Embed Size (px)
Citation preview
T R E N D S I N C A R E O F T H E E L D E R L Y
M A Y 2 , 2 0 1 8
D R M A R Y J A C K S O N
New Ideas/New Drugs in COPD“Old Doc, New Tricks”
Relationships with commercial interests:
Grants/Research Support: None
Speakers Bureau/Honoraria: None
Consulting Fees: None
Other: None
I do not intend to make therapeutic recommendations for medications that have not received regulatory approval
(e.g. off label use)
Freeport Physicians’ Education Days
Declaration of Conflict of Interest
Old Doc, New TricksDr. Mary Jackson
3
DISCLOSURE OF COMMERCIAL SUPPORT
This educational event has received unrestricted educational grants from the following organizations:
Amgen CanadaAstra Zeneca Canada
Bayer HealthCare PharmaGSK Canada
Janssen CanadaMerck Canada
Novartis Pharmaceuticals CanadaNovo Nordisk Canada
Pfizer Canada
Potential for conflict(s) of interest: AstraZeneca, GSK, Merck and Novartis produce products
referable to this presentation
Old Doc, New Tricks
Dr. Mary Jackson
4
Mitigating Potential Conflict of Interest:
Recommendations for drug therapy will be based on peer
reviewed journal articles and published guidelines
Old Doc, New Tricks
Dr. Mary Jackson
5
Goal: To review new inhalers/medications for COPD, their indications and where they fit into the current treatment pyramid
Objectives:1. Participants will understand when and how to use new
COPD meds2. Participants will understand where new medications fit
into the plan of care for COPD3. Participants will have an enhanced understanding of the
management of COPD
Old Doc, New TricksDr. Mary Jackson
Old “tricksters”….
Setting the stage…..
COPD is a costly, common problem
4th leading cause of death in the world
Gender gap in mortality has disappeared
13% of Canadians 35-79 are afflicted
Highest rate of hospital admissions amongst chronic illnesses in Canada
Setting the stage 2…
Diagnosis is often delayed
Spirometry is key to the diagnosis
Comprehensive management includes; smoking cessation, vaccination, education, action plans, inhaled medications, pulmonary rehabilitation, oxygen, surgery and palliative care
Goals of therapy: reduced dyspnea and reduce exacerbations
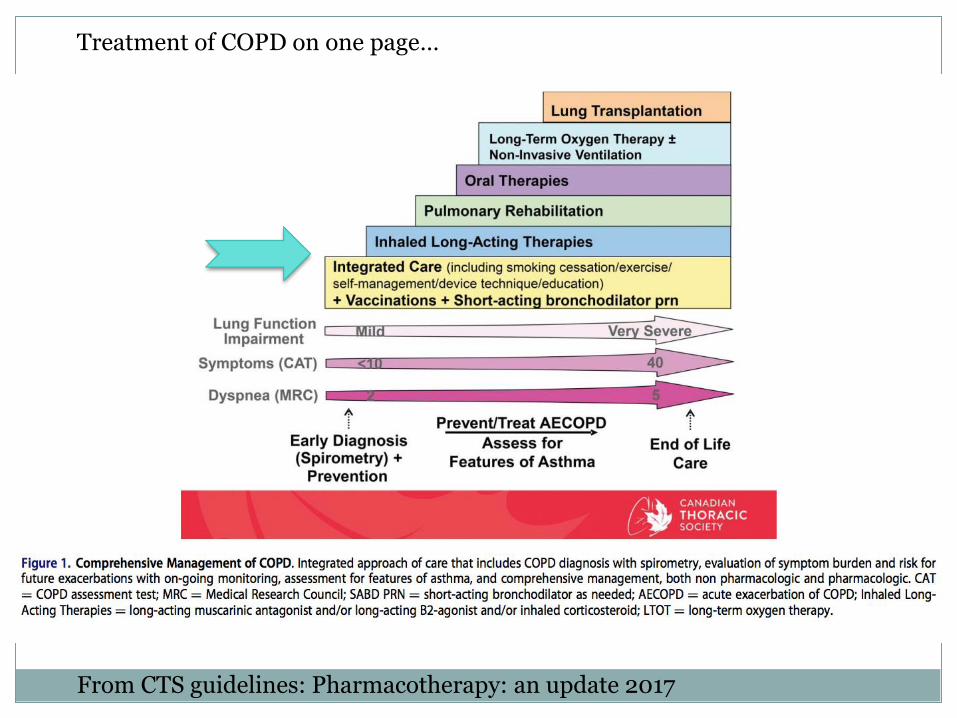
From CTS guidelines: Pharmacotherapy: an update 2017
Treatment of COPD on one page…
smgh.ca
A MEMBER OF THE ST. JOSEPH’S HEALTH SYSTEM
St. Mary’s General Hospital
911 Queen’s Blvd.
Kitchener, ON, Canada
N2M 1B2
Tel: 519.744.3311
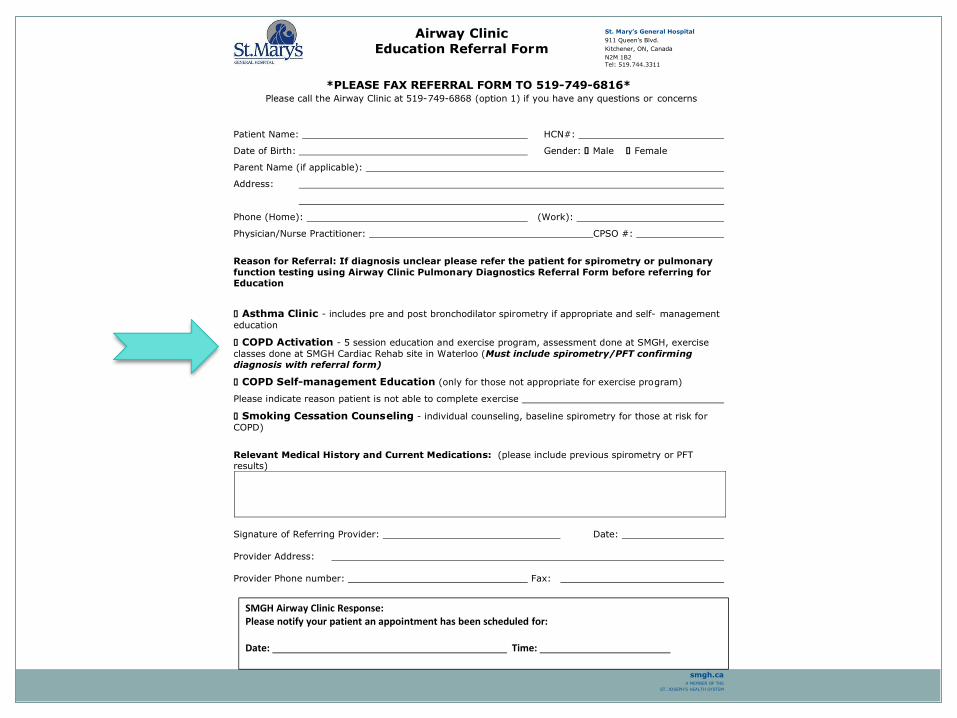
Airway Clinic
Education Referral Form
*PLEASE FAX REFERRAL FORM TO 519-749-6816*
Please call the Airway Clinic at 519-749-6868 (option 1) if you have any questions or concerns
Patient Name: HCN#:
Date of Birth: Gender: □ Male □ Female
Parent Name (if applicable):
Address:
Phone (Home): (Work):
Physician/Nurse Practitioner: CPSO #:
Reason for Referral: If diagnosis unclear please refer the patient for spirometry or pulmonary
function testing using Airway Clinic Pulmonary Diagnostics Referral Form before referring for Education
□ Asthma Clinic - includes pre and post bronchodilator spirometry if appropriate and self- management
education
□ COPD Activation - 5 session education and exercise program, assessment done at SMGH, exercise
classes done at SMGH Cardiac Rehab site in Waterloo (Must include spirometry/PFT confirming
diagnosis with referral form)
□ COPD Self-management Education (only for those not appropriate for exercise program)
Please indicate reason patient is not able to complete exercise
□ Smoking Cessation Counseling - individual counseling, baseline spirometry for those at risk for
COPD)
Relevant Medical History and Current Medications: (please include previous spirometry or PFT
results)
Signature of Referring Provider: Date:
Provider Address:
Provider Phone number: Fax:
SMGH Airway Clinic Response: Please notify your patient an appointment has been scheduled for: Date: Time:
New IdeasNew Drugs for Maintenance Therapy
Different COPD phenotypes
Severity: not just FEV1
Inhaled steroids: helpful and harmful
Magic of macrolides
Cell of the year: The
Eosinophil
Optimizing inhaler therapy in the era of choice: Cost, Compliance and Coordination
A few pearls….
COPD Phenotypes…
Concept of asthma/COPD overlap is not new….but has renewed interest
Important to recognize as the approach to inhaled medications in different in these individuals from COPD alone (?increased role for corticosteroids..)
ACOS = Asthma COPD Overlap Syndrome is the new buzzword
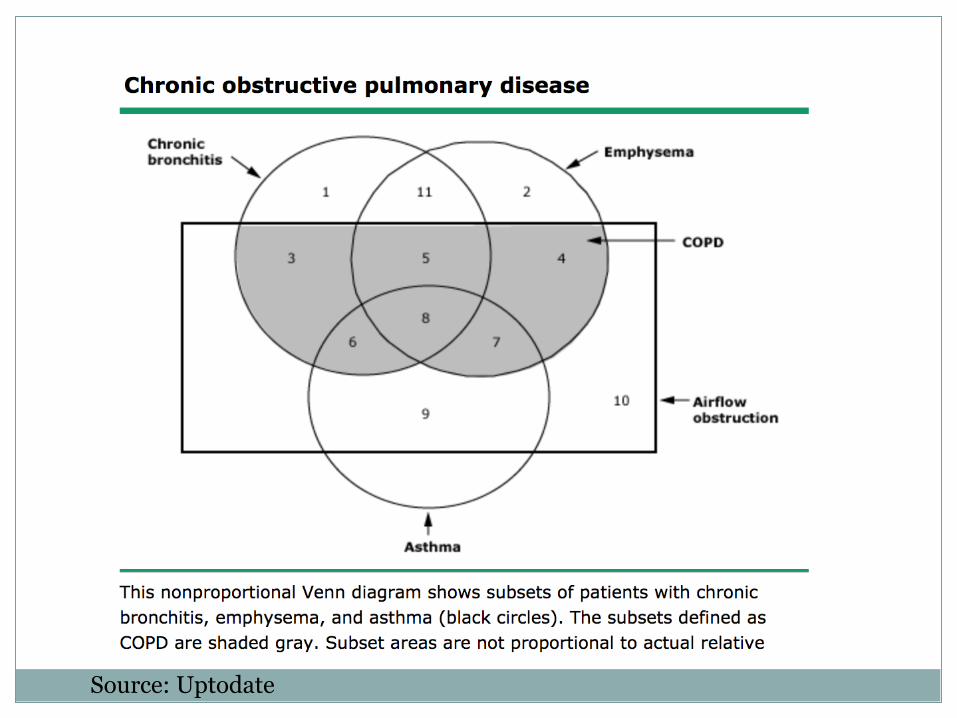
Source: Uptodate
ACOS: CTS definition
Required: 1. Diagnosis of COPD
2. History of asthma
3. Spirometry with persistent post BD fixed airflow obstruction. (FEV1/FVC < 70%)
Supportive: 1. BD improvement of 12% AND >200ml
2. Sputum eosinophilia
3. Blood eosinophilia (>300 ugL)
ACOS- “Old tricks”?
Assessing Severity/Goals of Therapy
How does the clinician choose inhaled therapies? lessen dyspnea, reduce exacerbations, improve exercise tolerance and quality of life?
Assess dyspnea: CAT score/MRC dyspnea score
Assess ability to do activities
Inquire about exacerbation frequency
New guidelines use degree of dyspnea and exacerbation frequency to determine therapy
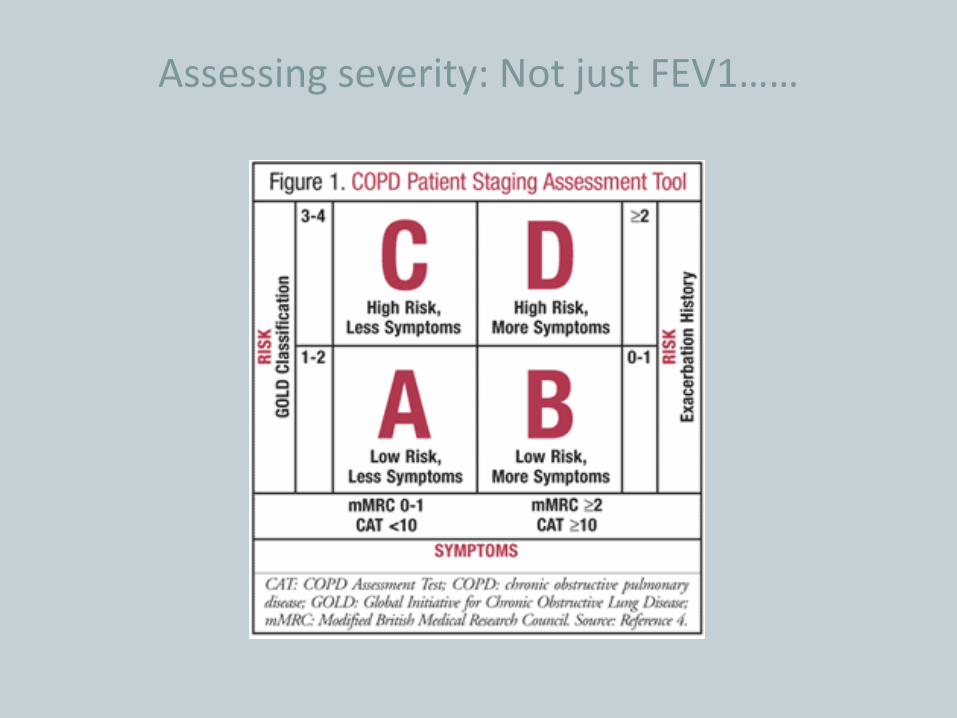
Assessing severity: Not just FEV1……
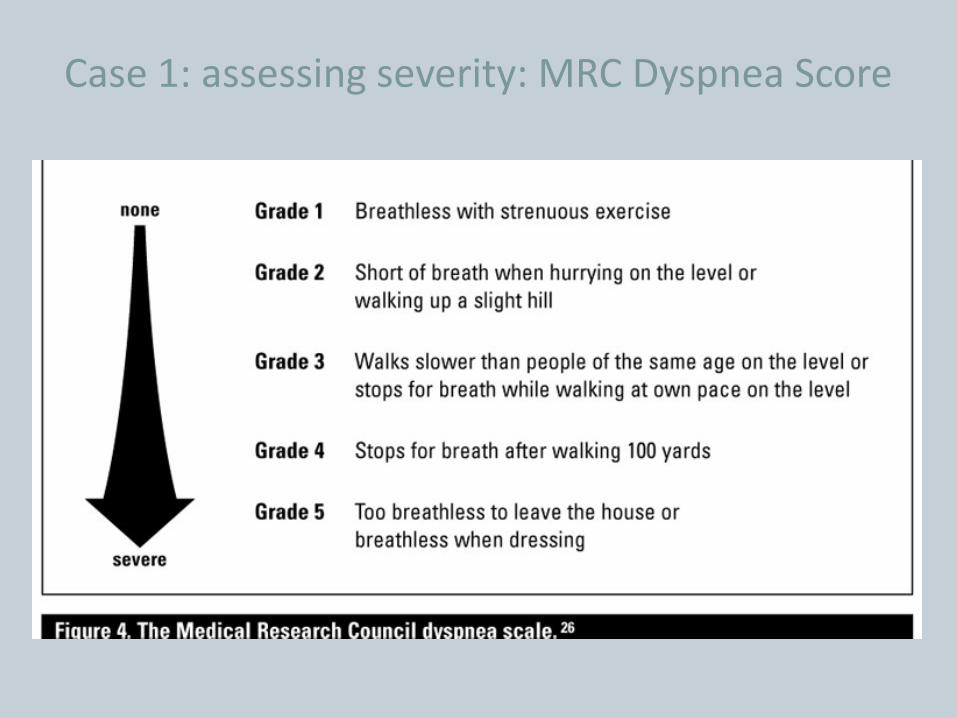
Case 1: assessing severity: MRC Dyspnea Score
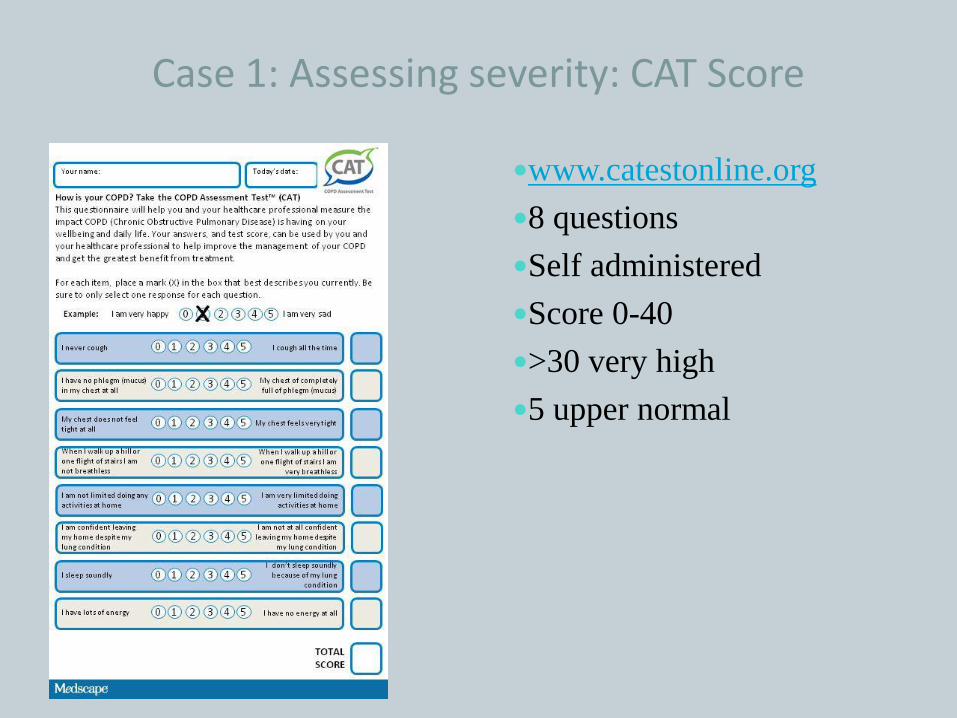
Case 1: Assessing severity: CAT Score
www.catestonline.org
8 questions
Self administered
Score 0-40
>30 very high
5 upper normal
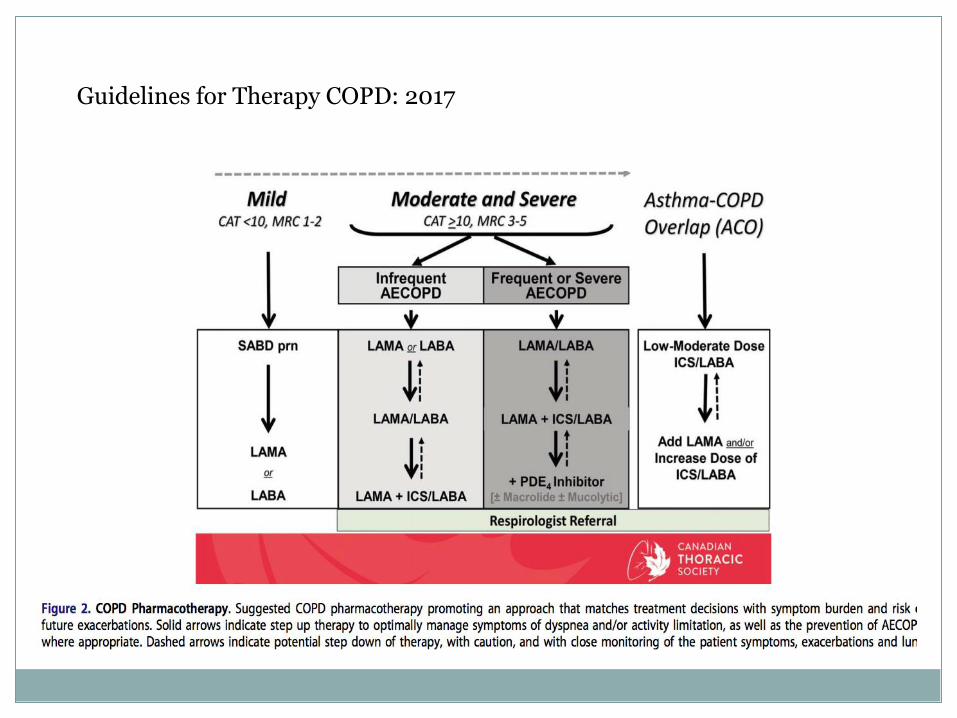
Guidelines for Therapy COPD: 2017
Frequent exacerbators do poorly
FEV1 is inversely proportional to exacerbation risk
A history of exacerbations predicts the future risk
AECOPD= an acute worsening requiring additional therapy
To reduce exacerbations;
add LAMA (better than LABA)
add ICS- low dose, consider subsequent stepdown
add macrolide,(roflumilast)/refer to respirology!
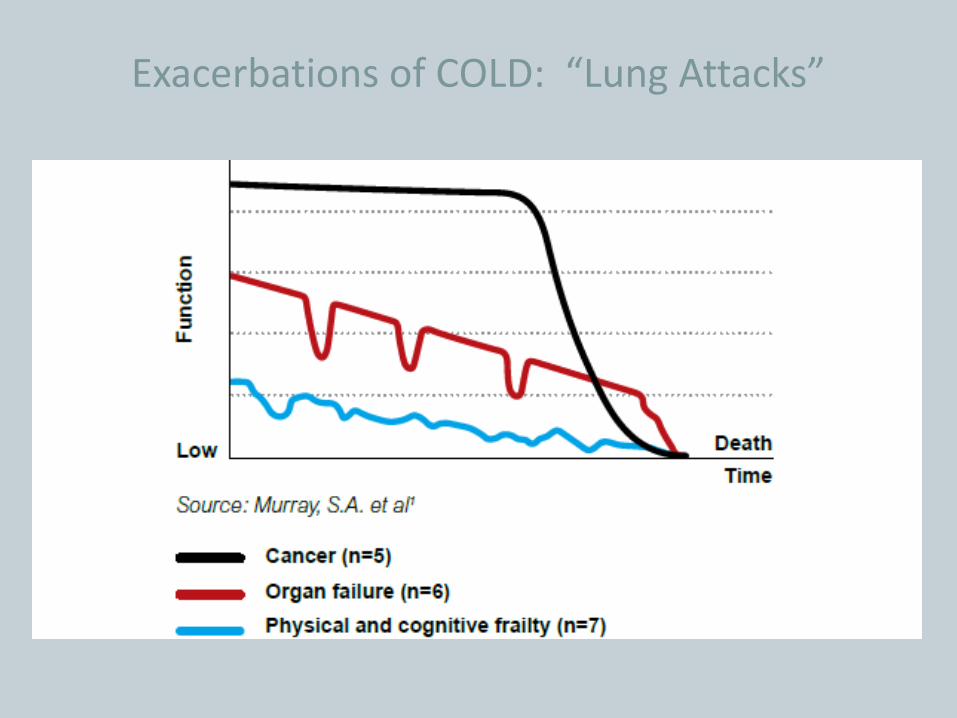
Exacerbations of COLD: “Lung Attacks”
Inhaled Corticosteroids(ICS): Helpful
In ACOS patients
In patients with moderate dyspnea and frequent exacerbations
In patients with severe dyspnea and frequent exacerbations
Local Systemic
Dysphonia
Topical candidiasis
HPA axis fxn can be affected, but effect infrequent(>1000mgm FC-7% abn ACTH stimLung infection. Slight incrrisk of pneumoniaOcular- conflicting data about effect on IOP?Osteoporosis-slight incr # risk in PM women on for long periods (>9 yrs)Bruising
Corticosteroids: Harmful
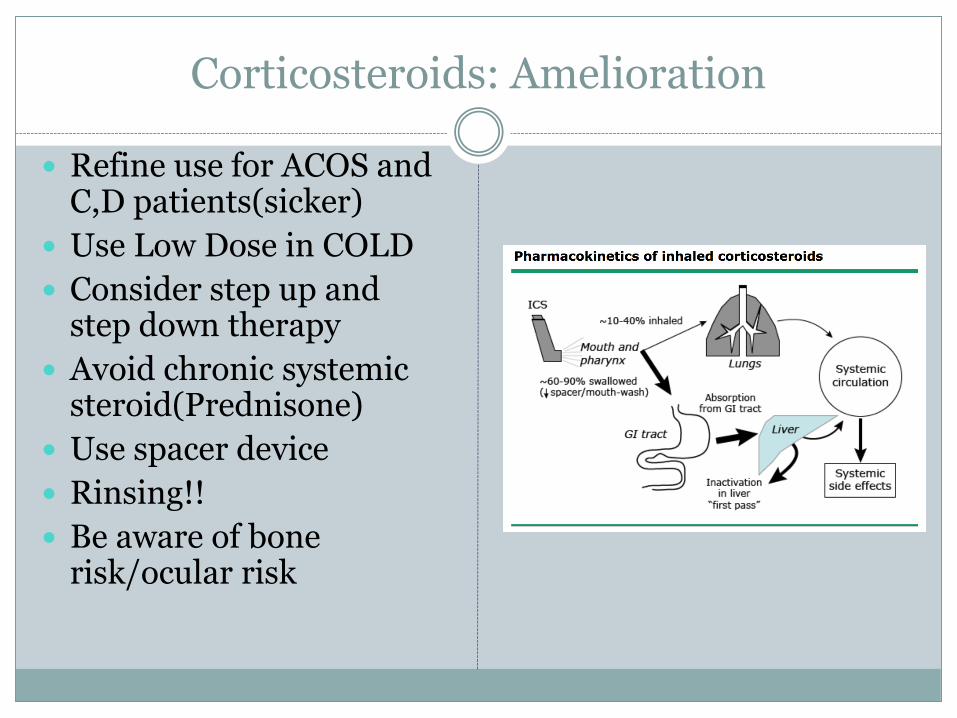
Corticosteroids: Amelioration
Refine use for ACOS and C,D patients(sicker)
Use Low Dose in COLD
Consider step up and step down therapy
Avoid chronic systemic steroid(Prednisone)
Use spacer device
Rinsing!!
Be aware of bone risk/ocular risk
Magic of Macrolides
Renewed interest in chronic antibiotic use in severe, refractory COPD
Azithromycin thought to have anti-inflammatory properties
Shown to delay time to first exacerbation, reduce frequency of exacerbations
Macrolides: practicalities
Consider when puffers aren’t enough and patient has frequent exacerbations
250 mg Monday, Wednesday, Friday
Avoid in those with long QT
If having acute bacterial bronchitis, stop macrolide and use another drug
Try drug holiday > 1 year
New Cell of the Year: The Eosinophil?
Respirologists have their own biologics…
Agents targeting IgE and interleukins (omalizumab, mepolizumab, reslizumab) now being used in difficult to control asthma
Subset of COPD patients with peripheral eosinophilia…
Suggestion that high eospredict those who respond to GCS
Recent studies looking at these drugs in “eosinophilicCOPD”….stay tuned….
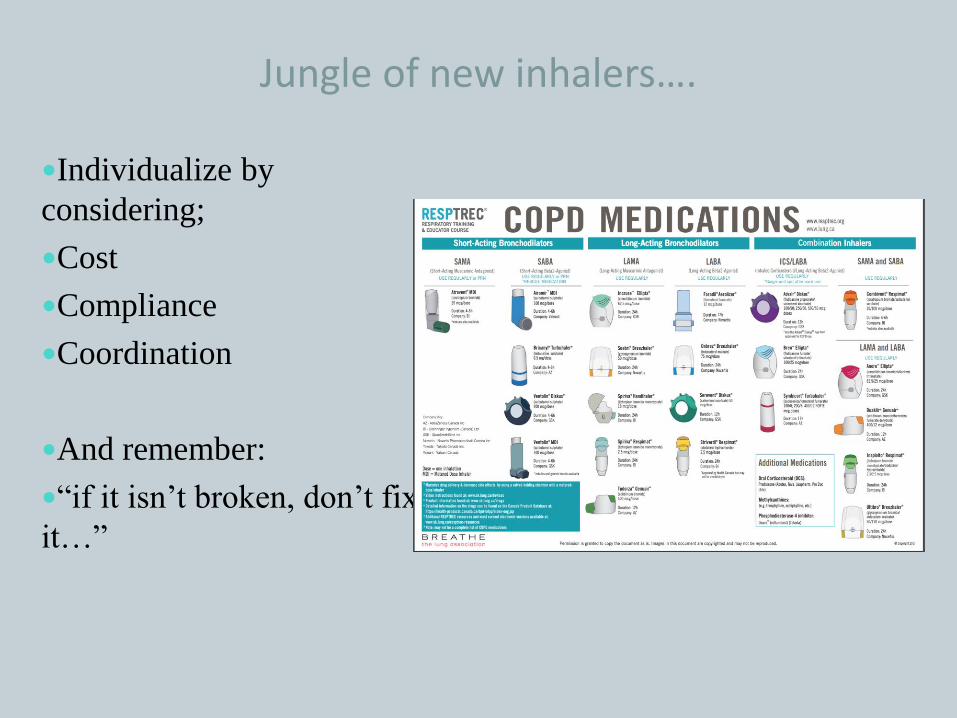
Jungle of new inhalers….
Individualize by
considering;
Cost
Compliance
Coordination
And remember:
“if it isn’t broken, don’t fix
it…”
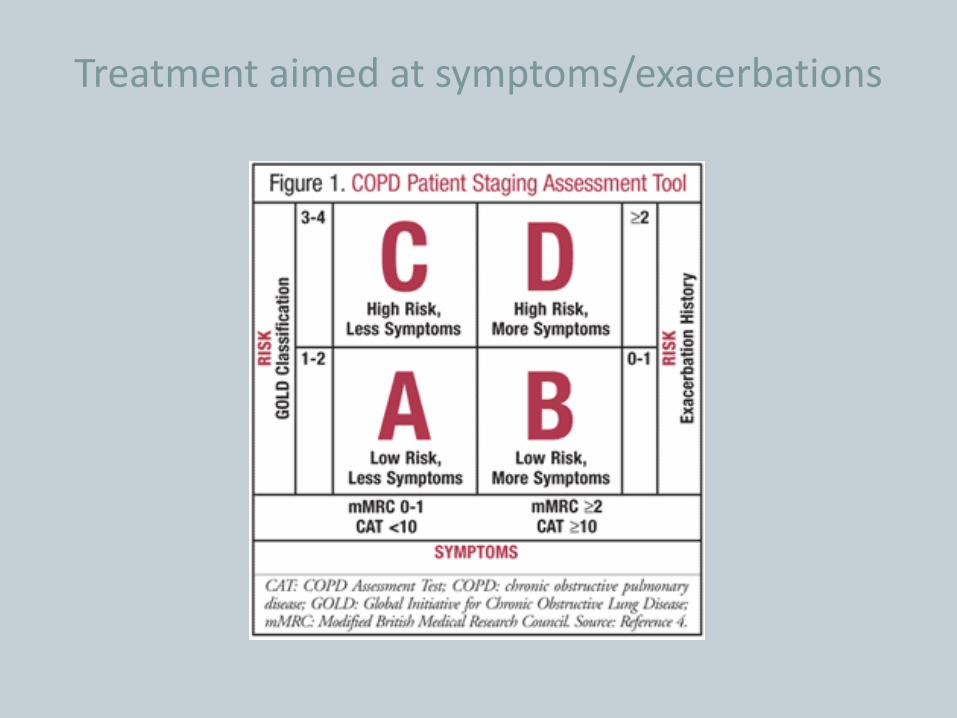
Treatment aimed at symptoms/exacerbations
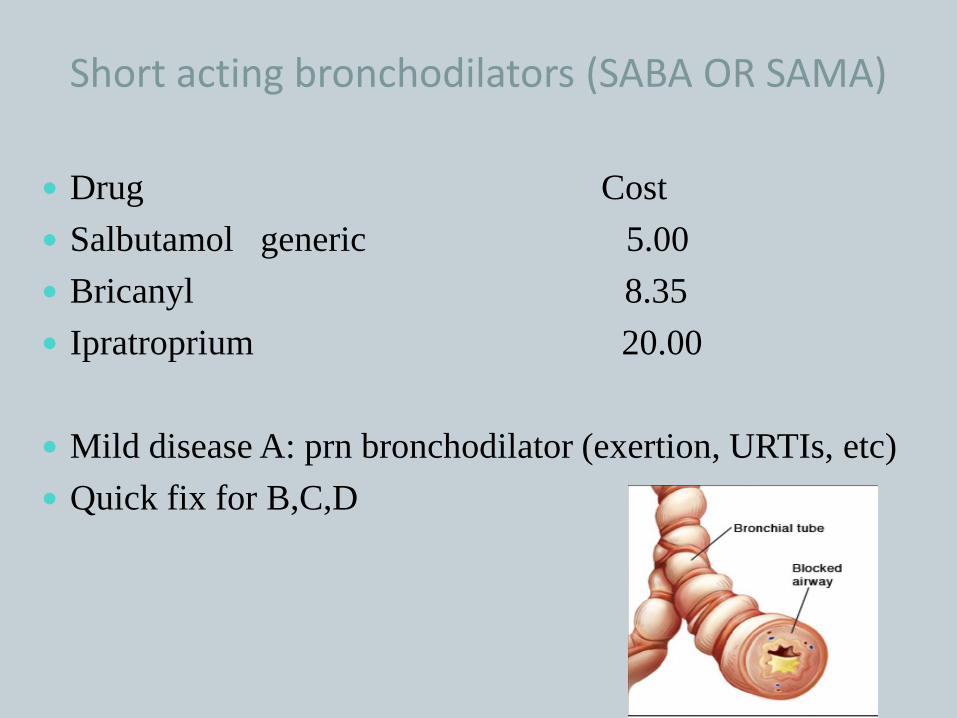
Short acting bronchodilators (SABA OR SAMA)
Drug Cost
Salbutamol generic 5.00
Bricanyl 8.35
Ipratroprium 20.00
Mild disease A: prn bronchodilator (exertion, URTIs, etc)
Quick fix for B,C,D
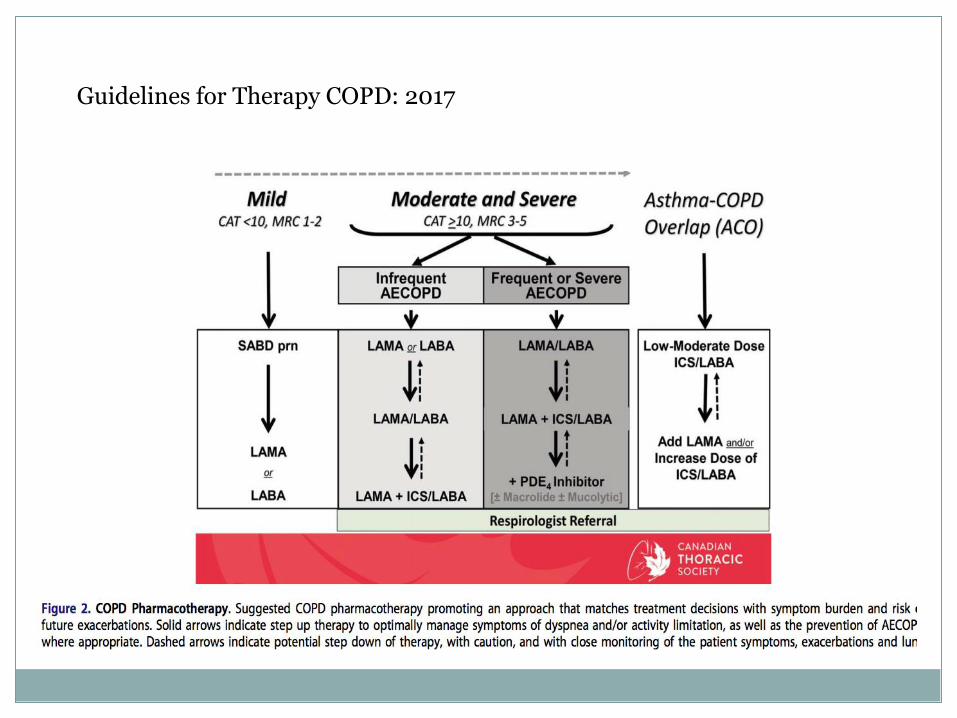
Guidelines for Therapy COPD: 2017
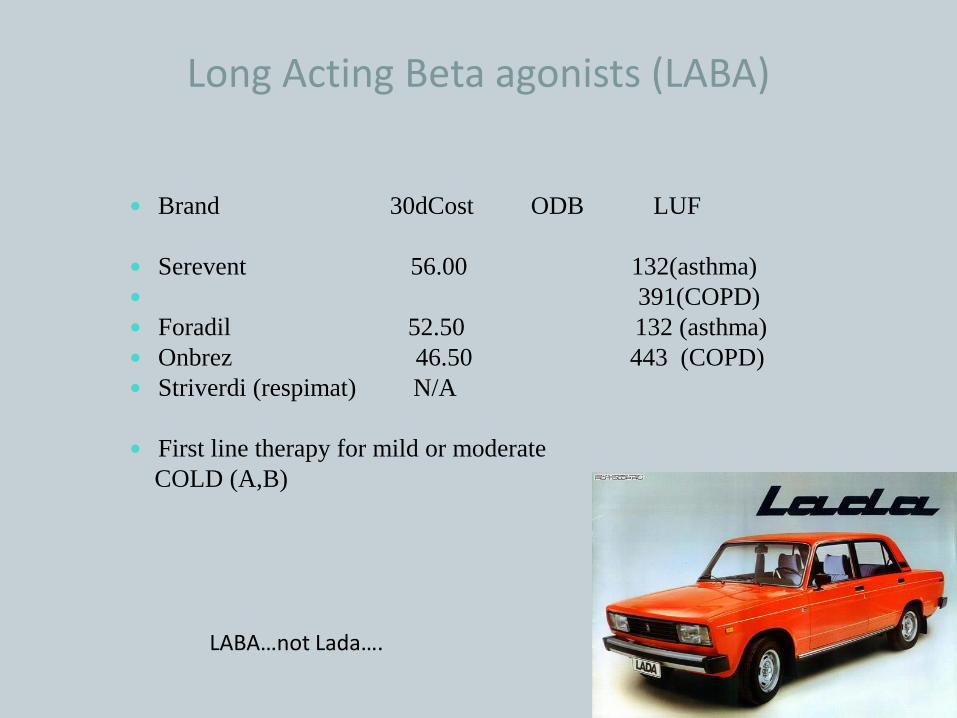
Long Acting Beta agonists (LABA)
Brand 30dCost ODB LUF
Serevent 56.00 132(asthma)
391(COPD)
Foradil 52.50 132 (asthma)
Onbrez 46.50 443 (COPD)
Striverdi (respimat) N/A
First line therapy for mild or moderate
COLD (A,B)
LABA…not Lada….
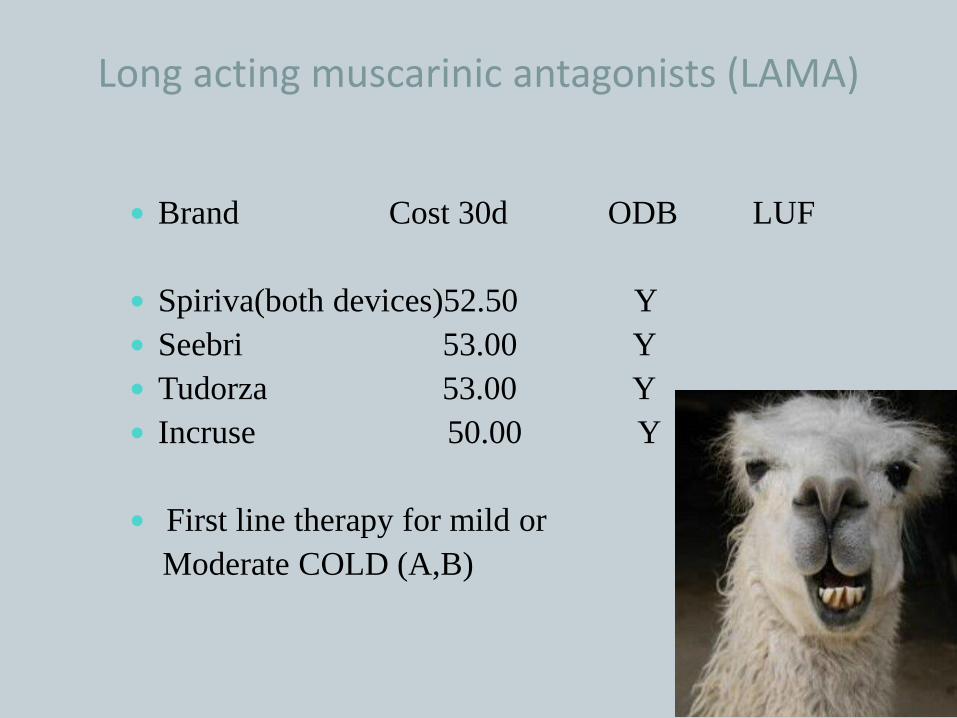
Long acting muscarinic antagonists (LAMA)
Brand Cost 30d ODB LUF
Spiriva(both devices)52.50 Y
Seebri 53.00 Y
Tudorza 53.00 Y
Incruse 50.00 Y
First line therapy for mild or
Moderate COLD (A,B)
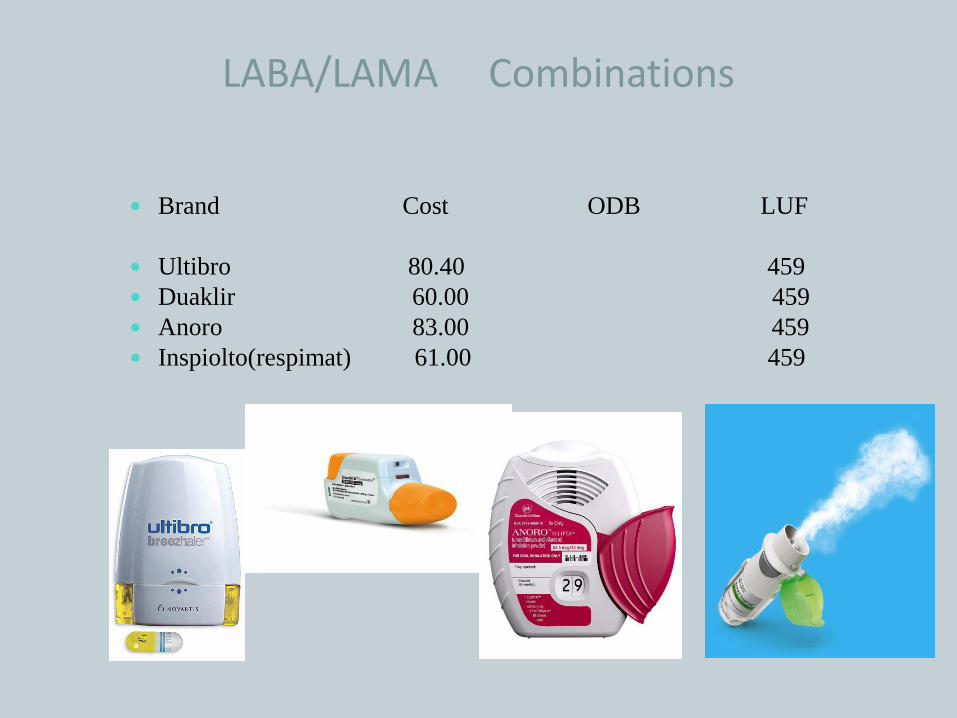
LABA/LAMA Combinations
Brand Cost ODB LUF
Ultibro 80.40 459
Duaklir 60.00 459
Anoro 83.00 459
Inspiolto(respimat) 61.00 459
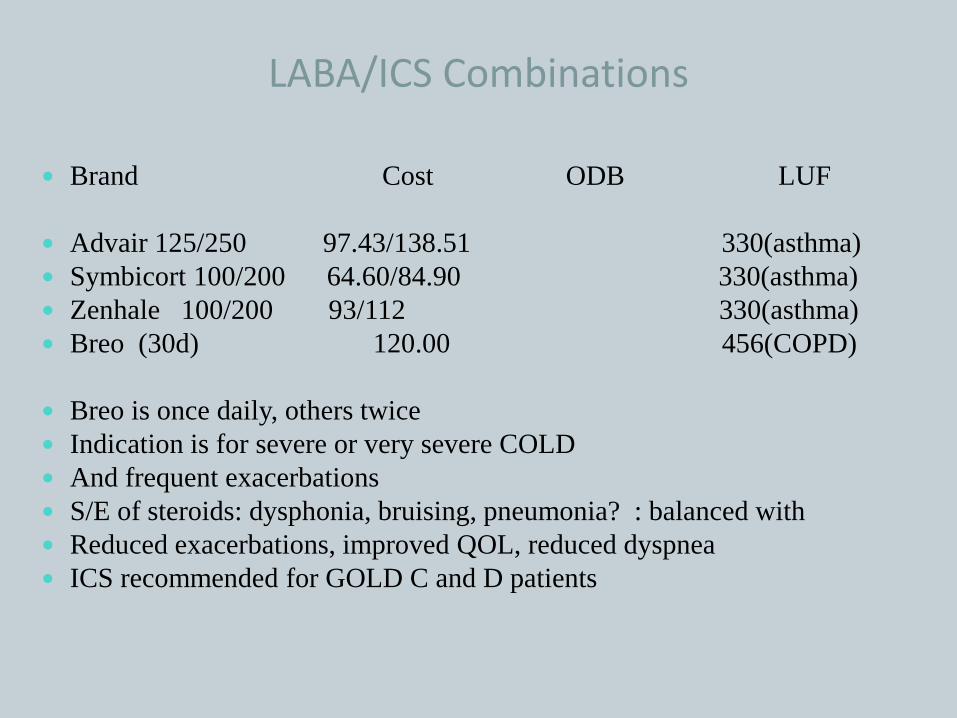
LABA/ICS Combinations
Brand Cost ODB LUF
Advair 125/250 97.43/138.51 330(asthma)
Symbicort 100/200 64.60/84.90 330(asthma)
Zenhale 100/200 93/112 330(asthma)
Breo (30d) 120.00 456(COPD)
Breo is once daily, others twice
Indication is for severe or very severe COLD
And frequent exacerbations
S/E of steroids: dysphonia, bruising, pneumonia? : balanced with
Reduced exacerbations, improved QOL, reduced dyspnea
ICS recommended for GOLD C and D patients
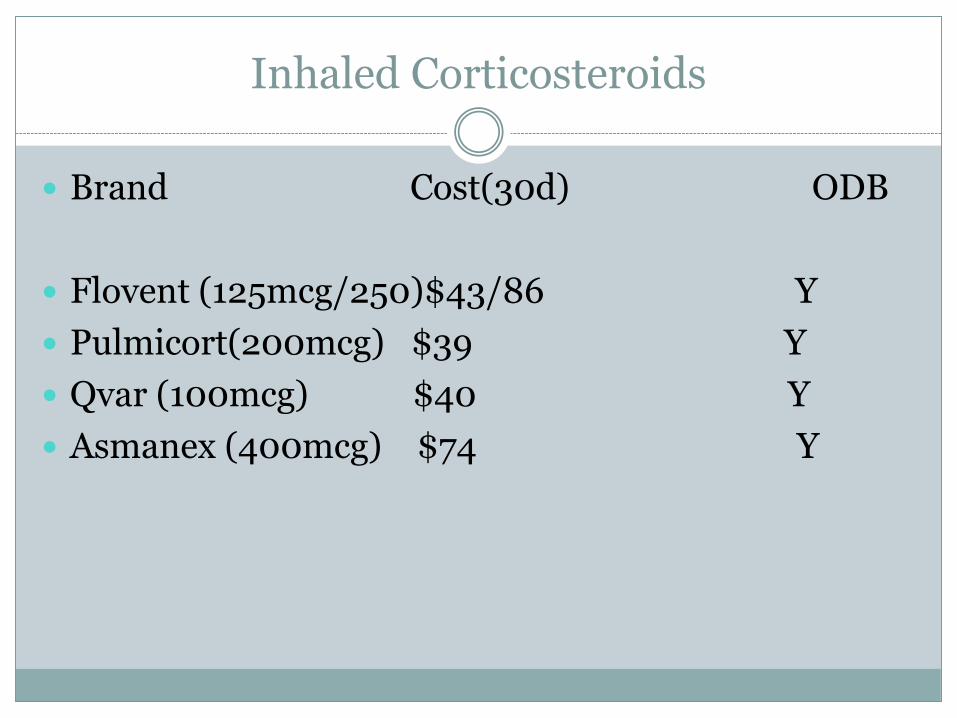
Inhaled Corticosteroids
Brand Cost(30d) ODB
Flovent (125mcg/250)$43/86 Y
Pulmicort(200mcg) $39 Y
Qvar (100mcg) $40 Y
Asmanex (400mcg) $74 Y

Triple combo….coming soon..
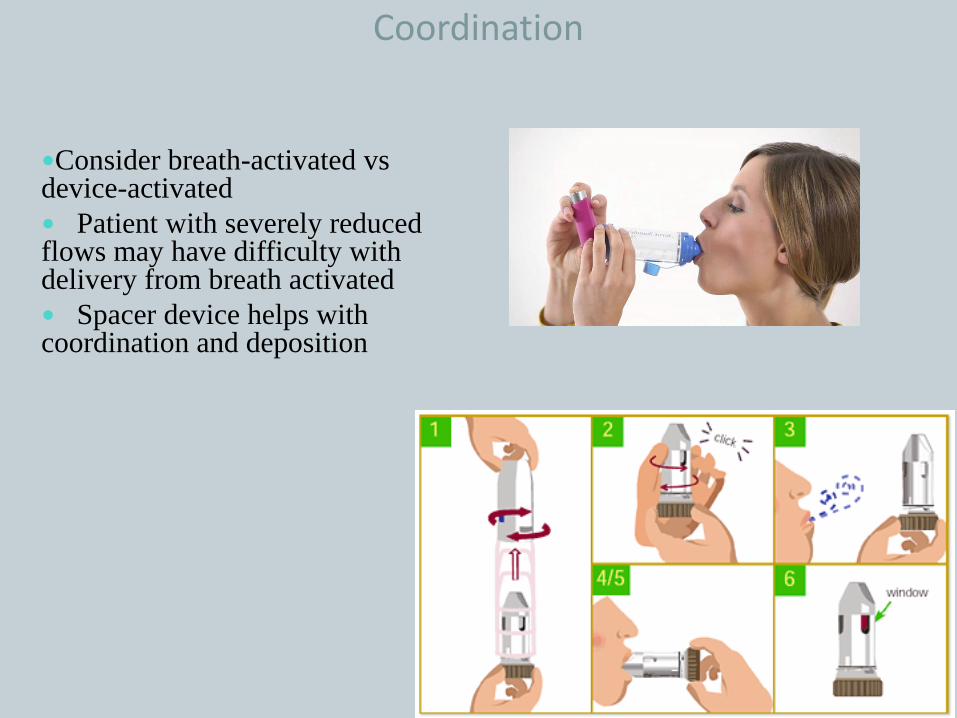
Coordination
Consider breath-activated vsdevice-activated
Patient with severely reduced flows may have difficulty with delivery from breath activated
Spacer device helps with coordination and deposition
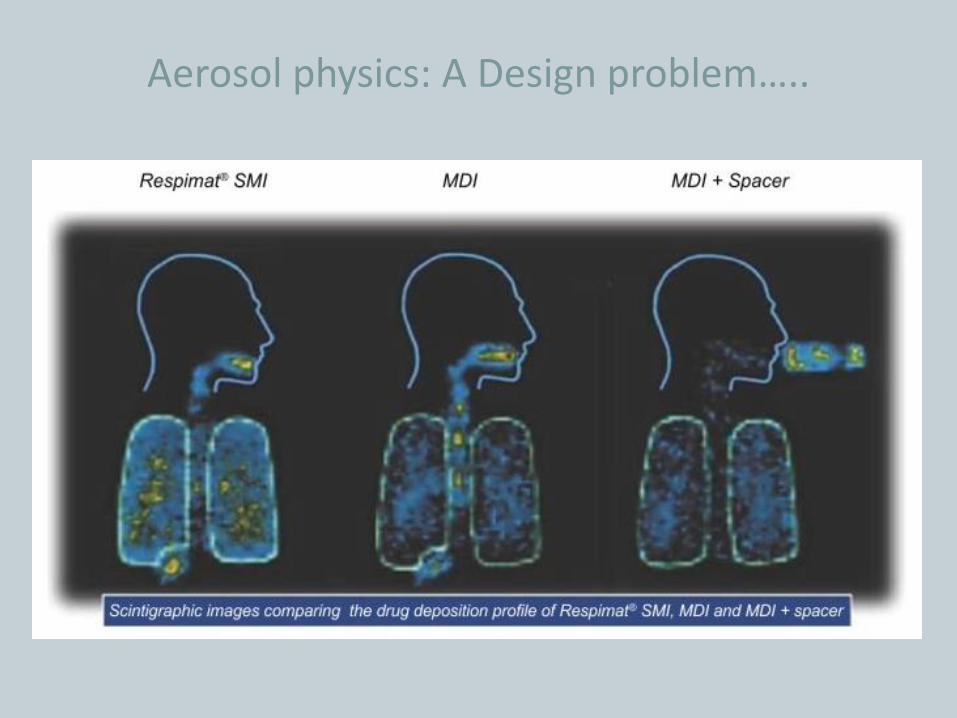
Aerosol physics: A Design problem…..
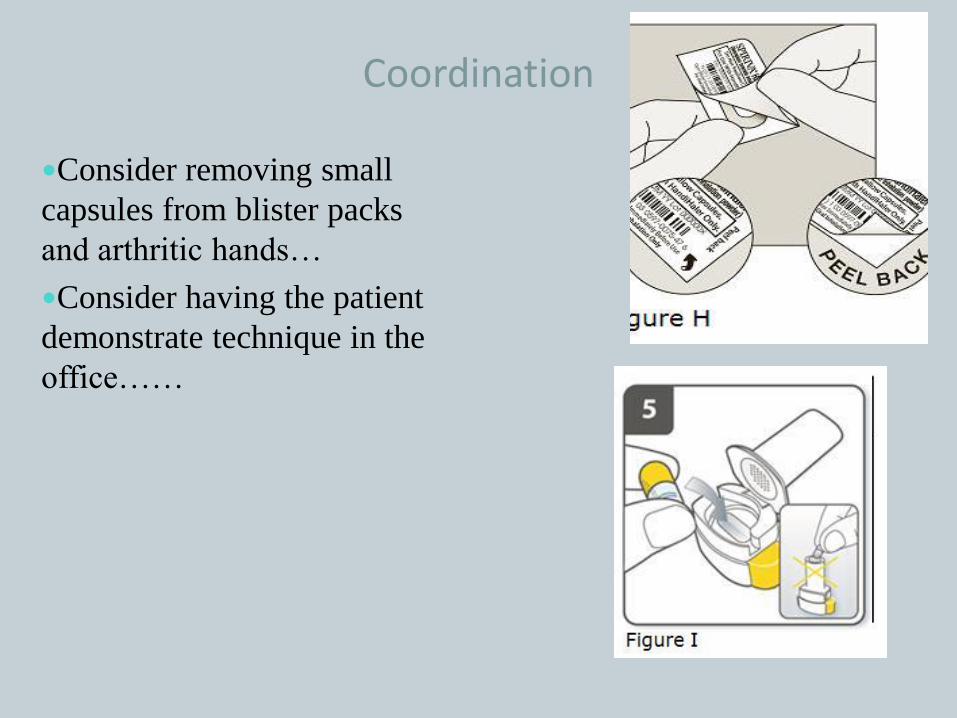
Coordination
Consider removing small
capsules from blister packs
and arthritic hands…
Consider having the patient
demonstrate technique in the
office……
Approach to Rx
Diagnose: COPD or ACOS (spirometry pre and post BD)
SABA in ALL
Choose which longactingdrugs you need
Consider cost, coordination and compliance in choosing drug/device
Final words….
Assess the severity of disease (dyspnea, exacerbations…)
Consider asthma overlap as an additional therapeutic issue
Smoking cessation will have more impact on survival than any inhalers…
Inhalers are designed to reduce SYMPTOMS- and reduce FLARES
Keep it simple – don’t make the treatment worse than the problem
Drug plan?
Coordination and Compliance
Reassessment: Step up and step down…
The End