Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Underestimation of papillary breast lesions by core biopsy:correlation to surgical excision
Stamatia Destounis • Posy Seifert • Patricia Somerville •
Philip Murphy • Renee Morgan • Andrea Arieno •
Wende Logan Young
Received: 11 January 2012 / Accepted: 7 March 2012
� The Japanese Breast Cancer Society 2012
Abstract
Background The purpose of this study was to evaluate
papillary lesions of the breast diagnosed at needle core
biopsy and the outcomes of follow-up imaging and surgical
findings.
Methods Retrospective review of 13,806 needle core
biopsies performed from 2004 to 2010 revealed 352
patients with 368 papillary lesions; 137 of these lesions
underwent surgical excision and 215 had a minimum of
2 year imaging follow-up. Outcomes of imaging follow-up
and underestimation of carcinoma by comparison to sur-
gical excision, as applicable, were determined. Patient
demographics, clinical presentation, BI-RADS� breast
density, palpability, biopsy methods, number of specimens,
and pathology were recorded. A two-tailed Fisher exact test
was used to assess associations between biopsy techniques
and the results of surgical excision as well as the associa-
tion between palpability and the results of surgical exci-
sion. SAS� V 9.1.3 was used to perform the calculations.
Results One hundred and thirty-seven lesions proceeded
to surgical excision. A total of 28 lesions were underesti-
mated; 21 of these were underestimated carcinomas. When
comparing biopsy devices in the underestimated group,
64 % were biopsied with directional vacuum-assisted
devices and 36 % with automated large core devices
(p \ 0.0706). In total 18 % of the palpable lesions were
underestimated, whereas 17 % of the nonpalpable lesions
were underestimated (p \ 0.6560); this was not a signifi-
cant difference.
Conclusions Overall, carcinoma was underestimated at
needle biopsy in 6 % (21/368) of papillary lesions diag-
nosed when compared to surgical excision. In cases that
underwent excision, 34 % (47/137) revealed carcinoma;
45 % (21/47) of these were underestimated carcinomas.
Lesion palpability and biopsy method did not affect
underestimation in this study population.
Keywords Breast imaging � Papillary lesions �Underestimation � Core needle biopsy
Introduction
Single or multiple papillary lesions are uncommon, found
in up to 5 % of biopsies [1], and can be found in any area
of the breast. These lesions at core biopsy result in a wide
range of findings, including benign without atypia, benign
with atypia, papillary ductal carcinoma in situ (DCIS), or
papillary invasive malignancy. Reports describe that pap-
illary malignancies can have areas of benign features,
whereas benign papillomas can have areas of mitoses
resembling atypia and carcinoma [2]. As a consequence,
papillary findings at core needle biopsy (CNB) remain
controversial and excision is not always recommended.
Studies have shown that papillary lesions found at CNB
can be underestimated carcinomas, suggesting that all
papillary lesions diagnosed at CNB should be excised
[3–12]. Conversely, other studies suggest that follow-up of
benign without atypia at CNB is a reasonable management
choice for the patients [13–18]. Our practice protocol is to
follow lesions diagnosed as benign without atypia at CNB
in asymptomatic patients rather than recommend open
surgical biopsy (OSB). OSB is recommended for lesions
diagnosed with atypia, malignancy, or if the patient is
S. Destounis (&) � P. Seifert � P. Somerville � P. Murphy �R. Morgan � A. Arieno � W. L. Young
Elizabeth Wende Breast Care, LLC., 170 Sawgrass Dr.,
Rochester, NY 14620, USA
e-mail: [email protected]
123
Breast Cancer
DOI 10.1007/s12282-012-0361-2

symptomatic, such as having persistent spontaneous dis-
charge, enlarging palpable lump, or worsening pain. The
purpose of this review was to identify the incidence and
circumstance of pathological underestimation of carcino-
mas at CNB initially diagnosed as papillary lesions.
Materials and methods
This institutional review board approved retrospective
review was conducted in compliance with Health Infor-
mation Portability and Accountability Act. Patient consent
was not required. A total of 13,806 CNBs from January
2004 to December 2010 were identified from an electronic
medical records database at an outpatient facility special-
izing in breast imaging. A comprehensive chart review
identified 352 patients with 368 papillary lesions, which
included papilloma, intraductal papilloma, atypical papil-
loma, papilloma with atypia, papillary neoplasm, papil-
loma with DCIS, papillary DCIS, encapsulated papillary
carcinoma, and solid papillary carcinoma, that fit the study
criteria. Further review demonstrated 137 lesions which
underwent surgical excision and 215 who had imaging
follow-up. If surgical excision was not performed, a min-
imum of 2 years of imaging follow-up was required for
inclusion in the study analysis. In the surgically excised
group, further analysis concentrated on underestimation.
Overestimation was not analyzed as the lesions were
determined to be completely excised at CNB. Study
information collected included patient demographics,
BI-RADS� breast density, lesion characteristics, core biopsy
information, histopathological results, and results of fol-
low-up.
Core needle biopsy procedure
Core needle biopsy procedures were performed by breast
imaging specialists with years of experience ranging from
6 to 35 years (average 12) utilizing stereotactic, ultrasound,
or magnetic resonance imaging (MRI) guidance. Auto-
mated large core (ALC) devices with 14-gauge needles or
directional vacuum-assisted (DVA) devices with 14-, 12-,
or 9-gauge needles were used. Image guidance, biopsy
device, needle size, and number of specimens were selec-
ted on the basis of considerations that included the char-
acteristics of image findings such as type (mass,
calcifications, architectural distortion), size, location, and
palpability, preference of the radiologist, and health con-
cerns of the patient. All CNB procedures were performed
using the facility’s standard operating procedures. Stereo-
tactic core biopsy was performed using a Hologic DSM
prone stereotactic table (LoRad; Hologic, Bedford, MA,
USA). Ultrasound-guided biopsy was performed utilizing
one of the following units: Siemens Antares (Siemens
Medical Solutions USA, Inc., Malvern, PA, USA), Philips
iU22 system (Philips Healthcare, Bothell, WA, USA), or
GE Logiq (GE Healthcare, Milwaukee, WI, USA). The
MRI-guided biopsies were performed on a 1.5-T GE
Echospeed (GE Healthcare) or a 1.5-T Siemens Symphony
(Siemens Medical Solutions USA, Inc.) equipped with a
dedicated surface breast coil. DVA biopsy was performed
using a Suros ATEC or Suros Celero (Hologic, Inc.), as
well as the Mammotome ST system (Ethicon Endo-Sur-
gery, Cincinnati, OH, USA). ALC biopsy utilized either
Manan (Manan Medical Products, Wheeling, IL, USA) or
Bard (CR Bard, Inc., Murray Hill, NJ, USA).
CNB pathology was submitted to one of three local
laboratories for interpretation, depending on insurance
carrier of the patient. The majority, however, were sent to
one lab where six breast pathologists reviewed all cases.
The experience of the pathologists ranged from 4 to
30 years (average 17 years) where a daily conference for
case review was conducted.
All CNB results were reviewed by the attending radi-
ologist for concordance with imaging findings. Recom-
mendation for OSB or follow-up depended upon the core
pathology results and clinical presentation. If the core
pathology results were discordant with imaging and/or
pathology revealed atypia or malignancy, OSB was rec-
ommended. For benign without atypia findings in asymp-
tomatic patients, the patient was instructed to return in
6 months for follow-up examination. For study purposes,
an asymptomatic patient was defined as ‘‘no symptoms;
such as enlarging lump, enhancing mass, or nipple dis-
charge.’’ A subset of patients was recommended for OSB
despite benign findings as a result of clinical presentation
such as continued nipple discharge. Surgical results for
these patients were requested and then also compared with
imaging findings and CNB pathology results by the
attending radiologist.
Statistical analysis
To assess the associations between biopsy techniques and the
results of surgical excision, a two-tailed Fisher exact test was
used. The same test was used for the association between
palpability and the results of surgical excision. SAS� V 9.1.3
was used to perform the calculations. An alpha (a) level of
\0.05 was used to determine significance.
Results
One hundred and thirty-seven lesions diagnosed at CNB
proceeded to surgical excision. Two hundred and fifteen
patients with benign findings at CNB were recommended
Breast Cancer
123

for imaging follow-up, which could include mammo-
graphic, sonographic, or MRI imaging. Follow-up ranged
from 2 to 6 years, with an average of 3.8 years. Three
ipsilateral cancer diagnoses and one contralateral cancer
diagnosis have been made in follow-up, all of which were
in different quadrants from the papillary lesion. One
atypical finding and three benign findings in the ipsilateral
breast have been made. Additionally, one atypical finding
and five benign findings in the contralateral breast have
been made.
Patient demographics and clinical characteristics, as
well as imaging findings of the 137 lesions that proceeded
to surgical excision, are shown in Tables 1 and 2. CNB was
performed on all 137 lesions. DVA was utilized for 78 %
(n = 107) of biopsies with a 9-, 12-, or 14-gauge needle
with an average of 7.8 samples taken. The remainder
(22 %, n = 30) utilized an ALC device with a 14-gauge
needle, with an average of 3.1 samples taken. Ultrasound-
guided biopsy was performed for 53 % (n = 73); 43 %
(n = 59) of the lesions were biopsied stereotactically and
MRI guidance was used for 4 % (n = 5). At CNB, 53 of
the lesions had a benign diagnosis, 52 were atypical, and 32
malignant.
Upon surgical excision, a total of 81/137 (59.1 %)
diagnoses remained the same; 44/81 (54.3 %) of these were
benign, 11/81 (13.6 %) atypical, and 26/81 (32.1 %)
malignant. Comparison between CNB and OSB diagnoses
is shown in Table 3. Of the 53 benign lesions diagnosed at
CNB that were excised, 9 had an upgraded diagnosis; 7 to
atypia and 2 to malignancy (both in situ carcinoma). Fifty-
two atypical lesions were diagnosed at CNB and of those,
19 upgraded to carcinoma; 13 in situ (Figs. 1, 2) and 6
invasive. In total, 28 lesions were upgraded at surgical
excision; 21 (15 %) of these were upgraded to carcinoma.
Underestimated lesions
Of the 20.4 % (n = 28/137) that had an upgraded diag-
nosis at surgery, 25 % (n = 7) went from benign to atyp-
ical, 7 % (n = 2) benign to malignant, and 68 % (n = 19)
atypical to malignant. Eight of the 28 underestimated
lesions were palpable on physical examination and 11
reported discharge upon presentation. Of the 28 underes-
timated lesions, 1 occurred in a fatty breast (3.57 %), 13 in
scattered fibroglandular tissue (46.43 %), 7 in heteroge-
neously dense tissue (25 %), and 7 in extremely dense
tissue (25 %). Eighteen lesions (64 %) were biopsied with
DVA with an average of 9 samples (range 3–12) and 10
(36 %) with ALC, with an average of 3 samples retrieved
(range 1–5).
Specifically, of the 21 underestimated malignancies, 16
lesions presented as a mass at imaging, 10 were visualized
Table 1 Demographic and clinical characteristics of OSB cohort
(n = 130 patients, 137 lesions)
Characteristic Number of subjects Percent
Age, years (n = 130)
18–35 4 3.08
36–45 21 16.15
46–55 24 18.46
56–65 35 26.92
66–75 31 23.85
76? 15 11.54
Reason for presentation (n = 137)
Screening 38 27.74
Diagnostic 99 72.26
Breast density (n = 129)a
Fatty 6 4.62
Scattered 49 37.69
Heterogeneously dense 43 33.08
Extremely dense 31 23.85
Palpability (n = 137)
Nonpalpable 88 64.23
Palpable 45 32.85
Not performed 4 2.92
Discharge (n = 137)
Present 48 35.03
Not present 89 64.96
a Breast density was not available for one patient
Table 2 Imaging findings
Characteristic Number of subjects Percent
Imaging findings
Mass 92 67.15
Calcifications 7 5.12
Mass with calcium 5 3.65
Architectural distortion 1 0.73
Dilated duct/ductal enhancement 2 1.46
MRI enhancement 1 0.73
Filling defects 29 21.17
Total 137 100.00
Table 3 Comparison of histological findings from CNB and OSB
CNB findings OSB findings
Benign
without atypia
Benign
with atypia
Malignant
papillary
Benign without atypia 44 7 2
Benign with atypia 22 11 19
Malignant papillary 4 2 26
Breast Cancer
123

on both mammography and ultrasound; 4 of the 21 malig-
nancies were palpable. Three presented as filling defects
and all were seen on ductography only. Two calcifications
were seen on mammography only. Six of the patients pre-
sented with discharge. When looking at the breast density
composition of the 21 underestimated malignancies, 1 was
found in fatty tissue, 11 in scattered, 4 in heterogeneously
dense, and 5 in extremely dense. Biopsy methods of the
underestimated cancers are shown in Table 4.
Benign papillary lesions without atypia
with and without surgical excision
A total of 215 patients with a benign without atypia CNB
diagnosis were followed up with imaging, and a total of 53
with a benign without atypia diagnosis at CNB were rec-
ommended for surgical excision. In the group of patients
with imaging follow-up, the average patient age was
56 years (range 29–88). Palpability was reported in 209
cases with 19 lesions being palpable and 190 nonpalpable.
Discharge was present in 112 cases. In the group of patients
who had surgery the average age was 54 (range 18–78).
Fifteen lesions were palpable and 36 were nonpalpable; 2
did not have physical exam. Discharge was reported in 34
cases. A breakdown of lesion type for both groups is shown
in Table 5.
Discussion
Reported underestimation rates in the literature range from
6 to 39 % [19]; our findings are in line with such reports as
within the OSB cohort, we found a 20 % (28/137) under-
estimation rate. Our study findings indicated that benign
papillary lesions with atypia diagnosed at CNB had the
lowest accuracy rate (21 %), as a majority (68 %) of the
upgrades in our study came from this group. Many other
studies have had similar findings in regards to papillary
lesions with atypia having a high association with malig-
nancy at OSB [1, 3, 11, 13, 14, 17, 19]. Benign papillary
lesions at CNB had the highest accuracy rate (83 %), fol-
lowed by malignant papillary lesions (81 %).
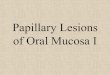
Fig. 1 A 77-year-old presented
for screening mammogram
(a, b). Mass-like areas were
identified (a–c, arrow).
Ultrasound (d) revealed a
hypoechoic mass. Ultrasound-
guided 14-gauge ALC was
performed, which revealed
papillary neoplasm. OSB
pathology revealed DCIS
Breast Cancer
123

When evaluating several variables to determine a cor-
relation to underestimation of carcinoma, we looked at
biopsy method, lesion palpability, and biopsy device. We
did not find any of these variables to be indicators of
underestimation in this study population. Ciatto et al. [20]
published a study of accuracy and underestimation of
malignancy with over 4,000 biopsies and concluded that
image-guidance method or lesion palpability did not sub-
stantially affect accuracy.
Of the 59 stereotactic guided biopsies that went to sur-
gery, underestimation was noted in 15 (25 %). Of the 73
ultrasound-guided biopsies, underestimation was noted in
12 (16 %). One underestimation was noted of the 5 MRI-
guided biopsies (20 %). Image guidance did not seem to be
a significant factor in underestimation. Arora et al. [19]
also determined that image guidance did not seem to be
associated with underestimation.
Palpability also was not a factor influencing underesti-
mation. Eighteen percent (n = 8/45) of the palpable lesions
were underestimated, whereas 17 % (n = 15/88) of the
nonpalpable lesions were underestimated (p \ 0.6560);
this was not a significant difference.
When comparing biopsy devices in the underestimated
group, we found that 64 % were biopsied with DVA and
36 % with ALC (p \ 0.0706). This does not support that
biopsy device is an influencing factor of underestimation.
When reviewing the underestimated cancers, we found that
52.38 % (n = 11/21) were biopsied with DVA and
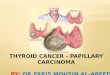
Fig. 2 A 76-year-old presented with a palpable mass in the left breast
at 5 o’clock. A mass was identified on mammography (a LCC;
b LMLO). Ultrasound revealed a partially cystic mass (c). Ultra-
sound-guided 12-gauge DVA revealed papillary neoplasm. Surgical
excision yielded multiple foci of DCIS
Table 4 Underestimated cancerous lesions and CNB methods
Characteristic Number of subjects Percent
Stereo 10 47.62
9 DVA 2 20.00
12 DVA 5 50.00
14 ALC 3 30.00
Ultrasound 10 47.62
12 DVA 3 30.00
14 ALC 7 70.00
MRI 1 4.76
9 DVA 1 100.00
Total 21 100.00
Table 5 Lesion type of benign without atypia lesions with and
without surgery
Characteristic Benign without
surgery
Benign with
surgery
Imaging findings
Mass 93 25
Calcifications 37 2
Mass with calcium 7 1
Architectural distortion 5 1
Dilated duct/ductal enhancement 2 1
MRI enhancement 1 0
Filling defects 70 23
Total 215 53
Breast Cancer
123

47.62 % (n = 10/21) with an ALC device. More specifi-
cally, we found a higher percentage of underestimations in
the group with lesions biopsied under ultrasound guidance
with a 14-gauge ALC device, which had an average of 3
samples taken (range 1–5). A previously published work
from our facility reviewed outcomes of 9- and 12-gauge
CNBs and found no difference. The analysis found 8.00 %
underestimation for the 12-gauge group and 8.24 % for the
9-gauge group. These results continue to support our cur-
rent practice of utilizing either needle gauge [21]. Other
studies have also evaluated the difference between devices
and found a range of results. Houssami and colleagues [22]
reported that (11-gauge) vacuum-assisted devices were
significantly less prone to underestimation than (14-gauge)
automated devices and go on to say that using larger core-
needle devices does reduce underestimation to an extent,
but does not eliminate the problem completely. Addition-
ally Philpotts et al. [23] reported no significant difference
between outcomes of (ultrasound-guided) DVA verses
ALC in terms of missed cancers, underestimations, com-
plications, or need for immediate second biopsy. Liberman
et al. [17] found that ALC was accurate with benign lesions
but still stated that OSB was indicated for atypia and
papillary DCIS, which supports our findings.
A large population of patients in this study were rec-
ommended for follow-up rather than OSB when a benign
CNB diagnosis was made. Overall, this proved to be the
correct approach for these patients within the follow-up
cohort; however, we did have three patients with sub-
sequent cancer diagnoses in the ipsilateral breast. These
cancers were located in different quadrants of the breast
and thus did not arise from the papillary lesion. Several
published studies have determined that follow-up of benign
lesions without atypia is adequate and excision is not
necessary. Syndor et al. [13] reported that 25 benign pap-
illary lesions diagnosed at CNB had a minimum of
24 month follow-up with no interval change. Similarly,
Rosen et al. [1] reported that 29 patients with mammo-
graphic follow-up were all found to be stable or had
decreased lesion size during the follow-up period. Mercado
and colleagues [12] found benign without atypia lesions
upgraded to atypia or cancer in 21 % of cases (9/42) and
recommend surgical excision because of the number of
upgrades. Our findings demonstrated that, for the majority
of benign papillary lesions without atypia, imaging follow-
up was appropriate.
Conclusion
Overall, we found a 20 % underestimation rate in the
patient cohort that had surgical excision. As a result of the
high upgrade rate for atypical papillary lesions we feel it is
necessary to recommend surgical excision when such a
diagnosis is made at CNB. Benign papillary lesions in
asymptomatic patients do not need to be surgically excised,
as we found these lesions at CNB had the highest accuracy
rate (83 %); however, close imaging surveillance is
required. Biopsy device, biopsy method, and lesion pal-
pability were not found to be significant indicators of
underestimation.
Acknowledgments The authors wish to thank Karen Ahlstrom,
Anne Horan, Rena Blair, Mary Ventrella, Dawn Riedy, MD and
David Cavanaugh, MA for their contributions to this manuscript.
References
1. Rosen EL, Bentley RC, Baker JA, Soo MS. Imaging-guided core
needle biopsy of papillary lesions of the breast. AJR. 2002;179:
1185–92.
2. Rosen PP, Hoda SD. Breast pathology: diagnosis by needle core
biopsy. 2nd ed. Philadelphia: Lippincott Williams & Wilkins;
2006.
3. Tseng HS, Chen YL, Chen ST, Wu YC, Kuo SJ, Chen LS, et al.
The management of papillary lesion of the breast by core needle
biopsy. EJSO. 2009;35:121–4.
4. Bernik SF, Troob S, Ying BL, Simpson SA, Axelrod DM, Siegel
B, et al. Papillary lesions of the breast diagnosed by core needle
biopsy: 71 cases with surgical follow-up. Am J Surg. 2009;
197:473–8.
5. Jaffer S, Nagi C, Bleiweiss IJ. Excision is indicated for intra-
ductal papilloma of the breast diagnosed on core needle biopsy.
Cancer. 2009;115:2837–43.
6. Skandarajah AR, Field L, Mou AYL, Buchanan M, Evans J, Hart
S, et al. Benign papilloma on core biopsy requires surgical
excision. Ann Surg Oncol. 2008;15(8):2272–7.
7. Shin HJ, Kim HH, Kim SM, Yang HR, Sohn JH, Kwon GY, et al.
Papillary lesions of the breast diagnosed at percutaneous sono-
graphically guided biopsy: comparison of sonographic features
and biopsy methods. AJR. 2008;190:630–6.
8. Rizzo M, Lund MJ, Oprea G, Schniederjan M, Wood WC,
Mosunjac M. Surgical follow-up and clinical presentation of 142
breast papillary lesions diagnosed by ultrasound-guided core-
needle biopsy. Ann Surg Oncol. 2008;15(4):1040–7.
9. Liberman L, Tornos C, Huzjan R, Bartella L, Morris EA, Der-
shaw DD. Is surgical excision warranted after benign, concordant
diagnosis of papilloma at percutaneous breast biopsy? AJR. 2006;
186:1328–34.
10. Ueng SH, Mezzetti T, Tavassoli FA. Papillary neoplasms of the
breast: a review. Arch Pathol Lab Med. 2009;133:893–907.
11. Cheng TY, Chen CM, Lee MY, Lin KJ, Hung CF, Wang PS,
et al. Risk factors associated with conversion from nonmalignant
to malignant diagnosis after surgical excision of breast papillary
lesions. Ann Surg Oncol. 2009;16:3375–9.
12. Mercado CL, Hamele-Bena D, Oken SM, Singer CI, Cangiarella
J. Papillary lesions of the breast at percutaneous core-needle
biopsy. Radiology. 2006;238:801–8.
13. Syndor MK, Wilson JD, Hijaz TA, Massey HD, Shaw de Paredes
ES. Underestimation of the presence of breast carcinoma in
papillary lesions initially diagnosed at core-needle biopsy.
Radiology. 2007;242(1):58–62.
14. Renshaw AA, Derhagopian RP, Tizol-Blanco DM, Gould EW.
Papillomas and atypical papillomas in breast core needle biopsy
specimens. Am J Clin Pathol. 2004;122(2):217–21.
Breast Cancer
123

15. Reynolds HE. Core needle biopsy of challenging benign breast
conditions: a comprehensive literature review. AJR. 2000;174:
1245–50.
16. Ahmadiyeh N, Stoleru MA, Raza S, Lester S, Golshan M.
Management of intraductal papillomas of the breast: an analysis
of 129 cases and their outcome. Ann Surg Oncol. 2009;16:
2264–9.
17. Liberman L, Bracero N, Vuolo M, Dershaw DD, Morris EA,
Abramson AF, et al. Percutaneous large-core biopsy of papillary
breast lesions. AJR. 1999;172:331–7.
18. Kim MJ, Kim EK, Kwak JY, Son EJ, Park BW, Kim SI, et al.
Nonmalignant papillary lesions of the breast at US-guided
directional vacuum-assisted removal: a preliminary report. Eur
Radiol. 2008;18(9):1774–83.
19. Arora N, Hill C, Hoda S, Rosenblatt R, Pigalarga R, Tousimis E.
Clinicopathologic features of papillary lesions on core needle
biopsy of the breast predictive of malignancy. Am J Surg. 2007;
194:444–9.
20. Ciatto S, Houssami N, Ambrogetti D, et al. Accuracy and
underestimation of malignancy of breast core needle biopsy: the
Florence experience of over 4000 consecutive biopsies. Breast
Cancer Res Treat. 2007;101(3):291–7.
21. Destounis S, Skolny M, Morgan R, Arieno A, et al. Rates of
pathological underestimation for 9 and 12 gauge breast needle
core biopsies at surgical excision. Breast Cancer. 2011;18:42–50.
22. Houssami N, Ciatto S, Ellis E, Ambrogetti D. Underestimation of
malignancy of breast core-needle biopsy: concepts and precise
overall and category-specific estimates. Cancer. 2007;109:
487–95.
23. Philpotts L, Hooley R, Lee C. Comparison of automated versus
vacuum-assisted biopsy methods for sonographically guided core
biopsy of the breast. AJR. 2003;180(2):347–51.
Breast Cancer
123