Embed Size (px)
Citation preview

Ultrasound in the forefootRAD Magazine, 41, 480, 18-20
Andrew CarneConsultant MSK radiologist
Nicki DelvesSpecialist MSK sonographer
Matthew SolanConsultant orthopaedic foot and ankle surgeon
Emma WoodConsultant MSK radiologist
Department of Radiology, Royal Surrey County Hospitalemail: [email protected]
IntroductionFoot pain is one of the most common musculo-skeletal complaints encountered. It affects nearlyone in five of people in the community, is associated with increased age, female sex, obesityand pain in other body regions. It has a signifi-cant detrimental impact on health-related qualityof life.
The majority of scans that we are asked to perform are to aid in the differential diagnosisand management of metatarsalgia. Metatarsalgiais pain in the ball of the foot. It is usually felt in the sole of the foot and is often described asbeing like “walking on pebbles”. Other people feel a more diffuse vague pain, ache or burning.Some people experience symptoms around onlyone or two toes, others have it throughout one orboth feet.
Ultrasound is the imaging modality of choice in our insti-tution. We take referrals from a combination of GPs, MSKtriage pathways and dedicated foot and ankle surgeons.Scans are then performed by either MSK radiologists orMSK sonographers.
Several pathologic conditions produce pain in the regionof the metatarsal bones and the cause may be difficult toestablish based solely on clinical findings. Although conven-tional radiography is still useful in detecting bone lesionsand showing the underlying foot architecture, it typicallydoes not help the diagnosis of early joint abnormalities orsoft-tissue disease causing forefoot pain.
What causes metatarsalgia? As clinical sonographers and radiologists our role includestaking a clinical history and performing a clinical examina-tion. Although the orthopaedic foot and ankle surgicaldepartment will have their established management path-ways that we, as diagnosticians, should be familiar with,many referrals will come directly from primary care andgeneral practitioners who will welcome onward managementadvice. We should not shy away from giving patients andtheir referring clinical colleagues advice, even if a manage-ment plan is limited to a referral to physiotherapy. In ourinstitution we have several one-stop clinics and these are avaluable learning opportunity, helping us to better under-stand the management options for patients. This type ofknowledge sharing should be actively encouraged.
Anything which puts extra stress on the front of the foot,resulting in forefoot overload, can lead to metatarsalgia.Common examples are:• obesity
• a tight calf due to a gastrocnemius contracture• hallux valgus or rigidus that can weaken the big toe and
throw extra stress onto the ball of the foot. This can alsohappen after an operation on the big toe, such as abunion correction
• certain foot shapes, particularly cavus foot, claw or ham-mer toes
• a stiff ankle• a stretched or irritated nerve in the ball of the foot (inter-
digital neuroma) or behind the ankle (tarsal tunnel syn-drome) can produce pain in the ball of the foot
• diabetes can produce problems with the small nerves inthe foot leading to a burning pain
• athletes or walkers occasionally get stress fractures of themetatarsal bones
• systemic inflammatory diseases affecting the forefootcover a wide range of pathologic conditions, includingrheumatoid arthritis, gout, Reiter’s disease and psoriasis
• high-heeled shoes.
Extended ultrasoundGenerally in musculoskeletal ultrasound, but specifically inthe forefoot, sonographers and radiologists should rise to thediagnostic challenge and take on greater clinical responsi-bility. It is not sufficient to simply say “no abnormalityfound”. We should understand the clinical possibilities anddiagnostic pathways involved in assessing the forefoot. Thisarticle outlines our protocol for the forefoot. The main advan-tage diagnostic ultrasound has over other imaging modalitiesis the ability to dynamically evaluate the patient while scan-ning (figure 1). We would also encourage you to offer a planby suggesting the best diagnostic pathway when a specificultrasound diagnosis cannot be made.
In order to evaluate the patient with a musculoskeletalproblem you can take either a targeted approach, eg lookfor a neuroma, or a more systematic (anatomical or clinical)approach, eg evaluate the structures in the region of inter-est. The latter requires an understanding of ultrasoundanatomy and the clinical differential diagnosis.Understanding all the clinical possibilities (not just thoseidentified on ultrasound) not only enhances the scanningprocess but gives us the opportunity to suggest an alterna-tive diagnosis by a process of exclusion.
The recommendations of this article are to undertake asystematic approach as even the most experienced clinicianscan be misled by symptoms. Every experienced radiologistwill have encountered synovitis or stress fracture mimickingthe presentation of a Morton’s neuroma.
Protocolled scanning• Always use a high resolution transducer, preferably with
a frequency of at least 15MHz, and if you are performinginjections then a hockey stick probe is often helpful
• The patient should initially be supine with the knee bentand the foot flat on the couch
• Scan the metatarsal bones longitudinally looking for evi-dence of callus formation or periosteal reaction to excludea stress fracture
• Scan the metatarsophalangeal (MTP) joints looking forsynovitis and/or erosive changes
• Straighten the knee and look at the plantar skin andscan the distal plantar fascia
• Examine the plantar plates, sesamoids and flexor tendonswhile passively hyperextending and flexing the toes
• Look between the metatarsal heads at the interdigitalnerves and the intermetatarsal bursae. This is easiest ifdone longitudinally balloting the interdigital spacebetween the transducer and a finger on the dorsum ofthe forefoot
• Consider scanning the tarsal tunnel and the contralateralfoot.
Ultrasound in the forefoot.qxp_Master-article 11/05/2015 13:47 Page 1
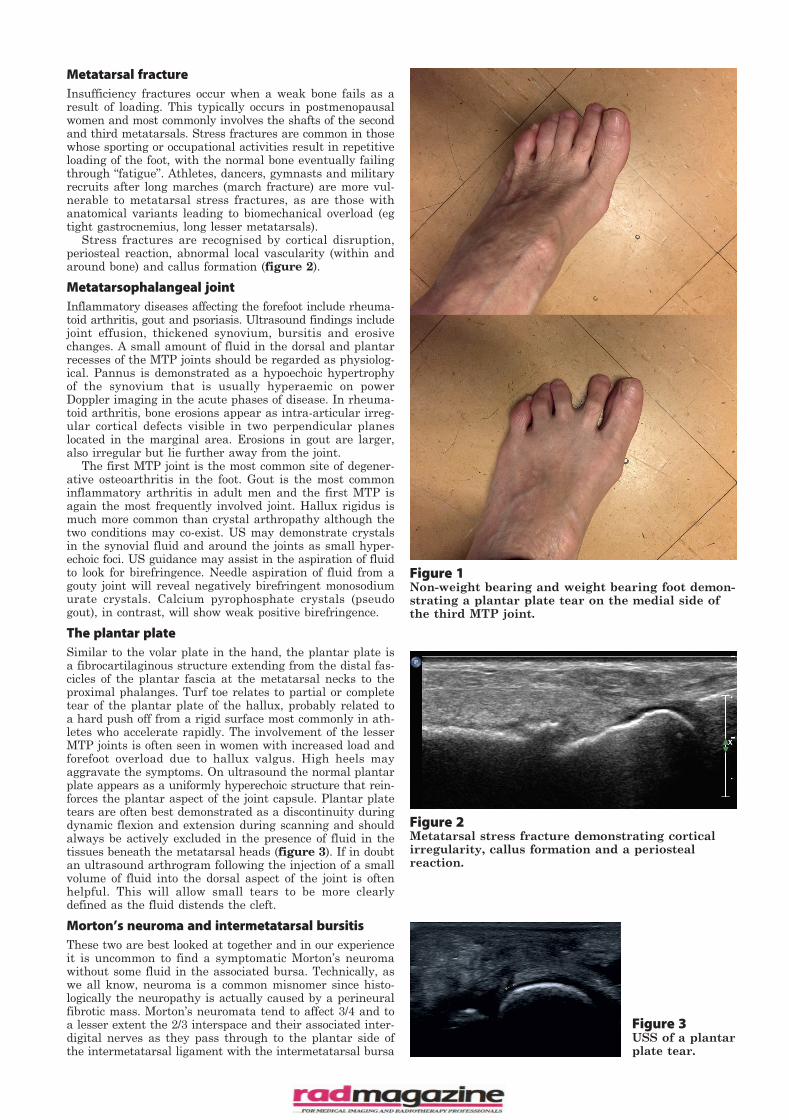
Figure 3USS of a plantarplate tear.
Metatarsal fractureInsufficiency fractures occur when a weak bone fails as aresult of loading. This typically occurs in postmenopausalwomen and most commonly involves the shafts of the secondand third metatarsals. Stress fractures are common in thosewhose sporting or occupational activities result in repetitiveloading of the foot, with the normal bone eventually failingthrough “fatigue”. Athletes, dancers, gymnasts and militaryrecruits after long marches (march fracture) are more vul-nerable to metatarsal stress fractures, as are those withanatomical variants leading to biomechanical overload (egtight gastrocnemius, long lesser metatarsals).
Stress fractures are recognised by cortical disruption,periosteal reaction, abnormal local vascularity (within andaround bone) and callus formation (figure 2).
Metatarsophalangeal jointInflammatory diseases affecting the forefoot include rheuma-toid arthritis, gout and psoriasis. Ultrasound findings includejoint effusion, thickened synovium, bursitis and erosivechanges. A small amount of fluid in the dorsal and plantarrecesses of the MTP joints should be regarded as physiolog-ical. Pannus is demonstrated as a hypoechoic hypertrophyof the synovium that is usually hyperaemic on powerDoppler imaging in the acute phases of disease. In rheuma-toid arthritis, bone erosions appear as intra-articular irreg-ular cortical defects visible in two perpendicular planeslocated in the marginal area. Erosions in gout are larger,also irregular but lie further away from the joint.
The first MTP joint is the most common site of degener-ative osteoarthritis in the foot. Gout is the most commoninflammatory arthritis in adult men and the first MTP isagain the most frequently involved joint. Hallux rigidus ismuch more common than crystal arthropathy although thetwo conditions may co-exist. US may demonstrate crystalsin the synovial fluid and around the joints as small hyper-echoic foci. US guidance may assist in the aspiration of fluidto look for birefringence. Needle aspiration of fluid from agouty joint will reveal negatively birefringent monosodiumurate crystals. Calcium pyrophosphate crystals (pseudogout), in contrast, will show weak positive birefringence.
The plantar plateSimilar to the volar plate in the hand, the plantar plate isa fibrocartilaginous structure extending from the distal fas-cicles of the plantar fascia at the metatarsal necks to theproximal phalanges. Turf toe relates to partial or completetear of the plantar plate of the hallux, probably related toa hard push off from a rigid surface most commonly in ath-letes who accelerate rapidly. The involvement of the lesserMTP joints is often seen in women with increased load andforefoot overload due to hallux valgus. High heels mayaggravate the symptoms. On ultrasound the normal plantarplate appears as a uniformly hyperechoic structure that rein-forces the plantar aspect of the joint capsule. Plantar platetears are often best demonstrated as a discontinuity duringdynamic flexion and extension during scanning and shouldalways be actively excluded in the presence of fluid in thetissues beneath the metatarsal heads (figure 3). If in doubtan ultrasound arthrogram following the injection of a smallvolume of fluid into the dorsal aspect of the joint is oftenhelpful. This will allow small tears to be more clearlydefined as the fluid distends the cleft.
Morton’s neuroma and intermetatarsal bursitisThese two are best looked at together and in our experienceit is uncommon to find a symptomatic Morton’s neuromawithout some fluid in the associated bursa. Technically, aswe all know, neuroma is a common misnomer since histo-logically the neuropathy is actually caused by a perineuralfibrotic mass. Morton’s neuromata tend to affect 3/4 and toa lesser extent the 2/3 interspace and their associated inter-digital nerves as they pass through to the plantar side ofthe intermetatarsal ligament with the intermetatarsal bursa
Figure 2Metatarsal stress fracture demonstrating corticalirregularity, callus formation and a periosteal reaction.
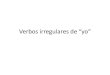
Figure 1Non-weight bearing and weight bearing foot demon-strating a plantar plate tear on the medial side ofthe third MTP joint.
Ultrasound in the forefoot.qxp_Master-article 11/05/2015 13:47 Page 2

situated just dorsal to it.Scanning techniques vary between users but since an US-
guided injection is often performed at the time of the scanwe prefer to scan longitudinally from the plantar surfacewith a hockey stick probe. This allows easy balloting fromabove and makes single-handed scanning and injectingthrough the webspace very easy to perform (figure 4).
US-guided injection of steroid in the forefoot is best per-formed with a premixed formulation so that volume of injec-tate is minimal in order to reduce pain.
Bursitis is compressible, deformable and more heteroge-neous in echogenicity. It has a variety of shapes, sizes andlocations and often has a close relationship with one of theMTP joints (and may communicate with it though this isoften difficult to prove with images). As already mentioned,beware that neuromas and bursitis often coexist and appearto occur together much more frequently than expected bychance alone – suggesting common aetiological factors.
Morton’s neuromata are incompressible, less hypoechoicand it is often possible to visualise the normal afferent inter-digital nerve with fusiform expansion around and insepara-ble from it at the point of maximal tenderness.
SummaryUltrasound of the forefoot is a quick and rewarding test buta variety of differential diagnoses should always be consid-ered. We recommend that you develop relationships with
your referrers to fully understand their requirements andavoid inconclusive reports without a suggestion of any addi-tional appropriate imaging.
Figure 4Single handed technique for scanning the inter-metatarsal space using a 15MHz hockey stick probe.
Ultrasound in the forefoot.qxp_Master-article 11/05/2015 13:47 Page 3