Embed Size (px)
Citation preview
Journal of Sport Rehabilitation, 1993, 2, 87-96§) 1993 Human Kinetics Publishers, Inc.
Unilateral Balance Training of NoninjuredIndividuals and the Effects on Postural Swaylithler.
Emily D. (:;ox, Scott M. Lephart, and James J. Irrgang
The purpose of this study was to provide. nonnative data on postural swayby comparing the mean gain score between two balance training groups anda control group. Twenty-seven recreational collegiate athletes (14 females,13 males. 18-36 years old) with no past documented lower extremity injuryor lesion of the vestibular system were randomly placed into three groups:control (nontraining), foam surt'ace training, or hard surface training. TheChattecx Dynamic Balance System (CDB) was utilized for objective post-and pretraining recordings. COB tests were perfonned on the training andnon training extremities with subjects' eyes open and eyes closed. Resultsrevealed no significant post to pre mean gain score differences within anygroup, nor was any significance revealed between group differences.Although no significant differences were revealed. trends indicated specificityof training toward testing mode. These data should assist clinicians inpreventing ankle injury or compensating for ankle instability with balance
training.
5SN"eb.,?ub-lign.~S in
~ for
vail-indi-.and
:d ati ad-
ilita-aign.
I use~ fee
reet,~nse[ the
Ligamentous injuries of the foot and ankle produce proprioceptive deficitsaffecting the muscles of the injured leg (4, 12). Proprioception is defined as "theawareness of postural movement, the changes in equilibrium, and the knowledgeof position, weight, and resistance of objects in relation to the body" (11).Proprioceptive information arises from mechanoreceptors in the skin, muscles,tendons, joint capsule, and ligaments. It includes information concerning staticposition, movement, and muscular forces. This information is relayed to thecentral nervous system (CNS) and back to the effector muscles (1, 14), whichreflexively assist in controlling joint position.
Injury to the ankle may affect its mechanoreception, resulting in apnormalinput to the CNS (13). Many articular nerve fibers terminate in mechanoreceptorswithin the capsule and ligaments about the ankle. They respond to changes injoint position, acceleration, and direction of movement. Injury to the ankle maylead to partial joint deafferentation, thus interfering with proprioceptive reflexes
-va
Emily D. Cox and James J. Irrgang are with the University of Pittsburgh Centerfor Sports Medicine Institute and Rehabilitation, Baum Blvd. at Craig St., Pittsburgh, PA15213. Scott M. Lephart is with the University of Pittsburgh Department of SportsMedicine. 104 Trees Hall, Pittsburgh, PA 15213.
87
Cox, Lephart. and !rrgang 88
that are mediated by articular mechanoreceptors. Deficits in proprioception mayadversely affect postural sway (4).
Glencross and Thorton (7) found a linear trend between the degree of errorand joint angle, with the largest error occurring at the largest angles of movement.They also found that the error was the greatest for individuals with second andthird degree ankle sprains. Gam (6) found that the total number ofmechanoreceptors decreased through repeated trauma. Therefore, fewermechanoreceptors are available to react when the terminal joint positions arereached, thus resulting in increases in the degree of error or postural sway (7).Tropp et al. (12) utilized force plate measurements to test subjects with injuredankles by having subjects complete a modified Rhomberg stance test on theinjured and noninjured extremities. No significant differences in postural swaywere observed. Based on the findings of Freeman and Dean (4), it has beenspeculated that the proprioceptive deficit can be substantially reduced if balancetraining is incorporated with a strengthening program duringpostinjury treatment.
Mechanoreceptors playa role in the fundamental organization of the CNS.Acting as transducers, they convert physical energy expressed as tension into anervous signal (14). There are four types of joint mechanoreceptors located inand around joints. Type I joint receptors are encapsulated Ruffini-like structureslocated in the superficial layers of the joint capsule. They are slowly adapting;thus they respond to pressure changes within the joint, and they signal static anddynamic tensile stresses (14). These receptors provide the CNS with informationin resting and active conditions. Type II joint receptors are encapsulated Pacinian-like structures located in the deep fibrous layers of the joint capsule. They arerapidly adapting and have a low threshold for activation (5, 10). They are dynamicmechanoreceptors that signal acceleration during passive or active movements.Type III or Golgi tendon organ-like receptors are located in the joint ligaments.They have a high threshold for activation and are slow adapting. Type III receptorsare active at the end ranges of joint motion. Type IV receptors are encapsulatedfree nerve endings and are found in the ligaments and joint capsule. These arepain receptors that respond to extreme mechanical or chemical irritation.
Postural stability can be defined as "the body's ability to maintainequilibrium at rest or during motion" (9). Postural stability is dependent on thecomplex reflex mechanisms involving vestibular and visual and mechanoreceptor
input.A number of balance training protocols are presently being utilized forrehabilitative testing and research. The thattecx Dynamic Balance System(Chattanooga, Tennessee, 1990) used in this study provides the clinician withobjective recordings in unilateral balance testing because it uses a force plateand computer printout. In regard to balance training, however, specific techniques,modes, duration, and frequency are not scientifically based. The modifiedRhomberg Test drill (stork stand), on a hard surface or a foam surface, is frequentlyutilized in most training rooms due to convenience and lack of expense. Thereis very little information regarding the efficacy of this training method. In thisstudy, which used the modified Rhomberg stance, it was postulated thatimprovements in proprioceptive feedback would occur with adequate stimulation.It was hypothesized that a 4-week progressive balance training program, utilizinga hard surface or a foam surface, would (a) result in a decreased standard deviationin postural sway compared to a control group, (b) produce a larger decrease in

Unilateral 8alance Training'ang 89
postural sway in the foam training group than in the hard surface group due tothe limited challenge presented by the hard floor, and (c) result in no significantdifference in the post- and pretraining testings in the eyes open and eyes closedgroups. Noninjured subjects were used for this study to demonstrate trainingeffects on uninjured extremities and to create a base for future research usingsubjects with previous injury. The present study was undertaken to help cliniciansdesign more effective functional rehabilitation programS that stress kinestheticsense and ultimately decrease or prevent ankle instability among athletes.
nay
rror~nt.lnd
ofwerare(7).:redthe
Methods
eennceent.NS.to aj inJresIn""0'andtionian-are
.mic~nts"
:nts.Itorsatedare
Subjects
Twenty-seven recreational male (n = 13) and female (n = 14) athletes (ages18-36) were recruited for this study. Recreational athlete was defined as anindividual who exercised regularly but did not take part in organized competition.The protocol was approved by the Biomedical Internal Review Board for Biomed-ical Research of the University of Pittsburgh, and all subjects signed a writtenconsent form outlining the risks of the study. None of the subjects had priordocumented lower extremity injury or lesion of the vestibular system. The subjectshad no prior experience with the CDB or any other balance training techniques.The dominant extremity was utilized for the training limb. We established domi-nance by asking each subject to identify. the leg he or she would use to kick aball.
Itain!
the
ptOf
Each subjec~ was randomly assigned to one of three treatment groups: acontrol group (no trait;ting), a foam surface group (treatment A), or a hard surfacegroup (treatment B). The preliminary analysis of the data demonstrated no signifi-cant differences among the groups. A BMPD Statistical Software program wasused. The statistical design used to test for treatment differences was a three-way analysis of variance CANOY A) (Group x Limb x Eye).
Chattecx Dynamic Balance System
The Chattecx Dynamic Balance System (CDB) was designed to measure posturalstability and was used to objectively assess post- and pretraining balance for allsubjects. The reliability of measuring postural sway during unilateral stance innormal subjects was confirmed in an unpublished study (2). The CDB consistsof four independent force-measuring transducers and is used to quantify posturalstability. Fluctuations in displacement of the center of pressure reflect tile amountof postural sway. The dispersion index, or sway index, was calculated as thestandard deviation around the mean of 100 data points per second during a 10-s test. Differences in the limits of postural stability between the involved andnoninvolved extremity, and in regard to joint and ligamentous instability, havebeen noted in several unpublished balance training studies (3, 8).
~ for;temwithJlate
ues,:fied:ntlyherethisthat
tion.
zingttion;e in
Testing Procedure
COB Post/Pretesting
The software used to operate the CDB was programmed through Key touchSoftware Technology. Testing was performed with subjects in a unilateral stance
Cox, Lephart. and !rrgang90
on the force plate; dominant and nondominant extremities were tested in randomorder. Subjects were barefoot for all testing and training procedures. Each sub-ject's foot was centered on the foot plate. The "ball" (metatarsal heads) of thefoot was placed on the marked area on the anterior plate. The length of the heelplate was adjusted so that the calcaneus was bisected by the posterior markedarea. The graph coordinates of the foot were entered into the system so that theforce plates could monitor the weight distribution accurately. This informationwas stored for posttesting. A viewing monitor was directed away from the subjectso it would not provide visual input (see Figures I and 2).
The recordings were made with each subject standing with the dominantknee extended (0°), the nondominant knee held at a 90° angle, and the hip inneutral position. Posture was maintained erect, the arms were crossed, and thehands touched the opposite shoulder. Each subject donned a safety harness toavoid injury from falling. Test recordings began when the subjects indicated theyperceived they were balanced. Each subject stood in bilateral support betweeneach test to avoid added fatigue. Each test was performed for 10 s.
~
Figure 1 -Example of subject on Chattecx Dynamic Balance System while testing.
91Unilateral Balance Training3ng
,)ffi.lb-theeel,edtheIonect
ant-In
the
.to
hey~en
Figure 2 -Example of Chattecx Dynamic Balance System.
Training SurfacesSubjects in treatment group A :lsed a foam surface that was 3 in. x 18 in. x 18in. and was of medium densir::. Subjects in treatment group B used. a hard,
smooth tile floor.
Treatment ProtocolThe training protocol for the foam and hard surface groups was the same. ~bjectstrained over a 4-week period. :hree times a week, for 5-min sessions. Duringeach training session, each subject had eyes closed and stood barefoot .on thedominant leg with arms crossed over chest and the nondominant knee maintainedin a flexed position. The nondcminant knee was flexed to midrange (450) thefirst 2 weeks and then progre55~d to a right angle (900) for the last 2 weeks.Balance training was not allo\..ej for the control group during the 4-week period.
Results
The results indicated no signit:-:ant differences (p < 0.05) in the mean post/pregain scores (see Table 1). No significant differences in the mean gain scoreswere revealed among the three groups when subjects were tested with eyes open
and eyes closed (see Figures 3-6).
:ing.
92 Cox, Lephart, and Irrga'ng
Table 1
Three-Way ANOV A Summary Table for Balance
Source D.F. Mean square F Tail prob.
Group1 Error
TrainedTrG2 Error
EyesEG3 Error
TrETrEG4 Error
224
12
24
12
24
12
24
91.2112437.21838
88.6690523.7099819.38856
59.7058119.4016917.77558
64.9674521.0235922.02886
2.45 O.107!i
4.571.22
O.O42~jO.312~
3.361.09
0.07930.3518
2.950.95
O.O98~:O.399~:
Note. Tr = trained; E = eyes (opened/closed); G = group (hard/foam/none).
POST TO PRE GAIN SCORES
6-
~-><wc~z0U5a:wa.(/)
Qz<w~wa:a..(/)0a.
-,,"!
-A..
..,.
CONTROL FOAM HARD
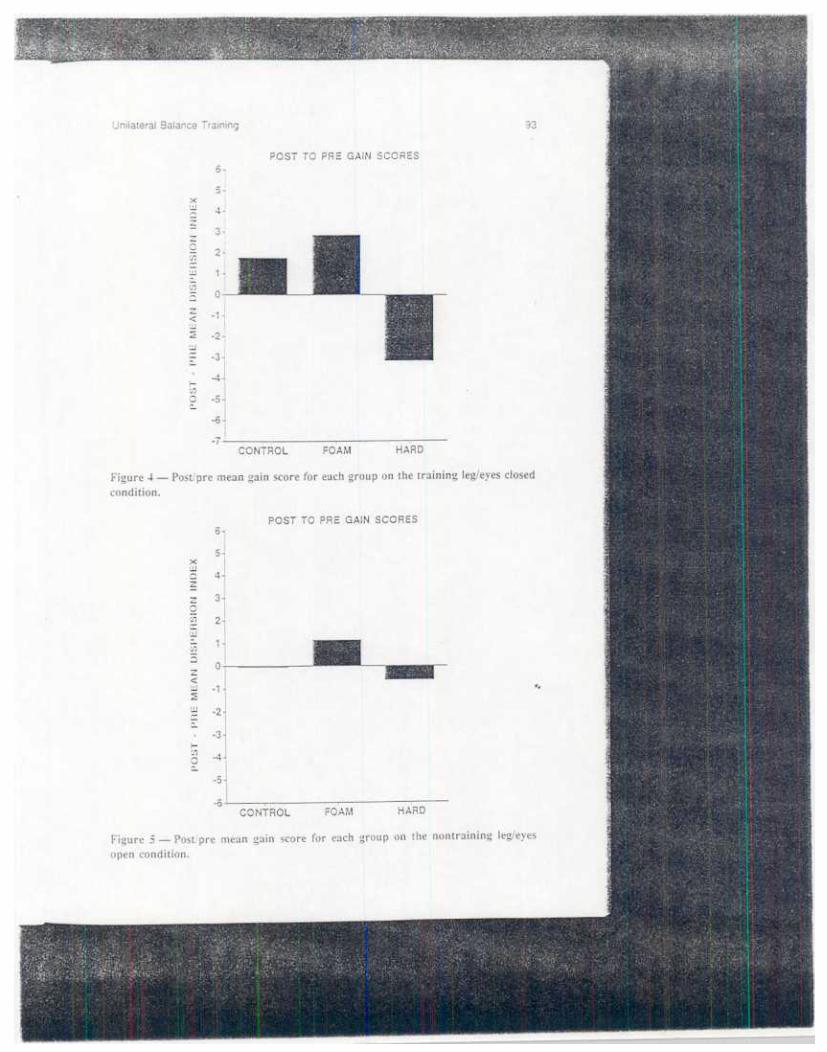
Figure 3 -Post/pre mean gain score for each group on the training leg/eyes opencondition. In Figures 3-6, lower or negative values represent improvements in balance.

94Cox, Lephart, and Irr~7ang
POST TO PRE GAIN SCORES
4-xUJ0
~z0ina:UJCo(/)
C5
z<UJ~
,
Q.
-1-
-2-
-3-
-4
w -5.a:~ -6.
-7-
-8.
-9-
-10J 0: ..CONTROL FOAM HARD
Figure 6 -Post/pre mean gain score for each group on the nontraining leg/ey(~sclosed condition.
We analyzed the data by viewing post/pre scores instead of pre/post scoresto demonstrate the changes in postural sway. A negative result indicated a decreas'~in the amount of sway, thus an improvement in balance. A positive result showedan increase in sway, therefore a regression of balance control.
Discussion
The present study examined the effects of balance training on postural sway. Theresults of this study revealed no significant post to pre mean gain score differenceswithin any group, nor was any significance revealed between group differences.However, an interesting trend was noted'in the results: The hard surface grouprevealed a consistent improvement in all four test measurements on the ChattecxDynamic Balance System. Implications may be drawn from this infonnation. First,the consistent pattern of decreases in postural sway post/pretest may indicateenhanced awareness of postural sway in the trained extremity, thus a potential steptoward injury prevention. Noninjured subjects were trained and tested so we couldview the changes that occur in a controlled setting in the absence of a pathology.Due to the lack of knowledge in the field of proprioception, these baseline findingsin noninjured subjects are valuable for future comparison with athletes who haveankle injuries. We were unable to apply the results observed in this study toclinically defined "nonnal" subjects. Future study in this area is urged.
Second, the results showed postural sway improvements in the hard surfacetraining group. This may simply be due to the fact that the training surface and
rgangUnilateral Balance Training95
the testing surface were similar. There \'-fere no large or consistent improvementsin the foam surf-ace training group. HoWever, decreases in post/pretest posturalsway results may have been evident if t~e testing surface had been foam insteadof a hard surface. There were limitatioljls in using the foam on the force plate,and therefore viewing test surface differ~nces between treatment groups was notpossible. Another factor in the improveftJents in the hard surface training groupwas training control. Subjects stated that the hard surt'ace provided a stablebase and 31l0wed for efficient balance training, with minimal opposite extremitysurface touchdown. This group stated the training' 'felt easier" with each session,Subjects in the foam surface group subjectively stated that there was no decreasein the challenge of balancing. These subjects complained of frequent loss ofbalance ;md no decreases in touchdown times, It is possible that the medium-density foam surface was too advanced for initial balance training. A higherdensity (allowing less deformity) foam may be necessary to provide the subjectwith a stronger base to begin training, prior to progressing to a more pliablesurface.
Numerous protocols are used for balance training, The unilateral Rhombergstance method for training was examined in this study due to its universalapplication in rehabilitation settings, This method is easy, can be implementedinto home programs, and can be used by athletes who do not have access tooptimal training equipment (e,g., when traveling). The results of this study maybe due to the training protocol and not to the training or testing surface type.Perhaps 5-min unilateral training sessions are too demanding on the involvedstructure, Shorter training sessions may increase the quality of training.
Due to the fact that noninjured subjects were utilized in this study, resultscannot be directly applied to the injured athlete. Due to the arrangements ofmechanoreceptors in the ankle, if there is no trauma disrupting the arrangementof these receptors, there mayor may not be room for improving their awareness.These are some points that must be addressed in future studies,
Summary
The findings of this study reveal the need for clinicians to explore balance training.Additional information provided from future research in the area of kinesthetictraining will allow for a more effective functional rehabilitation program.
..
References
I. Barrack. R. Proprioception in the anterioricruciate deficient knee. AJS,W. 17: 1-6,1989.2. Chattecx Corporation. The Balance System Clinical Desk Reference Manual (unpub-
lished report). Chattanooga. TN: Chattecx, 1990.3. Cox. E., and S. Lephart. Postural Swa.y to the Anterior Cruciate Deficient Individual
(unpublished report). Pittsburgh. PA: University of Pittsburgh Sports Medicine Insti-
tute. 1990. !4. Freeman, M.R., M.R.F. Dean, and M.. i Hanham. The etiology and prevention of
functional instability of the foot. J. Bon~ Joint Surg. 47(4):678-685. 1965.5. Freeman. M.R., and B. Wyke. Articula, reflexes at the ankle joint. Brit. J. Surg.
54(12):990-l001. 1967. i










![Unilateral acts of states: Ninth report on unilateral acts ... · 147 UNILATERAL ACTS OF STATES [Agenda item 6] DOCUMENT A/CN.4/569 and Add.1 Ninth report on unilateral acts of States,](https://img.pdfslide.net/doc/110x75/5f7232786650045f097b30a8/unilateral-acts-of-states-ninth-report-on-unilateral-acts-147-unilateral-acts.jpg)