Embed Size (px)
Citation preview

EXPEDITED ARTICLE
Brief Reports
Transplanted DopaminergicNeurons Develop PD PathologicChanges: A Second Case Report
Jeffrey H. Kordower, PhD,1* Yaping Chu, MD,1
Robert A. Hauser, MD,2 C.Warren Olanow, MD,3
and Thomas B. Freeman, MD4
1Department of Neurological Sciences, Rush UniversityMedical Center, Chicago, Illinois, USA; 2Department of
Neurology, University of South Florida, Tampa,Florida, USA; 3Department of Neurology, Mt. Sinai Schoolof Medicine, New York, New York, USA; 4Department of
Neurosurgery, University of South Florida, Tampa,Florida, USA
Abstract: This report describes pathological changeswithin the grafted neurons of another patient with Par-kinson’s disease (PD) who died 14 years posttransplanta-tion. Although numerous healthy appearing grafted neu-rons were present at this long-term time point, somedisplayed Lewy bodies as evidenced by alpha-synuclein,ubiquitin, and thioflavin-S staining. Additionally, therewas a general loss of dopamine transporter-immunoreac-tivity in grafted neurons. Some grafted cell displayed aloss of tyrosine hydroxylase. These data support theemerging concept that PD-like pathology is seen in younggrafted neurons when they survive long term. � 2008Movement Disorder Society
Key words: transplantation; substantial nigra; Lewy body
A series of 3 recently reported papers described
pathologic findings in patients with Parkinson’s disease
(PD) who had undergone fetal nigral transplantation 10
to 16 years prior.1–3 Two studies demonstrated that
substantial numbers of implanted dopaminergic neu-
rons contained inclusions that stained for ubiquitin and
alpha-synuclein and were identical to Lewy bodies.
The third reported healthy appearing grafted cells with
no inclusions,3 however subsequent analyses revealed
rare ubiquinated Lewy bodies within the graft of one
of their cases (O. Isacson, presented at the Michael J.
Fox Workshop, 2008). We now report the results of a
postmortem study on another individual with PD who
died 14 years after fetal nigral transplantation.
CASE REPORT
MK was a 38-year-old man at the time of diagnosis
followed by a 25-year progression of PD at which time
informed consent was obtained for bilateral fetal trans-
plantation.4 The patient initially had a good response
to levodopa therapy, but benefits were compromised by
severe motor complications that could not be satisfac-
torily controlled with manipulation of antiparkinsonian
medications. In June and July of 1994, the patient
underwent bilateral fetal nigral transplant procedures
using solid grafts derived from four donors aged 6.5 to
9 weeks post-conception per side. The patient enjoyed
substantial improvement for 12 years, but deteriorated
thereafter, and died 2 years later on May 18, 2008. Au-
topsy was obtained with a 3-hour-postmortem interval.
POSTMORTEM EXAMINATION
The brain was processed as previously described.5
Gross examination was unremarkable except for typical
PD pathology including depigmentation of the substan-
tia nigra pars compacta (SNc) and locus coeruleous.
On microscopic examination, there was profound loss
of tyrosine hydroxylase (TH) and melanized neurons in
the SNc coupled with characteristic intracytoplasmic
Lewy bodies which stained positively for ubiquitin,
alpha-synuclein, and thioflavin-S.
Within the left striatum there was robust survival of
implanted neurons in all graft deposits. In the right
striatum there were surviving graft deposits, but, there
were considerably fewer melanin or TH-positive cells.
These cells displayed classic morphology of midbrain
dopaminergic neurons with age-appropriate melanin
content. Grafts gave rise to large numbers of axons
that extensively innervated the postcommissural puta-
men in an organotypic manner as we have previously
Potential conflict of interest: None reported.
*Correspondence to: Dr. Jeffrey H. Kordower, Department of Neu-rological Sciences, Rush University Medical Center, 1735 West Har-rison Street, Chicago Illinois 60612, USA.E-mail: [email protected]
Received 12 September 2008; Revised 1 October 2008; Accepted3 October 2008
Published online 12 November 2008 in Wiley InterScience
(www.interscience.wiley.com). DOI: 10.1002/mds.22369
2303
Movement DisordersVol. 23, No. 16, 2008, pp. 2303–2306� 2008 Movement Disorder Society

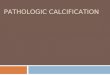
FIG. 1. Low- (A) and (B) high-power photomicrographs illustrating the robust immunoreactivity was seen within grafted neurons for VMAT2.In contrast (C,D) spare immunoreactivity was seen within grafted neurons stained for DAT. For the most part, grafted neurons displayed robustTH (E,F). (G) However, some melanin-containing grafted neurons failed to express TH (arrows). Scale bar in G represents the following magnifi-cations: 160 lm for A and C; 320 lm for E; 25 lm for B, D, F, and G.
2304 J.H. KORDOWER ET AL.
Movement Disorders, Vol. 23, No. 16, 2008

described. Virtually all grafted neurons stained posi-
tively for vesicular monoamine transporter 2 (VMAT2;
Fig. 1A,B). However, there was very little staining for
dopamine transporter (DAT; Fig. 1C,D) in all graft
deposits with some displaying virtually none. Although
most implanted cells stained positively for TH (Fig.
1E,F), many did not (Fig. 1G), in contrast to our previ-
ous findings. Within a minority of grafted melanin con-
taining neurons there were large intracellular inclusions
that stained for ubiquitin, alpha-synuclein, and Thiofla-
vin-S (Fig. 2). These were identical in staining pattern
and morphology to Lewy bodies found in the host
nigra (Fig. 2). Confocal microscopy confirmed that
inclusions were localized to grafted TH-positive dopa-
minergic cells. Lewy neurites were rarely encountered.
This staining pattern was similar within grafts bilater-
ally. Staining for CD45 cells demonstrated robust
expression, but was more marked on the right side
(data not shown).
DISCUSSION
This case demonstrates that dopamine neurons
implanted into the striatum of a patient with PD can
survive and reinnervate the striatum as we and others
have previously reported.1–3,5–7 Indeed, this observa-
tion has given hope to the concept that dopamine
transplantation strategies might prove beneficial for
patients with PD. It is now becoming clear, however,
that at least after some period of time, fetal nigral cells
implanted into the brain of patients with PD can
undergo the classical pathological changes of the disor-
der; namely, loss of DAT,8 loss of TH,9 and Lewy
body formation (e.g., Refs. 1–3). There can be no
doubt that these were grafted cells as they were located
within the graft borders within the striatum, contained
neuromelanin, displayed morphologic features of nigral
neurons and did not resemble endogenous striatal do-
pamine neurons. This observation confirms two previ-
ous reports which demonstrate similar PD pathology in
FIG. 2. Low- and high-power photomicrographs through the transplant stained for (A,B) alpha-synuclein, (D,E) ubiquitin, and (G,H) thioflavin-Swhich are morphologically indistinguishable from nigral neurons stained for (C) alphasynuclein, (F) ubiquitin, and (I) thioflavin-S in the hostnigra. Scale bar in I represents the following magnifications: A, D 5 160 lm; 5 lm for B, C, E, and F 5 5 lm; G 5 80 lm, and H, I 5 12 lm.
2305PD PATHOLOGIC CHANGES
Movement Disorders, Vol. 23, No. 16, 2008

patients undergoing postmortem examination �1 dec-
ade after transplantation.1,2 These phenotypic and mor-
phological changes also raise the possibility that these
cells were dysfunctional and might thereby account for
why transplantation has, to date, failed to provide ben-
efit in double blind clinical trials.
It is interesting to speculate on why these pathologi-
cal changes might have developed. The most parsimo-
nious explanation is that PD is an ongoing process that
can affect dopaminergic neurons despite their relatively
young age and ectopic location. It is noteworthy that
the classical changes of PD were found in implanted
neurons that were only 10 to 16 years of age and
would not be expected to manifest any of these
changes on the basis of normal aging alone. Alterna-
tively, it is possible that cell injury from some other
pathogenic factor might have damaged these implanted
cells and reproduced PD pathology but as a conse-
quence of an alternate etiology. In this regard, it is
noteworthy that there is evidence of increased CD45
expression and that it is more pronounced on the side
that was more affected. CD45 is a protein tyrosine
phosphatase, which has been shown to be an essential
regulator of T- and B-cell antigen receptor signaling. It
functions through either direct interaction with compo-
nents of the antigen receptor complexes, or by activat-
ing various Src family kinases required for the antigen
receptor signaling. Thus, we use this antibody as a
general marker of an immune response. It is also inter-
esting to note that implanted neurons were derived
from four different donors that were unrelated to the
recipient. This indicates that PD changes can develop
in neurons solely as a consequence of their environ-
ment and indicates that genetic factors are not required
in order for these changes to become manifest.
This case illustrates several other important features.
Firstly, Reduced DAT staining was seen bilaterally and
was much more pronounced than the reduction seen in
TH staining. This is similar to what we observed in
our previous case and suggests that this may represent
an earlier manifestation of dopaminergic injury and
may occur as a compensatory response to reduced do-
paminergic transmission over time. Indeed, DAT
serves to facilitate reuptake of dopamine from the syn-
apse and decreased DAT in grafted neurons may be a
response intended to enhance functional dopamine at
the synapse. On the other hand, staining for VMAT
was preserved in both of our cases suggesting that it is
a less sensitive index of cell injury than either TH or
DAT. This has important implications for brain imag-
ing of patients with PD and should be pursued.
In conclusion, although this is a single case report it
confirms that implanted cells can undergo neurodege-
nerative change in patients with PD and has important
implications for both PD pathogenesis and the future
of cell replacement therapies.
REFERENCES
1. Kordower JH, Chu Y, Hauser RA, Freeman TB, Olanow CW.Lewy body-like pathology in long-term embryonic nigral trans-plants in Parkinson’s disease. Nat Med 2008;14:504–506.
2. Li JY, Englund E, Holton JL, et al. Lewy bodies in grafted neu-rons in subjects with Parkinson’s disease suggest host-to-graftdisease propagation. Nat Med 2008;14:501–503.
3. Mendez I, Vinuela A, Astradsson A, et al. Dopamine neuronsimplanted into people with Parkinson’s disease survive withoutpathology for 14 years. Nat Med 2008;14:507–509.
4. Hauser RA, Freeman TB, Snow BJ, et al. Long-term evaluationof bilateral fetal nigral transplantation in Parkinson’s disease.Arch Neurol 1999;56:179–187.
5. Kordower JH, Rosenstein JM, Collier TJ, et al. Functional fetalnigral grafts in a patient with Parkinson’s disease: chemoana-tomic, ultrastructural, and metabolic studies. J Comp Neurol1996;370:203–230.
6. Kordower JH, Styren S, Clarke M, DeKosky ST, Olanow CW,Freeman TB. Fetal grafting for Parkinson’s disease: expression ofimmune markers in two patients with functional fetal nigralimplants. Cell Transplant 1997;6:213–219.
7. Mendez I, Sanchez-Pernaute R, Cooper O, et al. Cell type analy-sis of functional fetal dopamine cell suspension transplants in thestriatum and substantia nigra of patients with Parkinson’s disease.Brain 2005;28(Part 7):1498–1510.
8. Panzacchi A, Moresco RM, Garibotto V, et al. A voxel-basedPET study of dopamine transporters in Parkinson’s disease: rele-vance of age at onset. Neurobiol Dis 2008;31:102–109.
9. Chu Y, Le W, Kompoliti K, Jancovic J, Mufson EJ, KordowerJH. Nurr1 in Parkinson’s disease and related disorders. J CompNeurol 2006;494:495–514.
2306 J.H. KORDOWER ET AL.
Movement Disorders, Vol. 23, No. 16, 2008


























![[18F]Fluorodopa PETshows striatal dopaminergic dysfunction](https://img.pdfslide.net/doc/110x75/628e71a806be7c7a267428b6/18ffluorodopa-petshows-striatal-dopaminergic-dysfunction-.jpg)