Embed Size (px)
Citation preview

Trinity Delta
BerGenBio A rosy outlook for Axl
The potential of Axl as an oncology target is now widely accepted and
BerGenBio’s BGB324 is a first-in-class selective oral Axl inhibitor in clinical
development. Data shows that BGB324 can reduce resistance to targeted and
chemotherapies. However, it is now recognised that BGB324’s greatest
prospects could be as an immuno-oncology agent that acts both on tumour and
immune cells. There are currently six Phase II studies ongoing, with three in
immuno-oncology settings, and regular data read-outs are due over the coming
year. We value BerGenBio at NOK1,564m ($184m), or NOK31.34/share.
Year-end: December 2015 2016 2017E 2018E
Sales (NOKm) 0.0 0.0 0.0 0.0
Adj. PBT (NOKm) (72.1) (129.8) (194.1) (238.8)
Net Income (NOKm) (72.1) (129.8) (194.1) (238.8)
Adj. EPS (NOK) (296.3) (419.7) (4.3) (4.8)
Cash (NOKm) 74.0 161.8 348.6 114.3
EBITDA (NOKm) (72.7) (131.4) (194.2) (237.9)
Source: Trinity Delta Note: Adjusted numbers exclude exceptionals.
▪ BerGenBio is leading the Axl field BerGenBio leads the understanding of Axl biology and its lead programme, BGB324 is the most advanced selective oral Axl inhibitor in development. A key role of Axl in cancer is to promote epithelial-mesenchymal transition (EMT), which is linked to metastasis and drug resistance. Recently the broad ranging immune suppressive effects of Axl signalling in cancer have gained prominence. BerGenBio is developing a portfolio of therapies and targeting Axl.
▪ Axl inhibition promises to transform immuno-oncology Through a combination of direct and indirect effects, the inhibition of Axl has the potential to significantly enhance the activity of immuno-oncology therapies. Within a tumour, Axl signalling has been shown to enable tumour cells to both resist immune cell mediated killing and to support an immune-suppressive tumour microenvironment. Axl inhibition not only reverses these effects but also increases the anti-tumour activity of many immune cells, including cytotoxic T-cells.
▪ Six Phase II clinical studies underway To understand better BGB324’s potential, BerGenBio has a broad Phase II programme, with an emphasis on immuno-oncology. Three of the six trials are in combination with Merck’s pembrolizumab (Keytruda) in melanoma, lung and breast cancer. Data from all of the trials is expected throughout 2018.
▪ rNPV model suggests a valuation of NOK31.34/share We prudently value BerGenBio using a rNPV model based only on the indications/settings in which BGB324 is currently being assessed. This gives a value of NOK1,564m ($184m), or NOK31.34/share, with significant upside from positive clinical data. BerGenBio had NOK399m in cash at Q317, which should allow it to operate into H119 and deliver data from the current clinical trials.
Initiation of coverage
4 January 2018
Price (NOK) 21.30
Market Cap (NOKm) 1,063
Enterprise Value (NOKm) 664
Shares in issue 49.9m
12 month range (NOK) 19.00-26.50
Free float 57%
Primary exchange Oslo
Other exchanges N/A
Sector Healthcare
Company Code BGBIO
Corporate client Yes
Company description:
BerGenBio is a clinical-stage, drug
development company based in
Bergen, Norway and Oxford, UK. It is
developing innovative anti-cancer
therapies that act on the promising
Axl signalling pathway. The lead
oncology compound, BGB324, is in a
number of Phase II trials.
Analysts
Mick Cooper PhD
+44 (0) 20 3637 5042
Franc Gregori
+44 (0) 20 3637 5041
Jan
-18
No
v-1
7
Sep
-17
Jul-
17
May
-17
15
20
25
30

2
Trinity Delta
4 January 2018
BerGenBio
Investment case
BerGenBio is a clinical stage biotechnology company that is focussed on
exploiting its knowledge of the Axl signalling pathway as a drug target. It was
founded in 2007 by Prof James Lorens of the University of Bergen, Norway. His
pioneering work in understanding the role and biology of Axl is being explored in
oncology indications, with early clinical results showing encouraging activity. The
lead compound, BGB324, is undergoing "proof of concept" Phase II trials as both
a single agent and in combination therapy. Following an IPO in April 2017,
raising NOK400m ($47m) gross, BerGenBio is listed on the Oslo Exchange. The
company consists of 35 people, with research facilities in Bergen and the clinical
development functions in Oxford, UK.
Valuation
BerGenBio is a classic biotechnology company and is well suited to valuing using
an rNPV model. Using conservative assumptions throughout, we have ascribed a
risk-adjusted value to BGB324 in each indication, summed them and netted
against projected costs. Although BGB324 has clear commercial potential in
many other indications, we have attributed no value to those indications or to
the pre-clinical programmes. These latter assets are expected to progress into
the clinical stages in the near term and represent additional upside.
Despite our prudent approach, we value BerGenBio at NOK1,564m ($184m) or
NOK31.34 per share, which is 47% above the current share price. There are
multiple catalysts to drive further upside over the next 15 months, as data from
the six open-label Phase II trials are expected to report regular data.
Financials
BerGenBio had NOK399m at Q317, sufficient cash to operate into H119, after
raising NOK400m (gross) at NOK25/share during the IPO. Before then, the
company should report final ORR data from four clinical trials (acute myeloid
leukaemia [AML], non-small cell lung cancer [NSCLC] with erlotinib and with
pembrolizumab, and triple-negative breast cancer [TNBC] with pembrolizumab),
and interim data from the two other trials.
Sensitivities
The typical industry risks associated with clinical trials, regulatory hurdles,
financing, possible partnering discussions, and eventually pricing and
commercialisation apply. Currently, the main sensitivity relates to the novelty of
the Axl protein as a therapeutic target. Successful clinical outcomes would
clearly position BerGenBio at the forefront of an exciting, and lucrative, area;
however, inevitably such innovation carries a higher risk profile. The key near-
term inflection points are the results of various oncology trials currently
underway with BGB324. If successful, the next sensitivity would be whether
management opts to license the programme out or look to assume a degree of
self-commercialisation; at this stage, we expect they will seek a partner.
Pioneering novel drug classes
carries additional risk but
provides greater upside potential
Our model employs conservative
assumptions and suggests the
company is worth NOK1,564m
Current cash position suggests a
runway through to H119
The experts in Axl signalling with
a first-in-class selective
compound in the clinic

3
Trinity Delta
4 January 2018
BerGenBio
BerGenBio: A plethora of opportunities
BerGenBio was founded to commercialise the research of Prof James Lorens
(University of Bergen, Norway) to develop drugs that disrupt endothelial-
mesenchymal transition (EMT), and in particular inhibit the Axl receptor. Since
then, knowledge of Axl’s biology has grown (especially in the field of
immunology), and its link with aggressive tumours strengthened.
Axl is a tyrosine kinase receptor, which can activate EMT, cell migration,
proliferation, survival, and immune suppression pathways. The actual effect of
activating the Axl receptor is dependent on the cell type and physiological
context. Axl is broadly associated with advanced malignancy, inflammation and
EMT, which allows tumour cells to adapt and change their characteristics. This
engenders resistance to chemotherapy and targeted therapies, and promotes
metastasis. Of particular importance is that Axl enables tumour cells to escape
immune destruction and modulates the activity of immune cells. This is raising
considerable interest in the field of immuno-oncology.
The potential of Axl as a drug target led BerGenBio to in-license BGB324 from
Rigel Pharmaceuticals in 2011. Clinical development started in 2013 and this
compound is still the only selective oral Axl inhibitor in clinical development. The
Phase I study, in healthy volunteers, confirmed that BGB324 was well tolerated.
BerGenBio is now conducting an extensive Phase I/II trial programme in AML as
monotherapy, NSCLC with erlotinib, TNBC with pembrolizumab, NSCLC with
pembrolizumab. There are also two investigator-led trials underway, in NSCLC
with docetaxel and in metastatic melanoma with targeted and immuno-
oncology therapies. There is already promising initial data from the AML,
NSCLC/erlotinib and NSCLC/docetaxel trials. Final ORR data is expected in H218
from the AML, NSCLC/erlotinib, NSCLC/pembrolizumab and
TNBC/pembrolizumab trials (the company has a cash runway into H119).
BerGenBio is undecided on whether to advance BGB324 into Phase III by itself.
However, if the data from the current Phase II studies confirm the broad
potential of BGB324 to prevent resistance to chemotherapy and targeted
therapies, and enhance the activity of immuno-oncology, we would expect the
company to partner the asset on attractive terms.
At the forefront of understanding
the scope of Axl signalling
BerGenBio’s lead compound, BGB324, is being tested in six Phase II trials in
various cancers and a broad range of settings, including in combination with
immuno-oncology therapy. This programme highlights the considerable
potential of BGB324 as an oncology therapy. The compound is also the first-in-
class selective oral Axl inhibitor in clinical development, just as the
understanding around Axl’s biology confirms it is a highly promising oncology
drug target. Final ORR data from four of the ongoing trials are due to be
reported by the end of 2018, as well as interim data from all of the studies in
H118. Our rNPV model gives a valuation of NOK1,564m (NOK31.34 per share),
which could rise materially with positive results from the trials.
Axl is an integral element in
many cancer pathways
An extensive clinical trial
programme is underway in
multiple difficult tumour types,
with significant data points in
2018
Results from these key proof of
concept studies will determine
the future strategy

4
Trinity Delta
4 January 2018
BerGenBio
Axl inhibition is a novel and promising approach
The Axl receptor was first identified from a screen of genes associated with
chronic myeloid leukaemia in 1988, but it is only recently that its potential as a
drug target is being realised. Activation of Axl signalling has far reaching effects
on the immune system, the tumour microenvironment, and tumour cells
themselves. With the deeper understanding of Axl biology, it is becoming clear
that Axl inhibitors have considerable therapeutic potential in combination with
immuno-oncology therapies, as well as in overcoming resistance to
chemotherapy and targeted treatments.
Part of the reason for the delayed recognition in Axl as a drug target in cancer,
even though it is a tyrosine kinase receptor (RTK), is that it has a limited impact
on proliferation. At the same time, the important role of the immune system in
combatting tumours is now better understood, as is the process of epithelial to
mesenchymal transition (EMT) in enabling tumours develop drug resistance,
evade the immune system and metastasise.
Axl is a member of the TAM family of tyrosine kinase receptors together with
Mer and Tyro-3. The sole ligand for Axl is GAS6, which causes receptor
dimerisation, thereby triggering downstream signal transduction. TAM receptors
are important regulators of the innate immune system and macrophage
phagocytosis. Axl expression is in part distinguished from other TAMs by its close
association with inflammation and prevalence in malignancy.
Exhibit 1: Proportion of cancers expressing high levels of Axl
Source: BerGenBio
Axl has been known for some
time but its importance is only
now being appreciated
A member of the TAM family

5
Trinity Delta
4 January 2018
BerGenBio
Axl is present at low levels in adult tissues and it appears to have limited
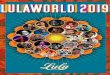
function; indeed, Axl knockout mice are normal. In contrast, it is commonly
expressed at high levels in many cancers and associated with a worse prognosis
for those patients (Exhibits 1 and 2). Interestingly, few activating mutations
(typical of RTKs) have been identified, suggesting that epigenetic regulation of
Axl is important.
Exhibit 2: Prognosis of breast, lung and AML patients with high and low levels of Axl expression
Source: BerGenBio
The biology of Axl is complex, with the protein being able to activate many
different signalling pathways (Exhibit 3), depending on the tissue context in
which the protein is activated, including promoting proliferation via MEK/ERK
and survival via PI3K-AKT signalling. It is however important to highlight two of
the other pathways:
▪ STAT1 signalling in dendritic cells plays an important role in immune
homeostasis and prevents excessive immune reactions;
▪ The pathway that activates Snail and Twist, which leads to EMT.
During an immune response, the STAT1 pathway is activated in macrophages
and dendritic cells by the cytokine IFN-γ binding to the IFN receptor. This is
crucial in stimulating an innate response to an infection, but to prevent an
excessive immune response, there is also a ‘safety switch’ triggered by the
increased expression of Axl. This results in the activation of SOCS3 genes that
down regulate pro-inflammatory cytokines and dampen the immune response.
Consistent with Axl and the other TAM proteins having a key role in immune
regulation, mice which lack all three of the TAM genes develop normally until 4-
6 weeks after birth when their spleens and lymph nodes become enlarged
before they develop inflammation and autoimmune syndromes. This finding
demonstrates that the key role of TAM genes is in modulating activity of the
immune system. Axl serves important roles in dampening the immune response
to infections and disease, while Mer is the main receptor for apoptotic (dead

6
Trinity Delta
4 January 2018
BerGenBio
and dying) cell removal by efferocytosis (a form of phagocytosis1); Tyro3 is a
negative regulator of Type 2 immune responses2
Exhibit 3: Signalling pathways that can be activated by Axl signalling
Source: BerGenBio
Within a solid tumour, Axl regulates the EMT of cells. The transition of tumour
cells from an epithelial to mesenchymal-like cell type supports strong invasive
characteristics. EMT also causes tumour cell secretion of anti-inflammatory
cytokines that suppress anti-tumour immunity. This is characteristic of “cold”
tumours with limited invasion of cytotoxic T cells.
During EMT, the expression of hundreds of genes change enabling the
acquisition of new cellular behaviours. This allows tumour cells to break away,
invade the surrounding tissue and vasculature, and access sites in other organs.
This plasticity further allows distant colonisation and the formation of secondary
tumours (metastasis). These phenotypic changes are closely associated with
reduced sensitivity to chemotherapy or targeted oncology drugs. In fact, one of
the reasons that cancers stop responding to treatment is that therapy-induced
stress triggers EMT. This insight has raised interest in targeting this mechanism.
11 Phagocytosis is the process through which cellular debris from apoptotic cells and microorganisms are ingested by phagocytes, such as macrophages and neutrophils. 2 Type 2 immune responses are generated following infection from helminths (parasitic worms) and exposure to allergens.
Epithelial to mesenchymal
transition (EMT) is a major factor
in aggressive tumours
Axl is linked to tumour resistance
in a number of ways…

7
Trinity Delta
4 January 2018
BerGenBio
Exhibit 4: Axl-driven epithelial-mesenchymal transition of tumour cells
Source: BerGenBio
Associated with the EMT of tumour cells, there are also changes that can enable
tumour cells to escape immune surveillance. Firstly, there is reduced expression
of MHCI proteins (Major Histocompatibility Class I protein) the proteins that
present protein fragments to cytotoxic T-cells. Secondly, the EMT cells express
higher levels of PD-L1, which inhibits the activity of cytotoxic T-cells. In
preclinical studies with radiation sensitive and resistant tumour cell lines, Axl
inhibition was shown to have a greater effect on restoring radiation sensitivity
than the use of checkpoint inhibitors and was found to increase infiltration by
cytotoxic T-cells.
Axl can also promote tumour progression through angiogenesis. The receptor is
needed for VEGF-A-induced migration of endothelial cells and the formation of
new blood vessels in tumours. Axl has also been linked to dormancy of
metastatic prostate cancer cells in the bone marrow, and cancer stem cell
activity in recurrent breast cancer.
Axl inhibitors in development
Interest in Axl as a therapeutic target for cancer and other therapeutic areas (eg
auto-immune diseases) has only recently grown, fuelled by its potential in
immuno-oncology. BerGenBio’s BGB324 is the first-in-class selective small-
molecule Axl inhibitor in clinical development that can address this opportunity.
The company’s leading position is thanks to the prescient in-licensing of the
compound (R428) from the San Francisco-based biotech, Rigel Pharmaceuticals
(discussed below). Exhibit 5 details other compounds in development that
inhibit Axl; the only other compound in clinical development with reasonable
specificity is Daiichi Sankyo’s DS-1205, but it appears that it is being developed
for use in combination with osimertinib (Tagrisso) in mEGFR NSCLC. The other

8
Trinity Delta
4 January 2018
BerGenBio
molecules with some degree of specificity for Axl are Ono Pharmaceutical’s
ONO-7475 (which binds to the other TAM protein, Mer) and Betta
Pharmaceuticals’ BPI-9016M, all of which are in Phase I development.
Exhibit 5: Oral Axl inhibitors in development
Compound (Company) Binding specificity Axl inhibition IC50 (nM)
Development stage
Indications
Cabozantinib
(Exelixis)
VEGF, Met, FLT3, c-KIT, Axl
7 Approved Approved in medullary thyroid cancer and renal cell carcinoma,
Ph II & III in other solid tumours
Gilteritinib/ASP2215 (Astellas)
FLT3, LTK, Axl, TRKA, RET ROS Mer,
0.7 Phase III AML (Phase III for FLT-mutation positive AML; Phase I for 1st line AML)
BGB324/R324 (BerGenBio/Rigel Pharmaceuticals)
Axl 14 Phase II AML, NSCLC, TNBC, malignant melanoma
MGCD265
(Mirati Therapeutics)
Axl, Met, RON, TIE, VEGFR2
<10 Phase II NSCLC and other solid tumours
Merestinib/LY2801653
(Eli Lilly)
Met, MSTR1, DDR1, TIE1, Mer Tyro3, Axl
11 Phase II AML, NHL and solid tumours
ONO-7475
(Ono Pharmaceuticals)
Axl, Mer N/A Phase I Acute leukaemia
BPI-9016M
(Betta Pharmaceuticals)
Axl, Met N/A Phase I Solid tumours
ASLAN002/BMS-777607 (Aslan Pharmaceuticals/BMS)
Axl, Ron, Met, Tyro3, Mer, FLT3
1.1 Phase I Solid tumours
S49076
(Servier)
Met, Axl, Mer, FGFRs
7 Phase I Solid tumours
TP-0903
(Tolero Pharmaceuticals)
Aurora A&B, JAK2, ALK, ABL, Axl, Mer
27 Phase I Solid tumours
DS-1205
(Daiichi Sankyo)
Axl 1.3 Phase I NSCLC (in combination with osimertinib)
LDC1267/Q107 (LDC/Qurient Therapeutics)
Met, Axl, Tyro3 19 Preclinical Immuno-oncology
Source: Trinity Delta
The specificity of BGB324 is important, as it means that it should be easier to
combine this compound with other drugs, compared to those with more
promiscuous inhibition profiles. The biology of Axl also indicates that
combination of the compound with other agents could result in successful
therapies for many tumours. Initial data on BGB324 supports the view that it can
be used in combination with various drug classes; BerGenBio has shown that
BGB324 can be combined with erlotinib (see below). In contrast, a trial with
Astellas’s gilteritinib with erlotinib in NSCLC had to be terminated after the
treatment of only 10 patients because of adverse events.
The Axl receptor is also being targeted using monoclonal antibodies and
antibody-drug-conjugates (ADC). Indeed, BerGenBio has two such preclinical
assets in its portfolio with BGB149, an antibody, and BGB601, an ADC. Other
companies have reported preclinical antibodies (eg Genentech’s YW327.6S2),
A promising profile allows use in
combination with other agents
BerGenBio has other Axl assets in
pre-clinical development

9
Trinity Delta
4 January 2018
BerGenBio
while the most advanced antibody-based product in clinical development is
Genmab’s ADC, Humax-AXL-ADC.
It is unclear at this stage which Axl targeting approach is the most effective, and
it is possible that this will depend on the indication. However, the favourable
manufacturing and convenience of an oral small molecule inhibitor for patients
are important strengths of BGB324.
Clinical development of BGB324
Exhibit 6 provides details of BerGenBio’s entire pipeline. As well as BGB324, the
company has two monoclonal antibodies against Axl in development; BGB149,
due to enter the clinic in H218, and BGB601, which is an ADC partnered with
ADC Therapeutics. These are also being developed in cancer indications, but no
details have been disclosed; they might have potential in other therapeutic
areas given the activity of Axl in other diseases.
The rest of this report is focused on BGB324 as it is currently BerGenBio’s only
clinical asset.
Exhibit 6: BerGenBio’s portfolio of products
Source: BerGenBio
The clinical development of BGB324 began with a Phase I study in healthy
volunteers in 2013/14, unusually for an oncology compound. This was possible
because of the clean safety profile shown during preclinical development. The
data from the Phase I study confirmed this favourable safety profile, with it
being safe and well-tolerated up to a dose of 1.5g per day and only grade 1
reversible adverse events were observed up to 1.0g per day.
BGB324 is the star of BerGenBio’s
development pipeline
Phase I study showed a very
clean safety profile

10
Trinity Delta
4 January 2018
BerGenBio
Exhibit 7: Clinical development programme for BGB324
Clinical trial name /
NCT number
Phase (trial status)
Indication (setting/number enrolled)
Next data
(Expected completion date)
Notes
BGBC001
(N/A)
Phase I
(completed)
Healthy volunteers
(-/n=32)
(Q114) Single ascending dose study. Results: Only Grade 1 AEs observed up to 1g per day, and well tolerated up to 1.5g per day. Predictable PK data with long plasma half-life of almost 4 days.
BGBC003
(NCT02488408)
Phase Ib/II
(recruiting)
Relapsed or refractory AML, High risk MDS (monotherapy or with cytarabine or decitabine/ n=75)
Jun 2018 (H218)
Open-label, Stage 1:dose escalation study to identify MTD as monotherapy (completed). BGB324 was well-tolerated, loading dose of 600mg on days 1 & 2, followed by 200mg daily dose selected for next stage. Stage 2: At recommended dose, tolerability study as monotherapy and in combination with cytarabine and decitabine.
BGBC004
(NCT02424617)
Phase Ib/II
(recruiting)
NSCLC
(monotherapy in heavily pre-treated patients and in combination with erlotinib in patients with an activating EGFR mutation / n=66)
Jun 2018 (H218)
Open-label, Stage 1:dose escalation study to identify MTD as monotherapy and in combination with erlotinib (completed). BGB324 was well-tolerated; selected a loading dose of 600mg on days 1 & 2, followed by 200mg daily dose for next stage. As monotherapy, ~1 year PFS in 2 of 8 patients; and with erlotinib, 4 of 8 patients had clinical benefit. Stage 2: At recommended dose of BGB324 and in combination with erlotinib, ORR, PFS, circulating Axl levels and safety will be assessed in c 40 patients.
BGBC007
(NCT03184558)
Phase II
(recruiting)
TNBC
(in combination with pembrolizumab / n=56)
Jun 2018
(H218)
Open-label study, in collaboration with Merck. Endpoints are ORR, DoR, PFS, OS, 12 month survival, response by biomarker expression (PD-L1) and safety.
BGBC008
(NCT03184571)
Phase II
(recruiting)
NSCLC
(previously treated adenocarcinoma of the lung in combination with pembrolizumab / n=48)
Jun 2018
(H218)
Open-label study, in collaboration with Merck. Endpoints are ORR, DoR, PFS, OS, 12 month survival, response by biomarker expression (PD-L1) and safety.
BGBIL005
(NCT02922777)
Phase Ib
(recruiting)
NSCLC
(previously treated, in combination with docetaxel / n=30)
June 2018
(H119)
Investigator-led, open-label study led by University of Texas Southwestern Medical Center. Dose escalation study (3+3 model) with docetaxel at 75mg/m2. Endpoints include identifying MTD for BGB324 in combination with docetaxel, and PD/PK assessments.
BGBIL006
(NCT02872259)
Phase Ib
(recruiting)
Metastatic melanoma
(previously treated stage IIIc/IV, with pembrolizumab or dabrafenib & trametinib / n=92)
H218
(H220)
Investigator-led, open-label study led by Haukeland University Hospital. Four-arm study with BGB324 in combination with pembrolizumab or dabrafenib & trametinib compared to pembrolizumab or dabrafenib & trametinib alone. Endpoints are ORR, PFS, DoR, OS and safety
Source: Trinity Delta
Since then BerGenBio has embarked on a broad clinical trial programme in a
range of cancer indications and different drug combinations (Exhibit 7). The
focus of the studies is moving towards exploring BGB324’s potential as an
immuno-oncology agent, as the ability of Axl inhibition to enhance anti-tumour
T-cell activity is better understood. While it is unusual for a small biotech
A wide-ranging clinical
programme is now underway…

11
Trinity Delta
4 January 2018
BerGenBio
company to embark on such wide-ranging clinical trials, it is rational and means
that it will be in the best position to maximise the value of the compound. The
company has also selected indications in which a high expression of Axl is
associated with a poor prognosis (Exhibit 3).
The approach, firstly, helps to mitigate the risks associated with developing a
compound against a novel target with such complex biology, which is only
starting to be better understood. Secondly, the data from the trials in different
settings (monotherapy, with an immuno-oncology drug, to alleviate drug
resistance) will help to indicate where BGB324 has most potential.
BerGenBio is also looking to reduce the risk profile of BGB324 development, by
including biomarker analysis in its clinical development plan. The aim is to
develop a companion diagnostic to identify patients most likely to benefit from
BGB324 treatment. Among the potential biomarkers being analysed are: tumour
Axl expression, soluble Axl in the blood, and known immune and EMT
biomarkers (protein and genomic).
We estimate that BGB324 could advance into Phase III in 2019, assuming
promising levels of efficacy are observed during the current studies. The pivotal
studies could in turn lead to a NDA in the US and MAA in Europe being filed in
2021/22 and BGB324 being approved in 2022/23.
Monotherapy in AML and MDS
BerGenBio’s first Phase II study is in relapsed/refractory acute myeloid
leukaemia (AML) and high-risk MDS patients (c 30% of MDS patients will end up
developing AML), indications that mainly affect people over the age of 45
(average age for AML: 67). Until recently there has been limited innovation in
therapy, which has essentially only seen modest variations on the 7+3
chemotherapy regimen of cytarabine and daunorubicin. The treatment
landscape is starting to evolve with the approval of Novartis’ midostaurin
(Rydapt), Agios/Celgene’s enasidenib (Idhifa) and Pfizer’s gemtuzumab
ozogamicin (Mylotarg) in 2017, but there is still much demand for a treatment
suitable to treat elderly patients with AML or MDS in these highly
heterogeneous indications.
High Axl expression is associated with a poor prognosis for AML patients and Axl
signalling drives proliferation, survival and chemo-resistance of AML cells,
making Axl an attractive target in AML and closely-related MDS. The potential of
BGB324 to treat AML and MDS was subsequently confirmed in preclinical
studies, in which BGB324 was shown to inhibit the Akt and MAPK pathways,
have a similar or greater affect than cytarabine, and have an additive anti-
tumour effect with cytarabine in two different AML cell lines.
BGB324 is now in a Phase Ib/II study in AML, started in 2014. The first part of the
study was the dose escalation stage with the following three dosing regimens: a
loading dose of 400mg for two days followed by a daily dose of 100mg; 600mg
A novel target with such complex
biology requires a comprehensive
clinical trial evaluation…
Axl biomarkers are also being
developed
Smooth progress could mean
pivotal trials by 2019 and
regulatory filings in 2021/22
AML and MDS are the first
indications being explored
Axl is associated with a poor
prognosis in AML and is an
important driver of the disease
Phase Ib element of the trial
showed encouraging side-effect
profile…
…that will inform future direction
of the development plans

12
Trinity Delta
4 January 2018
BerGenBio
then 200mg; and 900mg followed by 300mg. The most common side effects
were reversible mild and moderate gastrointestinal disorders (there was in the
lowest dosing cohort one dose-limiting toxicity [DLT], QTc prolongation, but this
was associated with a pre-existing condition). Based on these findings, combined
with the PK/PD data, the 600/200mg dosing regimen was taken forward into the
second stage of the trial.
There were also promising signals of anti-tumour activity (Exhibit 8) in the pre-
treated group of patients (average number of treatments =2). Encouragingly,
two (40%) of the five MDS patients achieved partial responses (PR); and four
(13%) of the 20 AML patients attained objective responses, including one
immunophenotypic complete response (iCR). The company also observed that
there were rapid changes in the signalling pathways downstream of Axl, and
interesting pro-differentiation effects on the leukaemic cells.
Assuming the data from this trial continues to impress (final data expected in
H218), we would expect the product to advance into Phase III development.
There is a clear need for well tolerated drugs in AML and high-risk MDS. It will,
however, be important for BerGenBio to identify which subgroup of AML
patients are likely to benefit most from BGB324 therapy. After limited
innovation over the last 15 years, in 2017 the FDA approved Novartis’s
midostaurin (Rydapt) for FLT3-mutation-positive AML, Agios/Celgene’s
enasidenib (Idhifa) for IDH2-mutation-positive AML, and Pfizer’s gemtuzumab
ozogamicin (Mylotarg) for CD33-positive AML.
Exhibit 8: Treatment outcomes during dose escalation stage of Phase I/II study in AML/MDS
Source: BerGenBio
A clear need for new drugs as
greater understanding drives
treatment differentiation

13
Trinity Delta
4 January 2018
BerGenBio
Fortunately, BerGenBio had the foresight to include a detailed biomarker
programme within the current Phase I/II study to identify those patients most
likely to respond to BGB324. AML is a heterogenous disease, and gradually
treatment options are improving as the underlying molecular drivers of the
disease are better understood. A specific companion diagnostic would also
potentially protect BGB324 from competition from Astellas’s gilteritinib, which is
in Phase III development for FLT3-mutation-positive AML and Phase I in first-line
AML, is very well tolerated by patients, and is a potent inhibitor of FLT3 and Axl.
We estimate that BGB324 could generate peak sales of $126m in AML and high-
risk MDS, which is based on 5% penetration of the US and European markets. In
the US, the American Cancer Society (ACS) estimates that there are 21,380 new
cases of AML per annum and 13,000 new cases of MDS. We note that there is
considerable divergence of opinion on the true incidence rate of MDS, the ACS
estimate that it is 4.8 per 100,000, but other groups believe is could be as high
as 13.1. We have used the ACS’s estimate. In the case of AML, we have also
adjusted for the cases which are FLT3-mutation positive (c 30%). We estimate
that the average cost of a course of treatment in all indications will be $80,000
in the US, with a 33% discount in Europe. It is particularly challenging to
estimate the potential pricing of BGB324, should it get to market, because of the
broad number of indications and settings in which it could be used.
NSCLC with mEGFR in combination with erlotinib
Patients with EGFR mutation (mEGFR) positive NSCLC (c 30% of cases) are often
treated with Roche’s erlotinib (Tarceva), but their cancers in most cases
normally will recur after 12 months. There are various reasons for the
progression. In half of the cases it is due to additional mutations, either in the
EGFR protein (eg T790M for which AstraZeneca developed osimertinib, Tagrisso)
or in other genes (eg c-Met). Another escape mechanism is EMT via increased
Axl signalling, and it is also known that EGFR and Axl interact in a positive
feedback loop.
BerGenBio has confirmed the potential of BGB324 to treat patients that have
developed erlotinib-resistant NSCLC in preclinical studies (Exhibit 9). The
company is now conducting a Phase I/II to explore further the ability to treat
patients with mEGFR NSCLC that are erlotinib-resistant.
The first part of the Phase Ib/II study that was started in 2015 has been
completed, and, as in the case of the AML study, the trial has already delivered
promising results. The Phase Ib involved dose escalation of BGB324 in heavily-
pre-treated, metastatic, second-line mEGFR patients as monotherapy (n=8) and
in combination with the standard dose of erlotinib (n=8). BGB324 was found to
be well tolerated in both settings up to 600mg loading dose on days one and
two, followed by a daily dose of 200mg per day.
Patient profiling should maximise
BGB324 potential benefit
Adopting conservative assumptions
throughout our forecasting
In combination with Roche’s
Tarceva (erlotinib) in NSCLC
Exploratory Phase I/II study in
erlotinib-resistant patients in place
Phase Ib element of the trial has
produced encouraging results

14
Trinity Delta
4 January 2018
BerGenBio
Exhibit 9: Preclinical data with BGB324 in combination with erlotinib in erlotinib-resistant HCC827 model
Source: BerGenBio; Note: In the HCC827 model, tumours develop erlotinib resistance at day 67 after becoming mesenchymal
There were also initial signs of anti-tumour activity as monotherapy and in
combination with erlotinib (Exhibit 10). In the monotherapy setting, in patients
with or without EGFR mutations, two of the eight people had a PFS of over 40
weeks. In the combination arm with BGB324 and erlotinib in patients resistant
to erlotinib, four of the eight patients had a PFS of over four months, with one of
them still with a stable disease after 88 weeks.
During the second part of the trial, 50 additional patients, with known activating
EGFR mutations and erlotinib-resistant tumours, will be treated with BGB324 in
combination with erlotinib. Interim data from that stage are expected to be
reported at ASCO in June 2018, with the trial being completed at the end of
H218.
There are an estimated 184,000 new cases of NSCLC per year in the US and
255,000 patients in Europe, of these 70% are classed as having Stage III or IV
cancer and c 30% of these cases are mEGFR positive. We estimate that BGB324
could be used to treat 15% of mEGFR patients in the US and 10% in Europe. This
suggests that BGB324 could achieve peak sales of $749m in this setting, with
peak sales being achieved over six years.
NSCLC is a sizeable opportunity
Top line data from Phase II
element expected in H118

15
Trinity Delta
4 January 2018
BerGenBio
Exhibit 10: Treatment outcomes during dose escalation stage of Phase I/II study in NSCLC as (a) monotherapy in metastatic NSCLC and (b) in combination with erlotinib in second-line mEGFR NSCLC
(a)
(b)
Source: BerGenBio
NSCLC and TNBC in combination with pembrolizumab
Immuno-oncology and, in particular, checkpoint inhibitors are transforming the
treatment of many cancer patients, converting the disease into a chronic
indication in some cases. However, it has proved challenging to increase the
proportion of patients that might benefit from the therapy above 30% in most
immunogenic cancers. Given the potential of Axl inhibition to make “cold”
tumours “hot” and increase T-cell activity, Merck and BerGenBio have formed a
collaboration to investigate the potential of combining pembrolizumab
(Keytruda) and BGB324 in adenocarcinoma NSCLC tumours and triple negative
breast cancer (TNBC)3. The belief is that BGB324 will overcome a tumour’s
resistance to a PD1 checkpoint inhibitor.
3 Triple negative breast cancer (TNBC) does not express oestrogen receptor, progesterone receptor or HER2 receptor, which means that there are limited treatment options for TNBC patients other than chemotherapy.
BGB324 being explored in
immuno-oncology regimens

16
Trinity Delta
4 January 2018
BerGenBio
Pembrolizumab has so far been approved for use in melanoma, NSCLC, head and
neck squamous cell carcinoma (HNSCC), classical Hodgkin lymphoma (cHL),
urothelial carcinoma, and microsatellite instability-high cancer (MSI-H). Despite
the broad label, there is still a strong belief that the drug could be used more
broadly if it was combined with the correct agents. For example, pembrolizumab
is only approved in NSCLC as a monotherapy in patients that have tumours with
high levels of PD-L1 expression in over 50% of the cancer (otherwise it must be
used in combination with chemotherapy). Similarly, initial data from the
KEYNOTE-086 study in TNBC shows that some patients did develop durable
responses from monotherapy; however, the overall response rate was only 5%
regardless of PD-L1 expression.
Preclinical studies by different groups have confirmed that BGB324 can act
synergistically with PD1/PD-L1 antibodies in targeting established tumours
(Exhibit 11). The beneficial effect of the two therapies in combination was
associated with higher levels of tumour infiltration by cytotoxic T lymphocytes,
natural killer cells and natural killer T cells, and lower levels of monocytic
myeloid derived suppressor cells (mMDSC, associated with immune suppression
and EMT). Recent studies document that BGB324 treatment inhibits key
immune suppressive arginase-expressing tumour associated macrophages and
increases dendritic cell populations that promote long term anti-tumour
immunity. These changes are all consistent with increased immune activity
against the tumours.
Exhibit 11: Preclinical activity of BGB324 in combination with PD1 and CTLA-4 antibodies
Source: BerGenBio
The Phase II trials in TNBC and NSCLC have already begun. In both studies,
patients will be receiving 200mg of BGB324 (after the loading dose of 600mg
during the first two days) with the standard dose of 200mg of pembrolizumab
every three weeks. During the studies, the level of PD-L1 expression in the
tumours will be measured by Merck; it will not be used as a selection criterion,
but there will be an analysis of the relationship between expression levels and
A clear need to improve more
patient outcomes
Pre-clinical studies suggest
BGB324 acts synergistically
Both TNBC and NSCLC trials due
to report results during 2018

17
Trinity Delta
4 January 2018
BerGenBio
clinical response. Both the NSCLC and TNBC trials are due to be completed in
H218 with interim data published at ASCO in June 2018
We estimate that BGB324 could generate peak sales of $1,210m and $751m
from use in combination with pembrolizumab in adenocarcinoma NSCLC and
TNBC, respectively, based on 15% market penetration in the US and 10% in
Europe. With approximately 40% of lung cancer cases being adenocarcinoma
NSCLC and 70% of those stage III/IV, there are c 62,300 and c 87,700 new cases
of unresectable, adenocarcinoma NSCLC per year in US and Europe, respectively.
In breast cancer, about 15% of cases are classed as TNBC suggesting there are
about 38,000 and 55,000 diagnosed with TNBC each year in the US and Europe,
respectively.
Clearly, if the data from the two studies are positive, we would expect the
development programme in immuno-oncology to expand to other indications
and checkpoint inhibitors. It is important to note that Merck has no rights to
BGB324 from the collaboration, and that during the trials it is only supplying
pembrolizumab and conducting the PD-L1 biomarker assays.
Adenocarcinoma NSCLC with docetaxel
BerGenBio is also exploring the potential of BGB324 to re-sensitise tumour cells
to chemotherapy, through an investigator-led Phase II trial. As previously
discussed, tumour cells change their characteristics during EMT and this can
render them resistant to chemotherapy. The study in second-line NSCLC with
docetaxel is being conducted by Dr David Gerber at the University of Texas
Southwestern Medical Center and there are again promising initial results.
In preclinical studies, BGB324 was shown to act synergistically with docetaxel in
two different models (Exhibit 12). In both cases, it appears that BGB324
prevents the tumour cells from becoming resistant to docetaxel, as they tend to
become after 10-15 days.
The clinical study with BGB324 in combination with docetaxel is a Phase Ib dose-
escalation study. The standard dose of docetaxel (75mg/m2 every three weeks)
is being used initially with a loading dose of 200mg of BGB324 followed by a
daily dose of 100mg, and then with the dose of BGB324 doubled, assuming the
combination is sufficiently well tolerated. This will be followed by up to 30 more
patients being treated with the best dosing regimen from the first stage of the
trial.
Initial data has only been published for the first ten patients from the trial, with
BGB324 being used at the lower dose, and there is already evidence of BGB324
reducing tumour resistance to docetaxel (Exhibit 13). One patient has so far
been treated for 34 weeks without progression, this compares to the median
PFS of about 12 weeks in this indication with docetaxel monotherapy. Further
data from this trial is expected at ASCO in June 2018.
Re-sensitisation of tumours to
traditional oncology treatments
being explored in NSCLC
NSCLC and TNBC are also sizeable
commercial opportunities
Success would open the door to
other potential indications

18
Trinity Delta
4 January 2018
BerGenBio
Exhibit 12: Preclinical data of BGB324 in combination with docetaxel
Source: BerGenBio
Exhibit 13: Initial Phase Ib data of BGB324 in combination with docetaxel in 2nd-line NSCLC
Source: BerGenBio
We forecast that BGB324 could achieve peak sales of $218m in second-line
NSCLC in combination with docetaxel. Of the 184,000 new NSCLC cases per year
in the US and 255,000 patients in Europe, around 30% receive chemotherapy
and c 60% of those advance to second-line therapy. We estimate that 30% of
those are treated with docetaxel so that there are about 33,000 patients treated
with docetaxel in the US and 46,000 in Europe. At this stage, we estimate that
BGB324’s market penetration will be 15% in the US and 10% in Europe.
The market opportunity with docetaxel in second-line NSCLC is relatively
modest. However, if there is impressive data from this Phase Ib trial, the
potential of BGB324 in combination with other chemotherapy regimens could
be explored in other indications. This would significantly increase the peak sales
potential of BGB324 in combination with chemotherapy.
Use of BGB324 with docetaxel
could lead to much broader use
with other chemotherapy
regimens

19
Trinity Delta
4 January 2018
BerGenBio
Malignant melanoma with various therapies
The final study with BGB324 is a Phase Ib, investigator-led study in metastatic
melanoma in combination with pembrolizumab, or dabrafenib (Raf inhibitor)
and trametinib (Mek inhibitor). This is a real-world study in 92 patients and as
such could provide the most valuable data.
The study is being conducted by Haukeland University Hospital, with patients
being treated across Norway in Bergen, Oslo, Tromso and Trondheim (an
additional site at Lorenskog is due to open). During the trial, patients are
allocated to different arms according to their BRAF status, and it also has a cross
over design as illustrated in Exhibit 14.
Exhibit 14: Clinical trial design for Phase II study in metastatic melanoma
Source: Haukeland University Hospital
Initial data from thirteen patients have so far been reported (Exhibit 15) and no
significant additive toxicity has been observed from the use of BGB324 in
combination with dabrafenib/trametinib or pembrolizumab. Further interim
data is expected to be published at ASCO in June 2018.
The treatment of metastatic melanoma has been transformed in recent years
with the approval of Raf and Mek inhibitors and immunotherapies. But, there
are limitations of both therapies; median PFS for dabrafenib/trametinib in the
Phase III COMBI-d trial was only 9.3 months and the overall response rate to
pembrolizumab was 33% and 34% (two dosing arms) in the Phase III KEYNOTE-
006 trial. Axl signalling has been implicated with both resistance to Raf and Mek
inhibitors, as well as enhancing immunotherapies (as discussed above), hence
the belief that BGB324 will improve the clinical outcomes in combination with
both therapeutic regimens for melanoma.
Investigator-led trials are also
underway in melanoma

20
Trinity Delta
4 January 2018
BerGenBio
Exhibit 15: Initial data from the Phase II study in metastatic melanoma
Source: Haukeland University Hospital
We estimate that BGB324 could achieve peak sales of $200m in metastatic
melanoma, by penetrating 15% of the US market and 10% of the European.
There are about 9,700 deaths in the US and 15,700 in Europe from melanoma.
In-licensing deal with Rigel for BGB324
BerGenBio was initially focused on developing a monoclonal antibody against
Axl, but opportunistically decided to in-license various selective Axl inhibitors
from Rigel in June 2011 in a backend weighted deal, once it became aware of
them. Since then, BerGenBio has prioritised the development of the small
molecule BGB324, which was R324.
Under the terms of the deal, BerGenBio obtained the worldwide exclusive rights
to BGB324 and eight back-up compounds with the right to sub-license the assets
(and subsequently, it exercised its option to in-license nine other Axl inhibitors
from Rigel for $2m in June 2016). In exchange, BerGenBio agreed to make
various payments to Rigel; it has so far paid: time-based payments of $0.5m in
2011 and 2012, a similar payment of $1.7m in 2016, and $3.3m in February 2017
relating to the initiation of first Phase II study for the first product. In the future,
payments will depend on whether the product is developed/commercialised in
house or by a partner.
If BerGenBio continues to develop and commercialises BGB324 itself, the
company will have to make the following payments:
▪ $8m milestone on initiation of first Phase III study for the first product;
▪ $12m milestone on submission of an NDA (or equivalent) for the first product; and
The in-licensing of BGB324 was
an inspired deal
Payment terms are back-end
loaded and depend on terms of
eventual commercialisation

21
Trinity Delta
4 January 2018
BerGenBio
▪ $15m milestone for approval of first drug.
▪ Tiered royalties of 5%, 7% or 9% of net sales, if sales are under $500m, between $500m and $1bn, or over $1bn
If BerGenBio out-licenses BGB324, payments based on a revenue sharing model
will need to be made to Rigel according to the schedule below.
▪ 60% of revenues, if partnered prior to completion of Phase Ia;
▪ 50% after completion of the first Phase Ia;
▪ 45% after completion of the first Phase Ib study;
▪ 40% after completion of first Phase II trial;
▪ 35% after completion of first Phase II trial with 60 or more patients; or
▪ 30% after completion of a Phase III study.
BerGenBio is considering whether to partner BGB324. The final decision will
depend on the clinical data; however, we believe that it is most likely that
BerGenBio will look to partner BGB324 with a large player on completion of the
current programme of Phase II studies. Assuming data from the trials confirm
BGB324’s potential to treat a broad range of tumours and in combination with
various other regimens (targeted therapy, immuno-oncology, and
chemotherapy), considerable resources would be required to conduct a broad
Phase III oncology programme. This would be necessary to maximise the value
of BGB324.
Both the Phase Ib/II trials in AML and with erlotinib are expected to recruit over
60 patients. We therefore believe that in the event that BerGenBio enters into a
sub-licensing agreement, it will pay 35% of revenue receipts to Rigel.
Sensitivities
The main risk with BerGenBio at the moment relates to the outcome of the
clinical trials. The initial results are promising, but the true potential of BGB324
will only become apparent at the end of the current Phase II studies. The broad
programme, combined with the biomarker analysis, partially de-risks the
company, but it should be recognised that BerGenBio is developing a first-in-
class product, and the biology of Axl is particularly complex and only partly
understood. It should also be noted that BGB324 might also have a greater
effect on overall survival (OS) than progression free survival (PFS), because of
BGB324’s effect on the immune system and tumour metastasis.
The company is yet to decide whether to take BGB324 to market by itself or with
a partial/full out-licensing of BGB324. The novelty of the compound, while
making the development process more challenging, means that it is likely to be
commercially attractive to prospective partners, especially as it has such broad
potential as an oncology therapy (assuming the current trials are successful).
Should BerGenBio look to partner BGB324, it is important to realise that the best
Clinical trials results are the key
near-term determinants
We believe a licensing deal is
likely in order to maximise the
overall value of BGB324
Axl’s novelty means extensive
trials are required but it also
makes BGB324 very attractive

22
Trinity Delta
4 January 2018
BerGenBio
deal might not be the one with the greatest bio-dollars, but the one with the
most committed partner that will devote sufficient resources to optimise the
product’s development.
BGB324 is currently being developed for AML/MDS, NSCLC, TNBC and metastatic
melanoma in various settings (monotherapy, with targeted therapies, with
chemotherapy and with the checkpoint inhibitor pembrolizumab). The results of
the Phase II studies will determine if the programme is expanded or contracted.
This decision will be based on both scientific and commercial considerations.
The potential of BGB324 as an immuno-oncology therapy agent is particularly
exciting, however, this field is highly competitive.
Although BGB324 is currently the only selective Axl inhibitor in development,
there will probably be more entering the clinic now that the important role that
Axl plays in EMT, chemotherapy resistance and immuno-oncology is better
understood. Clearly, the rate at which BerGenBio can advance BGB324 will
determine the first-mover advantage for the compound, should it reach the
market.
On top of these specific risks, there are also the other usual ones associated with
drug development, including patent litigation, financing and regulatory
uncertainties. Regarding its patent position, the composition of matter patent
(PCT/US07/089177) is due to lapse in 2027 without an extension, and there is a
patent pending covering the use of BGB324 (PCT/GB2014/053548), which
should protect the compound from competition through to 2034. There are also
various other patents (awarded and pending), which could provide a degree of
protection through to 2036.
Valuation
With BerGenBio being a classic drug development company, it is well-suited to
being valued using a rNPV methodology. Typically, the rNPV of the individual
clinical projects (adjusted for the success probabilities) are summed and netted
against the costs of running the operation. In the case of BerGenBio, we
estimate the value of BGB324 in each indication in which it is currently being
developed. The success probabilities in each indication are based on standard
industry criteria for each stage of the clinical development process but are
flexed to reflect the data from the different indications.
Using this approach, we value BerGenBio at NOK1,564m ($184m), which is
equivalent to NOK31.34/share; the details of our valuation are shown in Exhibit
14. The valuation is based on cash flows through to 2034, when we estimate
that BGB324 will lose patent protection. Throughout the valuation we have used
conservative assumptions, in line with our policy. For example, we do not
assume meaningful revenues from BGB324 before 2023, and exclude any value
from BGB324 in any indications beyond those currently being investigated, or
from the rest of its portfolio.
Valuation using a rNPV approach
suggests a value of NOK1,564m
($184m), or NOK31.34 a share
Everything hinges on the current
proof of concept trials
Axl’s role will inevitably attract
other, and possibly larger and
better funded, players
All the other usual drug
development risks also apply

23
Trinity Delta
4 January 2018
BerGenBio
Being prudent, we have assumed the average cost of treatment across all
indications will be $80,000 in the US and two thirds the price in Europe. This
compares to an estimated average cost of treating a patient with AstraZeneca’s
osimertinib (Tagrisso) of $200,000 and Merck’s pembrolizumab (Keytruda) of
$150,000. We believe this is sensible given the limited clinical data. Also,
BGB324 has the potential to be used to treat most solid tumours, either in
combination with chemotherapy or immuno-oncotherapies, and has very low
cost of goods, so a relatively low price might be settled upon to ensure that
reimbursement issues do not hinder adoption of BGB324.
The shares are currently trading at 47% below our valuation of BerGenBio, we
expect this difference to be reduced over the coming year as data is regularly
reported from the six Phase II trials. Four of the clinical trials are also expected
to report final ORR and PFS data by the end of 2018, as well as interim results
from the other studies, which could result in significant increases to our
valuation.
Exhibit 14: rNPV-based valuation of BerGenBio
Indication Total NPV ($m)
Total NPV (NOKm)
Likelihood of success
rNPV ($m)
rNPV
(NOKm)
rNPV/share (NOK)
Notes
AML/MDS 32.9 280.0 30% 7.0 59.3 1.19 Peak sales: $126m
Launch year: 2023
NSCLC with erlotinib
212.2 1,803.3 30% 57.7 490.0 9.82 Peak sales: $749m
Launch year: 2023
NSCLC with pembrolizumab
347.4 2,952.7 20% 62.0 527.0 10.56 Peak sales: $1,210m
Launch year: 2023
TNBC with pembrolizumab
210.5 1,789.0 20% 33.4 283.7 5.68 Peak sales: $751m
Launch year: 2023
NSCLC with docetaxel
62.1 527.5 20% 10.7 90.9 1.82 Peak sales: $218m
Launch year: 2023
Metastatic melanoma
37.7 320.4 20% 5.9 50.0 1.00 Peak sales: $200m
Launch year: 2025
Milestones 242.8 2,063.6 See notes 84.8 720.6 14.44 Milestones totalling $400m,
Likelihood of receipt: 50% to 20%
Rigel payments (497.3) (4,226.9) (124.3) (1,056.2) (21.16) 35% of revenues payable to Rigel
Net cash 47.0 399.2 47.0 399.2 8.00 At Q317
Total 695.1 5,908.7 184.0 1,564.4 31.34
Royalty rate 18%
Discount rate 12.5%
Exchange rate (NOK/$)) 8.5
Tax rate 27% Starting in 2025
Source: Trinity Delta. Note: Valuation assumes BGB324 is out-licensed in 2019. The value of each indication includes the current R&D expenses associated with the current clinical trials.
The low costs of production
mean even prudent price
assumptions are attractive
The expected raft of news flow
provides multiple possible value
inflection points

24
Trinity Delta
4 January 2018
BerGenBio
Financials
BerGenBio had a cash position of NOK399m (c $47m) in cash and no debt at
Q317, reflecting the successful IPO. The company raised NOK375m net
(NOK400m gross), after issuing 16m shares at NOK25 per share on 6 April, ahead
of the shares starting to trade the following day on the Oslo Stock Exchange. We
estimate that this will allow the company to operate into H119, by which time it
should have reported ORR data from the trials in AML (monotherapy), NSCLC
with erlotinib, NSCLC with pembrolizumab and TNBC with pembrolizumab, as
well as interim data from the other studies.
The operating costs have increased rapidly in recent years due to BGB324
starting clinical development and the subsequent expansion in the number and
size of clinical studies. They were NOK58.8m in FY14, NOK72.9 in FY15 and
NOK131.6m (including payments of NOK31.1m to Rigel) in FY16. We expect this
trend to continue with operating costs of NOK194.4m (including a milestone
payment of NOK27.9m to Rigel) in FY17 and NOK238.1m in FY18. We currently
expect the operating expenses to fall slightly in FY19 to NOK233.7m, though this
could vary significantly depending on the outcome of the current clinical trials
and whether BerGenBio decides to take BGB324 into Phase III development.
Cash runway into H119, sufficient
to deliver multiple data points
from all trials.
Operating costs forecast to rise
rapidly as number and size of
clinical trials increase

25
Trinity Delta
4 January 2018
BerGenBio
Exhibit 15: Summary of financials
Source: BerGenBio, Trinity Delta Note: Adjusted numbers exclude exceptionals. The short-term debt in FY19 is indicative of the company’s funding requirement
Year-end: Dec 31 NOKm 2015 2016 2017E 2018E 2019E
INCOME STATEMENT
Revenues 0.0 0.0 0.0 0.0 0.0
Cost of goods sold 0.0 0.0 0.0 0.0 0.0
Gross Profit 0.0 0.0 0.0 0.0 0.0
Personnel costs (25.2) (20.6) (24.3) (26.1) (27.4)
Other expenses (47.6) (110.8) (169.9) (211.8) (206.2)
Amortisation & depreciation (0.2) (0.2) (0.2) (0.2) (0.1)
Underlying operating profit (72.9) (131.6) (194.4) (238.1) (233.7)
Other revenue/expenses 0.0 0.0 0.0 0.0 0.0
EBITDA (72.7) (131.4) (194.2) (237.9) (233.6)
Operating Profit (72.9) (131.6) (194.4) (238.1) (233.7)
Interest income 2.5 3.0 2.1 0.5 0.2
Interest expense (1.7) (1.3) (1.8) (1.3) (8.8)
Other financing costs/income 0.0 0.0 0.0 0.0 0.0
Profit Before Taxes (72.1) (129.8) (194.1) (238.8) (242.3)
Adj. PBT (72.1) (129.8) (194.1) (238.8) (242.3)
Current tax income 0.0 0.0 0.0 0.0 0.0
Net Income (72.1) (129.8) (194.1) (238.8) (242.3)
EPS (NOK) (296.3) (419.7) (4.3) (4.8) (4.9)
Adj. EPS (NOK) (296.3) (419.7) (4.3) (4.8) (4.9)
DPS (NOK) 0.0 0.0 0.0 0.0 0.0
Average no. of shares (m) 0.2 0.3 45.0 49.9 49.9
Gross margin N/A N/A N/A N/A N/A
EBITDA margin N/A N/A N/A N/A N/A
BALANCE SHEET
Current assets 82.0 174.1 365.1 130.9 39.2
Cash and cash equivalents 74.0 161.8 348.6 114.3 22.7
Short-term investments 0.0 0.0 0.0 0.0 0.0
Accounts receivable 0.0 0.0 0.0 0.0 0.0
Other current assets 8.0 12.3 16.6 16.6 16.6
Non-current assets 0.4 0.4 0.4 0.2 0.0
Property, plant & equipment 0.4 0.4 0.4 0.2 0.0
Investments in portfolio companies 0.0 0.0 0.0 0.0 0.0
Other non-current assets 0.0 0.0 0.0 0.0 0.0
Current liabilities (12.1) (21.3) (30.2) (33.7) (183.2)
Short-term debt 0.0 0.0 0.0 0.0 (150.0)
Accounts payable (5.3) (10.7) (14.0) (17.4) (16.9)
Other current liabilities (6.8) (10.6) (16.2) (16.2) (16.2)
Non-current liabilities (5.6) 0.0 0.0 0.0 0.0
Long-term debt 0.0 0.0 0.0 0.0 0.0
Other non-current liabilities (5.6) 0.0 0.0 0.0 0.0
Equity 64.7 153.3 335.3 97.4 (144.0)
Share capital 2.5 3.4 5.0 5.0 5.0
Other 62.3 149.9 330.3 92.4 (148.9)
CASH FLOW STATEMENTS
Operating cash flow (62.9) (124.3) (188.3) (234.3) (241.6)
Profit before tax (72.1) (129.8) (194.1) (238.8) (242.3)
Non-cash adjustments 6.5 3.8 (0.5) 0.6 0.9
Change in working capital 2.7 1.7 5.9 3.4 (0.5)
Interest paid 0.0 0.0 0.4 0.5 0.2
Taxes paid 0.0 0.0 0.0 0.0 0.0
Investing cash flow 0.0 (0.3) (0.2) 0.0 0.0
CAPEX on tangible assets 0.0 (0.3) (0.2) 0.0 0.0
Change in investments in portfolio companies 0.0 0.0 0.0 0.0 0.0
Other investing cash flows 0.0 0.0 0.0 0.0 0.0
Financing cash flow 10.5 212.4 375.2 0.0 150.0
Proceeds from equity 9.2 213.7 375.2 0.0 0.0
Increase in loans 1.3 (1.3) 0.0 0.0 150.0
Dividends 0.0 0.0 0.0 0.0 0.0
Other financing cash flow 0.0 0.0 0.0 0.0 0.0
Net increase in cash (52.4) 87.8 186.7 (234.3) (91.6)
Exchange rate effects 0.0 0.0 0.0 0.0 0.0
Cash at start of year 126.4 74.0 161.8 348.6 114.3
Cash at end of year 74.0 161.8 348.6 114.3 22.7
Net cash at end of year 74.0 161.8 348.6 114.3 (127.3)

26
Trinity Delta
4 January 2018
BerGenBio
Company information
Contact details
Jonas Lies vei 91,
5009 Bergen,
Norway
Tel: +47 559 61 159
www.bergenbio.com
Top institutional shareholdings % holding
Meteva AS 29.89
Investinor AS 13.24
Sarsia Seed AS 4.24
Verdipapirfondet Alfred Berg Gamba 3.71
MP Pensjon PK 3.67
KLP Aksjenorge 2.61
JP Morgan Chase Bank, London (Wellccome Trust) 2.55
Datum Invest AS 2.42
Sarsia Development AS 2.39
Bera AS 2.17
Top institutional investors 66.89
Other shareholders 33.11
Total shareholders 100.00
Source: BerGenBio

27
Trinity Delta
4 January 2018
BerGenBio
Key personnel
Person Position Biography
Stein Holst Annexstad Non-Executive
Chairman
Joined in February 2016 He has senior industry experience, both at executive and Board levels. He is former executive of Dyno Industrier AS (fine chemicals), and became the CEO of the pharmaceutical firm Nycomed AS (subsequently merged with Amersham Plc and thereafter merged with GE). He was head of AS Isco Group, an Executive Search and Corporate Advisory Group. He co-founded in 1996 NorgesInvestor AS, an Oslo-based Private Equity firm, and was in 2008 the first Chairman of Investinor AS (the VC of the Norwegian State). He was Chairman of Algeta ASA, the pharmaceutical startup that developed Xofigo and was acquired by Bayer in 2014. Other previous Chairman positions comprise commercial banking, business school, public R&D and various industrial enterprises.
Richard Godfrey CEO Joined as Chief Executive Officer in 2008. He has over 25 years’ industry experience in drug development and commercialisation. Previously, he served as CEO of Aenova Inc., a specialist biopharmaceutical company and prior to that was the Managing Director of DCC Healthcare Ltd. He also held positions at Catalant, Eli Lilly and Reckitt Benckiser in R&D and commercial roles. He qualified as a Pharmacist from Liverpool University and received his M.B.A. from Bath University.
Petter Nielsen CFO Joined in 2015 as CFO. He was previously CFO at GexCon, an R&D company that developed into an international group of companies focusing on commercial products and services. Prior to that he worked in the Transaction Advisory Services group at Ernst & Young. He has an MSc in Auditing and an MSc in Economics and Business Administration, both from the Norwegian School of Economics.
Prof James Lorens CSO Co-founder and CSO of BerGenBio, and also a Professor at the Department of Biomedicine at the University of Bergen. He leads a large internationally active academic research laboratory comprising 22 researchers, that is focused on cancer research. Prof. Lorens is an author of more than 85 peer-reviewed articles and numerous patents. He worked at Rigel after completing his postdoctoral studies at Stanford University and has managed many large collaborations with major pharmaceutical and biotechnology companies.
Dr Murray Yule Clinical
Development
Officer
Joined in 2011. Since 1998 has been involved with oncology clinical development, he has supervised multiple early phase clinical studies, and planned and executed global development strategies for several anticancer drugs for top-ten pharmaceutical companies. His work has led to licensing approvals for novel tubulin binders in solid tumours and epigenetic therapies in acute leukaemia. He completed his medical training in oncology at Addenbrookes Hospital, Cambridge and holds a PhD in experimental pharmacology.

Trinity Delta, 15 Eldon Street, London, EC2M 7LD. Contact: [email protected]
Trinity Delta BerGenBio
Mick Cooper PhD CFA [email protected] +44 20 3637 5042 Lala Gregorek [email protected] +44 20 3637 5043 Franc Gregori [email protected] +44 20 3637 5041
Disclaimer
Trinity Delta Research Limited ("TDRL"; firm reference number: 725161), which trades as Trinity Delta, is an appointed representative of Equity Development Limited ("ED"). The contents of this report, which has been prepared by and is the sole responsibility of TDRL, have been reviewed, but not independently verified, by ED which is authorised and regulated by the FCA, and whose reference number is 185325.
ED is acting for TDRL and not for any other person and will not be responsible for providing the protections provided to clients of TDRL nor for advising any other person in connection with the contents of this report and, except to the extent required by applicable law, including the rules of the FCA, owes no duty of care to any other such person. No reliance may be placed on ED for advice or recommendations with respect to the contents of this report and, to the extent it may do so under applicable law, ED makes no representation or warranty to the persons reading this report with regards to the information contained in it.
In the preparation of this report TDRL has used publically available sources and taken reasonable efforts to ensure that the facts stated herein are clear, fair and not misleading, but make no guarantee or warranty as to the accuracy or completeness of the information or opinions contained herein, nor to provide updates should fresh information become available or opinions change.
Any person who is not a relevant person under section of Section 21(2) of the Financial Services & Markets Act 2000 of the United Kingdom should not act or rely on this document or any of its contents. Research on its client companies produced by TDRL is normally commissioned and paid for by those companies themselves (‘issuer financed research’) and as such is not deemed to be independent, as defined by the FCA, but is ‘objective’ in that the authors are stating their own opinions. The report should be considered a marketing communication for purposes of the FCA rules. It has not been prepared in accordance with legal requirements designed to promote the independence of investment research and it is not subject to any prohibition on dealing ahead of the dissemination of investment research. TDRL does not hold any positions in any of the companies mentioned in the report, although directors, employees or consultants of TDRL may hold positions in the companies mentioned. TDRL does impose restrictions on personal dealings. TDRL might also provide services to companies mentioned or solicit business from them.
This report is being provided to relevant persons to provide background information about the subject matter of the note. This document does not constitute, nor form part of, and should not be construed as, any offer for sale or purchase of (or solicitation of, or invitation to make any offer to buy or sell) any Securities (which may rise and fall in value). Nor shall it, or any part of it, form the basis of, or be relied on in connection with, any contract or commitment whatsoever. The information that we provide is not intended to be, and should not in any manner whatsoever be, construed as personalised advice. Self-certification by investors can be completed free of charge at www.fisma.org. TDRL, its affiliates, officers, directors and employees, nor ED will not be liable for any loss or damage arising from any use of this document, to the maximum extent that the law permits.
Copyright 2018 Trinity Delta Research Limited. All rights reserved.
More information is available on our website: www.trinitydelta.org