Embed Size (px)
Citation preview

Understanding Your Role
in Maximizing Revenue in a FQHC
Cynthia M Patterson President N Charleston SC 29420-1093 [email protected] P: (843) 597-8437 F: (888) 697-8923

“Have systems in place to maximize collections and reimbursement for its cost…including written billing, credit, and collection policies and procedures.”-(Section 300(k)(3)(F) and(G) of the PHS Act)
Health Center must show “due diligence” in collecting fees for services

“Revenue maximization requires…prompt and accurate billing of third party payers…,and timely follow-up on all uncollected amounts”
“Participation in insurance programs used by the health center’s population is of critical importance…”

Front Desk-is the first line of defense for getting correct patient demographic, insurance & Sliding Fee documentation
◦ Collecting at the POS
◦ Getting correct Insurance information
◦ Verification of coverage and Eligibility*
◦ Patient Education

Billing- is the last opportunity to maximize revenue
◦ Billing frequency
◦ Provider Credentialing
◦ Working denials, Aging Reports, and Self Pay
◦ Patient Education

Front Desk and Billing Staff
Working Together

A.I.D.E.T. ◦ Acknowledgement
◦ Introduce
◦ Duration
◦ Explanation
◦ THANK YOU
A.I.D.E.T. ◦ Not just for Staff-Patient relationships
◦ Also important for Staff-Staff relationships

Acknowledge the other persons position and realize that it is just as important as yours
Introduce educational material and knowledge across departments
Give the Duration of completing the process or correcting information
Provide Explanation for processes so that everyone understands you are not just making this stuff up.
Thank you and thank each other for their contribution to the success of the Practice

Staff must be able to communicate in order to correct processes that will decrease denials and maximize cash flow
We are all in this together. There is no “I” in team.
Participate in ongoing training opportunities and stay abreast of industry changes.

Failure to obtain current patient information ◦ Check eligibility of Sliding Fee ◦ Check eligibility of Insurance
Failure to collect on previous patient account balances
Failure to collect co-payments and minimum
fees at POS ◦ Not collecting co-payments is violating your
contract with payer who require them

Physicians not recording all services performed during the office visit
Not filing claims timely
Not working denials timely

Failure to code correctly and not having codes updated in your PMS
Failure to educate patients about the Health Center’s payment expectations
Failure to redirect claims properly
Not credentialing the Health Center and providers with Insurance Companies


Denials are claims returned by third party payers and patient accounts must be adjusted or charges redirected to the patient
◦ Patient not eligible
◦ Provider not enrolled
◦ Time Expired
Some denied claims can be appealed

Return Claims are claims returned by a third-party payer in which action can be taken to get current and future claims paid or claims in which the patient has not fulfilled their responsibility
◦ Coding Errors
◦ Additional Information Required
◦ Patient has other Insurance
◦ Payment applied to deductible

If not using a computer generated report, is there anyone in the office responsible for collecting this information?
Does your vendor offer a reporting system?
How often do you look at your denials?
What does your Denial Report tell you?
Who are you sharing your report with?
What steps are you putting in place to correct them?
How are you measuring your progress?

Sort denials by type
◦ Coding Errors
◦ Insurance Eligibility
◦ Credentialing
◦ Capitation
◦ Timely Filing

Sort by Department
◦ Front Desk
◦ Clinical
◦ Billing
◦ Administration (if Credentialing is not handled in the Billing Department)

Sort Denials by Plan of Action
◦ Adjustment to patient’s account
◦ Update information and re-bill to Insurance Company
◦ Provide Additional Information and re-bill to Insurance Company
◦ Redirect charges to the patient
◦ Other-Company needs to take action

Community Health Center USA
Quarterly Billing Activity Summary Sheet
October-November 2010
Commonly Used Denials
Medicare Medicaid Private Select Quarterly Total
Previous
Year To Date
Previous YEAR (Currently being tracked by Finance) Quarter
Adjustment to Pts. Acct
Time Expired 1 49 1 51 82 239 771
Duplicate 65 82 57 18 222 322 807 1,337
Suspended Claim 9 9 36 45 175
Capitation Payment 6 325 331 729 1,806 2,762
Update Information and Re-bill to Insurance
Additional Information Needed 9 1 43 1 54 79 255 715
Incorrect ID Number 12 14 3 29 33 92 308
Other Insurance 13 16 46 3 78 78 199 289
Incorrect Insurance Address 3 3 13 29 22
Coding Error-Re bill to Insurance
Code Not Covered 25 35 21 81 124 226 521
Missing 4th or 5th Digit 1 2 3 5 11 42
Incorrect Code 11 15 26 35 88 169
Pt.. with Ins – Redirect to Pt..
Applied Deductible 47 47 69 171 391
Family Planning 15 15 17 46 250
HMO 14 26 40 64 112 391
No Prior Authorization 56 88 144 65 226 199
Not Primary Care Provider 73 3 76 126 211 874
Out of Network 5 5 12 20 42
> Allowed Amount 1 7 1 9 35 62 487
Service Not Covered 8 43 51 100 243 714
Visits Exceeded 0 0 0 2
Patient w/o Ins- Redirect to Pt.
Not Eligible 6 15 18 39 81 239 354
Service After Cancellation Date 13 13 22 52 139
Service Prior To Coverage 1 1 4 6 38
Other
Refund Request 21 21 6 29 7
Part of Primary Procedure 0 11 13 96
Provider Not Eligible 3 3 2 5 24
Amount Withheld 1 1 1 2 101
Other 6 16 11 33 17 61 521
Total Claims Denied 117 268 495 505 1,385 1,742 5,295 11,741
Sort By Payer
Sort By Denial Types
Track Totals In Order to Measure
Your Progress


What Next?
◦ Established a Plan of Action
◦ Make sure staff is properly trained
◦ Measure your progress

Not all denied claims should be considered lost revenue. There are times when claims can be redirected to the patient.
◦ Patient has not met their deductible
◦ Patient does not have coverage or coverage ended
◦ Services not covered
◦ Patient has exceeded number of visits

Redirecting claims to patients
◦ When redirecting charges to a patient it is good to
call the patient before they get the statement in the mail.
◦ Let the patient know the reason why the charges are being redirected and ask for additional insurance information (they may have other coverage you are not aware of)

Educate them about the Sliding Fee Program and inform the patient of any payment plan your Center may have

Insurance Companies are not perfect, they make mistakes too.
Know when to Appeal a claim
Make sure the claim is valid
Make sure that the initial claim was filed timely

Be sure that services provided was covered on DOS
Be able to prove the patient had coverage on that DOS ◦ Verify correct ID number was entered
◦ Show printout from verification system
In some cases you will need to make sure the Insurance Company is aware that your Center is a FQHC

Some claims can be corrected and resubmitted to the third-party payer for payment ◦ Incorrect ID number
◦ Diagnosis Code invalid or missing 4th or 5th digit
◦ Additional information is needed

Some Insurance Company may require you to notated on the claim that it is a “Corrected Claim” – this helps to avoid the claim being returned again for untimely filing.

Always bill secondary Insurance Company
If a patient has Medicare and Medicaid
◦ Medicaid is always secondary
◦ If payment received from Medicare is less than your Medicaid encounter make sure to bill the difference to Medicaid. Do not consider the claim ‘Paid-in-Full”

Medicare and Medicaid ◦ Easiest source of revenue
Private Insurance Claims ◦ Insurance Claims >120 days
◦ Insurance Claims >90 days
Always check with your Insurance Company to determine filing period for timely filing
Aging Reports can be used during the same time you are addressing return claims. ◦ Can allow you to clear a patient’s account balance

Aging Reports should be reviewed and updated when posting payments
If you are manually posting also look at the past DOS to make sure that there are no outstanding items or missing payments.

Statements need to be mailed the same time every month
Bad addresses should be flag in the PMS and patient should be required to update their information before being checked in during the next visit.
If staffing permits patients should be contacted in an effort to obtain the correct information
Offer payment plans and payment-by-phone

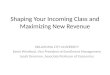
A Medicaid Manage Care plan did not pay for DOS because the diagnosis code did not match the procedure code
Procedure Code 99213 Office Visit
87880 Rapid Strep
ICD-9 079.99
(unspecified viral infection)

Research the diagnosis code (encounter, patient notes)
Communicate with the Provider why the claim was returned and indicate that a different code will be needed
Resubmit the claim to the Insurance Company

Private Insurance Company returned claims because the CPT code is considered to be part of the VFAC program.
◦ Verify CPT Code and program association
◦ Correct claim to reflect CPT Code with appropriate immunization/administration code
◦ Resubmit claim to payer for reimbursement
◦ Note: Payer will adjust charges for CPT Code associated with VFAC but will pay for administration

Missing Patient Info.
& Insurance
Info.
Diagnosis Code Does Not Match Age
Missing NPI
Number
Patient DOB Does NOT Match Diagnosis

Claim was returned by payer because the primary diagnosis is not covered
◦ If there are multiple diagnosis you may try billing
the secondary diagnosis as primary
◦ If there is only one diagnosis you may have to adjust charges according to the EOB

The Private Insurance Company denied a claim because the patient was not covered a the time of service ◦ Check for insurance on file
◦ Check charts or notes to see if Insurance Verification was completed on the DOS
◦ Verify ID number is correct and check eligibility
◦ If patient was not covered, charges should be redirected to the patient

Missing Modifier
Missing Diagnosis for Sick
Visit Missing NPI
Number

Contracted Center’s claim was returned by Insurance Company and the allowed amount was applied to the patient’s deductible
◦ Redirect the allowed amount that was applied to the
deductible to the patient
◦ Call the patient and inform them and reeducate them about the Sliding Fee Program and payment options.

List your top 4 denials
Determine cause of denials (by Department, Personnel, MIS)
Develop plan of action to address denial type and resolution
Determine if denial can be rebilled or should the patient account be adjusted

SMILE AND ASK ◦ Fees and Co-payments
MUST Verify Patient Demographic ◦ Name Spelled Incorrectly
◦ Date of birth doesn’t match
◦ Subscriber number missing, invalid, or missing digits
◦ Zip Code (Medicare)

MUST Verify Insurance Coverage at every visit ◦ Coverage Terminated ◦ Coordination of Benefits (Patient has other
insurance)
MUST Verify Service Covered by Insurance Company
MUST Verify ICD-9, CPT or HCPCS Codes ◦ Usage of 4th or 5th digit ICD-9 codes ◦ Proper use of modifiers

MUST Bill Frequently ◦ Claims not billed timely
Be aware that some payers are requesting that claims be submitted within 90 days from the DOS
Make sure your Practice and Providers are properly credentialed
Know your Insurance Company and understand how services affect your facility

Know billing regulations by payer
Make sure that your facility has policies and procedures in place for billing and collections
Remember: Revenue DOES NOT start in the Billing Department

Verify Insurance Eligibility for Every Patient at Every Visit
Eligibility of Medicare should be verified for patients <65 years old
Eligibility of Medicaid should be verified for children age 0-18 years old ◦ Establish a relationship with the Medicaid Eligibility
Worker in your area to assist with this process
Verify Primary and Secondary Insurance

Medicaid Manage Care Plans ◦ When verifying Medicaid ALWAYS verify if the
patient is in a Medical Homes Network or Manage Care Plan
◦ If the patient is not assigned to your facility or physician make sure to obtain prior authorization for the PCP
◦ Educate the patient about changing their PCP with the Insurance Company if they plan on continuing to use your services
◦ Authorization and Referral numbers are reported in field 17A of the HFCA 1500. Not reporting this number may cause denials

NaviNet.com (Aetna, Cigna, Select Health)
Webclaims.scmedicaid.com/SCWST/welcome/info.aspx
SouthCarolinaBlues.com
Clearinghouse (i.e. ZirMed, Payer Path)
Telephone
Company Direct Website

Medicare is primary to Medicaid
Medicare is primary to Private Insurance ◦ Retired-Medicare is still primary
◦ Actively Employed- Private Ins is primary
Private Insurance is Primary to Medicaid
Multi-Private Insurance

Improves proper classification of patients
Improves workflow
Improves proper billing
Reduce denials
INCREASE REVENUE

Always check eligibility Enter the name as it appears on the card Enter the policy number as it appears on the
card Relationship Fields ◦ Always chose ‘Self’ for Medicare (Advantage) and
Medicaid (Manage Care) ◦ Relationships should be properly identified for
other Private Insurance companies (Self, Child, Spouse)
◦ Patients with their own ID number classify as ‘Self’
Verify the patient’s date of birth and zip code

Medicaid Patients ◦ Family Planning
Family planning only covers contraceptives, V25.__
Other medical services may be charged directly to the patient
Medicaid does not allow a Well Child Care Visit (EPSDT) and Sick visit to be reported separately on the same date of service even if using a modifier
To maximize reimbursement charges, they should always be more than the allowable amount

Injections- the forcing of a liquid into a part, as into the subcutaneous tissue, the vascular tree, or an organ ◦ Bill E&M code with a ‘25’ modifier ◦ Include the NDC# for the injections on the claim ◦ Administration Code- CPT 96372 for J Codes (use 20610 for Major Joint)
Use your CPT code book to verify administration code based on ‘point’ of injections

Immunizations- a process or procedure that protects the body against an infectious disease. (vaccination)
◦ Include the NDC# for each immunization on the claim ◦ Administration Codes CPT 90471-90474 for Adults (age 19 and over) 90471 Single or combination vaccine (intramuscular) 90472 Each additional vaccine 90473 Administered by intranasal or oral route 90474 Each additional vaccine
Used when there is no face-to-face counseling

CPT 90460 & 90461 for Children
90460 Single or combination vaccine
90461 Each additional component
HCPCS G codes are still reported to Medicare w/ with a limited number of vaccines
G0008 - Influenza (90658)
G0009 - Pneumonia (90732)
G0010 - Hepatitis B (90746)
G9141 - Flu H1N1 (G9142)

Effective January 1, 2012
Changes with format in collecting and reporting data
You are responsible for making sure your practice, billing service, or clearinghouse are in compliance

Paper Claim Box 24/ EDI Loop 2310B ◦ Rendering and Attending Provider Number
NPI is the primary identification allowed
Paper Claim Box 33/ EDI Loop 2010AA ◦ Billing Provider primary service address
NO PO Box- MUST be a Physical Address
Zip Codes (anywhere on the claim form) ◦ A full 9-digit format is required (12345-6789)

Electronic FQHC Medicare Claim Acceptance ◦ Loop 2300-CLM07 Provider Accept Assignment Code- ‘A’
◦ Loop 2300-CL101 Admission Type Code- ‘3’ (Elective) 1-Emergency, 2-Urgent Care, 3- Elective, 4-Newborn, 5-
Trama Unit, and 9-Information Not Available
◦ Loop 2300-CL102 Admission Source Code- ‘2’ (Clinic/Physician Office)
◦ Loop 2300-CL103 Patient Status Code- ‘01’ (Discharge Self Care)