-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
1/34
Rational
Primary Health Care delivery is acore contribution to
NSHDPimplementation. Over 90% of inputs in the Health
services delivery and Humanresources for health SDAs
ofNHSDP(Leadership & Governance,Health financing, NHIS,
Communityparticipation & Ownership,Partnership for health,
Research forhealth).
In order to improve participationand ownership by the
servicedelivery points , the PHC reviewsshould focus on the
operationalunit which is the LGAs.
NHSDP Costing Analysis, 2010
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
2/34
Challenges of NHSDP operational planning
The 2011 State Operational Plans were not consistent with the
level of ambition of theSSHDPs, costed activities were mainly based
on lower level inputs and that budgetsare not consistent with the
NHSDP allocation criteria. More funding still allocated forclinical
services and capital costs.
The 2011 Operational Plans showed no prioritization to focus on
Primary Health Careas the anchor of Service Delivery and Human
Resources for health and there was nolink of the planning process
and actual budget allocation.
There was no logical framework for reviewing the data inputs and
linkages with theon-going work on developing the M&E Framework
for results-based monitoring.
There are multiple systems for data collection and reporting
that are unrelatedleading to duplication with no feedback to the
Service Delivery Points (States andLGAs).
Despite several processes that have been put in place including
1) incorporating the
ATM indicators into HMIS and the 2) development of the
Integration andDecentralisation Guidelines; Programs and Partners
still collect and manage theirown M&E systems.
There is no current system to develop capacity for the LGAs to
fully own andimplement PHC programs.
There was no systematic process for quantifying the bottlenecks
and no outline forassigning roles and responsibilities in managing
the identified corrective actions.
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
3/34
Process of PHC Review
Harmonize indicators, collect and validate existing data
fromdifferent sources (Progs + NHMIS) in order to inform
PHCreviews.
Use PHCs reviews to identify, remove & follow up
bottlenecksto improve service delivery.
Develop LGA PHC action plans to address bottlenecks
throughcoordinated actions of all stakeholders.
Support development of LGA annual Operational plans thatderives
from and contributes to the SSHDPs.
Provide feedback to inform State and Federal planning
andreview.
D.I.V.A methodology for PHCUOR
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
4/34
Framework
Improved Health Plan Results
Conduct PHC Reviews
Using DIVA methodology
Implement PHCUOR and Minimum Standards
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
5/34
The 4 steps of DIVA
Identify disparities and analyze barriers to
access of services (Diagnose)
Prioritize and implement solutions to
overcome identified barriers (Intervene)
In real-time, monitor progress in reducing
barriers (Verify)
Adjust solutions and strategies during
implementation as needed (Adjust)
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
6/34
What is D-I-V-A?
A systematic, flexible, outcome-based
approach to equitable programming and real-
time monitoring that strengthens the ward
health system, complementing and building
on what exists.
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
7/34
Prioritization of interventions
Main causes of morbidity and mortalityidentified and linked to
poverty.
Core package of intervention determined by
service delivery point. Clinical , Population based and
Community/Households.
Coverage of interventions varies by state andLGAs.
Need for context specificity in planning.
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
8/34
Increasing No. of Interventions and Skilled Staff
9
Burden
of
Disease
Increasing Resources Required
MalariaVPDDiarrheaetc
MaternalNewbornChild Health
etc
HypertensionCanceretc
Canceretc
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
9/34
Neonatal, 37%
Pneumonia, 19%
Diarrhea, 17%
Malaria, 8%
Measles, 4%
HIV/AIDs, 3%
Injuries, 3%
Other, 10%
Under-nutrition
(underlying cause)
Major Causes of U-5 Deaths in Nigeria
Up to 1 million
children die
before the age of
five.
50% underlying
cause is under
nutrition.
36% are neonatal
deaths (284,000).
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
10/34
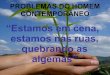
Equity & Impact : High Burden diseases in Q1 have known,
very effective, low cost interventions
40.726.9
50
11
56.3
22.1
6.6
1.6
36.7
13.9
4.9
1.6
21.6
8.8
0
50
100
150
200
250
Nigeria: Nigeria Q1 Nigeria: Nigeria Q5 (richest)
(Under Five Mortality Rate per 1000 Live Births)
Others
Injuries
AIDS
Pneumonia
Measles
Malaria
Diarrhea
Neonatal
Examples of using a Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
11/34
8 Tracer Interventions for PHC ReviewsDefined National priority
Tracer interventions
1. PMTCT and ARV prophylaxis
2. Immunization
3. Childhood Illnesses Malaria
4. Ante Natal Care
5. Skilled Birth Attendance & Community based NewBorn
Care
6. Infant and Young Child Feeding
7. Vitamin A Supplementation
8. Community Management of Acute malnutritionIdentify the most
deprived LGAs
Adapt to the existing health system and ongoing processes
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
12/34
D-I-V-A approach:
scope and applicability
Health
WASH
Nutrition
HIV/
AIDSHealthSystem
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
13/34
BOTTLENECK ANALYSIS
CONCEPT
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
14/34
A health system bottleneck can be defined as
a constraint, problem, barrier that hinders
the health performance
A bottleneck is a loss of system efficiency
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
15/34
Using a bottleneck analysis to
investigate low coverage
There are many interventions that are known tobe effective at
reducing maternal and childmortality
Most of these interventions are already includedin Nigeria
National HSDP
These interventions do not always reach thepeople that need them
most, due to bottlenecks
within the health system Resolving problems causing bottlenecks
requires
both evidence-based interventions AND evidence-based strategies
at federal, State and LGA levels
16
I d i B l k A l i
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
16/34
Tanahashi: a bottleneck constrains the flow of
resources through a health system, limiting the
output; i.e. coverage of an intervention
Multiple
interventions
Introduction to Bottleneck Analysis
I t d ti t B ttl k A l i
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
17/34
Introduction to Bottleneck Analysis
Bottleneck analysis is a horizontal approach
18
Nutrition HIV EPI
Facility-Based services
Population oriented
outreach services
Community based services
(Family oriented )
FamilyPlanning TB SocialservicesWASH
Effective Quality coverage for specific target populations
I t d ti t B ttl k A l i
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
18/34
Six coverage determinants, from supply to demand side,
analyze where health system bottlenecks exist.
A bottleneck is a loss of system efficiency
19Adapted from Tanahashi T. Bulletin of the World Health
Organization, 1978, 56 (2)
http://whqlibdoc.who.int/bulletin/1978/Vol56-No2/bulletin_1978_56(2)_295-303.pdf
Availabilityessential health commodities
Adequate coveragecontinuity/completion
Initial utilizationfirst contact of
multi-contact services
Accessibilityphysical access of services
Effective coverage quality/impact
Target Population
Availabilityhuman resources
Introduction to Bottleneck Analysis
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
19/34
We look for bottlenecks between
the determinants of coverage
Determinants are major health system functionsthat DETERMINE the
level of coverage possiblefor an intervention.
Supply-side determinants:1. Availability of essential
commodities.
2. Availability of human resources.
3. Geographical accessibility.
Demand-side determinants:4. Initial use: the first contact
5. Adequate and complete use
6. Effective, or Quality, Coverage that gets IMPACT
20
Introduction to Bottleneck Analysis
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
20/34
The Tanahashi Model to assess system bottlenecks
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% District withLLITN's or nets +
insecticide in stock
% villages with HRproviding LLITNs
% villages selling ordistribution LLITN or
nets + insecticide
% householdshaving at least one
bed net
% pregnant womenusing MN last night
% pregnant womenusing ITMN
Nigeriaapplication2006
21
Adapted by T. OConnell from Tanahashi T. Bulletin of the World
Health Organization, 1978, 56 (2)
http://whqlibdoc.who.int/bulletin/1978/Vol56-No2/bulletin_1978_56(2)_295-303.pdf
TargetPopula
tion
GAP
Introduction to Bottleneck Analysis
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
21/34
0%
25%
50%
75%
100%
COMMODITIES: %
health facilities
with no Essential
Meds stock-out
HUMAN RES: %
PHC facilities with
sufficient
professionals
ACCESS: %
families living
near health
facility with
sufficient staff
UTILISATION: % 0-
59 mos
w/pneumonia
taken to trained
provider
CONTINUITY: % 0-
59 mos ARI/fever
cases Tx
w/antibiotics by
trained worker
EFFECTIVE COV: %
0-59 mos. ARI and
fever cases
treated by IMCI-
trained worker
Clinical management of U5 pneumonia
Coverage Determinants and Bottlenecks:
improving coverage of Quality treatment of ARI
Introduction to Bottleneck Analysis
22
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
22/34
Introduction to Bottleneck Analysis
Commodities
A
vailabilityofthec
orrecthuman
resources
Points
ofaccess/distribution
Initia
luseofproducto
r
service
Con
tinuoususeof
pro
ductorservice
QUALITY0%
10%
20%
30%
40%
50%
60%
70%
Stock of
antibiotics in
district
# of fully
trained VHTs
vs. national
target
% villages with
complete VHT
Child with
ARI seen by
VHT
Child given
antibioticsChild
completes full
antibiotic
treatment < 24
hrs
1 Bottleneck is
too few access
points for CHWs
w/antibiotics
A 2nd major
bottleneck is
QUALITY: few
children finish
antibiotic course
Too much $$ (so
Moms save
antibiotics for nexttime); thus quality is
low
23
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
23/34
Identify bottlenecks in the Tracer Interventions
0%
25%
50%
75%
100%
ITN in
district
HEWs Families
with Net
Using net Using
treated
net
36%
20% 16%
4% 1%
We do not
have enough
bednets!
And we do nothave enough
people to give
them out!
And few
people are
sleeping
under them!
And they are
not treated: we
are not getting
IMPACT!!!Example:
Removing
coverage
bottlenecks
to scale up
ITNs
Identify the main supply, demand, and quality bottlenecks
Introduction to Bottleneck Analysis
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
24/34
0%
25%
50%
75%
100%
ITN in
district
HEWs Families
with Net
Using net Using
treated
net
36%
20% 16%
4%1%
80% 80%75%
72%65%
Trained and
deployed
HEWs in the
LGAs
Behavioralchange
communication
campaign
Policy decision:
long lasting ITN
20072005
Procured
>200,000 ITN
Corrective measures identified
Example:
Removing
coverage
bottlenecks
to scale up
ITNs
Introduction to Bottleneck Analysis
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
25/34
83 %
33 % 33 % 25 %
6 %
0 %
10 %
20 %
30 %
40 %
50 %
60 %
70 %
80 %
90 %
100 %
Commodity Human Resources Geographical Access Utilization
Continuity Quality
Example: PMTCT Bottleneck Analysis
Nigeria
Targ
etPopulation
GAP
26
Introduction to Bottleneck Analysis
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
26/34
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Proportion of ANC
centers without
stock out of HIV test
kits over the last 3
months
Number of HF staff
trained for PMTCT
% of HFs that
provide ANC
services with HIV
counselling and
testing in PMTCT
% of pregnant
women who know
their HIV status
% of pregnant
women who
received ARVs to
reduce MTCT
% of infants born to
HIV+ women
receiving ARV
prophylaxy to
reduce MTCT
PMTCT (Ikeja, Lagos)
Bottleneck 2:
Pregnant W. not
attending ANC
Plausible Cause: Trained
staff concentrated in
model facilities
Corrective Action: Train
staff from other facilities
Plausible Cause: Lack of
awareness of available
services and benefits of ANC
Corrective Action: Increase
social mobilization/ social
marketing
Bottleneck 1: Only 4
out of 10 facilities
provide CT
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
27/34
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% of HFs without
stock out of SP in
the last 3 months
% of ANC
providers trained
on prevention of
Malaria in
Pregnancy
% of HFs
providing ANC
% of pregnant
women who
received IPT1
% of pregnant
women who
received IPT2
during the last
birth
% of pregnant
women who
received IPT2 in
3rd trimester
IPTp in Makurdi PHC, Benue State
Bottleneck 2: Apparent
dropout
Plausible Cause:Distance/financial barrier.
(+ Underreporting).
Corrective Action: Provision of
transportation OR stipend for
transportation
Bottleneck 2:
Insufficient trained
staff
Plausible Cause: No
recent training in 2011.
Small # trained due to $.
Corrective Action: Advocacywith State and partners to
release funds for training
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
28/34
Analyze the bottlenecks and their
possible causes
Carried out by the existing Committees
State /LGAs with key stakeholders (including private sector,
civil society and community representatives) in
collaboration
with regional/provincial health officers/supervisors
Includes these steps:
1. Analyze the root causes of identified bottlenecks
(Causality Analysis)2. Identify and prioritize context-specific
and equityfocused solutions
3. Validate findings and recommended solutions through
astakeholder consultation
A l t
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
29/34
Analyze root causesa. Supply side causality analysis
Type of bottleneck Common bottlenecks Causes of common
bottlenecks
Availability of
human resources
Lack of OR insufficient
availability
Lack of established positions
Ineffective recruitment Ineffective deployment
High vacancy rates and turn over
High absenteeism
Lack of OR Insufficient skills Lack of staff training
opportunities
Lack of mentoring and supervision
Lack of OR Insufficient
motivation
Insufficient, inequitable, untimely salaries
Lack of performance-based incentives
Disruptive working environment
Lack of physical facilities and/or equipment
Geographic
accessibility
Lack of OR Insufficient health
facilities
Facilities are not functional
Lack of OR Insufficient outreach
sessions (not done, not of
sufficient scope and/or quality)
Ineffective planning
Infective implementation
Lack of OR Insufficient
community coverage (CHWs)
Community health workers are not carrying out designated
activities
Financial barriers (direct costs, indirect costs and
insufficient
social protection mechanisms)
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
30/34
Analyze root causes:b. Demand side causality analysis
Type of bottleneck Common bottlenecks Causes of common
bottlenecks
Initial utilization
Financial barriers Family cannot afford to pay user fees or to
travel long
distances to facilities
Socio-cultural barriers andgender dynamics
Mothers must obtain permission from others inhousehold prior to
seeking care
Social norms are not supportive to specific
interventions
Belief that illness is caused
by factors that cannot be
addressed at health facility
(e.g witchcraft)
Limited information (for example on childhood illness
danger signs) available to families in deprived settings
Timely, continued
utilisation
Loss to follow-up/drop-outs Lack of active follow up systems
Negative experience with provider/facility
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
31/34
Analyze root causes:b. Quality causality analysis
Type of
bottleneck
Common
bottlenecks
Causes of common bottlenecks
Initialutilization
Low quality
Timeliness
Completeness
Appropriateness
Regular standards: not developed,
not approved, and not used
Inadequate staffing and skills in
quality of care
Service organization: overload,
inadequate equipment and supply
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
32/34
Identification of corrective
measures
Carried out by existing Committees
State /LGAs with key stakeholders (including private
sector, civil society and community representatives) in
collaboration with regional/provincial health
officers/supervisors
Includes these steps:1. Identify and prioritize context-specific
and equityfocused solutions
2. Validate findings and recommended solutionsthrough a
stakeholder consultation
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
33/34
Summarize bottlenecks, solutions and strategies
INTERVENTION:. Quarter/Year:
Determinant
/ Indicator?
Baseline
as of:
_______
Main
Bneck?
(mark
X)
Plausible Causes
(indicate if further
investigation required)
Proposed Solutions Responsible
person &
partners
involved
Timeframe Target as
of:
_________
-
7/28/2019 Understanding PHC Reviews and the Nigeria planning and
implementation framework- Dr Eboreime Ejemai
34/34
Conclusion
The PHC Reviews will contribute to the successfulimplementation
of the National Health Plan and theachievement of results in line
with health-relatedMDGs.
Collective action and responsibilities are requiredfrom the
Federal, State and LGAs levels for improvingthe delivery of
services for children, women andother vulnerable populations.
Partners and Donors will require to fully buy-in andcontribute
to the PHC Reviews.
Government leadership and ownership is cardinal.