Embed Size (px)
Citation preview

Trends &Patterns of Child Malnutrition in India:A Disaggregated Analysis
Anand Sharma
Anand Sharma is Assistant Professor, Economics& Public Policy, Indian Institute of ManagementRohtak.Email: [email protected]
Using National Family HealthSurvey (NFHS) data, this paperexamines in detail the trends andpatterns in child malnutrition atthe national and state levels dur-ing 2005-06 and 2015-16. Itanalyses the regional variationsin the nutritional status of chil-dren below five years and at-tempts to provide explanationsfor the observed pattern. In ad-dition, the study examines thesocio-economic inequalities inchild malnutrition.At the all-Indialevel, the study finds a limitedimprovement in the nutritionalstatus of children between NFHS-3 and NFHS-4. The socio-eco-nomic inequalities in child mal-nutrition continue to persist dur-ing this period implying that arelatively greater proportion ofmalnourished children are con-centrated in poor households inboth rural and urban India.
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 67
Introduction
Children of today represent the hu-man capital of tomorrow (Nair, 2007) andtherefore, no country can afford to ne-glect the health and well-being of chil-dren. Previous studies have found a posi-tive association between human capitaland economic growth (Barro, 2001; Collin& Weil, 2018). This implies that neglect-ing the nutritional and well-being aspectsof children may have negative effects onoverall economic growth and develop-ment. The literature has also establishedthat child malnutrition is likely to have anadverse effect on cognitive development,learning outcomes in school, labor pro-ductivity, and wage earnings (e.g.Strauss& Thomas, 1998; Grantham-McGregoret. al., 1999; Hoddinott, 2009; Niti Aayog,2017).India ranks at 103 out of 119 coun-tries in the Global Hunger Index 2018 andaccounts for the highest number ofstunted children (nearly 47 million) in theworld (Global Nutrition Report, 2018).Child malnutrition rates in India exceedthose in sub-Saharan Africa and areabout five times more than in China(Gragnolati et. al., 2006; Kumar, 2007;

Anand Sharma
68 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
World Bank, 2013). In 2015-16, more thanone-third of children below five yearswere stunted and underweight in India(IIPS& ICF, 2017). This dismal perfor-mance by India in child nutrition coupledwith strong economic growth has led toconsiderable research in this area (Nie,Rammohan, Gwozdz, Sousa-Poza, 2016;Haddad, 2009). Scholars have used theterm “South Asian enigma” (Ramalingaswami et al., 1996) to explain India’sparadoxical case. At the all-India level,child malnutrition rates vary by place ofresidence (rural/urban), caste, andwealth. For example, in 2015-16, 38.3percent children (below five years) wereunderweight in rural India whereas about29 percent children were underweight inurban India (IIPS& ICF, 2017).There are considerable disparities inindustrial and economic developmentacross the Indian states (Sharma, 2017).The trends in child malnutrition at nationallevel do not reveal the considerable dis-parities across different states. For ex-ample, in 2015-16 about 12 percent ofchildren below five years were under-weight in Sikkim whereas this figure was47.8 percent for Jharkhand (IIPS& ICF,2017). The proportion of stunted childrenacross states also ranges from 20 percent(in case of Goa) to about 48 percent (incase of Bihar). It is generally believed thata mere focus on economic growth is likelyto reduce the incidence of child malnutri-tion in various states. However, the poornutritional performance of economicallyadvanced states such as Gujarat,Maharashtra, and Karnataka does not pro-vide support to this argument. On the otherhand, low income north-eastern states
such as Manipur, Nagaland, Mizoram, andArunachal Pradesh have shown betterperformance with respect to child malnu-trition. These observations warrant a de-tailed analysis of child malnutrition at theregional level.Several studies have attempted to ana-lyze and explain the extent of child mal-nutrition in India. Majority of the existingstudies focus on explaining the regionaldisparities in child malnutrition in Indiaover last few decades (e.g. Nair, 2007;Radhakrishna & Ravi, 2004; Kumar, 2007;Cavatorta, Shankar & Flores-Martinez,2015; Yadav, Ladusingh & Gayawan,2015). However, most of the existing stud-ies are restricted to 2005-06 and there-fore do not provide any information aboutthe child malnutrition at state level duringrecent years. The present study examinesin detail the trends and patterns of childmalnutrition at regional level. The studyalso examines the socio-economic in-equalities in child malnutrition during 2005-06 to 2015-16.
Related Literature on ChildMalnutrition
Using NFHS data, several studiesfind the existence of significant inter-stateand rural-urban disparities in child mal-nutrition in the case of India. One of theimportant findings of these studies is that
Middle income states have shownbetter performance with respect tochild nutrition than high-incomestates.

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 69
middle income states have shown betterperformance with respect to child nutri-tion than high-income states.These stud-ies also argue that poverty reduction hasnot led to substantial improvement in nu-tritional outcomes of Indian children (e.g.Radhakrishna, Rao, Ravi & Reddy, 2004;Nair, 2007; Deaton &Dreze, 2009).Studies have attempted to provideseveral explanations for the prevalenceof inter-state disparities in child malnu-trition. Cavatorta et. al., (2015) have ex-tensively reviewed the two strands ofliterature which explain these variations.The first strand of literature argues thatstates differ with respect to nutritionalachievements because of differences inendowments (UNICEF, 1990; Nair,2007; Kumar & Kumari, 2014). Theseendowments include factors such asavailability of health facilities, hospitals,maternal literacy, agricultural productionand household wealth. Nair (2007) findsthat these disparities have increased be-tween NFHS-1 (1992-93) and NFHS-3(2005-06). He argues that economicallyunderdeveloped and populous statessuch as Uttar Pradesh (U.P.) and Biharhave witnessed an increase in the ex-tent of child malnutrition which cannotbe tackled by merely emphasizing onachieving high economic growth. In or-der to achieve better nutritional out-comes, the study suggests measures likeincreasing women’s age at first childbirth, implementing timely lactating prac-tices and improving maternal literacy.Other studies at the regional level havealso reached similar conclusions on theextent of inter-state and rural-urban dis-parities with respect to child malnutri-
tion in India (e.g. Kumar, 2007; Pathak& Singh, 2011).On the other hand, second strand ofliterature argues that similar endowmentsin some states may give rise to drasticallydifferent nutritional results (Harriss&Kohli, 2009; Cavatorta et. al., 2015). Thismay happen because states differ in termsof quality of public services, institutions,and policies. Cavatorta et. al., (2015) ana-lyze the interstate disparities in child mal-nutrition (measured by height for age) bycomparing the performance of Bihar, UttarPradesh, Madhya Pradesh and Gujarat(poor performing states) with that of TamiNadu (good performing state). Their re-sults highlight that differences in stuntingacross states are not significantly ex-plained by differences in endowments.Other studies have also examined the roleof institutions and policies in affecting childmalnutrition in India (Walton, 2009;Balarajan& Reich, 2016).
Differences in stunting acrossstates are not significantly ex-plained by differences in endow-ments.
It is argued that interaction of socialand economic factors affects the extentof child malnutrition. Studies have estab-lished that there exists a close link be-tween the socio-economic factors andchild health (Wagstaff, 2000; Kumar,Kumari &Singz, 2015; Pulok, Sabah&Enemark, 2016).There are severalstudies for developing countries whichhave examined the extent of socioeco-nomic inequalities in child malnutrition

Anand Sharma
70 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
(e.g. Wagstaff, 2000; Subramanyam,Kawachi, Berkman &Mazumdar, 2010;Kumar et. al., 2015; Prakash & Jain,2016; Pulok et. al., 2016; Nie et. al.,2016). The relationship between povertyand socioeconomic inequalities and childmalnutrition is analyzed by Mazumdar(2010) using NFHS-3 data (for 2005-6).He finds importance of poverty in ex-plaining the observed disparities in childmalnutrition among different sections ofthe society. His results also highlight thatthe poor sections of the population beara relatively greater burden of child mal-nutrition. However, this study is restrictedto a single point of time and does notanalyze the how these inequalities havechanged over time.There exist studies which have exam-ined the trend of socioeconomic inequali-ties in child malnutrition during NFHS-1(1992-93) and NFHS-3 (2011-12). Major-ity of these studies find that these inequali-ties have witnessed an increase in Indiaover the last two decades (e.g.Subramanyam et. al., 2010; Pathak &Singh, 2011; Kumar et; al., 2015; Prakash& Jain 2016). A study by Pathak & Singh(2011) which studies only the trends ofeconomic inequalities with regard to childmalnutrition finds an increase betweenNHFS-1 (1992-93) and NFHS-3 (2011-12). This study also argues that poor chil-dren are at a greater disadvantage andsuffer from severe malnutrition. In addi-tion to economic inequalities (measured byhousehold wealth), Subramanyam et. al.,(2010) analyze the trends of social dis-parities in child malnutrition by examiningfactors such as caste, gender, and mater-nal education. This study finds no inequali-
ties in child malnutrition by caste and gen-der. It also asserts that inequalities in mal-nutrition by maternal education are sig-nificantly lesser than those by householdwealth. However, for urban India Kumaret. al. (2015) find exactly the opposite re-sult. They find evidence of increasing so-cioeconomic inequalities in India during thelast two decades and advocate the imple-mentation of policies specific to urban ar-eas of the country.Household wealth and maternal lit-eracy explain the prevalence ofsocio-economic inequalities inchild malnutrition.
In addition to the trend analyzes ofinequalities in malnutrition, various schol-ars have also attempted a detailed exami-nation by doing a decomposition analysisof the inequalities (e.g. Joe, Mishra&Navaneetham, 2009; Kumar & Kumari,2014; Cavatorta et. al., 2015; Prakash &Jain 2016; Nie et. al., 2016). Using con-centration indices and concentrationcurves, these studies find that householdwealth and maternal literacy explain theprevalence of socio-economic inequalitiesin child malnutrition. On the basis ofNFHS-3 (2005-06) data, Mazumdar(2010) finds that household wealth andmaternal education predominantly explainsthe disparity in child malnutrition. He ar-gues that policymakers should aim atachieving social and economic develop-ment which may reduce the prevalenceof child malnutrition in India. Similar con-clusions are obtained by Prakash & Jain(2016) who analyze the socio-economicinequalities in child malnutrition between

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 71
NFHS-1 (1992-93) and NFHS-3 (2005-06). They advocate the need for continu-ous review of target- based schemes andincreasing the focus on parental educa-tion. Several studies have exclusively ana-lyzed the determinants of socio-economicinequalities in child malnutrition for urbanIndia (Kumar et. al., 2015) whereas oth-ers have focused on rural India (Cavatortaet. al., 2015). These studies also point outthe existence of significant rural-urban dif-ferentials with respect to child malnutri-tion.Some studies have also argued thatchildren belonging to scheduled castes(SCs) and scheduled tribes (STs) havepoor nutritional status as compared toother children (e.g. Van de Poel &Speybroeck, 2009; Yadav et. al., 2015).However, scholars find that the link be-tween caste and nutritional status of chil-dren become weak once householdwealth and maternal education are takeninto consideration (Subramanyan et. al.,2010). This supports the findings of de-composition- based studies which arguethat both these factors significantly con-tribute to socio-economic inequalities inchild malnutrition.The present study focuses on exam-ining the interstate disparities in childmalnutrition in India between NFHS-3(2005-06) and NFHS-4 (2011-12). It ex-amines the trends and patterns at regionallevel across caste, residence and genderand attempts to provide possible expla-nations for the observed patterns. In ad-dition, this paper analyses the socioeco-nomic inequality trends in child malnutri-tion in India.
Data Sources &Methods
National Family Health Survey(NFHS) data of the two rounds carriedout in 2005-06 (NFHS-3) and 2015-16(NFHS-4) is the major database used inthis study. NFHS is administered andcoordinated by International Institute ofPopulation Sciences (IIPS), Mumbai un-der aegis of Ministry of Health & FamilyWelfare, Government of India. NFHS hasa broader coverage of states, covering99% of population in 29 states (Nair,2007; IIPS& ICF, 2008). NFHS providesuseful information related to health andfamily welfare with an objective to ana-lyze the performance of health sector(IIPS& ICF, 2017).This study examines the nutritionalstatus of children aged below five yearson the basis of three anthropometricmeasures: ‘weight-for-age’, ‘weight-for-height’, and ‘height-for-age’. Childrenare classified as underweight, wastedand stunted when the respective z-scoreis below minus two standard deviationsof median values of international refer-ence group (Dibley et. al., 1987; WHO,2010; Kumar & Kumari, 2014). However,following the literature we examine indetail the level of child nutrition in termsof ‘weight-for-age’ (i.e. percentage ofunderweight children). This is done be-cause ‘weight-for-age’ comprehensivelymeasures both long-term and short-termnutritional performance (Nair, 2007;Deaton & Dreze, 2009) and it is the onlyinformation which is comparable acrossrounds (Kumar & Kumari, 2014; Prakash& Jain, 2016).

Anand Sharma
72 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
In this study, we compare the childmalnutrition performance across differ-ent states to examine the inter-state dis-parities during the ten year period be-tween NFHS-3 (2005-06) and NFHS-4(2015-16). We also compare the perfor-mance of states with India as a whole tosee which states have performed belowthe national average. Following Nair(2007), we compute the relative statemalnutrition index (RSMI) by comparingthe level of child malnutrition in a statewith the national level. The formula usedis: RSMI = (MNS/MNN)*100 w h e r eMNS and MNN denotes malnutrition in astate and nation respectively. The per-centage change in RSMI betweenNFHS-3 and NFHS-4 indicates the con-vergence/divergence in malnutrition per-formance across states.Further, the study attempts to exam-ine the socio-economic inequalities inchild malnutrition(by place of residence)between NFHS-3 (2005-06) and NFHS-4 (2015-16). This is done by using study‘concentration curve’ (CC) and ‘concen-tration index’ (CI). Previous studies onhealth and nutrition have extensively usedthese to study socio-economic inequali-ties in child malnutrition (Wagstaff et. al.,1991; Kakwani et. al., 1997; Kumar et.al., 2015). CC graphically depicts thesocio-economic inequalities in child mal-nutrition (Pulok et. al., 2016). It plots thecumulative percentage of population (or-dered by wealth/income) against the cu-mulative percentage of health variable(Wagstaff et. al., 1991; Pulok et. al.,2016). This curve is analogous to the‘Lorenz curve’ with diagonal represent-ing the line of equality. Closer this curve
is to the line of equality, lesser is the in-equality in health and vice-versa.However, scholars argue that CC isa graphical illustration and does not giveany information about the magnitude ofsocio-economic inequalities in health(Pulok et al., 2016; Prakash & Jain,2016). CI gives a quantitative measureof socio-economic inequalities in health.It is defined as twice the area betweenCC and line of equality with values rang-ing from -1 to +1 (Wagstaff et. al., 1991;Mazumdar, 2010). The negative valuesindicate the uneven concentration ofhealth variable among economicallyweaker sections of the population. Wecompute the CI for three measures (un-derweight, wasting, and stunting) forNFHS-3 (2005-06) and NFHS-4 (2015-15) by place of residence (rural and ur-ban). Following Wagstaff et. al. (1991)and Kakwani et. al. (1997), CI is com-puted by the formula:Concentration Index (CI) = 2 Cov(y, h)/µWhere Cov (y, h) is the covariancebetween relative rank in terms of wealthindex, y and health variable, h and µ isthe mean of health variable.
Findings & Discussion
First, we examine the trends and pat-tern of child malnutrition at the nationallevel during the ten year period cover-ing NFHS-3 (2005-06) and NFHS-4(2015-16). This analysis is done by resi-dence (urban/rural) and caste catego-ries. We explain the performance and

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 73
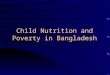
state of child health in India by studyingthe condition of basic health servicessuch as vaccination of children, facili-ties related to maternity care etc. Then,we examine the inter-state disparities inchild malnutrition in terms of stunted,wasted and underweight children be-tween the two rounds of NFHS. We alsolook at rural-urban and caste-wise dif-ferentials in child malnutrition at the re-gional level. Finally, this section dis-cusses the trend in socio-economic in-equalities in child health by residencebetween NFHS-3 and NFHS-4.The proportion of children belowfive years who were stunted, wasted,and underweight at the all-India level areshown in Fig. 1. According to NFHS-4,about 38 percent children were stunted,21 percent children were wasted, and
36 percent children were underweightin 2015-16. The proportion of Indianchildren who are stunted is matched byunderdeveloped countries such asSudan, Mali, Chad, and Zambia. EvenIndia’s neighboring countries such asBangladesh, Bhutan, Nepal, and SriLanka perform better with respect to thisindicator (International Food Policy Re-search Institute, 2016). Figure 1 alsoshows that India has not been able toachieve significant gains in nutritionalperformance during the ten-year periodbetween NFHS-3 and NFHS-4. In ad-dition, the proportion of wasted childrenhas increased from 19.8 percent inNFHS-3 (2005-06) to 21 percent inNFHS-4 (2015-16). The proportion ofunderweight children is reduced by lessthan 7 percent during the ten-year longperiod.Fig. 1 Nutritional Status of Children Below 5 Years (in percentage) in NHFS-3 & NFHS-4
Source: NFHS-4 Fact Sheets (2015-16)Table 1 shows that rural areas of thecountry are at a comparatively disadvan-tageous position than the urban areas.The proportion of stunted and under-
weight children below five years in ruralIndia exceeds those in urban India byabout 10 percent. However, the diver-gence is much less with respect to the

Anand Sharma
74 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
proportion of wasted children. The poorstate of child health in rural regions of India would affect the future productiv-ity and economic performance of theseregions. The comparatively dismal stateof child nutrition in rural India is the re-sult of continuous neglect of health fa-cilities and infrastructure which requiresdrastic policy reforms from the govern-ment.
The proportion of stunted and un-derweight children below fiveyearsin rural India exceeds thosein urban India by about 10 percent.
Table 1 Child Malnutrition by Place of Residence (All India) (Percentage of Stunted, Wasted& Underweight Children) NFHS-4 (2015-16)
NFHS-4 (2015-16) NFHS-3 All- India(2005-06) Children under five Urban Rural India India % Change Remarksyears who are
Stunted 31 41.2 38.4 48 -9.6 ImprovesWasted 20 21.5 21 19.8 1.2 DeterioratesUnderweight 29.1 38.3 35.8 42.5 -6.7 ImprovesSource: NFHS-3 & NFHS-4
Some scholars argue that women be-longing to scheduled castes (SCs), sched-uled tribes (STs), and other backwardclasses (OBCs) are in a disadvantageousposition with respect to availability andutilization of health care services (e.g.Navaneetham & Dharma-lingam, 2002).This is likely to have a significant effecton child health and well-being. Table 2depicts the nutritional status of childrenbelonging to different social groups. Theproportion of stunted, wasted, and under-weight children among SCs, STs, andOBCs is higher than those in the ‘Other’category. For example, in NFHS-4, about
39 percent children were underweight inSC group, 35 percent in ST group, and 36percent in OBC group, whereas about 27percent children were underweight in theOther group. The relatively disadvanta-geous social groups have not witnessed asignificant improvement between NFHS-3 and NFHS-4. Table 2 highlights this lim-ited improvement in nutritional status ofchildren among the social groups betweenthe two NFHS rounds.Previous studies have pointed out thecrucial role of maternal health, child im-munization, and access to basic healthservices in affecting child health (Joe et.al., 2009; Kumar, 2007).Table 3 clearlyshows the limited progress with respectto indicators related to child feeding prac-tices and maternal care. For example, thepercentage of children under age 6 monthswho were exclusively breastfed increased
The proportion of stunted, wasted,and underweight children amongSCs, STs, and OBCs is higher thanthose in the ‘Other’ category.

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 75
Table 2 Nutritional Status of Children by Caste in NFHS-3 & NFHS-4
Percentage of SC ST OBC OtherChildren Below5 Years Who Are NFHS-3 NFHS-4 NFHS-3 NFHS-4 NFHS-3 NFHS-4 NFHS-3 NFHS-4Stunted 50.38 43.24 46.61 39.6 45.7 39.33 35.84 30.56Wasted 19.92 21.71 20.38 21.71 19.09 20.86 15.59 17.96Underweight 44.11 39.42 39.2 34.84 39.76 36.15 29.28 26.93Source: Calculated from NFHS-3 and NFHS-4 datafrom about 46 percent in NFHS-3 to 55percent in NFHS-4. This increase of only9 percentage points over a period of tenyears appears quite insignificant. On theother hand, there has been a decline inthe proportion of children aged 6-8 monthsreceiving solid/semi-solid food and breastmilk. Access and availability of facilitiesrelated to mother’s health are also a pri-mary determinant of child health and well-being. Table 3 highlights the limitedTable 3 State of Basic Health Services (All India) in NFHS-3 & NFHS-4
Parameters NFHS-3 NFHS-4Child immunization and Vitamin A supplementation (percent)Children age 12-23 months fully immunized (BCG, Measles, and 43.5 62three doses each of polio/DPT)Children age 12-23 months who have received BCG 78.2 91.9Children age 12-23 months who have received three doses of polio vaccine 78.2 72.8Children age 12-23 months who have received three doses of DPT vaccine 55.3 78.4Children age 12-23 months who have received measles vaccine 58.8 81.1Children age 9-59 months who have received Vitamin A dose in last 6 months 16.5 60.2Child Feeding practices (percent)Children under age 3 years breastfed within one hour of birth 23.4 41.6Children under age 6 months exclusively breastfed 46.4 54.9Children age 6-8 months receiving solid or semi-solid food and breastmilk 52.6 42.7Maternity Care (percent)Mothers who had antenatal check-up in the first trimester 43.9 58.6Mothers who had at least 4 antenatal care visits 37 51.2Mothers who had full antenatal care 11.6 21Source: NFHS-3 & NFHS-4
progress with respect to maternity careindicators. For example, the proportion ofwomen receiving full antenatal care in-creased to 21 percent in NFHS-4 fromabout 12 percent in NFHS-3. This impliesabout one-fifth of the pregnant womenhad access to full-antenatal care.One-fifth of the pregnant womenhad access to full-antenatal care.
The trends at the national level do notreveal the inter-state disparities in nutri-tional status of children. Tables 4 to 7 at-tempt to highlight the child malnutritionscenario at the regional level. Table 4 re-veals the percentage of children under five

Anand Sharma
76 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
who are malnourished (stunted, wasted,and underweight) across the states basedon NFHS-4 data. The percentage ofstunted children under five ranges frombelow 25 percent in Goa, Tripura andPunjab to above 45 percent in Bihar,Jharkhand and Uttar Pradesh. Except,Meghalaya, the north-eastern states haveperformed better than the national aver-age in this indicator. Similarly, Table 4 high-lights considerable variation across stateswith respect to the proportion of wasted
children. For example, the proportion ofwasted children is close to 6 percent in arelatively economically underdevelopedstate like Mizoram whereas this figure isclose to 26 percent in a relatively devel-oped state like Karnataka. The proportionof underweight children also vary drasti-cally across the different states with low-est proportion in Sikkim and highest inBihar. The coefficient of variation revealsthat the variation across states is largestin proportion of underweight children.Table 4 State-wise Child Malnutrition in NFHS-4 (2015-16)
State Percentage of Percentage of Percentage of Under-Stunted Children WastedChildren weight ChildrenAndhra Pradesh 31.4 17.2 31.9Arunachal Pradesh 29.4 17.3 19.4Assam 36.4 17 29.8Bihar 48.3 20.8 43.9Chhattisgarh 37.6 23.1 37.7Goa 20.1 21.9 23.8Gujarat 38.5 26.4 39.3Haryana 34 21.2 29.4Himachal Pradesh 26.3 13.7 21.2Jammu & Kashmir 27.4 12.1 16.6Jharkhand 45.3 29 47.8Karnataka 36.2 26.1 35.2Kerala 19.7 15.7 16.1Madhya Pradesh 42 25.8 42.8Maharashtra 34.4 25.6 36Manipur 28.9 6.8 13.8Meghalaya 43.8 15.3 28.9Mizoram 28.1 6.1 12Nagaland 28.6 11.3 16.7Odisha 34.1 20.4 34.4Punjab 25.7 15.6 21.6Rajasthan 39.1 23 36.7Sikkim 29.6 14.2 14.2Tamil Nadu 27.1 19.7 23.8Telangana 28 18.1 28.4Tripura 24.3 16.8 24.1Uttar Pradesh 46.3 17.9 39.5Uttarakhand 33.5 19.5 26.6West Bengal 32.5 20.3 31.6Coefficient of Variation (C.V.) 22.31 29.51 34.25Source: NFHS-4

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 77
Table 5 State-wise Underweight Children (%) by Place of Residence in NFHS-4 (2015-16)
State Urban Rural Overall Rural-Urban ratioAndhra Pradesh 28.4 33.1 31.9 1.17Arunachal Pradesh 13.8 20.9 19.4 1.51Assam 21.4 30.8 29.8 1.44Bihar 37.5 44.6 43.9 1.19Chhattisgarh 30.2 39.6 37.7 1.31Goa 25.3 21.2 23.8 0.84Gujarat 32 44.2 39.3 1.38Haryana 28.5 29.9 29.4 1.05Himachal Pradesh 17.1 21.6 21.2 1.26Jammu & Kashmir 17 16.5 16.6 0.97Jharkhand 39.3 49.8 47.8 1.27Karnataka 31.5 37.7 35.2 1.20Kerala 15.5 16.7 16.1 1.08Madhya Pradesh 36.5 45 42.8 1.23Maharashtra 30.7 40 36 1.30Manipur 13.1 14.2 13.8 1.08Meghalaya 22.9 29.9 28.9 1.31Mizoram 8.5 15.7 12 1.85Nagaland 13.6 17.9 16.7 1.32Odisha 26.2 35.8 34.4 1.37Punjab 22.4 21.1 21.6 0.94Rajasthan 30.7 38.4 36.7 1.25Sikkim 12 15.4 14.2 1.28Tamil Nadu 21.5 25.7 23.8 1.20Telangana 22.1 33.1 28.4 1.50Tripura 21.7 25 24.1 1.15Uttar Pradesh 33.7 41 39.5 1.22Uttarakhand 25.6 27.1 26.6 1.06West Bengal 26.2 33.6 31.6 1.28Coefficient of variation (C.V.) 33.08 34.50 34.25Source: NFHS-4
Several studies have argued that ru-ral areas of India are at a greater disad-vantage in comparison to the urban ar-eas with respect to the nutritional per-formance of children (Smith et. al., 2005;Kumar, 2007; Cavatorta et. al., 2015).The data shown in Table 5 supports thisview. In all the states (except Jammu &Kashmir, Goa, and Punjab), the propor-tion of underweight children under fivein rural areas is considerably higher thanin urban areas. The rural-urban differ-
Rural areas of India are at agreater disadvantage in compari-son to the urban areas with respectto the nutritional performance ofchildren.
ential is highest in Mizoram, ArunachalPradesh, and Telangana. It is importantto examine the reasons for differentialnutritional performance at the state level.

Anand Sharma
78 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
The health facilities related to child andmaternal care play a vital role in influ-encing child health. Table 6 compares theindicators related to child and maternalcare in four top-ranked(Mizoram,Manipur, Sikkim, and Kerala) and fourbottom-ranked (Jharkhand, Bihar,Madhya Pradesh, and Uttar Pradesh)child malnutrition (in terms of proportionof underweight children under five)
states. This comparison makes it clearthat indicators of child and maternal careare significantly better in the four top-ranked states. For example, the propor-tion of women whose body mass index(BMI) is below normal ranges from 25to 43 percent in the four bottom-rankedstates. On the other hand, this figureranges from 8 to 18 percent in the fourtop-ranked states.Table 6 Health Indicators in Low& High Child Malnutrition States(Percentage of Under-
weight Children Below Five Years)
Some Indicators of Child care Some Indicators of Maternal careBest and Under- Children Children Children Mothers Births Womenworst weight under of 6-8 with who had assisted whoseperforming children three months diarrhoea at least by a BMI isstates below years receiving in the last four trained belowfive years breastfed solid or 2 weeks antenatal birth normalwithin one semi-solid who care visits attendanthour of food and received for theirbirtho breast milk ORS last birthFour top-ranked statesMizoram 12 70.3 68.2 70 61.4 83.6 8.4Manipur 13.8 65.4 78.8 60.2 69 77.2 8.8Sikkim 14.2 66.5 61.8 NA 74.7 97.1 11.2Kerala 16.1 64.3 63.1 49.4 90.1 99.9 18Four bottom-ranked statesJharkhand 47.8 33.1 47.2 44.8 30.3 69.6 42.9Bihar 43.9 34.9 30.8 45.2 14.4 70 30.4M.P. 42.8 34.4 38.1 55.2 35.7 78 28.4Uttar Pradesh 39.5 25.2 32.6 37.9 26.4 70.4 25.3Source: NFHS-4
The four bottom-ranked states alsohave a relatively lower per capita incomein 2015-16. Table 7 shows that thesestates also lie at the bottom in terms ofper capita income. This points out to thefact that economic growth and childhealth are strongly associated. However,it is also clear from Table 7 that economi-cally advanced states such as
Maharashtra, Gujarat, and Haryana haveshown a dismal performance with re-spect to child nutrition. Therefore,thisstudy confirms the findings of previousstudies which argue that a high rate ofeconomic growth does not necessarilybring improved nutritional outcomes forchildren (Deaton &Dreze, 2009;Subramanyam et. al., 2010).

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 79
Table 7 Comparison of Per Capita Income & Child Malnutrition: State-wise
State Child malnutrition, Rank by Per capita income Rank by incomeNFHS-4 (% of under- malnutrition (Rs.) in 2015-16 (atweight children) 2011-12 prices)Goa 23.8 10 278601 1Sikkim 14.2 3 195066 2Haryana 29.4 16 133591 3Uttarakhand 26.6 13 126306 4Maharashtra 36 22 122588 5Gujarat 39.3 25 120683 6Kerala 16.1 4 119665 7Tamil Nadu 23.8 11 114581 8Karnataka 35.2 21 113303 9Himachal Pradesh 21.2 8 112723 10Telangana 28.4 14 112267 11Punjab 21.6 9 100141 12Mizoram 12 1 91845 13Andhra Pradesh 31.9 19 86118 14Arunachal Pradesh 19.4 7 83536 15Rajasthan 36.7 23 68048 16Tripura 24.1 12 64173 17Chhattisgarh 37.7 24 63791 18Nagaland 16.7 6 60663 19Jammu & Kashmir 16.6 5 59924 20Odisha 34.4 20 58165 21West Bengal 31.6 18 57255 22Meghalaya 28.9 15 56039 23Assam 29.8 17 50642 24Madhya Pradesh 42.8 27 47646 25Manipur 13.8 2 46389 26Jharkhand 47.8 29 44524 27Uttar Pradesh 39.5 26 36923 28Bihar 43.9 28 23987 29Source: NFHS-4 & ESO, Punjab
Next, we compare the extent of childmalnutrition (in terms of proportion of un-derweight children below five years) indifferent states with the all-India level.This is shown in Table 8 by computingthe RSMI for 2005-06 (NHFS-3) and2015-16 (NFHS-4).According to NFHS-3 data, MadhyaPradesh shows the worst performance incomparison to the all-India level. Out of
the 27 states listed in Table 8, 13 statesshow a child malnutrition level which ex-ceeds the national average. Sikkim andMizoram show best performance in childmalnutrition. Table 8 also shows that eco-nomically developed states such asGujarat, Haryana, Uttarakhand, andKarnataka perform worse than the na-tional average. In 2015-16 (NFHS-4)Madhya Pradesh is replaced by Bihar asit shows the worst relative position.

Anand Sharma
80 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
Table 8 State-wise Relative Child Malnutrition (% of Underweight Children Below Five Years)in NFHS-3 (2005-06) & NFHS-4 (2015-16)
State Value of RMN in Value of RMN in Percentage changeNFHS-3 (2005-06) NFHS-4 (2015-16) in RMNArunachal Pradesh 86.13 54.19 -37.08Assam 85.39 83.24 -2.52Bihar 144.40 122.63 -15.08Chhattisgarh 121.54 105.31 -13.35Goa 72.29 66.48 -8.04Gujarat 118.88 109.78 -7.66Haryana 106.34 82.12 -22.77Himachal Pradesh 91.50 59.22 -35.28Jammu & Kashmir 82.29 46.37 -43.65Jharkhand 144.45 133.52 -7.57Karnataka 100.55 98.32 -2.22Kerala 62.86 44.97 -28.45Madhya Pradesh 149.28 119.55 -19.92Maharashtra 96.18 100.56 4.55Manipur 57.67 38.55 -33.16Meghalaya 127.67 80.73 -36.77Mizoram 53.80 33.52 -37.70Nagaland 63.48 46.65 -26.51Odisha 104.66 96.09 -8.19Punjab 65.27 60.34 -7.57Rajasthan 106.12 102.51 -3.40Sikkim 53.80 39.66 -26.27Tamil Nadu 78.38 66.48 -15.18Tripura 103.62 67.32 -35.03Uttar Pradesh 107.08 110.34 3.04Uttarakhand 100.61 74.30 -26.15West Bengal 94.14 88.27 -6.24Source: Calculated using NFHS-3 & NFHS-4 dataAccording to NFHS-4, the number ofstates performing below the national av-erage is reduced from 13 to 8. Despitelow income levels, the north-eastern statessuch as Mizoram, Sikkim, Manipur, andNagaland continue to perform better thanthe national average. The inferior perfor-mance of states such as Gujarat andMaharashtra provides more support to theargument that economic growth is inad-
equate to lead to significant improvementsin health and nutrition.In agreement with the existing stud-ies, we find that a relatively greater pro-portion of malnourished children are con-centrated in poor households in both ru-ral and urban India.This is shown in partsa, b and c of fig. 2 which depict the con-centration curves (CC) for stunting,

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 81
wasting, and underweight in rural andurban India for NFHS-3 (2005-06) andNFHS-4 (2015-16). All the curves lieabove the line of equality in NFHS-3 andNFHS-4. This implies a larger concen-tration of malnourished children amongthe economically weaker sections of thesociety in both rural and urban areas.The
negative values of CIs shown in Table 9provide further support to the presenceof socioeconomic inequalities in child mal-nutrition. CI values in Table 9 also re-veal that the inequalities in stunting haveremained unchanged whereas there ap-pears to be a slight reduction in inequali-ties with respect to wasted and under-weight children during NFHS-3 (2005-06) and NFHS-4 (2015-16). The pres-ence of these inequalities is an obstaclein raising the level of human developmentand requires appropriate policy reformsfrom the government.
Relatively greater proportion ofmalnourished children are concen-trated in poor households in bothrural and urban India.
Table 9 Concentration Index of Child Malnutrition in India (NFHS-3 & NFHS-4)
NFHS-3 (2005-06) NFHS-4 (2015-16)Stunting Overall (India) -0.1294 -0.1271Urban -0.1095 -0.1051Rural -0.0951 -0.1041Wasting Overall (India) -0.1224 -0.0796Urban -0.0728 -0.0563Rural -0.0985 -0.0704Underweight Overall (India) -0.1291 -0.1075Urban -0.0979 -0.0836Rural -0.0976 -0.0904Source: Calculated from NFHS-3 & NFHS-4 dataFig. 2 (a) Concentration Curves of Stunted Childrenin Rural & Urban India: NFHS-3 &
NFHS-4

Anand Sharma
82 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
Figure 2: (b) Concentration curves of Wasted children in Rural & Urban India: NFHS-3&NFHS-4
Figure 2: (c) Concentration Curves of UnderweightChildren in Rural & Urban India: NFHS-3& NFHS-4
Conclusion & Policy Implications
This study examined the trends andpattern of child malnutrition at the na-tional and state levels during the ten-yearperiod covering NFHS-3 (2005-06) andNFHS-4 (2015-16). At the all-India level,the study finds that about 36 percent chil-dren below five years were underweight,21 percent were wasted, and 38 percentwere stunted in 2015-16. Compared to
NFHS-3, these figures reveal a limitedimprovement in the nutritional status ofchildren over the ten-year period. It isalso clear that rural India suffers moreseverely with a significantly higher pro-portion of malnourished children.The disparities across states havenot undergone a significant changeduring 2005-06 and 2015-16.

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 83
The study finds significant variationsin child malnutrition levels acrossstates.The disparities across states havenot undergone a significant change dur-ing 2005-06 and 2015-16. On an aver-age, the north-eastern states such asMizoram, Manipur, and Sikkim have lowrates of child malnutrition and performbetter than other states. Bihar,Jharkhand, Madhya Pradesh and UttarPradesh are the worst performers withproportion of underweight children in therange of 40 to 48 percent. We find thatthe key reason for this differential per-formance across states appears to be thediffering status of child and maternal careindicators. The best-performing stateshave better health care indicators. Thestudy also finds that states such asGujarat, Maharashtra, and Karnatakahave high rates of child malnutrition de-spite strong economic performance.The NFHS data suggests limited ac-cess and reach of health infrastructureand related health care services. There-fore, it is important for the governmentto initiate major reforms in the healthsector across states.Further, an effectiveimplementation of the existing nutritionschemes such as National Midday MealScheme and Integrated Child Develop-ment Services (ICDS) would help in re-ducing the incidence of severe malnutri-tion. Several studies have argued thatmaternal education plays an importantrole in tackling the problem of child mal-nutrition (Joe et. al., 2009; Christiaensen& Alderman, 2004; Prakash & Jain,2016) as it improves the understandingof health and nutrition issues (Miller &Rodgers, 2009). Therefore, it is impor-
tant to accord a high priority to educa-tion, especially of rural women. The gov-ernment should undertake substantial in-vestment in education and literacy pro-grams and carry out a continuous moni-toring of the seprograms.Several initia-tives of the government such as‘BetiBachao, BetiPadhao’, ‘KasturbaBalika Vidyalaya’, and ‘Rajiv GandhiScheme for Empowerment of AdolescentGirls’ are steps in the right direction. Ithas also been pointed that ensuring mar-riage and pregnancy at the right age,adopting healthy breastfeeding practices,and better antenatal care practices wouldhelp in tackling the problem of child mal-nutrition (Nair, 2007; Niti Aayog, 2017).In this regard, sustained and targetedefforts from the policymakers are neededwhich may lead to an improvement in thenutritional outcomes for children.References
Aayog, N. I. T. I. (2017), Government ofIndia. Nourishing India—National Nutri-tion Strategy. Retrieved from niti.gov.in/writereaddata/files/document_publicationBalarajan, Y. & Reich, M. R. (2016),”PoliticalEconomy of Child Nutrition Policy: aQualitative Study of India’s IntegratedChild Development Services (ICDS)Scheme”, Food Policy, 62: 88-98.Barro, R. J . (2001),”Human Capital andGrowth”, American Economic Re-
view, 91(2): 12-17.Cavatorta, E., Shankar, B. & Flores-Martinez, A.(2015),”Explaining Cross-state Disparitiesin Child Nutrition in Rural India”, World
Development, 76: 216-37.Christiaensen, L. & Alderman, H. (2004),”ChildMalnutrition in Ethiopia: Can MaternalKnowledge Augment the Role of

Anand Sharma
84 The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019
Income?” Economic Development and Cul-tural Change, 52(2): 287-312.
Collin, M. & Weil, D. (2018),”The Effect of In-creasing Human Capital Investment on Eco-nomic Growth and Poverty: A SimulationExercise”, Policy Research Working PaperNo. 8590, World Bank.Deaton, A. &Dreze, J. (2009),”Food and Nutri-tion in India: Facts and Interpretations”,
Economic and Political Weekly: 42-65.Dibley, M. J., Staehling, N., Nieburg, P. &Trowbridge, F. L. (1987),”Interpretation ofZ-score Anthropometric Indicators Derivedfrom the International Growth Reference”, The American Journal of Clinical Nutri-
tion, 46(5): 749-62.Global Nutrition Report (2018), Shining a Lightto Spur Action on Nutrition, World Health
Organization.Gragnolati, M., Bredenkamp, C., Shekar, M., DasGupta, M. & Lee, Y. K. (2006), India’sUndernourished Children: a Call for Reformand Action, The World Bank.Grantham-McGregor, S. M., Fernald, L. C.&Sethuraman, K. (1999),”Effects of Healthand Nutrition on Cognitive and BehavioralDevelopment in Children in the First ThreeYears of Life. Part 1: Low Birthweight,Breastfeeding, and Protein-energy Malnu-trition”, Food and Nutrition Bulletin, 20(1):53-75.Haddad, L. (2009),”Lifting the Curse: Overcom-ing Persistent Undernutrition in India”,
IDS Bulletin, 40(4): 1-8.Harriss, J. & Kohli, N. (2009),”Notes on the Dif-fering ‘States’ of Child Undernutrition inRural India”, IDS Bulletin, 40(4): 9-15.Hoddinott, J. (2009),”Early Childhood NutritionIncreases Adult Wages”,EuroChoices [Spe-cial Issue], 8: 34–37International Food Policy Research Institute(2016),Global Nutrition Report: 2016:From Promise to Impact: Ending Malnu-trition by 2030, Washington, D.C.
International Institute for Population Sciences(IIPS) and ICF. (2008), National FamilyHealth Survey (NFHS-3), 2005-06: India,Mumbai: IIPSInternational Institute for Population Sciences(IIPS) and ICF. (2017). National FamilyHealth Survey (NFHS-4), 2015-16: India.Mumbai: IIPSJoe, W., Mishra, U. S. &Navaneetham, K.(2009),”Inequalities in Childhood Malnu-trition in India: Some Evidence on GroupDisparities”, Journal of Human Develop-
ment and Capabilities, 10(3): 417-39.Kakwani, N., Wagstaff, A. & Van Doorslaer, E.(1997),”Socioeconomic Inequalities inHealth: Measurement, Computation, andStatistical Inference”, Journal of Econo-
metrics, 87-103Kumar, A. S. (2007),”Why Are Levels of ChildMalnutrition Not Improving?” Economic
and Political Weekly: 1337-45.Kumar, A., & Kumari, D. (2014),”Decomposingthe Rural-urban Differentials in ChildhoodMalnutrition in India, 1992–2006, Asian
Population Studies, 10(2): 144-62.Kumar, A. Kumari, D.& Singh, A. (2014),”In-creasing Socioeconomic Inequality in Child-hood Undernutrition in Urban India: Trendsbetween 1992–93, 1998–99 and 2005–06", Health Policy and Planning, 30(8):1003-16.Mazumdar, S. (2010),”Determinants of Inequal-ity in Child Malnutrition in India: the Pov-erty-Undernutrition Linkage”, Asian Popu-
lation Studies, 6(3): 307-33.Miller, J. E. & Rodgers, Y. V. (2009),”Mother’sEducation and Children’s Nutritional Sta-tus: New Evidence from Cambodia”,Asian
Development Review, 26(1): 131-65.Nair, K.R.G. (2007),”Malnourishment amongChildren in India: A Regional Analysis”,
Economic and Political Weekly: 3797-03.Navaneetham, K. &Dharmalingam, A. (2002),“Utilization of Maternal Health Care Ser-

Child Malnutrition in India
The Indian Journal of Industrial Relations, Vol. 55, No. 1, July 2019 85
vices in South India”,Social Science & Medi-cine, 55(10): 1849-69.
Nie, P., Rammohan, A., Gwozdz, W. & Sousa-Poza, A. (2016),”Developments in Under-nutrition in Indian Children Under Five: ADe-compositional Analysis”, IZA Discus-sion Papers, No. 9893, Institute for theStudy of Labor (IZA), Bonn.Pathak, P. K. & Singh, A. (2011),”Trends in Mal-nutrition among Children in India: Grow-ing Inequalities across Different EconomicGroups”, Social Science & Medicine, 73(4):576-85.Pulok, M. H., Sabah, M. N. U. &Enemark, U.(2016),”Socioeconomic Inequalities ofChild Malnutrition in Bangladesh”, Inter-
national Journal of Social Econom-ics, 43(12): 1439-59.
Prakash, M. & Jain, K. (2016),”Inequalitiesamong Malnourished Children in India: ADecomposition Analysis from 1992-2006", International Journal of Social Eco-nomics, 43(6): 643-59.
Radhakrishna, R. & Ravi, C. (2004),”Malnutri-tion in India: Trends and Determinants”,Economic and Political Weekly: 671-76.
Radhakrishna, R., Rao, K. H., Ravi, C. & Reddy,B. S. (2004),”Chronic Poverty and Malnu-trition in 1990s”, Economic and PoliticalWeekly, 3121-30.
Ramalingaswami, V., Jonsson, U. & Rhode, J.(1996),”Commentary: the Asian Enigma,inThe Progress of Nations: UNICEF, NewYork, NY.Sharma, A. (2017),”Inter-state Analysis of Manu-facturing Performance in India: 2001-02 to2013-14",Indian Journal of Industrial Re-
lations, 52(4): 570-85.
Strauss, J. & Thomas, D. (1998), Health, Nutri-tion, and Economic Development”, Journalof Economic Literature, 36(2): 766-817.
Subramanyam, M. A., Kawachi, I., Berkman, L.F. & Subramanian, S. V. (2010),”Socioeco-nomic Inequalities in Childhood Undernu-trition in India: Analyzing Trends between1992 and 2005", PLoS One, 5(6): e11392.UNICEF (1990), “Strategy for Improved Nutri-tion of Children and Women in DevelopingCountries”, UNICEF Policy Review, NewYork, NY.Van de Poel, E. &Speybroeck, N. (2009),”De-composing Malnutrition Inequalities be-tween Scheduled Castes and ScheduledTribes and the Remaining IndianPopulation”,Ethnicity & Health, 14(3): 271-87.Wagstaff, A., Paci, P. & Van Doorslaer, E.(1991),”On the Measurement of Inequali-ties in Health”, Social Science & Medi-
cine, 33(5); 545-57.Wagstaff, A (2000),”Socioeconomic Inequalitiesin Child Mortality: Comparisons acrossNine Developing Countries”, Bulletin of the
World Health Organization, 78: 19-29.Walton, M. (2009),”The Political Economy ofIndia’s Malnutrition Puzzle”, IDS Bulle-
tin, 40(4): 16-24.World Bank (2013),”Helping India Combat Per-sistently High Rates of Malnutrition”, Re-trieved from http://www.worldbank.org/en/news/feature/2013/05/13/helping-india-combat-persistently-high-rates-of-malnu-tritionYadav, A., Ladusingh, L. &Gayawan, E.(2015),”Does a Geographical Context Ex-plain Regional Variation in Child Malnutri-t ion in India?”, Journal of Public
Health, 23(5): 277-87.