Embed Size (px)
Citation preview
Annals of Otology. Rhinology & Laryngology 119(11):772-781.© 2010 Annals Publishing Company. All rights reserved.
Unilateral Deafness in Adults: Effects on Communicationand Social Interaction
Ona B. Wie, PhD; Are Hugo Pripp, ScD; Ole Tvete, MS
Objectives: The aim of this study was to explore the self-reported consequences of profound unilateral deafness regard-ing communication and social interaction and to compare subjects' speech perception scores to those of normal-hearingindividuals who were rendered temporarily unilaterally deaf.
Methods: Cross-sectional data from 30 individuals with unilateral deafness and 30 individuals with normal hearing(age, 14 to 75 years) were obtained through structured interviews and tests of audiovisual, auditory-only, and visual-onlyspeech perception.
Results: In individuals with permanent unilateral deafness, 93% reported that hearing loss affected communication.Eighty-seven percent reported problems with speech perception in noisy settings. Other consequences were feelings ofexclusion, reduced well-being, and extensive use of speech perception strategies. Inducing temporary unilateral deafness(through short-term blocking of one ear) in normal-hearing subjects produced similar effects on speech perception (27%score) as those experienced by unilaterally deaf subjects (25% score).
Conclusions: Individuals with unilateral deafness experienced a significant disability in auditory function that affectedtheir communication and social interaction. The major challenges were communicating in situations with backgroundnoise, in poor acoustic surroundings, and with limited access to speech-reading or direct listening. Under certain listeningconditions, long-standing unilateral deafness seemed to yield no advantage over temporary deafness on one side.
Key Words: auditory rehabilitation, quality of life, self-rated hearing difficulty, speech perception, unilateral deafness.
INTRODUCTION
Previous research has demonstrated that unilateraldeafness can be experienced as a significant disabil-ity that causes difficulty with communication andspeech perception, especially in environments withnoise and in poor acoustic conditions.'-^ Bateman etaP found deficits related to auditory dysfunction in72% of their patients with unilateral deafness fol-lowing acoustic neuroma surgery. Hansson' foundaudiological, psychosocial, and existential conse-quences of unilateral deafness, indicating that in-dividuals with unilateral deafness experienced in-creased stress levels and a feeling of exclusion in so-cial settings. There is further evidence that moderateto severe unilateral hearing loss can have negativeconsequences for children in educational settings.^'^CoUetti et al"^ confirmed the superiority of binauralversus monaural hearing, but they did not find sig-nificant differenees between binaurally and monau-rally hearing subjects in areas of educational, social,and employment achievement.
Hearing problems in unilaterally deaf individualsare often explained by the lack of binaural summa-
tion, the implications of the head shadow effect, andthe inability to utilize intensity and time or phasedifferences that would be apparent were the sig-nals entering two ears instead of one."'^ Lackingthe advantages of binaural hearing, these individu-als face difficulties with speech perception on thedeaf side, difficulties with sound localization, anddifficulties with speech perception in groups or withbackground noise in trying to segregate the signalfrom the noise. Earlier studies have confirmed thatthese difficulties can result in communication dis-tress when unilateral deafness occurs after surgery,such as acoustic neuroma surgery or surgery for avestibular schwannoma.^-'' Several studies have con-firmed that children with moderate to severe unilat-eral hearing loss are at risk for educational delays.*-^There is, however, less information regarding theeffects of unilateral deafness on communication inadolescents and adults, particularly with respect tosocial interactions and psychosocial consequences.
The main aim of this study was to explore theself-reported consequences of profound unilateraldeafness in adolescents and adults regarding com-munication and social interaction in everyday situa-
From the Department of Otolaryngology (Wie, Tvete) and the Biostatistics and Epidemiology Unit (Pripp), Oslo University Hospital,Rikshospitalet, Norway.Correspondence: Ona B. Wie, PhD, Dept of Otolaryngology, Oslo University Hospital, 0027 Rikshospitalet, Norway.
772
Wie" et al. Unilateral Deafness in Adults 773
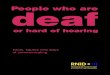
TABLE 1. DEMOGRAPHIC INFORMATION ON 30 PARTICIPANTS WITH UNILATERAL DEAFNESS
Sex
FMFFFFFMMMMFMFFFFFFMMM
FFMMMMMF
SP
1Cause
Acoustic neurinomaAcoustic neurinomaMalformationMalformationMeaslesMeniere's diseaseMeniere's diseaseMeningitisMumpsMumpsMumpsMumpsMumpsOtitis mediaOtitis mediaRubellaSudden deafnessSudden deafnessSudden deafnessTraumaTraumaTraumaTraumaTraumaUnknownUnknownUnknownUnknownUnknownUnknownAverageSDMinimumMaximum
— speech perception.
Side ofDeafness
RRRRRRLRRLLLLLRLLLRRLRRLLRRLLR
Tinnitus
YesYesNoNoNoYesYesNoNoYesYesNoNoNoNoNoYesYesYesNoYesYes
YesYesYesYesNoNoNoYes
Age(y)36512015485758632319512755634916326347512544
4375674929341432
41.917.314.075.0
Age atDeafiiess
(y)3243006
423668
12152
164
121
295843
06
36
413000000
14.117.10.0
58.0
Duration ofDeaßiess
(y)48
201542152257157
362539593716354
51198
3962674929341432
27.819.23.0
67.0
Visual-Only SP
21%3%1%5%
12%23%
2%17%8%5%5%
10%21%16%19%12%5%0%
13%0%7%4%
28%15%24%15%37%30%6%
12%13%9.60.0
37.0
Auditory-Only SP
53%20%28%66%18%40%
9%0%
18%20%
8%26%35%6%
24%30%10%2%
17%39%15%38%
29%2%
12%39%42%39%14%44%25%
16.260.0
66.0
Audio-visual
SP
90%79%93%92%75%77%75%52%95%83%59%63%93%64%82%92%91%26%85%88%60%82%
96%83%88%
100%88%93%79%91%80%
15.9826.0
100.0
tions. The matters of particular interest were as fol-lows: 1) To what degree is unilateral deafness ex-perienced as a communication handicap affectingsocial interaction? What are the major areas of diffi-culty, and what are the psychosocial consequences?2) To what extent do people with unilateral deafnessuse strategies to compensate for their hearing loss insocial interactions? 3) In those with unilateral deaf-ness, is there a relationship between self-reportedspeech perception in noisy settings and measuredspeech perception in such settings? 4) Is it possibleto "learn" to hear better in noise over time as one'sexperience with unilateral deafness grows?
METHODSParticipants. The study sample consisted of 30
profoundly unilaterally deaf adolescents and adults(16 women and 14 men; ages, 14 to 75 years; meanage, 42 years). Table 1 provides an overview of thesubjects' demographic information. Pure tone airconduction threshold testing was conducted andshowed a hearing threshold in the poor ear of morethan 60 dB hearing level at the frequencies 250 to6,000 Hz. The ear with normal hearing conformedto ISO (International Organization for Standardiza-tion) standard 7029:1992 for normal air conductionhearing thresholds. A masking level of 70 dB wasused in the hearing ear to detect the hearing level ofthe deaf ear.'-̂ Sixteen participants had right-sideddeafness, and 14 had left-sided deafness. The sub-jects' mean (±SD) duration of deafness was 28 ± 19years (range, 3 to 67 years). On the basis of infomia-
774 Wie et al. Unilateral Deafness in Adults
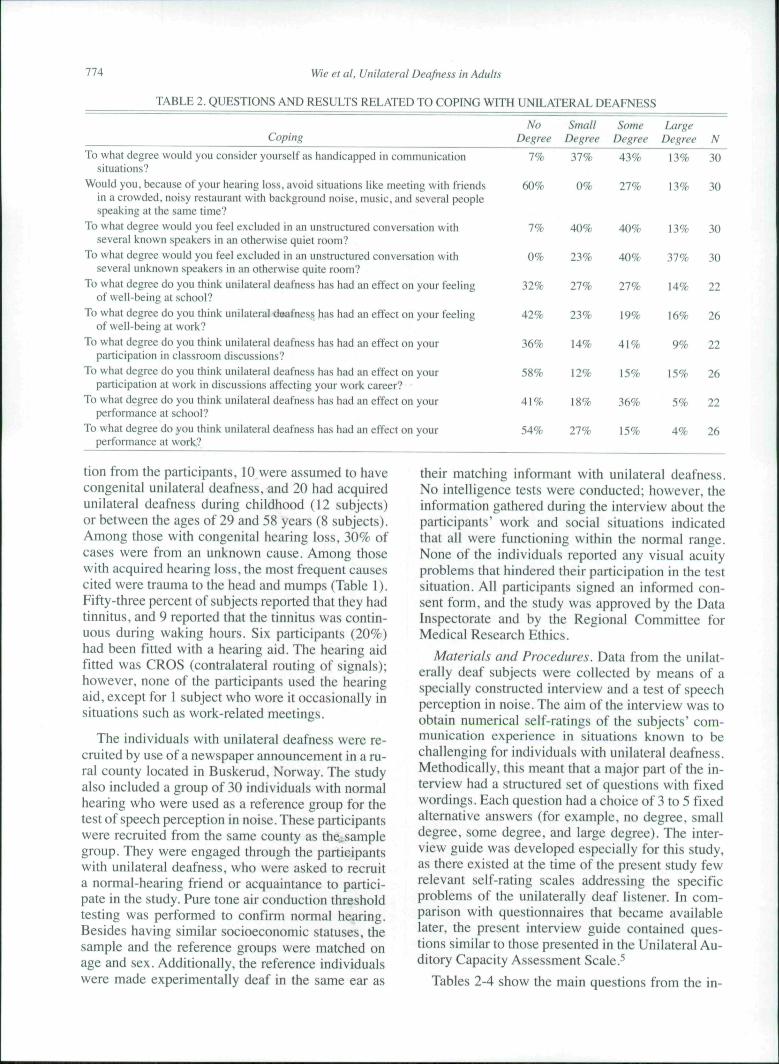
TABLE 2. QUESTIONS AND RESULTS RELATED TO COPING WITH UNILATERAL DEAFNESS
CopingNo Small Some Large
Degree Degree Degree Degree NTo what degree would you consider yourself as handicapped in communication
situations?Would you. because of your hearing loss, avoid situations like meeting with friends
in a crowded, noisy restaurant with background noise, music, and .several peoplespeaking at the same time?
To what degree would you feel excluded in an unstructured conversation withseveral known speakers in an otherwise quiet room?
To what degree would you feel excluded in an unstructured conversation withseveral unknown speakers in an otherwise quite room?
To what degree do you think unilateral deafness has had an effect on your feelingof well-being at school?
To what degree do you think unilateral dsafness has had an effect on your feelingof well-being at work?
To what degree do you think unilateral deafness has had an effect on yourparticipation in classroom discussions?
To what degree do you think unilateral deafness has had an effect on yourparticipation at work in discussions affecting your work career?
To what degree do you think unilateral deafness has had an effect on yourperformance at school?
To what degree do you think unilateral deafness has had an effect on yourperformance at work?
7% 37% 43% 13% 30
60% 0% 27% 13% 30
7%
0%
32%
42%
36%
58%
41%
54%
40%
23%
27%
23%
14%
12%
18%
27%
40%
40%
27%
19%
41%
15%
36%
15%
13%
37%
14%
16%
9%
15%
5%
4%
30
30
22
26
22
26
22
26
tion from the participants, 10 were assumed to havecongenital unilateral deafness, and 20 had acquiredunilateral deafness during childhood (12 subjects)or between the ages of 29 and 58 years (8 subjects).Among those with congenital hearing loss, 30% ofcases were from an unknown cause. Among thosewith acquired hearing loss, the most frequent causescited were trauma to the head and mumps (Table 1).Fifty-three percent of subjects reported that they hadtinnitus, and 9 reported that the tinnitus was contin-uous during waking hours. Six participants (20%)had been fitted with a hearing aid. The hearing aidfitted was CROS (contralateral routing of signals);however, none of the participants used the hearingaid, except for 1 subject who wore it occasionally insituations such as work-related meetings.
The individuals with unilateral deafness were re-cruited by use of a newspaper announcement in a ru-ral county located in Buskerud, Norway. The studyalso included a group of 30 individuals with normalhearing who were used as a reference group for thetest of speech perception in noise. These participantswere recruited from the same county as the.samplegroup. They were engaged through the participantswith unilateral deafness, who were asked to recruita normal-hearing friend or acquaintance to partici-pate in the study. Pure tone air conduction thresholdtesting was performed to confirm normal hearing.Besides having similar socioeconomic statuses, thesample and the reference groups were matched onage and sex. Additionally, the reference individualswere made experimentally deaf in the same ear as
their matching informant with unilateral deafness.No intelligence tests were conducted; however, theinformation gathered during the interview about theparticipants' work and social situations indicatedthat all were functioning within the normal range.None of the individuals reported any visual acuityproblems that hindered their participation in the testsituation. All participants signed an informed con-sent form, and the study was approved by the DataInspectorate and by the Regional Committee forMedical Research Ethics.
Materials and Procedures. Data from the unilat-erally deaf subjects were collected by means of aspecially constructed interview and a test of speechperception in noise. The aim of the interview was toobtain numerical self-ratings of the subjects' com-munication experience in situations known to bechallenging for individuals with unilateral deafness.Methodically, this meant that a major part of the in-terview had a structured set of questions with fixedwordings. Each question had a choice of 3 to 5 fixedalternative answers (for example, no degree, smalldegree, some degree, and large degree). The inter-view guide was developed especially for this study,as there existed at the time of the present study fewrelevant self-rating scales addressing the specificproblems of the unilaterally deaf listener. In com-parison with questionnaires that became availablelater, the present interview guide contained ques-tions similar to those presented in the Unilateral Au-ditory Capacity Assessment Scale.-''
Tables 2-4 show the main questions from the in-

Wie et al. Unilateral Deafness in Adults 775
TABLE 3. QUESTIONS AND RESULTS RELATED TO USE OF SPEECH PERCEPTION STRATEGIES (N = 30)
Strategy UseNo Small Some Large Totally
Degree Degree Degree Degree Dependent
You are in a room with background noise, participating in an unstructured 0% 0%conversation with multiple speakers. If the speech comes from the sameside as your deaf ear. would you turn your hearing ear toward the speaker?
You are in a room with background noise, participating in an unstructured 3% 13%conversation with multiple speakers. To what degree must you look at theface of the one who is speaking in order to follow the conversation?
You are in a room with a long reverberation time, participating in an 10% 13%unstructured conversation with multiple speakers. To what degree must youlook at the face of the one who is speaking in order to follow the conversation?
You are in a quiet room, participating in a structured conversation with multiple 17% 10%speakers. If the speech comes from the same side as your deaf ear. wouldyou turn your hearing ear toward the speaker?
You are in a quiet room, participating in a structured conversation with multiple 37% 33%speakers. To what degree do you look at the face of the one who is speakingin order to follow the conversation?
0%
13%
33%
27%
13%
37%
40%
30%
37%
13%
63%
30%
13%
10%
terview and the participants' responses to the ques-tions. The following characteristics were addressed.First, we studied the communication experience andcoping strategies used in different interaction situ-ations, eg, the amount of experience communicat-ing with known versus unknown speakers, a senseof well-being in communication, and the amount ofparticipation and performance in communicating(Table 2). Second, degree of strategy use, such asspeech-reading and positioning strategies, was ex-amined. The speech-reading strategy involves theuse of visual clues, such as movements of the speak-er's lips, facial movements, gestures, and body lan-
guage, to decode the contents of spoken language. Apositioning, or head-turning, strategy was indicatedby the subject's attempt to achieve direct listeningby turning the hearing ear toward the speech source(Table 3). Finally, we examined self-reported speechperception in different acoustic surroundings, suchas in quiet surroundings, in the presence of back-ground sound, and in rooms with poor acoustics (Ta-ble 4). To ensure that the questions were easily un-derstood, we pretested all questions on individualswith unilateral deafness who were not participatingin the study. One researcher conducted all the inter-views.
TABLE 4. QUESTIONS AND RESULTS RELATED TO SELE-REPORTED SPEECH PERCEPTION (N = 30)
Speech Perception and UnderstandingMost Some NoWords Words Words Often Sometimes Rarely
You are in a quiet room, participating in a structured conversationwhere the conversation moves from one person to another.How well do you hear?
You are in a room with a long reverberation time, as in churches orlarge halls with brick walls. How well do you hear in aone-on-one conversation?
You are in a room with a long reverberation time, listening toinformation given only through loudspeakers. How well doyou hear?
You are in a room with background noise, such as music and severalpeople having different conversations. How well do you hear in aone-on-one conversation?
Wiu are in a quiet room, participating in a structured conversationwhere the conversation moves from one person to another. Wouldyou understand the subject matter in the conversation?
You are in a room with a long reverberation time, as in churches orlarge halls with brick walls. Would you understand the subjectmatter in a one-on-one conversation?
You are in a room with a long reverberation time, listening toinformation given only through loudspeakers. Would youunderstand the subject matter in the conversation?
You are in a room with background noise, such as music and severalpeople having different conversations. Would you understand thesubject matter in a one-on-one conversation?
100% 0%
47% 40% 13%
37% 40% 23%
13% 50% 37%
100% 0%
67% 23% 10%
57% 30% 13%
47% 47%
776 Wie et al. Unilateral Deafness in Adults
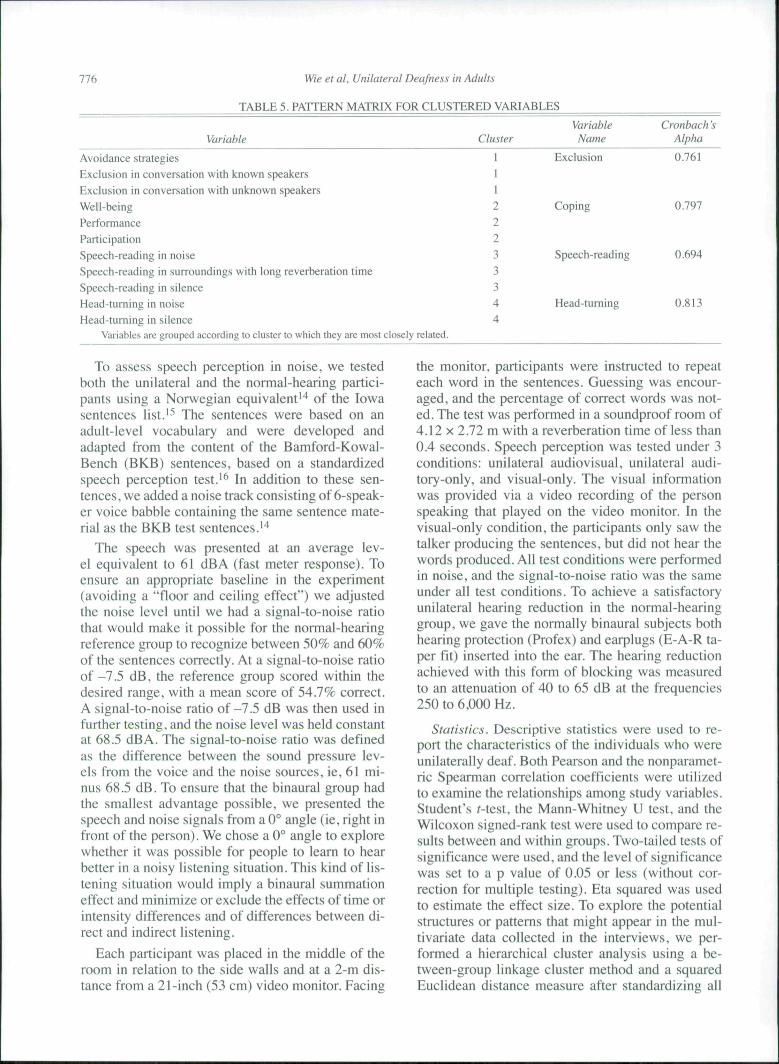
TABLE 5. PATTERN MATRIX FOR CLUSTERED VARIABLES
Variable
Avoidance strategiesExclusion in conversation with known speakersExclusion in conversation with unknown speakersWell-beingPerformanceParticipationSpeech-reading in noiseSpeech-reading in surroundings with long reverberation timeSpeech-reading in silenceHead-turning in noiseHead-turning in silence
Variables are grouped according to cluster to which they are most closely related.
Cluster
11122233344
VariableName
Exclusion
Coping
Speech-reading
Head-turning
Cronbach 'sAlpha
0.761
0.797
0.694
0.813
To assess speech perception in noise, we testedboth the unilateral and the normal-hearing partici-pants using a Norwegian equivalent'"* of the Iowasentences list,'^ The sentences were based on anadult-level vocabulary and were developed andadapted from the content of the Bamford-Kowal-Bench (BKB) sentences, based on a standardizedspeech perception test,"' In addition to these sen-tences, we added a noise track consisting of 6-speak-er voice babble containing the same sentence mate-rial as the BKB test sentences,''*
The speech was presented at an average lev-el equivalent to 61 dBA (fast meter response). Toensure an appropriate baseline in the experiment(avoiding a "floor and ceiling effect") we adjustedthe noise level until we had a signal-to-noise ratiothat would make it possible for the normal-hearingreference group to recognize between 50% and 60%of the sentences correctly. At a signal-to-noise ratioof -7,5 dB, the reference group scored within thedesired range, with a mean score of 54.7% correct.A signal-to-noise ratio of-7.5 dB was then used infurther testing, and the noise level was held constantat 68,5 dBA, The signal-to-noise ratio was definedas the difference between the sound pressure lev-els from the voice and the noise sources, ie, 61 mi-nus 68,5 dB, To ensure that the binaural group hadthe smallest advantage possible, we presented thespeech and noise signals from a 0° angle (ie, right infront of the person). We chose a 0° angle to explorewhether it was possible for people to learn to hearbetter in a noisy listening situation. This kind of lis-tening situation would imply a binaural summationeffect and minimize or exclude the effects of time orintensity differences and of differences between di-rect and indirect listening.
Each participant was placed in the middle of theroom in relation to the side walls and at a 2-m dis-tance from a 21-inch (53 cm) video monitor. Facing
the monitor, participants were instructed to repeateach word in the sentences. Guessing was encour-aged, and the percentage of correct words was not-ed. The test was performed in a soundproof room of4,12 X 2,72 m with a reverberation time of less than0.4 seconds. Speech perception was tested under 3conditions: unilateral audiovisual, unilateral audi-tory-only, and visual-only. The visual informationwas provided via a video recording of the personspeaking that played on the video monitor. In thevisual-only condition, the participants only saw thetalker producing the sentences, but did not hear thewords produced. All test conditions were performedin noise, and the signal-to-noise ratio was the sameunder all test conditions. To achieve a satisfactoryunilateral hearing reduction in the normal-hearinggroup, we gave the normally binaural subjects bothhearing protection (Profex) and earplugs (E-A-R ta-per fit) inserted into the ear. The hearing reductionachieved with this form of blocking was measuredto an attenuation of 40 to 65 dB at the frequencies250 to 6,000 Hz,
Statistics. Descriptive statistics were used to re-port the characteristics of the individuals who wereunilaterally deaf. Both Pearson and the nonparamet-ric Spearman correlation coefficients were utilizedto examine the relationships among study variables.Student's i-test, the Mann-Whitney U test, and theWilcoxon signed-rank test were used to compare re-sults between and within groups. Two-tailed tests ofsignificance were used, and the level of significancewas set to a p value of 0,05 or less (without cor-rection for multiple testing). Eta squared was usedto estimate the effect size. To explore the potentialstructures or patterns that might appear in the mul-tivariate data collected in the interviews, we per-formed a hierarchical cluster analysis using a be-tween-group linkage cluster method and a squaredEuclidean distance measure after standardizing all
speech perceptionin noise
Speech perceptionfrom loudspeaker in
surroundings with longreverberation time
Speech perception insurroundings with long -
reverberation time
Speech perceptionin silence
Wie et at, Unitaterat Deafness in Adutts
Known speakers
111
1.77
2.13
2.33
3.00
1A few of
the words
2Some of
the words
3Most of
the words
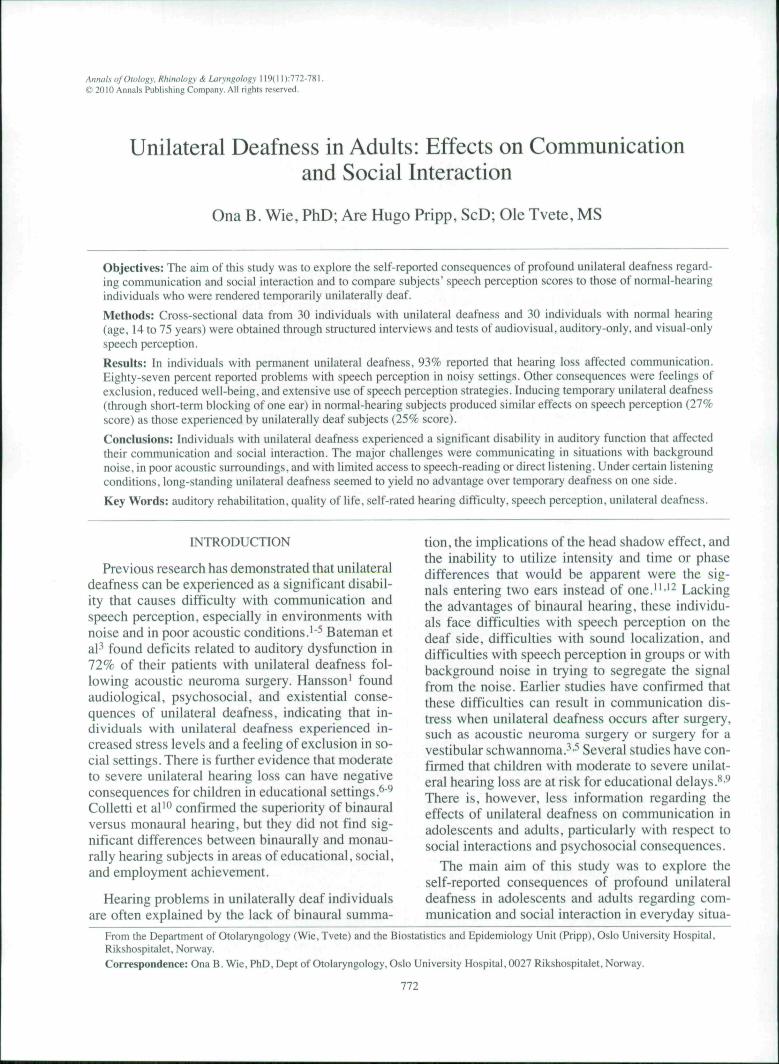
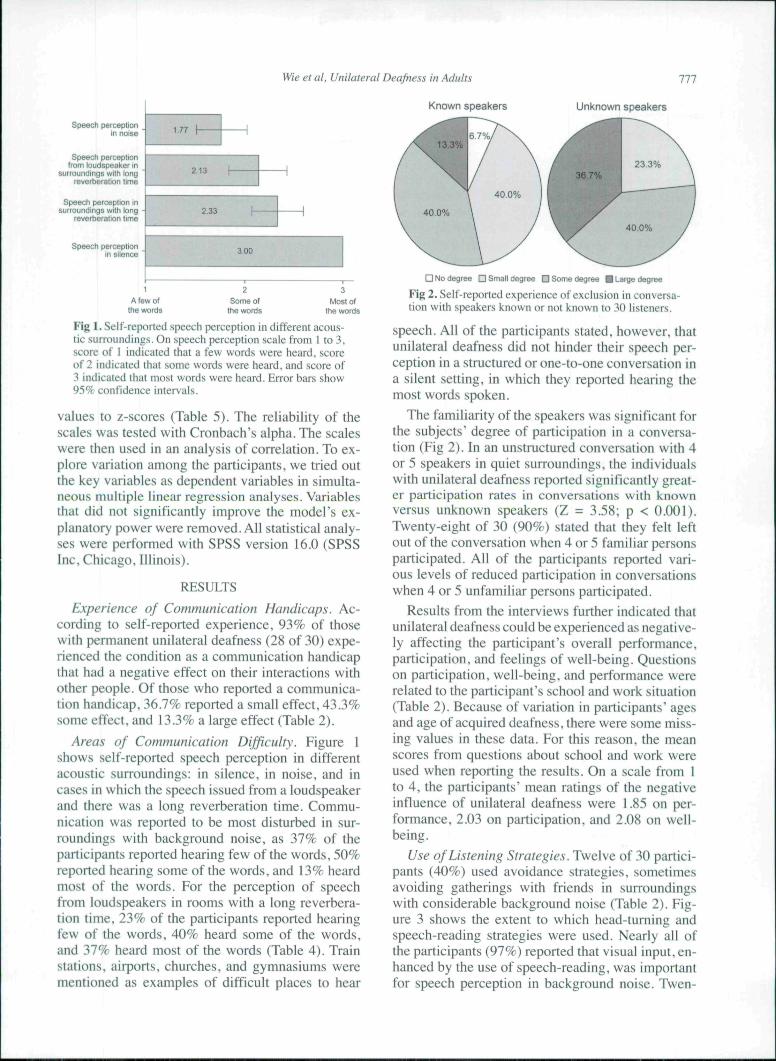
Fig 1. Self-reported speech perception in different acous-tic surroundings. On speech perception scale from 1 to 3,score of I indicated that a few words were heard, scoreof 2 indicated that some words were heard, and .score of3 indicated that most words were heard. Error bars show95% confidence intervals.
values to z-scores (Table 5). The reliability of thescales was tested with Cronbach's alpha. The scaleswere then used in an analysis of correlation. To ex-plore variation among the participants, we tried outthe key variables as dependent variables in simulta-neous multiple linear regression analyses. Variablesthat did not significantly improve the model's ex-planatory power were removed. All statistical analy-ses were performed with SPSS version 16.0 (SPSSInc, Chicago, Illinois).
RESULTS
Experience of Communication Handicaps. Ac-cording to self-reported experience, 93% of thosewith permanent unilateral deafness (28 of 30) expe-rienced the condition as a communication handicapthat had a negative effect on their interactions withother people. Of those who reported a communica-tion handicap, 36.7% reported a small effect, 43.3%some effect, and 13.3% a large effect (Table 2).
Areas of Communication Difficulty. Eigure 1shows self-reported speech perception in differentacoustic surroundings: in silence, in noise, and incases in which the speech issued from a loudspeakerand there was a long reverberation time. Commu-nication was reported to be most disturbed in sur-roundings with background noise, as 37% of theparticipants reported hearing few of the words, 50%reported hearing some of the words, and 13% heardmost of the words. Eor the perception of speechfrom loudspeakers in rooms with a long reverbera-tion time, 23% of the participants reported hearingfew of the words, 40% heard some of the words,and 37% heard most of the words (Table 4). Trainstations, airports, churches, and gymnasiums werementioned as examples of difficult places to hear
Unknown speakers
D No degree D Small degree D Some degree • Large degree
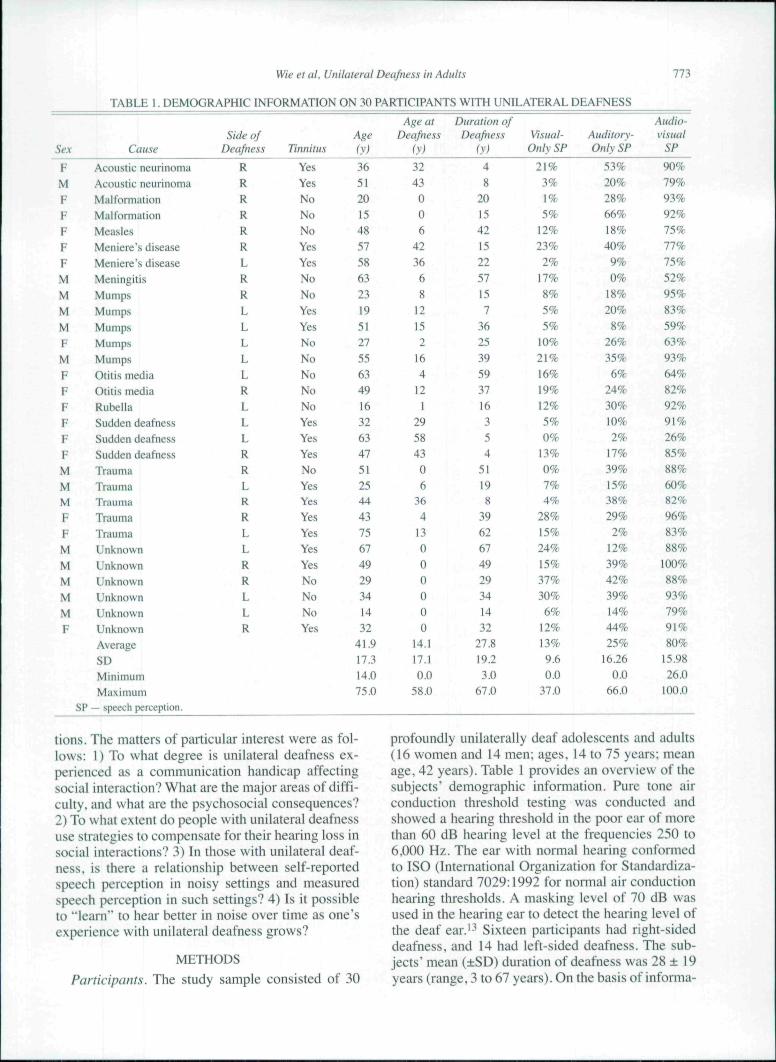
Fig 2. Self-reported experience of exclusion in conversa-tion with speakers known or not known to 30 listeners.
speech. All of the participants stated, however, thatunilateral deafness did not hinder their speech per-ception in a structured or one-to-one conversation ina silent setting, in which they reported hearing themost words spoken.
The familiarity of the speakers was significant forthe subjects' degree of participation in a conversa-tion (Eig 2). In an unstructured conversation with 4or 5 speakers in quiet surroundings, the individualswith unilateral deafness reported significantly great-er participation rates in conversations with knownversus unknown speakers (Z = 3.58; p < 0.001).Twenty-eight of 30 (90%) stated that they felt leftout of the conversation when 4 or 5 familiar personsparticipated. All of the participants reported vari-ous levels of reduced participation in conversationswhen 4 or 5 unfamiliar persons participated.
Results from the interviews further indicated thatunilateral deafness could be experienced as negative-ly affecting the participant's overall performance,participation, and feelings of well-being. Questionson participation, well-being, and performance wererelated to the participant's school and work situation(Table 2). Because of variation in participants' agesand age of acquired deafness, there were some miss-ing values in these data. Eor this reason, the meanscores from questions about school and work wereused when reporting the results. On a scale from Ito 4, the participants' mean ratings of the negativeinfluence of unilateral deafness were 1.85 on per-formance, 2.03 on participation, and 2.08 on well-being.
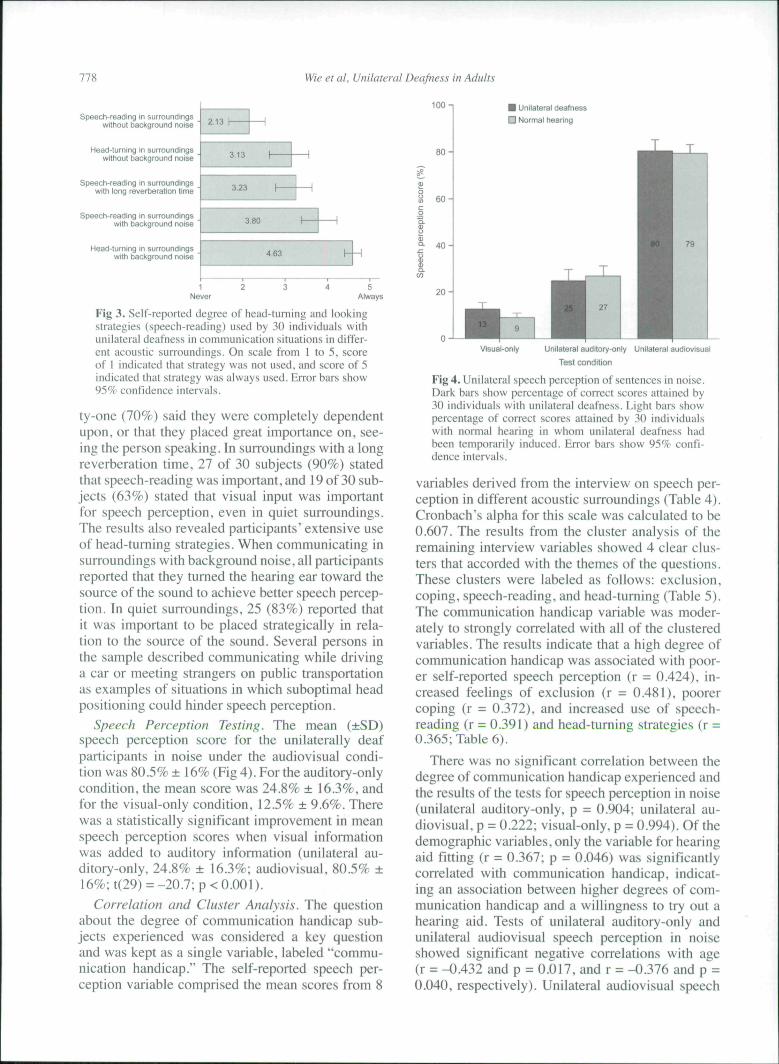
Use of Listening Strategies. Twelve of 30 partici-pants (40%) used avoidance strategies, sometimesavoiding gatherings with friends in surroundingswith considerable background noise (Table 2). Eig-ure 3 shows the extent to which head-turning andspeech-reading strategies were used. Nearly all ofthe participants (97%) reported that visual input, en-hanced by the use of speech-reading, was importantfor speech perception in background noise. Twen-
778 Wie et al. Unilateral Deafness in Adults
Speech-reading in surroundingswithout background noise
Head-turning in surroundingswithout background noise
Speech-reading in surroundingswith long reverberation time
Speech-reading in surroundingswith background noise
Head-turning in surroundingswith background noise
100 n • Unilateral deafness
D Normal hearing
3.13
3.23
3.80
463
1 2Never
5Always
Fig 3. Self-reported degree of head-turning and lookingstrategies (speech-reading) used by 30 individuals withunilateral deafness in communication situations in differ-ent acoustic surroundings. On scale from 1 to 5. scoreof 1 indicated that strategy was not used, and score of 5indicated that strategy was always used. Error bars show95% confidence intervals.
ty-one (70%) said they were completely dependentupon, or that they placed great importance on, see-ing the person speaking. In surroundings with a longreverberation time, 27 of 30 subjects (90%) statedthat speech-reading was important, and 19 of 30 sub-jects (63%) stated that visual input was importantfor speech perception, even in quiet surroundings.The results also revealed participants' extensive useof head-turning strategies. When communicating insurroundings with background noise, all participantsreported that they turned the hearing ear toward thesource of the sound to achieve better speech percep-tion. In quiet surroundings, 25 (83%) reported thatit was important to be placed strategically in rela-tion to the source of the sound. Several persons inthe sample described communicating while drivinga car or meeting strangers on public transportationas examples of situations in which suboptimal headpositioning could hinder speech perception.
Speech Perception Testing. The mean (±SD)speech perception score for the unilaterally deafparticipants in noise under the audiovisual condi-tion was 80.5% ± 16% (Fig 4). For the auditory-onlycondition, the mean score was 24.8% ± 16.3%, andfor the visual-only condition, 12.5% ± 9.6%. Therewas a statistically significant improvement in meanspeech perception scores when visual informationwas added to auditory information (unilateral au-ditory-only, 24.8% ± 16.3%; audiovisual, 80.5% ±16%; t(29) == -20.7; p < 0.001).
Correlation and Cluster Analysis. The questionabout the degree of communication handicap sub-jects experienced was considered a key questionand was kept as a single variable, labeled "commu-nication handicap." The self-reported speech per-ception variable comprised the mean scores from 8
Visual-only Unilateral auditory-oniy Unilateral audiovisual
Test condition
Fig 4. Unilateral speech perception of sentences in noise.Dark bars show percentage of correct scores attained by30 individuals with unilateral deafness. Light bars showpercentage of correct scores attained by 30 individualswith normal hearing in whom unilateral deafness hadbeen temporarily induced. Error bars show 95% confi-dence intervals.
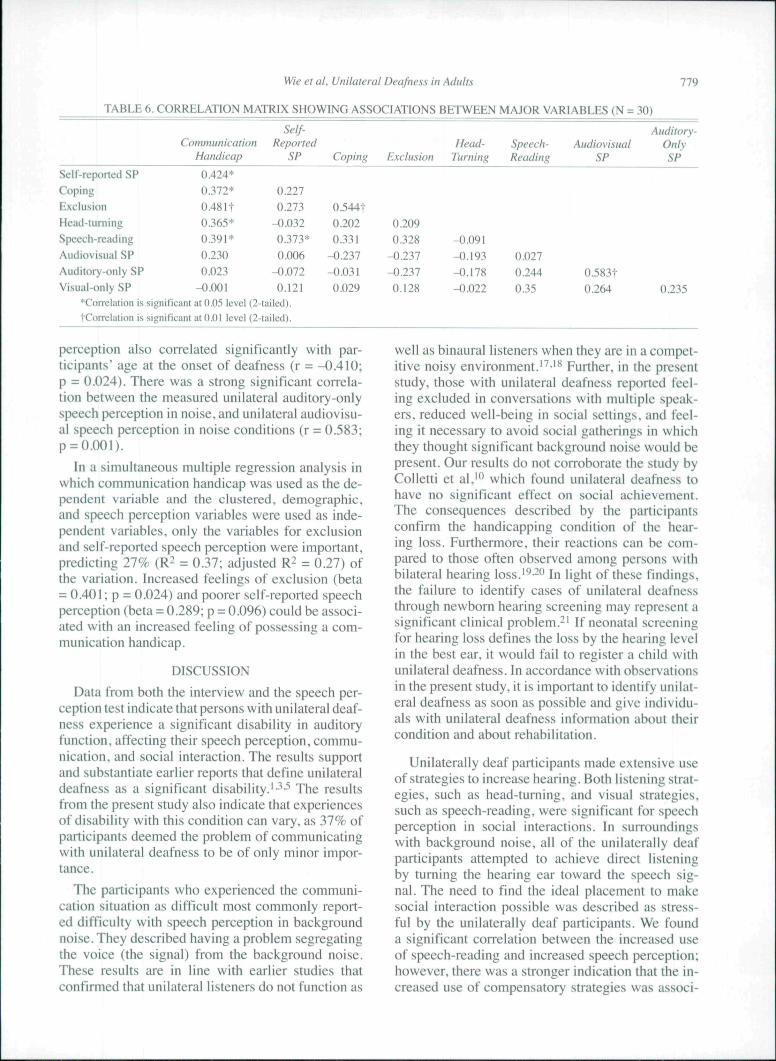
variables derived from the interview on speech per-ception in different acoustic surroundings (Table 4).Cronbach's alpha for this scale was calculated to be0.607. The results from the cluster analysis of theremaining interview variables showed 4 clear clus-ters that accorded with the themes of the questions.These clusters were labeled as follows: exclusion,coping, speech-reading, and head-turning (Table 5).The communication handicap variable was moder-ately to strongly correlated with all of the clusteredvariables. The results indicate that a high degree ofcommunication handicap was associated with poor-er self-reported speech perception (r = 0.424), in-creased feelings of exclusion (r = 0.481), poorercoping (r = 0.372), and increased use of speech-reading (r = 0.391) and head-turning strategies (r =0.365; Table 6).
There was no significant correlation between thedegree of communication handicap experienced andthe results of the te.sts for speech perception in noise(unilateral auditory-only, p = 0.904; unilateral au-diovisual, p = 0.222; visual-only, p = 0.994). Of thedemographic variables, only the variable for hearingaid fitting (r = 0.367; p - 0.046) was significantlycorrelated with communication handicap, indicat-ing an association between higher degrees of com-munication handicap and a willingness to try out ahearing aid. Tests of unilateral auditory-only andunilateral audiovisual speech perception in noiseshowed significant negative correlations with age(r = -0.432 and p = 0.017, and r = -0.376 and p =0.040, respectively). Unilateral audiovisual speech
Wie et al. Unilateral Deafness in Adults 779
TABLE 6. CORRELATION MATRIX SHOWING ASSOCIATIONS BETWEEN MAJOR VARIABLES (N = 30)
CommunicationHandicap
Self-Reported
SP Coping ExclusionHead-
TurningSpeech-Reading
AudiovisualSP
Auditory-OnlySP
Self-reported SPCopingExclusionHead-turningSf)eech-readingAudiovisual SPAuditory-only SPVisual-only SP
0.424*0.372*
0.48 It0.365*0.391*0.2300.023
-0.001
0.2270.273
-0.0320.373*0.006
-0.0720.121
0.544t0.2020.331
-0.237-0.0310.029
0.2090.328
-0.237-0.2370.128
-0.091-0.193-0.178-0.022
0.0270.2440.35
0.583t0.264 0.235
'Conelation is significant at 0.05 level (2-tailed).
tCorrelation is significant at 0.01 level (2-tailed).
perception also correlated significantly with par-ticipants' age at the onset of deafness (r = -0,410;p = 0.024). There was a strong significant correla-tion between the measured unilateral auditory-onlyspeech perception in noise, and unilateral audiovisu-al speech perception in noise conditions (r = 0.583;p = 0.001).
In a simultaneous multiple regression analysis inwhich communication handicap was used as the de-pendent variable and the clustered, demographic,and speech perception variables were used as inde-pendent variables, only the variables for exclusionand self-reported speech perception were important,predicting 27% (R^ = 0.37; adjusted R2 = 0.27) ofthe variation. Increased feelings of exclusion (beta= 0.401 ; p = 0.024) and poorer self-reported speechperception (beta = 0.289; p = 0.096) could be associ-ated with an increased feeling of possessing a com-munication handicap.
DISCUSSION
Data from both the interview and the speech per-ception test indicate that persons with unilateral deaf-ness experience a significant disability in auditoryfunction, affecting their speech perception, commu-nication, and social interaction. The results supportand substantiate earlier reports that define unilateraldeafness as a significant disability.'•^••'' The resultsfrom the present study also indicate that experiencesof disability with this condition can vary, as 37% ofparticipants deemed the problem of communicatingwith unilateral deafness to be of only minor impor-tance.
The participants who experienced the communi-cation situation as difficult most commonly report-ed difficulty with speech perception in backgroundnoise. They described having a problem segregatingthe voice (the signal) from the background noise.These results are in line with earlier studies thatconfirmed that unilateral listeners do not function as
well as binaural listeners when they are in a compet-itive noisy environment.'^'** Further, in the presentstudy, those with unilateral deafness reported feel-ing excluded in conversations with multiple speak-ers, reduced well-being in social settings, and feel-ing it necessary to avoid social gatherings in whichthey thought significant background noise would bepresent. Our results do not corroborate the study byColletti et al,'" which found unilateral deafness tohave no significant effect on social achievement.The consequences described by the participantsconfirm the handicapping condition of the hear-ing loss. Furthermore, their reactions can be com-pared to those often observed among persons withbilateral hearing loss.'''-" In light of these findings,the failure to identify cases of unilateral deafnessthrough newborn hearing screening may represent asignificant clinical problem.-' If neonatal screeningfor hearing loss defines the loss by the hearing levelin the best ear, it would fail to register a child withunilateral deafness. In accordance with observationsin the present study, it is important to identify unilat-eral deafness as soon as possible and give individu-als with unilateral deafness information about theircondition and about rehabilitation.
Unilaterally deaf participants made extensive useof strategies to increase hearing. Both listening strat-egies, such as head-turning, and visual strategies,such as speech-reading, were significant for speechperception in social interactions. In surroundingswith background noise, all of the unilaterally deafparticipants attempted to achieve direct listeningby turning the hearing ear toward the speech sig-nal. The need to find the ideal placement to makesocial interaction possible was described as stress-ful by the unilaterally deaf participants. We founda significant correlation between the increased useof speech-reading and increased speech perception;however, there was a stronger indication that the in-creased use of compensatory strategies was associ-
780 Wie et al. Unilateral Deafness in Adults
ated with an increased feeling of having a commu-nication handicap. These findings support earlier re-ports of increased stress levels in individuals withunilateral deafness.'
The results from the speech perception in noisetest in the present study underscore the significanteffect of visual support on speech perception, whichbacks up numerous studies that have previouslydemonstrated that visual speech information is ben-eficial for comprehending speech and for speechperception in noise.-^ We found a 56% increase inword recognition from the auditory-only conditionto the audiovisual condition. This difference couldbe very important for facilitating communication,and it should be taken into consideration when plan-ning a unilaterally deaf person's rehabilitation, suchas in classroom settings, in other learning situations,and in work situations. These findings are in linewith those of earlier reports.̂ •2-''"2-''
The degree of communication handicap that par-ticipants experienced did not significantly correlatewith the results of the tests for auditory-only or au-diovisual speech perception in noise. This findingmost likely indicates that the test we used to mea-sure speech perception did not sufficiently measureunilateral speech perception in daily situations. Thismay be because in daily life, sound and speech fre-quently enter the ears from angles other than 0°. Ad-ditionally, earlier studies, such as that of Hallberget al,-" have concluded that the psychosocial con-sequences of hearing loss cannot be predicted fromaudiometric data alone. In concurrence with Hall-berg at al,-" we conclude that the psychosocial con-sequences of unilateral deafness, such as decreasedfeelings of well-being, poor coping, increased feel-ings of experiencing a handicap, and feelings of ex-clusion in social interactions cannot be predictedfrom the applied speech perception tests in noise.Our findings indicate, however, a closer associationbetween the participants' self-reported speech per-ception and their experiences of the psychosocialconsequences of unilateral deafness.
An interesting finding of the present study wasthat having more experience with unilateral deaf-ness did not yield an advantage to participants withunilateral deafness under the applied test condition.We found no difference in unilateral speech per-ception test scores between the groups tested. Thenormal-hearing group, who were rendered tempo-rarily unilaterally deaf, achieved speech perceptionscores similar to those of the group who had beenunilaterally deaf for 3 to 67 years. The strategies re-ported in this study might seem to have a positiveeffect on speech perception, but such effects were
not observed under the applied test condition, whenspeech and noise were entering the two ears from a0° angle. This finding might indicate that for spe-cific listening situations, long-standing experiencewith unilateral deafness yields no advantage overtemporary deafness on one side. Our findings sug-gest a rehabilitative approach that takes into con-sideration how different listening environments canaffect the communication situation for unilaterallydeaf individuals. To further explore our findings, itwould be interesting to explore the influence of in-tervention programs that develop targeted strategiesfor enhancing speech perception in noise.
Only 20% of the participants in the present studyhad been fitted with a hearing aid, and only 1 per-son used the hearing aid on an occasional basis.Participants' self-reported reasons for not using theCROS hearing aid were that there was too much set-noise from the aids and that the open plug in thenormal-hearing ear covered up too much of the nat-ural sound. This finding aligns with earlier studiesindicating that the conventional CROS hearing aidsystem was successful in only 10% of patients withtotal deafness on one side and normal hearing on theother side.'- Recent studies, however, have shownincreased user satisfaction with a bone-anchoredhearing aid.-^ At present, there is a rising interest inthe use of cochlear implants in the rehabilitation ofunilateral deafness. Vermeire and Van de Heyning-^found significant improvement in speech under-standing in noise and in the subjective self-assess-ment of hearing status after cochlear implantation inindividuals with unilateral deafness and incapacitat-ing tinnitus.
Some caveats to the current study are that thenumber of participants included in the study wassmall and that only a limited number of factors werestudied. We chose an experimental setting with agiven level of noise and a 0° signal-to-noise anglein order to generate the smallest advantage possiblefor binaural versus unilateral listeners; thus, the re-sults might differ under conditions outside this ex-perimental setting. Among the participants, 44% re-ported that having unilateral deafness was of minoror no significant importance to their communicationsituation. Further research, including a larger num-ber of participants and more comprehensive obser-vation of possible contributing factors, is warranted.The interview used was constructed for this studyonly. Thus, it would be helpful to further standardizethe questionnaires and interviews to include a rangeof factors applicable to unilateral deafness.
CONCLUSIONSThe major finding in this present study was that
Wie et al. Unilateral Deafness in Adults 781
persons with unilateral deafness experienced a sig-nificant disability in auditory function that affectedtheir speech perception, communication, and socialinteraction. Second, the major areas of difflcultywere communicating in background noise, in pooracoustic surroundings, and with limited access tospeech-reading or direct listening. The feeling ofexclusion in communication situations with multi-ple speakers was a common experience that couldlead to the avoidance of social interaction. The thirdfinding was that the communication handicap expe-rienced by subjects was not associated with the re-sults of a test for speech perception in noise. This
finding might indicate that the test we used did notaccurately simulate unilateral speech perception indaily life. Eurther, it is likely that other factors af-fecting individual coping strategies play a centralrole in the degree to which one considers unilateraldeafness to be a communication handicap. Einally,we observed that under the applied test condition,the participants with long-standing unilateral deaf-ness seemed to have no advantage over those whohad come to the condition more recently, as theydid not have better speech perception in noise thandid the normal-hearing reference group who experi-enced temporary deafness on one side.
REFERENCES1. Hansson H. Unilateral deafness, audiological, social psy-
chological and existential aspects [Thesis]. Stockholm, Swe-den: University of Stockholm, 1993.
2. Anders,son G, Ekvall L, Kinnefors A, Nyberg G, Rask-Andersen H. Evaluation of quality of life and symptoms aftertranslabyrinthine acoustic neuroma surgery. Am J Otol 1997; 18:421-6.
3. Bateman N, Nikolopoulos TP, Robinson K, O'DonoghueGM. Impairments, disabilities, and handicaps after acousticneuroma surgery. Clin Otolaryngol Allied Sei 2000:25:62-5.
4. Ruscetta MN, Arjmand EM, Pratt SR. Speech recogni-tion abilities in noise for children with severe-to-profound uni-lateral hearing impairment. Int J Pediatr Otorhinolaryngol 2005;69:771-9.
5. McLeod B, Upfold L, Taylor A. Self reported hearingdifficulties following excision of vestibular schwannonia. Int JAudiol 2008:47:420-30.
6. Bess FH, Tharpe AM. Performance and management ofchildren with unilateral sensorineural hearing loss. Scand Au-diol Suppl 1988:30:75-9.
7. Lieu JE. Speech-language and educational consequencesof unilateral hearing loss in children. Arch Otolaryngol HeadNeck Surg 2004:130:524-30.
8. English K, Church G. Unilateral hearing loss in children:an update for the 1990s. Lang Speech Hear Services Schools1999:30:26-31.
9. Tharpe AM. Unilateral and mild bilateral hearing loss inchildren: past and current perspectives.TrendsAmplif 2008:12:7-15.
10. Colletti V, Fiorino FG, Canier M, Rizzi R. Investigationof the long-term effects of unilateral hearing loss in adults. Br JAudiol 1988:22:113-8.
11. Markides A. Advantages of binaural over unilateral hear-ing. In: Markides A, ed. Binaural hearing aids. London, Eng-land: Academic Press, 1977:276-98.
12. Valente M, Valente M, Enrietto J, Layton KM. Fitting.strategies for patients with unilateral hearing loss. In: ValenteM,ed. Strategies for selecting and verifying hearing aid fittings.2nd ed. New York, NY: Thieme Medical Publishers, 2002:253-71.
13. Stach BA. Clinical audiology. An introduction. 2nd ed.New York, NY: Del mar, 2010.
14. Teig E, Lindeman HH, Tvete O, Hanche-Olsen S, Ras-mussen K. Audiovisual test programs in native languages. Testmaterial in Norwegian on a video disc controlled by laser bar
code. Adv Otorhinolaryngol 1993;48:199-202,
15. Tyler RS, Preeee JP, Tye Murray N. Iowa audiovisualspeech perception laser videodi.sc. Iowa City, Iowa: The Uni-versity of Iowa Hospitals Department of Otolaryngology-Headand Neck Surgery, 1987.
16. Bench J, Kowal A, Bamford J. The BKB (Bamford-Kowal-Bench) .sentence lists for partially-hearing children. BrJ Audiol 1979:13:108-12.
17. De Jonge R. Selecting and verifying hearing aid fittingsfor symmetrical hearing loss. In: Valente M,ed. Strategies for se-lecting and verifying hearing aid fittings. 1st ed. New York, NY:Thieme Medical Publishers, 1994:180-204.
18. Welsh LW, Welsh JJ, Rosen LF, Dragonette JE. Function-al impairments due to unilateral deafness. Ann Otol Rhinol Lar-yngol 2004:113:987-93.
19. Kramer SE, Kapteyn TS. Festen JM. The self-reportedhandicapping effect of hearing disabilities. Audiology 1998:37:302-12.
20. Hallberg LR, Hallberg U, Kramer SE. Self-reportedhearing difficulties, communication strategies, and psychologi-cal general well-being (quality of life) in patients with acquiredhearing impairment. Disabil Rehabil 2(M)8:3O:2O3-I2.
21. Ross DS, Holstrum WJ, Gaffney M, Green D, Oyler RF,Gravel JS. Hearing screening and diagnostic evaluation of chil-dren with unilateral and mild bilateral hearing loss. Trends Am-plif 2008:12:27-34.
22. Dodd B. The role of vision in the perception of speech.Perception 1977:6:31-40.
23. Bronkhorst AW, Plomp R. A clinical test for the assess-ment of binaural speech perception in noise. Audiology 1990:29:275-85.
24. Woodhouse L, Hickson L, Dodd B. Review of visualspeech perception by hearing and hearing-impaired people:clinical implications. Int J Lang Comtnun Disord 2009:44:253-70.
25. Arnold P, Hill F. Bisensory augmentation: a speechread-ing advantage when speech is clearly audible and intact. Br JPsychol 2001:92:339-55.
26. Linstrom CJ, Silvcrman CA, Yu GP. Efficacy of thebone-anchored hearing aid for single-sided deafness. Laryngo-scope 2009:119:713-20.
27. Vermeire K, Van de Heyning P. Binaural hearing aftercochlear implantation in subjects with unilateral sensorineuraldeafness and tinnitus. Audiol Neurootol 2009:14:163-71.
Copyright of Annals of Otology, Rhinology & Laryngology is the property of Annals Publishing Company and
its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's
express written permission. However, users may print, download, or email articles for individual use.