-
7/31/2019 Troponin Past and Present
1/20
TroponinPast, Present, and Future
Allan S. Jaffe, MD
Abstract:Cardiac troponin is the analyte of choice for
the diagnosis of cardiac injury. It is highly specific for
the heart and much more sensitive than prior biomark-
ers. Because of this increased sensitivity, clinicians
have had to struggle with elevations in novel clinical
situations. We have developed new understandingsabout coronary
artery disease but also have begun to
appreciate that many other entities as well can result in
cardiac injury. As assays have increased in sensitivity
over time, this trend has, if anything, accelerated. This
review attempts to put the past, the present, and the
future into a clinical perspective that will help
clinicians. (Curr Probl Cardiol 2012;37:209-228.)
Cardiac troponin has become the marker of choice for the
evalua-
tion of patients with possible myocardial injury.1,2 Because
our
understanding of cardiac troponin (cTn) is still evolving
and
because old friends like the NB isoenzyme of creatine kinase
(CKMB)
who have served us well often are hard to give up,3 it has taken
a long
time for troponin to be used as efficiently as guidelines and
experts have
suggested.4,5 Indeed, because of its improved sensitivity
compared to
prior markers, clinicians have been very reluctant to use
troponin at the
99th percentile of the upper reference limit (URL) because so
many
patients had elevated values of troponin even with the
first-generation
assays.3,5 This level of sensitivity has increased still further
with modern
day assays.6 Thus, many clinicians and laboratories have used
higher
cutoffs for cTn to reduce the frequency of elevations of
troponin that
clinicians have a difficult time explaining.3,5 This of course
simply makes
the literature and the field far more difficult for clinicians
to understand
because the heterogeneity of cutoff values leads to tremendous
confusion
in the literature and mixed messages about how clinicians should
use
cTn.3,5 The present articulation attempts to resolve some of
these issues
Curr Probl Cardiol 2012;37:209-228.0146-2806/$ see front
matterdoi:10.1016/j.cpcardiol.2012.02.002
Curr Probl Cardiol, June 2012 209
-
7/31/2019 Troponin Past and Present
2/20
and provides a common sense way of dealing with cTn and cTn
elevations. As part of being able to accomplish this important
task, certain
basic information about troponin is obligatory and a certain
limited
understanding of the analytical constraints that come with
measuringtroponin is also of importance. This article does not
attempt to review in
detail all of these elements but instead identifies those that
are critical and
provides appropriate references so that those who are interested
in more
information can augment their understanding about these
important
issues.
Cardiac Troponin Basics
The cTn complex consists of 3 separate proteins encoded by
differentgenes. These include cardiac troponin T (cTnT), cardiac
troponin I (cTnI),
and cardiac troponin C.7 Each protein plays an important role
in
regulating the interaction of actin and myosin filaments and
thus on
cardiac contraction. Troponin C is encoded by 2 genes, 1
specific for fast
twitch skeletal muscle and a second expressed in both
slow-twitched
skeletal muscle and cardiac muscle.8 Thus, it might not be
expected to
have cardiac specificity and, indeed, that is the case. Both
cTnT and cTnI
come from unique genes.7
It appears that both cTnI and cTnT have highcardiac specificity.
The history in regard to cTnI is fairly clear. As best we
can tell, it has never been expressed during neonatal
development nor in
pathologic circumstances in any tissue outside of the heart.7
The situation
for cTnT is more complex. Fetal isoforms of the protein are
expressed
during neonatal development and there were isoforms of cTnT that
were
detected by the initial assay for cTnT many years ago. Part of
this was
because there was some cross-reactivity between the antibodies
used to
detect cTn and skeletal muscle troponin. However, it also
appeared thatthere might be re-expressed isoforms of cTnT in
diseased skeletal muscle,
particularly in renal failure patients. New antibodies were
developed that
eliminated this problem such that the cross-reacting antibodies
that were
found were eliminated.9-11 Recently, we described that some
patients who
have skeletal muscle disease express proteins that are detected
by the
antibodies used in the standard and high-sensitivity cTnT assay.
Whether
these are re-expressed isoforms is unclear but they do appear
capable of
causing a signal with the cTnT assay.
12
Because of the high sensitivity ofthe cTnT, it is impossible to
know for sure that there is no concomitant
cardiac disease, but, at least in a few cases where extensive
evaluations
have been done, that has not appeared to be the case. The
frequency of
this phenomenon is unclear at present and it would be a mistake
to think
that all elevations that are difficult to explain are false
positives caused by
210 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
3/20
this mechanism.12 Nonetheless, it does appear that some patients
with
skeletal muscle disease will have elevated values of cTnT but
not cTnI
and that, unless clinicians are astute to this possibility, the
possibility of
confusing such patients with those who have cardiovascular
disease could
occur (Fig 1). Ongoing research is attempting to define the
extent to
which this phenomenon occurs.
In addition, it is important to understand the way in which the
troponinsare released. It appears, in contrast to some proteins,
such as CK-MB,
which are only localized in the cytosol of myocytes, that
troponin has
multiple localizations.13,14 The initial studies used gentle
buffers and
defined a pool of troponin, which was called the cytosolic pool,
which
was roughly of the same magnitude as that of CK-MB.15 In looking
back
at these studies, it appears, given the way in which they were
done, a
better term for this pool might be the early releasable pool
because it is
not clear that all the protein is localized in the cytosol of
cells.
7
Nonetheless, it is thought that this is the pool that is
released early after
a cardiac insult and thus leads to early elevations of cTn.
However,
because this pool is similar in size for both CK-MB and cTn, one
could
be confused as to why troponin might be more sensitive. In fact,
it is more
sensitive because the so-called release ratio, ie, the amount of
protein
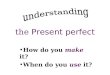
FIG 1. Detection of skeletal muscle proteins by the antibodies
used in the cTnT assay. Westernblot of SMD from patients with
myopathies in lanes 1-4, normal human heart muscle in lane 5,and
normal human soleus muscle in lane 6. Note molecular weight
designations on theordinate. The antibodies used in the standard
cTnT assay (M7 and M11-7) and those used inthe high-sensitivity
assay (M7 and 5D8) all tag a protein at a molecular weight of about
39 kDa.This suggests strongly that the 2 antibodies in each of
these assays would detect these proteinsin blood, indicating that
there is a good possibility that elevations in cTnT or the high
sensitivitycardiac troponin T assay could occur because of diseased
skeletal muscle. (Reproduced withpermission.12)
Curr Probl Cardiol, June 2012 211
-
7/31/2019 Troponin Past and Present
4/20
released into the circulation over the amount that is depleted
from heart,
is far greater for the cTn than it is for CK-MB, which is
degraded
locally.16 Thus, greater amounts of protein are elaborated for
any given
insult via this early releasable pool. This early increase of
cTn is followedby a longer period when troponin is released from
what is thought to be
from a more structurally bound pool that is released as the
damaged area
is remodeled. This provides an explanation for why troponin
elevations
persist for many days, perhaps even weeks, despite its short
half-life in
the blood.15 These kinetics have been used to argue that perhaps
troponin
could be released in the absence of necrosis. Specifically, what
has been
suggested is that perhaps increases in the early release comes
from the
early releasable pool and may not represent cell death but
ratherreversible injury. It is then suggested that the more
sustained release,
which represents the breakdown of the structural pool, is
associated with
cell death. Thus, it has been argued that the presence of only
early but not
late release would indicate reversible injury. Alternatively, it
has been
argued that all the release is due to cell death. This is an
intriguing
scientific argument and there is tremendous controversy over
this partic-
ular issue.17 At present, there are inadequate data to
adjudicate which of
these hypotheses are correct, in part because we have only
recently begunto develop sensitive enough assays to be able to
probe whether the values
we observe are elevated or normal after transient increases.17
Even if the
values go down totally, there probably will still be controversy
about
whether the cells need to be irreversibly injured. When this
issue first
became important in the biomarker field, it did not appear that
the heart
could regenerate in any substantive way. We now know that that
is not the
case and that cardiac regeneration can and does occur.18
Consequently,
perhaps now this is a less important issue. Nonetheless, because
this has beendescribed in certain patients with exercise as well as
in certain disease
entities, it has become an important area of controversy for
clinicians. This
author would argue, given that most elevations of cTn, perhaps
exercise
aside, are associated with an adverse prognosis, that from the
clinical
perspective this distinction is not worth being concerned
about17 and that
troponin should be considered a marker of cardiac damage or
injury and that
such injury should be taken as a sign of underlying
cardiovascular disease in
almost all instances
17
except perhaps exercise.
Important Preanalytic and Analytical FactorsNo assays are
perfect. No antibodies are perfect. Therefore, it should be
expected that there will be problems at times with cTn assays.
It is
important, particularly as we move toward more highly sensitive
assays,6
212 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
5/20
that we take these into account because, absent doing that, we
run the risk
of being confounded because small changes with these highly
sensitive
assays would be of importance. Some of these include the
following:
1. Preanalytic factors. These include issues like hemolysis,
which is
known to increase cTn values for some assays and reduce cTnT
values
with that assay. It is suggested that even small amounts of
hemolysis
may be important with the modern day highly sensitive assays19
(Fig
2). There also are other potential problems, the most common of
which
is fibrin in the sample, which can stick to the well of the
plate and
cause false-positive results for that reason. Therefore,
clinicians shouldnot be uncomfortable about calling and challenging
the laboratory in
regard to specific results.
2. Analytical factors. In addition, there are other analytical
issues that
may need to be taken into account in some patients. The most
common
are what is called cross-reacting or heterophilic antibodies.
This
designation refers to a group of antibodies either made to
the
antibodies that are used to make the cTn assay or which
cross-react to
those antibodies and come from some sort of human disease
processthat can cause the assay to be falsely elevated. The most
well-
publicized situation occurred during the early assay days
when
rheumatoid factor was shown to cross-react with one of the
cTnI
assays, leading to confusion.20 This is no longer a problem,
but
heterophilic antibodies still exist, although most companies
have done
FIG 2. Hemolysis and cardiac troponin. Influence of hemolysis on
the values obtained with 2different troponin assays, the cTnI assay
from Ortho and the high sensitivity cardiac troponin Tassay from
Roche. With very sensitive assays, these problems become more
crucial. (Repro-duced with permission.19)
Curr Probl Cardiol, June 2012 213
-
7/31/2019 Troponin Past and Present
6/20
a good job of eliminating them. With very highly sensitive
assays,
however, even small amounts of these could be problematic.6
Thus,
clinicians must question values that do not appear to fit the
clinical
picture. The situation where one might suspect such antibody
inter-ference is in a patient who has high values that do not
change over
time. In most situations, elevations of cTn do increase and
then
decrease over time. There is an occasional renal failure patient
who
may have high values that do not change but most other
marked
elevations should either increase or decrease. If one finds a
pattern like
this, there are several things that good laboratories can do.7
The first
is to add additional blocking antibodies to the sample and see
if that
resolves the problem. These are widely available in what are
calledheterophile blocking tubes and all good laboratories should
have
access to them. A second approach is to dilute the sample.
Samples
that have interferences of any kind will not change until the
interfering
substance is eliminated. Thus, the failure of a sample to dilute
linearly
should lead to a suspicion of some sort of interfering
substance.
Sometimes these interfering substances can be more complex but
the
vast majority can be diagnosed easily if one remembers the
sugges-
tions made above. There are a variety of other relatively less
frequentproblems, including macrotroponemias (troponin linked to
immuno-
globulins), which have recently been described.21
There are major initiatives going on in an attempt to
standardize cTn
assays but they thus far have not been highly successful.22,23
Thus, it
should be clear that the numbers generated with any given assay
cannot
and are not related in any way to the numbers generated with
other assays.
This in part reflects the different ways of measuring used by
various
companies but also differences in antibodies as well. All of
this informa-
tion in greater detail can be found in recent reviews.24
Decision Limits and PrecisionThis is a critical issue of which
clinicians often are not aware. The
decision limit suggested since 2000 has been the 99th percentile
of a
normal reference population designated usually as URL.25 This is
roughly
3 SDs from the mean of a normal population and was selected
tominimize the frequency of false positives and to take advantage
in a good
sense of that word of the sensitivity of cTn assays. Although
initiated in
2000, because of the reluctance of many clinicians to use these
low
cutoffs because of the difficulty in explaining more subtle
increases, these
cutoffs often have not been used and this can cause confusion.4
Even
214 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
7/20
more recently, high-level sophisticated studies using cTn have
failed to
use the recommended cutoff values.26 Thus, this remains a
problem that
clinicians need to be aware of both when seeing patients and
when
reading the literature. Part of the reluctance in this area
occurred with theconcern that imprecision at the low end might
cause false-positive
elevations.27 This was a reasonable concern when there was no
clue as to
where the normal values existed. Thus, some laboratories argued
that one
should use a cutoff value where there was a high level of
precision so that
one would not potentially overlap with normal values. This led
to the
concept that the cutoff value might be the 10% coefficient of
variation
(CV) value.27 However, over time, it has become clear clinically
that
normal values are substantially far from anything measured today
withthe exception of very high sensitivity troponin assays and thus
the most
predictive clinical cutoff to use is the 99th percentile.7 A
recent article
from the Global Task Force on the redefinition of myocardial
infarction
was developed in part to clarify this previously confusing
issue.5 This
issue was in part even more confounding for cTnT than for cTnI
because
with that assay most normal values are undetectable and thus, to
define a
rising pattern, one often had to go significantly above the 99th
percentile
and frequently the value used was the 10% CV value, making
itadditionally more difficult for clinicians who used that assay to
under-
stand the concept of the 99th percentile. Nonetheless, values
above the
99th percentile URL should be taken seriously as they imply
cardiovas-
cular disease and in almost all instances patient risk.7
A recent article provides a good example of the need to use
lower rather
than higher cutoff values. In the study, the investigators first
evaluated the
outcomes of 1038 individuals presenting with chest discomfort
evaluated
with a contemporary but fairly sensitive cTnI assay using a high
cutoffvalue. They then compared those outcomes to those of 1054
individuals
evaluated with the same assay using a lower cutoff value (the
10% CV
cutoff). Each group was stratified into 3 subgroupsclearly
normal,
clearly abnormal, and a middle group that was initially called
normal and
subsequently called abnormal. The primary outcome was the
combination
of recurrent myocardial infarction and death at 1 year. They
found that the
rates of the use of statins and dual antiplatelet therapy at
discharge, were
similar in the clearly normal and clearly abnormal groups but
improvedsignificantly in the middle group, as might be expected.
Importantly, these
changes in treatment translated into improved outcomes. In the
first
cohort, the primary outcome occurred in 39% of patients in this
middle
(identified as normal) group compared to 7% in the clearly
normal group
and 24% in the clearly abnormal group. During the second part of
the
Curr Probl Cardiol, June 2012 215
-
7/31/2019 Troponin Past and Present
8/20
study, the event rates were similar for those 2 groups but
improvedsignificantly in the group newly called abnormal. The
outcomes in this
group improved from 39% to 21% and were statistically similar to
those
in the clearly elevated group (Fig 3).
As acknowledged by the authors, these results might have been
even
better had the 99th percentile URL value been used.28
Interpretation of Troponin Results
It is now clear with more sensitive cTn assays that the
development ofstructural heart disease over time causes values of
cTn to rise slowly.29,30
It appears that they do not rise acutely but are chronically
elevated. Thus,
minor elevations of cTn will be seen more and more frequently as
assay
sensitivity increases. Therefore, the concept of using a
solitary cutoff
value for cTn as abnormal and indicative of an acute event is
fraught with
FIG 3. Better treatment associated with using lower cutoff
values of cTn. Effect of altering thecutoff value deemed as
abnormal in patients with acute coronary syndromes. The top curves
inbold and dashed lines represent patients with very low clearly
normal values, and they did well.Two of the curves in the middle
designate patients with marked elevations (solid line and
smalldashed line) and they did not do as well as those who were
normal. Because this value was
clearly abnormal during both phases of the study, the patients
did comparably. The lower curverepresents those patients considered
normal during the initial (validation) phase of the study andthey
did poorly. When they were included as being abnormal in the
subsequent (implementa-tion) phase of the study as indicated by the
third curve in the middle (larger dashes and dots),they received
treatment and improved their prognosis to be similar to those
treated previously(the groups with clearly abnormal values). These
data confirm the advantage of using lowerrather than higher cutoff
values for cTn. (Reproduced with permission.26)
216 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
9/20
danger. If the value is markedly elevated, because most of these
structural
abnormalities are associated with only minor degrees of
elevation (with
the possible exception of a rare patient with renal failure),
then this may
still be a useful concept.31 However, one cannot and should not
believethat a solitary cutoff will work for all assays. For that
reason, one of the
important issues now that people are attempting to resolve is
how to
define best a changing pattern of values, which might
distinguish those
individuals with acute disease from those with more chronic
elevations.32
This is a highly complex topic, in particular, with
high-sensitivity cTn
assays. With non-high-sensitivity assays, the best that can be
done is to
use a metric, asking the question whether the value is different
from
analytical variability. It is known for any 2 values that they
aresignificantly different analytically if they are roughly 3 SDs
of the
variance around the values from each other. Thus, by knowing the
metrics
of a given assay, laboratorians can provide an estimate as to
whether these
values are above the variation given the imprecision of that
assay. This is
more complex than it appears because at very low values assay
variability
goes up substantially. Thus, although this value is probably
close to 20%
once elevations have occurred, when one is dealing with values
near the
normal range or perhaps slightly below it, these values could
besubstantially higher even with some assays as high as 100 or
200%.33
Therefore, the task of defining that when a significant change
occurs that
should be taken care of and developed by the laboratory
community, who
should report these data to help clinicians with this.7
For high-sensitivity assays, the issues are more complex. With
high-
sensitivity assays, one can measure results in normals
repetitively and
define what is known has biological variation.34 Unfortunately,
biological
variation may be higher than what may be clinically significant
and thisis a tension in the field.33 However, the theory of
biological variation
would argue that if one is using a change that is below the
level of
biological variation, one at least has the risk of including
patients who are
in that category because of changes related solely to biological
and
analytical issues. Thus, it should be clear and is the case that
the use of
any paradigm looking at a changing pattern is very likely to
increase
specificity for acute change but may reduce sensitivity.35 At
present,
many people using high-sensitivity assays are attempting to
argue foreither percentage changes or absolute changes as the best
metrics to
define a changing pattern.33 These data will play out over time.
It is this
authors opinion that absolute values as recently reported36 may
turn out
to be somewhat better only because, as values increase, the
percentage
values will cause changes to be mandated that are unlikely to
occur except
Curr Probl Cardiol, June 2012 217
-
7/31/2019 Troponin Past and Present
10/20
with very large infarctions, making the use of percentages less
efficient.
By contrast, as values rise, the use of absolute values will
impinge on the
biological variation discussed above and likely lead to the
exclusion of
some patients who have significant disease. This issue is
presently veryconflicting and needs further investigation.33
Although the distinction between chronic and acute elevations
is
important, it is also important to understand that, whereas
previously
assays, because of their relative insensitivity, detected mostly
patients
with acute ischemic heart disease, cTn, given its improved
sensitivity,
detects many other pathophysiologies. This can include
tachycardia or
hyper-/hypotension-induced supply-demand abnormalities and
therefore
ischemia as well as a variety of other acute and chronic cardiac
stressors
diseases. Reviews on these topics can be found elsewhere.37
Conse-
quently, an elevated troponin or even a changing pattern should
not be
taken as indicative of acute myocardial infarction (AMI) but
solely of
cardiac injury. It is true that very high values of cTn are seen
rarely with
the exception of an occasional renal failure patient and with
either
myocarditis or AMI.31 Thus, high values (these are assay
specific) can be
intuited to be due to myocardial infarction or myocarditis.
However,modest elevations need to be triaged clinically and cannot
be assumed to
be due to unstable coronary heart disease. In point of fact, not
only could
elevations be due to a variety of other acute etiologies (Table
1) but in
addition they could be due to coronary artery disease that is
stable. Recent
data suggest that elevations occur in patients with stable
coronary disease
but that that group probably is the higher risk subset of those
with stable
coronary disease38 and the frequency of these elevations is
increasing as
assay sensitivity increases.39,40
It could turn out eventually that we willfind that cTn
elevations identify those with chronic stable disease who are
at risk and there are some data to suggest that, the worse the
disease, the
higher the cTn value,40 and the worse the prognosis.38,39 It is
also of
interest that women have lower values for any given extent of
coronary
artery disease than men.40 However, chronic stable disease, like
hypo-
tension or hypertension without coronary artery disease, does
not imply
that there was necessarily acute plaque rupture and a
myocardial
infarction in need of intervention. Thus, what is necessary is a
clinicalstory highly suggestive of ischemic heart disease coupled
with a rising
pattern of cTn. It should be noted that if one sees patients
with elevated
cTn (but not a rising pattern) and then relies only on cardiac
catheteriza-
tion, one might presume that many of them have myocardial
infarctions
because they have coronary artery disease. However, again, a
solitary
218 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
11/20
elevation of cTn does not infer that coronary artery disease is
unstable
because this could occur with stable coronary artery disease as
well.
Another area that is interesting and difficult to deal with in
regard to cTnis congestive heart failure. cTn elevations are quite
common in this
situation, particularly with acute heart failure,41 and can
occur with
chronic heart failure as well.42 These occur with or without the
presence
of coronary artery disease so they likely represent acute left
ventricular
dilation,43 supply-demand imbalance, and endothelial
dysfunction.44
Again, whether these patients should be called AMIs is an issue
now
being discussed for the new guidelines.
Michael H. Crawford: The complexities and difficulties with the
troponinassay that Dr Jaffe expertly enumerates have been a source
of greatfrustration for clinicians. Few blood-based laboratory
tests are as difficult tointerpret as troponin, yet our less
knowledgeable colleagues often think thatthe reported value is as
definitive as a serum sodium level. Add to this the
TABLE 1. Causes of cTn elevations in the absence of overt acute
ischemic heart disease
Damage related to secondary myocardial ischemia (MI type 2)
Tachy- or bradyarrhythmias
Hypo- or hypertension, eg, hemorrhagic shock, hypertensive
emergency
Acute and chronic heart failure without significant concomitant
coronary artery disease
(CAD)
Hypertrophic cardiomyopathy
Coronary vasculitis, eg, systemic lupus erythematosus, Kawasaki
syndrome
Coronary endothelial dysfunction without significant CAD, eg,
cocaine abuse
Damage not related to myocardial ischemia
Cardiac contusion
Cardiac incisions with surgery
Radiofrequency or cryoablation therapy
Rhabdomyolysis with cardiac involvement
MyocarditisCardiotoxic agents, eg, anthracyclines, Herceptin,
carbon monoxide poisoning
Severe burns affecting 30% of body surface
Indeterminant or multifactorial group
Apical ballooning syndrome
Severe pulmonary embolism or pulmonary hypertension
Peripartum cardiomyopathy
Renal failure
Severe acute neurological diseases, eg, stroke, trauma
Infiltrative diseases, eg, amyloidosis, sarcoidosis
Extreme exertion
Sepsis
Acute respiratory failure
Frequent defibrillator shocks
Reproduced with permission.7
Curr Probl Cardiol, June 2012 219
-
7/31/2019 Troponin Past and Present
12/20
progressive increase in the sensitivity of the assays and you
have a recipe foroverutilization of health care resources. The
latest insult to clinicians is thepoint-of-care assay, which can be
done by minimally trained individuals atthe bedside. Although it is
highly variable and uses a markedly different
normal range, it is being touted as the first arbiter of
hospital admission.Fortunately, at my institution, the results were
so inaccurate that we wereable to discontinue it after a couple of
weeks. As Dr Jaffe points out, thenewer high-sensitivity troponin
assays have not caught on yet in the USA,mainly because of poor
reproducibility, but this problem will be overcome.Emergency
Department doctors will embrace this assay because it willreduce
the false negatives that result in lawsuits. Also, it may permit
theearlier detection of myocardial infarction, resulting in a
faster turnover in theEmergency Department, which is desirable for
patient care as well. However,false positives will abound. The
bottom line is that things will worsen before
they improve.
Diagnosis of Acute Myocardial InfarctionAs should be apparent,
the diagnosis of AMI is heavily determined by
the clinical situation. Thus, the situation must be a
circumstance where
the clinical situation and/or signs and symptoms of the patient
lead to a
strong suspicion of AMI before measuring cTn.45 This could be at
times
the clinical circumstance that exists because diabetics may have
relativelyunrecognized AMIs or, in surgery patients who are not
doing well, even
if they do not complain of chest pain. In the postoperative
circumstance,
symptoms may not be present and electrocardiography (ECG)
changes
can be frequent and nonspecific.46 Thus, one needs to have an
open mind
and not insist on the classic presentation. By contrast, the
idea that simply
because a cTn is elevated that acute coronary event has occurred
is also
not an appropriate stance. Thus, the first issue of importance
in the
diagnosis of AMI is the clinical circumstances around the
presentation ofany given patient. The second circumstance is,
assuming appropriate of
the presentation, is a rising and/or falling pattern of troponin
values.1
AMI, being an acute event, should show an increasing pattern of
values
and then a decreasing pattern of values. This can be problematic
if the
time of onset of symptoms is unclear because the persistence of
elevations
of cTn; one lead is to find relatively slowly changing values of
cTn on the
tail end of the curve. This can be a problem for clinicians to
sort out but
the only way to deal with this issue is clinically. There are no
biochemicaldeterminants that can answer that question.
One also needs to be aware that there are variants of AMI that
can
occur. For example, there are subsets of patients, more often
women, who
can have AMI without overt coronary artery disease47,48 (Fig 4).
Whether
this is due to endothelial dysfunction or the fact that an
inciting event,
220 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
13/20
such as a thrombus or a small dissection, may have resolved
before
angiography is unclear at present but such cases clearly exist.
They appear
to be associated with a better prognosis than certain other
circumstances
but that does not mean that AMI should not be diagnosed.49
Several series
have examined this type of presentation and found that
magnetic
resonance imaging often is often helpful in these individuals.
It may well
be that identifying these groups, whether it is the females with
endothelial
dysfunction or the broader group who do not have fixed coronary
disease,may be clinically helpful. In fact, it may be that, as the
sensitivity of
cTn assays increase, the percentage of such patients, because it
is
thought that their cTn values are somewhat lower, may
increase.
Therefore, the prior data, developed with less sensitive cTn
assays,
that an elevated cTn in patients with chest discomfort makes
them
good candidates for an aggressive therapeutic approach,
including
aggressive anticoagulation IIB/IIIA agents and an early
invasive
strategy, may no longer be the case.Possible Nonacute Myocardial
Infarction Etiologiesfor Elevations of Troponin
One of the most common reasons for marked elevations of cTn that
has
recently emerged is that of acute myocarditis. Early on, it was
clear that
FIG 4. MRI proof of AMI in a patient with chest pain but near
normal coronary arteries. Delayedenhancement sequence from magnetic
resonance imaging of a woman with chest pain,elevated and rising
cTn values, but what appeared to be normal angiographic
coronaryarteries. The area of abnormality shows an area of delayed
hyperenhancement due togadolinium in the subendocardium. This
pattern is highly suggestive of myocardial infarction.(Reproduced
with permission.47)
Curr Probl Cardiol, June 2012 221
-
7/31/2019 Troponin Past and Present
14/20
myocarditis could be a mimicker,50 but a recent article
examining patients
who present with what appears to be acute infarction but have
normal
coronary arteries angiographically found a small percentage of
individuals
who have the pattern associated with AMI but a larger percentage
ofindividuals who had what appears to be acute myocarditis.51 The
therapeutic
significance of such a diagnosis is not clear yet but it is now
well established
that this is a diagnosis that should be considered a possible
mimicker of AMI.
Michael H. Crawford: Another cause of AMI mimic with normal
coronaryarteries is stress cardiomyopathy. In our tertiary care
hospital, this diagnosis
is more common than myocarditis. Usually, it is characterized by
apicalballooning that resolves after several days, but some
patients may havepersistent heart failure, shock, or death. Rarely,
the wall motion abnormalityinvolves mainly the mid-left ventricular
wall. In subarachnoid hemorrhagepatients, the basal walls are
preferentially involved (Zaroff JG, Rordorf GA,Ogilvy CS, et al.
Regional patterns of left ventricular systolic dysfunction
aftersubarachnoid hemorrhage: evidence for neurally mediated
cardiac injury.J Am Soc Echocardiogr 2000;13:774-9). The common
theme is that the wallsinvolved do not follow a single coronary
artery distribution. Aside from theunusual wall motion
distribution, these patients presentation is similar to AMIwith the
major exception that it occurs much more commonly in women. You
have to have a high index of suspicion in postsurgical patients
who are notdoing well hemodynamically and have elevated troponin
levels, for stresscardiomyopathy, because these patients are often
sedated and do notcomplain of chest pain. The ECG resembles a
typical stent thrombosiselevation MI, which is why the diagnosis is
usually made at cardiac cathe-terization. In the right clinical
setting with the characteristic echocardio-graphic findings,
coronary angiography can often be reserved for those whodo not do
well.
As assay sensitivity increases, there also are likely to be an
increasedpercentage in what are thought to be AMIs related to
supply-demand
imbalance.1 These could be due to hypotension or hypertension,
or
tachycardia with or without hypotension, but more likely than
not they
reflect some underlying cardiovascular pathology. However,
because they
may be related more to the supply-demand imbalance than to acute
plaque
rupture, these individuals may be far less in need of aggressive
therapy
and an invasive strategy. There is presently ongoing discussion
as to
whether this group should be culled out separately or should be
subsumedunder the rubric of AMI. The dilemma of this issue is
clear. Should young
individuals with Wolf-Parkinson-White syndrome who have
severe
tachycardia and elevated cTn who often have peculiar chest
symptoms
and even ECG changes be considered to have AMI? How this evolves
in
the guidelines remains to be determined.
222 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
15/20
Patients who are critically ill often have elevated cTn
values.52 Whether
they are due to supply-demand imbalance and therefore may meet
the
definition of AMI or whether such elevations are due to direct
toxic
effects of catecholamines, sepsis, and other drugs is unclear.
Theimportant concept, however, is they are all associated with an
adverse
prognosis both short and longer term.52 What to do acutely is
unclear
other than to treat the underlying disease optimally but these
patients
continue to be at risk even if they survive to discharge.52
However, often,
the concept of the elevated cTn is out of sight and out of mind
at a point
when perhaps intervention would be helpful. For that reason,
these
patients should be at least evaluated clinically and, if they
have structural
heart disease as is likely, that it be addressed. At present,
there are noguidelines for subsequent management and this is an
area of need that will
likely be helped with time. A similar circumstance occurs in
patients with
elevated cTn values who are postoperative.46 It appears that
some of the
morbidity, perhaps a great deal associated with postsurgical
problems, has
to do with cardiovascular abnormalities, perhaps mostly a
supply-demand
imbalance but perhaps some plaque rupture as well.46 If indeed
these
events are due to a supply-demand imbalance, careful scrutiny of
patients
potentially at risk may be necessary to intervene when they this
occurswith the idea of reducing the morbidity of cardiovascular
disease in this
circumstance. There is a large ongoing trial attempting to
define the
frequency of these acute cardiovascular problems and the
preliminary
results with a high sensitivity assay suggest that it s quite
high.53
Michael H. Crawford: Critically ill or postsurgical patients who
are not doingwell hemodynamically often have troponin measured to
screen for ischemic
heart disease. Whether this is an appropriate use of troponin
measurement isdebatable, but it frequently occurs and cardiology is
almost always subse-quently involved in the patients care. Most
such cases have no history orECG findings consistent with a typical
AMI. Thus, most are probably coronarysupply-demand mismatch
situations with so-called demand ischemia.Many have no underlying
heart disease, but you do not want to miss thosewho do have
coronary artery disease. Consequently, I usually advise thosetaking
care of the patient to obtain a cardiac stress test with imaging
whenthe patient has recovered enough to tolerate testing. Rarely,
we do cardiaccatheterization as a first step in such patients
unless they are not doing well.
ExerciseThere is tremendous controversy about whether exercise
acutely dam-
ages the heart because of the elevations seen in cTn.17,54 This
is not a new
issue. It has been around for years because elevations of CK-MB
were
Curr Probl Cardiol, June 2012 223
-
7/31/2019 Troponin Past and Present
16/20
also observed with exercise and found not to indicate
cardiovascular
disease.17 Nonetheless, given the high specificity of cTn for
the heart, this
has become a major question again. At present it is clear that
there does
not appear to be an acute hazard associated with the mild to
modestelevations in cTn seen in patients who have undergone extreme
exercise,
such as a marathon.17 However, those elevations should resolve
promptly
and should not be marked. If they are marked or do not resolve
within a
day or so with present-day cTn assays, they should not be
considered
because of the extreme exercise. In addition, it is not at all
clear whether
in the long run we will find that there may be some detrimental
effects
because of exercise.55 There are suggestions in several
situations that
perhaps there are long-term negative consequences. This remains
to bebetter defined.
The FutureAll of these problems will become much more difficult
with high-
sensitivity assays. These assays are starting to be used around
the world
with the exception of the USA. They will detect still more
patients at
risk.33 They will detect more minor elevations and with them new
disease
entities to be considered.33
However, they also will increase the rapiditywith which AMI is
diagnosed,56 increase the number of patients identi-
fied,57 and in the long run allow us to monitor things, such as
drug
toxicity,58 that may be subtle and hard to do. It is worth
noting that even
with present-day assays there are some preliminary data in this
area in
particular developed around Adriamycin cardiotoxicity58 and
carbon
monoxide poisoning.59
This is an exciting time. We will in the long run have many
more
questions and many more answers. For now, following these
relativelystraightforward guidelines will help clinicians begin to
capture the great
promise of cTn assays.
Michael H. Crawford: Dr Jaffe, one of the worlds experts on
myocardialbiomarkers, has contributed an excellent review of the
laboratory and clinicalissues surrounding cTn measurements. Despite
considerable issues with thetechnical aspects of the various assays
available, cTn has become the pivotaldiagnostic step in the
diagnosis of AMI. Current efforts are improving the
sensitivity of the assays in the hopes that a more sensitive
assay will allow forearlier diagnosis of AMI, which will lead to
earlier treatment and betteroutcomes. This attractive concept has
yet to be proven and the only thingapparent to clinicians is the
increase in false positives. It is clear that cTncomes from the
heart, so these false positives clinically represent conditionsthat
are not AMI, but release cTn into the blood. It seems that
myocardialischemia because of an imbalance between myocardial
oxygen supply and
224 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
17/20
demand can under certain circumstances release cTn. This fits
with currentthinking about ischemia and heightens awareness that
many ill hospitalizedpatients may have underlying coronary artery
disease. Thus, it is notsurprising that cTn detection indicates a
poor prognosis. What is moredifficult to understand is why
apparently normal individuals can have elevatedcTn levels, such as
after vigorous exercise. We still have a great deal to learnabout
cTn, but it has quickly become a key test in our evaluation of
suspectedmyocardial infarction or ischemia. Its detection is
necessary to diagnose AMInow and elevated levels in other clinical
situations suggest a poor prognosis,probably because of underlying
heart disease.
Acknowledgment: The author appreciates the expert secretarial
assistanceof Michelle Small.
REFERENCES
1. Thygesen K, Alpert JS, White HD, et al. for the Redefinition
of Myocardial
Infarction. Universal definition of myocardial infarction. J Am
Coll Cardiol
2007;50:2173-95.
2. Morrow DA, Cannon CP, Jesse RL, et al. National Academy of
Clinical
Biochemistry Laboratory Medicine Practice Guidelines: clinical
characteristics and
utilization of biochemical markers in acute coronary syndromes.
Clin Chem2007;53:552-74.
3. Saenger AK, Jaffe AS. Requiem for a heavyweight: the demise
of creatine
kinase-MB. Circulation 2008;118:2200-6.
4. Jaffe AS, Katus H. Acute coronary syndrome biomarkers: the
need for more
adequate reporting. Circulation 2004;110:104-6.
5. Jaffe AS, Apple FS, Morrow DA, et al. Being rational About
(im)precision: a
statement from the biochemistry subcommittee of the joint
European Society of
Cardiology/American College of Cardiology/American Heart
Association/World
Heart Federation task force for the definition of myocardial
infarction. Clin Chem
2010;56:941-3.6. Wu AH, Jaffe AS. The clinical need for
high-sensitivity cardiac troponin assays for
acute coronary syndromes and the role for serial testing. Am
Heart J
2008;155:208-14.
7. Thygesen K, Mair J, Katus H, et al. Recommendations for the
use of cardiac
troponin measurement in acute cardiac care. Eur Heart J
2010;31:2197-204.
8. Parmacek MS, Solaro RJ. Biology of the troponin complex in
cardiac myocytes.
Prog Cardiovasc Dis 2004;47:159-76.
9. Katus HA, Looser S, Hallermayer K, et al. Development and in
vitro character-
ization of a new immunoassay of cardiac troponin T. Clin Chem
1992;38:386-93.
10. Ricchiuti V, Apple FS. RNA expression of cardiac troponin T
isoforms in diseased
human skeletal muscle. Clin Chem 1999;45:2129-35.
11. Ricchiuti V, Voss EM, Ney A, et al. Cardiac troponin T
isoforms expressed in renal
diseased skeletal muscle will not cause false-positive results
by the second
generation cardiac troponin T assay by Boehringer Mannheim. Clin
Chem
1998;44:1919-24.
Curr Probl Cardiol, June 2012 225
-
7/31/2019 Troponin Past and Present
18/20
12. Jaffe AS, Vasile VC, Milone M, et al. Diseased skeletal
muscle: A noncardiac
source of increased circulating concentrations of cardiac
troponin T. J Am Coll
Cardiol 2011;58:1819-24.
13. Remppis A, Scheffold T, Greten J, et al. Intracellular
compartmentation of troponinT: release kinetics after global
ischemia and calcium paradox in the isolated
perfused rat heart. J Mol Cell Cardiol 1995;27:793-803.
14. Adams JE 3rd, Schechtman KB, Landt Y, et al. Comparable
detection of acute
myocardial infarction by creatine kinase MB isoenzyme and
cardiac troponin I.
Clin Chem 1994;40:1291-5.
15. Jaffe AS, Landt Y, Parvin CA, et al. Comparative sensitivity
of cardiac troponin I
and lactate dehydrogenase isoenzymes for diagnosing acute
myocardial infarction.
Clin Chem 1996;42:1770-6.
16. Vatner SF, Baig H, Manders WT, et al. Effects of coronary
artery reperfusion on
myocardial infarct size calculated from creatine kinase. J Clin
Invest
1978;61:1048-56.
17. Jaffe AS, Wu AH. Troponin releasereversible or irreversible
injury? Clin Chem
2012;58:148-50.
18. Anversa P, Leri A, Kajstura J. Cardiac regeneration. J Am
Coll Cardiol
2006;47:1769-76.
19. Bais R. The effect of sample hemolysis on cardiac troponin I
and T Assays. Clin
Chem 2010;56:1357-9.
20. Krahn J, Parry DM, Leroux M, et al. High percentage of false
positive cardiac
troponin I results in patients with rheumatoid factor. Clin
Biochem 1999;32:477-80.21. Legendre-Bazydlo LA, Haverstick DM,
Kennedy JL, et al. Persistent increase of
cardiac troponin I in plasma without evidence of cardiac injury.
Clin Chem
2010;56:702-5.
22. Apple FS. Standardization of cardiac troponin I assays will
not occur in my
lifetime. Clin Chem 2012;58:169-71.
23. Christenson RH, Bunk DM, Schimmel H, et al., on behalf of
the IFCC Working
Group on Standardization of Troponin I. Put simply,
standardization of cardiac
troponin I is complicated. Clin Chem 2012;58:165-8.
24. Apple FS, Collinson PO, for the IFCC Task Force on Clinical
Applications of
Cardiac Biomarkers. Analytical characteristics of
high-sensitivity cardiac troponinassays. Clin Chem
2011;58:54-61.
25. Alpert JS, Thygesen K, on behalf of the Global Task Force
for redefinition of
myocardial infarction. Myocardial infarction redefinedA
consensus document of
the Joint European Society of Cardiology/American College of
Cardiology com-
mittee for the redefinition of myocardial infarction. Eur Heart
J 2000;21:1502-13.
26. Mills NL, Churchhouse AMD, Lee KK, et al. Implementation of
a sensitive
troponin I assay and risk of recurrent myocardial infarction and
death in patients
with suspected acute coronary syndrome. JAMA
2011;305:1210-6.
27. Apple FS, Wu AH, Jaffe AS. European Society of Cardiology
and American
College of Cardiology guidelines for redefinition of myocardial
infarction: how to
use existing assays clinically and for clinical trials Am Heart
J 2002;144:981-6.
28. Mills NL, Walker S, Newby DE. Sensitive troponin I assay in
patients with
suspected acute coronary syndromereply. JAMA 2011;306:489.
29. Omland T, de Lemos JA, Sabatine MS, et al. A sensitive
cardiac troponin T assay
in stable coronary artery disease. N Engl J Med
2009;361:2538-47.
226 Curr Probl Cardiol, June 2012
-
7/31/2019 Troponin Past and Present
19/20
30. Kavsak PA, Xu L, Yusuf S, et al. High-sensitivity cardiac
troponin I measurement
for risk stratification in a stable high-risk population. Clin
Chem 2011;57:1146-53.
31. Twerenbold R, Jaffe AS, Reichlin T, et al. High sensitive
troponin T measurements.
What do we gain and what are the challenges? Eur Heart J
2012;33:579-86.32. Jaffe AS. Chasing troponin: how low can you go
if you can see the rise? J Am Coll
Cardiol 2006;48:1763-4.
33. Thygesen K, Mair J, Giannitsis E, et al. How to use
high-sensitivity troponins in
acute cardiac care. Eur Heart J 2012 (in press).
34. Fraser CG, Harris EK. Generation and application of data on
Biological variation
in clinical chemistry. Crit Rev Clin Lab Sci 1989;27:409-37.
35. Aldous SJ, Florkowski CM, Crozier IG, et al. Comparison of
high sensitivity and
contemporary troponin assays for the early detection of acute
myocardial infarction
in the emergency department. Ann Clin Biochem 2011;48:241-8.
36. Reichlin T, Irfan A, Twerenbold R, et al. Utility of
absolute and relative changes
in cardiac troponin concentrations in the early diagnosis of
acute myocardial
infarction. Circulation 2011;124:136-45.
37. Jaffe AS. The 10 commandments of troponin, with special
reference to high
sensitivity assays. Heart 2011;97:940-6.
38. Hsieh BP, Rogers AM, Na B, et al. Prevalence and prognostic
significance of
incidental cardiac troponin T elevation in ambulatory patients
with stable coronary
artery disease: data from the heart and soul study. Am Heart J
2009;158:673-9.
39. Korosoglou G, Lehrke S, Mueller D, et al. Determinants of
troponin release in
patients with stable coronary artery disease: insights from CT
angiography
characteristics of atherosclerotic plaque. Heart
2011;97:823-31.
40. Laufer EM, Mingels AM, Winkens MH, et al. The extent of
coronary atheroscle-
rosis is associated with increasing circulating levels of high
sensitive cardiac
troponin T. Arterioscler Thromb Vasc Biol 2010;30:1269-75.
41. Gibler WB, Cannon CP, Blomkalns AL, et al. Practical
implementation of the
guidelines for unstable angina/non-ST-segment elevation
myocardial infarction in
the emergency department: a scientific statement from the
American Heart
Association Council on Clinical Cardiology (Subcommittee on
Acute Cardiac
Care), Council on Cardiovascular Nursing, and Quality of Care
and OutcomesResearch Interdisciplinary Working Group, in
Collaboration With the Society of
Chest Pain Centers. Circulation 2005;111:2699-710.
42. Binder J, Ommen SR, Chen HH, et al. Usefulness of brain
natriuretic peptide levels
in the clinical evaluation of patients with hypertrophic
cardiomyopathy. Am J
Cardiol 2007;100:712-4.
43. Feng J, Schaus BJ, Fallavollita JA, et al. Preload induces
troponin I degradation
independently of myocardial ischemia. Circulation
2001;103:2035-7.
44. Katz SD, Hryniewicz K, Hriljac I, et al. Vascular
endothelial dysfunction and
mortality risk in patients with chronic heart failure.
Circulation 2005;111:310-4.
45. Diamond GA, Kaul S. How would the Reverend Bayes interpret
high-sensitivity
troponin? Circulation 2010;121:1172-5.
46. Landesberg G, Beattie WS, Mosseri M, et al. Perioperative
myocardial infarction.
Circulation 2009;119:2936-44.
47. Martinez MW, Babuin L, Syed IS, et al. Myocardial infarction
with normal
coronary arteries: a role for MRI? Clin Chem 2007;53:995-6.
Curr Probl Cardiol, June 2012 227
-
7/31/2019 Troponin Past and Present
20/20
48. Reynolds HR, Srichai MB, Iqbal SN, et al. Mechanisms of
myocardial infarction in
women without angiographically obstructive coronary artery
diseasee. Circulation
2011;124:1414-25.
49. Ong P, Athanasiadis A, Borgulya G, et al. 3-Year follow-up
of patients with
coronary artery spasm as cause of acute coronary syndrome: the
Caspar (coronary
artery spasm in patients with acute coronary syndrome) Study
Follow-Up. J Am
Coll Cardiol 2011;57:147-52.
50. Franz WM, Remppis A, Kandolf R, et al. Serum troponin T:
diagnostic marker for
acute myocarditis. Clin Chem 1996;42:340-1.
51. Assomull RG, Lyne JC, Keenan N, et al. The role of
cardiovascular magnetic
resonance in patients presenting with chest pain, raised
troponin, and unobstructed
coronary arteries. Eur Heart J 2007;28:1242-9.
52. Babuin L, vasile VC, Rio Perez JA, et al. Elevated cardiac
troponin is an
independent risk factor for short- and long-term mortality in
medical intensive careunit patients. Crit Care Med
2008;36:759-65.
53. Kavsak PA, Walsh M, Srinathan S, et al. Cardiac troponin T
elevations following
noncardiac surgery. Clin Chem 2011;57:1021-4.
54. Hickman PE, Potter JM, Aroney C, et al. Cardiac troponin may
be released by
ischemia alone, without necrosis. Clin Chim Acta
2010;411:318-23.
55. Whyte GP, Sheppard M, George KP, et al. Arrhythmias and the
athlete: mecha-
nisms and clinical significance. Eur Heart J
2007;28:1399-400.
56. Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis
of myocardial
infarction with sensitive cardiac troponin assays. N Engl J Med
2009;361:858-67.
57. Rosalki SB, Wilkinson JH. Reduction of-ketobutyrate by human
serum. Nature
1960;188:1110-1.
58. Cardinale D, Colombo A, Sandri MT, et al. Prevention of
high-dose chemotherapy
induced cardiotoxicity in high-risk patients by
angiotensin-converting enzyme
inhibition. Circulation 2006;114:2474-81.
59. Henry CR, Satran D, Lindgren B, et al. Myocardial injury and
long-term mortality
following moderate to severe carbon monoxide poisoning. JAMA
2006;
295:398-402.