Embed Size (px)
Citation preview

lar fibrocartilage of
LM: The role of ra-ography in the di-ations of the distal3, 1983: peribration of the"ocartilage complex44:376, 1984e of the hook of thefissed. J Trautna
dleden. Nord Med
: injuries. Contemp
joiut. Orthop Clin
~aui% of the distal’:26. 1984tomography in the
d Sur~9A:602, 1984~ LR: Arthrographyk6, 1972)f the exteusor carpi~led 11:183, 1983~e de traitement chi-i isolees de l’extrem-irurgie 47:589-594,
~rography revisited.
at radioulnar joint. J~81t al: Fracture of the
J Bone Joint Surg
tr injuries. Contemp
r BW, et al: The ex-I Hand Surg 9A:495,
:he hamate by a golf
Roentgen aspects of[ pisotriquetral joint.
10) J: Volar dislocation¯ 12:1083, 197"2)f the pisi-cuneiform
Medical Group, Inc.Complex, Suite 501
Vest La Veta AvenueOrange, CA 9!668
Management of Wrist Problems 0749-0712/87$0.00+.20
Ulnar Lengthening and Shortening
Ronald L. Linscheid, MD*
The concept of altering the length of one ofthe forearm bones to achieve a therapeutic result
¯ for a clinical problem at either the elbow or tk~ewrist is scarcelv new. Excision of the distal ulnafbr pain at the distal radioulnar joint ~,r and ex-cision of the radial head for post-traumaticchanges or arthritic problems proximally arewell known. The orthopedic literature suggeststhat these procedures are in fact efficacious mthe great majority of instances.~:,~s-~s Such de-structive procedures do, however, lead tomarked alterations in a complex mechanicalstructure represented by the two bones of theforearm, the interosseous membrane, the orbic-ular ligament, and the triangular fibrocartilage--to mention only the major mechanical compo-nents. We are increasingly recognizing the oftenundesirable consequences of disturbing this sys-tem through excisions, malalignments, and mal-rotations.~,t° If one is to advocate therapeuticlengthening or shortening of one of the forear:m.bones there should, therefore, be firm evidencethat it will advantageously influence a clinicalproblem and that the procedure can be accom-plished reasonably without introducing othermechanical liabilities.
Hult6n~ introduced the observation that in-dividuals with an ulna that was shorter than theradial articular surf:ace at the lunate fossa meas-ured perpendicular to the longitudinal axis ofthe forearm were at greater risk to develop Kien-b6ek’s avaseular necrosis of the lunate. Althoughit has long been recognized that the relativeelongation of the ulna secondary to collapse ofthe radius at the fracture site following Colles’4
fracture leads to a variety of distal radioulnardifficulties, ~.v.a°,a it was not generally recognized
that a congenitally elongated ulna of a millimeteror two could produce a degenerative lesion be-txveen the ulnar head and the ulnar articularsurface of the lunate through a defect in thetriangular fibrocartilage until the recent contri-butions of Mikic-~ and Palmer.a4 It takes littleadditional thought to imagine that other diffi-culties at the distal radioulnar joint are also in-fluenced by a positive or negative ulnar vari-ance.~’a.aa Indeed, there is statistical evidencethat scapholunate dissociation is more commonin the negative variances and some suggestionthat triangular fibrocartilage tears are assoeiat6dwith a positive variance,s There are a numberof conditions that mav affect this relative lengthbesides congenital variations including frac-tures, epiphysiodesis, Madelung’s deformity,and other congenital deformities,s
As the primary functional advantage of havinga tnvo-bone forearm is rotational, at least as faras the primates are concerned, it is inevitablethat ~ve should also see problems associated withthis motion. Although one would expect this ro-tation to occur about a fixed axis running fromthe center of the radial head proximally-to thecenter of the ulnar head distally, the complexcurvature of the forearm bones, the asymmetryof the radial head, and the eccentric insertionof the triangular fibroqartilage cause the rota-tional axis to describe a quasiconicaI surface frompronation to supination. ~* This also results in theulnar head describing a dorsal to palmar trans-lation within the shallow sigmoid notch of theradius during this motion.TM This articular sur-face is usually offset from a parallel to the ro-tational axis by 20 degrees or more, and alsoslides distally about 1 mm, on average, from
*Professor of Orthopaedic Surgery, Mayo Medical School; Consultant in Orthopaedics and Surgery of the Hand, MayoClinic, Rochester, Minnesota
Hand Clinics--Vol. 3, No. 1, February 1987 69

70 Ronald L. Linscheid
supination to pronation.I~’,~a When the f~rearmis excessively loaded in torque so as to exceedits rotational constraints or complexly loaded incompression and torque, the articular surfacesmay undergo sufficient shear stress to developsymptomatic chondromalaeia. This is a conditionthat one can scarcely find mentioned in the lit-erature, but is a definite entity.2~ There appearsto be an increased susceptibility to this problemin individuals with a lax ligamentous habitus, inour experience.8
The ulnar head bears compressive stress onits distal surface ("pole") and primarily shearstress on its radial convex surface ("seat").36 Thetriangular fibrocartilage is composed of a centralcartilaginous surface bordered by two fibrous lig-amentous components arising from either sideof the sigmoid notch that coalesce to insert inthe fovea of the ulnar head and the proximalportion of the ulnar styloid. It extends distally,fusing with a "meniscal homologue" to insert onthe triquetrum enveloped by the fibrous exten-sion of the periosteum from the ulnar styloid.~a,a4
It is supported dorsally by the floor of the fifthand sixth dorsal extensor sheaths and palmartybv the ulnoearpal ligament.4’z The triangularfi]~rocartilage has numerous functions,ineludinge.a: l) transmission of compression fromthe carpus to the ulnar head, 2) resistance totension induced by distraction from the radius,3) constraint of the distal radioulnar joint in ro-tation, 4) constraint of the carpus to the ulna,and 5) continuation of the radiocarpal joint.
Palmer and coworkers have shown the .per-centage of joint compressive force carried by theulna varies with its length relative to the ra-dius. n.a4 The have also shown that the thicknessof the triangular fibroeartilage varies inverselywith the negative ulnar variance in a roughlylinear fashion.~ This tends to provide a marginof safety when considering an ulnar lengtheningas the thicker triangular fibrocartilage is moreapt to conform to the additional compression andshould be more resistant to attritional penetra-tion.
ULNAR SHORTENING
Ulnar recession has been of benefit in ourexperience for conditions associated with anulnar positive variance.8 This includes ulnolu-nate impingement and triangular fibrocartilagetears. The symptoms are generally associatedwith pain and tenderness between the ulnarhead and triquetrum. Crepitus may be presenton ulnar deviation. This may be accentuated by
displacing the ulnar head palmarly when. theforearm is in pronation and then stressing ulnardeviation, tloentgenograms in younger indivi-duals are generally unrewarding, but when theulnar head has eroded through the triangularfibrocartilage, a characteristic sclerosis and ero-s/on between the ulnar head and lunate is rec-ognizable, usually in patients past the fifthdecade"~,a4 (Figs. 1A and B). Ulnar recession al-lows this to be decompressed while not signifi-cantly altering the radioulnar contact. When thepositive variance exceeds several millimeters,the ulnar head is usually dorsally displaced overthe ulnar aspect of the carpus. When the ulnaplus is marked and the head dorsally subluxed,additional soft tissue imbrication following ul-nocarpal repositioning and pinning is desira-ble. i4
Triangular fibrocartilage tears also respond toulnar recession (Figs. 2A to F). A positive ar-throgram should be supported by diagnosticclinical signs of triangular fibrocartilage dys-function as perforations of the cartilage becomeincreasingly common after the fourth decade andare expected in the sixth decade. ~ Tendernessbetween ulnar head and triquetrum accentuatedby ulnar deviation when the ulnar head is de-pressed is suggestive, as is a palpable or audibleclick ~vith forceful motions of the wrist. It ispossible to have an incomplete rent in the prox-imal surface of the triangular fibrocartilage aswell, which is associated with a negative radio-carpal arthrogram. An arthrogram of the distalradioulnar joint showing a proximal rent, espe-cially if pain is relieved by a simultaneous li-docaineinfusion, is diagnostically helpful. Tearsof the lunotriquetral interosseous membranes,triquetrohamate impaction injuries, a~-d fourthand fifth carpometacarpal sprains are not infi-e-quently associated ~vith these lesions.~ Evenwith the most careful and discerning examina-tion, it is not always possible to elicit or properlyweigh the various findings in ulnar column
Congenital conditions, such as "forme fruste"of Madelung’s deformity, and post-traumaticconditions, such as premature epiphysiodesis,also produce symptomatic ulnar plus variance(Fig. 3A). Particularly in the former, one oftensees, in addition, a marked palmar angulation ofthe lunate fossa. This predisposes to a seeonda~3,remodeling deformity of the lunate, which slidesinto the defect between the deficit radius andthe dorsally displaced and elongated ulnar head.It is possible to perform an osteotomy palmarlya short distance proximal to the lunate fossa sothat the fossa may be refm’med (Fig. 3B).

Ulna," Lenglhening and Shortening71
almarly when themn stressing ulnarn younger indivi-ing, but when thelgh the triangularsclerosis and ero-and lunate is rec-
~ts past the fifth~’lnar recession al-l,virile not signifi-~ontact. When theveral millimeters,dly displaced ogers. When the ulna~torsallv subluxed,tion~ following ul-~inning is desira-
.rs also respond tof). A positive ar-ed by diagnosticibrocartilage dvs-cartilage become
fourth decade and~de. >a Tendernesstrum accentuatedulnar head is de-dpable or audiblef the xvrist. It is.~ rent in the prox-’ fibrocartilage asa negative radio-
;ram of the distalximal rent, espe-simultaneous li-
:lly helpful. Tears!OtiS membranes,uries, and fourthins are not infre-~ lesions. ~ Even~’erning examina-elicit or properlyin ulnar column
as "forme fruste"post-traumatic
epiphysiodesis,~ar plus variance)rmer, one oftennar angulation ofes to a secondarytare, which slideseficit radius and,~ated ulnar head.eotomy palmarly
lunate fossa soed (Fig. 3B).
Figure 1. A 67-year-old industrial worker ~vith increasing pain and crepitus of the right ~vrist. A, Positive ulnar varianceof 2 mm. B, High resolution. Note sclerotic evstic changes in ulnolunate area. (From Darrow JC, Linscheid RL, DobvnsJH, et al: Distal ulnar recession for disorders of~he distal radioulnar joint. J Hand Surg 10A:482-491, 1985; ~vith permissidn.)
section of the ulna removed for the concomitantulnar recession is used to block open the partMradial osteotomy.
Occasionally, the distal ulna appears to havean excessive angulation in its distal third, whichis best recognized on a sagittal forearm roent-genogram (Fig. 8B). If this appears clinically be associated with dorsal subluxation of the ulnarhead in pronation, the angulation may be cor-rected at the time of recession (Figs. 8C, D, andE).
The seat of the ulnar head, that convex surfacethat articulates with the sigmoid notch of the,,radius, is also susceptible to painful lesions. Themost common lesion is ehondromalaeia of the,,ulnar head produced by shear stress when it is:driven against the dorsal rim of the sigmoidnotch during forceful pronationz~ (Fig. 4). Thisis the same mechanism that produces dorsal sub-luxation or dislocation of the ulnar head and,indeed, these would seem to be all part of thesame spectrum of injuries. In the acute stage,the diagnosis is readily established by ballotingthe ulnar head in the sigmoid notch in a seriesof tests between full supination and pronation.
Placement of the forearm in a rotational positionwhere the injured cartilage is not subjected toshear stress for 4 to 6 weeks will usuallv resultin a satisfactory result in the acute situation. Castimmobilization in a long arm east in moderatesupination is most commonly used. This al-~o al-lows ligamentous attenuation to heal at physio-logic length.
Sometimes, however, repetitious rotation ofthe forearm will lead to a Chronic condition. Thegroup most at risk for this is those individualswith a lax ligamentous habitus, particularlyyoung women (Figs. 4A, B, and C). Their ulnarheads are often markedly prominent in prona-tion (Fig. 4D). We have seen two exampleswhere, at exploration, the articular cartilage waspartially peeled offthe ulnar head (Fig. 4E). Thiswould catch and block the normal pahnar }eturnof the ulnar head during supination.S
When the ulnar head is ballotable, there isnot infrequently a coneomitant laxity of the car-pus relative to the radius manifest as a sup/nationof the carpus. Normally, the ulnoearpal ligamentrunning obliquely from the palmar surface of the
triquetrum to the ulnar styloid is largely re-

72 Bonald L. Linscheid
Figure 2. Torn triangular fibrocartilage in a 56-year-old \voinan. She had had pain aud crepitus aggravated bv ulnardeviation for i0 months. A, Initial appearance of roentgenogram. B. Arthrogram shows the dve flo~ving through the triangularfibrocartilage into the distal radioulnar joint. C, Positive ulnar variance of 2 m~n. Note th~ position of the triquetrum. D,Radial deviation. E, Appearance after surgery (4 mm of recession). Negative ulnar variance is 2 ram. F, Lateral, normalaligmnent of distal ulna: excellent relief of symptoms. (From Darrow JC, Liuscheid IlL, Dobyns JH, et al: Distal nlnarrecession for disorders of the distal radioulnar joint. J Hand Surg IOA:482-491, 1985; with permission.)
sponsible for maintaining a stable relation-ship.~,a,4n4~ Assuming the ligament is otherwiseintact, it may be relatively elongated and pro-vide less stability ~vhen the ulnar has a plus var-iant. Ulnar recession in this instance tends totighten the ulnocarpal as well as the distal ex-tension of the triangular fibrocartilage, thus in-creasing the stability of the ulnar column.
Ulnar recession is of primary value iu decom-pressing those impiugement problems assoeiZated with an ulnar variaut or iu those chondro-malacia-related problems in the distal radiotdnm
joint (Fig. 4F). In the latter, the ulnar head notonlv recedes relative to the radius, but also mavdisplace laterally because of the obliquity of the,~
sigmoid notch. This acts to decompress the areaas xvell as to change the beariug surfaces. Thereseem to be infrequent sequelae to this proce--dure. To our knmvledge, no instance of Kien-b6ck’s disease~° has resulted from iutentioimllvproducing au ulnar minus variant. It shouldstressed, hmvever, that the amount of recessionis carefi~lly planned not to exceed a minus var--iance of $ ram.

Ulnar Lengthening and Shortening 73
;gravated by ulnaroug3a the triangularthe triquetrum. D,F, Lateral, normalet al: Distal ulnar
, ulnar head notls, but also mayobliquity of therepress the areasurfaces. Theres to this proee-.stance of Kien-ml intentionallynt. It should be,unt of recessioned a minus var-
Figure 3. A 21-year-old student who had increasing pain in her wrists during gymnastics is shown. A, Positive ulnarvariance of 13 ram. B, Lateral view shows dorsal subluxat:ion and increased angulation of distal ulna and increased palmarangulation of radial articular surface, suggestive of forme fruste Madelung’s deformity. C-E, Operative procedure. Ulnar
¯ recession of 10 mm. Radial osteotomy and plating were accomplished using the T-plate of the Association for the Study ofInternal Fixation. A five-hole dynamic compression plate maintained alignment of the ulna. (From Darrow JC, Linscheidt/L, Dobyns JH, et al: Distal ulnar recession for disorders of the distal radioulnar joint. J Hand Surg IOA:482-491, 1985;with permission.)

74 Ronatd L. Linscheid
Figure 4. A 40-year-old woman with ligamentous laxity had snapping, painful distal radioulnar joints bilaterally. A previousDarrach procedure on the right wrist required subsequent stabilization. A, The left wrist is now crepitant. B, The thumbis easily passively approximated to the forearm. C, Both ge~au and cubitus recurvatum were present. D, Roentgenogram isessentially normal. There is positive ulnar variance of i mm and a positive "piano key" sign. E, Intraoperative photographshows that the convex surface of the articular cartilage head of the ulna is avulsed from its proximal attachment and is beingstressed during pronation. F, Ulnar recession of 3 mm resulted in increased stability and lack of crepitance and pain onpronation. (From Darrow JC, Linscheid RL, Dobyns JH, e~! al: Distal ulnar recession for disorders of the distal radioulnar~oint~ ~ Hated Surg 1(3A:482-49]., 1985; with permission.)

bilaterally. A previouspitant. B, The thumbD, tloentgenogram is~operative photographtachment and is being"epitance and pain onf the distal radioulnar
ULNAR LENGTHENING
After describing some of the benefits accruingfrom ulnar shortening, it seems somewhat par-;.doxical that one could recommend the oppositeprocedure as well. Nevertheless, there are con-ditions that appear to be favorably influenced byulnar lengthening. Shortly after Hult6n’s de-scription of the ulnar minus variant associated~vith Kienb6ck’s disease,la,’~° it was suggestedthat either ulnar lengthening or radial shorten-ing might benefit that condition, as Numerousreports suggest this efficacy, 1.4o particularly thelong-term follow-up of Moberg.a2 Hereafter, onemay assume that radial shortening is synony-:~ous with ulnar lengthening.I~
The rationale of ulnar lengthening for Kien-.b6ck’s disease is to decompress that area of thelunate that is undergoing collapse because of the.joint compressive force actiug on the affectedsubcortical trabeculae. This is primarily the partarticulating ~vith the lunate fossa. The ulnar as-.pect of the proximal articular surface is ofte~minimally involved (Fig. 5). If the ulna is elon--gated, the triangular fibrocartilage is com-.r;ressed and acts to support the ulnar aspect":e lunate and the articular facet of the trique.-trum. Of necessity, this also induces a mild ra--dial deviation that increases the joint compres.-
sive force on the scaphoid. Arthrograms takenat the time of ulnar lengthening show an in-creased joint space1 (Figs. 6A and B). Ulnarlengthening does not change the secondary fea-tures such as lunate collapse, scaphoid palmarflexion, or extrusion of the lunate fragments bythe intruding capitate. It does, however, usuallyproduce prompt and sustained pain relief. Likemost treatments, the results are better in theearlier stages of the process. To date, the effec-tiveness of this approach over a 5-year periodhas been 85 per cent satisfactory.~.4°
Recently, we have used this approach for an-other condition which we chose to call "nondis-sociative carpal instability" (NDCI),~-~ but it hasalso been called midcarpal instability, ~ ulnarcolumn instability, ~:~44 and the CLIP syn-drome.~ Though still not ~vell understood, thiscondition causes weakness and usually a pro-nounced snap as the wrist angulates from radialdeviation to ulnar deviation,z~’,~’4 Under theimage intensifier, this corresponds to a suddenswitch of the proximal carpal row from palmarflexion to dorsiflexion. This conjunct rotation ofthe proximal row, which is usually seen as asmooth gradual transition in normal wrist mo-tion, occurs cataclysmically in NDCI. ~vVe notedin several patients that, if the triquetrum weresupported by thumb pressure from the ulnaraspect, the transition could be made less abrupt.In those patients with an ulnar minus variant,elongating the ulna appears to offer similar sup-port to the carpus. We believe that the lunatetranslates down the inclined plane of the radiusunder compression, rendering the radiolunateligaments taut, thus preventing the gradual ro-tation at the lunate. By supporting the proximalcarpal row from the ulnar side, the unstable stateis corrected and allows a normal conjunct rota-tion.
There is some reason to believe that bettersupport from the ulnar;aspect would removesome of the stress from the scapholunate liga-ment after repair of this ligament in seapholu-note dissociation as well, though clinical use hasas yet not been demonstrated.
Figure 5. Typical radiographic changes of KienbOck’sdisease, showing an ulnar variance of -8 mm, sclerosis,cystic changes, and fragmentation of the lunate. (From Ar-misread RB, Linscheid RL, Dobyns JH, et al: Ulnar length-ening in the treatment of Kienb6ck’s disease. J Bone Join.tSurg 64A:170-178, 1982; with permission.)
SURGICAL PROCEDURES
These procedures have been made possibleby the development of reliable hardware thatallows for reasonable precision in length alter-ation, alignment, and angulation to beachieved,aa Although there have been a few de-layed unions ~vhen accurate cuts, full apposition,and adequate compression have been achieved,

76 Ronald L. Linsck,:eid
Figure 6. Intraoperative ar-throgram of the ~vrist after comple-tion of the osteotomy and beforelengthening of the ulna. B, Im-mediately after the ulna is length-ened, the radiolunate joint spaceappears widened, as indicated bythe heightened band of contrastmedium in the radiolunate space.(From Armistead PtB, LinscheidRL. Dobyns JH, et al: Ulnarlengthening in the treatment ofKienb6ck’s disease. J Bone JointSurg 64A:170-178, 1982: ~vith per-mission.)
union is predictable between 6 and 10 weeks.The procedures are introduced in outline formbelow. 1.8
Ulnar Lengthening
Ulnar Recession
1. Preoperative measurement and planning.2. Incision along distal subcutaneous aspect
of’ulna and over the ulnar head (Fig. 7A).3. Application ofa DCP plate bent to conform
to the distal ulna with two screws in distal holes(Fig. 7B).
4. Alignment marks and an osteotomy markproximally with saw cut (Fig. 7B).
5. Transverse osteotomy (Fig. 7B).6. Optional inspection of distal radioulnar
joint by outward swing of distal ulna (Fig. 7C).7. Resection of predetermined length of ulna
(Fig. 7C).8. Mignment of distal segment and its at-
tached DCP plate (Fig. 7D).9. Fixation with compression screw and in-
sertion of remaining screws (Fig. 7D).10. Closure, immobilization.I1. Cast change, roentgenogram check at 6
weeks.
1. Preoperative measurement and planning(Fig. 8).
2,. Exposure of distal ulna.3. Three-quarter transverse osteotomy cut.4:. Application of Zimmer four- or six-hole
slotted plate with screws placed away from cut.5. Completion of osteotomy.6. Distraction with cervical laminectomy
spreader.5’. Tighten screws. 5"8. Obtain bicortical iliac crest graft of proper
thickness (3 to 6 ram) perpendicular to crest.9. Place graft in gap, cancellous aspect toward
radius.2[0. Loosen distal screws one turn to obtain
co~npression.11. Tighten screws.i[2. Trim redundant graft with bone biter.113. Place remaining graft material around os-
teotomy site.14. Closure and immobilization.115. Cast off and roentgenogram at 6 weeks.2If radial shortening is performed, we currently
prefer a palmar metaphyseal osteotomy with fix-ation by an ASIF T-plate.

Ulnar Lengthening and Shortening 77
Intraoperative ar-wrist after comple-eotomy and beforethe ulna. B, Im-the ulna is length-~lunate joint space~d, as indicated by
band of contrastradiotunate space.
~ad RB, LinscheidJH, et al: Ulnarthe treatment of
~ase. J Bone Joint78, 198~2; with per-
t and planning
,steotomy cut..ur- or six-holeaway from cut.
1 lamineetomy
" graft of proper~ular to crest.is aspect toward
turn to obtain
h bone biter.erial around os-
on.tin at 6 weeks.;d, we currently~otomy with fix-
B D
Figure 7. A, Incision over the subcutaneous border o~the distal ulna curved dorsally for exploration of the distal radioulnarand ulnocarpal joints. B, Applying the dynamic compression plate xvith two screxvs distally, marking of alignment, looseningthe plate by removing one screxv, and completing the osteotomy. C, The plate is reapplied distally, the interosseous membraneis released, and the distal radioulnar joint is inspected b’.¢ swinging the ulna out~vardly. D, Compression plating after repairand recessional osteotomy. In the latter part of this study, the fixation plates were changed from a 3.5 mm screw hole to a2.7 mm hole size, with a corresponding increase from five to eight or nine holes. (From Darro~v JC, Linscheid RL, Dobyns,~l, et al: Distal ulnar recession for disorders of the distal radioulnar joint. J Hand Surg 10A:482-491, 1985; xvith permission.)
Figure 8. Technique forlengthening the ulna by interposi-tional bone grafting and stabiliza-tion with a slotted plate. Length-ening of the osteotomized ulna andinsertion of the graft is facilitatedby using a laminar spreader to dis-tract the fragments. Note that theplate is applied before distraction.TFC = triangular fibrocartilage.(From Armistead RB, LinscheidRL, Dobyns JH, et al: Ulnarlengthening in the treatment ofKienbGck’s disease. J Bone JointSurg 64A:170-178, 1982; with per-mission.)
~mm
5ram
¯ graft
KIEI\IBOGkS DISEASE’ULNAR LENGTHENING

78 Ronald L. Linscheid
SUMMARY
Alteration in length of the distal ulna may pro-vide an attractive alternative to more destructiveprocedures commonly used for the treatment ofmechanical and degenerative problems at thedistal radioulnar joint. Ulnar recession hasshown effectiveness in ulnolunate impingement,triangular fibrocartilage tears, and symptomaticulnar plus variance. It has also been effective inchondromalacia of the ulnar head in the sigmoidnotch and in unstable distal radioulnar jointswhere recession alters the bearing surface andtightens the ulnocarpal ligamentous complex.Ulnar lengthening has been efficacious in re-lieving the symptoms of Kienb6ck’s disease bydecompressing the involved portion of the lu-nate and distributing joint compressive force onthe triquetrum and medial lunate articular sur-faces. It may also be of value in some instancesof NDCI associated with an ulnar minus variant.
REFERENCES
1. Armistead, t/B, Linscheid RL, Dobyns JH, et al: Ulnarlengthening in the treatment of Kienbock’s disease.J Bone Joint Surg 64A:170-178, 1982
2. Bowers WH: Distal radioulnar joint. In Rockwood CAJr, Green DP (eds): Fractures. Philadelphia, JB Lip-pincott, 1975, pp 743-769
3. Bowers WH: Distal radioulnar joint arthroplasty: Thehemiresection-interposition technique. J Hand Surg10A:169-178, 1985
4. Colles A: On the fracture of the carpal extremity of theradius. Edinb Med Surg J 10:182-186, 1814
5. Czitrom AA, Dobyns JH, Linscheid liL: Ulnar variancein carpal instability. Presented at 53rd annual meetingof the American Academy of Orthopaedic Surgeons,New Orleans, February, 1986
6. Darrach W: Forward dislocations at the inferior radioul-nar joint ~vith fracture of the lower third of the radius.Ann Surg 56:801, 1912
7. Darrach W: Partial excision of lower shaft of ulna fordeformity following Colles’ fracture. Ann Surg57:764-765, 1913
8. Darrow JC, Linscheid IlL, Dobyns JH, et al: Distalulnar recession for disorders of the distal radioulnarjoint. J Hand Surg 10A:482-491, 1985
9. Dobyns JH, Linscheid RL: Fractures and dislocationsof the wrist. In Rockwood CA Jr, Green DP (eds):Fractures in Adults. Edition 2. Philadelphia, JB Lip-pincott Company, 1984
10. Ekenstam F, Engkvist O, Wadin K: Results from re-section of the distal end of the ulna after fractures ofthe lower end of the radius. Scand J Plast ReconstrSurg 16:177-181, 1982
11. Ekenstam FW af, Palmer AK, Glisson RR: The load onthe radius and ulna in different positions of the wristand forearm. Acta Orthop Scand 55:363-365, 1984
12. Ekenstam FW af: The distal radio ulnar joint: An ana-tomical, experimental and clinic.al study with specialreference to malunited fractures of the distal radius.Thesis. Uppsala Universitet, 1984, pp 1-55
13. Ekenstam FW af, Hagert CG: Anatomical studies onthe geometry and stability of the distal radio ulnarjoint. Scand J Plast lieconstr Surg 19:17-25, 1985
14. Hui FC, Linseheid RL: Ulnotriquetral augmentationtenodesis: A reconstructive procedure for dorsal sub-luxation of the distal radioulnar joint. J Hand Surg7:230-236, 1982
15. Hulten O: Uber Anatomische Variationen der Hand-gelenkknochen. Ein Beitrag zur Kenntnis der Genesez~vei verschiedener Mondbeinverandernngen. ActaRadiol 9:155-168, 1928
16. Kapandji IA: The inferior radioulnar joint and prono-supination. In Tubiana R (ed): The Hand. Philadel-phia, WB Saunders Company, 1981, pp 121-129
17. Kapandji IA: A technique for shortening of the radius.Ann Chir Main 1:265-267, 1982
18. Kessler I, Hecht O: Present application of the Dar~achprocedures. Clin Orthop 72:254-260, 1970
19. Kessler I, Silberman Z: An experimental study of theradiocarpal joint by arthrography. Surg Gynecol Ob-stet 112:33-40, 1961
20. Kienbock R: Uber Tramnatische .Malazie des Mond-beins und Ihre Folgezustande: Entartungsformenund Kompressionsfrakturen. Fortschr Geb Rontgen16:78-103, i910-1911
21. Lichtman DM, Schneider JR, Swafford AR, et al: Ulnarmidcarpal instability---clinical and laboratory analy-sis. J Hand Surg 6:515-523, 1981
22. Linscheid RL, Dobyns JH, Beabout JW, et al: Traumaticinstability of the wrist: Diagnosis, classification andpathomechanics. J Bone Joint Surg 54A:1612-1632,1972
23. Linscheid RL, Dobyns JH, Beckenbaugh liD, et al:Instability patterns of the ~vrist. J Hand Surg8:682-686, 1983
24. Linscheid liL, Dobyns JH, Younge DK: Trispiral to-mography in the evaluation of wrist injury,. Bull HospJoint Dis Orthop Inst 44:297-308, 1984
25. Linscheid liL, Dobyns JH: Wrist sprains. In Tubiana li(ed): The Hand, Vol. 2. Philadelphia, WB SaundersCompany, 1985, pp 970-985
26. Louis DS, Hankin FM, Bowers WH: Capitate-radiusarthrodesis: An alternative method of radiocarpal ar-throdesis. J Hand Surg 9A:365-369, 1984
27. Macksoud WS, Dobyns JH, Linscheid ilL: Nondisso-ciative collapse of the proximal carpal ro,v. Presentedat 98th annual meeting of the American OrthopaedicAssociation, Coronado, California, June, 1985
28. Mikic ZD, Helal B: The value of the Darrach procedurein the surgical treatment of rheumatoid arthritis. ClinOrthop 127:175-185, 1977.."
29. Mikic ZD: Age changes in the triangular fibrocartilageof the ~vrist joint. J Anat 126:367-384, 1978
30. Milch H: Dislocation of the inferior end of the ulna:Suggestion for a new operative procedure. Am J Surg1:141-146, 1926
31. Milch H: Treatment of disabilities following fracture ofthe lower end of the radius. Clin Orthop 29:157-163,1963
32. Moberg E: Treatment of Kienbock’s disease by surgicalcorrection of the length of the radius or ulna. In Tub-iana R (ed): The Hand, Vol. 2. Philadelphia, Saunders Company, 1985, pp 117-120
33. Muller ME, Algower M, Schneider R, et al: Manual ofInternal Fixation. Edition 2. New York, Springer-Verlag, 1979
34. Palmer AK, Werner FW: The triangular fibrocartilagecomplex of the wrist--anatomy and function. J HandSurg 6:153-162, 1981

.tomical studies on~ distal radio ulnarg 19:17-25, 1985etral augmentationlure for dorsal sub-ioint. J Hand Surg
ationen der Hand-enntnis der Geneseranderungen. Acta
lr joiut and prono-~e Hand. Philadel-,81, pp 121-129:ning of the radius.
tion of the Darrach260, t970nental study of theSurg Gynecol Ob-
,lalazie des Mond-Entartungsformen
tschr Geb Rontgen
’,~rd All, et al: Ulnard laboratory analy-
jW, et al: Traumatic~, classification andtrg 54A:1612-1632,
nbaugh ltD, et al:’ist. J Hand Surg
e DK: Trispiral to-st injury,. Bull Hospi, 1984~rains. In Tubiana Rphia, WB Saunders
;H: Capitate-radius~d of radiocarpal ar-;69, 1984laeid t/L: Nondisso-rpal row. Presented~erican Orthopaedict, June, 1985~ Darrach procedureaatoid arthritis. Clin
agular fibrocartilage’-384, 1978or end of the ulna:"ocedure. Am J Surg
follo~ving fracture ofOrthop 29:157-163,
s disease by surgical|ius or ulna. In Tub-. Philadelphia, WB7-120r If, et al: Manual ofew York, Springer-
agular fibrocartilagend fuuction. J Hand
Ulnar Lengtt~ening and Shortening 79
3.5. Palmer AK, Glisson Ril, Werner FW: Ulnar variancedetermination. J Hand Surg 7:376-379, 1982
palmer AK, Werner FW: Biomechanics of the distalradioulnar joint. Clin Orthop 187:26-35, 1984
37. Palmer AK, Glisson RR, Werner FW: Relationship be-".ween ulnar variance and triangular fibrocartilage,.otnplex thickness. J Hand Surg 9A:681-683, 1984
3~. [;ersson M: Pathogenese und Behandlung der Kien-bockschen Lunatummalazia: Der Frakturtheorie itnLichte der Erfolge Operativer Radiusverkurzung(Hulten) und einer nenen Operationsmethode-U1-naverlangerung. Acta Chir Scand 92:(Suppl 98), 1945
39. Robbin ML, An KN, Linscheid t/L, et al: Anatomic andkinematic analysis of the human forearm using high-speed computed tomography. Med Biol Eng Comput24:164-168, 1986
40. Sundberg SB, Linscheid IlL: Kienbock’s disease: lie-suits of treatment with ulnar lengthening. Clin Or-thop 187:43-51, 1984
41. Tateisnik J: The ligaments of the wrist. J Hand Surg1:110-118, 1976
42. Tateisnik J: Wrist: Anatomy, function, and injury. AcadOrthop Surgeons Instruc Course Lect 27:61-87, 1978
43. Taleisnik J, Watson HK: Midcarpal instability caused bymalunited fractures of the distal radius. J Hand Surg9A:350-357, 1984
44. Taleisnik J: Triquetro-hamate and triquetro-lunate in-stabilities (medial carpal instability). Ann Chir Main3:331-343, 1984
Mayo Clinic200 First Street SW
Ilochester, MN 55905

Do not mark this box!Document: 11000228

Clinicaland Rel
.~placement of the U¯ osby, 1982 p l,
lct~ve surgery and~elley, W. N.,:, C. B. (eds.): Textlhiladelphia, W. B. Sau~
2Ommunication, 1988.cobs. M. A.: Total:op. 182:137, 1984."g, R. D., Poss, R., Tb~nd Sledge, C. B.:throplasty: Two to five~id arthritis. J. Bone
cci, P~ M.: Total elbow,,~t Surg. 62A:1252, 1980.ratanabe. S., and Prefect~fthe rheumatoid elbow,¯ Bone 3,oint Surg. 62A:27
an. R. S.: Complications ofty. Clin. Orthop. 170:204
R. S.. Dobyns, 3. H., andelbow arthroplasty__a tive
Mayo Clinic. J. Bone 3,oinl
-I., and Borden, L. S.: CaN-,ow arthroplasty: Two-to’~in. Orthop. 223:175, 1987.
Detailed Anatomy of the Articular Disc
of the Distal Radioulnar Joint
~ELIMIR D. MIKIO, M.D., D.Sc.*
articular disc of the distal radioulnar jointwas studied in 109 wrist joints from 64
adult cadavers. The disc is a strong fibro-mous semicircular biconcave structure
adapted to its various functional roles. Theof the disc at its radial attachment varied
ween 12 and 20 mm (in most cases, 14-16and the width, measured between the apex
the radial base, varied from 7 to 14 ram, (in9-11 ram). The thickness of the dorsal
palmar margins and the ulnar apex variedi’om 3 to 6 mm (in most cases, 4-5 ram), whereas
hickness of the central part varied from 0.5 tomm (in most cases, 1 ram) and in a number
eases was perforated. Because the incidence ofincreases progressively with the age
the perforations were assumed todegenerative in nature. Although the articular
a definable anatomic entity, it is intimatelyto surrounding elements to form a com-
plex anatomic and functional structure.
articular disc of the distal radioulnar
(discus articularis), known in the oldnomenclature as the triangular fibrocartilage:(fibrocartilago triangularis), is a forgotten
27 usually described in standard
of anatomy in a generalized waylittle detail. ~0’13"2°’5L6~’63"65 More atten-
been paid to it by surgeons who havegradually recognized its importance in the
From the Department of Orthopaedics and Trauma-’ of Medicine, Novi Sad, Yugoslavia.
* Associate Professor of Orthopaedics and Trauma-
Reprint requests to ~elimir Miki6, M.D., D, Sc., Me-fakultet, Hajduk Veljkova l, 21000 Novi Sad,
Received: February 8, 1988.
pathology of the wrist joint. L63’~ 1.14,18,19,25,-27,34.36,39.43.53,55.56,60,63,64 Recently, the articular
disc and its surrounding structures have beenstudied more thoroughly24"26"33"37’3a’42’45-5°;however, there is still significant controversyregarding its morphology and biomechanics.In an attempt to improve current knowledgeon this subject, a detailed study of the mor-phologic characteristics of the articular discwas made.
MATERIALS AND METHODS
One hundred nine wrist joints were studied in(;4 fresh adult cadavers ranging in age from 21 to94 years. Preparation was carried out within six to48 hours after death. The joints were dissectedfrom the dorsal aspect and were thoroughly exam-i,ned, after which the articular discs were com-pletely removed, inspected, and measured withcalipers and a ruler. The length, width, and thick-ness of all discs were measured, after which allspecimens were preserved in 4% formalin. In ad-dition, ten wrist joints from ten cadavers werecompletely excised by cutting the bones 6 cmproximally and distally. These joints were used for --sectioning in the horizontal plane and for study-ing the bone attachments of articular discs. Tenmacerated bones from the medical school collec-tion were also surveyed to observe the distal endsof the radius and ulna.
RESULTS
The articular disc is a strong fibrocartilagi-nous structure, triangular or somewhat se-micircular in shape, stretched between the
lower ends of the radius and ulna, and inter-posed between the ulnar head proximallyand the lunate and triquetral bones distally
123

124 Miki8 Clinicaland Relatecl
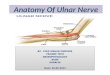
(Fig. I). The disc has two articular surfaces,the upper ulnar and lower carpal, and twocircumferential or capsular margins, dorsaland palmar. On the medial ulnar part, thereis the apex; laterally or radially, there is thebase of the disc.
The length of the disc measured at its; basenear the radial attachment varied between 12and 20 mm (Fig. 2). In most cases it mea-sured 14-16 mm (Fig. 3). The width of thedisc measured between the apex and radialbase varied from 7 to 14 ram, in most casesbeing 9-11 mm (Figs. 4 and 5).
The disc has a biconcave shape in both thesagittal (Fig. 6) and frontal planes (Fig. because its upper and lower articular surfacesare deepened and adapted to the convexity ofthe ulnar head proximally and the lunate’, andtriquetral bones distally. However, the con-cavity of the carpal surface is much less pro-nounced. The peripheral margins of the discare much heavier and stronger than the cen-tral part, where it is thinner and occasionallyperforated.
The thick and strong marginal part oli thedisc in the sagittal plane (Fig. 6) has the shapeof an approximately equilateral triangle, thebase of which is turned toward the dorsal orvolar capsular side, and its apex is turnedtoward the central thin area of the disc. Thesections in the frontal plane (Figs. 1 and 7)had peripheral parts that were thickened andhad a triangular shape. The ulnar part wasmuch larger than the radial.
The thickness of the dorsal and palmarmargins and of the ulnar apex varied from 3to 6 ram, in most cases being 4-5 mm (Fig.8). The thickness of the radial margin wasbetween 1 and 4 ram; however, in 75% of thecases, it was about 2 ram. The thickness ofthe central area varied from 0.5 to 3 ram,and in most cases was about 1 ram. Some-times the central area was so thin that it wastransparent (Fig. 2), and in a number of casesit was perforated. Perforations of variousshape and size occurred in 7.6% of the sub-jects in the third decade of life, 18.1% in thefourth, 40% in the fifth, 42.8% in the sixth,
and 53.1% in those older than 60 years
age.37 In one wrist of a 70-year-old subject,calcifications of the articular disc were notedmacroscopically.
In younger persons the carpal surface ofthe disc is whitish or yellow-whitish, smooth,and glistening. The border between the arti.ular surfaces of the radius and of the disc isdifficult to define (Fig. 9). On the upper sur-
face that articulates with the ulnar head, thedisc is also whitish or yellow-whitish,smooth, and shiny in younger persons; how-ever. in older subjects it appears more oftenmatted and irregular. In later decades of life,more obvious degenerative changes occur onboth sides of the disc; however, they arealways much more severe on the ulnar sideas reported cartier.~
The disc is attached by its base to the distaledge of the ulnar notch of the radius (incisuraulnaris radii). The massive dorsal and palmarmargins are firmly attached to the u-iangular,flattened facets at the distal ends of the dorsaland palmar edges of the ulnar notch in theradius, which could be identified on bothmacerated bones (Fig. 10) and fresh speci-mens (Fig. I1). The apex of the disc broadly inserted into a depressed area of theulnar head between the inferior articularfacet and the root of the ulnar styloid processitself (Fig. 1). The width of this depression,called the basistyloid fovea (Fig. 12), variedfrom 3 to 5 mm. Several vascular foramina,usually two in number, could consistently befound in the depression (Fig. 12). The foveacontinues proximally with a groove at thedorsomedial side of the distal ulna, whichprovides the floor for the extensor carpi ul-naris tendon sheath (Fig. 12). The mostproximal fibers of the ulnar part of the discare attached into the basistyloid fovea, whilethe fibers of the carpal part running in thedistal and medial directions are attached tothe styloid process. Between these two inser-tions, the anterior part of a vascularizedloose connective tissue forms the dorsal andradial walls of the prestyloid recess (Figs. 1, 7,9, 13, and 14). Whereas the insertion of the

and
er than 6070-year-old subular disc were noted:.
~e carpal surface)w-whitish, smoot~r between the arts and of the disc¯ On the uthe ulnar head,r yellow-whitislnge~ persons; how.tppears more often~ter decades of life,e changes occur onm~vever, they are: on the ulnar side
ts base to the distalhe radius (incisuradorsal and palmar:1 to the triangular,
ends of the dorsal~lnar notch in thelentified on bothI and fresh speci-~x of the disc is,ressed area of thenferior articular~ar styloid processf this depression,¯ (Fig. 12), varied~scular foramina,ld consistently beg. 12). The foveaa groove at the
stal ulna, whichxtensor carpi ul-
12). The most¯ part of the disc
loid fovea, whileL running in the; are attached tothese two inser-
’a vascularizeds the dorsal andrecess (Figs. l, 7,insertion of the
2451989
Articular Disc of Distal Radioulnar Joint 125
to the radius, especially of the dorsal and~ar margins, is fixed and firm, the inser-to the ulna is slightly lax and of a morems or ligamentous nature.
:;Medially the disc is continuous with theof the ulnar collateral ligament arisingthe sides of the styloid process (Fig. 1).
ligament runs distally and just distal tostyloid process it becomes thickened and
eniscuslike and inserts distally into the,us. The styloid process varied both in
and size. In 21 of 109 dissected wrists(19%). it was long and its tip was covered articular cartilage (Figs. 13 and 14). Other-
i:. wise, the tip of the styloid was free, embed-ded in the prestyloid recess, and covered bythe synovium. In this area. closely related to
styloid process, ulnarly and volarly of theapex of the articular disc. a recess (recessus
:praestyloideus), varying in shape and size,was found in all dissected joints (Figs. 1.9,and 14). Sometimes it was just a conical hol-
(Fig. 1), and sometimes it was a real sy-novial cavity (Figs. 9 and 14). The aperture
of the recess varied in diameter from 1 to 5ram, and sometimes it was hidden and cov-ered by the synovial fringes. It is rich in sy-novium and well vascularized. Occasionally,there is a red ring around the aperture. Thewidth of the cavity itself could be 5 mm, and
could be 10 mm.The thickened dorsal and palmar margins
of the disc are united to the dorsal and pal-mar radioulnar ligaments, which cannot besharply separated. These ligaments arestrengthened parts of the articular capsule ofthe distal radioulnar and wrist joints that are
attached to the dorsal and palmarins of the articular disc.
Very peripheral parts of the ulnar and car-~al surfaces of the disc (about 1 mm) arecovered by the synovial membrane comingfrom the capsule. At the radial attachments
¯ - of the dorsal and palmar margins of the disc,the synovial lining is present a little furthertoward the central part making small,tonguelike, well-vascularized fringes.
Volarly, the articular disc is associated
F’,:G. 1. Cross section of the frontal plane of theulnar part of the wrist joint of a 30-year-old sub-ject. R = radius, U = ulna, L = lunatum, T= triquetrum. Between the articular disc (D) andthe ulnar collateral ligament (UCL), a rather smalland conical prestyloid recess is located.
with the prominent, strong, intracapsularpalmar ulnocarpal ligament (Fig. 14) thatruns from the base of the ulnar styloid pro-cess and the anterior margin of the articular
F~G. 2. The excised articular disc of a 31-year-c,ld subject viewed from the carpal side. U = ulnarapex, R = radial base, where the length of the discwas measured. The peripheral zone of the disc iscovered by the synovial lining while the centralarea is rather thin and transparent.

126 Miki~ Clinical ~and Related
50 -- number o~c discs
20
15
o I , , , , I ~ , , ,10 15 20 mrn
[eng-I:h o~e discs in rnrn
FIG. 3. The distribution of" values of" the lengthof the articular disc at the radial base.
disc itself obliquely distal and lateral to thelunate, triquetral, and capitate bones. Dor-sally and medially, the articular disc isclosely related to the floor of the strongsheath of the extensor carpi ulnaris muscle(Fig. 9) that extends from its groove on theulna over the dorsum of the triquetrum tothe dorsal base of the fifth metacarpal.
DISCUSSION
The articular disc is undoubtedly an inter-esting and important structure of the wristjoint. From a phylogenetic point of view, it isa young formation because it has evolved :inprimates during the progressive retreat of theulna from its primitive articulation with thecarpal bones.2s-3°,44 The exclusion of the ulnafrom this joint was an essential prerequisitefor increased mobility of the hand and par-ticularly for an increased range of prona-tion-supination movements. During its evo-lution, the ulnar part of the wrist joint hasbeen subjected to radical change. The distalradioulnarjoint formed with its articular discthat plays an important role in the biome-
chanics of the forearm and wrist joint as ~whole.
The articular disc is obviously welladapted to its various functions. To supplythe demands of articulation, the disc has twoconcave smooth facets articulating withulna proximally and the carpal bones dis-tally. Interposed between these bone ele-ments that are otherwise incongruent, the ar-ticular disc forms the congruent surfaces forboth of them, allowing different types ofmovements on its upper and lower sides.3.4
The rotational movements of the ulnar headduring pronation and supination on the cor-responding surface of the articular disc pro-duce a much more intensive biomechanicalforce than the gliding movements of the car-pal bones on the lower side of the disc, whichis probably the reason that degenerativechanges are much more frequent and moreadvanced on the ulnar side of the disc.37
The articular disc has a significant role in
FIG. 4. Excised articular disc of a 43-year-oldsubject viewed from the carpal side. The widths ofthe discs were measured between the ulnar apex(U) and the radial base (R). The central zone ¯ this disc was rather thick and measured 2 mm.

Clinical
and wrist joint as
is obviouslyhnctions. To supply:ion, the disc has twoarticulating with thete carpal bones.’en these bone ele.incongruent, the ~ngruent surfaces for; different typesr and lower sides.3.!~ts of the ulnar headpination on the cor-e articular disc pro-~sive biomechanical~vements of the car-]e of the disc, whichthat degenerativefrequent and more~e of the disc.37
a significant role in
isc of a 43-year-old1 side. The widths of¢een the ulnar apex/’he central zone ofmeasured 2 mm.
2451989
Arl:icular Disc of Distal Radioulnar Joint 127
transmission of the axial load of the fore-
to the carpus and vice versa. The work. Koebke26 has provided sound morpholo-evidence of compressive forces acting be-
the lunatum and ulnar head, whichms that the disc is also subjected to con-
Siderable compressive strain. Partially the:ssive force is transmitted through thepart of the disc; however, some of the
:ompressive loading is converted to tensile:loading within the peripheral margins of thedisc) The disc fills the gap between the ulnar
and carpal bones and acts as a cushion
for the ulnar carpus to prevent ulnocarpal5.3~_.46 5o Thus, the thickness is an im-
portant feature of the articular disc and isapparently determined by the length of the
ulna relative to the radius (ulnar variance).The wrist, with a more positive ulnar variant,tends to be associated with a relatively thin-
ner articular disc and vice versa,46’5° which
4o number oi: discs
35 ¯
2
1
o 15 mm
FIG. 5. The distribution of values of the widthof the articular disc measured between the ulnarapex and the radial base.
FIG. 6. Cross section in sagittal plane near theradial base of the articular disc of a 40-year-oldsubject. The concavity of the ulnar surface (U) more pronounced than the concavity of the carpalsurface (C). In this plane the thicknesses of thedorsal (D) and palmar (P) margins were sured.
also influences the distribution of the loadacross the disc) In a positive ulnar variant,the compressive load through the center ofthe disc to the ulnar head is greatly in-creased,5.46-50 whereas in a negative variantmore of the force is probably converted totension)
A number of authors have confirmed thatthe most important functional role of the ar-ticular disc is in stabilizing the distal radioul-nar joint. It is not, of course, the only stabi-lizer of this joint, and there still exists somecontroversy concerning the significance of
various structures, especially the radioulnar28111215 17~331
ligaments in this function." " " - .... "40.41.49.50.54,58.62 There is no doubt that the ar-
ticular disc is ideally placed and that its shapeand structure correspond well to this biome-chanical role. In this regard the disc could beschematically divided into two zones: a pe-ripheral zone and a central zone. The periph-

128 Miki6and Related
FIG. 7. Cross section in frontal plane of the ar-ticular disc of a 38-year-old subject. In this planethe thickness of the apex (A), the radial base, andthe central zone was measured. The radial edge ofthe disc is attached here to the cartilage of theradius (R). The ulnar surface (U) is more concavethan the carpal surface (C).
eral zone is represented by the massive pal-mar and dorsal margins, which are thick,mechanically very strong, and firmly at-tached both to the radius and the ulna. Theyare often referred to as the volar and dorsal
radioulnar ligaments,9 which are incorrectbecause they are integral parts of the articu-lar disc itself. These misnomers are also con-fusing because the radioulnar ligaments areseparate structures that by themselves are tooweak to provide inherent stability of theulna; however, they are intimately attachedto the disc, and obviously both of thesestructures act simultaneously.22 Therefore,the palmar and dorsal margins, reinforced bythe radioulnar ligaments, appear to be theessential functional parts of the disc andare structurally adapted to bear tractionforces,5’9’21 the integrity of which is indis-pensable for the stability of the distal ra-dioulnar joint. The central zone of the disc,which is usually thin and often degenera-tively changed and perforated,37 is mechani-cally weak and provides negligible stability.
One interesting feature of the disc is thatits apex is fastened by two strong bands offibers, one in the basistyloid fovea and theother on the styloid process of the ulna.Loose connective tissue situated between
these two points of insertion is highly vaseu:larized, because it is linked with the vasc~foramina of the basistyloid fovea. Sometimesit is referred to as the ligamentum subcruen.
turn.~’24 That denomination is incorrect andi:should not be used because the structu~concerned is not a ligament but merely a partof the ulnar attachment of the articularIt seems to be important for the blood supplof the disc and of the prestyloid recess. Therichness of the prestyloid recess in highlycularized synovium could offer an extion for the early development of rheuma-toid changes in this area.24.~0 The foveal in-sertion of the disc is situated at the positionof the axis of the forearm rotation and pro-vides sufficient tension of the disc marginsduring the whole range of the pronosupina-tion and prevents the ulnar head from dislo-cation.9"1~’52 The traction exerted on the sty-
number o# discs
volor ~nd dorso[ edEe epex o# discsthickness o9 the rner~inel p~rts ~ in mm
F~o. 8. The distribution of values of the thick-hess of tlae volar and dorsal margins and the apexof the disc.
procachme~
impoa:
of the ar,and Jarlonger.and ulvand peduring
sigmokThe ~
atomicnectedintimaarticulz:led Paconcep-plex, irradiouI:ament.
~ carpi u
! betwee.
ulnarcess is
extens

Clinicaland
~rtion is highlyiked with the vasculold fovea, Sometigamentum subcru~,~tion is incorrect and~cause the structurelent but merely a partof the articular disfor the blood supply:
restyloid recess. Therec~ess in highly vas-
tld offer an explana.opment of rheuma.~.z4..~o The foveal in-
rated at the position:n rotation and pro-of the disc margins~f the pronosupina,~ar head from dislo,exerted on the sty-
~pex o# discs
calues of the thick-trgins and the apex
1989
process of the ulna through the disc at-~ment in abduction injuries leads toure of the styloid at its base with a con-ent instability of the distal radioulnar2t.39 Because of that, the fracture of the
mr styloid process should be considered asimportant injury of the articular disc and
t as a minor fracture.39 The ulnar insertionthe articular disc as a whole, as Mohiuddin
Janjua42 have also observed, is slightly
er than the distance between the radiusulna requires, which allows some playpermits the disc to follow the radius
Luring forearm rotation and also permits themovements of the ulnar head in the
) sigmoid notch of the radius.9
ii The articular disc is a clearly definable an-atomic entity, although it is intimately con-nected with its surrounding structures. These
intimate anatomic and functional ties of thearticular disc and the neighboring elementsled Palmer and Werner49 to introduce theconcept of the triangular fibrocartilage com-plex, incorporating the dorsal and palmar
ligaments, the ulnar collateral lig-ament, the meniscus homolog, the extensor
)i ulnaris sheath, and the articular discitself. 48-5° There is also a close relationship
the articular disc and the palmar ul-
FIG. 9. The distal articular surface of the rightof a 42-year-old subject. The border be-
tween the radial (R) and discal (D) surfaces hardly recognizable. Between the disc and theulnar collateral ligament (UCL), the prestyloid re-cess is situated, and above it is the tunnel for theextensor carpi ulnaris tendon.
Articular Disc of Distal Radioulnar Joint 129
I~IG. 10. The incisura ulnaris radii (IU) as seenon a macerated bone. At the distal ends of thedorsal (D) and palmar (P) edges of the ulnar:notch, the triangular flattened facets (F), whereLhe dorsal and palmar margins of the disc were..,attached, could be easily identified.
nocarpal ligament.5’35’36"~9 This connectionmust also have a contributory role in stabi- --lizing the distal radioulnar joint, and the pal-mar ulnocarpal ligament should also be oneof the components of the triangular fibrocar-tilage complex.~ "
The articular disc is liable to regressive al-terations that occur mostly in the thinner,central part of the disc, whereas the thickermargins are almost always saved, an impor-tant fact from a functional point ofview..Thecentral part of the disc is occasionally perfo-rated, but published accounts concerning thenature and incidence of the perforation varyconsiderably. Because the incidence of perfo-rations increases with age and all perforateddiscs show severe degenerative changes,37

130 Miki~Clinical,
and Related
3t
FIG. 1 1. The lower end of the radius of a 4:5-year-old subject (fresh specimen). The articulardisc is attached by its base to the distal edge seenbetween the ulnar (U) and lunate (L) articularfacets. The massive dorsal and palmar margins ofthe disc are attached to the triangular, flattenedfacets (F) seen on the dorsal and palmar ends-ofthis edge. There is also a low ridge between thescaphoid (S) and lunate (L) articular facets.
these changes are fundamentally of a degen-erative nature and part of the aging processe:5that could be influenced by various factors.Palmer and Werner49 have noted that rela.-
FIG. 13. The excised articular disc (D) of a 38-year-old subject with the prestyloid recess fromwhere the styloid process (S) covered by the artic-ular cartilage is protruded.
rive excess in ulnar length is associated withan increased incidence of disc perforation
and ulnolunate erosion.Calcification of the articular disc could
also be representative of the aging process,although it could indicate one of several sys-temic disease processes. It was found in only
)f ca
FIG. 12. The head of a macerated ulna seenfrom the carpal side. There is a depression (basi-styloid fovea) between the discal articular facet(D) and the massive styloid process (S)where vascular foramina could be also seen. The tip ofthe styloid process is covered by the compact,marblelike bone that is characteristic of the bonethat was covered by the articular cartilage.
FIG. 14. The interior of the ulnar part of thewrist joint viewed from the dorsocarpal side. R= radius, L = lunate, T = triquetrum, D = articu-lar disc, PUL = palmar ulnocarpal ligament. Thehead of a pin has been put into the large prestyloidrecess for size comparison. The tip of the styloidprocess covered by the articular cartilage is stand-ing out of the prestyloid recess.
19.

ticular disc (D) of prestyloid recess from
IS) covered by the
;th is associated with
; of disc
articular disc could)f the aging process,.te one of severalIt was found in
’the ulnar part of theie dorsocarpal side. Rdquetrum, D = articu-~ocarpal ligament. Theato the large prestyloidThe tip of the styloid
:ular cartilage is stand-,~ess.
2451989 Articular Disc of Distal Radiouinar Joint 131
specimen in this series. According tomer,~7 in the course of reviewing 1500
of the wrist, only two cases
,calcification of the articular disc werean incidence of less than 0.2%).
REFERENCES
Albert, S. M., Wohl, M. A., and Rechtman, A. M.:Treatment of the disrupted radio-ulnar joint. J.Bone Joint Surg. 45A:1373, 1963.Alexander. A. H.: Bilateral traumatic dislocation ofthe distal radioulnar joint, ulna dorsal: Case reportand review of the literature. Clin. Orthop. 129:238,1977.Barnett, C. H.: The structure and functions of fi-brocartilages within vertebrate joints. J. Anat.88:363, 1954.Barnett, C. H., Davies. D. V., and MacConail,M. A.: Synovial Joints. Their Structure and Me-chanics. London, Longmans. Green. 1961.Bowers. W. H.: The distal radioulnar joint. InGreen. D. P. (ed.): Operative Hand Surgery., vol. ed. 2. New York, Churchill Livingstone, 1988, p.939.
6. Coleman. H. M.: Injuries of the articular disc at thewrist. J. Bone Joint Surg. 42Bz522, 1960.
7. Dameron, T. B., Jr.: Traumatic dislocation of thedistal radio-ulnar joint. Clin. Orthop. 83:55, 1972.
8. Davidson, A. J., and Horwitz. M. T.: Recurrent orhabitual dislocation of the inferior radio-ulnar artic-ulation. Am. J. Surg. 41:115, 1938.
9. Ekenstam, F., and Hagert, C. G.: Anatomical stud-ies on the geometry and stability of the distal radioulnar joint. Scand. J. Plast. Surg. 19:17, 1985.Fick, R.: Anatomic und Mechanik der Gelenke.Jena, Fisher-Verlag, 1904.Gibson, A.: Uncomplicated dislocation of the infe-rior radio-ulnar joint. J. Bone Joint Surg. 7:180,1925.
~:.12.Graham, H. K., McCoy, G. F., and Mollan,R. A. B.: A new injury of the distal radio-ulnar joint.J. Bone Joint Surg. 67B:302, 1985.Grant, J. C. B:: A Method &Anatomy, ed. 3. Balti-more, Williams & Wilkins, 1944.Guillermo, J.: Le fibrocartilage de l’articulationradio-cubital inf~rieure chez l’adulte (En marge destraumatismes radio-carpiens). Rev. Orthop. 25:125,1938.
:15. Hagert, C. G.: Functional aspects on the distal ra-dioulnar joint. J. Hand Surg. 4:585, 1979.Hamlin, C.: Traumatic disruption of the distal ra-dioulnarjoint. Am. J. Sports Med. 5:93, 1977.HeiNe, K. G., and Freehafer, A. A.: Isolated trau-matic dislocation of the distal end of the ulna ordistal radio-ulnar joint. J. Bone Joint Surg.44A: 1387, 1962.
18.Hoegen, K., and Reske, W.: Ver~inderungen an derdreieckigen Bandscheibe des distalen Radio-Ulnar-Gelenkes. Z. Orthop. 87:525, 1956.
19.Hohman, D.: Angeborene St6rungen, Erkrankun-gen und Verletzungen des dis~alen Radio-Ulnarge-lenkes. Arch. Orthop. Unfall-Chir. 56:211, 1964.
20. Hollinshead, W. H.: Anatomy for Surgeons. TheBack and Limbs, vol. 3. New York, A. Hoeber-Harper, 1958.
21. Kapandji, I. O.: The inferior radioulnar joint andpronosupination. In Tubiana, R. (ed.): The Hand,vol. 1. Philadelphia, W. B. Saunders, 1981, p. 121.
22. Kaplan, E. B.: Functional and Surgical Anatomy ofthe Hand, ed. 2. Philadelphia, J. B. Lippincott,1965.
23, Kauer, J. M. G.: L’extension du ligament triangu-laire dans la region carpienne. Bull. Assoc. Anat.(Nancy) 142:1048, 1969.
2zl.Kauer, J. M. G.: The articular disc of the hand. ActaAnat. (Basel) 93:590, 1975.
25. Kessler, I., and Silberman, Z.: An experimentalstudy of the radiocarpal joint by arthrography. Surg.Gynec01. Obstet. 112:33, 1961.
26. Koebke, J.: A biomechanicat and morphologicalanalysis of human hand joints. Berlin, Springer-Verlag, 1983.
27. kang, F.: Das distale Radio-ulnargelenk. Hefte zurUnfallheilkunde 36:t, 1942.
28. Lewis. O. J.: Evolutionary change in the primatewrist and inferior radio-ulnar joint. Anat. Rec.151:275, 1965.
29. Lewis. O. J.: The hominoid wrist joint. Am. J. Phys.Anthrop. 30:251, 1969.
30. Lewis, O. J., Hamshere, R. J., and Bucknill, T. M.:The anatomy of the wrist joint. J. Anat. 106:539,1970.
3l. Lippman, R. K.: Laxity of the radio-ulnar joint fol-lowing Colles" fracture. Arch. Surg. 35:772, 1937.
32. MacConail, M. A.: The function of the intra-articu-lar fibrocartilages, with special reference to the kneeand inferior radio-ulnar joints. J. Anat. 66:210,1931.
33. Martinek, H., and Sp/ingler, H.: Zur Traumatologiedes Discus Articularis des Handgelenkes, 2. Teil:Operative Behandlung und Ergebnisse. Arch.Orthop. UnfalI-Chir. 87:299, 1977.
34. Mayer, J. H.: Colles’s fracture. Br. J. Surg. 27:629,1940.
35. Mayfield, J. K., Johnson, R. P., and Kilcoyne. R. F.:--The ligaments of the human wrist and their func-tional significance. Anat. Rec. 186:417, 1976.
36. Miki6, Z. D.: Galeazzi fracture-dislocation. J. BoneJoint Surg. 57A:I071, 1975.
37. Miki6, ~. D.: Age changes in the triangular fibro-cartilage.of the wrist joint. J. Anat. 126:367, 1978.
38. Miki6, ~. D.: Arthrography of the wrist joint. Anexperimental study. J. Bone Joint Surg. 66A:371,1984.
39. Miki6, 2;, Somer, T., Szfip, D., V~kony, N., andBampa-~ef~i6, G.: Injury of the carpal disc in frac-tures of the distal radial end. Magy. Traumatol.27:175, 1984.
40. Milch, H.: Dislocation of the inferior end of theulna. Suggestion for a new operative procedure.Am. J. Surg. 1:141, 1926.
41. Milch, H.: So-called dislocation of the lower end ofthe ulna. Ann. Surg. 1 t6:282, 1942.
42. Mohiuddin, A., and Janjua, Z. M.: Form and func-tion ofradioulnar articular disc. Hand 14:61, 1982.
43. Moore, T. M., Lester, D. K., and Sarmiento, A.: The

132 Miki~
andstabilizing effect of so’tissue constraints in artifi-cial Galeazzi fractures. Clin. Orthop. 194:189, 1985.
44. M6rike, K. D.: Zur Herkunft und Functio~t des ul-naren Diskus am Handgelenk. Morph. Jb. 105:365,1964.
45. Morrissy, R. T., and Nalebuff. E. A.: Dislocation ofthe distat radioulnar joint: Anatomy and clues toprompt diagnosis. Clin. Orthop. 144:154, 1979.
46. Palmer, A. K., Glisson, R. R., and Werner, F. W.:Ulnar variance determination, j. Hand Surg. 7:376,1982.
47. Palmer, A. K., Glisson, R. R., and Werner, F. W.:Relationship between ulnar variance and trinngularfibrocartilage complex thickness. J. Hand Surg.9A:681, 1984.
48. Palmer, A. K., Linscheid, R. k., Fisk, G. R.., andTaleisnik, J.: Symposium: Distal ulnar iniuriesContemp. Orthop. 7:81, 1983. "
49. Palmer, A. K., and Werner, F. W.: The triangularfibrocartilage complex of the wrist--anatomy andfunction. J. Hand Surg. 6:153, 1981. "
50. Palmer, A. K., and Werner, F. W.: Biomechanics ofthe distal radioulnar joint. Clin. Orthop. 187:26,1984.
51. Poirier, p., and Charpy. A.: Trait6 d’Anatomie Hu-maine. Paris, Massom 191 I.
52. Ray, R. D., Johnson, R. J., and Jamesson, R. M.:Rotation of the forearm. J. Bone Joint Surg.33A:993. 195 I.
53. Rieunau, G., Gay, R., Martinez, C., Mansat, C., andMansat, M.: L~sions de l’articulation radio-cubitaleinf~rieure dans les traumatismes de l’avant-bras et
du poignet. Int~ret de l’arthrographie.Orthop. [Suppl.J 57:253, 1971.
54. Rose-Innes, A. P.: Anterior dislocation,at the inferior radio-ulnar joint, j. Bone42B:515, 1960.
55. Rosenthal, A.: Die Verletzung des Discu:bei der typischen Radiusfraktur. Arch.262:390, 1949.
56. Sik, J.: Isolierte Sportverletzung des Discularis (triangularis) im Handgelenk. Kli~(Mosk.) 18:369, 1963.
57. Spinner, M.: Calcification of the triangularof the wrist. Bull. Hosp. Jt. Dis. 32:21, 197
58. Spinner, M., and Kaplan, E. B.: Extensornaris: Its relationship to the stability of 1
radio-ulnar joint. Clin. Orthop. 68:1 z~4, 19759. Taleisnik. J.: The ligaments of the wrist. J.Surg. i:110, 1976.
60. Taylor, G. W., and Parsons, C. L.: The role .....discus articularis in Colles’ fracture. J. Bo!Surg. 20:149, 1938.
61. Testut, L.: Trait~ d’Anatomie Humaine.Doin, 1904.
62. Vesely, D. G.: The distal radio-ulnar joint.Orthop. 51:75, 1967.
63. yon Lanz, T., and Wachsmuth, W.: Praktischlatomic. Berlin, Springer, 1935.
64. Weigh, K., and Spira, E.: The triangularlage of the wrist joint. Reconstr. Surg.11:139, 1969.
65. Williams, p. L., and Warwick, R.: Gra
ed. 36. Edinburgh, Churchill Livingstone, 1980