Embed Size (px)
Citation preview
UC
HS
C
Renal and Islet Transplantation in Diabetes
Renal and Islet Transplantation in Diabetes
Alex Wiseman, M.D.Director, Renal Transplant Clinic
University of Colorado Health Sciences Center
UC
HS
C
ObjectivesObjectives Compare treatment options of dialysis vs. kidney
transplantation in patients with diabetes and renal failure
Understand the importance of early kidney transplantation in patients with diabetes
Define current success rates of islet transplantation
List commonly encountered side effects following islet transplantation
Describe future directions for islet transplantation
UC
HS
C
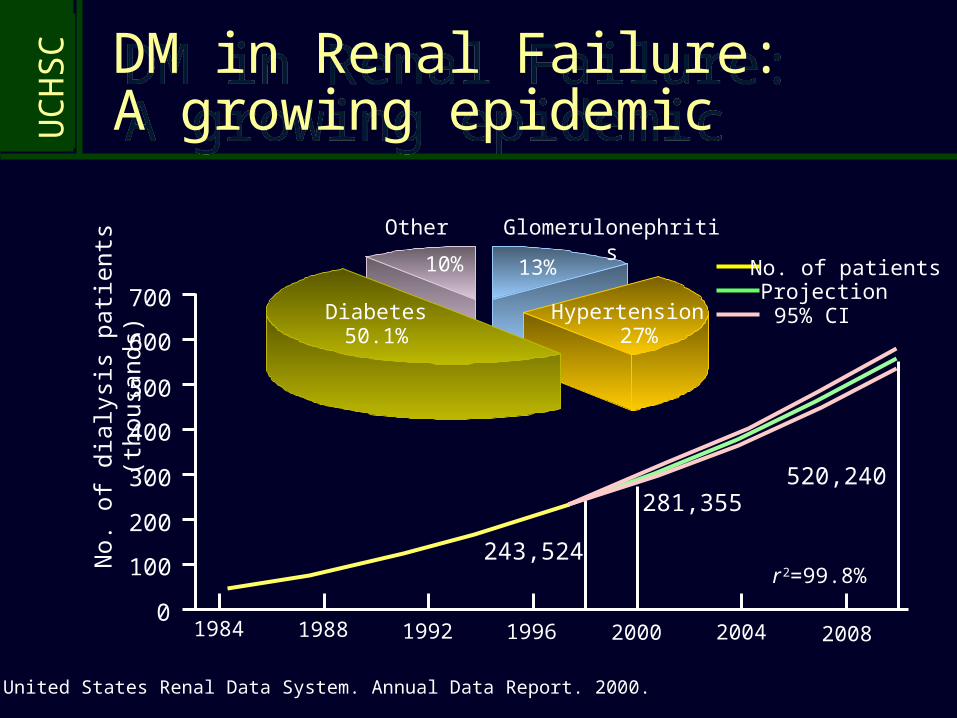
Diabetes50.1%
Hypertension27%
Glomerulonephritis
13%
Other
10%
United States Renal Data System. Annual Data Report. 2000.
No. of patientsProjection95% CI
1984 1988 1992 1996 2000 2004 20080
100
200
300
400
500
600
700
r 2=99.8%
243,524
281,355520,240
No.
of
dial
ysis
pat
ient
s (t
hous
ands
)DM in Renal Failure: A growing epidemicDM in Renal Failure: A growing epidemic
UC
HS
C
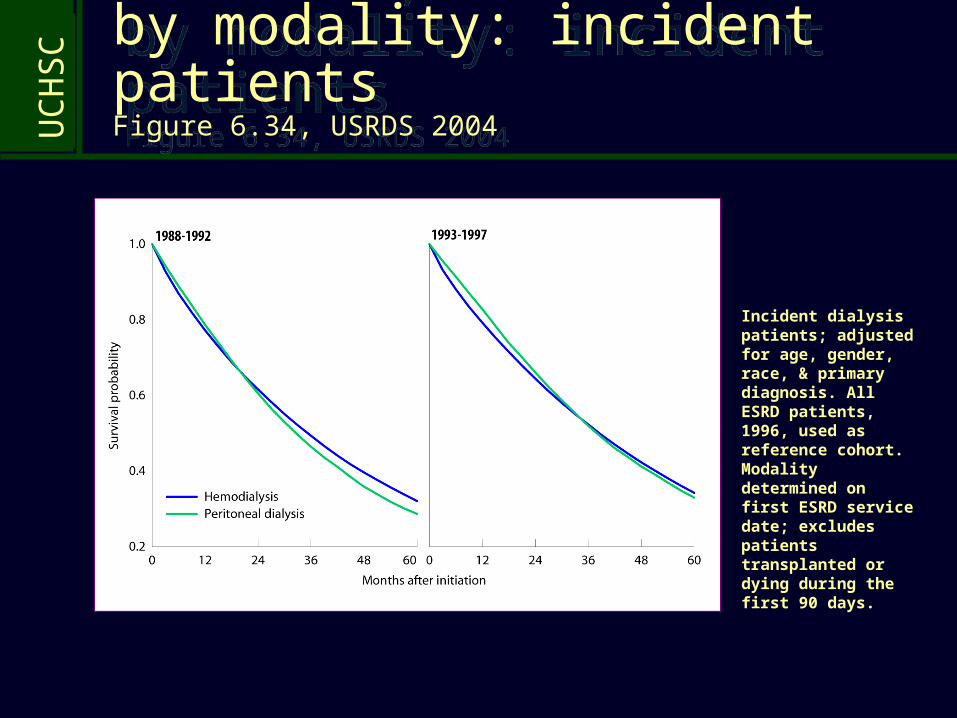
Incident dialysis patients; adjusted for age, gender, race, & primary diagnosis. All ESRD patients, 1996, used as reference cohort. Modality determined on first ESRD service date; excludes patients transplanted or dying during the first 90 days.
Adjusted five-year survival, by modality: incident patients Figure 6.34, USRDS 2004
Adjusted five-year survival, by modality: incident patients Figure 6.34, USRDS 2004
UC
HS
C
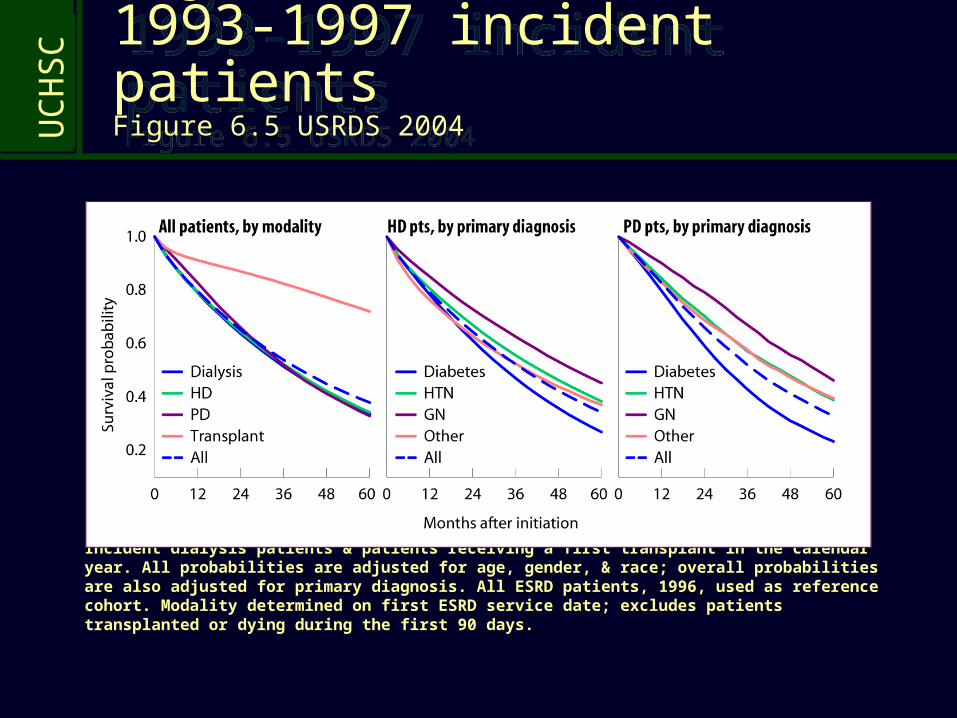
Incident dialysis patients & patients receiving a first transplant in the calendar year. All probabilities are adjusted for age, gender, & race; overall probabilities are also adjusted for primary diagnosis. All ESRD patients, 1996, used as reference cohort. Modality determined on first ESRD service date; excludes patients transplanted or dying during the first 90 days.
Adjusted survival: 1993-1997 incident patients Figure 6.5 USRDS 2004
Adjusted survival: 1993-1997 incident patients Figure 6.5 USRDS 2004
UC
HS
C
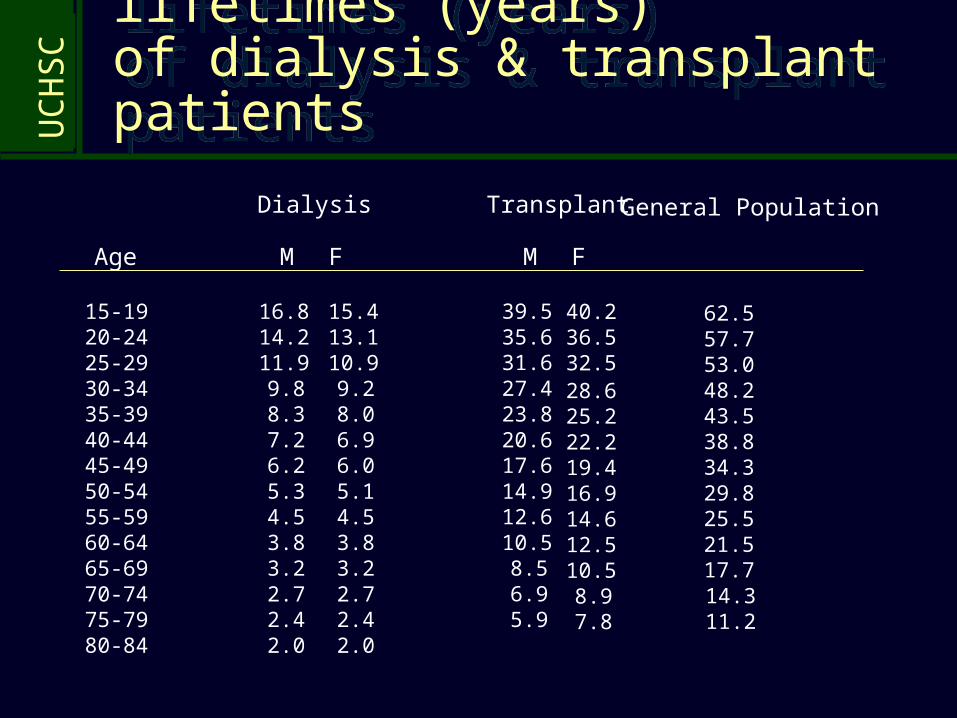
Expected remaining lifetimes (years) of dialysis & transplant patients
Expected remaining lifetimes (years) of dialysis & transplant patients
Dialysis Transplant
M F
39.5 40.235.6 36.531.6 32.527.4 28.623.8 25.220.6 22.217.6 19.414.9 16.912.6 14.610.5 12.58.5 10.56.9 8.95.9 7.8
Age
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84
M F
16.8 15.414.2 13.111.9 10.99.8 9.28.3 8.07.2 6.96.2 6.05.3 5.14.5 4.53.8 3.83.2 3.22.7 2.72.4 2.42.0 2.0
62.557.753.048.243.538.834.329.825.521.517.714.311.2
General Population
UC
HS
CHow much does a transplant benefit the patient?
How much does a transplant benefit the patient?
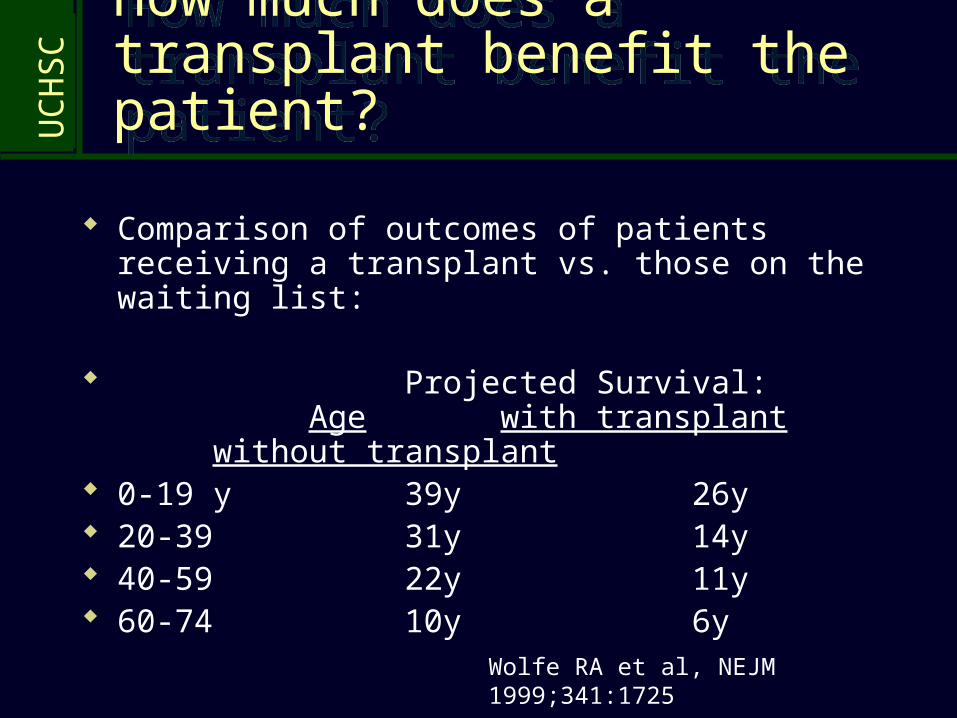
Comparison of outcomes of patients receiving a transplant vs. those on the waiting list:
Projected Survival:Age with transplant without
transplant 0-19 y 39y 26y 20-39 31y 14y 40-59 22y 11y 60-74 10y 6y
Wolfe RA et al, NEJM 1999;341:1725
UC
HS
CIn patients with diabetes, dramatic survival benefit with transplant
In patients with diabetes, dramatic survival benefit with transplant
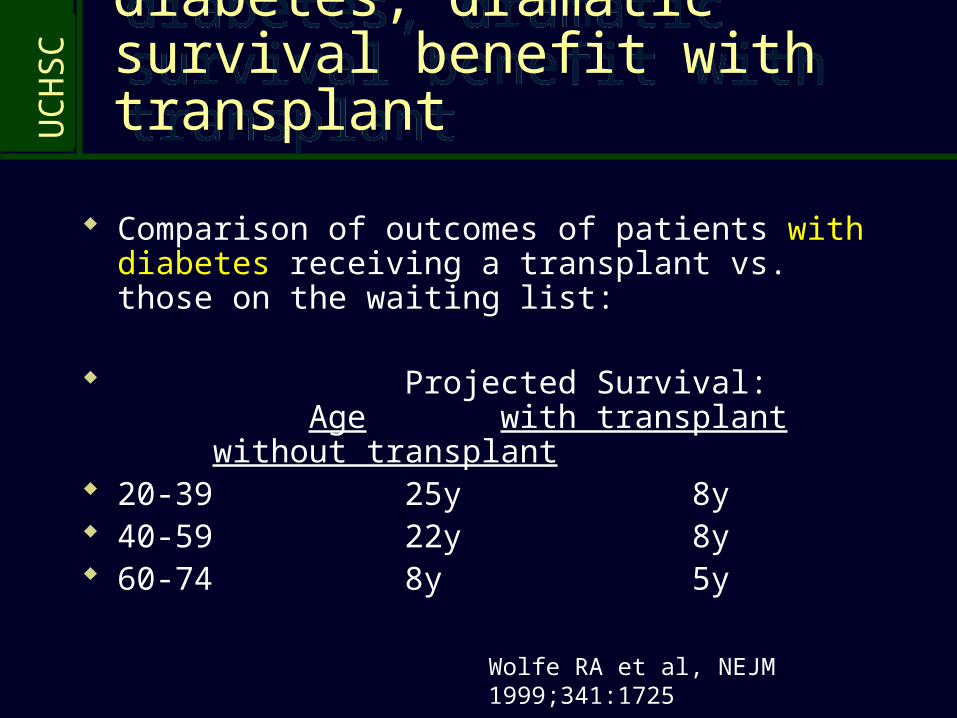
Comparison of outcomes of patients with diabetes receiving a transplant vs. those on the waiting list:
Projected Survival:Age with transplant without
transplant 20-39 25y 8y 40-59 22y 8y 60-74 8y 5y
Wolfe RA et al, NEJM 1999;341:1725
UC
HS
C
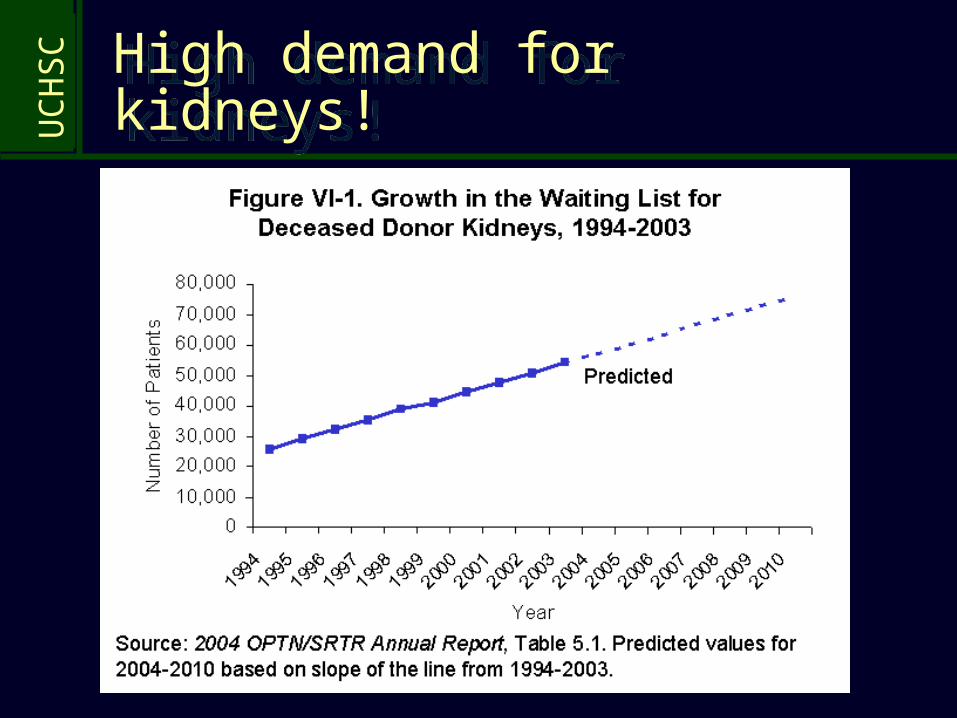
High demand for kidneys!High demand for kidneys!
UC
HS
C
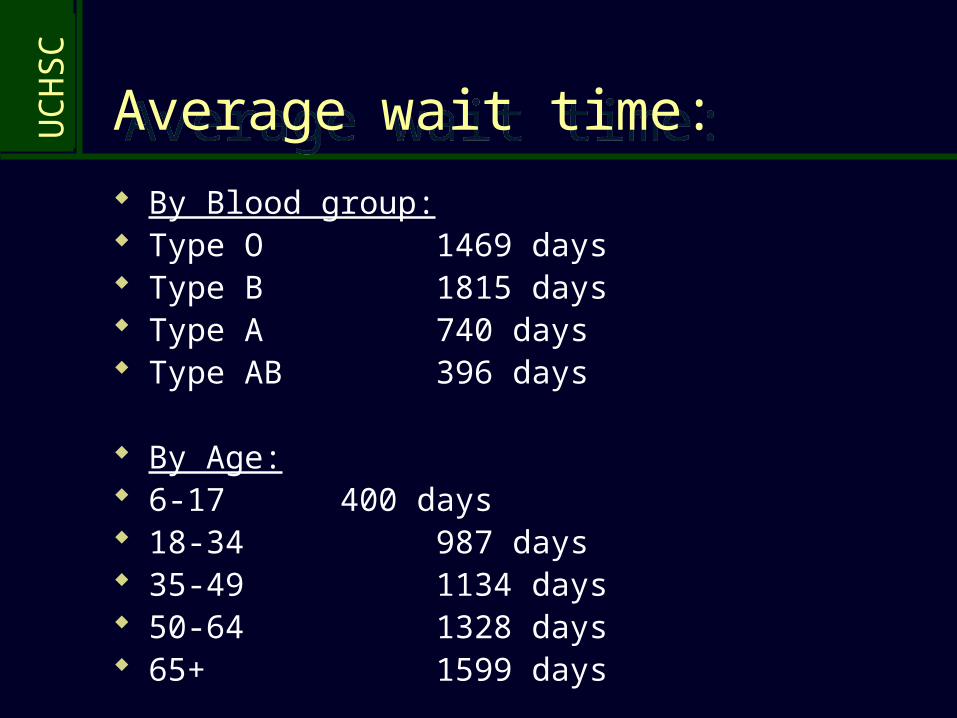
Average wait time:Average wait time: By Blood group: Type O 1469 days Type B 1815 days Type A 740 days Type AB 396 days
By Age: 6-17 400 days 18-34 987 days 35-49 1134 days 50-64 1328 days 65+ 1599 days
UC
HS
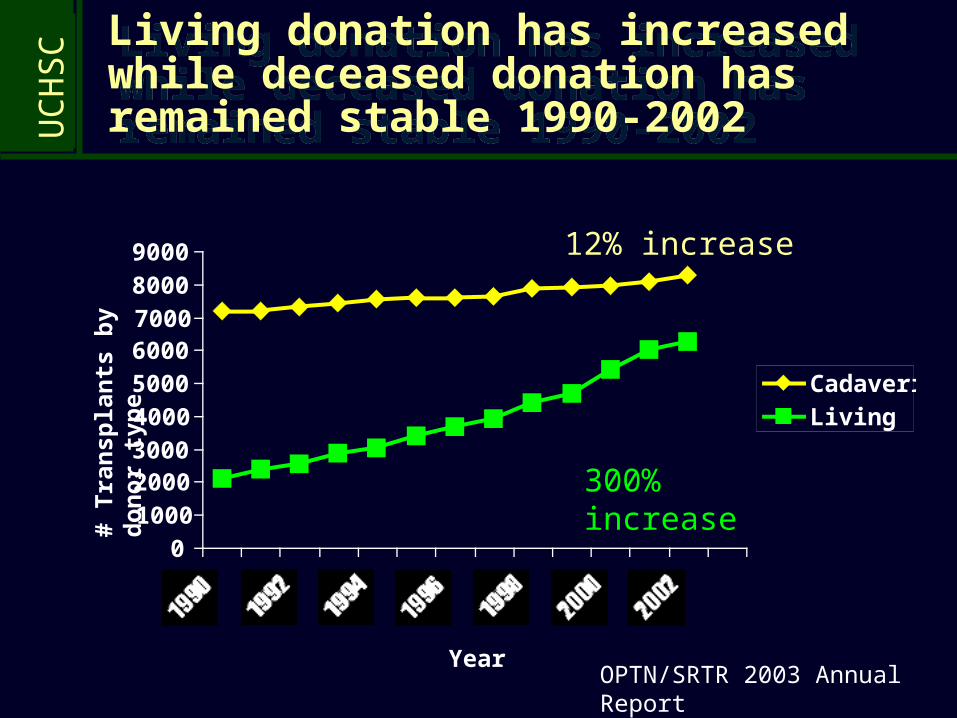
C Living donation has increased while deceased donation has remained stable 1990-2002
Living donation has increased while deceased donation has remained stable 1990-2002
0100020003000400050006000700080009000
1990 1992 1994 1996 1998 2000 2002
CadavericLiving
# T
rans
plan
ts b
y do
nor
typ
e
YearOPTN/SRTR 2003 Annual Report
300% increase
12% increase
UC
HS
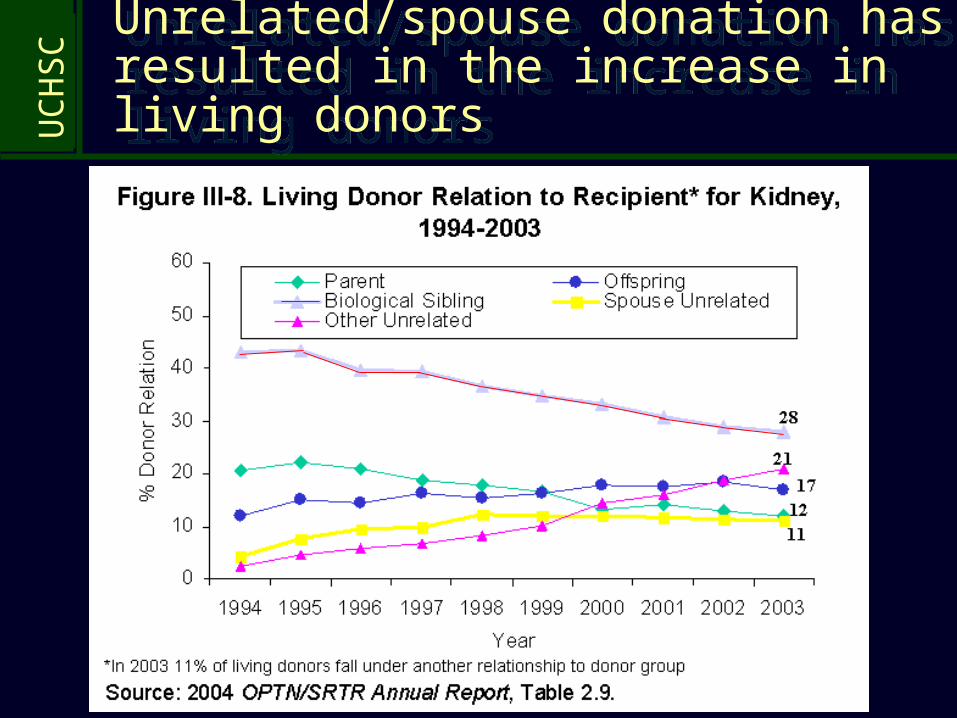
C Unrelated/spouse donation has resulted in the increase in living donors
Unrelated/spouse donation has resulted in the increase in living donors
UC
HS
C
HUMAN ISLET TRANSPLANTATION HUMAN ISLET TRANSPLANTATION
UC
HS
C
General Principle:General Principle:
Normalization of blood glucose (not merely control of blood glucose) will lead to improvements in: Survival Quality of life Protection from heart disease, kidney disease,
retinopathy, and nerve injury
The only method that normalizes blood glucose in patients with diabetes is treatment with insulin-producing cells
UC
HS
CMethods to treat with insulin-producing cellsMethods to treat with insulin-producing cells
Pancreas transplant Pancreas obtained from cadaver
donors, transplanted surgically within 12 hours
Surgical procedure involves general anesthesia, abdominal surgery, and a 7-10 day hospitalization
Complications: Thrombosis of pancreatic
vessels Pancreatic leak Infection
Islet Cell Transplant Islet tissue obtained from cadaver
organs by collagenase digestion of the pancreas and purification of islets via density gradients
Islets injected into portal vein for liver implantation, performed by interventional radiology, followed by a 1-2 day hospitalization
Complications: Bleeding Thrombosis
UC
HS
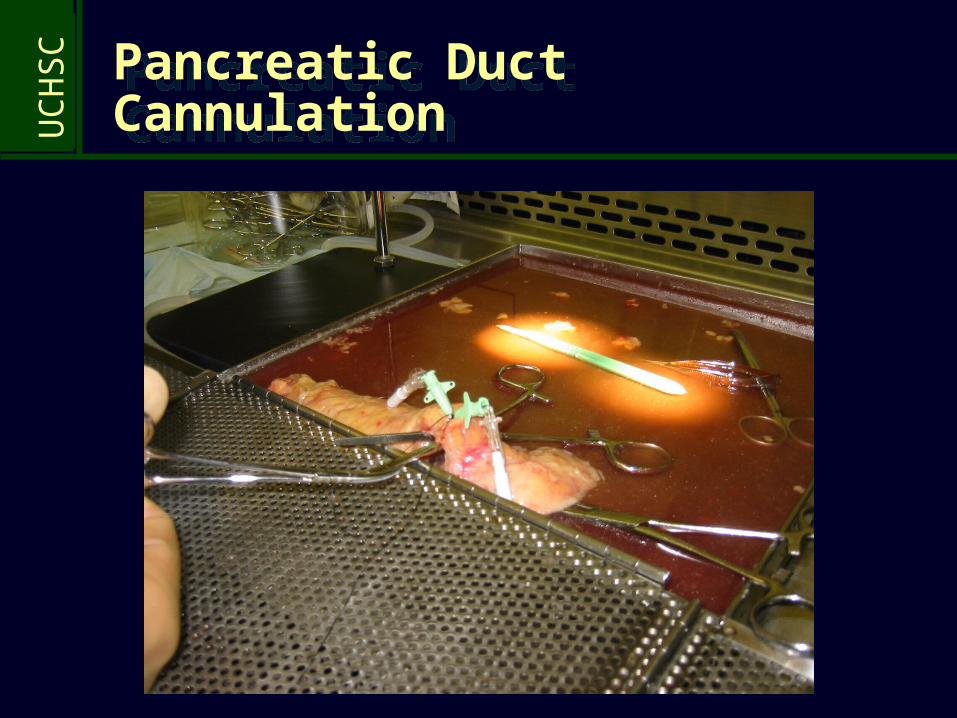
CPancreatic Duct CannulationPancreatic Duct Cannulation
UC
HS
C
Final islet prepFinal islet prep
UC
HS
C “Insulin independence after solitary islet transplantation in type 1 diabetic patients using steroid-free immunosuppression”
“Insulin independence after solitary islet transplantation in type 1 diabetic patients using steroid-free immunosuppression”
7 consecutive patients achieved euglycemia during a mean follow-up of 11 months, with normal HgbA1c and GTT
6/7 patients required >1 donor (>1 transplant) a median of 29 days from the first procedure
Mean islet equivalents =11,400/kg required to achieve euglycemia
Cadaveric pancreata from older donors >45 yo (70% would have been discarded)
Shapiro AMJ et al, NEJM 2000; 343:230
UC
HS
C600
500
400
300
200
100
2 4 6 8 10 12
2 4 6 8 10
600
500
400
300
200
100
012
a.m. p.m.
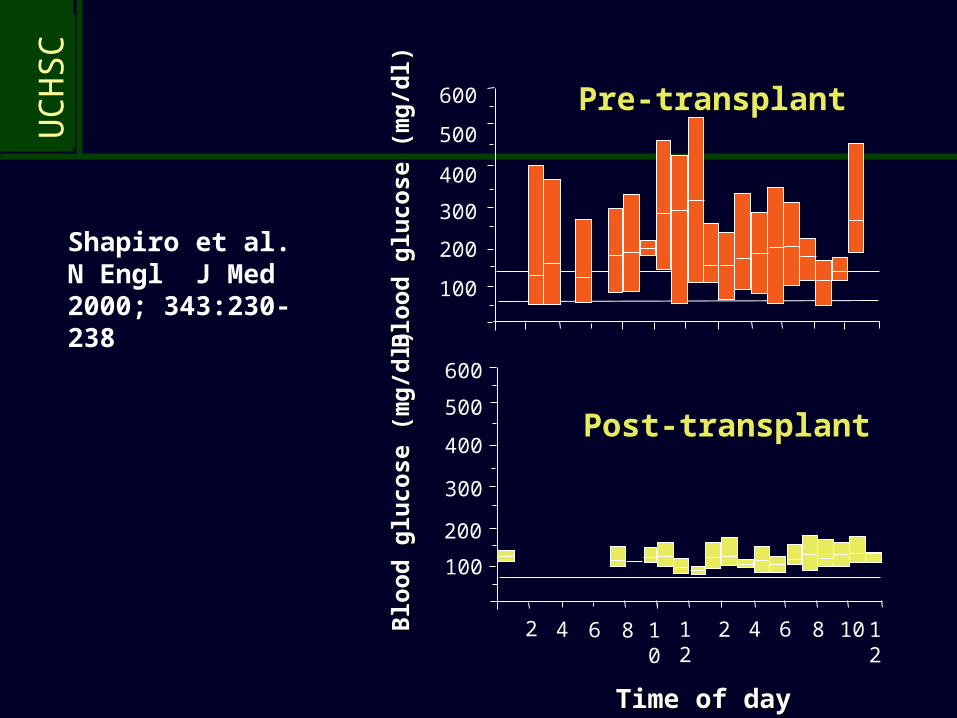
Post-transplantPost-transplant
Pre-transplantPre-transplant
Time of dayTime of day
Blo
od
glu
cose
(m
g/d
l)B
loo
d g
luco
se (
mg
/dl)
Blo
od
glu
cose
(m
g/d
l)B
loo
d g
luco
se (
mg
/dl)
Shapiro et al. N Engl J Med 2000; 343:230-238
UC
HS
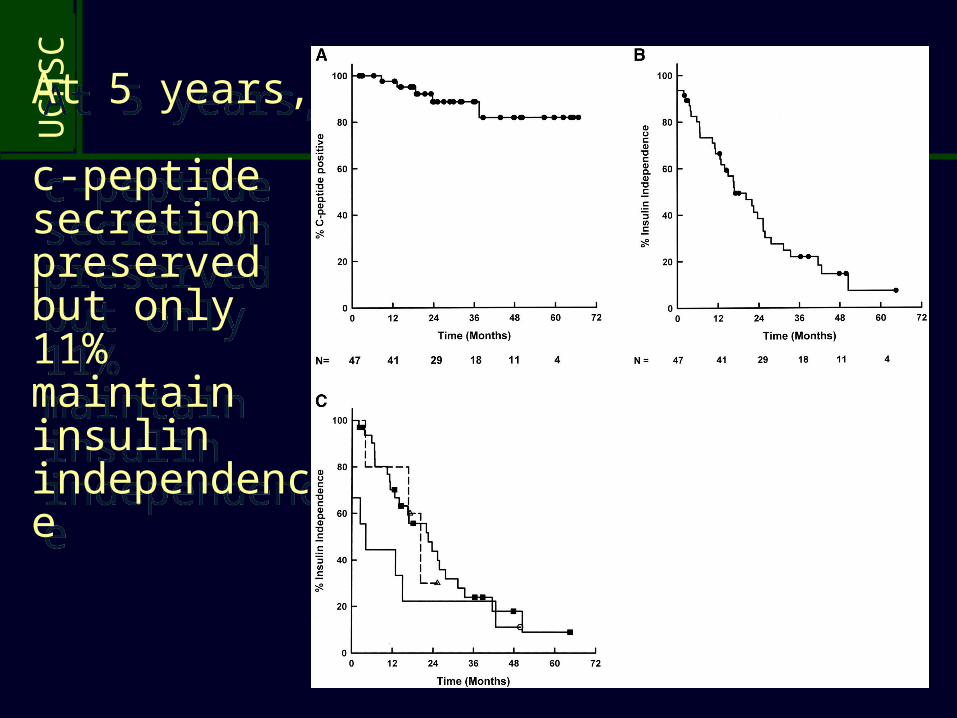
CThe Edmonton Protocol: update and follow-upThe Edmonton Protocol: update and follow-up
65 patients treated with islet transplantation: 44 completed therapy (defined by insulin independence) Median duration of insulin independence =15 months Mean islets transplanted=799,912
128 procedures: Bleeding in 15, portal vein thrombosis in 5 2+ antihypertensive meds in 42% (6% at entry) Statin use 83% (23% at entry)
Ryan EA, et al, Diabetes 2005; 54:2060
UC
HS
C
At 5 years, c-peptide secretion preserved but only 11% maintain insulin independence
At 5 years, c-peptide secretion preserved but only 11% maintain insulin independence
UC
HS
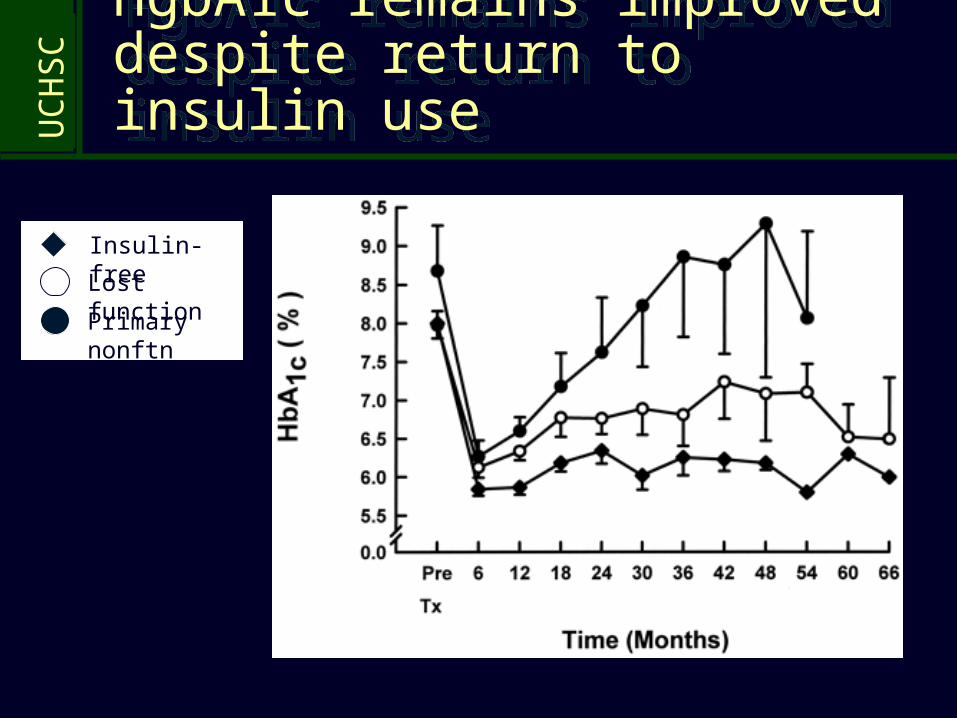
CHgbA1c remains improved despite return to insulin useHgbA1c remains improved despite return to insulin use
Insulin-free
Lost function
Primary nonftn
UC
HS
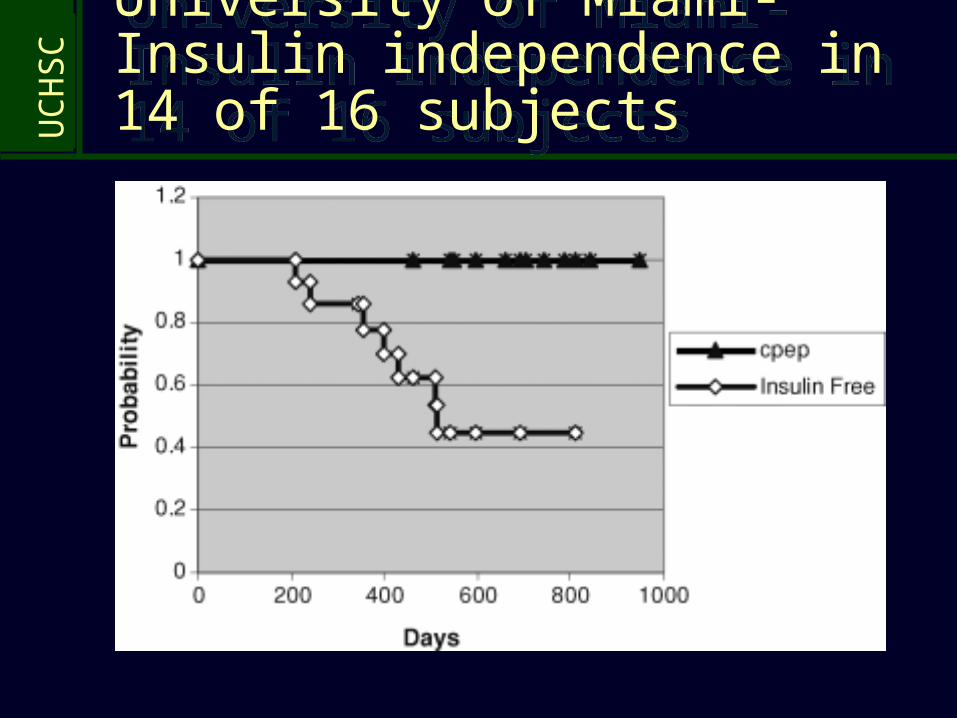
CUniversity of Miami-Insulin independence in 14 of 16 subjects
University of Miami-Insulin independence in 14 of 16 subjects
UC
HS
C
Copyright restrictions may apply.
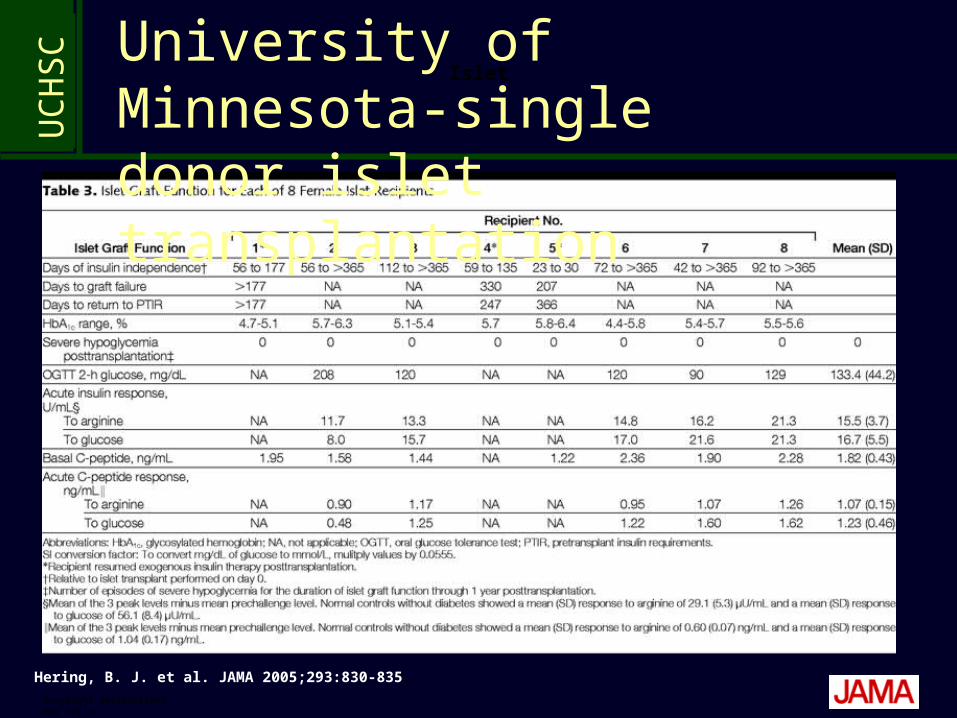
Hering, B. J. et al. JAMA 2005;293:830-835.
IsletUniversity of Minnesota-single donor islet transplantation
UC
HS
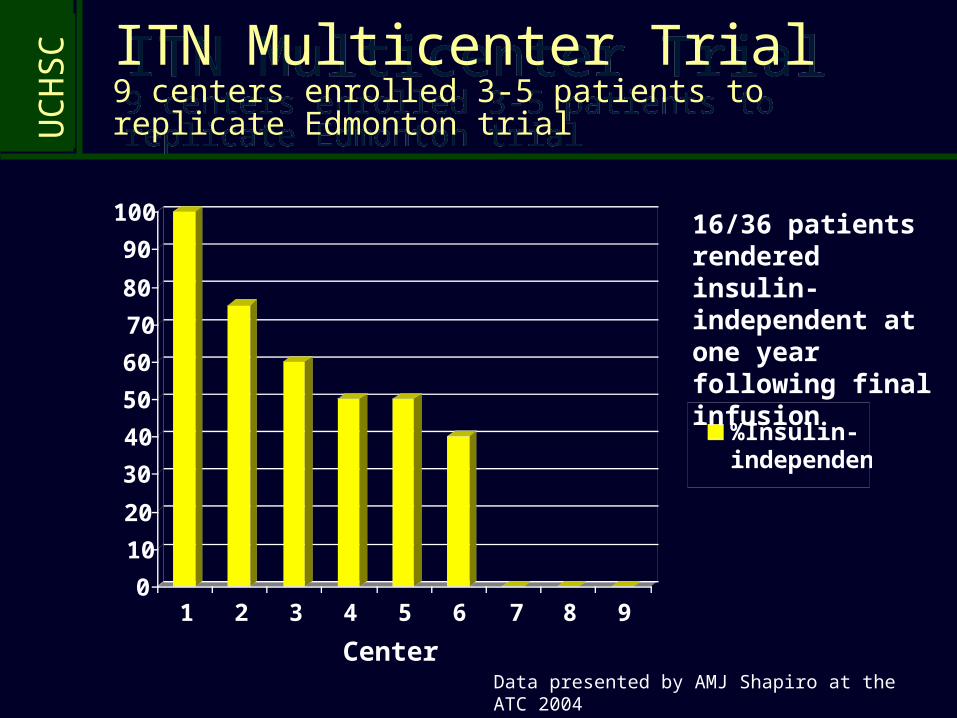
C ITN Multicenter Trial9 centers enrolled 3-5 patients to replicate Edmonton trial
ITN Multicenter Trial9 centers enrolled 3-5 patients to replicate Edmonton trial
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 8 9
%Insulin-independent
16/36 patients rendered insulin-independent at one year following final infusion
Data presented by AMJ Shapiro at the ATC 2004
Center
UC
HS
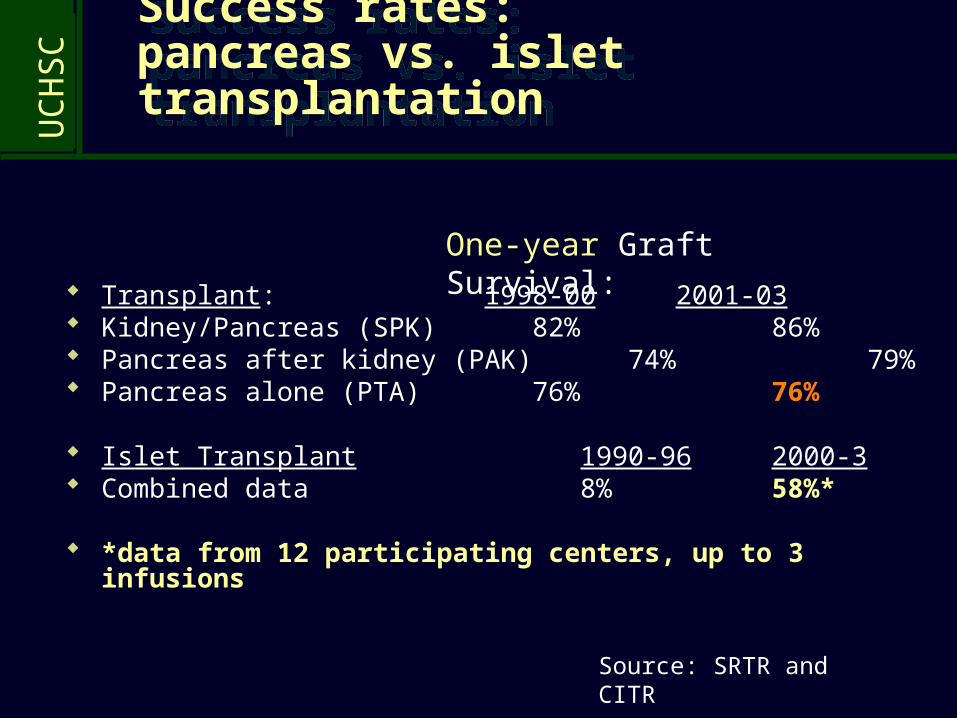
C Success rates: pancreas vs. islet transplantation
Success rates: pancreas vs. islet transplantation
Transplant: 1998-00 2001-03 Kidney/Pancreas (SPK) 82% 86% Pancreas after kidney (PAK) 74% 79% Pancreas alone (PTA) 76% 76%
Islet Transplant 1990-96 2000-3 Combined data 8% 58%*
*data from 12 participating centers, up to 3 infusions
One-year Graft Survival:
Source: SRTR and CITR
UC
HS
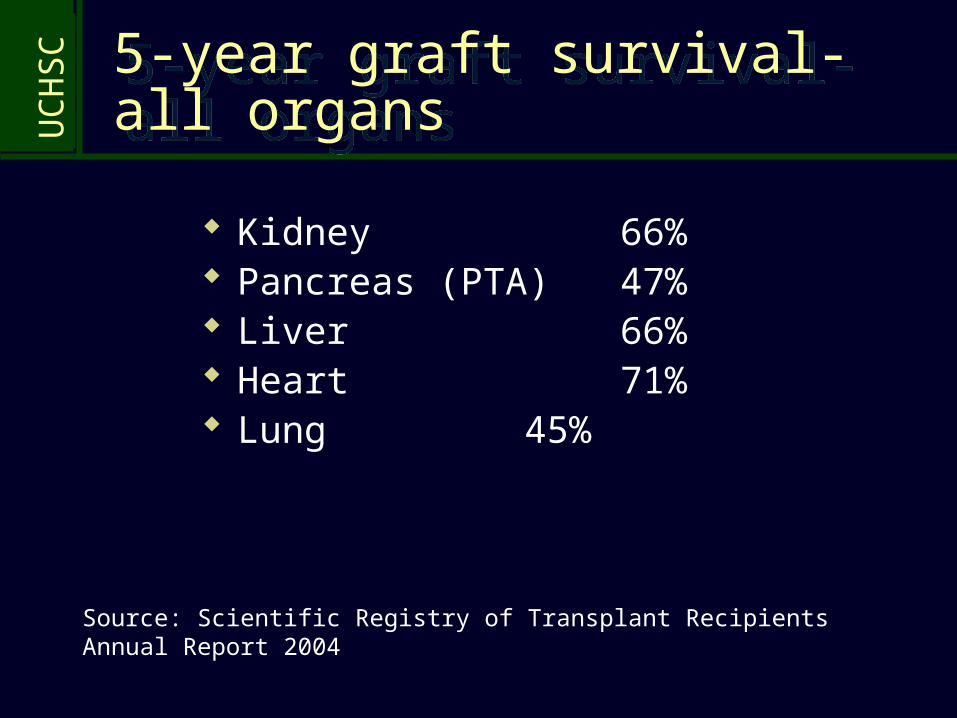
C5-year graft survival-all organs5-year graft survival-all organs
Kidney 66% Pancreas (PTA) 47% Liver 66% Heart 71% Lung 45%
Source: Scientific Registry of Transplant Recipients Annual Report 2004
UC
HS
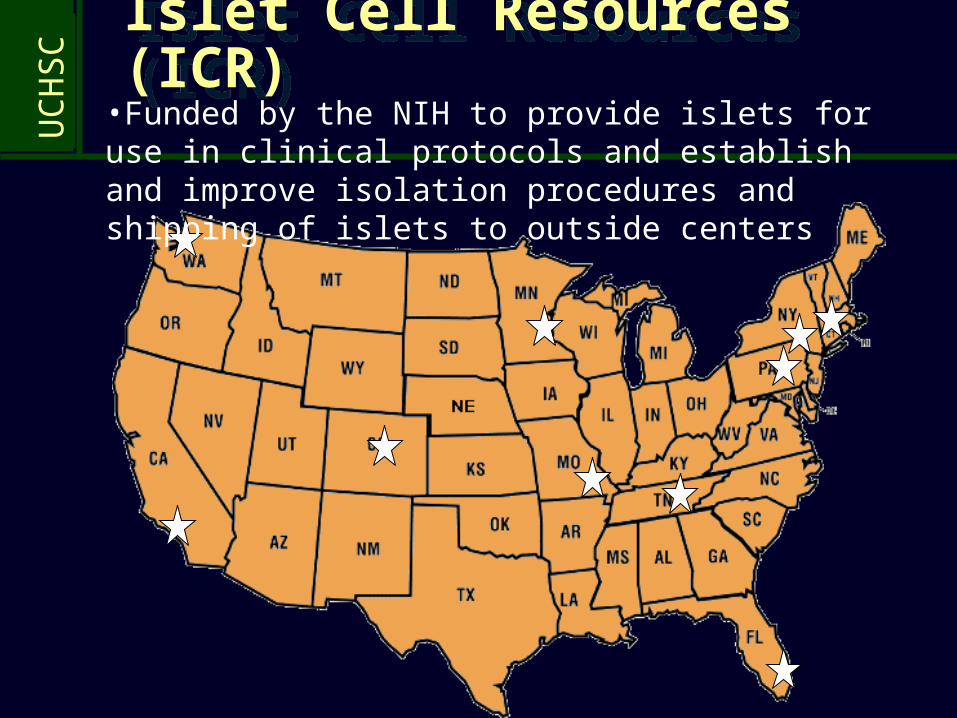
C Islet Cell Resources (ICR)Islet Cell Resources (ICR)
•Funded by the NIH to provide islets for use in clinical protocols and establish and improve isolation procedures and shipping of islets to outside centers
UC
HS
C Components of an Islet Transplant ProgramComponents of an Islet Transplant Program
Laboratory: cleanroom specifications, technical support (4-5 on call at all times), in-process environmental monitoring, post-isolation quality control testing
Clinical: recipient eval and post-transplant follow-up, OPO training/cooperation for organ allocation, transplant procedural coverage, inpatient care,immune/metabolic monitoring
Regulatory: IND for cellular therapy with FDA, annual reports to FDA and NIH, standard operating procedures for islet isolation/transplant, training documentation and equipment validation, UNOS certification and reporting, CITR reporting, DSMB reporting
Finance: NIH, UCH, GCRC, UCHSC, Barbara Davis Center
UC
HS
C
UC
HS
C
UC
HS
C
UC
HS
C
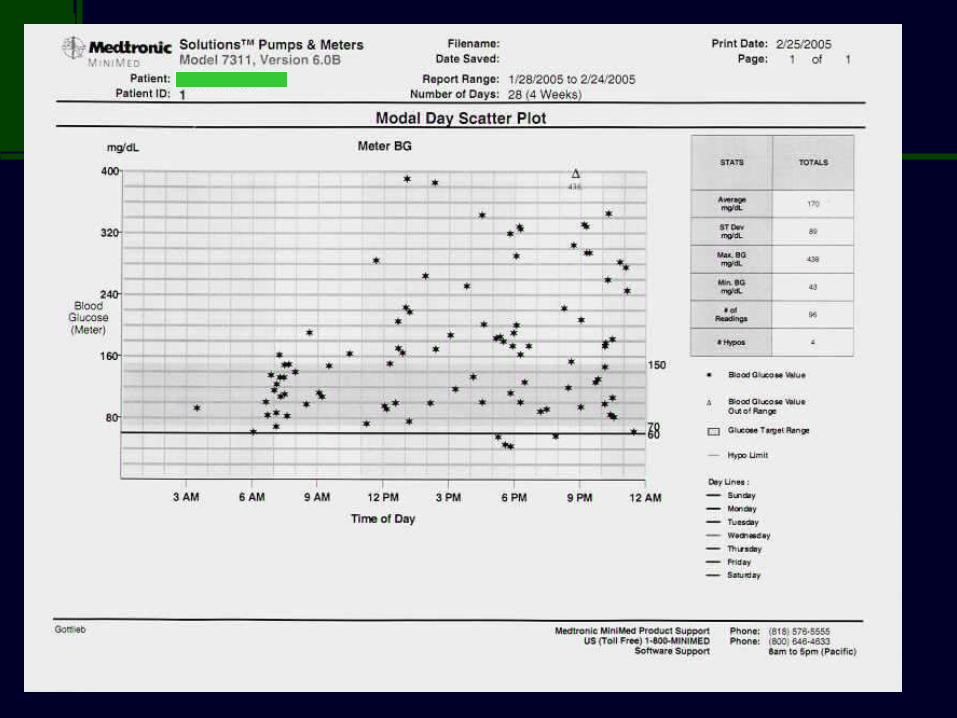
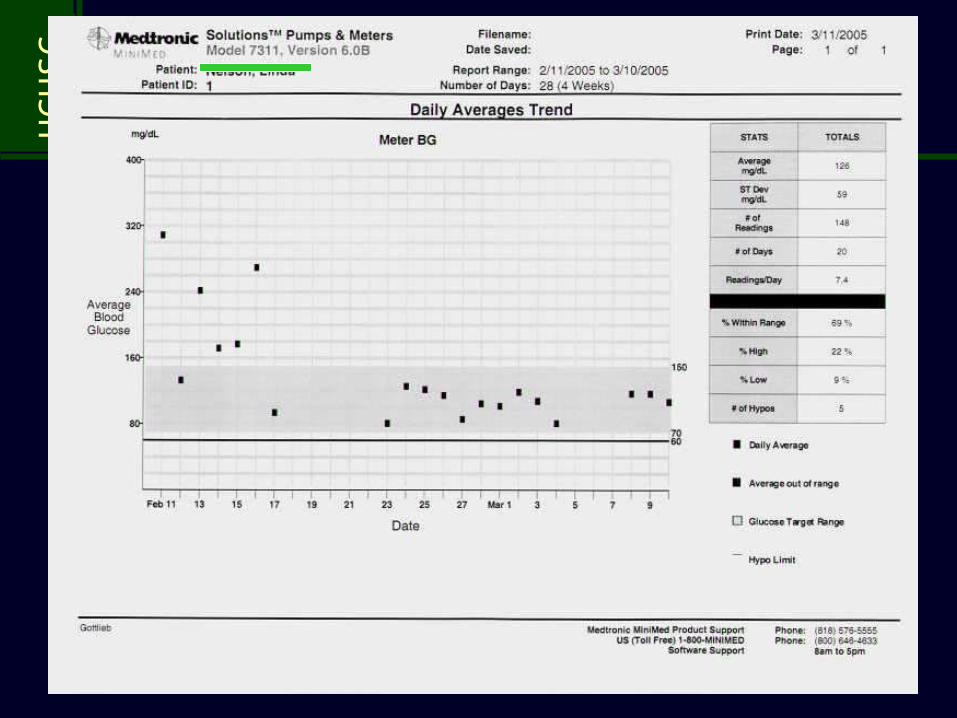
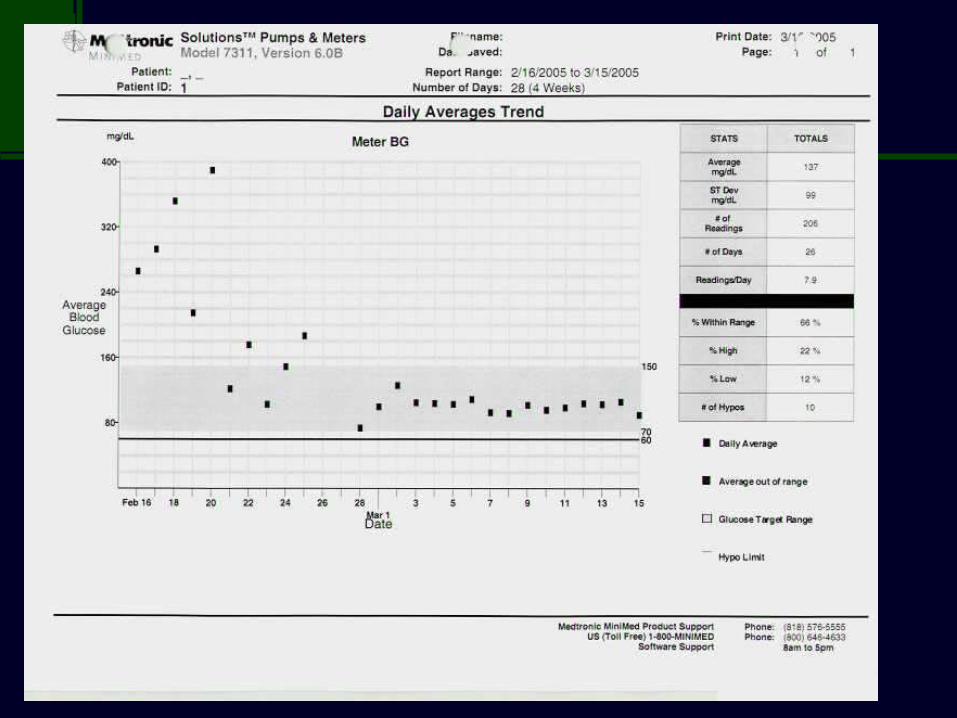
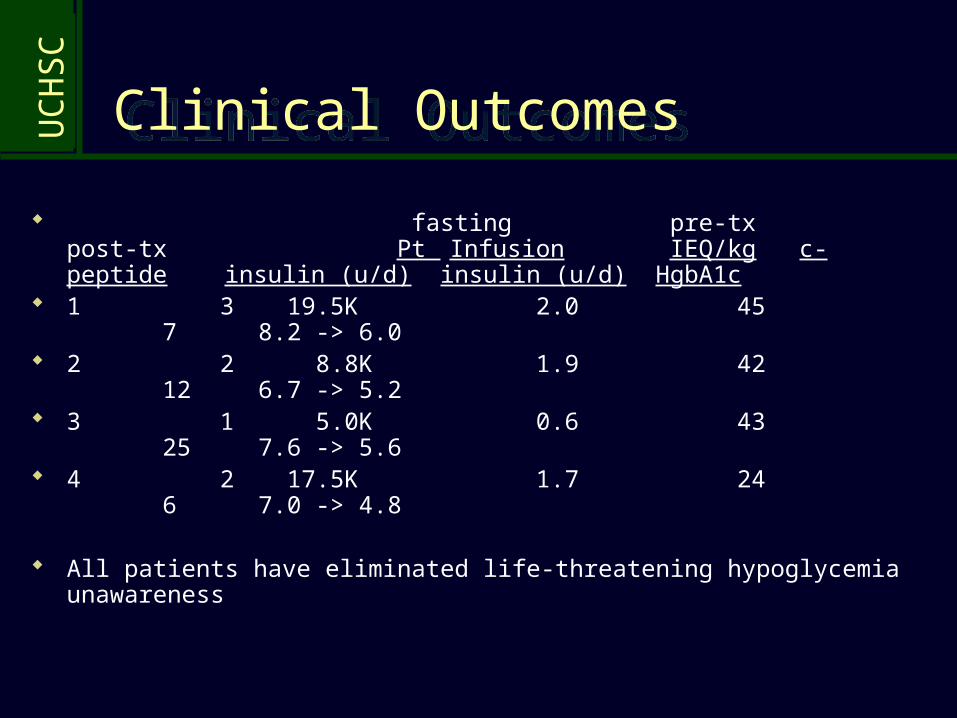
Clinical OutcomesClinical Outcomes
fasting pre-tx post-tx Pt Infusion IEQ/kg c-peptide insulin (u/d) insulin (u/d) HgbA1c
1 3 19.5K 2.0 45 7 8.2 -> 6.0
2 2 8.8K 1.9 42 12 6.7 -> 5.2
3 1 5.0K 0.6 43 25 7.6 -> 5.6
4 2 17.5K 1.7 24 6 7.0 -> 4.8
All patients have eliminated life-threatening hypoglycemia unawareness
UC
HS
C
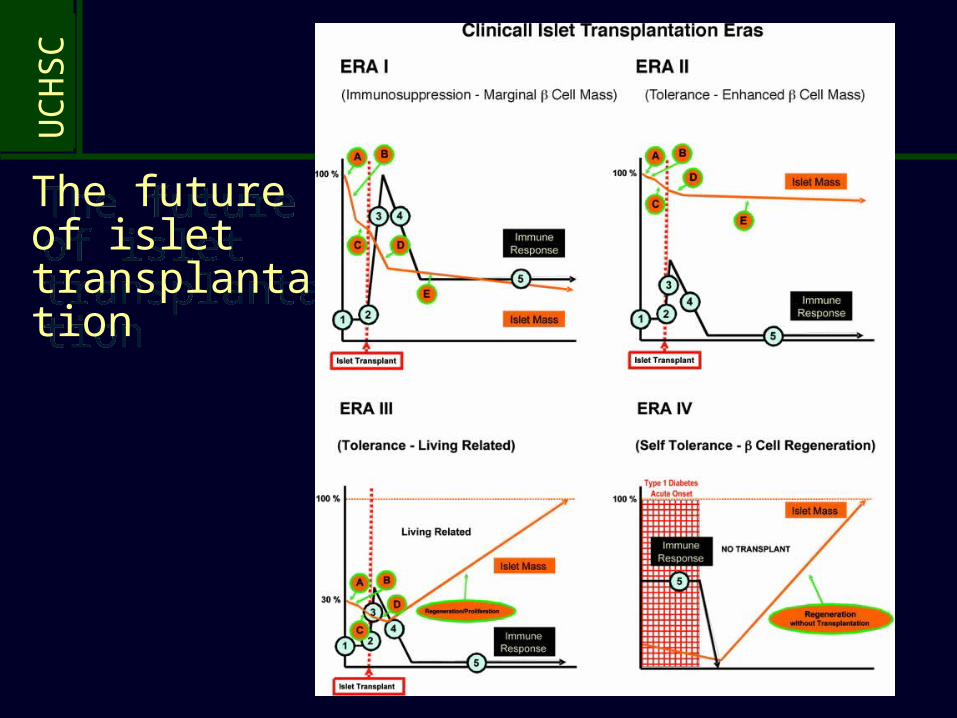
The future of islet transplantation
The future of islet transplantation
UC
HS
C
IsletsIslets
Possible Reasons for Islet Graft Failure
Allograft rejectionAllograft rejectionDisease recurrenceDisease recurrence
Insufficient islet massInsufficient islet mass Poor quality of isletsPoor quality of islets
Toxicity of anti-Toxicity of anti-rejection drugsrejection drugs
Failure to engraftFailure to engraft
Insulin resistanceInsulin resistance
UC
HS
C OBSTACLES TO SUCCESSFUL ISLET TRANSPLANTATION: Low engraftment of islets
OBSTACLES TO SUCCESSFUL ISLET TRANSPLANTATION: Low engraftment of islets
The transplanted cell mass is ~50% of the mass present in a normal individual
The engrafted cell mass is ~30% of the transplanted cell mass
Islet engraftment takes weeks before revascularization is completed, rendering islets susceptible to:
• Hypoxic injury• Nonspecific cell-mediated injury: “IBMIR”,
cytokine release, reactive oxygen intermediates elaborated during postoperative healing/wound reaction
UC
HS
C
Is islet transplantation safe? Is islet transplantation safe? Acute complications: Bleeding ~10-
15% Thrombosis ~5% Transaminitis~50%
Long-term complications: Renal function Hypertension Hyperlipidemia Mouth ulcers Risk of sensitization Risk of infection (CMV)
UC
HS
CIs islet transplantation safe?SAE Report CITR June 2005 Is islet transplantation safe?SAE Report CITR June 2005
150 participants: N=98 no SAE N=25 1 N=16 2 N=6 3 N=4 4 N=2 >4
52 pts had 102 SAE’s N=22 life-threatening N=61 hospitalization N=18 prolonged hosp stay
Most common SAE types: N=26 GI
disorder N=17 Blood/
lymph N=11 Infection
UC
HS
C
Adverse events:Adverse events: Patient 1: mouth ulcers, diarrhea, depression
Patient 2: mouth ulcers, abd pain (SAE), hyperlipidemia, neutropenia, life-
threatening clostridia septicum infection (withdrawl from trial)
Patient 3: mouth ulcers, abd pain (SAE), hyperlipidemia, rash
Patient 4: mouth ulcers, hypertension, liver hemorrhage (SAE), Cr 1.2 to
1.4 (off tacrolimus)
UC
HS
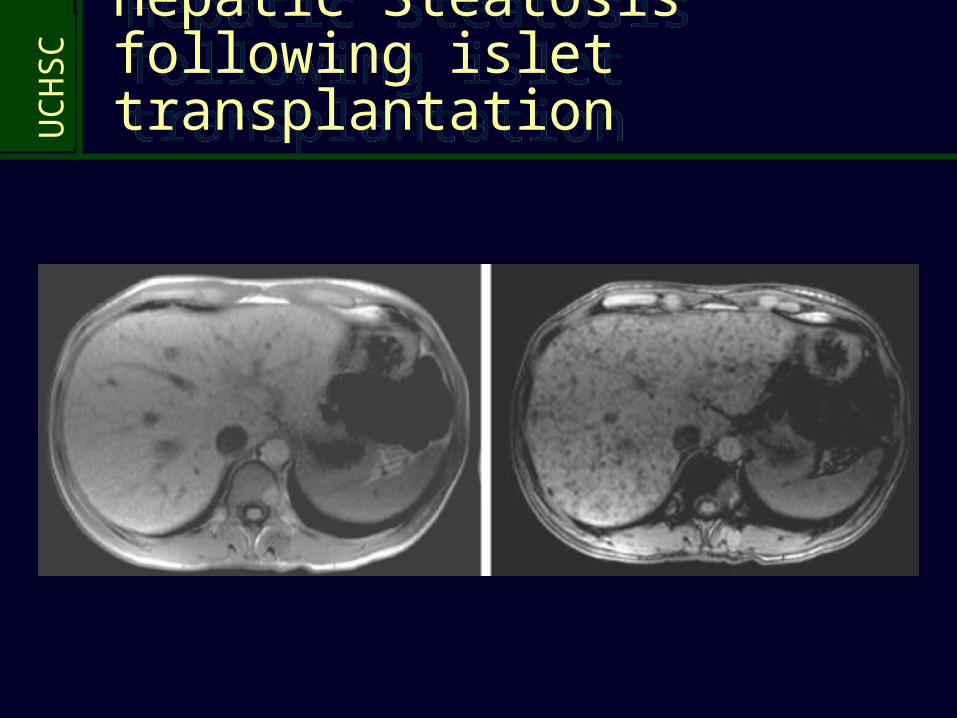
CHepatic Steatosis following islet transplantationHepatic Steatosis following islet transplantation
UC
HS
C In an era of scarce resources, should one patient population receive special consideration?
In an era of scarce resources, should one patient population receive special consideration?
Type 1 diabetic patients with life-threatening hypoglycemia?• Pro: Normoglycemia may be life-saving• Con: Immunosuppression risk/side effects
Diabetic patients with renal failure?• Pro: Immunosuppression not a factor• Con: Benefit of normoglycemia may not significantly impact
survival
Diabetic patients with early signs of organ damage? • Pro: Early intervention may prevent costly, life threatening
complications• Con: Enormous patient population
UC
HS
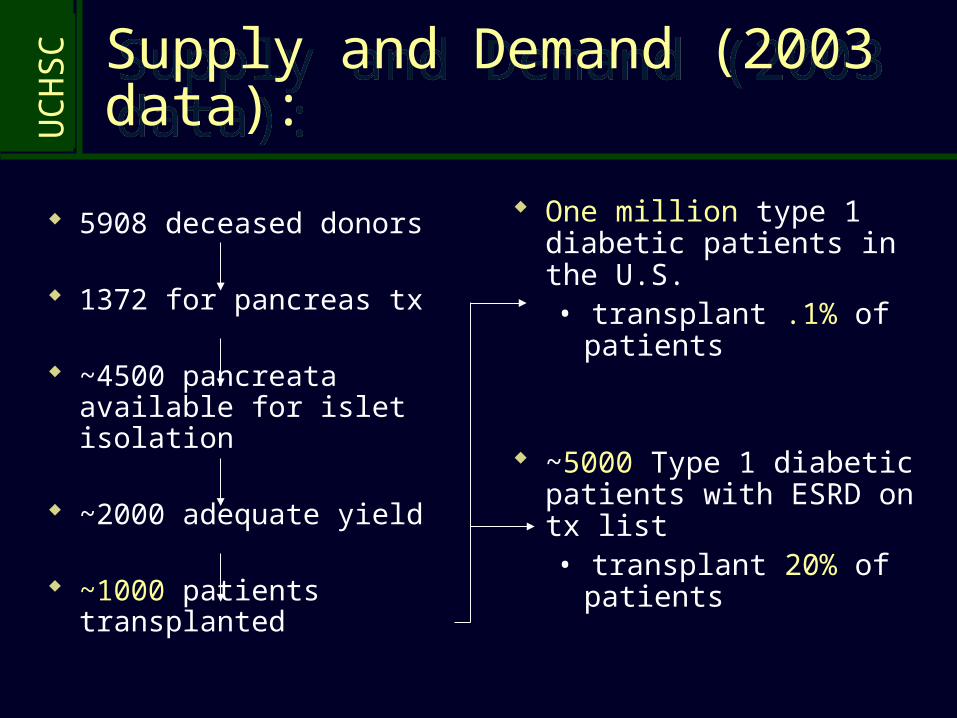
CSupply and Demand (2003 data): Supply and Demand (2003 data):
5908 deceased donors
1372 for pancreas tx
~4500 pancreata available for islet isolation
~2000 adequate yield
~1000 patients transplanted
One million type 1 diabetic patients in the U.S.• transplant .1% of patients
~5000 Type 1 diabetic patients with ESRD on tx list• transplant 20% of
patients
UC
HS
C
CONCLUSIONS:CONCLUSIONS:
Successful islet cell transplantation is now possible • Less invasive but less durable than pancreas transplants• Innovations in inhibiting early inflammation, reducing toxicity of
meds needed
Kidney transplantation is of paramount importance in the patient with diabetes and renal failure• Early referral (GFR 20-30 ml/min)• Evaluation of living donors
Organ allocation, patient selection, and payment for islet transplantation will remain controversial topics during the “growth” phase of development of islet transplant programs

























![[OS 202C] 20120102 Pancreatic Islet Physiology (Insulin)](https://img.pdfslide.net/doc/110x75/577cd5451a28ab9e789a55e6/os-202c-20120102-pancreatic-islet-physiology-insulin.jpg)



