Embed Size (px)
Citation preview

2/15/2018
New Directions in Movement DisordersCaroline Tanner, MD, PHD
Jill Ostrem, MD
UCSF Movement Disorder and Neuromodulation CenterRecent Advances in Neurology 2018
UCSF Weill Institute of
Neurosciences
UCSF Movement Disorders
NeurosurgeryPhilip Starr, MD, PhDPaul S. Larson, MDEdward F. Chang, MDDaniel Lim, MD, PhDKrzysztof Bankiewicz, MD, PhDCoralie De Hemptinne, PhDWhitney Chen, PhDDoris Wang, MD, PhD
NeuropsychologyCaroline Racine Belkoura, PhD
NursingMonica Volz, FNP, MSKaren Merchant, MSNSusan Heath, MS, RNGina Bringas-Cinco, RNAnnie Li Wong, NP
NeurologyJill Ostrem, MDNicholas Galifianakis, MDCaroline Tanner, MD, PhDMarta San Luciano, MDMaya Katz, MDIan Bledsoe, MD,MSJames Maas, MD, PHDChadwick Christine, MDMichael Aminoff, MDRobert Edwards, MDKen Nakamura, MD, PhDAlexandra Nelson, MD, PhDMichael Geschwind, MDAmy Viehoever, MD, PhDNijee Luthra, MD, PhDCameron Dietiker, MD
FellowsJessica Weinstein, MDKyle Mitchell, MDJennifer Choi, MDEthan Brown, MDMitra Afshari, MDMelissa Heiry, MDIdit Tamir, MD, PhD
Research /Support StaffSarah Wang, PhDKristen Dodenhoff, BAFarah KauserJoncarmen MergenthalerJanet AllenShatara BlackmonYasmeen GonzalezJeverly CalaunanKathleen Comyns, MPHSamantha Betheil, BACheryl Meng, MPH Danilo RomeroKanchi Mehta
PsychiatryAndrea Seritan, MD
Social WorkMonica Eisenhardt, LCSW
ChaplinJudith Long
Physical TherapyNancy Byl, PT, PhDHeather Bhide, PT
Disclosures
Caroline Tanner, MD, PHD• An employee of the San Francisco Veterans Affairs Medical Center and the University
of California – San Francisco. • Receives grants: the Michael J. Fox Foundation, the Parkinson’s Disease Foundation,
the Department of Defense, BioElectron, Roche/Genentech and the National Institutes of Health,
• Compensation for serving on Data Monitoring Committees: Biotie Therapeutics, Voyager Therapeutics and Intec Pharma
• Personal fees for consulting: Neurocrine Biosciences, Adamas Therapeutics, PhotoPharmics , 23andMe and Alexza
Jill Ostrem, MD• Consultant and speaker: Allergan Inc., Medtronic Inc.• Educational grant support: Medtronic Inc, Allergan Inc, AbbVie Inc, Boston Scientific
Inc.• Clinical trial support: Ceregene Inc., St. Jude Medical, Inc, Boston Scientific Inc, Cala
Health Inc, Google Inc
New Direction #1
• Parkinson’s Disease is not one disease and will be better managed with an individual treatment approach

2/15/2018
5
One Disease or Many? PD Subtypes
jamanetwork.com
PD Genetics
Genetic influence increasingly recognizedMonogenic forms (Mendelian inheritance)= mutation in single gene sufficient to cause PD
30% of all familial cases~5% of sporadic cases
Six regions contain genes that conclusively cause PD
The cause of PD is multifactorial• Several genes• Modifying effects of susceptibility factors• Environmental exposures• Gene-environment interactions
7
Penetrance/Effect Size
Age at onset of PDYoung-onset Late-onset
LRRK2SNCAVPS35
15-50%
~5%ParkinDJ-1 PINK1SNCA
PD Genet ics– Targeted Therapies
Gene Mutations Protein/Enzyme Function Age at onset
Phenotype Pathology
Dominantly inherited last-onset PD
SNCA Missense Alpha synuclein- structural brain protein
60 yr(30-80)
Levodopa responsive Diffuse lewy bodies
SNCA Locus duplication (and triplication)
31-71 yr Levodopa responsive, younger age, rapid progression, autonomic dysfunction, dementia, wide spread Lewy Bodies
Diffuse lewy bodies, prominent nigral and hippocampal loss
LRRK2 Missense: Arg1441Cys/Gyl/His; Try1688Cys, Gly2019Ser, IIe2020ThrPolymorphisms, protective haplotypes
Leucine-rich repeat kinase 2- enzyme when mutated causes Lewy-body phenotype –increased kinase activity
60 yrs(32-79)
Levodopa responsive, Like sporadic PD, slow progression, abduction-addition lower limb tremor, little dementia
Brain Stem LB, neurofibrillary tangle or TDP-43 pathology and/or nigral neuronal loss
VPS35 Missense: ASP620Asn 53 yrs(40-68)
Levodopa responsive tremor-dominant, dyskinesia and dystonia, occasionally dementia
Inconclusive- ? No LB
Juvenile and early-onset recessively inherited PD
PARK2 Numerous missence, exon deletion and duplication mutations
Parkin- a ubiquitin-protein ligase involved in protein degradation
<45yr (12-58)
Levodopa responsive, early dystonia, slow progression, hyperreflexia, dyskinesia, early gait and balance issues, less non-motor
Predominantly nigralneuronal lossOccasionally with synucleinor tau pathology
PINK1 Misssence: manyRare: locus and exon deletion
PTEN-induces putative kinase
<45yr (18-56)
Levodopa responsive, akinetic/ridgid postural instability, gait, slow progression, sleep benefit
One case with lewy bodies
DJ-1 Misense: Glu163lys, Leu166Pro Exon 1-5 deletion, g.168-185 dup
Positive regulator of androgen- receptor dependent transcription
<40 yr(24-39)
Like PINK-1, rare Unknown

2/15/2018
PD Mechanisms of Disease
Protein trafficking
• ubiquitin/protease system
• alpha-synuclein
Calcium-channel
• apoptosis
Inflammation
Oxidative stress
Mitochondrial dysfunction
Trinh J and Farrer M Nature Review, 2013.
LRRK2 Mutation
Phenotype• Like sporadic PD (later onset)• Variable clinical and pathological
phenotype• Levodopa responsive• Slow progression• Abduction-addition lower limb
tremor• Little dementia Video Courtesy of Dr. San Luciano and Darel Ogbonna
• Mutation in the leucine rich repeat kinase 2 (LRRK2) gene (G2019S) is the greatest known genetic cause of PD
• Most common monogenic cause of PD in Europe and North America• 30% penetrance• Mutations seem to heighten the activity of LRRK2 kinase
LRRK2 Treatment Approaches
LRRK2 based treatment• Inhibitors of LRRK2 kinase activity could potentially be used to
prevent or treat PD
Denali Therapeutics • Completed phase I study in control volunteers in 12/2017. • Reported 90% inhibition of LRRK2 activity (target engagement)• Well tolerated • Also testing a second compound in Phase I study. • Likely these drugs will move into phase II trial in LRRK2 PD
patients next.
PD and GBA Mutation
GBA mutations cause dysfunction in the glucocerebrosidase (Gcase) protein- leading to build-up of alpha-synuclein
More common in Ashkenazi Jewish descent /Gaucher or relative with Gaucher (lipids build up and enlarge organs)
5-10 % of PD patients carry this mutationGBA mutation - 20X increased risk of PDGBA mutations are common but overall chance of PD is still low
Phenotype• Slightly earlier age of onset• Initial symptom often
bradykinesia• More rapid motor disease
progression, more dyskinesia• More cognitive dysfunction• Less tremor• More depression
Video Courtesy of Dr. San Luciano and Darel Ogbonna

2/15/2018
GBA Treatment Approaches
Sanofi / Genzyme• Small molecule (GZ/SAR402671)
Venglustat -targeting cellular dysfunction in PD patients with a GBA mutation (also for Gaucher Type III disease and Fabry disease)
• Glucosylceramide synthesis inhibitor
• Pre-clinical GBS mutation PD models treated with similar compound had fewer alpha-synuclein aggregation and did better on memory tests
• Phase II international trial enrolling PD patients with GBA mutations (N=230)• First industry – sponsored Phase II clinical trial in genetically defined PD
population
Video Courtesy of Dr. Ian BledsoeHeterozygous carrier of N370S mutation
Mitochondrial Dysfunct ion in Genetic PD
• Overwhelming evidence implicates mitochondrial function being compromised in Parkinson’s disease
• Oxidative stress is found in PD tissue
Especially for genetic subtypes:• Parkin• PINK1• DJ-1• LRKK2
• Energy failure leads to neuronal cell death • Nigral dopaminergic neurons seem to be
selectively vulnerable to energy failure • Energy-based therapies have generally failed
in their application in PD
Mitochondrial Based Therapies
Parkin Mutation PD
Parkin- a ubiquitin-protein ligase involved in protein degradation Numerous missense, exon deletion and duplication mutations, No LB?
Phenotype:Levodopa responsive, dystonia, akinetic/ridged, postural instability, gait, slow progression, sleep benefit
Video Courtesy of Dr. Nick Galifianakis
DJ-1: Mitochondrial regulation, antioxidative stress, chaperonePARKIN: Mitochondrial autophagy, ubiquitin-protease systemPINK1: Mitochondrial serine/threonine-protein kinase, protects against mitochondrial dysregulationLRRK2: modulates mitochondrial dynamics and function
A Phase 2A Safety and Biomarker Study of EPI-589 in Mitochondrial Subtype and Idiopathic Parkinson’s Disease Subjects
Caldwell, 2008
Bioelectron – EPI-589
Phenotype:• (R)-troloxamide quinone (EPI-589) is a vitamin E
derivative and ORALLY available drug
• Aids in the catalysis of glutathione, an important antioxidant that aids in reducing oxidative stress
• Glutathione depletion has been linked to mitochondrial dysfunction
• Being developed for treatment of neurological diseases characterized by high levels of oxidative stress and mitochondrial pathology (i.e. ALS, PD, HD, mitochondrial diseases)
• Focus on safety and quantifying glutathione cycle biomarkers
2/15/2018
New Direction #2
• Newer formulations of carbidopa/levodopa are on the market or in development
Levodopa
• Most effective and widely used treatment in PD• Dopa decarboxylase (carbidopa) inhibits peripheral LD
metabolism- more levodopa CNS availability (improves tolerability reducing nausea)
• Early PD simple dosing schedules, becomes more complex in advanced PD
• Short half-life (1.5 hours)• As PD progresses, conversion of LD to dopamine,
storage, release, becomes unpredictable• Intermittent/pulsatile release of dopamine in the
striatum, produces changes in the postsynaptic receptors leading to motor complications and dyskinesia (70% after 5 years)
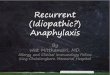
Motor Fluctuations
Typical Clinical Pattern of Wearing Off
Adapted from Hauser RA. Geriatrics. 2006;61:14-20.
Sym
pto
ms
no
t a
de
qu
ate
ly c
on
tro
lled
(“
off
time
”)
Sym
pto
ms
ad
eq
ua
tely
co
ntr
olle
d
(“o
n t
ime
”)
PD Medication PD Medication PD Medication
“Wearing off” period
Time
Ex tended Release Carb idopa /Levodopa
(Rytar y- IPX066) ( Im pax)
• New oral formulation of CD-LD (contains both IR and CR levodopa)
• Each Rytary capsule contains CD-LD (1:4) microbeads designed to dissolve at various rates allowing for release and absorption of LD over a longer timeframe

2/15/2018
Conversion to Rytary Carbidopa/Levodopa Entera l Suspens ionDuopa (AbbVie)
• Continuous intraintestinal infusion of C/L gel• Programmable pump to adjust dose • Prospective, double-blind, double dummy, double
titration study showed reduction in off time without increase in dyskinesia
• High complication rate, Costly
Practical Considerations
Dose titration: • Outpatient, but at least ½ day in office to initiate• Calculate based on current c\l dose• Infusion usually 16 hours • Morning dose a bolus • Continuous dose thereafter with option for extra doses
Return in one week for re-adjustment of doseMonitor B12, B6 (peripheral neuropathy)
• Costs: Est.~ $6000/month• Patient and caregiver understanding key to
success• Care of site• Handling of cassette• Pump program can be fixed or adjustable• Adjustable often better efficacy(Medical Letter 2015)
PD Drugs in Development
New Drug:Other LEVODOPA Formulations
• CVT-301 (Acorda)• Accordion Pill (Intec Pharma)• Dopafuse (SynAgile)• ND0612L “Pump Patch”
(Neuroderm)
Neuroprotective agents?• Inosine• Isradipine• Nicotine• NAC• Nilotinib• Monoclonal antibodies to
misfolded alpha-synulean• Affitope PD01A vaccine
Other DOPAMINE AGONISTS
• Apomorphine infusion (Ago-Go)
• Apomorphine sublingual film (APL-130277) (Sunovion)
Others• ADX48621-201 (Dipraglurant-IR) (Addex
Therapeutics)• AVP-923 (dextromethorphan/quinidine)
(Avanir Pharmaceuticals)• Eltoprazine (Amarantus Bioscience)• AQW051 (alpha7 nicotinic receptor)
(Novartis)• Nicotinic receptor agonists in PD
(AstraZeneca)• Preclinical stage of development• Candidate drug is already tested for
safety and tolerability in humans

2/15/2018
Carbidopa /Levodopa Inhaled Formulat ion
CVT-301 (AcordaTherapeut ics )
• Inhaled formulation of levodopa• Developed for rapid/reliable relief from debilitating off periods• Fine powder delivered via a small, plastic inhaler similar to an asthma
inhaler • Phase III showed safety and efficacy to improve motor function in PD
experiencing OFF periods• Filed new drug application with FDA 2017
• New levodopa formulation which surface area expands over time in the stomach to achieve longer half-life
• Used biodegradable polymeric films• Allows for maximum absorption before leaving
the stomach• Promising Phase II study results• Phase II study enrolled and study to be
completed in 2018
C a r b i d o p a / L ev o d o p a G a s t r o R et e n t iv e F o r mu l a t i o nA c c o r d i o n P i l l ( I n t ec P h a r ma d e l i ve r y s y s t em )
Cont inuous Ora l Carb idopa Levodopa
DopaFuse / OroFuse (SynAgi le )
• Continuous delivery of carbidopa/levopdopa via the mouth
• Device that uses a customized reusable retainer fitted to the top of the mouth/teeth with a miniature disposable propellant-driven drug pump
• Fresh drug pump each week –remove to eat
• Phase IIa study showed improved “off” time compared to regular C/L*
Stocchi F, et al. Abstract Movement Disorders Congress 2016
L i q u i d L e v o d o p a
S u b c u t a n e o u s C o n t i n u o u s D e l i v e r y ( N e u r o d e r m )
“ P u m p - p a t c h ” ( N D 0 6 1 2 L , N D 0 6 1 2 H , N D 0 6 0 8 0 )
• Levodopa/carbidopa formulation continuously administered subcutaneously “Pump-patch”
• May reduce or prevent motor complications• Small device (as big as a credit card) made up of a drug reservoir and a series of
micro-needles (painless) pump the therapy under the skin and into the blood stream
• Phase II study- Significant reduction on off time and well tolerated*• Phase III study planned
* Olanow W, et al. Abstract Movement Disorders Congress 2017

2/15/2018
Am antad ine ER
Gocovr i (Adam as)
• FDA approved for levodopa induced dyskinesia (first drug)
• Also some reduction in off time• Special concentration profile with time: initial
slow rise overnight, highest concentration achieved in the morning and daytime when most useful
• Once-a-day dosing, 137mg QHS for one week then increase to 274mg QHS
• SE: Hallucinations/ Peripheral Edema
Oertel et al Movement Disorders, 2017.
New Direction #3
• The field of DBS is about to get more complicated!
Historical DBS Considerations – Medtronic Devices
Vim Thalamus Subthalamic Nucleus Globus Pallidus
Single Channel Dual Channel•Which device?
•Which location?
St Jude Medical/AbbottInfinity DBS Systemnow FDA approved
• FDA approved 2016 for PD and ET• Constant current device• BluetoothTM wireless communication• Upgradeable software option• Bilateral frequency control • Communicates with Apple digital devices
(iPad mini/iPod touch)• Directional lead to allow for current
“steering”• Not MRI compatible• Non-rechargable

2/15/2018
Boston Scientific Vercise™ DBS System now FDA approved
• Soon to have Non-rechargeable and rechargeable neurostimulators• Tablet based programmer• Current steering and 8 electrode DBS leads• Directional leads• Fractional current delivery• Not MRI Compatible- may change soon?
New DBS directional leads
Traditional Medtronic Lead(Four concentric ring electrodes)
Two concentric ring electrodes (outer) Six non-concentric directional electrodes (middle)
New leads
New software to localization and visualize shape of electrical stimulation field
• Computational modeling / volume of tissue activation (VTA) and individualized direct programming
35
New Direction #4
• Therapeutics for PD directly target pathological alpha synuclein are now in clinical trails

2/15/2018
Immunotherapeutic Approach in PD-Anti Alpha-Synuclein
Prevent and promote the clearance of misfolded alpha-synuclein targeting the underlying disease mechanism and slow and ultimately halt the disease process.
Monoclonal Antibody Infusion against alpha-synuclein -blocks cell to cell transmission by blocking uptake of misfolded endogenous alpha synuclein
Roche – PRX002A Phase 2 Study of Anti-α-Synuclein Antibody in Early ParkiNson’s DiseAse
• PRX002 is an INFUSION of a humanized monoclonal antibody against an epitope on the C-terminus of human α-synuclein
• Aggregated and phosphorylated α-synuclein is the major component of pathological hallmark lesions in…
- PD: Lewy bodies, Lewy neurites
- MSA: glial cytoplasmic inclusions
• Antibody has a high affinity for pathologic forms of α-synuclein consisting of oligomers and fibrils, ultimately preventing propagation and neuronal cell death
• ENROLLING EARLY-PD PATIENTS (within 2 years from dx, H&Y <= 2, MAO-I-treated only, not anticipated to start a new dopaminergic rxfor 1 year)
Synaptic/Neuronal Loss and Pathological Spread Antibodies
neutralize and clear pathogenic
-synuclein
F. Hoffman-La Roche, Ltd.Aggregated,
extracellular Syn
Biogen – BIIB054
• BIIB054 is an INFUSION of a humanized monoclonal antibody against an epitope on the N-terminus of human α-synuclein
• Antibody has a high affinity for aggregated pathological forms of α-synuclein as well, to ultimately prevent propagation and neuronal cell death
• Adopted by the Parkinson’s Study Group
• ENROLLING EARLY-PD PATIENTS (within 3 years from dx, H&Y <= 2.5, UNTREATED for at least 12 weeks and not anticipated to start a dopaminergic rx for 6 months)
A Phase 2a Study of the Safety, Pharmacokinetics, and Pharmacodynamics of BIIB054 in Subjects with Parkinson’s Disease
Immunotherapeutic Approach in PD-Anti Alpha-Synuclein
Vaccine development against alpha-synuclein• AFFiRiS First in human trial to assess the safety and tolerability
(Europe) - Phase IA study showed positive safety and toxicity profile (N=32)
• Multiple (4) subcutaneous vaccinations with two doses were tested/ Patients developed intended alpha-synuclein- antibodies
• Multiple phase Ib trials ongoing/ Randomized to low or high booster immunizations
Preventing Toxic Protein Aggregation• Neuropore/UCB – NPT200-11 – Binds to alpha-synuclein and blocks
accumulation. Planning Phase Ib study in Europe• Proclara/Neurophage – NPT088 – Binds to alpha-synuclein and
amyloid- beta and tau. ALZ 1st and next would be PD

2/15/2018
New Direction #5
• Evaluate for Falls in PD. Very common and multifactorial in many patients.
Falls in the Elderly
Simon Fraser University Video Footage of Fallshttps://www.youtube.com/watch?v=Z3e1Xvnj8Wo
PD Postural Instabil ityConsequences of Falls
Falls Fractures• Reduced mobility• Prolonged hospital stay• Prolonged recovery after surgical repair• Increased placement outside of home• Increased mortality
Falls Head injuries • Concussion, subdural, etc. CNS injury• Reduced cognitive function, reduced mobility, seizures• Prolonged hospital stay• Increased placement outside of home• Increased mortality

2/15/2018
Osteoporosis & Parkinson’s Disease
Torsney et al, 2012
Prevention Falls Prevention• Environmental modification - remove obstacles,
correct footwear & eyeglasses, improve lighting, etc. • Avoid hypnosedatives• Physical therapy• Tai chi, dance • Monitor & treat Orthostatic Hypotension
Fracture Prevention- Reduce osteoporosis/osteopenia (vit.D, Calcium, bis-
phosphonates) - Reduce falls - “Learn how to fall”
Northera (Droxidopa capsules)• Treatment for neurogenic orthostatic hypotension associated
with PD, MSA, and pure autonomic failure• Converted to norepinephrine and causes vasoconstriction• Recently FDA approved (Chelsea Therapeutics)
• Dose 100mg TID (am, midday, late afternoon, >3hr before bedtime)
• Titrate up by 100mg every other day –max dose 600mg TID
• Box warning for risk of supine hypertension
New Direction #6
• It can be helpful to obtain a DatScan in these clinical situations:

2/15/2018
DatScan Mechanism & Indications
INDICATIONS AND USAGE*DaTscan is a radiopharmaceutical indicated for striatal dopamine transporter visualization using single photon emission computed tomography (SPECT) brain imaging to assist in the evaluation of adult patients with suspected Parkinsonian syndromes (PS).
In these patients, DaTscan may be used to help differentiate essential tremor from tremor due to PS (idiopathic Parkinson’s disease, multiple system atrophy and progressive supranuclear palsy).
DaTscan is an adjunct to other diagnostic evaluations.
*Bajal, 2013; FDA Product Label
Case 1• 68 yr old retired left handed pharmacist • History of GERD with increasing severity in recent months
taking metoclopramide , recently increased from 10 mg. TID to 15 mg. QID with good control of symptoms
• Has noticed sense of muscular stiffness, increased fatigue, occasionally a tremor at rest, affecting both upper extremities, more bothersome on the left side
• Referred to neurologist• Exam: Mild bilateral bradykinesia, intermittent resting tremor
left > right, slightly stooped posture, small steps, reduced arm swing bilaterally
• Gastroenterologist reluctant to discontinue metoclopramide given increased symptoms
• Referred for a SPECT scan
Case 1 SPECT with DatSCAN (123I-Ioflupane)
Normal scan
COMMENT: Metoclopramide blocks striatal dopamine receptors and can produce drug-induced parkinsonism. Symptoms resolve gradually after stopping drug treatment.
Case 2
• 78 year old retired high school English teacher• Brought to office by daughter • Recent history of fearfulness, believing there are intruders
in his home; called exterminator 4 times in 2 months to remove rats; loss of interest in reading, golfing; fell 2 weeks ago
• Lifelong history of “shakiness” on and off throughout adult life, particularly bothersome during public speaking; never treated
• Exam: Oriented to person, 2 years off on date, difficulty copying figures and generating lists of words; Mild postural tremor bilaterally; mild right hand resting tremor, reduced right arm swing, stooped posture, pull test: retropulsion 4-5 steps

2/15/2018
Case 2 SPECT with DaTSCAN (123I-Ioflupane)
Abnormal scan
Diagnostic accuracy of 123I-FP-CIT SPECT in possible dementia with Lewy bodies
O’Brien, British J Psychiatry 2009
• Dopamine transporter imaging can distinguish Dementia with Lewy Bodies from Alzheimer’s Disease: 100% of clinical AD at 12 months had normal scans at baseline
Case 2 Comment:
• 20 patients with a clinical diagnosis of DLB or other dementia & Datscan at diagnosis• Follow-up with detailed neuropathological autopsy• 8 DLB, 9 AD, 3 other diagnoses• Sensitivity initial clinical diagnosis of DLB was 75%, specificity was 42%• DatSCAN sensitivity was 88% and specificity was 100%• Conclusion: FP-CIT SPECT scans substantially enhanced the accuracy of diagnosis of DLB by
comparison with clinical criteria alone
Dementia with Lewy bodies: a comparison of clinical diagnosis, FP-CIT single photon emission computed tomography imaging and autopsy
WalkerJ Neurol Neurosurg Psychiatry 2007
Dopamine Transporter Imaging in Autopsy-Confirmed Parkinson’s Disease and Multiple System Atrophy
Laura D. Perju-Dumbrava, Movement Disorders, 2012
• Abnormal imaging in both PD and MSA
• Asymmetry possibly greater in MSA
• DATSCAN cannot differentiate
Case 3- ET• A 55 year old right handed woman, works as a jewelry artist• Recent sense of slight loss of fine movement dexterity,
especially in right hand • Fatigue and tremor of right hand more than the left hand• Neurologist examination:
– ? right upper extremity rigidity, possible cogwheel phenomenon
– mild bradykinesia throughout– fine tremor in the hands (right>left) – tremor at rest and with posture– normal gait
• Referred to observational trial in early PD • Referred for baseline DatScan

2/15/2018
Case 4 : SPECT with DATscan (123I-Ioflupane)
Normal Scan
New Direction #7
• Toxicant Exposure and Parkinson’s Disease
• Ask about military service!
Vietnam Veteran
Used defoliant agent orange
• 2009: Agent Orange Linked to Parkinson's Diseaseestablished service-connection:
• Certain Vietnam Veterans may be eligible for: disability compensation and health care benefits.
Agent Orange & Parkinson’s Disease Risk
2,4-D 2,4,5-T
2,3,7,8 tetrachlorodibenzodioxin
Operation Ranch Hand: 1962-197120 x 106 gallons Agent Orange

2/15/2018
Camp Lejeune N.C.
Sources of exposure: Drinking water, bathing,Inhalation, swimming, recreation
History:1953-1985 - Water contaminated with TCE & PCE (i.e., PERC) 1980 – Contaminants discovered1987- Wells closed1989 - EPA Superfund
500,000 – 1 million exposedMilitary: Marines, National Guard, reservistsCivilian: Family members, employees
Exposure levels: Est. monthly median (max. mean) ug/L: PCE: 85 (158); TCE: 366 (783)vs. US max. contaminant level: 5 ug/l
Dept. of Veterans Affairs 2017• 30 or more days of service • Entitled to benefits
New Direction #8
• There are new treatments for tardive dyskinesia
• Tardive dyskinesia is an uncontrolled movement that is associated with prolonged use of dopamine receptor blocking agents (DRBAs) for at least a few months
Tardive Dyskinesia Treatment of TD: American Psychiatric Association (APA)
American Psychiatric Association (APA)1
•TD treatment recommendations from Schizophrenia Practice Guideline (last published in 2004):
– Use second-generation antipsychotics due to “decreased risk of extrapyramidal side effects and TD”
– For TD, switch to a second-generation antipsychotic or reduce first-generation dose
– Perform a baseline assessment of abnormal involuntary movements with ongoing monitoring:• First-generation antipsychotics: Every 6
months (3 months for high-risk patients) • Second-generation antipsychotics: Every 12
months (6 months for high-risk patients)
APA Guideline Watch2
•Updated 2009 •No specific TD recommendations•“The distinction between first- and second-generation antipsychotics appears to have limited clinical utility”
1. Lehman AF, et al. Am J Psychiatry. 2004;161(2 Suppl):1-56. 2. American Psychiatric Association (APA), et al. Guideline Watch (September 2009). http://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/schizophrenia-watch.pdf. Accessed August 2017.

2/15/2018
Prospective Survey of TD in Psychiatric Outpatients - Preliminary Findings
20% Schizophrenia18% Schizoaffective disorder61% Mood disorder (Anxiety 37%, Bipolar 29%, Major depressive disorder 22%)1% Other
First and second generation antipsychotics associated with TD
Incidence rates in patients over age 55
• 25% after 1 year• 34% after 2 years• 53% after 3 years
Dopamine-Depleting DrugsReserpine and Tetrabenazine (TBZ)
Inhibit vesicular monoamine transporter (VMAT) at the presynaptic membrane of the nerve terminals
Expose monoamines to monoamine oxidase
Depletion of synaptic pool of monoamines
Reserpine:• Slower onset and prolonged duration of
effect• Inhibits both VMAT1 and VMAT2• Side effects of depression, orthostatic
hypotension and GI side effects
TBZ:• Quicker onset and shorter duration of effect• Inhibits only VMAT2• Side effects of depression, lethargy,
parkinsonism, akathisia
Valbenazine and DeutetrabenazineValbenazine Deutetrabenazine
Dosing Dosed once a day Dosed multiple times a day and with multiple tablets
Titration Requires no titration and 1 week to reach the recommended dose
Typically requires titration, often over the course of several weeks
Food Can be taken with or without food Needs to be taken with food
Selectivity A selective VMAT2 inhibitor with no appreciable binding affinity for dopaminergic (including D2) or serotonergic receptors
Not a selective VMAT2 inhibitor
EKG • Doesn't require an EKG to start treatment
• For patients at increased risk of a prolonged QT interval, assess the QT interval before increasing the dosage
• For patients at risk for QT prolongation, assess the QT interval before and after increasing total deutetrabenazine dosage above 24 mg per day
• Assess the QTc interval before and after increasing the dose of other meds known to prolong QTc
UCSF Movement Disorders and Neuromodulation Center
UCSF Mt Zion Campus1635 Divisadero Street, Suite 520, San Francisco, CA 94115
Referrals:• Clinical Consultations: 415-353-2311 (phone); 415-353-9060 (fax)• Clinical Trials: 415-353-8328; (Danilo Romero)




![r n a l o f Pain o u elief Journal of Pain & Relief · 2018. 3. 6. · Atypical odontalgia is a subtype of persistent idiopathic facial pain (PIFP) [10], which has pain characteristics](https://img.pdfslide.net/doc/110x75/60320a51cb58d26e8967360c/r-n-a-l-o-f-pain-o-u-elief-journal-of-pain-relief-2018-3-6-atypical-odontalgia.jpg)