6--12 years old12 years oldCentral venous catheterCentral venous catheterUse isotonic fluid: NSS, LRS, or 5% albuminUse isotonic fluid: NSS, LRS, or 5% albuminPRBCPRBC’’ss to replace blood loss or if still unstable to replace blood loss or if still unstable after 60cc/kg of crystalloid after 60cc/kg of crystalloid
anemia is poorly tolerated in the stressed, hypoxic, anemia is poorly tolerated in the stressed, hypoxic, hemodynamicallyhemodynamically unstable patientunstable patient
DextroseDextrose--containing solutionscontaining solutions
Indication:Indication:HypoglycemiaHypoglycemiaDaily maintenanceDaily maintenance
NotesNotesDo not use dextrose solution for fluid Do not use dextrose solution for fluid resuscitationresuscitation---------------------- HyperglycemiaHyperglycemia
GlucosuriaGlucosuriaHyperosmolarityHyperosmolarity

Commonly Commonly avialableavialable colloidscolloids
AlbuminAlbumin-- 5%, 20%5%, 20%Gelatin Gelatin –– HaemacelHaemacel, , GelofusineGelofusineComplex carbohydrate Complex carbohydrate –– HaesterilHaesteril, , PentastrachPentastrachBlood components : PRC, FWB, FFP, etc.Blood components : PRC, FWB, FFP, etc.

NotesNotes
Normal Saline/2 is a hypotonic crystalloid Normal Saline/2 is a hypotonic crystalloid solution.solution.In bleeding or severe anemic case consider In bleeding or severe anemic case consider blood components.blood components.
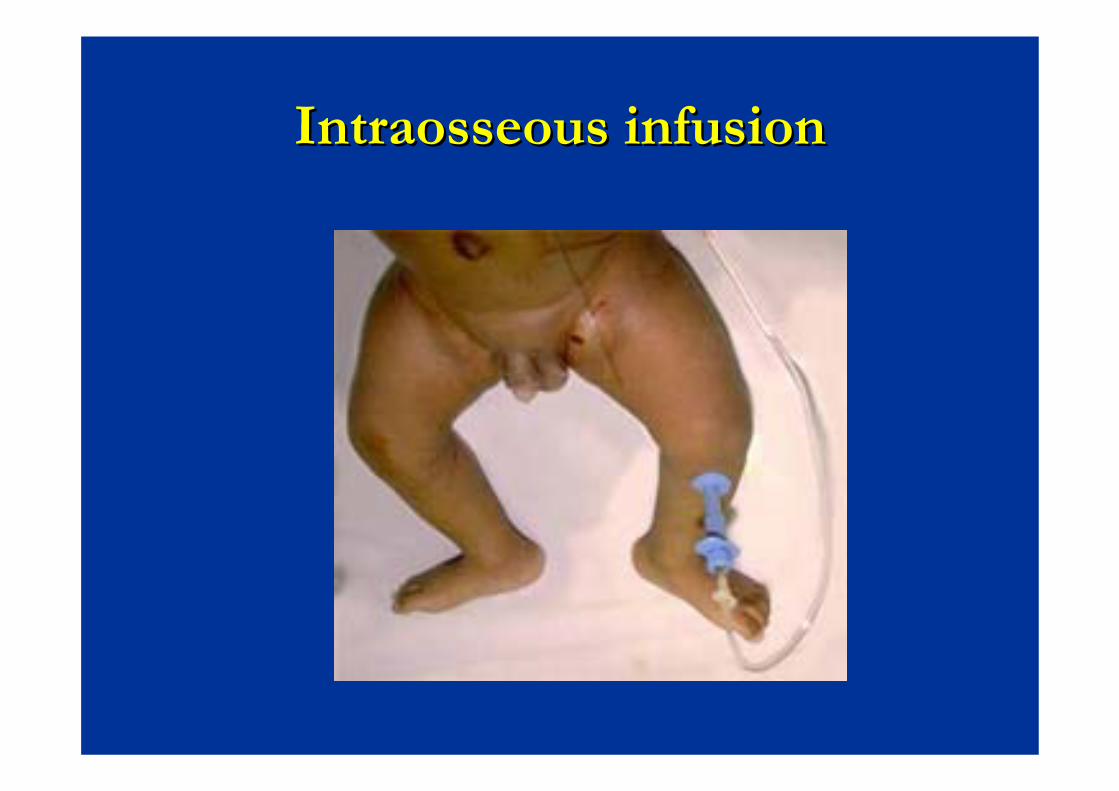
IntraosseousIntraosseous infusioninfusion
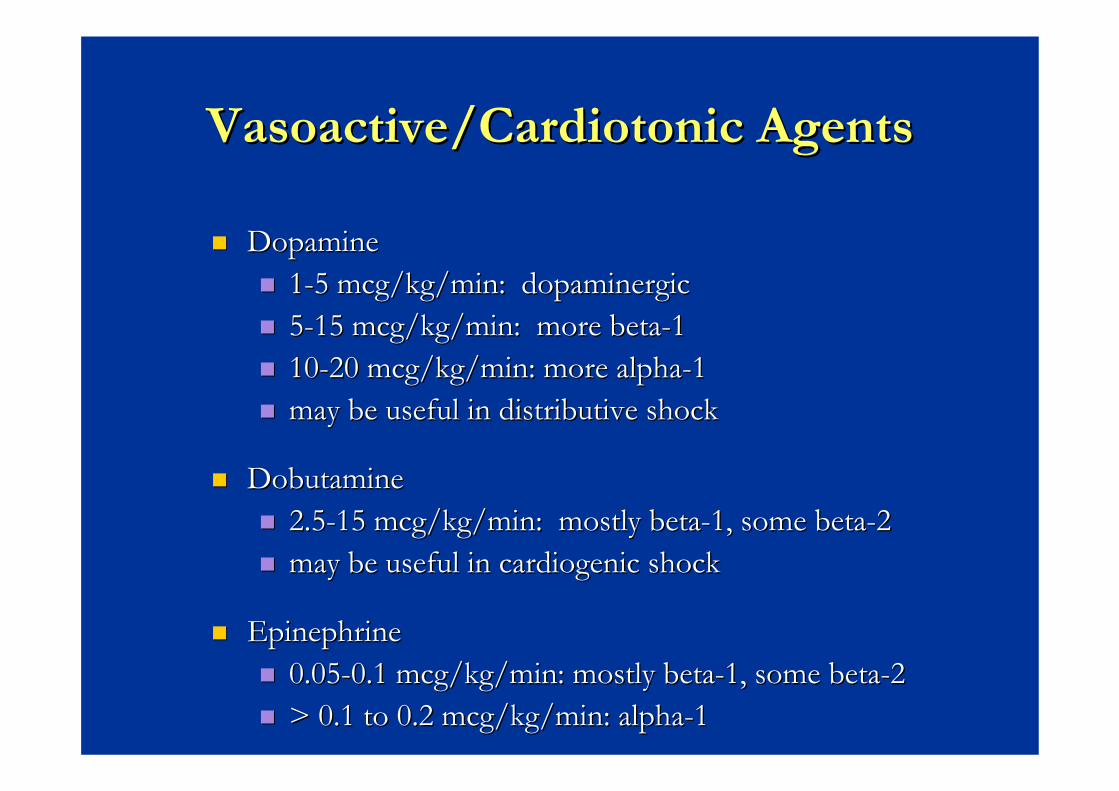
Vasoactive/CardiotonicVasoactive/Cardiotonic AgentsAgents
DopamineDopamine11--5 mcg/kg/min: 5 mcg/kg/min: dopaminergicdopaminergic55--15 mcg/kg/min: more beta15 mcg/kg/min: more beta--111010--20 mcg/kg/min: more alpha20 mcg/kg/min: more alpha--11may be useful in distributive shockmay be useful in distributive shock
DobutamineDobutamine2.52.5--15 mcg/kg/min: mostly beta15 mcg/kg/min: mostly beta--1, some beta1, some beta--22may be useful in may be useful in cardiogeniccardiogenic shockshock
EpinephrineEpinephrine0.050.05--0.1 mcg/kg/min: mostly beta0.1 mcg/kg/min: mostly beta--1, some beta1, some beta--22> 0.1 to 0.2 mcg/kg/min: alpha> 0.1 to 0.2 mcg/kg/min: alpha--11
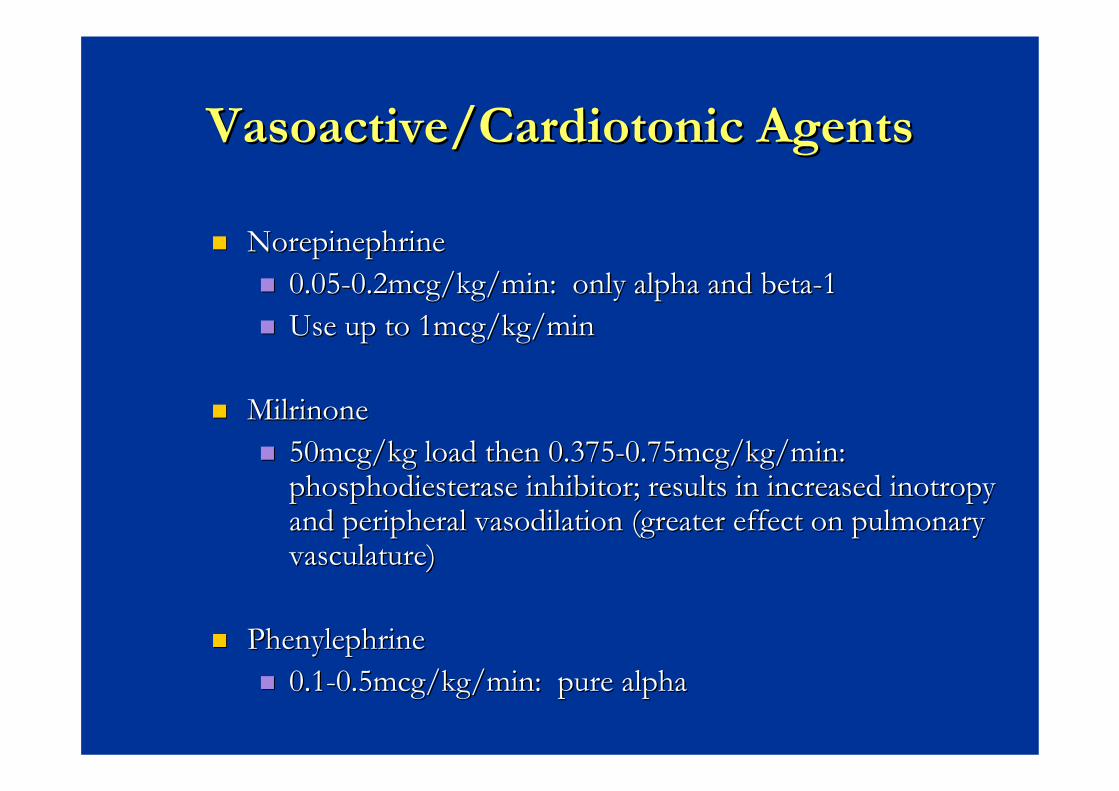
Vasoactive/CardiotonicVasoactive/Cardiotonic AgentsAgents
NorepinephrineNorepinephrine0.050.05--0.2mcg/kg/min: only alpha and beta0.2mcg/kg/min: only alpha and beta--11Use up to 1mcg/kg/minUse up to 1mcg/kg/min
MilrinoneMilrinone50mcg/kg load then 0.37550mcg/kg load then 0.375--0.75mcg/kg/min: 0.75mcg/kg/min: phosphodiesterasephosphodiesterase inhibitor; results in increased inhibitor; results in increased inotropyinotropyand peripheral and peripheral vasodilationvasodilation (greater effect on pulmonary (greater effect on pulmonary vasculature)vasculature)
PhenylephrinePhenylephrine0.10.1--0.5mcg/kg/min: pure alpha0.5mcg/kg/min: pure alpha

VasopressinVasopressin


คําถามคําถาม
หากทําการรักษาดังกลาวแลวไมดีขึ้นตองพิจารณาหากทําการรักษาดังกลาวแลวไมดีขึ้นตองพิจารณา
อะไรบางอะไรบาง


Systemic steroidsSystemic steroids
IndicationIndicationUnderlying possible deficiencyUnderlying possible deficiencyPurpuraPurpura fulminanfulminanFluid nonFluid non--responsiveresponsive

Metabolic IssuesMetabolic Issues
AcidAcid--BaseBase
Metabolic acidosis develops secondary to tissue Metabolic acidosis develops secondary to tissue hypoperfusionhypoperfusionProfound acidosis depresses myocardial contractility and Profound acidosis depresses myocardial contractility and impairs the effectiveness of impairs the effectiveness of catecholaminescatecholaminesTxTx: fluid administration and controlled ventilation: fluid administration and controlled ventilationBuffer administrationBuffer administration
Sodium Bicarbonate 1Sodium Bicarbonate 1--2meq/kg or can calculate a 1/2 2meq/kg or can calculate a 1/2 correction = 0.3 x weight (kg) x base deficitcorrection = 0.3 x weight (kg) x base deficithyperosmolarityhyperosmolarity, , hypocalcemiahypocalcemia, , hypernatremiahypernatremia, left, left--ward shift of the ward shift of the oxyhemoglobinoxyhemoglobin dissociation curvedissociation curve

Metabolic IssuesMetabolic Issues
ElectrolytesElectrolytes
ElectrolytesElectrolytesCalcium is important for cardiac function and for the Calcium is important for cardiac function and for the pressorpressor effect of effect of catecholaminescatecholaminesHypoglycemia can lead to CNS damage and is needed for Hypoglycemia can lead to CNS damage and is needed for proper cardiovascular functionproper cardiovascular functionCheck the BUN and Check the BUN and creatininecreatinine to evaluate renal functionto evaluate renal functionHyperkalemiaHyperkalemia can occur from renal dysfunction and/or can occur from renal dysfunction and/or acidosisacidosis

MonitoringMonitoring
ตองดูอะไรบางตองดูอะไรบาง

Monitoring of daily careMonitoring of daily care
Physical examinationsPhysical examinationsRecord ChartsRecord ChartsVital signsVital signsIntake/OutputIntake/OutputECG monitoringECG monitoringPulse Pulse oximetryoximetryBlood testsBlood tests





BP NIBP/IBPBP NIBP/IBP

Capillary Refill and peripheral temperature
Capillary Refill and Capillary Refill and peripheral temperatureperipheral temperature

Review/Trends/AlarmsReview/Trends/Alarms

CVP and other cardiac parametersCVP and other cardiac parameters
CVPCVPInvasive cardiac monitorInvasive cardiac monitor
Swan Swan GantzGantz -- : PWP, CO, PVR, SVR: PWP, CO, PVR, SVRMVOMVO22
Noninvasive cardiac monitorNoninvasive cardiac monitorEchocardiogramEchocardiogramCO by SaOCO by SaO22 waveformwaveform
Others : blood lactateOthers : blood lactate

Summary : Summary : Guide line for Guide line for HemodynamicHemodynamic supportsupport in in septic shockseptic shock

Early goal directed Early goal directed therapytherapyMaintain systemic Maintain systemic and organ and organ perfusionperfusionMonitor and Monitor and treatment multiple treatment multiple organ dysfunctionorgan dysfunction
ConclusionConclusion

Non-Conventional Management In Severe Sepsis & Septic Shock
Chalermthai Aksilp, MDQueen Sirikit National Institute of Child Health
Content
Prone positionProne position
Steroid TherapySteroid Therapy
Intravenous ImmunoglobulinIntravenous Immunoglobulin
Recommendation againstRecommendation against…………..

Prone Positioning

Prone PositioningProne Positioning
InternationalInternational GGuidelinesuidelines forfor MManagementanagement ofofSSevereevere SSepsisepsis && SSepticeptic SShockhock 20082008
Suggest prone positioning in ARDS patients Suggest prone positioning in ARDS patients requiring potentially injurious level of FiOrequiring potentially injurious level of FiO22 or or plateau pressure who are not at high risk for plateau pressure who are not at high risk for adverse consequences of positional changes adverse consequences of positional changes (2C)(2C)
International guidelines for management of severe sepsis and septic shock 2008.Crit Care Med 2008 ;36, 296-327

AlsaghirAlsaghir AH.AH.CritCrit CareCare MedMed 2008;362008;36 : 603: 603--609609

AlsaghirAlsaghir AH. AH. CritCrit CareCare MedMed 2008;362008;36 : 603: 603--609609
Effect of Prone on OxygenationEffect of Prone on Oxygenation
AlsaghirAlsaghir AH. AH. CritCrit CareCare MedMed 2008;362008;36 : 603: 603--609609
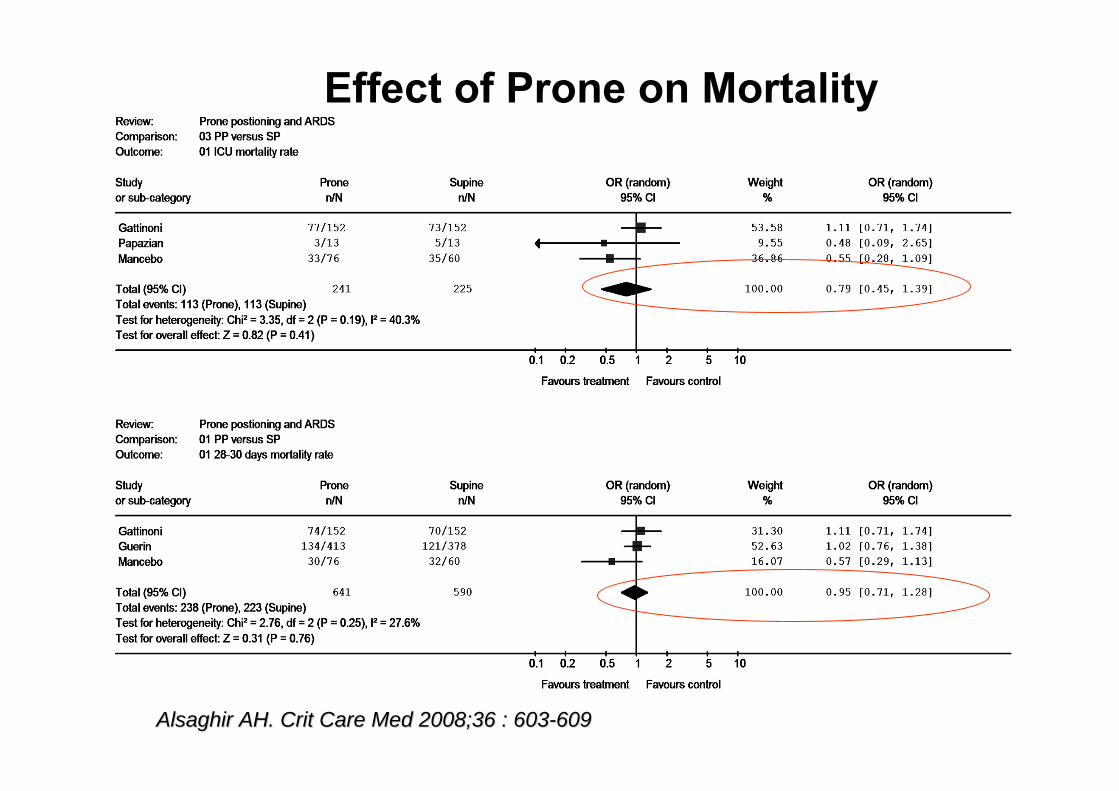
Effect of Prone on Mortality

AlsaghirAlsaghir AH. AH. CritCrit CareCare MedMed 2008;362008;36 : 603: 603--609609
Effect of Prone on Mortality in Severe ARDS
SAPS II, simplified acute physiology score (SAPS) II

Clinical Effects of ProneClinical Effects of Prone
70-80 % of patients respond to prone
50% respond to prone position & maintain good oxygenation when returned to the supine position
30% respond to prone but do not maintain when they are repositioned
Contraindications For Prone PositionContraindications For Prone Position
On ICD or flail chest On ICD or flail chest Increased intracranial pressureIncreased intracranial pressureHemodynamicHemodynamic instabilityinstabilityUnstable spinal cord injuryUnstable spinal cord injuryRecent abdominal or thoracic surgeryRecent abdominal or thoracic surgeryInability to tolerate prone positionInability to tolerate prone position
MonicaMonica SRSR.... ChestChest 20032003;;124:269124:269--274274
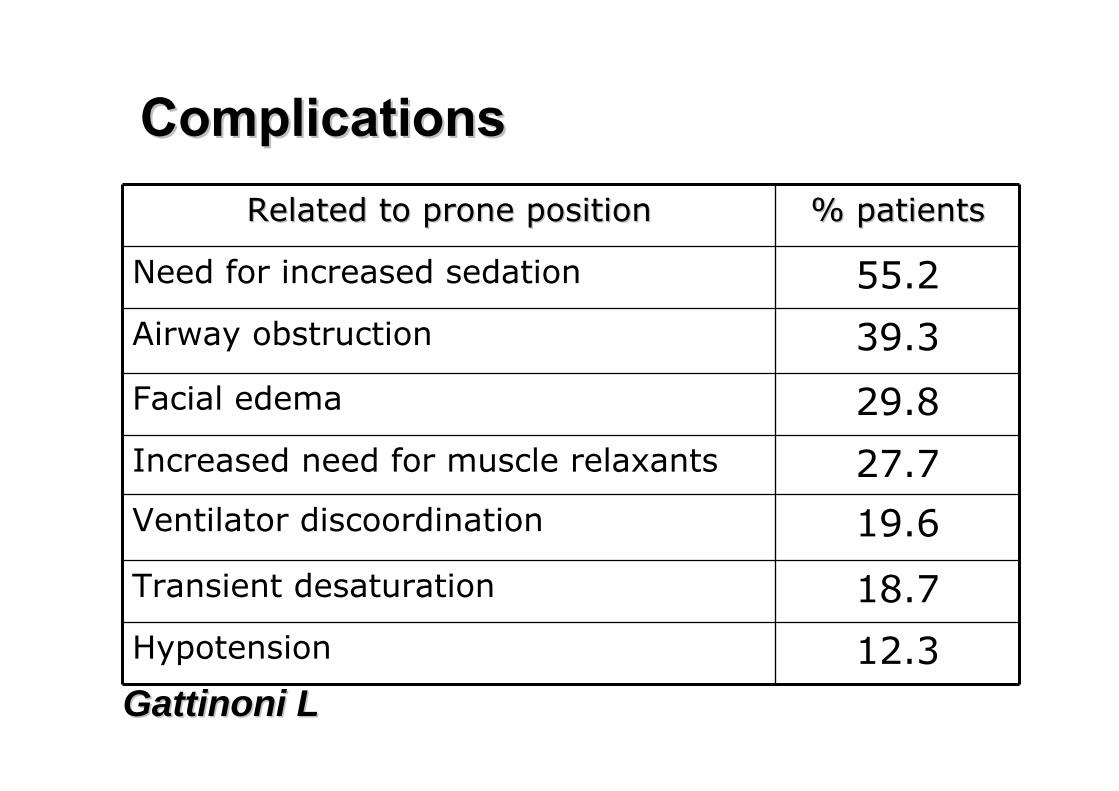
ComplicationsComplicationsRelated to prone positionRelated to prone position % patients% patients
Need for increased sedation 55.2
Airway obstruction 39.3
Facial edema 29.8
Increased need for muscle relaxants 27.7Ventilator discoordination 19.6
Transient desaturation 18.7
Hypotension 12.3GattinoniGattinoni LL

ComplicationsComplicationsSupineSupine ProneProne P ValueP Value
No. of new or worsening pressure sores/patients
1.9 + 1.3 2.7 + 1.7 0.004
Displacement of ETT(% of patients)
9.9 7.9 0.68
Loss of venous access(% of patients)
9.2 5.3 0.27
Displacement of ICD(% of patients)
0.7 3.9 0.12
GattinoniGattinoni LL

Prone Positioning (PP) Prone Positioning (PP) Mortality improvement with PP shown in
Those with the most severe hypoxemia by PaO2/FiO2 (< 88)Those exposed to high tidal volumeThose who improved CO2 exchange as a result of PP
Consider the complications associated with prone, which can be avoided with proper precaution
International guidelines for management of severe sepsis and septic shock 2008.CritCare Med 2008 ;36, 296-327

SteroidSteroid In Pediatric Septic ShockIn Pediatric Septic Shock
Suggest that hydrocortisone therapy
be reserved for use in children with catecholamine resistance and suspected or proven adrenal insufficiency
(grade 2C).
International guidelines for management of severe sepsis and septic shock 2008.Crit Care Med 2008 ;36, 296-327

Adrenal Insufficiency in Critically Adrenal Insufficiency in Critically ––Ill PatientsIll Patients
MechanismMechanism CausesCausesCentral Central Hypothalamic or pituitary disease Hypothalamic or pituitary disease
Brain injuryBrain injuryRecent steroid useRecent steroid use
Peripheral Peripheral Preexisting adrenal failurePreexisting adrenal failure
Acute adrenal failureAcute adrenal failure
Inadequate substrateInadequate substrateInterference ACTH actionInterference ACTH action
P450 impairment P450 impairment Increased clearanceIncreased clearanceGlucocorticoidGlucocorticoid receptor blockagereceptor blockageEndEnd--organ unresponsivenessorgan unresponsiveness
Associated with Associated with hyperpigmentationhyperpigmentation, hypoglycemia, , hypoglycemia, mild mild hyponatremiahyponatremia and and hyperkalemiahyperkalemia
Adrenal hemorrhage, autoimmune Adrenal hemorrhage, autoimmune adrenalitisadrenalitisLow cholesterolLow cholesterolSuraminSuraminKetoconazoleKetoconazole, , etomidateetomidate, sepsis, , sepsis, prematurityprematurity, age < , age <
6 months6 monthsRifampinRifampin, , phenytoinphenytoin, , phenobarbitalphenobarbitalMifepristoneMifepristoneCytokines decreases Cytokines decreases glucocorticoidglucocorticoid receptor receptor
sensitivity*sensitivity*
Other Sepsis / inflammationOther Sepsis / inflammation Circulating inflammatory cytokine Circulating inflammatory cytokine suppress HPA axis*suppress HPA axis*
FelmetFelmet K and K and CaicilloCaicillo J. .In : Fuhrman BP & Zimmerman J. Pediatric Critical Care.3J. .In : Fuhrman BP & Zimmerman J. Pediatric Critical Care.3rdrd ed. 2006 : 1462ed. 2006 : 1462--1473.1473.

Mechanism of Low Dose Corticosteroid Mechanism of Low Dose Corticosteroid
•• CortisolCortisol substitutionsubstitution•• AntiAnti--inflammationinflammation
Decrease Decrease ILIL--6,IL6,IL--8,soluble E8,soluble E--selectinselectinneutrophilneutrophil activationactivation
•• Increase vascular tone viaIncrease vascular tone viainhibit inducible nitric oxide inhibit inducible nitric oxide synthasesynthaseenhance adrenergic receptor expressionenhance adrenergic receptor expressionstimulate stimulate guanylateguanylate cyclasecyclase
KehD. Am J Respir Crit Care Med 2003 ; 167 : 512 - 520.
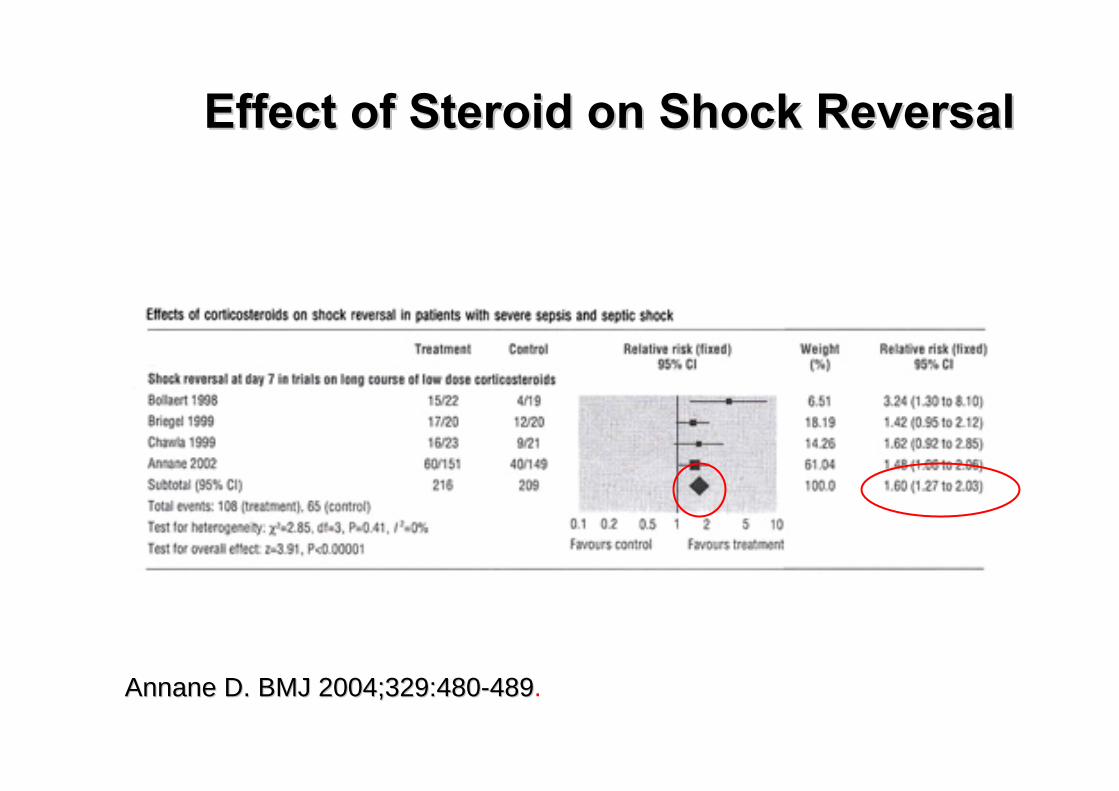
Effect of Steroid on Shock ReversalEffect of Steroid on Shock Reversal
AnnaneAnnane D. BMJD. BMJ 2004;329:4802004;329:480--489489.
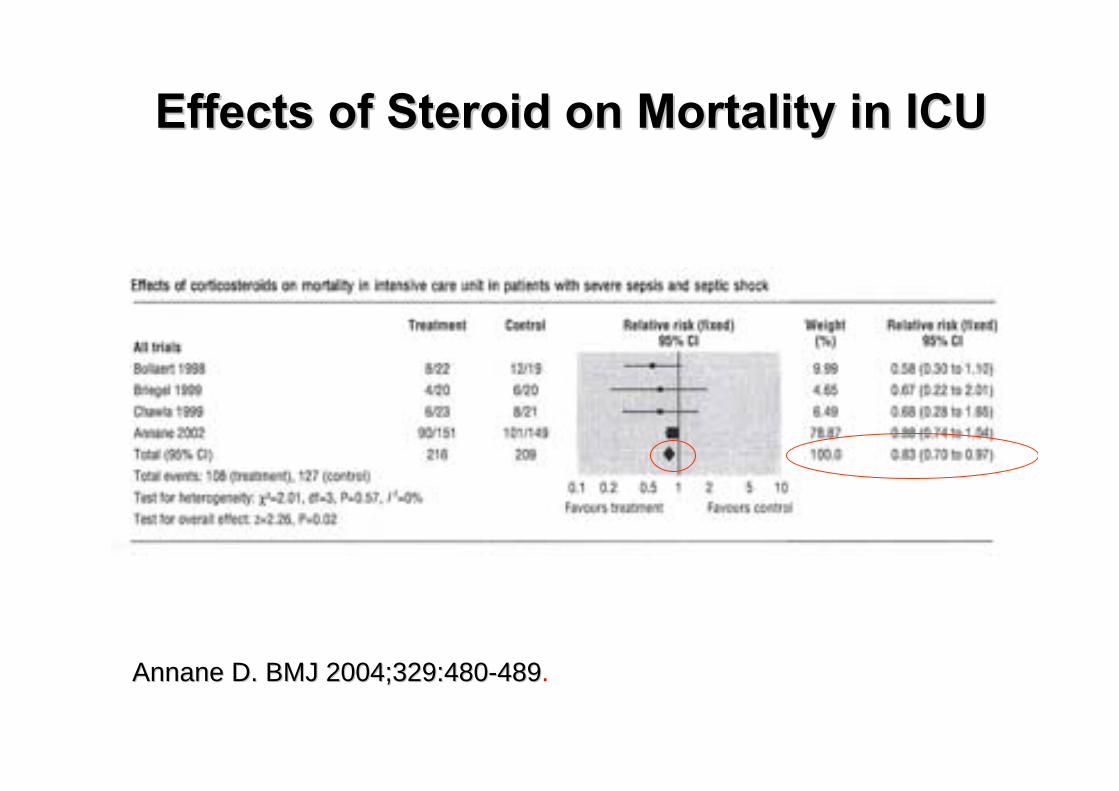
Effects of Steroid on Mortality in ICUEffects of Steroid on Mortality in ICU
AnnaneAnnane D. BMJD. BMJ 2004;329:4802004;329:480--489489.
CORTICUS StudyCORTICUS Study
European multiEuropean multi--center trial center trial
Steroid In Adult Septic Shock Steroid In Adult Septic Shock Include cases with septic shock, regardless of how Include cases with septic shock, regardless of how the blood pressure responded to the blood pressure responded to vasopressorsvasopressors
The resultsThe results
Failed to show a mortality benefitFailed to show a mortality benefitShow a faster resolution of septic shock in patients Show a faster resolution of septic shock in patients who received steroidwho received steroidThe use of the ACTH test did not predict the cases The use of the ACTH test did not predict the cases with faster resolution of shockwith faster resolution of shock
Sprung CL, Annane D. Abstr. Am Rev Respir Crit Care Med 2007; 175: A507

Retrospective Study In Pediatric Severe SepsisRetrospective Study In Pediatric Severe Sepsis
Study of prognostic factors associated with outcome in pediatric severe sepsis: What is the role of steroids?*.
6,693 pediatric patients were identified at 27 hospitals.
Conclusions: No evidence that steroids are associated with improved outcome in critically ill infants and children with sepsis. Although steroids may be given preferentially to more severely ill children,their use was associated with increased mortality (Odd ratio 1.9, 95%CI 1.7-2.2).
Markovitz.Pediatr Crit Care Med 2005; 6:270-274.

Indication of Steroid In Pediatric Septic ShockIndication of Steroid In Pediatric Septic Shock
CatecolamineCatecolamine resistance septic shock resistance septic shock Plus 1/2 itemsPlus 1/2 items1.1. Suspected adrenal insufficiency Suspected adrenal insufficiency
PurpuraPurpura fulminantfulminantPreviously received steroid Previously received steroid Pituitary or adrenal abnormalitiesPituitary or adrenal abnormalities
2.2. ProvenProven adrenal insufficiencyadrenal insufficiencyAbsolute adrenal insufficiencyAbsolute adrenal insufficiencyRelative adrenal insufficiency (Relative adrenal insufficiency (++))
International guidelines for management of severe sepsis and septic shock 2008.Crit Care Med 2008 ;36, 296-327

Proven Adrenal Insufficiency (AI)Proven Adrenal Insufficiency (AI)
1st Cortisol
2nd Cortisol
< 18 µg/dl absolute AI
< 9 µg/dl relative AI
> 9 µg/dl normal
ACTH
Pizarro CF. Crit Care Med 2005; 33: 855-859.
SteroidSteroid In Pediatric Septic ShockIn Pediatric Septic Shock
Suggest that hydrocortisone therapy
be reserved for use in children with catecholamine resistance and suspected or proven adrenal insufficiency
(grade 2C).
International guidelines for management of severe sepsis and septic shock2008. Crit Care Med 2008 ;36, 296-327
Steroid AdministrationSteroid Administration
•• Hydrocortisone 50 mg/mHydrocortisone 50 mg/m22/ 24 hr (~2 mg/kg/day)/ 24 hr (~2 mg/kg/day)
•• Add Add FludrocostisoneFludrocostisone 1 1 ugug/kg/day oral OD /kg/day oral OD (2C)(2C)(if hydrocortisone is not available and the steroid (if hydrocortisone is not available and the steroid
substituted has no significant substituted has no significant minerocorticoidminerocorticoid activity)activity)
•• Duration of treatment : several days and wean on Duration of treatment : several days and wean on
subsequent days when subsequent days when vasoprssorsvasoprssors are not required (2D)are not required (2D)
International guidelines for management of severe sepsis and septic shock 2008.Crit Care Med 2008 ;36, 296-327

Intravenous Immunoglobulin (IVIG)Intravenous Immunoglobulin (IVIG)
Suggest : polyclonal IVIG be considered in children with severe sepsis
Recent RCT in 100 pediatric patients with sepsis syndrome treated IVIG (dose 400 mg/kg/day x 3 day) showed reduction in mortality and length of stay and less progress to complications especially DIC
International guidelines for management of severe sepsis and septic shock 2008.Crit Care Med 2008 ;36, 296-327
El-Nawaway A.J Trop Pediatr 2005;51:271-278

No Graded RecommendationsNo Graded Recommendations
Glycemic control
Stress ulcer prophylaxis
Renal replacement therapy
Threshold of hemoglobin to transfuse

International guidelines for management of severe sepsis and septic shock 2008.Crit Care Med 2008 ;36, 296-327
Nadel S. Lancet 2007; 369 : 836-843
Recommend Against Recommend Against
The use The use rhAPCrhAPC in children (1B)in children (1B)
Result of a large pediatric RCT showed Result of a large pediatric RCT showed no mortality benefit with more CNS bleeding, no mortality benefit with more CNS bleeding, particularly in children younger than 60 daysparticularly in children younger than 60 days

SSC, an initiative of the European Society of Intensive Care Medicine, the International Sepsis Forum, and the Society of Critical Care Medicine, has been developed to improve the management, diagnosis, and treatment of sepsis

The SSC aims to reduce mortality from sepsis via a multi-point strategy, primarily: ◦ Building awareness of sepsis ◦ Improving diagnosis ◦ Increasing the use of appropriate treatment ◦ Educating healthcare professionals ◦ Improving post-ICU care ◦ Developing guidelines of care ◦ Facilitating data collection for the purposes of audit
and feedback

Phase I: October 2002, the Barcelona Declaration to improve survival in severe sepsis.Phase II:2003 To increase awareness and improve outcome in severe sepsis.Phase III:2006-7 To dedicated to the use of the managementguidelines to evaluate the impact on clinicaloutcome


GENERAL STRATEGIES◦ HEMODYNAMIC SUPPORT◦ ANTIBACTERIAL THERAPY◦ LOW PRESSURE VENTILATION◦ GLYCEMIC CONTROL◦ DIALYSISSEPSIS-SPECIFIC STRATEGIES◦ EARLY GOAL-DIRECTED THERAPY◦ RECOMBINANT HUMAN ACTIVATED PROTEIN C (RHAPC)◦ IMMUNOLOGICAL THERAPY - LOW-DOSE
CORTICOSTEROIDS

Quality improvement initiatives (Adults):Sepsis resuscitation bundleSepsis management bundle

The goal is to perform all indicated tasks 100% of the time within the first 6 hours of identification of severe sepsis.
The tasks are:1. Measure serum lactate2. Obtain blood cultures prior to antibiotic administration3. Administer broad-spectrum antibiotic, within 3 hrs of ED
admission and within 1 hour of non-ED admission

4. In the event of hypotension and/or a serum lactate > 4 mmol/La. Deliver an initial minimum of 20 ml/kg of crystalloid or an equivalentb. Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain mean arterial pressure (MAP) > 65 mm Hg
5. In the event of persistent hypotension despite fluid resuscitation (septic shock) and/or lactate > 4 mmol/La. Achieve a central venous pressure (CVP) of ≥ 8 mm Hgb. Achieve a central venous oxygen saturation (ScvO2) ≥70 % or mixed venous oxygen saturation (SvO2) ≥ 65 %

Efforts to accomplish these goals should begin immediately, but these items may be completed within 24hours of presentation for patients with severe sepsis or septic shock.1. Administer low-dose steroids for septic shock in accordance with a standardized ICU policy.
If not administered, document why the patient did not qualify for low-dose steroids based upon the standardized protocol.

2. Administer drotrecogin alfa (activated) in accordance with a standardized ICU policy.
If not administered, document why the patient did not qualify for drotrecogin alfa (activated).3. Maintain glucose control ≥ 70, but < 150 mg/dl4. Maintain a median inspiratory plateau pressure (IPP)* < 30 cm H2O for mechanically ventilated patients

Antibiotics◦ “We recommend” within 1 hrMechanical ventilation◦ No graded recommendationFluid resuscitation◦ “We suggest” boluses of 20 mL/kg over 5–10 mins, titrate to
clinical monitors

Vasopressors/ inotropes◦ “We suggest” dopamine as the first choice of support for the
pediatric patient with hypotension refractory to fluid resuscitation.
Therapeutic end points◦ “We suggest” that the therapeutic end points of resuscitation
of septic shock be normalization of the heart rate, capillary refill of 2 secs, normal pulses with no differential between peripheral and central pulses, warm extremities, urine output 1 mL·kg1·hr1, and normal mental status
Approach to pediatric septic shock◦ See diagramSteroids◦ “We suggest” that hydrocortisone therapy be reserved for use
in children with catecholamine resistance and suspected or proven adrenal insufficiency
Protein C and activated protein C◦ “We recommend” against the use rhAPC in children

DVT prophylaxis◦ “We suggest” the use of DVT prophylaxis postpubertal
children with severe sepsisStress ulcer prophylaxis◦ No graded recommendationsRenal replacement therapy◦ No graded recommendationsGlycemic control◦ No graded recommendations
Sedation/ analgesia◦ “We recommend” sedation protocols with a sedation goal when
sedation of critically ill mechanically ventilated patients with sepsis is required.
Blood products◦ No graded recommendationsIVIG◦ “We suggest” that immunoglobulin be considered in children with
severe sepsisECMO◦ “We suggest” that use of ECMO be limited to refractory
pediatric septic shock and/or respiratory failure that cannot be supported by conventional therapies