Embed Size (px)
Citation preview
Trauma Informed Systems Initiative San Francisco Department of Public Health
2014 Year in Review

Trauma Informed Systems Initiative
1
Trauma Informed Systems Initiative San Francisco Department of Public Health
2014 Year in Review
A Trauma Informed Public Health System for San Franciscans
Trauma is a pervasive, long-lasting, public health issue that affects our public health workforce and system. In
recent years the devastating impact of trauma on individuals, families and communities has drawn considerable
attention from service providers, researchers and policy makers. Like people, organizations are also susceptible
to trauma that affects its workforce in dynamic ways that contribute to fragmentation, numbing, reactivity and
depersonalization. When our systems are traumatized, it prevents us from responding effectively to each other
and the people we serve. The San Francisco Department of Public Health has developed a Trauma Informed
Systems Framework intended to help improve organizational functioning, increase resilience and improve
workforce experience. Our Trauma Informed Systems Workgroup, made up of staff and DPH employees is
leading this change effort, which includes the following components:
• Mandatory, foundational training to all 9,000 public health employees to create a shared language and
understanding of trauma for our workforce
• Development of an embedded Champions Learning Community (CLC) to support, apply and sustain the
application of the TIS principles and practices into the entire DPH workforce.
• Train the Trainer program to embed and harness trauma expertise with in our system and establish a
permanency of the initiative.
• Intentional efforts to align TIS with all our workforce and policy initiatives to insure TIS implementation
increases coherence, unifies our system and improves outcomes.
• Leadership Engagement and outreach to support leaders to integrate TIS principles into day-to-day
operations as well as promote system change at the program and policy level.
• Work towards establishing San Francisco as a Trauma Informed City insuring that the entire workforce
has a common language and principles.
Rationale
Trauma is broadly experienced, pervasive and has can have long lasting effects. We know from the growing
body of research on trauma, that the majority of Americans will experience a traumatic event at some point in
their lifetime1.
1 Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Koss MP, Marks JS. Relationship of childhood abuse and household dysfunction
to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. American Journal of Preventive Medicine 1998;14:245–258.
Trauma Informed Systems Initiative
2
“A system cannot be
truly trauma-informed
unless the system can
create and sustain a
process of
understanding itself. A
program cannot be safe
for clients unless it is
simultaneously safe for
staff and safe for
administrators. Lacking
such a process and
despite well-intentioned
training efforts, there
will be no true system
transformation in
systems that are now
for the most part,
“trauma organized”
repeating, rather than
healing, the injuries
previously experienced
by clients and staff “
-Sandra Bloom*
Getting its initial momentum from the work of Vietnam veterans, their
families, mental health professionals and clergy, the field of trauma has
grown in the past 3 decades. In the 1980’s and 1990’s a significant body
of research accumulated to validate the connection between a past
history of trauma, substance abuse and mental illness. Subsequently,
programs that specialized in trauma began to spring up through out the
country, publishing their research and creating the foundation for what
we know now about effective treatment for traumatized people and
necessary elements for recovery. 2 The subject of trauma, also sometimes
called "toxic stress" has attracted lots of energy in the mental health and
public health fields, partly because of a few very high profile studies
linking trauma to major health problems and relationship difficulties. The
Adverse Childhood Experiences Study (ACEs Study) for example, showed a
clear connection between how many ACE’s one has experienced (the
trauma-dose) and long-term, social problems and chronic illnesses like
heart disease, cancer, and diabetes. While the effects of toxic stress are
experienced broadly, disparities in health outcomes are acutely
experienced in disenfranchised communities suffering the long-term
effects of specific traumas such as community violence coupled with the
long-term effects of institutional discrimination, poverty, lack of access to
adequate resources. Addressing trauma for public health must be a top
priority. San Francisco’s Trauma Informed Systems (TIS) Initiative extends
the focus on the impact of toxic stress and trauma from the community
receiving services to the system delivering services.
A Trauma Informed System: Etiology and Recovery
The mission of the public health system at its most basic level is to
promote and protect the wellness of our community. The San Francisco
Department of Public Health has identified these objectives3 as a pathway
to this mission:
Assess and research the health of the community
Develop and enforce healthy policy
Prevent disease and injury
Educate the public and train health care providers
Provide quality, comprehensive, culturally-proficient health services
Ensure equal access to all
2 Jennings, A. (2008 Update). Models for Developing Trauma-Informed Behavioral Health Systems and Trauma-Specific Services. National Center for Mental Health Services, National Center for Trauma Informed Care, Funded by SAMSHA. 3 From www.sfdph.org. 2012-2013 Annual Report. San Francisco Department of Public Health *From Bloom. S (2010). Organizational Stress as a Barrier to Trauma Informed Service Delivery. Becker, M. Levine, B. A Public Health Perspective of Women’s Mental Health: New York, Springer (pp. 295-311)
Trauma Informed Systems Initiative
3
Trauma Informed Systems principles and
practices support reflection in place of reaction,
curiosity in lieu of numbing, self-care instead of
self-sacrifice and collective impact rather than
siloed structures.
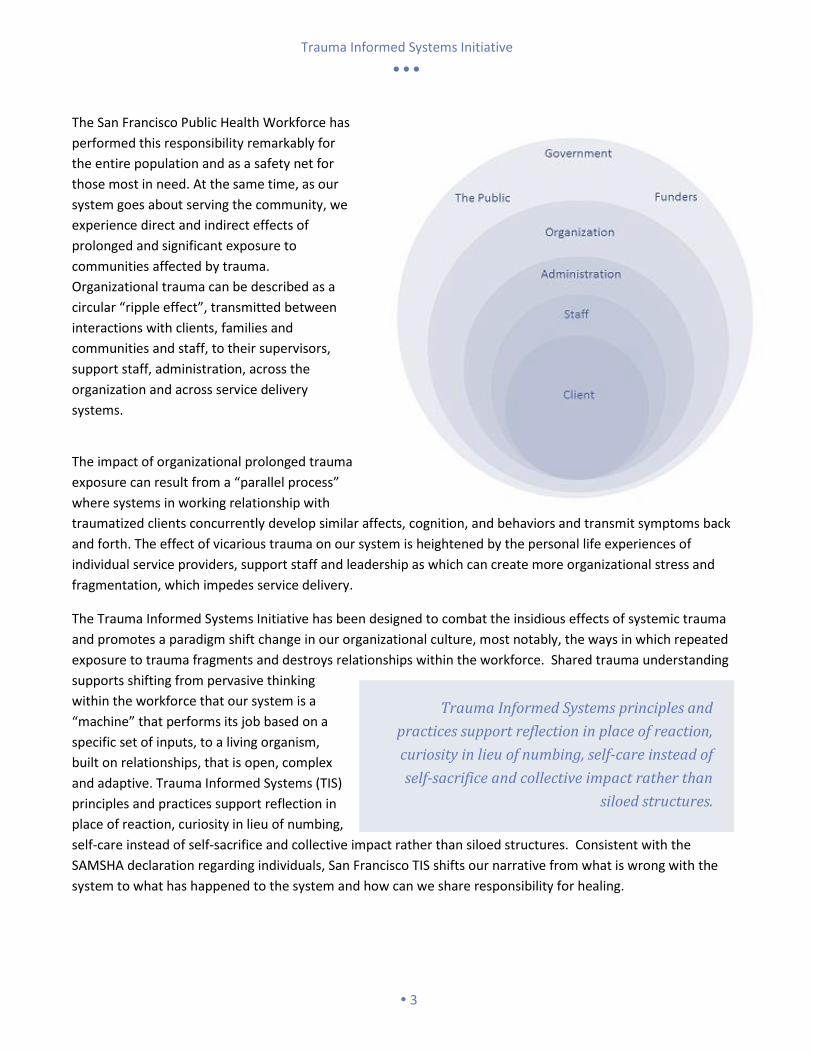
The San Francisco Public Health Workforce has
performed this responsibility remarkably for
the entire population and as a safety net for
those most in need. At the same time, as our
system goes about serving the community, we
experience direct and indirect effects of
prolonged and significant exposure to
communities affected by trauma.
Organizational trauma can be described as a
circular “ripple effect”, transmitted between
interactions with clients, families and
communities and staff, to their supervisors,
support staff, administration, across the
organization and across service delivery
systems.
The impact of organizational prolonged trauma
exposure can result from a “parallel process”
where systems in working relationship with
traumatized clients concurrently develop similar affects, cognition, and behaviors and transmit symptoms back
and forth. The effect of vicarious trauma on our system is heightened by the personal life experiences of
individual service providers, support staff and leadership as which can create more organizational stress and
fragmentation, which impedes service delivery.
The Trauma Informed Systems Initiative has been designed to combat the insidious effects of systemic trauma
and promotes a paradigm shift change in our organizational culture, most notably, the ways in which repeated
exposure to trauma fragments and destroys relationships within the workforce. Shared trauma understanding
supports shifting from pervasive thinking
within the workforce that our system is a
“machine” that performs its job based on a
specific set of inputs, to a living organism,
built on relationships, that is open, complex
and adaptive. Trauma Informed Systems (TIS)
principles and practices support reflection in
place of reaction, curiosity in lieu of numbing,
self-care instead of self-sacrifice and collective impact rather than siloed structures. Consistent with the
SAMSHA declaration regarding individuals, San Francisco TIS shifts our narrative from what is wrong with the
system to what has happened to the system and how can we share responsibility for healing.
Trauma Informed Systems Initiative
4
Approach
San Francisco Department of Public Health has chosen an innovative approach to responding to the impact of
trauma that starts with our own workforce, develops embedded leadership within our system and increases our
capacity to have productive conversations about what it means to be a Trauma Informed organization. In
September of 2012, San Francisco Department of Public Health’s Director, Barbara Garcia commissioned a
workgroup led by Dr. Ken Epstein, Director of Children, Youth and Families, to initiate an exploration of how our
Department of Public Health system could benefit from and take preliminary steps to become a Trauma
Informed System. Under a model of participatory leadership, the work group of subject matter experts from
within our system began the vetting process through focus groups and presentations throughout our system.
To date, the vetting process has included over 400 people within our public health system including providers,
non-providers, primary care and various peer and advocacy groups. Feedback, suggestions and observations
from these meetings has guided the development process from the beginning. Out of this process a formal
response was born in the Trauma Informed Systems Initiative.
Trauma Informed Systems Initiative Workgroup
The Trauma Informed Systems Initiative Workgroup is led by Dr. Ken Epstein and currently staffed by a full time
Coordinator, a team of 4 interns, a work group of subject matter experts and the support of the Community
Behavioral Health Services Training Department. The Initiative has based its change efforts on the Trauma
Informed System’s Principles and Competencies developed by the work group:
• Trauma Understanding
• Cultural Humility & Responsiveness
• Safety & Stability
• Compassion & Dependability
• Collaboration & Empowerment
• Resilience & Recovery
These six principles provide the framework for the foundational training curriculum as well as the starting place
for considering our staff to staff relationships, our programs and policies.4 Although the formal workforce
training is a major component of the initiative’s theory of change, we believe the implementation of long term
support and sustainable structures for knowledge transfer are the key to organizational change.
Implementation
The Trauma Informed Initiative is a six-pronged approach to developing, sustaining change in organizational and
workforce functioning.5 In addition to training for the entire workforce, TIS is utilizing the principles of
implementation science to insure that knowledge transfer is associated with structures that support
commitment to change, embedded champions, alignment and collaboration within and across systems,
4 For a the Trauma Informed Systems Principles and Competencies full document, see the appendix 5 For an the Trauma Informed Systems Program Structure, see the appendix

Trauma Informed Systems Initiative
5
Early Innovators
Laguna Honda Hospital and Rehabilitation Center Minority AIDS Initiative - Targeted Capacity Expansion Program (MAI-TCE), Ward 86, San Francisco General Hospital Primary Care Physicians, Community Behavioral Health Medical Providers, San Francisco Health Network
leadership participation and continuous evaluation. 6Below are brief examples of our current efforts in these
areas.
Workforce Training: Shared Understanding & Commitment To Change
In order to promote a shared culture, we must have a shared language and
understanding and begin to generate a commitment to change at all levels of the
organization. In this regard over a 24-month period the entire Department of
Public Health workforce of approximately 9,000 employees will receive
foundational information about the effects of trauma and some tools to initiate
change. The training initiates a system-wide conversation about the impact of
trauma and to build a common language with which to discuss incorporation of the trauma informed principles
across all levels of our public health system. After extensive vetting the TIS half-day, interactive training was
piloted on February 25, 2014 with Community Behavioral Health Leadership. By year-end 2014, 27 trainings
were offered in a total of three sites with morning and afternoon options, including the African American
Cultural Center and Laguna Honda Hospital. The training includes didactic sections, break outs groups and ends
with a Commitment to Change section where participants are asked to generate ideas about how to integrate
the trauma informed principles in their daily work life. Two evaluation tools are collected from participants at
each training:
A training evaluation designed to collect participant input on the training content, support for the trauma
informed systems initiative and ideas on how to improve the training.
A Commitment to Change form which collects participants’ specific commitments to integrate trauma
informed principles into their work life. These forms are filled out on
carbon copies: one for participants to keep and one collected for the
evaluation team.
The results of evaluations collected from March 27, 2014 through
September 25, 2014 can be found in the appendix.
Participants
Approximately 1,700 DPH employees have participated in the
Trauma Informed Systems workforce training since its first official
offering on March 27, 2014 following the pilot. The majority of
trainings were comprised of staff who registered themselves
based on their availability, resulting in a wide-variety of roles and
departments experiencing the training together. Several trainings
were initiated by leaders of departments or sections for staff to
6 Fixsen DL, Naoom SF, Blase, KA, Friedman, RM, Wallace, F. (2005) Implementation research: A synthesis of the literature. Tampa, FL: University of South Florida.
Workforce Training
Statistics 2014
27 Trainings 3 Locations
1787 Participants

Trauma Informed Systems Initiative
6
attend together, which resulted in groups of Early Innovators who committed to training and thinking together
about how to implement Trauma Informed principles in their context.
San Francisco General Hospital is currently working with our training and coordination team to offer a series of
trainings on site for their employees in 2015.
Alignment, Collaboration & Sustainability
Trauma informed systems work highlights the need for thoughtful, collaborative approaches to the complex
problems we are presented with as a public health workforce. In an effort to promote the principle of
Collaboration and Empowerment, the Trauma Informed Systems Initiative continues to foster collaborations
with other initiatives with in DPH and throughout the city and the region.
Alignment within DPH
Service Excellence and Relationship Centered Communication (RCC): RCC training is a staff development model that emphasizes safety, respect, support, and nurturing to achieve seismic shifts in how staff relate to each other and to clients. TIS has been working with RCC to pilot the integration of TIS into RCC. On June 6, 2014, we piloted a pairing of our Trauma Informed Systems Initiative workforce training and a Service Excellence training with Community Behavioral Health Psychiatrists. Behavioral Health is currently working on expanding this pilot in calendar year 2015
Black and African American Health Initiative (BAAHI): Ken Epstein has participated in the initiative to insure
that TIS aligns with the department’s efforts to address institutional disparities impacting African American
staff and the Health Disparities in the African American Community.
Cultural Humility: TIS has consulted with Dr. Ken Hardy since inception to help understand and incorporate a
systemic approach to TIS with a deeper understanding of the impact of racism on delivery systems and
communities and the connection with trauma. In addition, TIS has now initiated consultation with Dr.
Melanie Tervalon regarding the cultural humility section of the training.
Training and Workforce Development: TIS has participated in workforce development representing TIS.
Particular focus has been on understanding and aligning the workforce satisfaction survey with TIS evaluation
strategies. In addition the Training and Workforce Development department has participated in the core-
coordinating group since inception.
Systems of Care Collaboration
Now a leader in the field of Trauma Informed Systems work, SFDPH is providing leadership to the other agencies
with in San Francisco and throughout the Bay Area.
TIS is actively working with other city departments to discuss expanding the training city wide. This includes:
Juvenile Probation, SFUSD, First Five, DCYF, HSA, and SFPD.
TIS has produced early innovator trainings for the San Francisco Child Abuse Prevention Center and HSA
which included staff and leadership across systems such as Juvenile Justice, SFPD, District Attorney’s Office,
SFUSD and Child Welfare.
TIS has been working with several early innovator CBO’s to further expand the training.
Trauma Informed Systems Initiative
7
“Never doubt that a small
group of committed citizens
can change the world. Indeed
it is the only thing that ever
has.”
– Margaret Mead
San Francisco as a lead agency has been awarded a 4 year SAMSHA grant to help develop a Trauma Informed
Region including Children, Youth and Family Systems of Care from seven bay area counties. See Appendix for
an Executive Summary of the proposal awarded.
TIS has met with numerous foundations interested in either funding, expanding and coordinating efforts with
TIS. See Appendix for a full list.
Nationally TIS has established a consultation workgroup including other localities that are early innovators in
developing Trauma Informed Systems of Care, including Philadelphia, Maine, Upstate New York and San
Diego. San Francisco’s implementation is the only one that is embedded, lead and implemented by a public
agency.
Champions
Organizational change depends on embedded champions at all
levels of the organization. Champions help transmit ideas, pilot
changes and inspire others to support adoption of the principles and
practices. Champions have emerged since we initiated TIS and they
have informed the development of the training and shared ideas
about implementation. Since the very first workforce training, DPH
staff who have attended the training have been contacting our
workgroup with inspiring ideas for bringing trauma informed
principles to their own workplace. These Champions have come
from departments all across our system, various levels and roles and
all with a unique relationship to the impact of trauma in our workforce and the community we serve. Our first
Champions Meeting was held on November 14, 2014 at 1380 Howard Street and December 16, 2014 at 25 Van
Ness Ave, and attended by 34 inspiring members of our public health workforce. This first meeting included the
practice of Sandra Bloom’s Community Meeting Structure, an framework for trauma informed staff meetings,
and a sampling of a Relationship Centered Communication technique for quickly promoting relationship building
with clients or co-workers.
Still in the program development phase, the Champions Program will be shaped and built upon the research and
findings of a team of students from the University of California, Berkeley’s School of Social Welfare who are
currently conducting research on effective models for staff-led, organizational change. With the findings from
their research and an ongoing collaboration with Relationship Centered Communication, our founding
champions and initiative workgroup will continue to develop this instrumental piece of implementation in 2015.
Leadership
TIS was initiated as a mandatory training by Barbara Garcia, Public Health Director. The next challenge for
leadership is to incorporate all levels of leadership into participating supporting and utilizing the principles and
practices of TIS. One of the most striking results from our Six-Month Evaluation Report7 is the workforce’s
7 Fields-Loomis, B. (2014) Trauma Informed Systems Initiative Six Month Evaluation Report: March 27, 2014 – September 29, 2014. San Francisco Department of Public Helath. See Appendix I for Full Report.
Trauma Informed Systems Initiative
8
overwhelming support for the initiative coupled with the belief that the initiative will be “poorly implemented or
abandoned”. The leadership initiative has thus far taken the following steps:
Regular meetings with the Public Health Cabinet to report on progress and to receive directives and guidance on implementation and strategies for spread.
Meet with leadership teams in every area of DPH. Prior to training at Laguna Honda, Population Health and Ambulatory care TIS met with the leadership team to describe the training, answer questions and to discuss next steps. Next we will meet with SF General. This process will need to be repeated regularly to access implementation progress and report on the evaluation.
Children, Youth and Families has piloted incorporating TIS into the system of care including picking priority principles and aligning the 14/15 work plan within the scope of TIS.
Documents suggested for leadership use can be found in the appendix of this report.
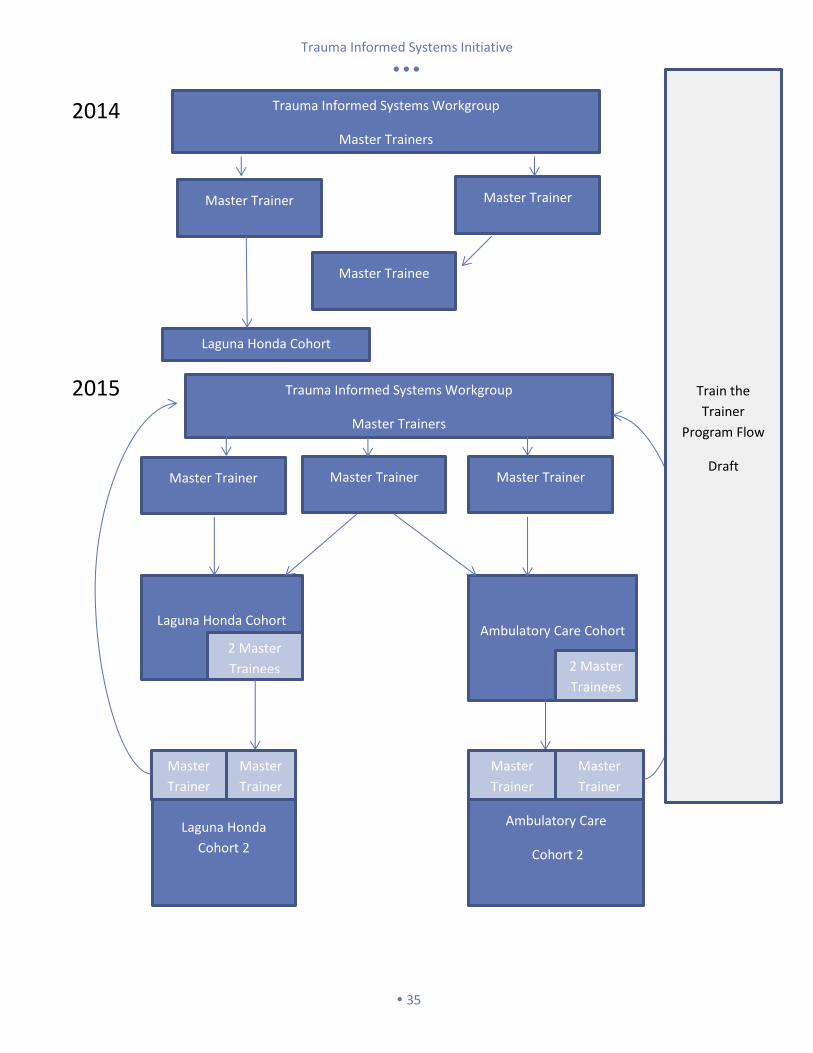
Train the Trainer
Through our vetting process we discovered what we had already suspected: that there already exists significant
expertise with in our department on trauma and system change, but that access to these sources of expertise
varies across our system. Our approach to the Train the Trainer component remains consistent with our theory
of change; that embedded, sustained support is crucial to the success of the wide-scale adoption of our
principles and system-wide understanding of trauma. The vision for Train the Trainer is to create embedded
trauma informed experts and leaders with in our organizations that can lead the transfer of knowledge. This
approach is not dependent on resources to fund outside consultants and creates a flexible, efficient and more
effective model for training and sustaining trauma informed principles.
The trauma informed principles of recovery and resiliency will remain integrated into our process of teaching
and recruiting trainers. We remain committed to our values of social justice and promoting health equity in the
development of trainers. Seeking to re-define what we traditionally consider “expert knowledge” on trauma we
encourage academics, medical professionals and those with lived-experience to apply for the program and value
their unique contribution to the education of our workforce. In the spirit of the Collaboration and
Empowerment principle, trainers will deliver the content in pairs of according to complimentary knowledge on
trauma.
In September of 2014, we began our first Train the Trainer cohort comprised of eight Laguna Honda Hospital
employees: nurse educators, training specialist and lived-experience experts. This training cohort is set to
complete the program in 2015. Commencement of our next cohort for is set for Spring 2015.8
Evaluation
An evaluation program designed to measure staff’s individual experience of the foundational training, readiness
and support for change and in implementing the trauma informed principles in their daily work life. The full
report in included in the appendix.
8 For a conceptual draft of the Train the Trainer Program Flow, see the Appendix

Trauma Informed Systems Initiative
9
Conclusion
Trauma exacts a great toll on San Franciscans, their families and communities; and in turn impacts our public
health system, its leaders, clinicians and staff. It can compromise the well being of our workforce, interactions
with one another, and the care we provide to our already vulnerable clients. Over the past year, the Trauma
Informed Systems Initiative has rolled out a feasible, very promising and sustainable approach. To date, over
20% of our workforce have been trained with an overwhelmingly positive response to the training, the call to
change, and empowerment to apply the TIS principles at all levels. Breaking the echoing cycle of personal to
organizational trauma in our system, across other City Agencies and throughout the San Francisco Bay Region is
within reach.
Trauma Informed Systems Initiative
10
Appendix Directory
Trauma Informed Systems Initiative, SFDPH
I. Trauma Informed Six-Month Data Report: March 27, 2014- September 29, 2014
II. Trauma Informed Principles and Competencies
III. Initiative Workgroup & Students
IV. Initiative Program Structure
V. Train the Trainer Conceptual Program Flow Draft
DPH Trauma Informed Leadership
VI. Bay Area Trauma Informed System of Care (BATISC) Executive Summary
VII. List of Interested Foundations

Trauma Informed Systems Initiative
11
SAN FRANCISCO DEPARTMENT OF PUBLIC HEALTH
Trauma Informed System Initiative: Six Month Data Report
March 27th, 2014 – September 25th, 2014
Prepared by Briana Loomis, PhD
October 23rd, 2014
Trauma Informed Systems Initiative
12
Contents
Feedback on Trauma 101 Training .............................................................................................................. 13 Immediate Impressions of Training Experience ................................................................................................................13
Overall Course ...............................................................................................................................................................13
Professional Relevancy ..................................................................................................................................................13
Objectives ......................................................................................................................................................................13
Speaker ..........................................................................................................................................................................14
Level of Educational Activity Content ............................................................................................................................14
Cultural and Linguistic Competency ..............................................................................................................................14
Commercial Bias ............................................................................................................................................................14
Improving the Trauma 101 Training ..................................................................................................................................15
Most Liked Components ................................................................................................................................................15
Least Liked Components ................................................................................................................................................16
Suggestions for Improvement .......................................................................................................................................18
Trauma 101 Training Data Snapshot .................................................................................................................................19
Feedback on the Trauma Informed System Initiative .................................................................................. 20
Support for TIS Initiative ....................................................................................................................................................20
Ideas for becoming a Trauma Informed System ...............................................................................................................21
Trauma Informed System Practice Change .................................................................................................. 23
Participant Identified Practice Changes ............................................................................................................................23
Commitment to Change (CTC) Project ..............................................................................................................................24
CTC Goals .......................................................................................................................................................................24
Participant Success with Implementing CTC Goals .......................................................................................................25
Participant Comments on CTC Experience ....................................................................................................................26

Trauma Informed Systems Initiative
13
Feedback on Trauma 101 Training
Immediate Impressions of Training Experience All scale based items used a 1 to 5 rating scale with 1=Disagree Most and 5=Agree Most. Sample sizes for items vary based on response rate and are provided for reference.
Overall Course (n=866): Averaged across all 14 training dates, participants gave the course a moderately high overall rating (“agree” 4.33 out of 5).
Participant Overall Course ratings were significantly related to their perceptions of course Relevancy to their work and also strongly correlated with perceptions of how well the course achieved its Objectives and overall impressions of the Speaker.
Professional Relevancy (n=883): Averaged across all 14 training dates, participants reported a moderately high level of agreement (“agree” 4.19 out of 5) that the course was professionally relevant.
Rating of Training Relevancy to Job and/or Professional Needs Mean
Discussions were relevant to my current job/professional needs 4.28
Handouts were useful to current job/professional needs 4.18
Exercises were relevant to current job/professional needs 4.07
Overall the course content was relevant to my current job/professional needs 4.23
Objectives (n=885): Averaged across all 14 training dates, participants reported moderately high approval (“agree” 4.45 out of 5) with how learning objectives were identified and met during the course.
4.14
4.38
4.12 4.27
4.54 4.39
4.23
4.48 4.56 4.64
4.13
4.42
4.14 4.2
27
-Mar
3-A
pr
10
-Ap
r
17
-Ap
r
24
-Ap
r
1-M
ay
8-M
ay
15
-May
22
-May
29
-May
5-J
un
12
-Ju
n
19
-Ju
n
26
-Ju
n
3-J
ul
10
-Ju
l
17
-Ju
l
24
-Ju
l
31
-Ju
l
7-A
ug
14
-Au
g
21
-Au
g
28
-Au
g
4-S
ep
11
-Se
p
18
-Se
p
25
-Se
p
Overall Course Rating
Overall Course Rating
Individual Training
Dates: Data on
participant
demographics,
workplace, etc.,
for each training
date is available
from the Training
Department.
Trauma Informed Systems Initiative
14
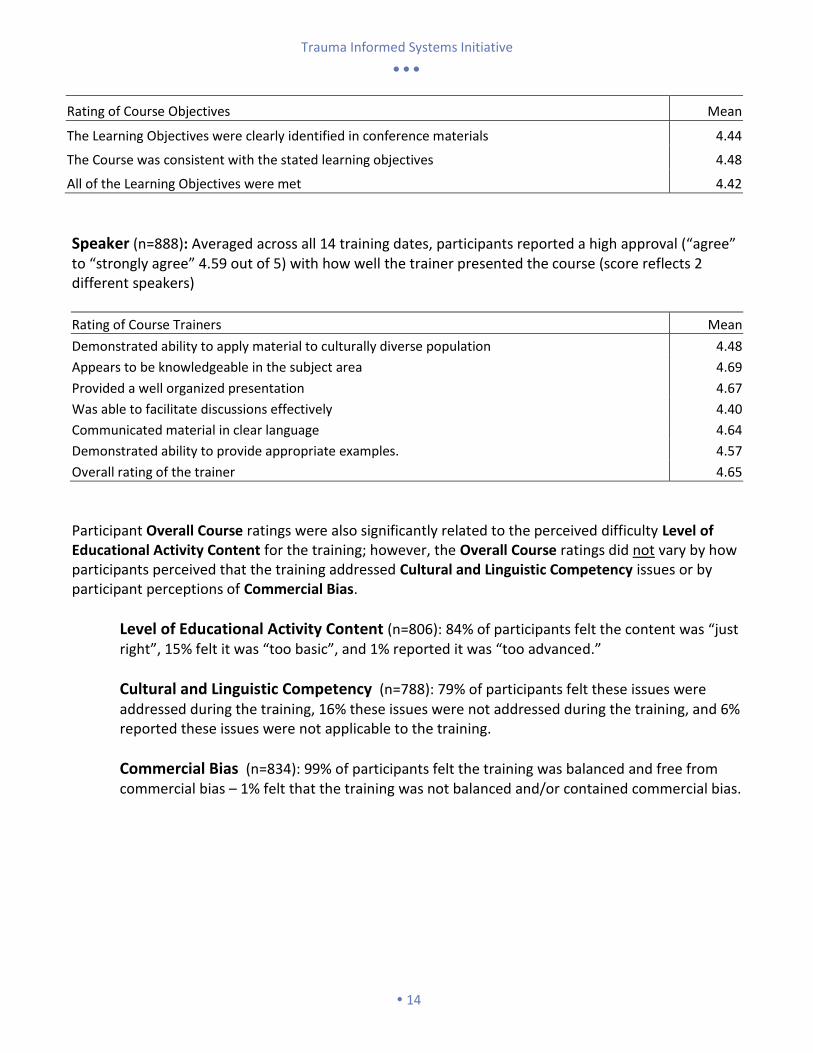
Rating of Course Objectives Mean
The Learning Objectives were clearly identified in conference materials 4.44
The Course was consistent with the stated learning objectives 4.48
All of the Learning Objectives were met 4.42
Speaker (n=888): Averaged across all 14 training dates, participants reported a high approval (“agree” to “strongly agree” 4.59 out of 5) with how well the trainer presented the course (score reflects 2 different speakers)
Rating of Course Trainers Mean
Demonstrated ability to apply material to culturally diverse population 4.48
Appears to be knowledgeable in the subject area 4.69
Provided a well organized presentation 4.67
Was able to facilitate discussions effectively 4.40
Communicated material in clear language 4.64
Demonstrated ability to provide appropriate examples. 4.57
Overall rating of the trainer 4.65
Participant Overall Course ratings were also significantly related to the perceived difficulty Level of Educational Activity Content for the training; however, the Overall Course ratings did not vary by how participants perceived that the training addressed Cultural and Linguistic Competency issues or by participant perceptions of Commercial Bias.
Level of Educational Activity Content (n=806): 84% of participants felt the content was “just right”, 15% felt it was “too basic”, and 1% reported it was “too advanced.”
Cultural and Linguistic Competency (n=788): 79% of participants felt these issues were addressed during the training, 16% these issues were not addressed during the training, and 6% reported these issues were not applicable to the training.
Commercial Bias (n=834): 99% of participants felt the training was balanced and free from commercial bias – 1% felt that the training was not balanced and/or contained commercial bias.
Trauma Informed Systems Initiative
15
Improving the Trauma 101 Training
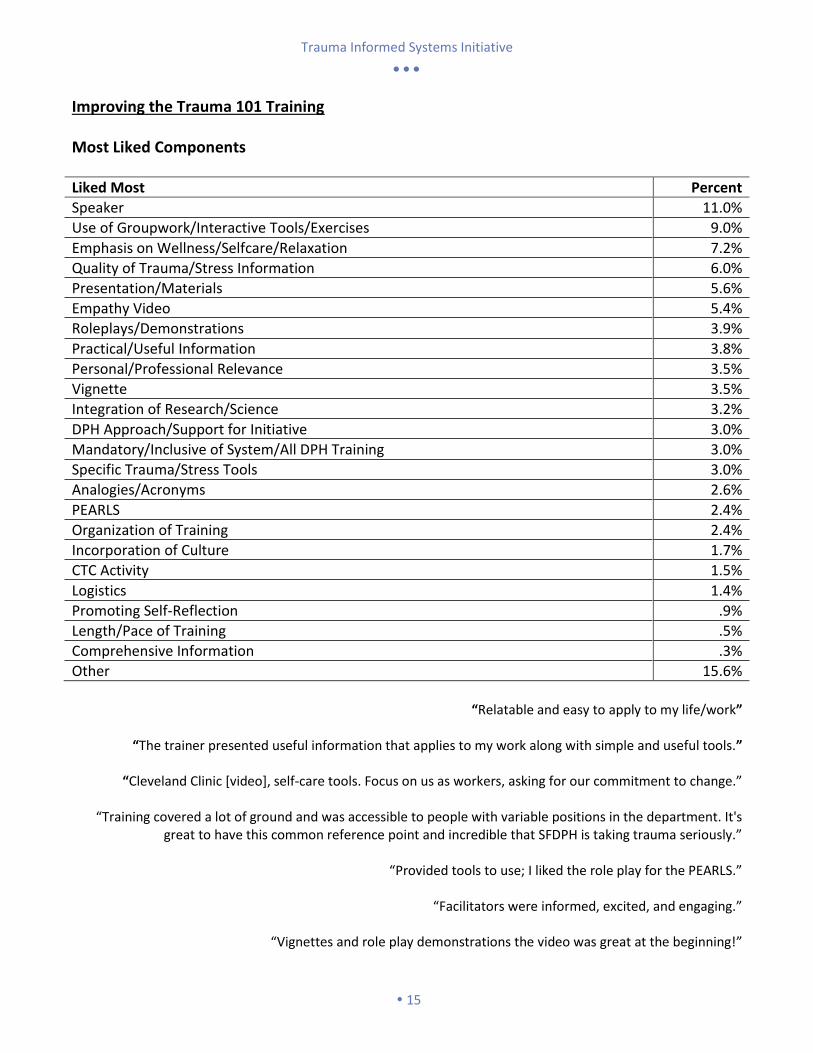
Most Liked Components
Liked Most Percent
Speaker 11.0%
Use of Groupwork/Interactive Tools/Exercises 9.0%
Emphasis on Wellness/Selfcare/Relaxation 7.2%
Quality of Trauma/Stress Information 6.0%
Presentation/Materials 5.6%
Empathy Video 5.4%
Roleplays/Demonstrations 3.9%
Practical/Useful Information 3.8%
Personal/Professional Relevance 3.5%
Vignette 3.5%
Integration of Research/Science 3.2%
DPH Approach/Support for Initiative 3.0%
Mandatory/Inclusive of System/All DPH Training 3.0%
Specific Trauma/Stress Tools 3.0%
Analogies/Acronyms 2.6%
PEARLS 2.4%
Organization of Training 2.4%
Incorporation of Culture 1.7%
CTC Activity 1.5%
Logistics 1.4%
Promoting Self-Reflection .9%
Length/Pace of Training .5%
Comprehensive Information .3%
Other 15.6%
“Relatable and easy to apply to my life/work”
“The trainer presented useful information that applies to my work along with simple and useful tools.”
“Cleveland Clinic [video], self-care tools. Focus on us as workers, asking for our commitment to change.”
“Training covered a lot of ground and was accessible to people with variable positions in the department. It's
great to have this common reference point and incredible that SFDPH is taking trauma seriously.”
“Provided tools to use; I liked the role play for the PEARLS.”
“Facilitators were informed, excited, and engaging.”
“Vignettes and role play demonstrations the video was great at the beginning!”
Trauma Informed Systems Initiative
16
“I truly appreciate Barbara Garcia for making this mandatory. I hope that all high level managers attend.”
“Practical tips for handling stress. Scope of training is extensive. Easy enough to understand - not too much
jargon.”
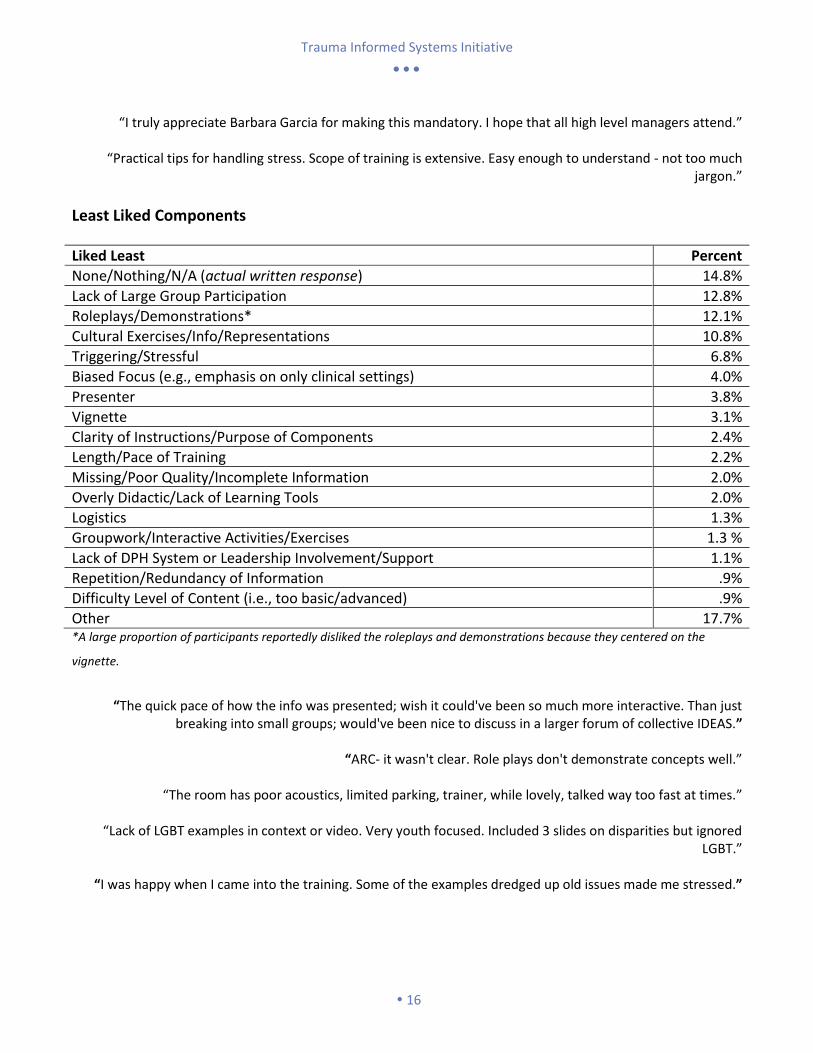
Least Liked Components
Liked Least Percent
None/Nothing/N/A (actual written response) 14.8%
Lack of Large Group Participation 12.8%
Roleplays/Demonstrations* 12.1%
Cultural Exercises/Info/Representations 10.8%
Triggering/Stressful 6.8%
Biased Focus (e.g., emphasis on only clinical settings) 4.0%
Presenter 3.8%
Vignette 3.1%
Clarity of Instructions/Purpose of Components 2.4%
Length/Pace of Training 2.2%
Missing/Poor Quality/Incomplete Information 2.0%
Overly Didactic/Lack of Learning Tools 2.0%
Logistics 1.3%
Groupwork/Interactive Activities/Exercises 1.3 %
Lack of DPH System or Leadership Involvement/Support 1.1%
Repetition/Redundancy of Information .9%
Difficulty Level of Content (i.e., too basic/advanced) .9%
Other 17.7% *A large proportion of participants reportedly disliked the roleplays and demonstrations because they centered on the
vignette.
“The quick pace of how the info was presented; wish it could've been so much more interactive. Than just
breaking into small groups; would've been nice to discuss in a larger forum of collective IDEAS.”
“ARC- it wasn't clear. Role plays don't demonstrate concepts well.”
“The room has poor acoustics, limited parking, trainer, while lovely, talked way too fast at times.”
“Lack of LGBT examples in context or video. Very youth focused. Included 3 slides on disparities but ignored LGBT.”
“I was happy when I came into the training. Some of the examples dredged up old issues made me stressed.”

Trauma Informed Systems Initiative
17
“Too focused on clinical/mental health settings. I would like to broaden the frame of DPH employees interact with community members, not just as clients or patients, but often in advocacy and code enforcement
situations."
“Need to better frame course for those whose clients are other employees/colleagues.”
“The group discussions and talk on culture - too basic for treating professionals
“Would love to have more science in it.”
“Comments from audience were not discouraged, per se, but it would have been good to hear more from the audience as a whole, not just our small groups.”

Trauma Informed Systems Initiative
18
Suggestions for Improvement
Suggested Improvements Percent
None/Nothing/N/A (actual written response) 11.8%
Increase Large Group Participation 9.8%
Provide Additional/Expanded Content (i.e., more detail/info on specific topics) 8.3%
Adjust Length/Pace of Training (e.g., too long/short, rushed/slow) 7.0%
Improve Logistics (e.g., seating, location, snacks, breaks, sound) 5.5%
Customize Trainings (e.g., by types of staff, setting, level of education) 5.3%
Offer More Relevant Materials/Examples (e.g., specific to work setting) 4.3%
Diversify Activities/Reduce Vignette Redundancy 3.8%
Use Smaller Groups (i.e., smaller breakouts and/or smaller whole group) 3.3%
Reduce Cultural Stereotypes/Bias (e.g., characters in vignette) 3.3%
Increase System/Leadership Support and Involvement 2.8%
Provide More Support/Resources/Tools Post-Training 2.8%
Discuss Impact of SFDPH System/Power/Resources (i.e., impact of system functioning) 2.5%
Improve Readability of Materials/Presentation (e.g., blurry slides, poor handout copies) 2.5%
Roleplay in Small Groups 1.8%
Present Vignette in Different Format (e.g., video, role play) .8%
Use Multiple Presenters .8%
Clarify Activity Instructions/Purpose of Components .8%
Other 23.1%
“Have co-facilitators. Develop staff development modules to use in the field.”
“More engagement between group such that having small group talks & comparing discussing with other small groups as a whole afterwards.”
“Some of the slides are too small (Pg. 45).”
“More information/training on specific community trauma (such as latino immigrant communites, etc.).”
“More examples, more roleplay of situations the audiences gives on the fly.”
“Include tools on team building and referrals.”
“More interactive work in a large forum with each other; touch-on more examples/ scenarios with complex trauma
survivors and the "domino effects" of trauma activation, etc.”
“More questions and answer period.”
“Break into smaller groups with more facilitated dialogue and more suggestions of applying material to job.”
“Clarify that the cleveland clinic video is about general observances 3 of the 5 people in my group got hung up on the people in the video not being "the population I serve"”
“I need more time to do the commitment change.”
Trauma Informed Systems Initiative
19
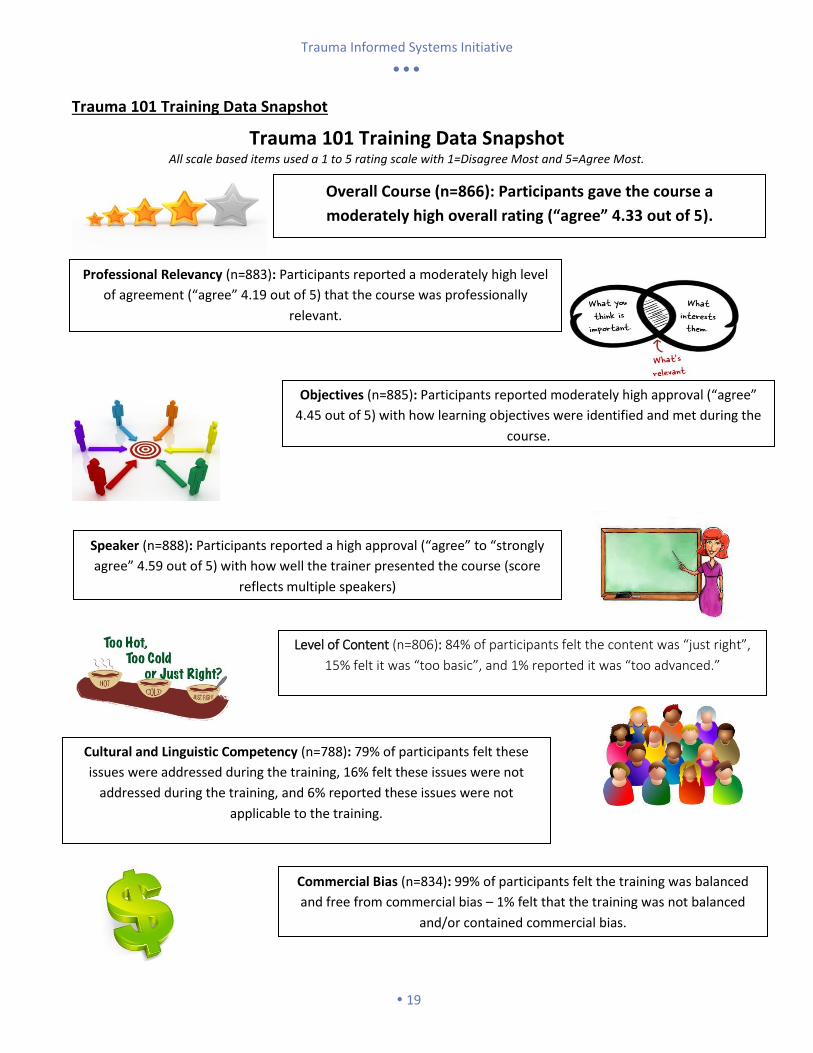
Trauma 101 Training Data Snapshot
Trauma 101 Training Data Snapshot All scale based items used a 1 to 5 rating scale with 1=Disagree Most and 5=Agree Most.
Overall Course (n=866): Participants gave the course a
moderately high overall rating (“agree” 4.33 out of 5).
Professional Relevancy (n=883): Participants reported a moderately high level
of agreement (“agree” 4.19 out of 5) that the course was professionally
relevant.
Objectives (n=885): Participants reported moderately high approval (“agree”
4.45 out of 5) with how learning objectives were identified and met during the
course.
Speaker (n=888): Participants reported a high approval (“agree” to “strongly
agree” 4.59 out of 5) with how well the trainer presented the course (score
reflects multiple speakers)
Level of Content (n=806): 84% of participants felt the content was “just right”,
15% felt it was “too basic”, and 1% reported it was “too advanced.”
Cultural and Linguistic Competency (n=788): 79% of participants felt these
issues were addressed during the training, 16% felt these issues were not
addressed during the training, and 6% reported these issues were not
applicable to the training.
Commercial Bias (n=834): 99% of participants felt the training was balanced
and free from commercial bias – 1% felt that the training was not balanced
and/or contained commercial bias.
Trauma Informed Systems Initiative
20
Feedback on the Trauma Informed System Initiative
Support for TIS Initiative
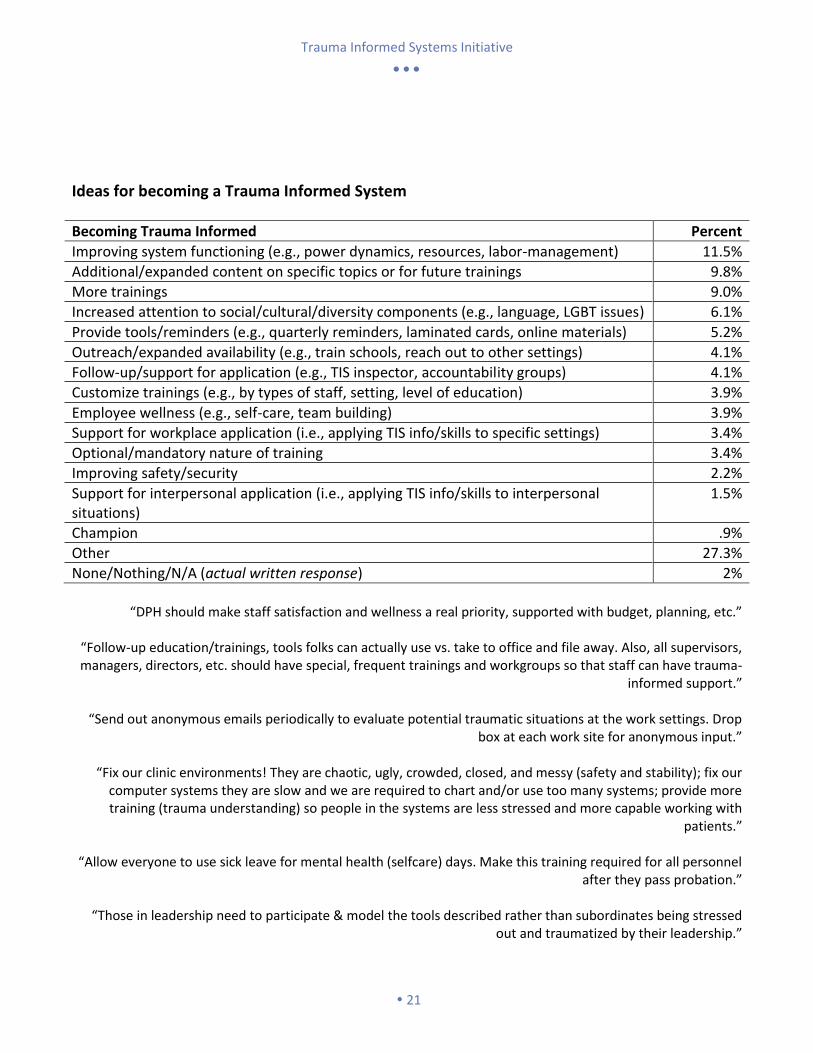
Rating of Trauma Informed System Initiative Mean
Being trauma informed is important for everyone in SFDPH. 4.74
I believe that using trauma informed principles will improve my worklife. 4.53
The trauma informed initiative will likely be abandoned or poorly implemented. 2.80
I want to help our system become more trauma informed. 4.19
SFDPH is already trauma informed and new efforts are not needed. 2.15
It will be easy for me to apply trauma informed principles in my work. 3.85 Scale based items used a 1 to 5 rating scale with 1=Disagree Most and 5=Agree Most.
Given that participants complete this scale immediately following the conclusion of the Trauma 101 Training, the Training may need to address weak areas (e.g., abandonment/implementation) more explicitly during the course of the training.
4.16 4.19
4.02 4.08 4.11 4.12
4.05 4.15 4.18 4.13
3.85
3.99 4.05
3.85
Initiative Support Rating
Initiative Support Rating
Support for Initiative (n=890): Averaged across all 14 training dates,
participants generally reported overall approval for the initiative (“agree” 4.06
out of 5); however, a number of participants expressed concern that the
initiative would be abandoned or poorly implemented (2.8 out of 5).
Individual Training
Dates: Data on
participant
demographics,
workplace, etc.,
for each training
date is available
from the Training
Department.
Trauma Informed Systems Initiative
21
Ideas for becoming a Trauma Informed System
Becoming Trauma Informed Percent
Improving system functioning (e.g., power dynamics, resources, labor-management) 11.5%
Additional/expanded content on specific topics or for future trainings 9.8%
More trainings 9.0%
Increased attention to social/cultural/diversity components (e.g., language, LGBT issues) 6.1%
Provide tools/reminders (e.g., quarterly reminders, laminated cards, online materials) 5.2%
Outreach/expanded availability (e.g., train schools, reach out to other settings) 4.1%
Follow-up/support for application (e.g., TIS inspector, accountability groups) 4.1%
Customize trainings (e.g., by types of staff, setting, level of education) 3.9%
Employee wellness (e.g., self-care, team building) 3.9%
Support for workplace application (i.e., applying TIS info/skills to specific settings) 3.4%
Optional/mandatory nature of training 3.4%
Improving safety/security 2.2%
Support for interpersonal application (i.e., applying TIS info/skills to interpersonal situations)
1.5%
Champion .9%
Other 27.3%
None/Nothing/N/A (actual written response) 2%
“DPH should make staff satisfaction and wellness a real priority, supported with budget, planning, etc.”
“Follow-up education/trainings, tools folks can actually use vs. take to office and file away. Also, all supervisors, managers, directors, etc. should have special, frequent trainings and workgroups so that staff can have trauma-
informed support.”
“Send out anonymous emails periodically to evaluate potential traumatic situations at the work settings. Drop box at each work site for anonymous input.”
“Fix our clinic environments! They are chaotic, ugly, crowded, closed, and messy (safety and stability); fix our
computer systems they are slow and we are required to chart and/or use too many systems; provide more training (trauma understanding) so people in the systems are less stressed and more capable working with
patients.”
“Allow everyone to use sick leave for mental health (selfcare) days. Make this training required for all personnel after they pass probation.”
“Those in leadership need to participate & model the tools described rather than subordinates being stressed
out and traumatized by their leadership.”

Trauma Informed Systems Initiative
22
“Target administrators and supervisors, have management shadow line workers to get a sense of their daily
experience, enhance work environments to solicit solutions/suggestions from line staff versus top-down management style.”
“Add some of pocket tools to DPH monthly calendar!”
“DPH Leadership walking the talk of creating safety and stability.”
“I feel like there could be some more involvement and impacts directly from those we are serving.”
“Management team needs to promote 'trauma informed' They need to act as our 'role model' They need to care
their staff. We are not a robot. WE have feeling, emotion. We need to be heard. We have been traumatized for long time. No way to vent. No way to help. No way to channel.”
“Annual evaluations of management/ supervisors to give critical but constructive feedback.”
“System wide gratitude practice for staff. Examine customer service practice, learn from other industries like
Nordstorms!”
“Needs to be BUILT IN to programming and organization of teams within DPH…facing so much pain/heartache.”
Trauma Informed Systems Initiative
23
Trauma Informed System Practice Change
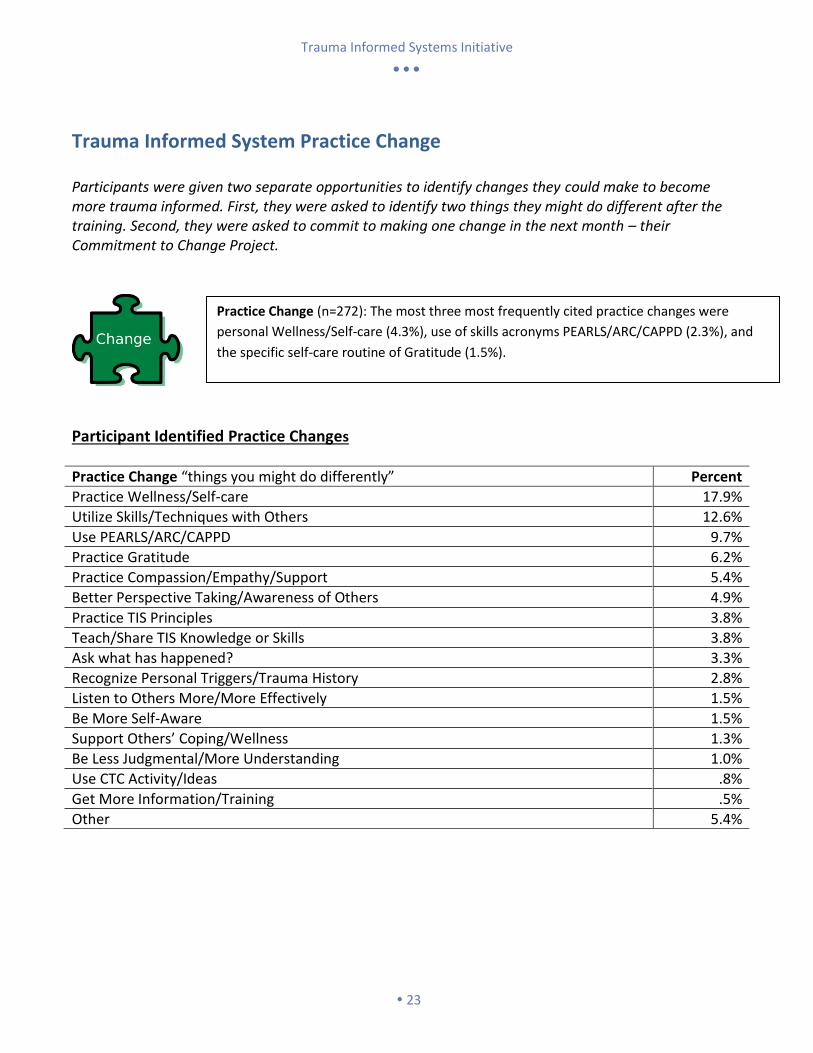
Participants were given two separate opportunities to identify changes they could make to become more trauma informed. First, they were asked to identify two things they might do different after the training. Second, they were asked to commit to making one change in the next month – their Commitment to Change Project.
Participant Identified Practice Changes
Practice Change “things you might do differently” Percent
Practice Wellness/Self-care 17.9%
Utilize Skills/Techniques with Others 12.6%
Use PEARLS/ARC/CAPPD 9.7%
Practice Gratitude 6.2%
Practice Compassion/Empathy/Support 5.4%
Better Perspective Taking/Awareness of Others 4.9%
Practice TIS Principles 3.8%
Teach/Share TIS Knowledge or Skills 3.8%
Ask what has happened? 3.3%
Recognize Personal Triggers/Trauma History 2.8%
Listen to Others More/More Effectively 1.5%
Be More Self-Aware 1.5%
Support Others’ Coping/Wellness 1.3%
Be Less Judgmental/More Understanding 1.0%
Use CTC Activity/Ideas .8%
Get More Information/Training .5%
Other 5.4%
Practice Change (n=272): The most three most frequently cited practice changes were
personal Wellness/Self-care (4.3%), use of skills acronyms PEARLS/ARC/CAPPD (2.3%), and
the specific self-care routine of Gratitude (1.5%).
Trauma Informed Systems Initiative
24
Commitment to Change (CTC) Project
CTC Goals
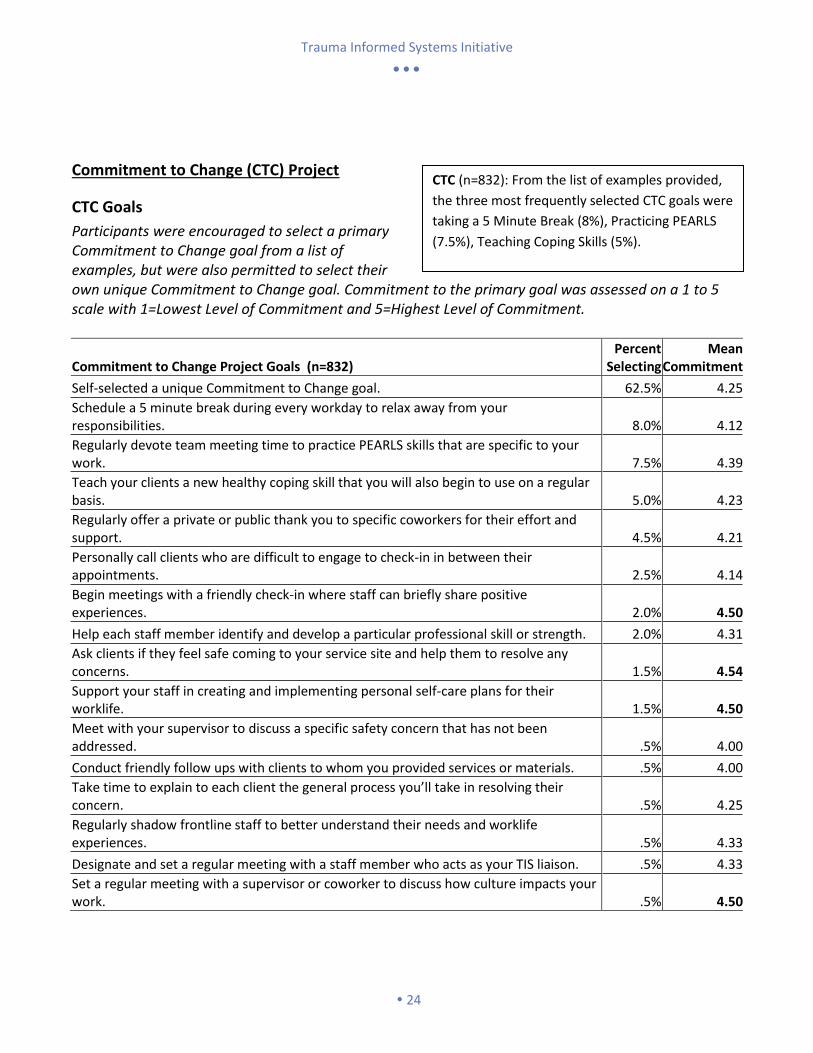
Participants were encouraged to select a primary Commitment to Change goal from a list of examples, but were also permitted to select their own unique Commitment to Change goal. Commitment to the primary goal was assessed on a 1 to 5 scale with 1=Lowest Level of Commitment and 5=Highest Level of Commitment.
Commitment to Change Project Goals (n=832) Percent
Selecting Mean
Commitment
Self-selected a unique Commitment to Change goal. 62.5% 4.25
Schedule a 5 minute break during every workday to relax away from your responsibilities. 8.0% 4.12
Regularly devote team meeting time to practice PEARLS skills that are specific to your work. 7.5% 4.39
Teach your clients a new healthy coping skill that you will also begin to use on a regular basis. 5.0% 4.23
Regularly offer a private or public thank you to specific coworkers for their effort and support. 4.5% 4.21
Personally call clients who are difficult to engage to check-in in between their appointments. 2.5% 4.14
Begin meetings with a friendly check-in where staff can briefly share positive experiences. 2.0% 4.50
Help each staff member identify and develop a particular professional skill or strength. 2.0% 4.31
Ask clients if they feel safe coming to your service site and help them to resolve any concerns. 1.5% 4.54
Support your staff in creating and implementing personal self-care plans for their worklife. 1.5% 4.50
Meet with your supervisor to discuss a specific safety concern that has not been addressed. .5% 4.00
Conduct friendly follow ups with clients to whom you provided services or materials. .5% 4.00
Take time to explain to each client the general process you’ll take in resolving their concern. .5% 4.25
Regularly shadow frontline staff to better understand their needs and worklife experiences. .5% 4.33
Designate and set a regular meeting with a staff member who acts as your TIS liaison. .5% 4.33
Set a regular meeting with a supervisor or coworker to discuss how culture impacts your work. .5% 4.50
CTC (n=832): From the list of examples provided,
the three most frequently selected CTC goals were
taking a 5 Minute Break (8%), Practicing PEARLS
(7.5%), Teaching Coping Skills (5%).
Trauma Informed Systems Initiative
25
There was no significant difference in overall level of commitment between participants who selected their goal from the list of examples and those that self-selected their own unique goal. Fifty-eight (58%) percent of participants identified both a primary and secondary Commitment to Change goal, although a secondary goal was optional.
Participant Success with Implementing CTC Goals
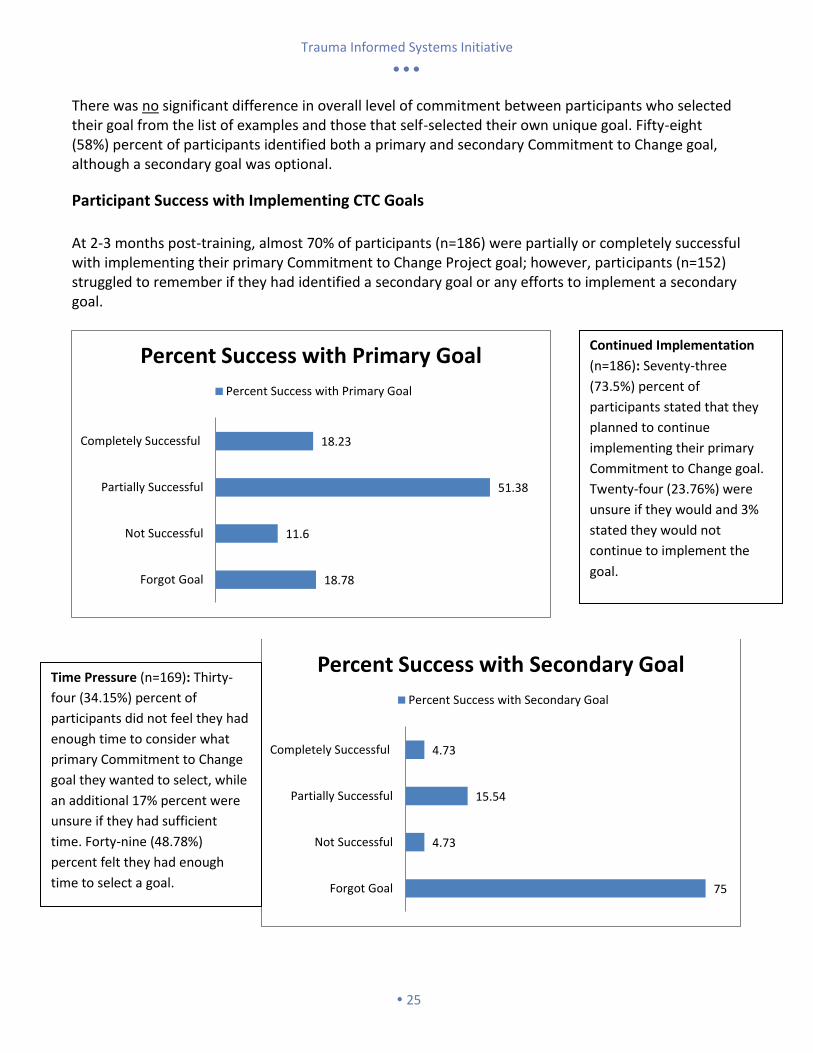
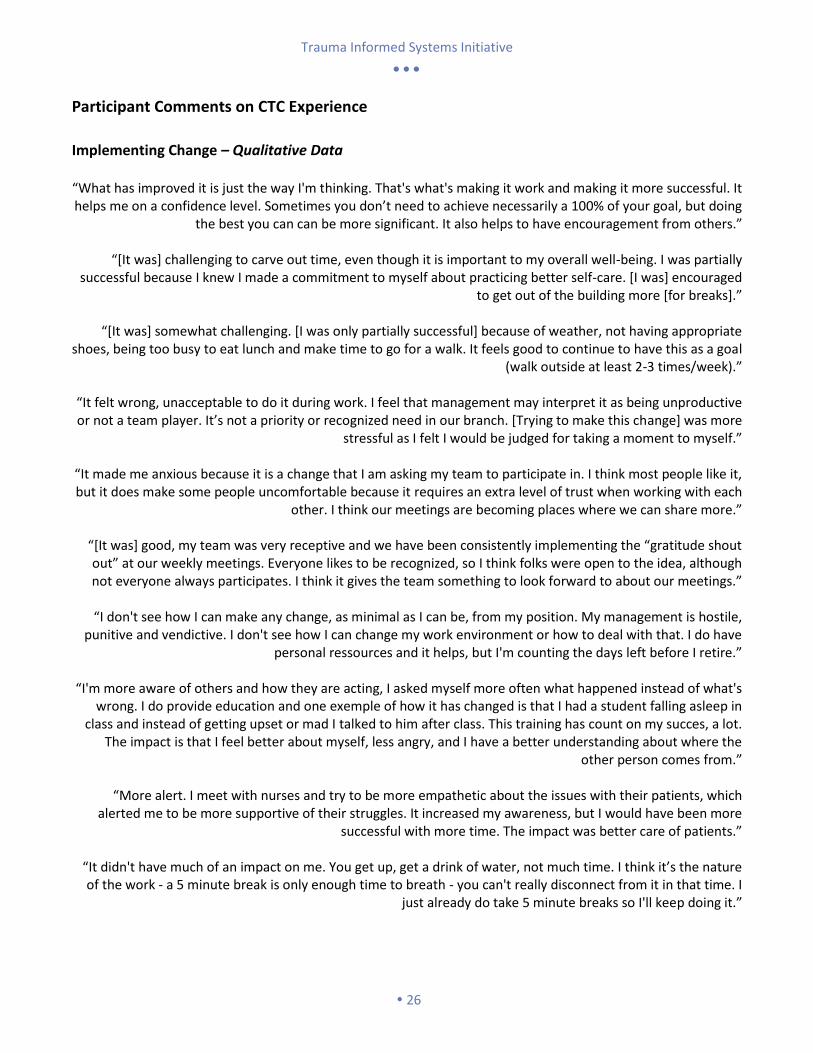
At 2-3 months post-training, almost 70% of participants (n=186) were partially or completely successful with implementing their primary Commitment to Change Project goal; however, participants (n=152) struggled to remember if they had identified a secondary goal or any efforts to implement a secondary goal.
18.78
11.6
51.38
18.23
Forgot Goal
Not Successful
Partially Successful
Completely Successful
Percent Success with Primary Goal
Percent Success with Primary Goal
75
4.73
15.54
4.73
Forgot Goal
Not Successful
Partially Successful
Completely Successful
Percent Success with Secondary Goal
Percent Success with Secondary Goal
Continued Implementation
(n=186): Seventy-three
(73.5%) percent of
participants stated that they
planned to continue
implementing their primary
Commitment to Change goal.
Twenty-four (23.76%) were
unsure if they would and 3%
stated they would not
continue to implement the
goal.
Time Pressure (n=169): Thirty-
four (34.15%) percent of
participants did not feel they had
enough time to consider what
primary Commitment to Change
goal they wanted to select, while
an additional 17% percent were
unsure if they had sufficient
time. Forty-nine (48.78%)
percent felt they had enough
time to select a goal.
Trauma Informed Systems Initiative
26
Participant Comments on CTC Experience
Implementing Change – Qualitative Data “What has improved it is just the way I'm thinking. That's what's making it work and making it more successful. It helps me on a confidence level. Sometimes you don’t need to achieve necessarily a 100% of your goal, but doing
the best you can can be more significant. It also helps to have encouragement from others.”
“[It was] challenging to carve out time, even though it is important to my overall well-being. I was partially successful because I knew I made a commitment to myself about practicing better self-care. [I was] encouraged
to get out of the building more [for breaks].”
“[It was] somewhat challenging. [I was only partially successful] because of weather, not having appropriate shoes, being too busy to eat lunch and make time to go for a walk. It feels good to continue to have this as a goal
(walk outside at least 2-3 times/week).”
“It felt wrong, unacceptable to do it during work. I feel that management may interpret it as being unproductive or not a team player. It’s not a priority or recognized need in our branch. [Trying to make this change] was more
stressful as I felt I would be judged for taking a moment to myself.”
“It made me anxious because it is a change that I am asking my team to participate in. I think most people like it, but it does make some people uncomfortable because it requires an extra level of trust when working with each
other. I think our meetings are becoming places where we can share more.”
“[It was] good, my team was very receptive and we have been consistently implementing the “gratitude shout out” at our weekly meetings. Everyone likes to be recognized, so I think folks were open to the idea, although not everyone always participates. I think it gives the team something to look forward to about our meetings.”
“I don't see how I can make any change, as minimal as I can be, from my position. My management is hostile,
punitive and vendictive. I don't see how I can change my work environment or how to deal with that. I do have personal ressources and it helps, but I'm counting the days left before I retire.”
“I'm more aware of others and how they are acting, I asked myself more often what happened instead of what's
wrong. I do provide education and one exemple of how it has changed is that I had a student falling asleep in class and instead of getting upset or mad I talked to him after class. This training has count on my succes, a lot.
The impact is that I feel better about myself, less angry, and I have a better understanding about where the other person comes from.”
“More alert. I meet with nurses and try to be more empathetic about the issues with their patients, which
alerted me to be more supportive of their struggles. It increased my awareness, but I would have been more successful with more time. The impact was better care of patients.”
“It didn't have much of an impact on me. You get up, get a drink of water, not much time. I think it’s the nature of the work - a 5 minute break is only enough time to breath - you can't really disconnect from it in that time. I
just already do take 5 minute breaks so I'll keep doing it.”
Trauma Informed Systems Initiative
27
Increasing Success – Qualitative Data
“I like the follow-up feature, it makes it accountable, makes you think about it. When you call or sent me reminders it reminded me of the training and the changes that I wanted to do.”
“[If I had found more/better] reasons to make myself leave the building for a brief break (e.g., getting lunch,
going to the post office). Fun reminders and a small reward for myself [would also have helped.]”
“Telling more peers about my goal [would have increased my success].”
“[It would have helped to have] manager buy-in and staffing resources to eliminate their need for me to do more than my designated workload. If managers/directors were trained in leadership and appreciation of
“human hours” and resource allocation. This would allow acceptance of employees taking care of their own needs and stress management. As it is, I have to do my meditation, breathing or stretches at home instead. This
further reduces personal/home time.”
“[It would have helped] if all of our team had attended the training relatively close to each other. Nothing [else], I made it a part of our agenda.”
“Nothing, I was succesfull. It was a great change.”
“Impressive! You actually did follow up! Follow up is unusual, it makes me see how much DPH values the
training. I hope Senior team have the training too. It would help to build more trust and apreciation on the management and trickle down. People don’t often trust their management and viceversa. It would be helpful.”
“What did help to remember was having people who modeled that behavior to me.”
“We should start talking about change from the beginning of the training. It was very helpful but at the end it is
not enough.”
“Nothing. I saw your e-mails and they made me think of the training and I remembered my commitment to change.”
“I started to think about doing it but then reverted back to the status quo because of my busy schedule. I
couldn't be consistent especially with all the other things I was learning in my new position. I think it is great
though that you guys are wanting to help us apply the training and if I had been more specific with my change I
think that would have helped a lot. Also, more reminders until I had integrated it - maybe an accountability
group.”
Trauma Informed Systems Initiative
28
Trauma Informed System (TIS) Core Principles & Suggested Competencies San Francisco Department of Public Health
Understanding Trauma & Stress Without understanding trauma, we are more likely to adopt behaviors and beliefs that are negative and unhealthy. However, when we understand trauma and stress we can act compassionately and take well-informed steps toward wellness. 1. Trauma – We understand that trauma is common, but experienced uniquely due to its many variations in form and impact. 2. Stress – We understand that optimal levels of positive stress can be healthy, but that chronic or extreme stress has damaging effects. 3. Reactions – We understand that many trauma reactions are adaptive, but that some resulting behaviors and beliefs may impede recovery and wellness. 4. Recovery – We understand that trauma can be overcome effectively through accessible treatments, skills, relationships, and personal practices. Compassion & Dependability Trauma is overwhelming and can leave us feeling isolated or betrayed, which may make it difficult to trust others and receive support. However, when we experience compassionate and dependable relationships, we reestablish trusting connections with others that foster mutual wellness. 1. Compassion – We strive to act compassionately across our interactions with others through the genuine expression of concern and support. 2. Relationships – We value and seek to develop secure and dependable relationships characterized by mutual respect and attunement. 3. Communication – We promote dependability and create trust by communicating in ways that are clear, inclusive, and useful to others. Safety & Stability Trauma unpredictably violates our physical, social, and emotional safety resulting in a sense of threat and need to manage risks. Increasing stability in our daily lives and having these core safety needs met can minimize our stress reactions and allow us to focus our resources on wellness. 1. Stability – We minimize unnecessary changes and, when changes are necessary, provide sufficient notice and preparation. 2. Physical – We create environments that are physically safe, accessible, clean, and comfortable. 3. Social-Emotional – We maintain healthy interpersonal boundaries and manage conflict appropriately in our relationships with others.
Trauma Informed Systems Initiative
29
Collaboration & Empowerment Trauma involves a loss of power and control that makes us feel helpless. However, when we are prepared for and given real opportunities to make choices for ourselves and our care, we feel empowered and can promote our own wellness. 1. Empowerment – We recognize the value of personal agency and understand how it supports recovery and overall wellness. 2. Preparation – We proactively provide information and support the development of skills that are necessary for the effective empowerment of others. 3. Opportunities – We regularly offer others opportunities to make decisions and choices that have a meaningful impact on their lives. Cultural Humility & Responsiveness We come from diverse social and cultural groups that may experience and react to trauma differently. When we are open to understanding these differences and respond to them sensitively we make each other feel understood and wellness is enhanced. 1. Differences – We demonstrate knowledge of how specific social and cultural groups may experience, react to, and recover from trauma differently. 2. Humility – We are proactive in respectfully seeking information and learning about differences between social and cultural groups. 3. Responsiveness – We have and can easily access support and resources for sensitively meeting the unique social and cultural needs of others. Resilience & Recovery Trauma can have a long-lasting and broad impact on our lives that may create a feeling of hopelessness. Yet, when we focus on our strengths and clear steps we can take toward wellness we are more likely to be resilient and recover. 1. Path – We recognize the value of instilling hope by seeking to develop a clear path towards wellness that addresses stress and trauma. 2. Strengths – We proactively identify and apply strengths to promote wellness and growth, rather than focusing singularly on symptom reduction. 3. Practices – We are aware of and have access to effective treatments, skills, and personal practices that support recovery and resiliency.
Trauma Informed Systems Initiative
30
Trauma Informed Systems Initiative Workgroup
Ken Epstein, Ph.D., LCSW Director, Children Youth and Families System of Care Community Behavioral Health Services San Francisco Health Network San Francisco Department of Public Health Trauma Informed Systems Initiative, Workgroup Leader Dr. Ken Epstein is currently the Children’s System of Care Director for San Francisco County Community Behavioral Health Services, where he also leads the vision and implementation of the Trauma Informed Systems Initiative. While leading the initiative at DPH, Dr. Epstein has initiated and convened numerous groups of trauma experts and interagency collaborations with in San Francisco and across the Bay Area. A notable collaboration is the Bay Area Trauma Informed System of Care (BATISC) Initiative comprised of 7 Bay Area counties, which was recently awarded a four year SAMHSA grant. Prior to his appointment to this position he has worked within family and youth service programs since 1981 as a line worker, clinician, program director, professor and chief executive officer. His professional interests have focused on providing clinical services and developing comprehensive family based services for children, youth and families experiencing alienation, conflict and loss. He has developed and directed comprehensive and integrated community based service systems including crisis services, hospital diversion, wrap-around, kinship, school-based and intensive outpatient services in Massachusetts, Vermont and California. Dr. Epstein is a Licensed Clinical Social Worker with a Ph.D. in clinical social work from Smith College, an MSW from UC Berkeley and a BA in community mental health from Hampshire College. Since 1991 Dr. Epstein has served as an Associate Clinical Professor and in the Department of Psychiatry at UCSF, where he has developed and directed an Intensive Family Therapy Training Program. In addition he has served as adjunct faculty at UCSF, School of Nursing, University of California Berkeley, School of Social Welfare and Smith College.
Lynn Dolce, MFT
Director, Foster Care Mental Health Children, Youth and Families Community Behavioral Health Services San Francisco Health Network San Francisco Department of Public Health Assistant Clinical Professor, UCSF
Curriculum Developer, Master Trainer
Lynn Dolce, MFT, has worked for over 25 years as a clinician, consultant, clinical supervisor, associate director and teacher. For the last
fifteen years, in partnership with SFGH Pediatrics, she has and developed and overseen pediatric mental health services for children,
youth and families at UCSF SFGH Child and Adolescent Services. She has served on the clinical faculty for UCSF since 2006 and has
distinguished herself as an excellent teacher and trainer. Ms. Dolce has worked closely with SFUSD to develop UCSF Healthy
Environments and Response to Trauma in Schools (HEARTS), a program that aims to promote school success for children and adolescents
who have experienced complex trauma. HEARTS has been awarded a 2013 Excellence in Partnership Award from the University
Community Partnership Council for its strong collaboration with San Francisco Unified School District. Currently, Ms. Dolce is the Director
for Foster Care Mental Health, SF DPH, CBHS, Children’s System of Care. Ms. Dolce also serves as a Master Trainer and Curriculum
Developer for the SF County DPH Trauma Informed System of Care Initiative; Transforming Stress and Trauma 101.

Trauma Informed Systems Initiative
31
Joyce Dorado, Ph.D.
Associate Professor Department of Adolescent Psychiatry USCF School of Medicine
Curriculum Developer, Master Trainer
Joyce Dorado, Ph.D., is the Co-Founder and Director of UCSF Healthy Environments and Response to Trauma in Schools (HEARTS), a program that aims to promote school success for children and adolescents who have experienced complex trauma. HEARTS has been awarded a 2013 Excellence in Partnership Award from the University Community Partnership Council for its strong collaboration with San Francisco Unified School District. Dr. Dorado is also the Director of Clinical Research and Evaluation, an Associate Clinical Professor at Child and Adolescent Services (CAS), Department of Psychiatry, UCSF-San Francisco General Hospital, and the former Co-Director of Clinical Training for the CAS Multicultural Clinical Training Program. Dr. Dorado earned her B.A. in Psychology at Stanford University, and her Ph.D. in Clinical Psychology from the University of Michigan. Her clinical service and research has focused on a public health approach to addressing complex trauma in schools, child victim/witness testimony, family violence, and psychological trauma in children, youth and families from under-resourced urban communities. She has been invited to speak about how to address trauma in schools at numerous events including the California Statewide Summit for Keeping Kids in School and Out of Court, has presented at national and international conferences, and has published her work in a number of books and journals. Dr. Dorado also serves as a Master Trainer and Curriculum Developer for the SF County DPH Trauma Informed System of Care Initiative; Transforming Stress and Trauma 101.
Michael Marcin, MD Medical Director O.M.I. Family Center Community Behavioral Health Services San Francisco Health Network San Francisco Department of Public Health Relationship Centered Communication Liaison Dr. Marcin is a practicing Child & Adolescent Psychiatrist, General Psychiatrist and the Medical Director of OMI Family Center, a comprehensive mental health clinic serving the richly diverse Oceanside, Merced and Ingleside neighborhoods of San Francisco. OMI is part of the larger network of clinics under the San Francisco Department of Public Health's Community Behavioral Health Service. The need for a more integrated approach to treating mental health disorders in youth, transitional ages, and adults with and without developmental disorders has guided Dr. Marcin throughout his professional career. His clinical interests include children and adults with social, cognitive, and emotional difficulties, such as those associated with Autism Spectrum Disorders and other developmental disorders. He is also the lead psychiatrist for the Anchor Program, a collaboration between CBHS and the Golden Gate Regional Center. He is committed to improving provider-client communication and experience. To this end he has joined the Trauma Informed System executive team with expertise and certification in Relationship Centered Communication by the American Academy on Communication in Healthcare. He received his Medical Doctorate from St. Louis University and completed residencies and fellowships in general and child & adolescent psychiatry at Emory University, where he was Chief Resident. Additionally, he holds a Masters of Clinical Research from Emory where he designed and implemented clinical research supported by an NIH professional development grant. Dr. Marcin has extensive experience in developing and running a successful small business, which includes strategic planning, setting the clinical standard and serving as clinical supervisor for more than 25 clinicians, wrap facilitators and support staff.
He has served as the program chair and a member of numerous statewide committees and initiatives. He is the recipient of national and international honors from the American Psychiatric Association, the American Academy of Child and Adolescent Psychiatry, the National Institute on Drug Abuse and Emory University School of Medicine. He has published his research in leading international journals and presented at national professional conferences.
Trauma Informed Systems Initiative
32
Briana Fields Loomis, Ph.D.
Evaluator Psychologist Child, Youth & Family System of Care Community Behavioral Health Services San Francisco Health Network San Francisco Department of Public Health Evaluating Psychologist, Commitment to Change Project
Briana Fields Loomis, PhD, is a psychologist and evaluator for the San Francisco Department of Public Health. Over the past decade, she
has conducted research, provided treatment, and offered trainings and consultation in the field of trauma psychology. With an emphasis
on crimes and trauma affecting women, children and youth, she has worked with first responders and the legal system, child welfare
professionals, and local governments, as well as clinicians to improve how we understand and care for those who have been victimized.
Norman Aleman, MSW
Training Manager Office of Workforce Development Community Behavioral Health Services San Francisco Health Network San Francisco Department of Public Health Cultural Competence, Training and Education Liaison
Norman Aleman, MSW, is the Training Manager under the Office of Workforce Development. For over eight years, he has been
responsible for over forty trainings, seminars, workshops, and conferences with over three thousand SF Department of Public Health staff
participating on a yearly basis. Educational activities range from evidence based programs to reduce stigma surrounding mental illness
and substance abuse to technical assistance in documentation and supervision in both primary care and behavioral health settings.
Kaytie Speziale, MFT
Trauma Informed Systems, Coordinator Community Behavioral Health Services San Francisco Health Network San Francisco Department of Public Health
Coordinator
Kaytie Speziale, MFT is currently the Coordinator for the SFDPH’s Trauma Informed Systems Initiative and overseeing the system-wide
training on basics of stress and trauma. A Marriage and Family Therapist by training, Kaytie specialized in the treatment of trauma for
children and their families in the Sacramento area at UC Davis Children’s Hospital and community mental health clinics before moving to
San Francisco. Kaytie's experience includes individual therapy, specialized behavioral support for children in residential treatment or
foster care, group facilitation and advocacy for those living with mental health needs.

Trauma Informed Systems Initiative
33
Students
Post-Doctoral Fellow
Diana Sistiva, Ph.D.
Dr. Diana Sistiva is a Post-Doctoral Fellow with the Trauma Informed Systems Initiative Evaluation Program. Trained as a Clinical
Psychologist, Dr. Sistiva has worked for several years as a therapist specializing in traumatized populations. Her experience includes
working at the Department of Public Health in Aubervilliers, France, in Early Childhood Wellbeing Promotion, as well as the Center for
Psychotrauma in Paris. Dr. Sistiva earned her doctoral degree jointly from University of Quebec in Montreal and University of Bordeaux 2
in France, and is currently dedicated to prevention and metal health promotion.
Graduate Interns
Jane Pomeroy, University of California, Berkeley
Lan Vu, University of California, Berkeley
Jane Pomeroy and Lan Vu are graduate students at the University of California, Berkeley in the School of Social Welfare. Jane Pomeroy is
studying Management and Planning. She is passionate about building healthy communities, and working to prevent gender-based
violence. Lan Vu is studying Community Mental Health. She has a great interest in trauma-informed care and aspires to provide early
intervention and prevention to improve client outcomes.
Jane and Lan will complete their research on best practices for organizational change by May 2015. They aim to make recommendations
to the San Francisco Department of Public Health regarding the implementation of a Change Champions Model, a key step in supporting
our staff-led change efforts to become a Trauma-Informed System.
Undergraduate Intern
Tanusree Sreedharan, California State University, San Francisco
Tanusree Sreedharan is an undergraduate student of the College of Health and Social Sciences, majoring in Health Education, taking the
majority of her coursework around program planning, implementation, and community organizing. Tanu has volunteered for most of her
life in her community in the Tri-Valley and she has worked extensively with youth in the San Francisco Unified School District. She
continues to volunteer in high schools as a communication and advocacy educator and is committed to promoting resiliency to increase
positive health and well-being.
Trauma Informed Systems Initiative
34
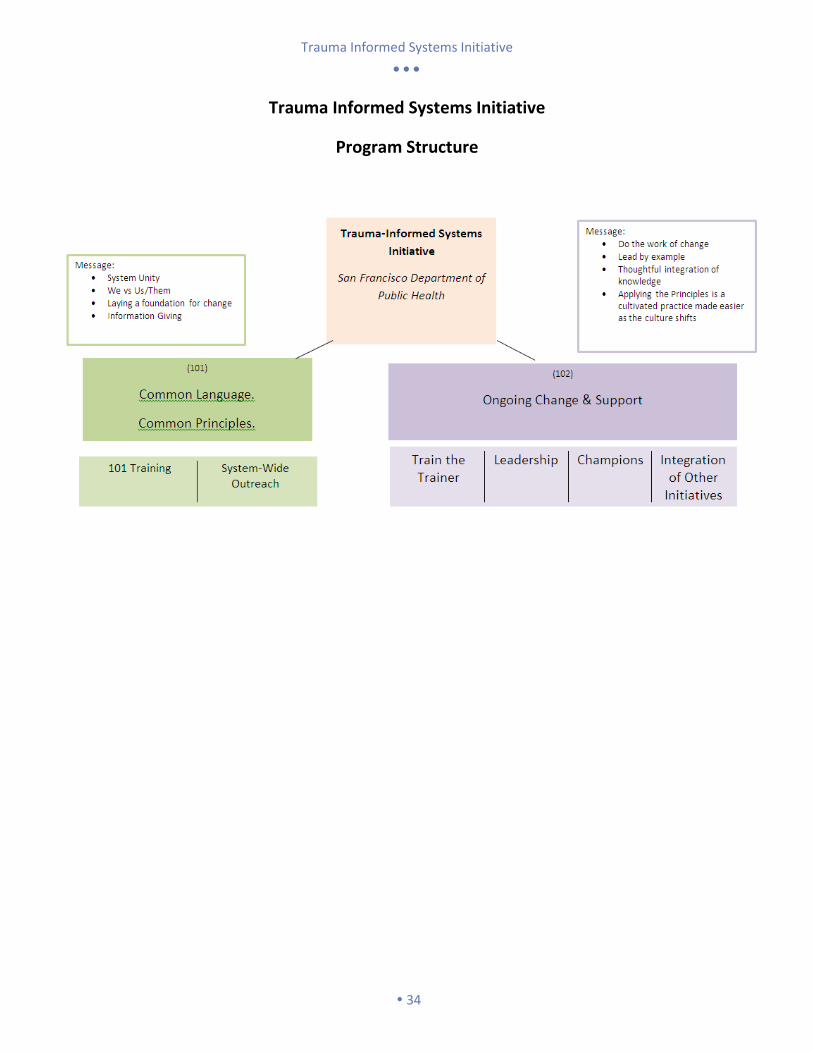
Trauma Informed Systems Initiative
Program Structure
Trauma Informed Systems Initiative
35
2014
2015
Master Trainer Master Trainer
Master Trainee
Laguna Honda Cohort
Trauma Informed Systems Workgroup
Master Trainers
Master Trainer Master Trainer Master Trainer
Laguna Honda Cohort Ambulatory Care Cohort
2 Master
Trainees
Laguna Honda
Cohort 2
2 Master
Trainees
Ambulatory Care
Cohort 2
Master
Trainer
Master
Trainer
Master
Trainer
Master
Trainer
Trauma Informed Systems Workgroup
Master Trainers
Train the
Trainer
Program Flow
Draft
Trauma Informed Systems Initiative
36
Bay Area Trauma Informed System of Care (BATISC) Executive Summary
Abstract In October 2014, The Bay Area Trauma Informed Regional Collaborative group, was awarded a SAMHSA grant for their proposal to respond to trauma on a systems level, by creating a shared and trauma informed regional infrastructure to implement, sustain, and improve services for children and youth affected by trauma. The grant award will span 4 years in the amount of $1,000,000 which will include the funding of the group’s key activity: a regional clearinghouse and coordinating center designed to integrate existing knowledge, incorporate new ideas, address challenges to training and sustaining an effective and diverse trauma informed work force and develop mechanisms to support implementation and sustainability of best practices.
Background Regional Directors of County Behavioral Health systems came together in July of 2012 to develop and share plans to take trauma-informed practices, knowledge, and approaches to a new level of regional coordination. The group began a planning process to launch a Regional Trauma Informed System of Care initiative designed to:
Develop a regional understanding and shared approach to our response to trauma and its effects,
Embed leaders including youth and parent peers to be champions of change within and across our systems serving children and youth,
Support and maintain change efforts through deploying experts and consumer voices within our region.
Address common and pervasive patterns of disproportionality with respect to historical trauma and fragmented service delivery systems.
The Directors have since met on a quarterly basis. Through these meetings, the group has drafted strategic planning documents, shared local approaches to systems change, and identified key goals and strategies for regional collaboration. Initial goals focus on resource sharing, policy coordination, coordination of care, and cross-systems coordination. Early planning efforts have also been vetted at the regional level with systems partners, parent partners, and consumer focus group participants. Through the BATISC planning group, several of the counties shared their modules and materials with the rest of the members of the Collaborative, and San Francisco, San Mateo and Santa Clara made space available in their local in-person trainings for participation by staff from other counties. The partners continued to share the idea that with a funded and lasting infrastructure and dedicated staff for this regional effort, this type of sharing will be consistent and coordinated. All of the counties will be able to benefit from jointly conducted training and the integration of shared learning approaches across the counties. In addition, the effort to implement an organized response to trauma and complex trauma and to improve access to services for children placed out of county can only be coordinated through a regional body with support and infrastructure.

Trauma Informed Systems Initiative
37
The Bay Area is fortunate to have national experts in trauma throughout the region. This expertise, however, remains in separate silos in university settings, challenged by needing to constantly seek soft funding, called upon to train other localities in the U.S or around the world, or simply challenged to reach beyond their program or facility. As a result, the opportunities to deliver and translate this local knowledge and expertise into practice for Bay Area community systems and programs have been few. In 2013, to combat this disconnection and fragmentation, the San Francisco Foundation convened a conference to engage local trauma experts in a conversation about barriers to developing and sustaining a workforce competently trained in the pervasive impacts of trauma on children, families, communities, and institutions. The expert summit concluded that that the Bay Area needed a centralized clearinghouse with a diverse advisory and oversight to help integrate practices, develop common principles and organize resources in a way that focus on knowledge transfer to the workforce, practice changes, and the sustainability of changed practice.
Goals Overarching Goal: Transform the regional, overlapping systems into a coordinated, trauma-informed, youth-guided and family driven, evidence-based system of care. 1) BATIS Center: Develop a regional center to support and sustain a system of care that is trauma-informed, youth-guided, family-driven, and culturally competent. 2) Training: Develop training resources for dissemination to county staff, providers, and consumers. 3) Coordination of Care: Establish a regional model to provide coordinated services for youth and children placed out of county, and children, youth, and families served by multiple systems within counties. 4) Policy and Practice Sustainability: Develop and sustain promising practices from the project and incorporate them throughout the region. For more information about the BATISC project, contact Kaytie Speziale with the San Francisco Department of Public Health at [email protected]
Trauma Informed Systems Initiative
38
San Francisco Trauma Informed Systems Interest
Government
Worker’s Compensation Division
District Attorney’s Office Mayor’s Office, Hydra Mendoza-McDonnell SFPD, Police Chief HSA Probation
CBOs/Non-Profits
Child Abuse Prevention Center
SF Hope Center for Youth Wellness Bay Area Academy Edgewood JVS (@ Laguna Honda) Castro Mission Health Center Baker Places Inc. Glide Mission Mental Health Sunset Mental Health A Woman's Place Encompass Community Services, Santa Cruz California Parent Training Institute, Santa Rosa San Francisco Health Plan Mercy Housing National Council on Alcoholism Stonewall Project The Sage Project
Foundations
San Francisco Foundation
The Kresge Foundation
Tipping Point Community The Annie E. Cassey Foundation
UCSF
Alicia Lieberman Matt State

Trauma Informed Systems Initiative
39
Published by the Trauma Informed Systems Initiative, San Francisco Department of Public Health. Released on December 17, 2014.




















![Trauma Informed Care [Read-Only] Informed Care... · What is Trauma Informed Care? ... blood flow & electrical activity influence brainblood flow, ... stress/fear. ((yChild Trauma](https://img.pdfslide.net/doc/110x75/5b1f59b07f8b9a1b1e8b51d7/trauma-informed-care-read-only-informed-care-what-is-trauma-informed-care.jpg)







