Embed Size (px)
Citation preview

University of Groningen
Early risk factors for chronic rejection after lung transplantationZweers, Noëlle
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2006
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Zweers, N. (2006). Early risk factors for chronic rejection after lung transplantation. [S.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 22-08-2021


Early risk factors for chronic rejection after lung transplantation
Noelle Zweers

Publication of this thesis was financially supported by:
Groningen University Institute for Drug Exploration (GUIDE) Faculteit der Medische Wetenschappen RuG Stichting Klinische Immunologie Harlan Nederland Novartis Pharma B.V. Wyeth Pharmaceuticals B.V. Greiner Bio-One Netherlands Boston Scientific Benelux B.V.
Printed by PrintPartners Ipskamp B.V. Enschede, The Netherlands
Cover illustration: Two chest radiographs of transplanted left lungs. Left picture: on the right side of this picture a transplanted left lung with a good lung function is shown. Right picture: the right side of this picture shows a transplanted left lung that is rejected.
Early risk factors for chronic rejection after lung transplantation Noelle Zweers Thesis University of Groningen ISBN-number: 90-367-2495-3
Copyright© 2006 by Noelle Zweers All rights reserved. No part of this book may be reproduced or transmitted, in any form or by any means, without permission of the author.

Stellingen behorende bij bet proefschrift
Early risk factors for chronic rejection after lung transplantation
I . Tegenwoordig wordt in klinische longtransplantatie vooral gebruik gemaakt van hersendode donoren. In de toekomst zal daar meer en meer van afgeweken moeten worden om de overleving na longtransplantatie te verbeteren (dit proefschrift).
2. In tegenstelling tot de algemeen heersende gedachte binnen de klinische longtransplantatie wordt chronische rejectie na longtransplantatie niet alleen gekarakteriseerd door bronchiolitis obliterans, maar ook door veranderingen in de bloedvaten (dit proefschrift).
3. In het huidige transplantatiebeleid wordt vooral rekening gehouden met cytomegalovirus- en Epstein-Barr-virusinfecties terwijl het voorkomen
en bestrijden van luchtweginfecties minstens zo belangrijk is (dit proefschrift ).
4. Het ontstaan van chronische rejectie na longtransplantatie wordt niet bepaald door een risicofactor maar door een combinatie van risicofactoren ( dit proefschrift).
5. Het succesvol afronden van een promotieonderzoek wordt meer bepaald door de mate van doorzettingsvermogen dan door intelligentie van de AIO.
6. De werkstress van een onderzoeker wordt in het weekend vaak afgereageerd op amateurscheidsrechters.
7. Door iedereen standaard als orgaandonor in het registratiesysteem op te nemen wordt een bewuste keuze voor of tegen orgaandonatie gestimuleerd.
8. Door de snelle ontwikkeling op het gebied van de technologie zal er in de toekomst naast de welbekende muisarm ook de iPod-duim ontstaan.
9. "Logic takes you from A to B; imagination takes you everywhere" (Einstein), maar een groter AIO-budget zal het maken van verre reizen wel vergemakkelijken.
Noelle Zweers Groningen, 1 maart 2006


RIJKSUNIVERSITEIT GRONINGEN
Early risk factors for chronic rejection after lung transplantation
Proefschrift
ter verkrijging van het doctoraat in de Medische Wetenschappen
aan de Rijksuniversiteit Groningen op gezag van de
Rector Magnificus, dr. F. Zwarts, in het openbaar te verdedigen op
woensdag 1 maart 2006 om 14.45 uur
door
Noelle Zweers
geboren op 9 januari 1976 te Huissen

Promotor:
Co-pro motor:
Beoordelingscommissie:
Prof. dr. L.F .M.H. de Leij
Dr. J. Prop
Prof. dr. G .H. Koeter Prof. dr. C.G.M. Kallenberg Prof. dr. R.J. Ploeg

Voor mijn ouders

Paranimfen: A.H. Petersen A.B. Geerts

Contents
Chapter 1 General introduction 9
Chapter 2 Aim of the thesis 21
Chapter 3 Donor brain death aggravates chronic rejection after lung transplantation in rats 25
Chapter 4 Acceptance of the lung is not abrogated by a local Sendai virus infection after lung transplantation in rats 43
Chapter 5 Cytomegalovirus infection in immunocompromised rats increases the number of immune effector cells and alloreactivity after lung transplantation 59
Chapter 6 Enhanced alloreactive T cell responses in HCMV-carrying lung graft recipients through HCMV-induced recipient CD45RA +CD2TCD8+ effector type T cell accumulation and donor endothelial-cell ICAM-1 and MICA expression 75
Chapter 7 General discussion 95
Chapter 8 Summary 103
Chapter 9 Nederlandse samenvatting (voor niet-ingewijden) 107
References 114
Abbreviations 138
Dankwoord 140


Chapter 1
General introduction

- Chapter 1 -
Achievements in clinical lung transplantation; a historical perspective
Lung transplantation is, compared to grafting of other organs, a rather young therapy. The first human lung transplantation was performed in 1963, but suffered from many complications due to the inability to perform complete and adequate immunosuppression (1). Long-term clinical success was not realized until 1981. At that time a successful combined heart-lung transplantation was performed (2). It took, however, until 1983 before the first successful transplantation of a single lung was reported (3).
During recent years, lung transplantation has become an accepted treatment option for patients suffering from end-stage pulmonary diseases. Although it remains to be confirmed that lung recipients experience a benefit in terms of duration of survival, it is without doubt an improvement of quality of life for the majority of patients ( 4, 5). The main indications for clinical lung transplantation are chronic obstructive pulmonary disease (COPD), idiopathic pulmonary fibrosis (IPF), cystic fibrosis (CF), a 1 -antitrypsin deficiency emphysema and primary pulmonary hypertension (PPH) (6).
Nowadays, different types of lung transplantation can be distinguised. Single lung transplantation is most commonly applied for COPD and IPF. Bilateral lung transplantation is performed in case of CF or PPH ( 6, 7). Living donor lobar transplantation is a new option and was introduced due to limited supply of donor organs. Although recently introduced, this approach has shown to be quite promising (8-10).
The development of adequate immunosuppression in lung transplantation has suffered from many pitfalls. This is caused by the high incidence of infections associated with the exposure of the grafted lung to environmental air with potential pathogens, the size of the organ and high content of lymphoid tissue ( 11, 12). After more than 30 years study the most efficacious immunosuppression seems to be a combination of induction and maintenance therapy. Almost 50% of the patients receive an induction therapy with anti-lymphocyte antibodies, monoclonal anti-CD3 antibody, or anti-interleukin-2-receptor monoclonal antibodies. This induction therapy is still subject of debate since some groups believe it may be deleterious in some patients to achieve long-term graft function and patient survival (6, 13). As maintenance therapy, the majority of lung transplant recipients
10

- General introduction -
receive a calcineurin inhibitor (cyclosporin-A or tacrolimus), a cell-cycle inhibitor (azathioprine or mycophenolate mofetil), and steroids (6, 13).
In many transplantation centers the one-year survival rate of patients after both single and bilateral lung transplantation is almost 80%, but the long-term survival rates are unfortunately not as good. At 5 years and 10 years after transplantation the survival rates are respectively 49% and 24% (6).
Clinical lung transplantation and complications
In spite of adequate immunosuppression, lung grafts like all solid organ transplants, suffer from complications that cause failure of the grafts. These complications can result in failure early and late after transplantation.
Early graft failure The early complications can be categorized into problems associated with
surgery, infection, and acute rejection. Mostly, these complications occur within the first days, weeks or months after transplantation.
Surge,y Problems associated with surgery usually occur within hours to days after
transplantation and are usually caused by immediate inflammatory responses associated with the surgical procedure and in some cases inadequate airway anastomosis. The surgical problems are characterized by a decrease in gas exchange, a diminished lung compliance, and occurrence of peripheral infiltrates (7, 14).
Another complication that can occur directly after transplantation is acute graft dysfunction or primary graft failure, in which early abnormalities after implantation are associated with pulmonary hypertension and rapidly progressive pulmonary edema (15, 16).
Infection As outlined in the preceding section, infections occur more frequent in
lung transplant recipients than in recipients of other solid organs, because of the higher levels of chronic immunosuppression and the constant exposure of the lungs to the external environment with potential pathogens (11, 12). The infections can be of bacterial, fungal, or viral origin.
11

- Chapter I -
The most common infection after lung transplantation is of bacterial origin with pneumonia as a consequence. This occurs most often in the first two months after transplantation. In the majority, bacterial pneumonia is caused by gram-negative bacilli (11, 12).
Fungal infection is another major threat and contributes significantly to the high morbidity and mortality rates in lung transplant recipients. Early fungal infections are mostly related to surgical complications, while in the period of 1-6 months after grafting opportunistic, relapsed, or residual infections can be observed. Fungal infections that develop after 6 months are usually associated with increased immunosuppression of the recipient due to the treatment of rejection or bronchial airway mechanical abnormalities. The majority of fungal infections in lung transplant recipients is caused by Aspergillus species, followed by Candida, Pneumocystis carinii, and Cryptococcus ( 12, 17).
Viral infections are also common after lung transplantation (12). Cytomegalovirus (CMV), a member of the J3-herpes virus family, is a common viral infection in lung transplant recipients ( 18, 19). CMV may be acquired from the donor lung, from blood products transfused from a seropositive donor, or from reactivation of endogenous virus. CMV infection usually occurs 1-3 months after transplantation, but this can be delayed by prophylactic administration of antiviral medication. CMV infection is often subclinical, but it can cause CMV disease which manifests clinically with rather nonspecific complaints and can be accompanied by a mononucleosis-like syndrome of fever, leukopenia and pneumonitis (12, 20). Patients at highest risk for CMV disease are those recipients who are seronegative for CMV and who receive an allograft from a seropositive donor, as well as those patients with CMV infection who require additional immunosuppressive therapy for treatment of rejection (21, 22). During recent years an effective therapy has been developed against CMV disease. This therapy consist of 2-4 weeks administration of intravenous ganciclovir (11, 20).
CMV is not the only herpes virus that can cause complications in lung transplant recipients; also Epstein-Barr virus (EBV) is associated with severe post-transplant diseases. It has been shown that EBV is responsible for post-transplant lymphoproliferative disease (PTLD). PTLD 1s characterized by uncontrolled B lymphocyte proliferation after transplantation. The incidence of PTLD in lung and heart-lung transplant recipients ranges from 1.5-9% (12, 23, 24). The initial treatment of PTLD is
12

- General introduction -
to decrease immunosuppression in order to allow the recipient's own immune system to remove the infected cells (25), however, chemotherapy and, more recently, treatment with monoclonal antibodies directed against CD20 (a B-cell antigen), are often required to successfully delete the infected B-cells involved in the PTLD (26, 27).
Besides CMY and EBY, also other viruses can contribute to complications in lung transplant recipients. These viruses are mostly respiratory viruses, such as influenza virus A and B, parainfluenza virus, respiratory syncytial virus and adenovirus. These virus infections occur over a broad time period after lung transplantation. In contrast to the systemic occurrence of CMY and EBY, these respiratory viruses infect only specific parts of the lung. Mostly this is the upper respiratory track in healthy persons. However, in immunocompromised patients these infections also involve the lower respiratory track (28-30). Respiratory infections are often mild and self-limiting, but can also lead to severe, life-threatening illnesses. The treatment of respiratory virus infections in lung transplant recipients remains rather empirical ( 12, 28, 29).
Acute rejection Acute rejection typically occurs in the first weeks up to six months after
transplantation. However, many studies report late acute rejection after this time period which implies that the risk of rejection remains present far after the transplantation procedure. Acute rejection can be accompanied by symptoms such as fever, cough and dyspnea (31 ). Acute rejection is usually diagnosed by a decrease in lung function and can be confirmed histologically in transbronchial biopsies. The most obvious feature of acute rejection is the presence of perivascular lymphocytic infiltration (32). Acute rejection is usually treated with a brief course of high-dose steroids, e.g. methylprednisolone (31 ).
Late graft failure With the growing success of clinical programs and the tremendous
advances made in technologies improving survival rates of patients, a new problem has developed, i.e. chronic rejection of the lungs. Chronic rejection of the lungs is predominantly characterized by an ongoing fibroproliferative process of the airways called bronchiolitis obliterans (BO). BO causes inflammation and fibrosis of the lamina propria and lumen and can be identified clinically by a progressive gradual decline in pulmonary function (33). Almost 50% of the lung recipients develop BO within 5 years after
13

- Chapter l
lung transplantation (6, 34, 35). Results of single center studies indicate that the incidence of BO can be reduced by refined patient surveillance (unpublished data). At present, BO is considered to be the major threat for long-term survival of engrafted lungs. Patient survival at 5 years after transplantation is 20-40% lower in patients with BO than in patients without BO. An even more dramatic illustration of the consequences of BO is the patient survival rate at 5 years after the onset of BO which is only 30-40% (6, 36).
The time between transplantation and first symptoms of BO can range from a few months to several years, but the median time of diagnosis is 16-20 months (35). The histopathologic features of BO are eosinophilic hyaline fibrous plaque formation in the submucosa of the small airways which results in partial or complete luminal occlusion. If inflammatory cells are present, the lesion is considered to be active and is characterized by intrabronchiolar and/or peribronchiolar submucosal and peribronchiolar mononuclear cell infiltrates. This is usually associated with ongoing epithelial damage. The injury of epithelial cells resulting from persistent inflammation in small airways leads to excessive fibroproliferation due to ineffective epithelial regeneration and aberrant tissue repair. If submucosal and peribronchiolar inflammatory infiltrates are absent, the lesion is considered to be inactive (32, 37).
The diagnosis of BO is based on histological examination of a transbronchial lung biopsy. These biopsies are usually difficult to obtain. Therefore, a clinical description of BO was introduced: the bronchiolitis obliterans syndrome (BOS) (38-40). BOS is a diagnosis based on the decline of pulmonary function, measured as forced expiratory volume in one second (FEVl ).
Table I. Bronchiolitis obliterans syndrome classification system (39)
Classification BOSO FEVl > 90% of baseline and
FEF25-75 > 75% of baseline BOS Op
BOSl BOS2 BOS3
FEVl 81-90% of baseline and/or FEF25-75 � 75% of baseline FEV 1 66-80% of baseline FEVl 51-65% of baseline FEVl< 50% of baseline
FEVJ:.forced expiratory volume in one second; FEF25-75%: forced mid-expiratory flow rates.
14

- General introduction -
A stable posttransplant baseline FEVl is defined as BOS stage 0. In patients who have a decrease in FEV 1, stages of BOS from 1 to 3 are defined based on the magnitude of the decrease. A "potential-BOS stage" (BOS 0-p) is defined as a decrease in mid-expiratory flow rates (FEF25-75) and/or FEVl (Table I).
To date, there are no effective therapies to prevent or to cure BO. Current treatment of BO includes: 1) modifying the maintenance therapy, for instance switching from cyclosporin-A to tacrolimus or switching from mycophenolate to azathioprine; 2) adding inhaled immunosuppressants, for instance aerosolized cyclosporin-A; 3) augmenting the immunosuppression, for instance high-dose methylprednisolone, anti-lymphocyte antibodies, methotrexate or cyclophosphamide; and/or 4) using other immune therapies, for instance total lymphoid irradiation or photopheresis ( 13, 37, 41). It should be emphasized, however, that these treatments can, at best, slow down the process of BO, but can not cure BO.
Besides BO, accelerated vascular sclerosis affecting pulmonary arteries and veins has been described as a manifestation of chronic rejection after lung transplantation, but this feature is not investigated thoroughly. Up to now only three studies described vascular changes after lung transplantation (42-44).
Risk factors for chronic rejection
Multiple factors have been implicated in the cause of chronic rejection after lung transplantation. In the next section the present views on mechanisms and factors determining success or failure of lung grafts will be discussed.
Surgery Complications associated with surgery are caused by inadequacies in the
technical procedures, such as incomplete airway anastomosis, physical trauma, or acute graft dysfunction (7, 14-16). With the advances made in transplantation surgery during the past two decades it has become evident that more factors before and during the surgical procedure can contribute to long-term failure. A phenomenon that will occur during transplantation is ischemia-reperfusion injury, which is inevitable in the period between removing the organ from the donor and anastomosis in the recipient. Ischemia-reperfusion induces a number of deleterious inflammatory
15

- Chapter 1 -
processes ( 45). Directly after reperfusion, reactive oxygen and other free radicals are released through the activity of iNOS in the transplanted organ. This is the basis for a whole sequence of effects, such as the release of tumor necrosis factor (TNF)-a, interferon (IFN)-y, interleukin (IL)-8, IL-10, IL-12 and IL-18 by both endothelial and inflammatory cells in the vicinity. These mediators will further activate both the neutrophils and vascular endothelium of the recipient. Activation of these cell types induces the further expression of adhesion molecules on both the neutrophils and donor endothelium leading to sustained inflammation (45). We think that this early aspecific inflammatory process may not only initiate acute rejection, but can have also a long-term effect after transplantation. In line with this, it has been suggested that ischemia-reperfusion injury increases the risk of BO after lung transplantation (46, 47).
During recent years, another pre-transplant factor has been identified that contributes to failure of transplanted organs, namely brain death. Brain death has been shown to have effects on hemodynamic stability, hormone regulation, and heart function (48-52). In humans, massive irreversible brain injury induces pulmonary inflammation with increased neutrophil infiltration and increased expression of interleuking-8 mRNA (53). Brain death in rats results in increased levels oflL-1, IL-2, IL-6, TNF-a, and IFNy in peripheral organs including the lung (54-57). Also, increased expression of immediate early genes FOS and JUN, intercellular adhesion molecule (ICAM)-1, vascular cell adhesion molecule (VCAM)-1, major histocompatibility complex (MHC) class II and increased infiltration of neutrophils are seen in kidneys and livers from brain-dead rats (54-56). Furthermore, accelerated acute rejection of heart and kidney allografts in rats has been observed after transplantation of grafts from brain-dead donors (58, 59). Whether brain death has an effect on the development of chronic rejection has still to be investigated.
Infection CMV infection is a common viral complication after lung transplantation
and has been suggested as a causative factor in the development of chronic rejection (60-64). In healthy individuals CMV causes a persistent and latent infection. In the immunocompromised host CMV can reactivate. Due to the strong immunosuppression lung transplant recipients, more than other organ transplant recipients, are at risk for CMV infection and disease (18, 19). At present, the exact role of CMV in aggravation of chronic rejection is subject
16

- General introduction
of debate with studies that show that CMV is associated with graft failure in lung transplant patients ( 61, 62), while other studies claim an absence of effect (65, 66). In part this might be explained by an incomplete insight in the pathogenesis of the contribution of CMV infection on chronic rejection.
Respiratory viruses, such as influenza A and B virus, parainfluenza virus, human respiratory syncytial virus, and adenovirus infect mostly the upper respiratory track in healthy persons. However, in immunocompromised patients, these infections also involve the lower respiratory track (28-30). Some clinical studies indicate that respiratory viral infections can cause acute airway damage after transplantation (67, 68). The mechanism leading to allograft damage by respiratory viruses has been suggested to occur via stimulation of production of cytokines such as IL-1, TNF, IL-6 and IL-8 during viral replication (69-72). Current clinical data suggest a possible role for respiratory viruses in the development of BO, but this relationship remains to be confirmed (30, 73-75).
Acute rejection Acute allograft rejection remains one of the most common complications
after lung transplantation (31). This process may start in the absence of adequate levels of immunosuppression when the immune system of the host detects non-self antigens in the transplanted donor organ. These non-self antigens are mostly derived from the major histocompatability complex (MHC) of the donor. Host T cells can recognize these non-self antigens via two different pathways, i.e. the indirect and direct pathway. In the indirect pathway, donor MHC alloantigens, either class I or class II molecules, are internalised by recipient antigen presenting cells before being processed and presented to T cells as a foreign peptide, with a response to recipient MHC molecules as a consequence. This is the classical way in how the immune system normally recognizes antigens. The direct pathway however is unique to transplantation. In this pathway, the T cell receptor (TCR) directly recognizes an intact allo-MHC in the donor organ as foreign. This direct recognition can occur both on the level of MHC-I and on the level of MHCII. The TCR of CDS+ T cells recognizes allo-MHC class I antigens, whereas the TCR of CD4+ T cells recognizes allo-MHC class II antigens. Irrespective of the type of binding the net result is the same: expansion of the alloreactive T cell population and eventually cytolysis of the donor tissue by these T cells as a consequence (76). Both pathways can lead to acute rejection.
1 7

- Chapter I
Most lung transplant recipients have at least one episode of acute rejection. The majority of these acute rejection episodes occur within six months after lung transplantation (77, 78). Acute rejection has been identified in many studies as a statistical risk factor for chronic rejection. Importantly, more frequent acute rejection episodes enhances the risk for chronic rejection. Also, the risk increases when the acute rejection is histologically severe or when it persists or reoccurs after treatment (79-82). There are also some studies that describe the role of late acute rejection in the development of chronic rejection (80, 81 ).
Hypothesis
At present, chronic rejection with BO as a consequence is considered to be the major and leading threat for long-tenn function and survival of lung grafts. Unfortunately, a complete insight in the etiology and pathophysiology of chronic rejection is lacking. Both alloimmunedependent and alloimmune-independent factors appear to play a role in the development of chronic rejection. Based on the above review of risk factors for chronic rejection we hypothesize that early damage before, during or early after transplantation can cause an inflammatory response which can have an effect on the development of chronic rejection after lung transplantation.
More understanding of the processes responsible for chronic rejection is required in order to design means to interfere with the processes. To provide sufficient insight in the etiology and pathogenesis of chronic rejection, animal models are required that mimic the human BO after transplantation. Experimental studies have used different animal models to study BO. These will be discussed in more detail in the next paragraph.
Animal models for chronic rejection
Heterotopic trachea transplantation The first model consists of a heterotopic trachea transplantation. This is a
useful and a commonly applied model to study the pathogenesis of BO. In this model tracheas are transplanted subcutaneously. This model is applied mainly in rats and mice (83-86). Transplantation of tracheas subcutaneously leads to consistent and reproducible airway obliteration, called the obliterative airway disease (OAD). It has been shown that the histological
1 8

- General introduction -
findings resemble those of human BO. This heterotopic transplantation model has provided us with new insights in the pathogenesis of OAD. It has been shown that damage to the bronchial epithelium causes complete luminal epithelial loss which leads to fibrous obliteration of the airway lumen (84, 87, 88). This is corroborated by studies showing that the loss of airway epithelium either by enzymatic removal in isografts (84, 89) or by transplant rejection in allografts results in OAD (89, 90). The reseeding of epithelial cells in the isografts or regrowth in allografts reduced the degree of OAD.
Also, the trachea transplantation model has been very useful in elucidating immunological processes in the development of BO. It has been shown that the severity of rejection by CD4+ and CD8+ T cells, macrophages, and granulocytes determine the degree of OAD (9 1-93). Furthermore, it has been shown that an allogeneic transplantation of tracheas showed a strong and persistent Thi response (expression of IL-2 and IFN-y) after transplantation (92, 94). Also, the chemokines Rantes and monocyte chemotactic protein (MCP)-1 were found to be increased late after transplantation (94-96).
Heterotopic bronchial transplantation In a second model, pieces of terminal bronchi were transplanted
subcutaneously in pigs. This model was used, because it resembles the clinical situation more closely than the trachea transplantation model, because human BO originates in terminal bronchi. In this model, the epithelium disappeared already 2 weeks after transplantation and total luminal obliteration with fibrous tissue developed within 2 1 days after transplantation (97, 98). Studies using this pig model showed an influx of immune cells like CD4+ T cells, CD8+ T cells and other MHC class II expressing cells in lung fragments with total luminal obliteration of the bronchi (99).
Although the heterotopic models can be useful for studying BO, it should be emphasized that there are some essential differences with the clinical situation which might influence the progress of BO development. First, the tracheas and pieces of terminal bronchi are transplanted non-vascularized and depend on vascular access on neovascularization after grafting. Second, in the heterotopic models airway obliteration develops within a few weeks after transplantation as a result of acute rejection, only when the
19

- Chapter 1 -
transplantation is performed between fully MHC mismatched animals and no immunosuppression is given. In the clinical situation BO is a chronic process and usually develops during a period of months despite the presence of immunosuppression.
Orthotopic lung transplantation The third model for studying BO is the orthotopic lung transplantation
model. This model is performed in large animals such as pigs and in small animals such as rats. Lung transplantation studies in large animals that show chronic changes are scarce. Al-Dossari et al. (100) demonstrated BO after lung transplantation in pigs. In this study, the pigs were given the triple-type immunosuppression (cyclosporin-A, azathioprine, and prednisone) and six months after transplantation, the lungs showed progressive fibrous inflammatory occlusion of the bronchioles typical of BO. The orthotopic lung transplantation model in rats is more convenient and used more often. A rat lung transplantation model was developed in Groningen (101, 102). In this model they were the first to show that BO was secondary to acute pulmonary rejection (103). Also in a rat model Matsumura et al. (104) and Hirt et al. ( 105) described airway inflammation with destruction of the subepithelial layer of the smaller airways which resulted in severe BO in lung grafts on day 60 and 100 after transplantation. These results were corroborated by Y asufuku et al. (106) who observed BO at 70 days after lung transplantation.
The orthotopic lung transplantation model seems more suitable for studying BO, because this model resembles the clinical situation more closely than the heterotopic models. Therefore, we choose the orthotopic transplantation of lungs in rats as model to investigate risk factors for chronic rejection after lung transplantation.
20

Chapter 2
Aim of the thesis

- Chapter 2 -
Chronic rejection after lung transplantation is considered to be a major threat for long-term survival of engrafted lungs. In the clinical situation, chronic rejection manifests as bronchiolitis obliterans with failure of the graft as a consequence. Although, many factors have been assumed to be involved in the development of chronic rejection, a complete insight in the etiology and pathophysiology of chronic rejection after lung transplantation is still lacking. Therefore, the overall aim of this thesis is to study whether damage before, during or early after transplantation has an effect on the development of chronic rejection after lung transplantation. This will be done in an orthotopic lung transplantation model in rats and also in humans.
As reviewed in Chapter 1 pre-transplant factors such as the transplant surgery, ischemia-reperfusion injury, and brain death may have deleterious effects on the quality of the lung and are therefore considered to be early factors in the initiation of chronic rejection.
In Chapter 3, we investigated the hypothesis that brain death increases inflammatory mediators in the donor lung and subsequently aggravates chronic rejection of the lung after transplantation in rats.
Not only pre-transplant factors but also early post-transplant risk factors such as infections and acute rejection are assumed to be involved in the development of chronic rejection. Therefore, we studied the role of two types of virus infections in the pathophysiology of chronic rejection. First, we looked at a respiratory virus infection with Sendai virus, which locally infects epithelial cells of the airways. Next, we analyzed a virus infection which disseminates systemically, i.e. CMV infection.
In Chapter 4 we studied whether acceptance of the lung can be abrogated by local Sendai virus infection in the lungs of rats.
However, not only a local infection, but also a systemic virus infection may lead to a higher risk for chronic rejection. This is not necessarily caused by direct damage of the organ by the virus, but can also be caused by virus-induced changes in the recipient's immune system. In Chapter 5 we tested the hypothesis that one mechanism by which CMV could enhance rejection of lung grafts is through generation of immune effector cells during CMV infection and immunosuppression. These effector cells may have the capacity to promiscuously recognize CMV-infected tissue cells, including CMV-infected allogeneic tissue cells, which can lead to an increased lung graft infiltration. The relevance of these findings for the clinical situation is studied in Chapter 6 in which we tested the hypothesis that human CMV (HCMV) may enhance graft-directed responses by accumulation of effector type CD45RA+CD8+CD2T T cells that, through
22

- Aim of the thesis -
expression of NKG2D (an activating receptor), promiscuously recognise HCMV-infected and MICA (an MHC class I related chain molecule) expressing target cells.
Finally, the results described in this thesis are summarized and discussed in Chapter 7.
23

24

Chapter 3
Donor brain death aggravates chronic rejection after lung transplantation in rats
Noelle Zweers 1, Arjen H. Petersen 1
, Joost A.B. van der Hoeven2,
Aalzen de Haan 1 , Rutger J. Ploeg2, Lou F .M.H. de Leij 1 , Jochum Prop 1 '3
1 Department of Pathology and Laboratory Medicine, Medical Biology section, 2Department of Surgery, and 3Thorax center, University Medical
Center Groningen, University of Groningen, The Netherlands
Transplantation 2004, 78 (9): 1251 - 1258

- Chapter 3
Abstract
Background. Many rec1p1ents of lung transplants from brain-dead donors develop bronchiolitis obliterans, a manifestation of chronic rejection. It has been shown that brain death increases inflammatory mediators and accelerates acute rejection in kidney, liver, and heart transplants. In this study, we investigated the hypothesis that brain death increases inflammatory mediators in the donor lung and subsequently aggravates chronic rejection of the lungs after transplantation in rats.
Methods. Brain death was induced in f 344 rats by inflation of a subdurally placed balloon catheter. After 6 hr, donor lungs were assessed for influx of leukocytes, expression of cell adhesion molecules, and cytokine mRNA expression. For assessment of the lung after transplantation, lungs from brain-dead F344 rats were transplanted in WKY rats. Lung function after transplantation was monitored by chest radiographs during an observation period of 100 days. At the end of this period the lungs were histologically examined; also, cytokine mRNA expression was measured. Lungs from ventilated living donors and living donors served as controls.
Results. After 6 hr of brain death, influx of polymorphonuclear cells and macrophages and expression of vascular cell adhesion molecule-I in the donor lungs was increased. After transplantation at postoperative day 1 00, the lung function was significantly decreased compared with allografts from living donors. In the lung allografts from brain-dead donors histologic symptoms of chronic rejection were obvious, including severe intimal hyperplasia but without bronchiolitis obliterans. IL-2 mRNA was significantly increased in allografts from brain-dead donors compared to living donors.
Conclusions. This study shows that brain death induces an inflammatory response in the donor lung and subsequently aggravates chronic rejection after transplantation. This may explain the clinical difference in long-term function between lungs from cadaveric donors and living donors.
Introduction
Lung transplantation has become a therapeutic method for patients with end-stage pulmonary diseases. Despite receiving immunosuppressive therapy, 50% of the lung recipients develop chronic rejection within 5 years after lung transplantation ( 1 07). Chronic rejection after lung transplantation
26

- Donor brain death aggravates chronic rejection of lung grafts -
usually manifests as bronchiolitis obliterans (33), a fibroproliferative process identified histologically by inflammation and fibrosis of the lamina propria and lumen (32), and clinically by a progressive decline in pulmonary function (33). Besides bronchiolitis obliterans, accelerated vascular sclerosis affecting pulmonary arteries and veins has been described as a manifestation of chronic rejection ( 42, 43). The pathogenesis of chronic rejection is still unclear, but many risk factors have been implicated in the development of chronic rejection after lung transplantation, including number and severity of acute rejection episodes, cytomegalovirus infection and human leukocyte antigen mismatching (79, 80).
Strikingly low is the incidence of chronic rejection in pediatric lungs transplanted from living donors compared with cadaveric donors (108, 109). An obvious difference between living and cadaveric donors is brain death of the latter. Brain death has been shown to have effects on hemodynamic stability ( 48-50), hormone regulation ( 48, 50) and heart function (51, 52). Also, an increase of inflammatory mediators has been shown in kidneys and livers from brain-dead rats (54-56). After transplantation of organs from brain-dead donors, acute rejection of heart and kidney transplants was found to be accelerated in rats (58, 59). Although little is known about the effect of brain death on the lung (54), it is conceivable that the positive results after pediatric living-donor transplantations correlate with the absence of brain death. However, such an effect of the donor condition on the long-term results after lung transplantation has never been investigated.
Therefore, we investigated the hypothesis that brain death increases inflammatory mediators in the donor lung and subsequently aggravates chronic rejection of the lungs after transplantation. For this study, a rat strain combination prone to result in mild chronic rejection was used (104, 105).
Materials and Methods
Experimental design In this study, we examined the effect of brain death in the donor lung and
in the lung after transplantation in rats. The effect of brain death in donor lungs was studied in Fischer F344 rats. In these rats, brain death was induced by inflating a subdurally placed balloon catheter. After 6 hr of brain death, lungs were taken out and immunohistochemically stained for inflammatory markers; also, cytokine mRNA expression was measured
27

- Chapter 3
(n=4). Ventilated living donors without brain death induction (n=3) and living donors (n=3) served as controls.
In the transplantation study, left lungs of F344 rats after 6 hr of brain death were transplanted in Wistar Kyoto (WKY) rats (n=4). Lungs transplanted from ventilated living donors (n=3) and living donors (n=3) served as controls. As additional control groups without rejection syngeneic transplantations from brain-dead donors and living donors were performed (n=3 in each group), using F344 rats for donor and recipient. Lung function after transplantation was monitored at regular intervals by chest radiographs during an observation period of 1 00 days. At the end of this period, the lungs were histologically examined for symptoms of chronic rejection; also, cytokine mRNA expression was measured in the lungs.
Animals Specific pathogen-free inbred male F344 (RTl Ivl ) and WKY (RTl 1) rats
weighing 250-350 g were obtained from Harlan (Horst, the Netherlands). The rats were fed standard rat chow and acidified water ad libitum. Animal experiments were performed after receiving approval of the institutional Animal Care Committee of the Groningen University. All animals received human care in compliance with the Dutch Law on Experimental Animal Care.
Brain death procedure A model of brain death was used as described previously for a study
focussed on liver and kidney after brain death in our institution (55, 56). Rats were intubated and ventilated on a pressure controlled MK2 infant ventilator (Loosco, Amsterdam, The Netherlands) with a mixture of nitrous oxide and oxygen and with a stroke rate of 50 strokes/min and peak inspiratory pressure of 14 to 1 6 cm H20. Halothane anesthesia was used in all donor rats until the induction of brain death. Intra-arterial blood pressure was monitored by means of a PE50 catheter placed in the left femoral artery and attached to a transducer and recorder (Life Scope 9, Nihon Kohden Corporation, Japan).
To induce brain death, a balloon catheter (Fogarty 4F, Baxter Health Care Corporation, Irvine, CA) was introduced into the subdural space through a frontolateral burr hole. The balloon catheter was inflated for 1 min with 0.5 ml of saline, thus increasing the intracranial pressure, which lead to immediate brain death. The onset of brain death was indicated by a sharp increase and subsequent drop of blood pressure. Brain death was confirmed
28

- Donor brain death aggravates chronic rejection of lung grafts -
by the absence of corneal reflexes and an apneu test. From 30 min after brain death induction, the rats were ventilated with 30% oxygen in air until 6 hr after brain death induction. The rats were kept normotensive by colloid infusion (0.9% saline containing hydroxyethyl starch (HES), 5 g/%) in the tail vein during the 6 hr of brain death. Normotension was defined by a mean arterial pressure (MAP) between 80 mmHg and 120 mmHg. The infusion was started 15 min after brain death induction, allowing a short phase of hemodynamic stabilization after brain death. Body temperature was monitored by a rectal probe and maintained at a temperature of 37°C with a heating blanket (Harvard Apparatus, Holliston, MA).
Ventilated living animals served as controls. In these animals, a frontolateral burr hole was created without inducing brain death. The rats were ventilated for 6 hr and were kept normotensive.
Lung transplantation procedure For the transplantation study, left lungs were transplanted orthotopically
as described previously (101). Briefly, the donor lung was dissected from brain-dead donors, ventilated living donors and living donors, with immediate flushing of the vascular bed with cold saline. The recipient's left lung was removed and replaced with the donor lung; the pulmonary vein and artery were anastomosed first, followed by the bronchus.
Lung function after transplantation To monitor the function of the transplanted lungs during the 100 days
follow-up period, chest radiographs were taken at regular intervals under halothane anesthesia. Of each chest radiograph, a ventilation score of the left lung was determined by two blinded independent observers (110). The ventilation scores range from 6 for normal looking lungs to O for opaque lungs.
Immunohistochemistry of donor lungs For detection of inflammatory markers in the donor lungs, cryostat
sections of snap-frozen lung tissue were evaluated immunohistochemically. To this end, the lungs were taken out from the donors and were intratracheally infused with OCT compound (Tissue-tek, Miles, Inc., Elkhart, IN) diluted 1: 1 in saline. A part of the lung was snap-frozen in liquid nitrogen and stored at -80°C until immunohistochemical evaluation. The snap-frozen lung tissue was cut in 5-µm sections, acetone fixed (for 10
29

- Chapter 3 -
min at room temperature), and air dried. Sections were incubated with 0.075% hydrogen peroxide for 30 min to block endogenous peroxidase. Sections were rinsed in 0.01 M phosphate-buffered saline (PBS) and incubated with the primary antibodies indicated below for 60 min. The primary antibodies used, were directed against polymorphonuclear (PMN) cells (His 48), macrophages (EDl and ED2), CD4+ T cells (ER2), CD8+ T cells (OX-8), vascular cell adhesion molecule (VCAM)-1 (5F10) and intercellular adhesion molecule (ICAM)-1 (1A29). After washing with PBS, sections were incubated for 30 min with a second-step peroxidase conjugated rabbit anti-mouse antibody (DAKO A/S, Glostrup, Denmark) in a 1 :40 dilution in PBS supplemented with 1 % normal rat serum. After washing with PBS, peroxidase activity was visualized using 3-amino-9-ethyl carbazole (Sigma, St. Louis, MO) for 10 min. Sections were counterstained with Mayer's hematoxyline (Merck, Darmstadt, Germany) and mounted in Kaiser's glycerol gelatin (Merck). As a control, sections were incubated with PBS instead of the primary antibodies. No staining was observed in these control sections.
Quantitation of immunohistochemical staining was assessed blindly by light microscopy. In the sections stained for PMN cells, macrophages, CD4+
T cells, and CD8+ T cells, quantitation of stained cells was performed by counting the total number of positive cells per microscopic field in ten fields at 400x magnification. The amount of VCAM-1 and ICAM-1 staining was scored as negative (no staining), weakly positive, or strongly positive.
Histological analysis of transplanted lungs To analyze symptoms of chronic rejection in transplanted lungs, these
lungs and the nontransplanted right lungs were removed at day 100 after transplantation. A part of the lung was snap frozen in liquid nitrogen en stored at -80°C for polymerase chain reaction (PCR) analysis (see below). Most of the lung was fixed in formalin and embedded in paraffin. The embedded lungs were cut in 3-µm sections and stained with hematoxylineosin and with Verhoeff-van Gieson for elastin fibres.
To assess thickness of the intima of pulmonary vessels, Verhoeff-stained sections were analyzed blindly using morphometry. In each section, using a light microscope with a camera attached, images were made from several blood vessels at a magnification of 400x. In these images the percentage of intima surface area was calculated from the total surface area within the internal elastic lamina using a computer graphics program (Adobe
30

- Donor brain death aggravates chronic rejection of lung grafts -
Photoshop Elements 1.0; Adobe Systems Inc., San Jose, CA). In each lung a mean of 22 (range 10-35) blood vessels were analyzed.
Real-time reverse-transcriptase PCR for cytokine mRNA expression Real-time reverse-transcriptase {RT) PCR was performed to quantify
cytokine mRNA expression in snap-frozen lung tissue, cut in 10-µm sections. Total RNA was isolated from four sections of 10 µm using the Strataprep Total RNA Microprep Kit (Stratagene, Amsterdam, The Netherlands) as described in the manufacturer's protocol. Total RNA was subsequently reverse-transcribed to cDNA in 20 µl of reaction mixture containing 2 µl lOx RT buffer, 2 µl of 5 mM dNTP mixture, 1 µl Sensicript reverse transcriptase (Sensiscript kit, Qiagen, Leusden, the Netherlands), 2 µl 66 of µM oligo-dT primer (Invitrogen, Leek, The Netherlands), 1 µl RNase inhibitor (10 U/µl, Invitrogen), 2 µl of RNase-free water, and 10 µl of RNA. The mixture was incubated at 37°C for 60 min, then inactivated at 93°C for 5 min. The cDNA was stored at -20°C until further analysis.
Real-time RT-PCR was performed using interleukin (IL)-2, IL-4, IL-10, and transforming growth factor {TGF)-P Taqman Pre-Developed Assay Reagents (Applied Biosystems, Foster City, CA). Primers and F AM-MGB labeled probes were designed by the manufacturer. P-actin was used as an internal control for differences in starting mRNA concentrations. The sequences for the P-actin specific primers and FAM-TAMRA labeled probe were as follows: forward primer, 5'-ACCGTGAAAGATGACCCAGAT-3'; reverse primer, 5'-TGGTACGACCAGAGGCATACAG-3'; and probe, 5'AGACCTTCAACACCCCAGCCATGTACGTA-3'. PCR reactions were performed in 384-well optical reaction plates and contained 2x Taqman Universal PCR Master Mix (Applied Biosystems), the 20x primer and FAM-labeled probe mixture for the cytokines or primers-probe mixture for P-actin (50 µM sense and antisense primers, and 5 µM FAM-labeled probe), RNase-free water, and 1 µl of sample cDNA in a total volume of 20 µI. PCR reactions were run on an ABI Prism 7900 Sequence Detection System (Applied Biosystems) with the following protocol: 50°C for 2 min, 95°C for 10 min, and then 40 cycles at 95°C for 15 sec and 60°C for 1 min. Each sample was run in triplicate.
Results of the real-time PCR data were represented as Ci value, the threshold cycle. The C1 value was defined as the PCR cycle number at which the fluorescent signal crossed the threshold line. Differences in the C1
for the cytokines and the Ci for P-actin, called �C1, were calculated to
31

- Chapter 3 -
normalize for the differences in quality and amount of input cDNA. The �Ct
for each experimental sample was subtracted from the �Ct of normal lung tissue, i.e. the ��Ct value. The n-fold difference of the experimental samples relative to normal lung tissue was expressed as 2Mct_
Statistical Analysis All results are expressed as mean ± standard error of the mean (SEM).
Statistical comparisons between groups were performed by the MannWhitney U-test. A value of P<0.05 was considered statistically significant.
Results
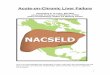
Brain death procedure The effect of induction of brain death on blood pressure showed a typical
pattern (Fig. 1). Before brain death, the MAP was 94.0 ± 0.9 mm Hg. During induction of brain death, MAP increased to maximum values of 178.3 ± 2.6 mm Hg and then gradually declined within 15 min to hypotension (i.e. a mean value of 66.0 ± 2.8 mm Hg). After infusion of hydroxy-ethyl starch (HES), from 15 min after brain death induction, MAP was stabilized at normotension (i.e. a mean value of 102. 7 ± 4.4 mm Hg). In the ventilated living control rats, the MAP remained constant at a mean of 92.6 ± 0.7 mm Hg during the 6-hr period.
The procedure for induction of brain death in F344 rats proved to be consistent and reproducible. Of a total of 22 procedures (including pilot experiments for this study), only 4 inductions were not successful; these resulted from severe hypotension after brain death induction that was not recoverable.
Immune activation in donor lungs Brain death induced a significant influx of leukocytes into the lungs. The
number of PMN cells in the brain-dead donor lung was significantly higher compared with ventilated living donors and living donors (Fig. 2). Also, the number of ED I -positive macrophages was significantly increased after 6 hr of brain death compared with controls. The number of ED2-positive macrophages showed a pattern similar to the ED 1 staining, but the absolute numbers were smaller. The number of CD4 T cells and CD8+ T cells in the donor lung was low, and no significant increase in CD4+ T cells and CD8+ T
32

- Donor brain death aggravates chronic rejection of lung grafts -
cells counts were found in brain-dead donors compared with ventilated living donors and living donors.
240 1 1 Balloon
j inflation
200 l
1 60 ai
E ,S. 1 20 .. 0.
40
0
HES infusion -
- Brain-dead donor
- - - - Venti lated l iving donor
,,,__ - - Jr- - - r,-- - - - .,.. - - ."TIit - -
II , 0 1 0 20 30 40 50 60 60 1 20 1 80 240 300 360
Time (minutes)
Figure 1. Changes in MAP after induction of brain death in rats. MAP is expressed as mean ± SEM Brain death caused an immediate increase and subsequent decline of the MAP to hypotension. After infi1sion of HES from I 5 min after brain death induction, the MAP returned to normotension. MAP of ventilated living control rats remained normotensive throughout the period of 6 hr.
Of the adhesion molecules, VCAM-1 was strongly expressed on endothelial cells in lungs of brain-dead donor rats. VCAM-1 was stained weakly in lungs of ventilated living donors, and no VCAM-1 expression was seen in lungs of living. !CAM-I -staining showed no differences in expression between lungs of brain-dead donors and controls due to high constitutive expression of ICAM-1 in alveolar epithelium in all groups.
Cytokine mRNA analysis for IL-2, IL-4, IL-10, and TGF-P revealed no increases caused by brain death.
33

- Chapter 3
40 * • Brain-dead donor
D Ve ntilated living donor
D Liv ing donor
"0 30
.!:! CL
u 20
u *
cii 10 0
o l PM N ED1 + M 0 ED2+ M0 CD4+ T cells CDS+ T cells
Figure 2. lmmunohistochemical analysis of leukocyte infiltration in lungs of brain-dead donors, ventilated living donors, and living donors. Values are the mean ± SEM number of positive cells per microscopic field. After 6 hr of brain death, numbers of P MN cells, ED]positive macrophages (M0) and ED2-positive macrophages in the lung were increased compared with the control groups. P< 0.05 compared with ventilated living donors and living donors.
Chronic rejection of transplanted lungs
Lung function The lung function of rats, as monitored by ventilation scores on chest
radiographs, showed distinct differences between the groups during the follow-up period of 100 days after transplantation (Fig. 3). Allografts from brain-dead donors, ventilated living donors and living donors showed all a good lung function shortly after transplantation, indicating that the transplantation procedure was successful. Subsequently, the ventilation score decreased at 14 days after transplantation, a phenomenon consistent with a rejection episode (102). This decrease was more pronounced (P < 0.05) in lungs from allogeneic brain-dead donor rats than in lungs from allogeneic living donor rats. From 14 days onward, the ventilation scores of allografts from brain-dead donor rats remained to be low until the end of the observation period: in half of these lungs, function was virtually absent, but
34

- Donor brain death aggravates chronic rejection of lung grafts -
the rats survived with a functional right lung. The ventilation scores of allografts from ventilated living donors at 14 days after transplantation were slightly higher compared with brain-dead donors and remained so until 100 days after transplantation. The chest radiographs of living donors clearly improved to normal ventilation scores at 100 days after transplantation, being significantly better than the chest radiographs of lungs from braindead donor rats. Syngeneic lungs from brain-dead donors and living donors showed normal ventilation scores until the end of the observation period, indicating that brain death had no influence on lung function in the absence of rejection.
6
5
:;i 4 C 0
� = 3 C
#
* 0 ------- --- --�- ----
0 20 40 60 80
Days after transplantation
1 00
_._ Allo BD -e- Allo VLD --.- Alie LD --- syn BD -a- Syn LD
Figure 3. Lung function after transplantation determined as ventilation scores of left lung grafts on chest radiographs. Values are expressed as mean ± SEM The lung jimction of allografts from brain-dead donors (Alla BD) is significantly decreased compared with living donors (Alla LD) and ventilated living donors (Alla VLD). Lungs of syngeneic braindead donors (Syn BD) and syngeneic living donors (Syn LD) showed normal ventilation scores. *P<0. 05 compared with allogeneic living donors; #P< 0. 05 compared with allogeneic ventilated living donors.
Histology All lung allografts at 100 days after transplantation showed phenomena
of rejection as judged from light microscopical evaluation (i.e. perivascular, peribronchiolar, and interstitial leukocyte infiltration). Peribronchiolar and
35

- Chapter 3
perivascular infiltrates were severe in the lungs from brain-dead donors. The dense perivascular infiltrates extended into alveolar septa and spaces (Fig. 4A). In two of the lungs, alveolar spaces were almost completely filled with cells or fibrosis, consistent with the poor chest radiography scores. The lungs from living donors showed less severe perivascular infiltrates and were devoid of peribronchiolar and interstitial infiltration (Fig. 4B). Leukocyte infiltration in the lungs from ventilated living donors were intennediate between those in the other two groups. Syngeneic brain-dead donors and living donors showed normal lungs with open alveoli and no infiltration of cells.
Figure 4. Histology of lung al/ografts JOO days after transplantation. (A) Venule in lung allograft from brain-dead donor showing heavy perivascular and interstitial leukocyte infiltration (hematoxylin-eosin; magnification xJOO). (BJ Venule in lung allograft from living donor showing only small perivascular infiltrates (hematoxylin-eosin; magnification xJOO). (CJ Bronchiole in lung allograft from brain-dead donor showing no signs of bronchiolitis obliterans in the airways such as epithelial damage or fibrosis (Verhoeff-van Gieson; magnification x50). (DJ Artery in lung al/ograft from brain-dead donor showing significant hyperplasia of the intima within the e/astica interna (arrows) (Verhoeff-van Gieson; magnification xJOO).
36

- Donor brain death aggravates chronic rejection of lung grafts -
In all lungs of this study, bronchiolitis obliterans was remarkably absent, even in airways with severe lymphocytic infiltration; epithelial damage or fibrosis was not observed in any of the lungs (Fig. 4C).
Intimal hyperplasia, however, was observed in many of the pulmonary vessels. Severe intimal hyperplasia was observed in vessels of allografts from brain-dead donor rats at 100 days after transplantation (Figs. 4D and 5). Morphometric analysis showed that the mean surface area of the intima in arteries and veins in allografts from brain-dead donors was approximately 50% and was significantly increased compared with allografts from ventilated living donors and living donors. Syngeneic lungs from brain-dead donors and living donors showed normal blood vessels with a mean surface area of the intima of approximately 10%, again indicating that the effect of brain death is not seen in the absence of rejection.
60
*
GI "' GI 40
� � "' 20
0
Allo 8D Allo VLD Allo LD Syn 8D Syn LD
Figure 5. Morphometric analysis of the intima of pulmona,y vessels in lungs transplanted ji·om allogeneic brain-dead donors (A/lo BD), ventilated living donors (A/lo VLD), and living donors (A/lo LD), and in lungs of syngeneic brain-dead donors (Syn BD) and living donors (Syn LD). Values are expressed as mean ± SEM Lung allografts ji-om brain-dead donors showed a significant increase in the mean surface area of the intima of blood vessels compared with lungs ji-om ventilated living donors and living donors. P<0.05 compared with allogeneic ventilated living donors, allogeneic living donors, and syngeneic brain-dead donors; "P< 0. 05 compared with syngeneic living donors.
37

- Chapter 3 -
lntragraft cytokine mRNA expression In lungs transplanted from allogeneic brain-dead donors IL-2 mRNA was
significantly increased compared to lungs from allogeneic living donors (Fig. 6). No increases of IL-4, IL-10, or TGF-f3 mRNA expression were found in lungs of allogeneic brain-dead donors compared to living donors. IL-2, IL-4, and IL-10 mRNA expression was significantly increased in lungs from allogeneic living donors compared with syngeneic living donors.
30 O ct Q) z
:(l a::E 20
e u Q) C C
� :ii: 10 - 0 .E >, :z u
0
30 0 ct Q) z
:(I 11::E
20 e u Q) C C
� :ii: 1 0 - 0 .E >, :z u
0
A. IL-2
*
Allo Allo Allo
BD VLD LD
C. IL-4
I •
#
•
Iii Syn Syn
BD LD
# - -
Allo Allo Allo Syn Syn
BD VLD LD BD LD
30
20
1 0
0
30
20
1 0
B. IL-1 0
# I I 11 Allo Allo Allo
BD VLD LD
D. TGF-13
... -Syn Syn
BD LD
o I •--.-• - - -Allo Allo Allo Syn Syn
BD VLD LD BD LD
Figure 6. Cytokine mRNA expression in lungs transplanted from allogeneic brain-dead donors (Alla BD), ventilated living donors (A/lo VLD), and living donors (A/lo LD), and in lungs of syngeneic brain-dead donors (Syn BD) and living donors (Syn LD). Values are expressed as mean ± SEM Lung allografts from brain-dead donors showed a significant increase in IL-2 mRNA expression compared with allografts from living donors. In all allograft groups, the mRNA of IL-2, Jl-10, and IL-4 was higher than in the syngeneic groups. •P<0.05 compared with allogeneic living donors; #P< 0.05 compared with syngeneic living donors.
38

- Donor brain death aggravates chronic rejection of lung grafts
Discussion
This study shows that brain death induces an inflammatory response in the donor lung and aggravates chronic rejection long-term after lung transplantation. Such immediate and long-term effects have been suggested in several studies, but all experimental studies so far were focussed on heart, kidney, and liver transplantation and only one of these included long-term observations. This article is the first to correlate immediate effects of brain death in the donor with long-term outcome after lung transplantation.
Our first conclusion is that brain death of the donor rat induces an inflammatory response in the donor lungs: increased numbers of PMN cells and macrophages and increased VCAM-1 expression were found. This is in line with the clinical observation that massive irreversible brain injury induces pulmonary inflammation with increased neutrophil infiltration and increased expression of IL-8 mRNA (53). In experimental studies on kidney and liver, Takada et al. (54) and van der Hoeven et al. (55, 56) found a similar increase in PMN cells and macrophages after brain death in rats. Also, increased VCAM-1 expression has been shown in kidneys, livers and hearts of rats 6 hr after brain death (55, 56, 111). Thus, the inflammation that we found in the lung after brain death is consistent with clinical and experimental observations of increased inflammation in the lung and in other organs after brain death.
Can this inflammatory response in the donor lung induce changes after transplantation? It has already been shown that, after heart and kidney transplantation, brain death of the donor results in accelerated acute rejection, with increased expression of cytokines, chemokines, and adhesion molecules and infiltration of leukocytes 7 days after transplantation (58, 59). In our study, acute rejection was not investigated histologically but was monitored by lung function based on chest radiographs obtained at various time points after transplantation (102). In this way, function of lung transplants from brain-dead donors was decreased at 14 days after transplantation. This decrease is indicative of an intensive episode of acute rejection similar to the increased acute rejections in other organ grafts from brain-dead donors (58, 59).
Our second conclusion is that brain death of the donor rat aggravates chronic rejection long-term after lung transplantation. This is supported by the decreased lung function; heavy perivascular, peribronchiolar, and interstitial leukocyte infiltration; severe intimal hyperplasia in blood vessels
39

- Chapter 3 -
of the transplant; and increased cytokine mRNA expression (IL-2). We presume that the mechanism leading to the aggravated chronic rejection is initiated by the inflammatory response in the lungs from brain-dead donors. On transplantation, the activated endothelial cells -expressing elevated levels of VCAM-1 (Fig. 3), ICAM-1, P-selectin and E-selectin (54)- will stimulate adhesion of leukocytes to the endothelium as well as the subsequent transendothelial migration. Among the infiltrating cells, alloreactive T cells will be activated intensively by the graft's major histocompatibility complex class I and class II antigens, which have been shown to be expressed abundantly in organs from brain-dead donors (54, 55, 59). This activation may be additionally intensified by the presence of increased numbers of passenger leukocytes (55) and levels of cytokines (59). All these components have been described to contribute to increased immunogenicity of transplanted organs, which on its tum will intensify the process of acute rejection. This may well be the central factor in the mechanism of chronic rejection, as it has been shown convincingly in patients after lung transplantation that the number and severity of acute rejection episodes is the most important risk factor for the development of chronic rejection (79, 80). So far, the long-term effect of brain death was only investigated by Pratschke et al. ( 112) after kidney transplantation in rats. They showed an accelerated progression of chronic rejection, with a decreased survival of kidney allografts, decline in renal function, and progressive deterioration in renal morphology. Furthermore, they showed an increase in cytokine mRNA expression such as IL-1, tumor necrosis factora, and TGF-13 in allografts from brain-dead donors. In our study, we also find that brain death induced cytokine mRNA expression (IL-2). This IL-2 mRNA increase indicates that there is immune activation in lung allografts from brain-dead donors even long-term after transplantation. It has already been shown that IL-2 expression is associated with chronic rejection (94, 113, 114). Therefore, this supports the conclusion that brain death aggravates chronic rejection after transplantation. Consistent with the results of Pratschke et al., we conclude that brain death has a detrimental long-term effect after lung transplantation in rats.
It is striking that brain death in our study resulted in severe intimal hyperplasia without bronchiolitis obliterans of the transplanted lung. Intimal hyperplasia, as seen in this study, is a common phenomenon of chronic rejection in lungs and other organs after transplantation (42, 43, 115, 116). Also, some intimal hyperplasia was observed in our lungs from ventilated
40

- Donor brain death aggravates chronic rejection of lung grafts -
living donors and living donors. This is not unexpected, because this rat strain combination has been described as a combination prone to result in mild chronic rejection with intimal hyperplasia in blood vessels (104, 105). Besides intimal hyperplasia, bronchiolitis obliterans has been described in the airways of lungs transplanted in this rat strain combination. This is the other phenomenon commonly associated with chronic rejection of lung transplants (105, 106). However, in our study using the same rat strain combination, no fibrosis in the airways was observed in any of the groups. The reason that no airway fibrosis was observed in our study is not clear, but many factors can play a role, such as minimal differences in transplantation procedure and ischemia time.
In conclusion, brain death has a detrimental effect on the donor lung, affecting long-term transplant outcome after transplantation by aggravating chronic rejection. Our study may explain the clinical difference in long-term function between lungs from cadaveric donors and living donors ( 108, 109). Furthermore, it supports the idea that injury inflicted on an organ at the time of transplantation may have long-lasting effects on its outcome.
Acknowledgements
We thank M. Groen from the Department of Pathology and Laboratory Medicine for assistance with the histology stainings.
41

42

Chapter 4
Acceptance of the lung is not abrogated by a local Sendai virus infection after lung transplantation in rats
Noelle Zweers 1, Janneke de Vries 1
, Arjen H. Petersen 1, Lou F.M.H. de
Leij 1 , Jochum Prop 1 '2, Aalzen de Haan 1
1 Department of Pathology and Laboratory Medicine, Medical Biology section, 2Thorax center, University Medical Center Groningen, University of
Gron in gen, The Netherlands
Supported in part by a grant from the Netherlands Asthma Foundation

- Chapter 4
Abstract
Background. Infection with respiratory viruses may enhance rejection of lung grafts. In the present study, we investigated whether a local Sendai virus infection (Parainfluenza 1 virus) could abrogate the acceptance of rat allografted lungs that, despite inflammation peaking at day 28, are accepted due to a short-term cyclosporin-A treatment after transplantation.
Methods. Rats received a lung transplant and were given cyclosporin-A (CsA) on post-operative days 2 and 3. Four weeks after transplantation the rats were infected intratracheally with Sendai virus. Controls consisted of non-infected transplanted rats that were also immunosuppressed with CsA. The effects of Sendai infection on cellular infiltration and epithelial changes as well as infiltration of leukocytes, i.e. CD45+ cells, CD3+ T cells, CD4+ T cells, and CD8+ T cells and cytokines were investigated.
Results. Infiltration in allografted non-infected lungs peaked at four weeks after transplantation. Sendai infection increased peribronchiolar infiltration in transplanted lungs at 1 and 3 weeks after infection. However, no evident increase in graft rejection was seen: Sendai infection did not increase perivascular infiltrates and epithelial changes in lung grafts. Although, Sendai infection increased infiltration of CD3+ T cells in transplanted lungs, it did not enhance the infiltration CD45+ cells, CD4+ and CD8+ T cells and intragraft IFN-y, IL-2, IL-10, TGF-p, and IL-4 cytokine mRNA expression. In non-transplanted lungs, Sendai infection increased CD8+ T cell infiltration and IFN-y, and IL-10 mRNA expression.
Conclusions. The overall data support the view that acceptance of the lung, induced by a short-term CsA treatment, is not abrogated by a local Sendai virus infection after lung transplantation in rats.
Introduction
Engrafted lungs are exposed to airborne pathogens including a large variety of respiratory viruses ( 11, 12, 29). Local damage induced by these respiratory viruses, such as influenza virus, parainfluenza virus, human respiratory syncytial virus, and adenovirus have been suggested to trigger acute rejection of lung transplants (67, 68). Current clinical data also suggest a possible role for respiratory viruses in the development of chronic rejection manifested as bronchiolitis obliterans after lung transplantation (30, 73, 75). Additionally, in an experimental rat model, it was shown that
44

- Sendai virus does not abrogate the acceptance of the lung -
infection with Sendai virus (Parainfluenza 1 virus) aggravated epithelial damage in the presence of an ongoing process of chronic rejection (117, 118)
Besides direct effects of viral infection on the grafted tissue, infection with viruses may also influence immune responses leading to graft acceptance. Such immune responses are for example those that follow specific tolerance inducing treatments using antibodies that block T cell costimulation (119, 120). In rat transplantation where only a short-term cyclosporin-A (CsA) treatment is used, such immune responses emerge including the development of regulatory T cells (121, 122). In addition, the anti-inflammatory cytokines IL-10, TGF-P,.and IL-4 have been shown to play a role in graft acceptance (123-126).
Viral infection, such as lymphocytic choriomeningitis virus (LCMV) infection, however, has been shown to abrogate tolerance of mouse skin graft induced by anti-CD40L antibody plus donor-specific transfusion or, alternatively, induced by CTLA4-Ig plus anti-CD40L treatment (127, 128). A negative effect on graft-accepting immune responses has not yet been demonstrated for local virus infections such as viral infection of the airways of lung transplants. Previous data showed, however, that respiratory virus infection of airway epithelial cells triggers the production of proinflammatory cytokines, such as IL-I , TNF, IL-6, and IL-8 (69, 71, 74). This suggest that these infections may also negatively influence an accepting immune response of lung grafts. Such studies have not been performed in experimental lung transplantation yet.
Therefore, in the present study we investigated the role of a local Sendai virus infection on the acceptance of rat allografted lungs induced by a shortterm CsA treatment. We hypothesized that a local viral infection of the airways would induce inflammation and promote immune responses that are involved in graft rejection. To investigate this, the histopathological cellular infiltration and epithelial changes, as well as immunohistochemical infiltration of CD45+ cells, CD3+ T cells, CD4+ T cells, and CD8+ T cells, together with pro- and anti-inflammatory cytokines were assessed in noninfected and infected lung grafts.
45

- Chapter 4 -
Materials and Methods
Experimental design Left lungs from Brown Nmway (BN) rats were transplanted to MHC
incompatible Lewis (LEW) recipients. The recipients were immunosuppressed with CsA on post-operative days 2 and 3. In this model, lungs are accepted without continuous immunosuppression and despite the persistence of leukocyte infiltration in grafted lungs (129). First, the pathological changes in non-infected allografted lungs were investigated between 1 and 32 weeks after transplantation (groups of n=4). Next, effects of a local infection with Sendai virus at four weeks after transplantation was investigated. Antiviral antibody responses were measured in rat peripheral blood samples with ELISA. At 1, 3, and 8 weeks after infection, grafted left and control right lungs were analyzed for histopathological changes (groups of n=7). In addition, at 1 week after infection, the lungs were analyzed immunohistochemically for leukocyte common antigen (CD45), CD3+ T cells, CD4+ T cells, and CDR� T cells. Also, real-time reverse-transcriptase PCR was used to quantify mRNA expression of the pro-inflammatory cytokines such as IFN-y and IL-2 that are known to be involved in graft rejection, and anti-inflammatory cytokines such as IL-10, TGF-P,, and IL-4 that are known to be involved in graft acceptance.
Animals Specific pathogen-free inbred male BN (RTl n) and LEW (RTl 1) rats
weighing 200-300 g were obtained from Harlan (Horst, the Netherlands). Non-infected rats were housed individually in a specific pathogen-free rodent quarter of the Central Animal Laboratory of Groningen University. During infection, the rats were housed in an infection facility, in individual cages with filter tops specially designed to avoid contamination between the cages (Tecniplast Gazzada S. a r.l., Buguggiate (VA), Italy). All rats were fed standard rat chow and acidified water ad libitum. Animal experiments were perfonned after receiving approval of the institutional Animal Care Committee of Groningen University. All animals received human care in compliance with the Dutch Law on Experimental Animal Care.
Lung transplantation procedure Left lungs were transplanted orthotopically as described previously
(101). Briefly, the donor lung was dissected with immediate flushing of the
46

- Sendai virus does not abrogate the acceptance of the lung -
vascular bed with cold saline. The recipient's left lung was removed and replaced with the donor lung; the pulmonary vein and artery were anastomosed first, followed by the bronchus. To exclude technical failures, the function of transplanted lungs was monitored by chest radiographs at day 3 after transplantation and at the day before infection (i.e. four weeks after transplantation). All rats showed normal chest radiographs of the transplanted lung on day 3 after transplantation and on the day before infection.
Immunosuppression All rats received short-term cyclosporin-A (CsA, Novartis, Basel,
Switzerland) immunosuppression: CsA, dissolved in olive oil, was injected intramusculary on post-operative days 2 and 3 at a dosage of 25 mg/kg body weight.
Infection with Sendai virus Sendai virus (Parainfluenza type 1) was used to induce a respiratory
infection. Culture and preparation of the virus was performed by the I CLAS Reference centre for rodent viruses (Nijmegen, the Netherlands). Rats were intubated under halothane anesthesia and 0.2 ml of Sendai virus inoculum (5.6 x 103 tissue culture infectious dose of 50% [TCID5o] per ml DMEM medium) was intratracheally injected.
ELISA Antiviral antibody responses were measured in peripheral blood of rats.
Blood samples were taken before infection and at regular intervals after infection. Sendai-specific antibody titres (IgG) were measured by standard ELISA (by the ICLAS Reference centre for rodent viruses, Nijmegen, the Netherlands). Geometric mean titres were calculated by log transformation of the reciprocal of the highest dilution of the serum sample showing a positive reaction to Sendai virus antigens.
Histological analysis of the lungs Transplanted lungs and the non-transplanted right lungs were removed
and fixed in formalin. The lungs were embedded in paraffin and cut in 3-µm sections. Paraffin sections were stained with hematoxylin-eosin. Sections were analyzed according to the international classification of pulmonary allograft rejection from the lung rejection study group (32). In brief, the
47

- Chapter 4 -
lungs were examined for perivascular cellular infiltration, for peribronchiolar cellular infiltration, and for epithelial changes. Perivascular and peribronchiolar infiltration were graded from O to 4. Epithelial changes were graded from O to 2 with grade O indicating no changes, grade 1 mild epithelial changes (simple squamous epithelium and/or vacuoles in the epithelium) and grade 2 severe changes ( epithelial changes with dissociation of the epithelium from the basement membrane, epithelial ulceration, fibrinopurulent exudates, and epithelial necrosis).
Immunohistochemistry of the lungs For detection of leukocyte infiltration in the lungs, cryostat sections of
snap-frozen lung tissue were evaluated immunohistochemically. To this end, the lungs were taken out from the rats and snap-frozen in liquid nitrogen. A part of the snap-frozen lung tissue were cut in 5-µm sections, acetone fixed (for 10 min at room temperature), and air dried. Sections were incubated with 0.075 % hydrogen peroxide for 30 min to block endogenous peroxidase. Sections were rinsed in 0.01 M phosphate buffered saline (PBS) and incubated with the primary antibodies indicated below for 60 min. The primary antibodies used, were directed against leukocyte common antigen (CD45; OX-1), CD3+ T cells, CD4� T cells (OX-35), and CD8+ T cells (OX-8). After washing with PBS, sections were incubated for 30 min with a second-step peroxidase conjugated rabbit anti-mouse antibody (DAKO A/S, Glostrup, Denmark) in a 1 :40 dilution in PBS supplemented with 1 % normal rat serum. After washing with PBS, peroxidase activity was visualized using 3-amino-9-ethyl carbazole (Sigma, St. Louis, MO) for 10 min. Sections were counterstained with Mayer's hematoxyline (Merck, Darmstadt, Germany) and mounted in Kaiser's glycerol gelatin (Merck). As a control, sections were incubated with PBS instead of the primary antibodies. No staining was observed in these control sections.
Quantitation of immunohistochemical staining was assessed blindly by light microscopy. In the sections stained for CD45+ cells, CD3+ T cells, CD4+ T cells, and CD8+ T cells, quantitation of stained cells was performed using a semiquantitative scoring system with five grades: 0, no positive cells; 1, minimal with scattered positive cells; 2, mild with small clusters or one area with dense positive cells; 3, moderate with more than one area or a large area plus clusters of positive cells; 4, severe with whole tissue dense positive cells.
48

- Sendai virus does not abrogate the acceptance of the lung -
Real-time RT-PCR for cytokine mRNA expression Real-time reverse-transcriptase (RT) PCR was performed to quantify
cytokine mRNA expression in snap-frozen lung tissue of non-infected and Sendai-infected rats. As reference, cytokine mRNA expression was measured in cryopreserved samples from acutely rejected lung grafts isolated in a previous study. The lung tissue was cut in 10-µm sections. Total RNA was isolated from four sections of I O µm using the Strataprep Total RNA Microprep Kit (Stratagene, Amsterdam, The Netherlands) as described in the manufacturer's protocol. Total RNA was subsequently reverse-transcribed to cDNA using 6.6 µM oligo-dT primers (Invitrogen, Leek, The Netherlands) in combination with the Sensiscript kit (Qiagen, Leusden, The Netherlands). The mixture was incubated at 37°C for 60 min and then inactivated at 93°C for 5 min. The cDNA was stored at -20°C until further analysis.
Real-time RT-PCR was performed using IFN-y, IL-2, IL-10, TGF-P, and IL-4 Taqman Pre-Developed Assay Reagents (Applied Biosystems, Foster City, CA). Primers and F AM-MGB labeled probes were designed by the manufacturer. P-actin was used as an internal control for differences in starting mRNA concentrations. The sequences for the P-actin specific primers and FAM-TAMRA labeled probe were as follows: forward primer 5 '-ACCGTGAAAGATGACCCAGAT-3' ; reverse primer 5 '-TGGTACGACCAGAGGCAT ACAG-3 ' ; and probe 5 'AGACCTTCAACACCCCAGCCATGTACGT A-3 '. PCR reactions were performed in 384-well optical reaction plates and contained 2x Taqman Universal PCR Master Mix (Applied Biosystems), the 20x primer and FAM-labeled probe mixture for the cytokines or primers-probe mixture for P-actine (50 µM sense and antisense primers, and 5 µM FAM-labeled probe), RNase-free water, and I µl of sample cDNA in a total volume of 20 µl. PCR reactions were run on an ABI Prism 7900 Sequence Detection System (Applied Biosystems) with the following protocol : 50°C for 2 min, 95°C for 10 min, and then 40 cycles at 95°C for 15 sec and 60°C for I min. Each sample was run in triplicate.
Results of the real-time PCR data were represented as C1 value, the threshold cycle. The C1 value was defined as the PCR cycle number at which the fluorescent signal crossed the threshold line. Differences in the Ci for the cytokines and the C1 for P-actin, called L1Ci, were calculated to normalize for the differences in quality and amount of input cDNA. The L1C1 for each experimental sample was subtracted from the i1C1 of normal lung
49

- Chapter 4
tissue, i.e. the ��Ct value. The n-fold difference of the experimental
samples relative to nonnal lung tissue was expressed as 2Mci_
Statistical Analysis All results are expressed as mean ± standard error of the mean (SEM).
Statistical comparisons between groups were performed by the MannWhitney U-test. A value of P<0.05 was considered statistically significant.
Results
Histopathological changes in non-infected rats Lungs of non-infected, transplanted rats showed minimal perivascular
and peribronchiolar infiltrates at 1 week after transplantation. These infiltrates increased at 4 weeks after transplantation. From four weeks onwards the infiltrates gradually declined until minimal perivascular infiltration and no peribronchiolar infiltration were seen at 32 weeks after transplantation (Figs. lA and B). The peak of infiltration was seen at 4 weeks after transplantation. The central airways of the non-infected, transplanted rats showed mild epithelial changes in the first 6 weeks after transplantation. In the period after that the epithelial changes increased (Fig. l C).
The non-transplanted right lungs of non-infected rats showed normal pulmonary parenchyma without evidence of perivascular infiltration, peribronchiolar infiltration, or epithelial changes during the 32 weeks after transplantation (data not shown).
Antiviral antibody responses At 4 weeks after transplantation, during peak infiltration of leukocytes in
the grafted lungs, a local Sendai infection was induced by intratracheal injection of the virus. This infection uniformly resulted in high blood levels of Sendai virus specific IgG from 1 week post-infection on (Table 1 ) . Similar levels were observed in non-transplanted rats without immunosuppression or non-transplanted rats given a short treatment of CsA.
50

- Sendai virus does not abrogate the acceptance of the lung -
4 GI � 3 u Ill
� 2
ij: 1
2
A. Perivascular infiltrates
1 2 3 4 6 8 1 2 1 6 32 Weeks after transplantation
C. Epithelial changes
2 3 4 6 8 1 2 16 32 Weeks after transplantation
4
8 3 Ill C 0 2 .:: I!? � 1 .E
0
B. Peribronchiolar infiltrates
2 3 4 6 8 1 2 1 6 32 Weeks after transplantation
Figure 1. Histopathological changes in non-infected lung grafts: Al perivascular infiltrates; Bl peribronchial infiltrates; Cl Epithelial changes. Values are expressed as mean ± SEM Results show a peak of infiltration al 4 weeks after transplantation. Epithelial changes remain present from 6 weeks after transplantation.
Table 1. AntibodJ:_ rese_onses in e_erie_heral blood after Sendai infection Weeks after Allografted, Non-trans�lanted rats
infection CsA treated rats No immunos uppres sion CsA treated 0 0.0 ± 0.0 ° 0.0 ± 0.0 0.0 ± 0.0
2.4 ± 0.2 2.4 ± 0. 1 0.0 ± 0.0 2 3.3 ± 0. 1 3. 1 ± 0. 1 3. 1 ± 0.0 3 3.5 ± 0. 1 3.2 ± 0. 1 3.3 ± 0. 1 4 3.5 ± 0. 1 3.4 ± 0. 1 3.0 ± 0. 1 5 3.3 ± 0. 1 3.4 ± 0. 1 2.9 ± 0. 1 8 3.3 ± 0. 1 3.4 ± 0.2 3. 1 ± 0.0
a Geometric mean titre ± SEM
5 1

- Chapter 4
Histopathological changes in Sendai-infected rats Perivascular infiltration in the infected allografted lungs was not different
from that in lungs of allografted, non-infected rats (Fig. 2A).
A. Perivascular infiltrates
I : 1 .2 2
� 1 -j
0 3 8
Weeks after infection
C. Epithelial changes
2
0
3 8
Weeks after infection
! 4 1 � 3
i 2 == r.;:::: .E 1 -1
0
B. Peribronchiolar infiltrates
*
*
1 3 8 Weeks after infection
D Non-infected
• Sendai-infected
Fig11re 2. Histopathological changes in Sendai-infected lung grafts. Black bars represent scores in Sendai-infected transplanted lungs at 1, 3, and 8 weeks after infection. White bars represent scores in non-infected lungs at comparable time points after transplantation. Values are expressed as mean ± SEM Results show that Sendai infection increases
peribronchiolar infiltrates in transplanted lungs. Sendai infection did not increase perivascu/ar infiltrates and epithelial changes in transplanted lungs compared with non-infected lungs. P<0.05 compared with non-infected, transplanted rats.
Peribronchiolar infiltration however was significantly higher in Sendaiinfected lung grafts at 1 and 3 weeks after infection compared with the
52

- Sendai virus does not abrogate the acceptance of the lung -
infiltration in non-infected lung grafts (Fig. 2B). Sendai infection did not enhance epithelial changes in lung grafts (Fig. 2C).
The non-transplanted right lungs of Sendai-infected rats showed normal pulmonary parenchyma without evidence of perivascular infiltration, peribronchiolar infiltration or epithelial changes during 1, 3, and 8 weeks after infection (data not shown).
Immune cell infiltration in lungs Sendai infection increased the infiltration of C03+ T cells at 1 week after
infection in lung allografts (Fig. 3B). The C045+ cell, C04+ T cell, and cog+ T cell infiltration, already moderate in non-infected lung grafts, however did not increase further in infected lung grafts (Figs. 3A, C, and 0). This is in line with the infiltrations observed in the histopathological analysis (Fig. 2).
In the non-transplanted right lungs Sendai infection resulted in minimal to mild infiltration: the increase reached statistical significance only for cog+ T cells (Fig. 30). The infiltration of C045+ cells, C03+ T cells, C04+
T cells, and C08+ T cells was much lower in the non-transplanted right lungs than in the allografted lungs (Fig. 3).
Intragraft cytokine mRNA expression In addition to cellular infiltration, we analyzed the expression of relevant
cytokines in infected and non-infected lung grafts. One week after Sendai infection in lung allografts, the mRNA levels of the pro-inflammatory cytokines IFN-y and IL-2, being high and low respectively, were not different compared with levels in non-infected lung grafts (Figs. 4A and B). Similarly, rnRNA levels of the anti-inflammatory cytokines IL-10, TGFp, and IL-4 did not change in Sendai-infected lung grafts compared with non-infected lung grafts (Figs. 4C, D and E). In particular IL- IO rnRNA was highly expressed in infected as well as non-infected allografts (Fig. 4C). To compare these accepted lung allografts with acutely rejecting allografts, we analyzed rejected lung transplants from a previous study. The rnRNA levels of the pro-inflammatory cytokines IFN-y and IL-2 as well as the antiinflammatory cytokine IL- I O in rejecting lung grafts were much higher: the mRNA level expressed as n-fold increase of cytokine rnRNA for IFN-y was 330.4, for IL-2 was 34.3, and for IL-10 was 102.6. The rnRNA levels of the anti-inflammatory cytokines TGF-P (5.0) and IL-4 (4.0) in rejecting lung grafts were comparable with the levels found in the present study.
53

- Chapter 4 -
In non-transplanted lungs expression of cytokines mRNA was generally low, although Sendai infection did increase expression of IFN-y and IL- I 0 mRNA significantly (Figs. 4A and C).
4
3
! 8 2 en
1
0
4
A. CD45
- Sendai + Sendai
Transplanted left lung
C. CD4
- Sendai + Sendai
Transplanted left lung
Q _ I - Sendai + Sendai
Control right lung
D - Sendai + Sendai
Control right lung
4
3
2
1 1
0 ;
8. CD3
Cl _ I - Sendai + Sendai
Transplanted left lung
D. CDS
- Sendai + Sendai
Transplanted left lung
-6 • - Sendai + Sendai
Control right lung
#
-----, • - Sendai + Sendai
Control right lung
Figure 3. Immune cell infiltration in transplanted and non-transplanted lungs of rats infected or not with Sendai virus. Black bars represent scores in Sendai-infected transplanted lungs at 1 week after infection. White bars represent scores in non-infected lungs at comparable time point after transplantation. Values are expressed as mean ± SEM Sendai infection induces an increase of CD3+ T cells in transplanted lungs and CD8+ T cells in non-transplanted lungs. P<0.05 compared with non-infected, transplanted rats; # P<0. 05 compared with non-infected, non-transplanted rats.
54

- Sendai virus does not abrogate the acceptance of the lung -
A. IFN-y B. IL-2
200 20 - * m � 1 50 1 5 IV It: * e! E g ! 1 00 ·- ·- 1 0
"C � - 0
� i 50 5 z
0 0 RCMV- RCMV+ RCMV- RCMV+ RCMV- RCMV+ RCMV- RCMV+
CsA- CsA- CsA+ CsA+ CsA- CsA- CsA+ CsA+
C. IL-10 D. IL-4
20 20
0 c( 1 5 1 5 a, z Kl It:
e! E u a, 1 0 1 0 -= -= * "C �
l - 0 .E >, 5 � 5 z u
0 0 RCMV- RCMV+ RCMV- RCMV+ RCMV- RCMV+ RCMV- RCMV+ CsA- CsA- CsA+ CsA+ CsA- CsA- CsA+ CsA+
E. TGF-13
20
0 c( 1 5 a, z Ill It:
� E • Transplanted g ! 1 0 ·- ·- D Non-transplanted "C � - 0 .E >, 5 z u *
0 ......__, RCMV- RCMV+ RCMV- RCMV+
CsA- CsA- CsA+ CsA+
Figure 4. lntragraft cytokine mRNA expression in transplanted and non-transplanted lungs of rats infected or not with Sendai virus. Black bars represent cytokine mRNA expression in Sendai-infected transplanted lungs at I week after infection. White bars represent cytokine mRNA expression in non-infected lungs at comparable time point after transplantation. Values are expressed as mean ± SEM No increases in cytokine mRNA expression were seen after Sendai infection in transplanted lungs. However, Sendai infection induces an increase of IFN-yand IL-JO mRNA in non-transplanted lungs. P<0.05 compared with non-infected, non-transplanted rats.
55

- Chapter 4
Discussion
This study shows that a local infection with Sendai virus can change the immune responses in lung transplants. However, despite the slightly increased peribronchiolar infiltration and increased infiltration of C03+ T cells after Sendai infection, we did not find other, more evident symptoms of increased graft rejection, i.e. perivascular infiltration, epithelial changes, C04+ T cell and C08+ T cell infiltration, and expression of proinflammatory cytokines. Thus, a local viral infection with Sendai virus in a lung allograft does not consistently abrogate acceptance of the graft.
This study was not flawed by technical problems in the experiments. The lung transplantation in rats is a procedure that has been performed routinely in our institute for many years (101, 118, 129). Furthermore, the Sendai infection was clearly effective. It induced high systemic antibody responses against Sendai virus antigens in the infected rats. Sendai infection further increased infiltration and cytokine mRNA expression at 1 week after infection in non-transplanted rats. That does not preclude that a more severe infection might have caused more histopathological damage in the transplants. Furthermore, changing the interval between transplantation and viral infection would have little influence in the outcome: in parallel experiments in which rats were infected at 2, 8, and 24 weeks after transplantation, no evidence of increased graft rejection was found (data not shown).
The limited effect of the Sendai infection on rejection of the lung grafts can be explained by several mechanisms. First, infiltrating T cells in allografts can have regulatory properties rather than cytotoxic properties. Regulatory T cells, such as C04+ T cells expressing C025 for example, are important in the induction and maintenance of tolerance after transplantation, including lung transplantation (130, 131). Besides C04+ T cells, C08+ T cells may possess regulatory properties, as recently demonstrated in a rat kidney transplantation model that used oral exposure to alloantigen to induce tolerance ( 132). Importantly, a recent study showed that short-term low dose CsA treatment of rat recipients of heart transplants promoted the development of regulatory T cells (122). It is likely therefore that in our model, where also a short-term low dose CsA treatment is used, the development of regulatory T cells is supported. These cells may, if present in sufficient numbers, have counteracted the cytotoxic activity of alloreactive T cells that entered the graft as a result of the pro-inflammatory
56

- Sendai virus does not abrogate the acceptance of the lung -
response induced by the Sendai virus infection. Future experiments should demonstrate whether the T cells in our study have regulatory properties by performing additional typing of, for example, the CD4+ T cells for CD25.
Furthermore, the presence of regulatory cells is consistent with the cytokine mRNA expression found in the study, although the interpretation of cytokine expression is complicated. On the one hand, the expression of anti-inflammatory cytokines is generally associated with allograft acceptance (123-126). On the other hand, expression of pro-inflammatory cytokines such as IFN-y and IL-2 is seen in graft rejection (123, 133). In contrast with this concept is a recent study, showing an early accumulation of IFN-y in grafts from tolerized animals, suggesting that Thl cytokines may play a role in tolerance induction ( 134, 135). In our long-term accepted lung allografts, anti-inflammatory cytokines were expressed, but also proinflammatory cytokines. This expression of pro-inflammatory cytokines, however, is low compared with the expression in acutely rejected lung grafts. Furthermore, the cytokine expression was not influenced by the Sendai infection, indicating a stable situation of graft acceptance. This might explain why, despite increased peribronchiolar infiltration and increased infiltration of CD3- T cells in Sendai-infected lung grafts, the acceptance of the lung grafts is not abrogated and no rejection is induced by a Sendai infection.
Finally, it is also possible that the lung tissue is protected against an immune attack. Cells can upregulate a protein that specifically inhibits granzyme B activity, a cytotoxic T cell protein. Protease inhibitor 9 (PI-9), an intracellular serpin that inhibits granzyme B, is known to protect cells from the action of cytotoxic T lymphocytes. PI-9 is highly expressed in renal transplant recipients with subclinical rejection and the data suggest that a high expression of PI-9 can serve as one of the factors protecting allografts from rejection in spite of the presence of inflammatory cell infiltrates (136).
In conclusion, our results show that acceptance of rat lung grafts, induced by a short CsA treatment, is a process which can not be abrogated by a local Sendai virus infection.
57

58

Chapter 5
Cytomegalovirus infection in immunocompromised rats increases the number of immune effector cells and
alloreactivity after lung transplantation
Noelle Zweers 1, Nienke van der Werf 2
, Arjen H. Petersen 1, Flip A. Klatter2
,
Jan-Luuk Hillebrands2, Jan Rozing2
, Lou F.M.H. de Leij 1 , J. Prop 1•3
, Aalzen de Haan 1
1Department of Pathology and Laboratory Medicine, Medical Biology section, 2Department of Cell Biology, Immunology section, and 3Thorax
center, University Medical Center Groningen, University of Groningen, The Netherlands

- Chapter 5 -
Abstract
Background. It has been suggested that CMV infection enhances the development of chronic rejection after transplantation, including lung transplantation where CMV infection is associated with an increased development of bronchiolitis obliterans. In this study we tested the hypothesis that one mechanism by which CMV could enhance rejection of lung grafts is through generation of immune effector cells during CMV infection and immunosuppression. These effector cells may have the capacity to promiscuously recognize CMV-infected tissue cells, including CMV-infected allogeneic tissue cells, which can lead to an increased lung graft infiltration.
Methods. Rats received a lung transplant and were immunosuppressed with cyclosporin-A (CsA) and, subsequently, infected with rat cytomegalovirus (RCMV). Other experimental groups consisted of noninfected immunosuppressed transplanted rats, non-infected nonimmunosuppressed transplanted rats and infected non-immunosuppressed transplanted rats. Control groups consisted of (RCMV-infected and CsA immunosuppressed) non-transplanted rats. The effects of RCMV infection on leukocyte subsets in peripheral blood and inflammatory responses in the grafted lung with local expression of cytokines were analyzed, as well as the capacity of the immunocompromised and RCMV-exposed recipient's immune system to respond to (allogeneic) RCMV-infected tissue cells in vitro.
Results. This study shows that RCMV infection induced an increase of NKRP 1 + cells, i.e. NK cells and CD8�KRP 1 + T cells at day 14 after transplantation in peripheral blood of transplanted rats despite CsA treatment. A RCMV infection potentiated an immune response with the capacity to respond to allogeneic RCMV-infected, but not uninfected, tissue cells, such as fibroblasts. Finally, RCMV infection in immunosuppressed and transplanted rats induced an increase of CD8+ T cell infiltration in lung grafts but did not enhance intragraft IFN-y, IL-2, IL-10, IL-4, and TGF-P cytokine mRNA expression.
Conclusions. The overall data support the view that CMV infection modulates both the recipient's immune system as well as the immunogenicity of allogeneic (transplant) tissue cells, and that both activities are needed for an enhanced graft reactive response.
60

- CMV infection increases immune effector cells and alloreactivity -
Introduction
Several lines of evidence have supported the view that CMV infection aggravates acute and chronic rejection after solid organ transplantation (60, 137). For example, in experimental transplant models such as kidney, heart, and trachea transplantation in rats CMV infection was found to enhance chronic rejection (138-140). Clinical data also suggest that CMV infection enhances the development of chronic rejection after transplantation, including lung transplantation where CMV infection is associated with an increased development of bronchiolitis obliterans (61-64). However, data describing that CMV does not contribute to enhanced rejection after solid organ transplantation have also been published (65, 141, 142). The conflicting results on the role of CMV in transplantation may be due to the fact that the mechanism by which CMV enhances transplant rejection has remain obscure.
CMV infection has been shown to have effects on the recipient's immune system as well as on tissue cells which may both contribute to an enhanced graft-directed immune response. With respect to the immune system, it has been shown that CMV infection enhanced NK cell and CD8+
T cell numbers and, importantly also increased numbers of a cytotoxic CD8+
T cell subpopulation in transplanted rats and immunosuppressed renal transplant patients (effector type CD8+ T cells; CD8+CD45RA+CD2T in humans) (143-145). Whether these CMV-induced immune effector cells display an enhanced graft reactive response has not been investigated yet. With respect to the tissue itself, it has been shown that CMV-infected tissue cells have a higher capacity to activate immune effector cells. For example, CMV-infected human endothelial cells are capable of activating alloreactive T cells, partly due to induced increase of immediate early genes with concomittant increase of the adhesion molecules intercellular cell adhesion molecule (ICAM)-1 and leukocyte function-associated antigen (LF A)-3 (146, 14 7). Previous studies also indicated that lung grafts in particular are sites where CMV can reactivate and, most likely, re-infect graft tissue cells (148-150). It remains to be investigated if immune effector cells generated under CMV infection and immunosuppression have the capacity to interact with allogeneic tissue cells of lung grafts, and if infection with CMV renders allogeneic tissue cells more susceptible to recognition by the (CMVexposed) immune system.
6 1

- Chapter 5
In the present study we tested the hypothesis that CMV could enhance rejection of lung grafts through generation of immune effector cells during CMV infection and immunosuppression. These effector cells may have the capacity to promiscuously recognize CMV-infected tissue cells, including CMV-infected allogeneic tissue cells, which can lead to an increased lung graft infiltration. To test this hypothesis, rats received an allogeneic lung transplant and were immunosuppressed with cyclosporin-A (CsA). Subsequently, rats were infected with rat cytomegalovirus (RCMV). The effects of RCMV infection on leukocyte subsets in peripheral blood and inflammatory responses in the grafted lung with local expression of cytokines were analyzed, as well as the capacity of the immunocompromised and RCMV-exposed recipient's immune system to respond to (allogeneic) RCMV infected tissue cells in vitro.
Materials and Methods
Experimental design Left lungs from Brown Norway (BN) rats were transplanted to Lewis
(LEW) recipients. Rats were infected with rat cytomegalovirus (RCMV) on day 1 after transplantation and were treated with cyclosporin-A (RCMV+CsA+ group, n=3). Other experimental groups consisted of noninfected immunosuppressed transplanted rats (RCMV-CsA +, n=3), noninfected non-immunosuppressed transplanted rats (RCMV-CsA-, n=3) and infected non-immunosuppressed transplanted rats (RCMV+CsA-, n=3). Analysis of leukocyte subsets in peripheral blood by flow cytometry was performed at days 0, 7, 14, and 28 after transplantation. Rats were killed at day 28 after transplantation. Proliferative capacity of rat lymphocytes against (RCMV-infected) syngeneic and allogeneic fibroblasts was measured. Lungs were examined for leukocyte infiltration and cytokine mRNA expression. Four control groups consisted of (RCMV-infected and/or CsA immunosuppressed) non-transplanted LEW rats that were examined in the same way as the transplanted rats.
Animals Specific pathogen-free inbred male BN (RT 1 ") and LEW (RT 11) rats
weighing 250-350 g were obtained from Harlan (Horst, The Netherlands). The rats were fed standard rat chow and acidified water ad libitum. Animal experiments were performed after receiving approval of the institutional Animal Care Committee of the Groningen University. All animals received
62

- CMV infection increases immune effector cells and alloreactivity -
human care in compliance with the Dutch Law on Experimental Animal Care.
Lung transplantation procedure Left lungs were transplanted orthotopically as described previously
(101 ). Briefly, the donor lung was dissected with immediate flushing of the vascular bed with cold saline. The recipient's left lung was removed and replaced with the donor lung; the pulmonary vein and artery were anastomosed first, followed by the bronchus.
Infection with RCMV RCMV infection was performed by intraperitoneal (i.p.) injection of 2 x
106 plaque forming units (pfu) of RCMV (Maastricht strain). The RCMV stock was obtained by homogenization of salivary glands of acutely infected and irradiated rats as described previously (151 ). Control rats were mockinfected and were injected i.p. with normal salivary gland homogenate obtained from non-infected rats.
Immunosuppression Rats received cyclosporin-A (CsA, Novartis, Basel, Switzerland),
dissolved in olive oil, intramuscularly according to the following protocol: 10 mg/kg body weight CsA on post-operative day 2, 5 mg/kg body weight on post-operative day 4, and 2 mg/kg body weight twice a week from day 7 until day 28.
Analysis of peripheral blood leukocyte subsets To determine the effect of RCMV infection on the different subsets of
leukocytes in peripheral blood, 1 ml of blood was taken from the rats by orbital puncture at 0, 7, 14, and 28 days after transplantation. Part of the blood was used to count the total number of leukocytes per ml of blood using a Coulter Counter Z l (Coulter, Hialeah, FL). The remaining blood was centrifuged after a 1: 1 dilution with PBS (20 min, 2500 rpm, 4 °C). Buffy coats were taken and erythrocytes were lysed with NH4Cl. For fourcolour flow cytometric analysis 5 x 105 cells were resuspended in PBS containing 5% newborn calf serum and 0.1 % sodium azide (PBS/NCS/azide). Cells were incubated for 60 min with different cocktails of monoclonal antibodies. Monoclonal antibodies used in this study were FITC-labeled anti-CD45RC (OX22, Pharmingen, San Diego, CA), FITClabeled anti-CD8 (OX8), PE-labeled anti-CD4 (OX35), PE-labeled anti-
63

- Chapter 5
CD8 (OX8), PE-labeled anti-CD28 (JJ3 1 9), PE-labeled anti-NK cell (NKR
P l A), PerCP-labeled anti-TCR a� (R73), biotin-labeled anti-CD25 (IL2R a chain) and biotin-labelled anti-ART2 (DS4.23). After washing, streptavidinAPC (Pharmingen) was added to label biotin for 30 min. Cells were washed
twice and resuspended in 300 µl PBS/NCS/azide. The labeled cells were analyzed on a flow cytometer (F ACS Calibur, Becton Dickinson, San Jose, CA). Data were analyzed by gating on living cells and leukocytes using Winlist 5 .0 (Verity Software House, Topsham, ME) and absolute numbers of cells were calculated.
Proliferation Assay To determine the recipient (LEW) spleen cells capacity to respond to
(RCMV-infected) syngeneic (LEW) and allogeneic (BN) embryonic fibroblasts, ex vivo proliferative responses were measured at 28 days after transplantation. Allogeneic and syngeneic RCMV-infected rat embryonic fibroblasts (REF) and uninfected REF were used as stimulator cells and were prepared as described previously ( 1 52, 1 53). Responder cells were prepared by harvesting the spleens from the rats and forcing them through an iron grid. Next, erythrocytes were lysed with Na.CI and the splenocytes were resuspended in RPMI-1 640 medium (Gibco BRL, Life technologies B.V., Breda, The Netherlands) supplemented with 1 0% fetal calf serum at a final concentration of 2 x 1 06 cells/ml. Splenocytes (2 x 1 05 cells/well) were
incubated for four days at 37°C and 5% CO2 in 200 µl complete RPMI-1 640 medium in 96-well round bottom culture plates in the presence of RCMVinfected REF or uninfected REF at a responder:stimulator ratio of 10 : 1 or in the absence of REF (medium control). As a positive control, responder cells
were stimulated with Concanavalin-A (Con-A, 1 0 µg/ml). Proliferation was
detennined by adding 0.5 µCi of 3H-thymidine to each well for the final 1 8 hours of culture. Incorporation of 3H-thymidine was measured on a liquidscintillation counter (Canberra Packard, Meriden, CT), and results were given as desintegrations per second (dps).
Immunohistochemistry of lungs For detection of leukocyte infiltration in the lungs, cryostat sections of
snap-frozen lung tissue were evaluated immunohistochemically. To this end, the lungs were taken out from the rats and a part of the lung was snap
frozen in liquid nitrogen. The snap-frozen lung tissue was cut in 5-µm sections, acetone fixed (for 1 0 min at room temperature), and air dried.
64

- CMV infection increases immune effector cells and alloreactivity -
Sections were incubated with the primary antibodies indicated below for 60 min. The primary antibodies used, were directed against leukocyte common antigen (CD45, OX-1), CD4+ T cells (OX-35), and CD8+ T cells (OX-8). Sections were rinsed in 0.01 M phosphate-buffered saline (PBS) and were incubated with 0.075% hydrogen peroxide for 30 min to block endogenous peroxidase. After washing with PBS, sections were incubated for 30 min with a second-step peroxidase conjugated rabbit anti-mouse antibody (DAKO A/S, Glostrup, Denmark) in a 1 :40 dilution in PBS supplemented with 2% normal rat serum. After washing with PBS, peroxidase activity was visualized using 3-amino-9-ethyl carbazole (Sigma, St. Louis, MO) for 10 min. Sections were counterstained with Mayer's hematoxyline (Merck, Darmstadt, Germany) and mounted in Kaiser's glycerol gelatin (Merck). As a control, sections were incubated with an isotype control antibody (Hu5/3-2.1, mouse IgG 1, anti-human ICAM-1) instead of the primary antibodies. No staining was observed in these control sections.
Quantitation of immunohistochemical staining was assessed blindly by light microscopy. In the sections stained for CD45, CD4+ T cells, and CD8+
T cells, quantitation of stained cells was performed using a semiquantitative scoring system with five grades: 0, no positive cells; 1, scattered positive cells; 2, small clusters or one area with dense positive cells; 3, more than one area or a large area plus clusters of positive cells; 4, whole tissue dense positive cells.
Real-time reverse-transcriptase PCR for cytokine mRNA expression Real-time reverse-transcriptase (RT) PCR was performed to quantify
cytokine mRNA expression in snap-frozen lung tissue, cut in 10-µm sections. Total RNA was isolated from four sections of 10 µm using the Strataprep Total RNA Microprep Kit (Stratagene, Amsterdam, The Netherlands) as described in the manufacturer's protocol. Total RNA was subsequently reverse-transcribed to cDNA using 6.6 µM oligo-dT primers (Invitrogen, Leek, The Netherlands) in combination with the Sensiscript kit (Qiagen, Leusden, the Netherlands). The mixture was incubated at 37°C for 60 min and then inactivated at 93°C for 5 min. The cDNA was stored at -20°C until further analysis.
Real-time RT-PCR was performed using IFN-y, IL-2, IL-10, IL-4, and TGF-P Taqman Pre-Developed Assay Reagents (Applied Biosystems, Foster City, CA). Primers and FAM-MGB labeled probes were designed by the manufacturer. P-actin was used as an internal control for differences in
65

- Chapter 5 -
starting mRNA concentrations. The sequences for the 13-actin specific primers and FAM-TAMRA labeled probe were as follows: forward primer, 5'-ACCGTGAAAGATGACCCAGAT-3' ; reverse primer, 5'-TGGTACGACCAGAGGCATACAG-3' ; and probe, 5'-AGACCTTCAACACCCCAGCCATGTACGTA-3'. PCR reactions were performed in 384-well optical reaction plates and contained 2x Taqman Universal PCR Master Mix (Applied Biosystems), the 20x primer and FAM-labeled probe mixture for the cytokines or primers-probe mixture for !3-actin (50 µM sense and antisense primers, and 5 µM FAM-labeled probe), RNase-free water and 1 µl of sample cDNA in a total volume of 20 µI. PCR reactions were run on an ABI Prism 7900 Sequence Detection System (Applied Biosystems) with the following protocol: 50°C for 2 min, 95°C for 10 min, and then 40 cycles at 95°C for 15 sec and 60°C for 1 min. Each sample was run in triplicate.
Results of the real-time PCR data were represented as Ct value, the threshold cycle. The Ct value was defined as the PCR cycle number at which the fluorescent signal crossed the threshold line. Differences in the C1 for the cytokines and the Ci for 13-actin, called �C1, were calculated to normalize for the differences in quality and amount of input cDNA. The �Ct for each experimental sample was subtracted from the �Ct of normal lung tissue, i.e. the ��C1 value. The n-fold difference of the experimental samples relative to normal lung tissue was expressed as 2Mct_
Statistical Analysis All results are expressed as mean ± standard error of the mean (SEM).
Statistical comparisons between groups were performed by the MannWhitney U-test. A value of P<0.05 was considered statistically significant.
Results
Effects of RCMV infection on numbers of immune effector cells RCMV infection of non-transplanted and non-immunosuppressed rats did
not enhance absolute numbers of circulating NK cells (NKRP 1 + cells), CD8+ T cells, effector CD8 subpopulations (CD8+CD45RC+ ART2- and CD8�KRPI +), or CD4+ T cells (Fig. 1 ). In transplanted, but non-infected, rats that did not receive immunosuppression, all studied cell populations increased in number after transplantation (Fig. 1 ). A RCMV infection after transplantation however did not further increase their numbers, but at some
66

- CMV infection increases immune effector cells and alloreactivity
A. NKRP1+
I!! 9000 .8 "b E � ::, ><6000 C -., .!!? !; 83000
) o � 0
a. coa• .. 3000
! "b § � 2000
0 10 20 30
� i1000 � i5 -.. 0 � 0
0 10 20 30
c. coa•co4sRc•ARr2·
0 10 20 30
D. coa·NKRP1 +
j "b
600
§ ";c 400
; -;;;- � � � 200
� o I " 0 ' ' ' 0 10 20 30
E. co4•
9000
=� o +-�-��
3000
0 10 20 30
0 10 20 30
0 10 20 30
9000
6000
3000
::i-O--o-------0
3000
0 10 20 30
0 10 20 30
0 10 20 30
9000
6000
3000 �
3000
0 10 20 30
0 10 20 30
400
300 1
0 10 20 30
: 11 � : • : k 200
W � 200 � 200
�
0 +------,--
0 10 20 30 0
0 10 20 30 o .-1 ���
0 10 20 30
1 1=�* =r: =� =� � B 2000 2000 2000 -� 2000 � .. 0 � o - o o -�--� o ---
0 10 20 30
non-Tx
0 10 20 30 0 10 20 30
Time after transplantation (days) Tx non-Tx
0 10 20 30
Tx -CsA +CsA
Figure 1. Flow cytomehy analysis of NK cells (A), CD8+ T cells (B), CD8+ CD45RC+ ARTT effector T cells (C), CDB+NKRPJ+ T cells (D) and CD4+ T cells (E) in peripheral blood of (transplanted and CsA immunosuppressed) RCMV-infected (closed circles) and noninfected (open squares) rats. Values are the mean ± SEM number of cells (x UY) per ml blood. RCMV infection induced an increase in the absolute numbers of NK cells and CDB�NKRPJ+ T cells in transplanted and immunosuppressed rats at 14 days after transplantation compared with non-infected rats. P<0.05 compared with non-infected rats.
67

- Chapter 5
time points rather resulted in decreased cell numbers in the peripheral blood: significantly lower numbers were observed for CD8+ T cells at day 7 (Fig. 1B) and CD8+CD45RC+ARTT T cells at day 14 (Fig. I C). In contrast, in transplanted rats that received immunosuppression, numbers of immune effector cells such as NKRPl+ NK cells and CD8 �KRP1 + T cells increased at day 14 as a result of the RCMV infection (Figs. IA and 1D). Thus, increased numbers of immune effector cells in transplanted rats are induced by RCMV infection, but only under CsA-mediated immunosuppression.
Proliferative capacity of rat lymphocytes against (RCMV-infected) syngeneic and allogeneic fibroblasts
To analyse whether RCMV infection induced a higher anti-graft response, we tested the alloreactivity of spleen derived lymphocytes from (RCMV-infected and CsA immunosuppressed) control and transplanted rats against fibroblasts (i.e. non-professional APCs), which have a low intrinsic capacity to activate T cells, but which may become immunostimulatory upon infection with RCMV. Figs. 2A, B, C, and D show that lymphocytes from non-infected rats (treated or not with CsA) did not respond to syngeneic or allogeneic fibroblasts and also not when the fibroblasts were infected with RCMV. These responder cells however were capable to proliferate strongly upon Con-A stimulation ( data not shown). In contrast, lymphocytes from RCMV-infected animals (transplanted and nontransplanted) without CsA immunosuppression proliferated upon stimulation with allogeneic andsyngeneic RCMV-infected fibroblasts (Figs. 2A and 2B). Lymphocytes from non-transplanted rats that were RCMVinfected but also CsA immunosuppressed showed even higher proliferative responses against allogeneic and syngeneic RCMV-infected fibroblasts (Fig. 2C). Such a response was diminished in transplanted rats (Fig. 2D). Thus, RCMV infection potentiates an alloreactive response which acts both at the level of the recipient's immune system and at the level of the allogeneic (RCMV-infected) tissue cell.
68

- CMV infection increases immune effector cells and alloreactivity -
1000
! J 8oo
:§ 6 600 E ·->. 1a � � 400 ::c ... M 8 200 ·=
iii QI Q, C: :E.
'6 C: ·- 0 E ; .t !! '*;' &. ::c ... M 0 -�
1 000
800
600
400
200
A. -CsA, non-Tx
* *
Allo Allo Syn Syn Medium -RCMV+RCMV -RCMV+RCMV
C. +CsA, non-Tx
* *
* * * 0 ���.IL.
Allo Allo Syn Syn Medium -RCMV +RCMV-RCMV +RCMV
1000
800
600
400
200
1000
800
600
400
200
0
B. -CsA, Tx
*
*
Allo Allo Syn Syn Medium -RCMV +RCMV-RCMV +RCMV
D. +CsA, Tx
* *
Allo Allo Syn Syn Medium -RCMV +RCM -RCMV +RCM
Figure 2. In vitro proliferative responses of lymphocytes from RCMV-infected (black bars) and non-infected (white bars) rats that were non-transplanted and non-immunosuppressed (A), transplanted and non-immunosuppressed (B), non-transplanted and immunosuppressed (C), or transplanted and immunosuppressed (D) against (RCMV-infected) allogeneic (allo -RCMV and allo+RCMV) and (RCMV-infected) syngeneic (syn-RCMV and syn+RCMV) fibroblasts. Values are expressed as mean ± SEM RCMV infection in non-transplanted CsA immunosuppressed rats induced proliferative responses of spleen cells against allogeneic and syngeneic RCMV-infected fibroblasts. Such a response was diminished in transplanted rats. P<O. 05 compared with non-infected rats.
Immune cell infiltration in lungs Analysis of the cellular infiltration by immunohistochemistry showed
that CD45+ cells, CD4+ T cells, and CDS+ T cells were increased in lungs of transplanted and CsA immunosuppressed rats and transplanted rats that were RCMV-infected and CsA immunosuppressed at 28 days after transplantation compared with non-transplanted rats (Table 1 ). RCMV infection resulted m a higher infiltration of CDS+ T cells in
69

- Chapter 5
immunosuppressed and transplanted lungs compared with CD8 T cell infiltration of lungs from rats without RCMV infection. Thus, RCMV infection enhances CD8+ T cell infiltration in transplanted lungs of immunosuppressed rats.
Lungs from non-immunosuppressed and transplanted rats were not analyzed for immune cell infiltration, because these lungs were completely rejected at 28 days after transplantation and the tissue was not usable for analysis.
Table 1. Immune cell infiltration in transplanted and non-transplanted lungs of immunosuppressed rats infected or not with RCMV
Group CD45 CD4 CDS Median (range)
RCMV+csA+ Tx 3 (3-4) *
non-Tx 1 ( 1 - 1 )
RCMV-CsA+ Tx 3.0 (3-4) *
non-Tx 1 .0 ( 1 - 1 )
Median (range)
3 (3-4) *
0 (0-0)
3 (2-4) *
0 (0-0)
Median (range)
3 (3-4) * #
0 (0-0)
1 ( 1 -2) *
0 (0-0)
Median values (and range) are shown. See Materials and Methods for details of grading. •P<0.05 compared with non-transplanted rats; #P<0.05 compared with non-infected, transplanted rats.
Intragraft cytok.ine mRNA expression In addition to cell infiltration, cytokine expression was analyzed in lung
grafts. In transplanted lungs of untreated rats there is a significant higher expression of IFN-y, IL-2, IL-10, IL-4, and TGF-� mRNA compared withlungs of non-transplanted rats (Fig. 3; RCMV-CsA- black bars vs white bars). RCMV infection did not increase IFN-y, IL-2, IL-10, IL-4, and TGF-� mRNA expression in lung grafts from non-immunosuppressed and transplanted rats (Fig. 3; black bars; RCMV-CsA- vs RCMV+CsA-). CsA treatment did not inhibit IFN-y, IL-2, IL-10, IL-4, and TGF-� mRNA expression in lung grafts from non-infected rats (Fig. 3; black bars; RCMVCsA- vs RCMV-CsA+). Finally, RCMV infection did not further increase IFN-y, IL-2, IL-10, IL-4, and TGF-� mRNA expression in lung grafts from immunosuppressed and transplanted rats (Fig. 3; black bars; RCMV-CsA+ vs RCMV+CsA+). Thus, RCMV infection has no effect on cytokine mRNA expression in lung grafts.
70

200
0 3! � 1 50 Ill
a:: f E g ! 1 00 ·- -
"Cl .lll: - 0
J? i 50 z
0
20
0<( 1 5 CII z Ill a::
� E U C11 C: C: ·- ·- 1 0
"Cl .lll: - 0 .2 >, 5 z u
0
20
0 <( 1 5 CII z Ill a:: � E U C11 C: C: 1 0 ; :i: - 0
J? i 5 z
0
- CMV infection increases immune effector cells and alloreactivity -
A. IFN-y 20
* 1 5
1 0
5
0 RCMV- RCMV+ RCMV- RCMV+ CsA- CsA- CsA+ CsA+
C. IL-10
20
1 5
* 10
5
RCMV- RCMV+ RCMV- RCMV+ 0
CsA- CsA- CsA+ CsA+ E. TGF-13
*
RCMV- RCMV+ RCMV- RCMV+ CsA- CsA- CsA+ CsA+
B. IL-2
RCMV-CsA-
D. IL-4
RCMV-CsA-
RCMV+ RCMV-CsA- CsA+
RCMV+ RCMV-CsA- CsA+
• Transplanted D Non-transplanted
*
RCMV+ CsA+
RCMV+ CsA+
Figure 3. Intragraft cytokine mRNA expression in lungs from transplanted (black bars) and non-transplanted (white bars) rats that were untreated (RCMV-CsA-), only RCMV-infected (RCMV+CsA-), only CsA immunosuppressed (RCMV-CsA +), or RCMV-infected and CsA immunosuppressed (RCMV+CsA+). Values are expressed as mean ± SEM In transplanted lungs there is a significant higher expression of IFN-y, IL-2, IL-IO, IL-4, and TGF-/3 mRNA compared with lungs of non-transplanted rats. RCMV infection has no effect on cytokine expression in lung grafts. P<O. 05 compared with non-transplanted rats.
71

- Chapter 5
Discussion
This study shows that RCMV infection induced an increase of NK cells and CD8"NKRP 1 + T cells in peripheral blood of transplanted and immunosuppressed rats. A RCMV infection potentiated an immune response with the capacity to respond to allogeneic RCMV-infected, but not non-infected, tissue cells, i.e. fibroblasts. Also, RCMV infection of immunosuppressed and transplanted animals induced an increase of CDS+ T cell infiltration in lung grafts but did not enhance intragraft IFN-y, IL-2, IL-10, IL-4, and TGF-� cytokine mRNA expression. The data show that RCMV infection modulates both the recipient's immune system as well as the immunogenicity of allogeneic (transplant) tissue cells, and suggest that these activities may act in concert to enhance the graft reactive response.
Previous studies have described the importance of NK cells as early mediators of host defense against viral infections, including CMV ( 154-157). In our study, absolute numbers of peripheral blood NK cells were not increased in RCMV-infected non-transplanted rats but only in transplanted and RCMV-infected rats. Apparently, transplantation of allogeneic tissue is needed to induce NK cell accumulation, a process which is efficiently suppressed by CsA-mediated immunosuppression in non-infected animals but less efficiently in RCMV-infected animals. In this respect, it can be argued that a CMV infection augments NK cell proliferation by induction of type I interferons and, consequently, induction of IL-15 which is known to be a potent inducer of NK proliferation (157-162). This could occur independent of the CsA-mediated suppression of IL-2-induced NK cell proliferation, since CsA does not inhibit IL-15 production. Whether the induced NK cells specifically target to the graft remains unclear. Petersson et al. (163) described that immunization of rats with allogeneic cells induces NK cells with a specificity for the haplotype of the cells used for immunization. These NK cells were activated upon interaction with nonclassical MHC molecules, e.g. (allogeneic) MHC class lb RTl -E (164). These data suggests that an adaptive NK response can occur after transplantation. This response may be augmented by CMV infection, a process which is partly not sensitive to calcineurin-inhibitor mediated immunosuppression. Future experiments should demonstrate whether the increase in CDS+ T cell infiltration in lung grafts due to RCMV infection, as found in our study, is parallelled by an infiltration with NK cells.
72

- CMV infection increases immune effector cells and alloreactivity -
In addition to NK cells, peripheral blood CD8+ T cells did also increase in number upon RCMV infection (CD8�KRP1+ T cells in RCMV+CSA+ group vs RCMV-CsA+ group at day 14 after transplantation). Also, an increase in CD8+ T cells was found in the lung grafts. However, no increase of effector type CD8+ T cells, with the phenotype CD8+CD45RC+ ARTT in rats (165, 166), was seen in our study. Interestingly, increases in CD8+
effector type T cells (CD45RA+CD2T in humans) are seen in renal transplant patients infected with CMV (1 45). The fact that CD8�KRP1 + T cells in CMV-infected and transplanted rats did only show increases shortly after transplantation can be explained by a higher infiltration of CD8+ T cells in transplanted lungs of these animals (Table 1 ). It is possible that CD8+ T cells acquired different migratory capacities which adds to their increased graft-infiltrating capacity.
This study showed high proliferative responses of spleen derived lymphocytes from RCMV-infected rats against syngeneic fibroblasts, but also against fully mismatched allogeneic fibroblasts, suggesting a 'promiscuous' recognition of RCMV infected tissue cells. These high proliferative responses show that non-professional APC's, i.e. fibroblasts, gain the capacity to activate T cells after RCMV infection. Previous studies have shown possible mechanisms by which CMV-infected fibroblasts can become more immunogenic. First, it has been shown that the adhesion molecules ICAM-1 and LFA-3 are increased on human CMV-infected fibroblasts (146). Secondly, MHC class I related chains (MIC) molecules, distant homologs of MHC class I, can be increased on fibroblasts and endothelial cells upon CMV infection. Engagement of NKG2D, an activating receptor present on NK and CD8 T cells, with MIC induces CD8+ T cell responses (167). At present, no rat MIC molecules are known, but recently a homologue of human NKG2D has been found in the rat, namely NKR-P2 (168). It is also possible that RTl -E, a non-classical MHC class I molecule, is increased on CMV-infected cells which subsequently can activate NK cells and T cells, as discussed above. Surprisingly, proliferative responses of lymphocytes against allogeneic RCMV-infected fibroblasts were only seen in immunosuppressed control rats and not in transplanted rats. This may, however, be due to the fact that the CMVinduced cells have disappeared from the circulation and infiltrated in the inflamed transplanted lung. In our study, this scenario is likely since the transplanted lungs are highly infiltrated with T cells compared to nontransplanted control lungs.
73

- Chapter 5 -
Our results suggest that in the rat an interplay between the recipient's immune system (accumulation of NK cells and CD8�1 + T cells) and CMV-induced effects on the levels of the allogeneic (transplant) tissue cells with increased immunogenicity, may result in an enhanced transplant reactive immune response.
74

Chapter 6
Human cytomegalovirus enhanced alloreactivity in lung graft recipients with chronic rejection is mediated through
recipient CD8+CD45RA +CD2T effector T cell proliferation with NKG2D expression and donor endothelial-cell ICAM-1
and MICA expression
Aalzen de Haan 1 , Noelle Zweers 1 , Monica M. G. Dondorff 1 , Jochum Prop 1
, Erik A.M. Verschuuren2, Wim van der Bij2, Alexander Steinle3
, Lou F.M.H de Leij 1
, and Cees G.M. Kallenberg2
1 Department of Pathology and Laboratory Medicine, Medical Biology section, 2Department of Internal Medicine, University Medical Center Groningen, University of Groningen, The Netherlands, 3Department of
Immunology, Eberhard-Karls University, Tubingen, Germany

- Chapter 6
Abstract
Background. Infection with the human cytomegalovirus (HCMV) has been suggested to increase the risk for acute and chronic rejection after lung transplantation. The mechanisms by which HCMV enhances graft-directed responses remain unclear. Here we hypothesize that HCMV has dual effects, both on the recipient's immune system as well as on transplant tissue cells: HCMV induces recipient effector type CDS+ T cells that, via expression of NKG2D, broadly recognise HCMV-infected and MICAexpressing donor target cells. These effects, acting in concert, enhance graft reactive responses.
Methods. Peripheral blood samples from HCMV-carrying and nonHCMV carrying lung transplant recipients were analyzed for CDS+ T cell expression of CD45RA and CD27, identifying narve, memory, and effector type T cells. CD2T and CD27+ CDS+ T cells were investigated for ex vivo intracellular IFN-y production upon anti-CD3 stimulation. Expression of NKG2D on recipient CD2T and CD27+ CDS T cells, and its induction by IL-2 or IL-15, was measured as well. Also, the capacity of HCMV-infected HUVEC expressing ICAM-1 and MICA, to stimulate the proliferation of T cells was analyzed in HUVEC-T cell co-cultures using CFSE dye dilution analysis. Responding cells were analyzed for CD27 and NKG2D expression.
Results. Increasing percentages of effector type CDS+CD45RA +CD2T T cells were observed after transplantation in HCMV-carrying recipients, but not in non-HCMV carrying recipients. Early accumulation was associated with the development of chronic rejection. Recipient CDS+CD2T T cells had a high capacity to produce IFN-y. Expression of NKG2D was not higher on recipient CD8+CD2T T cells compared to CD27+ CDS+ T cells or healthy control CD2T or CD27+ CD8+ T cells, but could be upregulated by ex vivo exposure to IL-2 and IL-15. HCMV infection of HUVEC in vitro increased their ICAM-1 expression and, slightly, their MICA expression. HCMV-infected allogeneic HUVEC induced proliferation of effector type CD8+ T cells, evidenced by loss of CD27 expression and gain of NKG2D expression. This process was supported by IL-2, ICAM-1-LFAl , and NKG2D-MICA interactions.
Conclusion. HCMV may enhance graft-directed responses by supporting the proliferation of effector type CD8+CD2T T cells that express NKG2D
76

- Human CMV increases alloreactivity by effector T cell proliferation -
together with the induction of expression of ICAM-1 and the NKG2D ligand MICA on graft tissue cells.
Introduction
Chronic rejection is the most significant long-term cause of morbidity and mortality after solid organ transplantation. In lung transplantation this complication manifests itself as bronchiolitis obliterans, i.e. the scarring and occlusion of bronchioles. In the clinical situation chronic rejection manifests itself as the bronchiolitis obliterans syndrome (BOS), with a declining lung function evidenced by decreased forced expiratory volume in 1 second. Acute rejection episodes and a positive human cytomegalovirus (HCMV) serological status of the donor or recipient have both been identified as risk factors for the development of BOS ( 61, 169-17 1 ). In this respect, it has been suggested that effects of HCMV infection on the development of chronic rejection results from enhancement of alloimmunity, for example during alloreactive T cell responses in acute rejection (137, 172, 173). The precise mechanism by which CMV enhances alloimmunity however has remained unclear.
Recent findings indicate that human CMV infection enhances distinct processes in the host's immune system. These processes include for example the generation of effector type CD8+CD45RA +CD2T T cells in immunocompromised transplant rec1p1ents, at dispense of naYve CD8+CD45RA +CD27+ T cells, memory CD8+CD45RA-CD27+, or memoryeffector CD8+CD45RA-CD2T T cells (145, 174). On the level of tissue cells, CMV infection may upregulate adhesion molecules such as ICAM-1 which enhances stimulation of alloreactive T cells ( 146, 147). Recently, it was found that tissue cells, such as fibroblasts and endothelial cells, also express non-classical MHC I related chains (MICA) after HCMV infection ( 167). This molecule lowers the treshold for activation of HCMV-specific CD8+ T cells through engagement of the NKG2D 'killer activating' receptor expressed (167, 175). It is possible that, in a similar way as for the recognition of syngeneic HCMV-infected cells, the expression of MICA on CMV-infected allogeneic graft cells lowers the threshold for activation of potentially alloreactive CD8+ T cells resulting in a higher proportion of alloreactive CD8- T cells. Thus, HCMV infection or reactivation may predispose to enhanced alloimmunity and (chronic) rejection of lung grafts through the generation of T cells with enhanced effector function and a
77

- Chapter 6 -
broader recognition of graft cells by potentially alloantigen crossreactive T cells. At present it is unknown if, and to what extent, functional effector type CD8+CD45RA +CD2T T cells expressing the NKG2D receptor emerge in HCMV-carrying lung transplant recipients. Furthermore, it is unknown if NKG2D-MICA interactions are involved in the stimulation of alloreactive CD8+ T cells by HCMV-infected cells.
In this study, we investigated peripheral blood CD8+ T cell phenotypes, with respect to CD45RA and CD27 expression, that emerge in HCMVcarrying lung transplant recipients (HCMV-seropositive recipient or donor) and lung transplant recipients that do not carry HCMV (HCMVseronegative recipient and donor). Both phenotypes were related to BOS development after transplantation. Patient CD27+ and CD2T CD8+ T cells were further analyzed for function by analysing ex vivo the capacity to produce IFN-y and in vivo and ex vivo cytokine-induced NKG2D expression. The effect of in vitro CMV infection of human umbilical cord vascular endothelial cells (HUVEC) on the expression of intercellular cell adhesion molecule (ICAM)-1 and MICA was analyzed as well as the proliferation of CD8+ T cells cocultured with (CMV-infected) allogeneic HUVEC and the role of ICAM- 1 and MICA herein. Finally, proliferating CD8+ T cells were analyzed for CD27 and NKG2D expression.
Materials and Methods
Patients Patients included in the study received a lung transplant between Januari
1997 and May 2001. Ten patients were included that developed chronic transplant dysfunction, i.e. brochiolitis obliterans syndrome (BOS), due to chronic rejection within the first year after transplantation. Ten patients that remained good graft function in the first year after transplantation were also included. Selection of the patients was mainly based on availibity of samples of cryopreserved peripheral blood mononuclear cells (PBMNC). Controls were HCMV-seropositive healthy laboratory personnel. Patient characteristics are indicated in Table 1. Seven patients were non-HCMVcarrying recipients (HCMV -/- for recipient/donor, respectively; Table 1 ). Other matches included HCMV-/+ (n=3; Table 1), HCMV+/- (n=4; Table 1) and HCMV+/+ (n=6; Table 1). These patients are referred to as HCMVcarrying recipients. Patients did not receive HCMV-prophylaxis with
78

- Human CMV increases alloreactivity by effector T cell proliferation
ganciclovir in the early period after transplantation. Intravenous ganciclovir (Cymevene, Roche) was given in some patients when recurrent HCMV viral
Table J. Patient characteristics Patient BOS" Acute rejection° HCMVC HCMV viral Ganciclovir
numb. of treatm. match loadd : numb. of treatments /ATG or OKT3 (rec./don.) numb. ofpos. (additional
load detection treatment) (peak load)
1 no 5 1 1 (OKT3) - / - - -2 no 1 - / - - -3 no 0 + / + 2 (16) -4 no 1 + / + I (2) -5 no 2 - / - - -6 no 1 + / - 2 (335) -7 no 1 + / - 8 (8) 1 8 no 2 - / - - -9 no 0 - / - - -1 0 no 4 + / - 1 (3) -1 1 yes I O I 1 (ATG) + / + 3 1 (28) -1 2 yes 4 - / - - -1 3 yes 5 + / - 1 5 (32) I 1 4 yes 2 + / - 1 1 (35) 2 1 5 yes 5 I 1 (OKT3) - / + 27 (300) 1 1 6 yes 3 - / - - -1 7 yes 3 1 1 (ATG) + / - 1 5 (28) 2 1 8 yes 8 - / + 9 (36) 3 1 9 ves 7 / 1 (ATG) + / + 4 1 (96) 1 20 yes 6 - I + 1 8 (89) 1
(hyper immune globulin)
° Chronic transplant dysfunction (BOS) by chronic rejection in the first year after transplantation according to criteria defined by the ISHLT (16) b Number of acute rejection treatments in the first year after transplantation. Treatments consisted of steroid pulses and/or A TG or OKT3. BOS patients had more frequent acute rejection compared to good graft function patients (8 vs 1 patients with :'S 2.5 rejection episodes, for patients with good graft function and BOS patients, respectively, and 2 vs 9 patients with 2'. 2.5 rejection episodes for patients with good graft function and BOS patients, respectively; p=0.007, Chi-square testing with Yates ' correction). c Match based on HCMV-serology d HCMV viral load in the first year after transplantation measured by HCMV-pp65 antigenemia assay (14). Numbers indicate number of positive tests and peak load (positive cells/ 50.000 peripheral blood leucocytes). HCMV-canying BOS patients had more positive HCMV-pp65 antigenemia tests compared to HCMV-canying patients with good graft function (5 vs 1 patients with :'S 10 pos. HCMV antigenemia tests for patients with good graft function and BOS patients, respectively, and O vs 7 patients with 2'. 10 pos. HCMV antigenemia tests for patients with good graft fimction and BOS patients, respectively; p=0.012, Chi-square testing with Yates ' correction).
79

- Chapter 6 -
load was found with positive HCMV pp65-antigenemia (176). Immunosuppressive therapy and criteria for the diagnosis of acute rejection and BOS have been described previously (38, 177).
Peripheral Blood Mononuclear Cells and T cell isolation PBMNC from pre-transplant and post-transplant blood samples (3, 6, 12,
and 24 months after transplantation) were isolated using Lymphoprep (Nycomed, Oslo, Norway) and cryopreserved in liquid nitrogen until further analysis. Control samples were obtained from healthy laboratory personnel and processed as indicated above. T cells used for ex vivo T cell stimulation with (HCMV-infected) HUVEC (see below) were isolated from PBMNC samples of HCMV-seropositive healthy donors using Lymfokwik-T (One Lambda, LA, USA) and labeled with 5-(and-6)-carboxyfluorescein diacetate succinimidyl ester (CFSE; Molecular Probes Europe BV, Leiden, The Netherlands). Briefly, 0.5 nmol CFSE was added to 10xl06 T cells/ml and incubated for 10 min at 37°C in a shaking waterbath. Next, excess of CFSE was quenced by adding an equal volume of FCS. Finally, cells were washed twice with RPMI.
Flow cytometric analysis Cryopreserved PBMNC were thawed and surface marker-specific
monoclonal antibodies were applied. These antibodies included anti-CD8-APC, anti-CD45RA-CyQ and anti-CD27-PE (BD Biosciences). After incubation at 4 °C for 30 min, the cells were washed twice with 3 ml of icecold PBS/1 % BSA, resuspended in 400 µl of PBS/ I% BSA and all remaining cells were analyzed on a FacsCalibur (Becton Dickinson) using a life gate on the CD8+ T cells. For analysis of NKG2D expression cells were first incubated with a primary monoclonal antibody specific for NKG2D (clone 149810; R&D Systems Inc.). After a 30 min incubation at 4°C, cells were washed and FITC-labeled goat anti-mouse IgG 1 (Southern Biotechnology Associates) was added. Next, cells were incubated for 30 min at 4°C. After washing 2% normal mouse serum was added, and 10 min later, surface marker-specific monoclonal antibodies were applied and samples were processed as indicated above. Some samples were analyzed for numbers of HCMV-specific T cells using HLA-tetramers. In these cases tetramer staining (HLA-A2 tetramer carrying the pp65 derived peptide
80

- Human CMV increases alloreactivity by effector T cell proliferation -
NLVPMVATV; a gift from Dr I. Ten Berge, Amsterdam) was done as previously described (178).
Ex vivo stimulation assays for intracellular IFN-y production and NKG2D expression
For analysis of ex vivo intracellular IFN-y production thawed PBMNC were resupended in RPMI supplemented with 10% FCS. Next, cells at 2x106 cells/ml were placed in a 4 ml polystyrene tubes (Greiner) afterwhich anti-CD3 MoAb (WT32 hybridoma supernatant; 10%) and a crosslinking goat-anti-mouse IgG polyclonal antibody (Jackson Laboratories; 10 µg/ml) was added. Samples were incubated for overnight at a 5° slant at 37°C and 5% CO2 • Brefeldin A (Sigma; 10 µg/ml) was used as a blocker of cytokine secretion and added to the samples after the initial 6 hr of culture. After stimulation samples were washed with PBS containing 1 % BSA, and resuspended in a small volume PBS containing 1 % BSA and 5% human AB serum. Then, surface marker-specific antibodies were added (CyQ-labeled anti-CD3; IQproducts, The Netherlands and APC-labeled anti-CDS and PElabeled anti-CD27; BD Biosciences) and cells were incubated for 15 min at room temperature. Next, FACS lysing solution (BD Biosciences) was added and cells were incubated for 10 min at room temperature. Cells were then spun down and resuspended in F ACS permeabilizing solution (Becton Dickinson) and incubated for 10 min at room temperature. After washing human IFN-y-specific FITC-labeled antibody or a FITC-labeled isotypematched control antibody (BD Biosciences) was added and cells were incubated for 30 min. After washing stained cells were analyzed on a flow cytometer (FacsCalibur, Becton Dickinson) by gating on lymphocytes and CD3-positive cells with subsequent analysis of IFN-y expression in gates representing CD8+CD27+ cells and CD8+CD2T cells. Data were analyzed by WinList 3D (Verity software house, Maine, USA). Usually over 20.000 events (CD8 T cells) were acquired for the analysis.
For analysis of IL-2 or IL-15-induced expression of NKG2D thawed PBMNC were resupended in RPMI/10% FCS and placed at 2x106 cells/ml in 4 ml polystyrene tubes (Greiner) afterwhich IL-2 (20 IU/ml; Cetus) or IL-15 (10 ng/ml; R&D systems Inc.) was added. After 24 hr incubation different T cell subsets were analyzed for NKG2D expression as described above.
8 1

- Chapter 6 -
HCMV-infected HUVEC and co-incubation with T cells HCMV (cell-bound HCMV strain TB42; ref.(179))-infected Human
Umbilical Cord Vascular Endothelial Cells (HUVEC) were thawed and mixed at a 1 :3 ratio (infected: non-infected HUVEC) with freshly isolated HUVEC (pooled from 3 umbilical cords) before plating in 6 wells plates. Control plates (non-infected HUVEC) contained freshly isolated HUVEC only. Establishment of HCMV infection, usually over 70 % of cells at day 3, was confirmed using immunofluorescent staining with MoAb E 13 directed against HCMV IE-proteins (Seralab, Sussex, UK). At day 3 HUVEC were irradiated (20 Gy) and washed before co-incubation with CFSE-labeled T cells (3x106 T cells/well) in RPMI/1 0% FCS. In some cases blocking antibodies to ICAM-1 (clone 5/3-2.1), NKG2D (clone 149810; R&D Systems Inc.), IL-2R (Basiliximab, Novartis Pharma BV), and IL-15 (clone 34593.11; R&D Systems Inc.), at 5-10 µg/ml, were added. Part of the (HCMV-infected) HUVEC was used for analysis of surface expression of ICAM-1 and MICA, using anti-human ICAM-1 ( clone 5/3-2.1) and antihuman MICA ( clone AMO-1) MoAb. Secondary step staining procedures were similar as for NKG2D staining (see above).
After 7 days of coculture T cells were harvested and proliferation (CFSE dye dilution) and surface marker expression (routine F ACS staining, as described above) of CDS+ T cells was analyzed on a FacsCalibur flow cytometer (Becton Dickinson).
Statistical analysis Differences in numbers or proportions of CDS+ T cell subpopulations
with expression of IFN-y or NKG2D were analyzed by the Mann-Withney U-test. Increases in cytokine-induced NKG2D expression were analyzed by the Wilcoxon paired test. Categoric data were analyzed by the Chi-square test with Yates' correction. A value of P<0.05 was considered statistically significant.
Results
Emergence of CD8+CD45RA +CD2T effector T cells in HCMV-carrying recipients in vivo
When comparing phenotypes of CDS.. T cells obtained from lung transplant recipients carrying HCMV with that of non-carrying recipients, prominent changes were seen in the CD8+CD45RA"' CD2T effector type T
82

- Human CMV increases alloreactivity by effector T cell proliferation -
cell population. Fig. IA shows that all HCMV-carriers (HCMV -/+, +/- or +/+ matches) had strongly increased percentages of CD45RA+CD2T effector type CD8+ T cells in time, whereas non-carriers had low and stable percentages of this population. In the latter group CD8+ T cells were predominantly of the nai"ve phenotype: usually over 60% of the total CD8+ T cell population were CD8+CD45RA+CD27+ T cells (data not shown). The emergence of CD8+CD45RA+CD2T T cells in HCMV carriers was associated with a persistent HCMV viral load in some patients (patients 7, 11, 13, 14, 15, 18, 19, and 20; Table 1) but not in others (patients 3, 4, 6, and 1 O; Table 1 ). Expansions of effector CD8+ T cells in HCMV carriers was not clearly associated with expansions of HCMV-specific T cells: only 2 of 7 HLA-A2.1 + recipients had clear expansions of HCMV pp65 tetramerpositive. CD8+ T cells (patient 13: 0.03 to 3.8% and patient 14: 0.82% to 8.9%; measured 4 and 12 months post-transplant, respectively). In the remaining 5 HLA-A2.1 T patients, pp65 tetramer-positive CD8+ T cells were detectable (range: 0.12 %-5% ), but did clearly increase.
Early increases in effector T cells is associated with development of BOS
Recipients that developed BOS in the first year after transplantation had a higher percentage of peripheral blood CD8+CD45RA +CD2T effector type T cells compared with patients with good transplant function, particularly at 3 and 6 months after transplantation (Fig. 1B).
A
1 00
N Ill C -75 (.J ai + u
� :, � c C 0
50
(.J iii + -co 0 c :: 25 (.J 0 ::,e 0
0
pre 3 6 12 18 24
Months after transplantation
83

- Chapter 6 -
B . 75 *
Q ,,, u -+ Q)
� � 50 It) co -.:l' Q c U u -+ J!! 25 co 0 c -u o
� 0 0 G BOS G BOS G BOS
Pre-Tx 3 Mo 6 Mo
Figure J. Longitudinal analysis of the CD8+CD45RA.CD2 T T cell subpopulation in peripheral blood samples at different time intervals after lung transplantation. Increasing percentages of CD8+CD45RA +CD2T T cells are seen after transplantation in HCMVcar,ying recipients (HCMV +/- or -/+ or +/+, recipient/donor HCMV-serology status; black squares, Panel A) but not in non-HCMV-car,ying recipients (HCMV -/-, recipient/donor HCMV-serology status; open squares, Panel A). Recipients that developed chronic rejection (BOS; n=J0) in the first year after transplantation had a higher percentage of peripheral blood CD8+CD45RA+CD2T effector type T cells compared with recipients with good transplant function (G; n= I 0) at 3 and 6 months after transplantation. (Panel B; bars indicate mean percentage ± SD; single or double asterisks indicate p< 0.05 or p<0.01, respectively; Mann-Withney U-test}.
BOS patients had more acute rejection episodes and more positive HCMV pp-65 antigenemia tests compared to patients with good graft function {Table 1).
A higher capacity to produce IFN-y ex vivo in recipient derived CD8+CD2T T cells compared to CD8+CD27+ T cells
Next, the capacity of recipient effector type CD8� T cells to produce IFN-y was tested. To this end, recipient PBMNC were stimulated with antiCD3 MoAb and, thereafter, intracellular IFN-y production was analyzed in narve/memory(-effector) T cells (CD8+CD27+ T cells) and effector type CD8+ T cells (CD8+CD2T T cells). Short-term anti-CD3 MoAb stimulation of CD8+ T cells did not induce loss of CD27 expression (data not shown). Fig. 2 shows that CD8+CD2T T cells from samples taken before and 3 months after transplantation, but not 6 months after transplantation, had a higher capacity to produce IFN-y ex vivo compared to CD8+CD27+ T cells,
84

- Human CMV increases alloreactivity by effector T cell proliferation -
demonstrating effector type T cell functions in CDS+CD2T T cells from immunosuppressed lung transplant recipients.
,2 C .... 0 0 :;:::
30
:l!! 3 20 CII Q. U O I- Q. co .c Q � o + 1 0 + co z O !:!:: (.)
Pre-Tx 3 Mo 6 Mo
c::::J CD8+CD27+
- CD8+CD27-
Figure 2. CD8+CD2T T cells have a higher capacity to produce IFN-ythan CD8+CD27+ T cells. Recipient T cells were ex vivo stimulated with anti-CD3 MoAb and tested for intracellular IFN-r production using flow cytomefly. Bars indicate mean percentage ± SD of 8 recipients. Asterisks indicate significant higher percentages IFN-l cells (for pretransplant and 3 months samples p< 0. 05, for 6 months samples p=0.09; Mann-Withney U-test).
NKG2D expression on recipient CD8+CD27+ and CD8+CD2T T cells and ex vivo upregulation by IL-2 and IL-15
Expression of NK.G2D could enhance activation of effector CDS T cells when engaged by its ligand MICA. Therefore, the expression of NKG2D was analyzed on HCMV-carrying recipient naYve/memory(-effector) T cells (CDS+CD27+ T cells) and effector CDS+ T cells (CDS+CD2T T cells). In the period with proliferation of effector CDS+CD2T T cells, i.e. 3-6 months after transplantation, the fraction of HCMV-carrying recipient CDS+CD2T T cells that expressed NKG2D was comparable to that seen in HCMVseropositive healthy controls, i.e. individuals without HCMV reactivation or emergence of effector CD8+ T cells (Fig. 3). Moreover, a similar fraction of recipient or control CD8
+CD2T T cells expressed NKG2D compared to CDS+CD27+ T cells. When PBMNC were cytokine-stimulated and analyzed for NKG2D expression on CD27+ versus CD2T CD8+ T cells a higher expression of NK.G2D was induced by IL-2 or IL-15 in CD8+CD2T T cells, but not in CD8+CD27+ (Fig. 3).
85

C 1 00
iii 0 ... ; £ .!!! 75 .... :::J 0 C. + 0 C C. 50 N .C c., :::J � 1/1 z ct, 25 � c 0 u
- Chapter 6
* * * *
IL-2 IL-1 5 IL-2 IL-1 5
CD8+CD27+ T cells CD8+CD27- T cells
D Controls
• Lung Tx
Figure 3. NKG2D is expressed on both CD27+ and CD2 T CDB+ T cells. NKG2D expression was tested on HCMV-car,ying recipient and healthy control T cells ex vivo in the absence and presence of IL-2 and IL-I 5. A significant increase in NKG2D expression could be induced by Il-2 or IL-J5 in CD8+CD2T T cells, but not in CD8+CD27• (Bars indicate mean percentage ± SD of JO controls and JO patients; patients samples were obtained 3-6 months after transplantation; significant increases compared to baseline values, i.e. in the absence of CJ tokines, is indicated by asterisks; p<O.O5; Wilcoxon paired test).
This was seen in T cells from both controls and lung transplant patients (Fig. 3). Control experiments showed that short-term incubation of CD8+ T cells with IL-2 or IL-15 did not induce loss of CD27 expression (data not shown; in agreement with others, ref.(180)).
In vitro proliferation of NKG2D+ and CD27- CDS+ T cells upon interaction with allogeneic HCMV- infected HUVEC
The expression of NKG2D or loss of CD27 may result from activation of CD8 T cells and presumably also from interaction with (HCMV-infected) allogeneic tissue cells. Figure 4A shows that HCMV infection strongly increased the capacity of allogeneic HUVEC to induce proliferation in peripheral blood CD8+ T cells from HCMV seropositive healthy controls. Proliferating CD8 T cells that were co-incubated with HCMV-infected allogeneic HUVEC also showed an increased expression of NKG2D compared to non-proliferating cells or proliferating CD8+ T cells coincubated with non-infected allogeneic HUVEC (Fig. 4B). Furthermore, proliferating CD8+ T cells that were co-incubated with HCMV-infected allogeneic HUVEC showed a decreased CD27 expression compared to the CD27 expression on proliferating CD8+ T cells co-incubated with noninfected allogeneic HUVEC (Fig. 4B). Thus, interaction of CD8+ T cells
86

- Human CMV increases alloreactivity by effector T cell proliferation -
A HUVEC HUVEC/CMV
co C 0
,. CFSE
B HUVEC HUVEC/CMV
1 % 1 • 3% 1 % .. � C 0 u
� l! 0 .!!! ' �
,r
� 1 8% 10%
C N (!) ::ii::
� z • •
� ,r
• 18°/o· 44% .....
'!��f.:: N C 0
• � 9%'·
� , .. ... ,r
CFSE
Figure 4. Enhanced CD8+ T cell proliferation upon co-incubation with HCMV-infected HUVEC. CFSE dye dilution of gated CD8+ cells was analyzed after co-incubation with non-infected and HCMV-infected HUVEC (Panel A). Representative data from 3 experiments is shown. Percentages of divided cells within the CD8 population is indicated in the upper left quadrant. Gated CD8+ T cells from co-cultures with HCMV-infected HUVEC showed an marked increase in NKG2D-expression and loss ofCD27 expression in proliferated CD8+ T cells in comprison with proliferated CD8 T cells from co-cultures with non-infected HUVEC (Panel B; left graph and right graphs for non-infected and infected HUVEC, respectively). Percentages indicated in the quadrants are percentages within the total gated CD8+ T cell population.
87

- Chapter 6
with HCMV-infected allogeneic HUVEC induces expansion of CD8-CD45RA +CD2T T cells, a subpopulation that emerges in HCMVcarrying lung transplant recipients in vivo, as shown above.
U) -::s 0 u ai (.)
HUVEC
MICA
Ill -C: ::I I 0 u ai (.)
, HUVEC
HUVEC/CMV
ICAM-1
Figure 5. /CAM-I and MICA expression on non-infected and HCMV-infected HUVEC. HUVEC and HCMV-infected HUVEC at day 3 after infection was analyzed for MICA and /CAM-I expression by flow cytomefly: constitutive expression with a slight upregulation in infected HUVEC was demonstrated for MICA and no expression and strong enhanced expression was demonstrated for !CAM-I, respectively.
Blocking of ICAM-1 or NKG2D reduces the proliferation of CD2r and NKG2D+ CDS+ T cells upon interaction with HCMV- infected HUVEC
Uninfected HUVEC stained negative for ICAM-1 but positive for MICA. HCMV-infected HUVEC demonstrated a slight upregulation of MICA expression whereas ICAM-1 was strongly upregulated (Fig. 5).
A o , 0
Ill C: ::I 0 0 a-lCAM-1 u 0 ..... u
C0 Control Ab C u 0
88

B
- Human CMV increases alloreactivity by effector T cell proliferation
Control Ab
a-lCAM-1
a-NKG2D
a-lL2R
a-lL-15
NKG20
C 1 38% N (!) � z
C N (!) � z
4%
7%
& 29% C N (!) t � z
7%
� 12% C N (!) � � z
C N (!) " � z
6%
CD27
� 24% 36% ,.._ N C l (.J
Figure 6. Blocking JCAM-1 or NKG2D reduced the proliferation of CD8+ T cells but not NKG2D expression or loss of CD27 expression. Blocking antibodies to both NKG2D (shaded area) and JCAM-1 (dotted line) reduced proliferation in CD8+ T cells after 7 days of culture with HCMV-infected HUVEC (Panel A). Gated CD8+ T cells harvested at day 7 of coculture with HCMV-infected HUVEC, in the presence of blocking antibodies, were analyzed for NKG2D (Panel B; left graphs) or CD27 (Panel B; right graphs) expression. Representative data from 3 experiments is shown. Antibodies to ICAM-1 or NKG2D did not prevent the expression of NKG2D or loss of CD27 expression on proliferating CD8+ T cells, but reduced the number of divisions in proliferating cells (Panel A and B). IL-2R blocking Ab, but not IL-15 blocking Ab, inhibited proliferation, NKG2D expression, and loss of CD27 (Panel B). Percentages indicated in the quadrants are percentages within the total gated CD8+ T cell population.
89

- Chapter 6 -
Blocking antibodies to ICAM-1 and NKG2D reduced the number of divisions in proliferating cells (Fig. 6A), but did not prevent the expression of NKG2D or loss of CD27 expression on proliferating CD8+ T cells (Fig. 68). Proliferation of HCMV-infected HUVEC-activated CD8+ T cells, expression of NKG2D, and loss of CD27 expression was prevented by blocking the IL-2R, but not by blocking IL-15 (Fig. 6B).
Discussion
In the present study we found in vivo accumulation of CD8+CD45RA +CD2T T cells in HCMV-carrying lung transplant recipients, particularly in those that developed BOS. These cells were functional with respect to IFN-y production and showed NKG2D expression which could be upregulated by IL-2 and IL-15. HCMV-infected HUVEC in vitro, expressing the NKG2D ligand MICA and highly expressing ICAM-1, induced proliferation of CD8+ T cells with increased NKG2D expression and loss of CD27 expression. Blocking antibodies against ICAM-1 and NKG2D decreased CD8+ T cell proliferation upon in vitro culture with HCMV-infected HUVEC, but did, however, not inhibit increases in NKG2D expression or loss of CD27. These data point to a role for HCMV in enhancing graft reactive responses in which HCMV-mediated effects both on the recipient's cellular immune system, i.e. effector CD8+CD2T NKG2D+ T cell proliferation, as well as on graft tissue cells that express ICAM-1 and the NKG2D ligand, MICA, may play a role.
Our data are in agreement with findings of other investigators who also observed increased numbers of CD8+CD45RA +CD2T T cells in primary HCMV infected children and primary and secondary HCMV infection in kidney transplant recipients ( 145, 181 ). Notably, the proportion of CD8+CD45RA +CD2T T cells that emerge (and persist) in lung transplant recipients appears to be much higher when compared to previous reports: mean percentages of approximately 17% were found in kidney transplant recipients (145) vs 65% in our lung transplant recipients. This may be due to high reactivation of HCMV in lungs by the relatively large amounts of lymphatic tissue in lungs that harbor latent HCMV (20). Moreover, latent HCMV virus that is carried in recipient immune cells that are recruited into lung transplants efficiently reactivates as a result of immune cell activation, particularly after lung transplantation, thus transfering virus to the graft (182, 183). The high immunogenicity of lung transplants may therefore
90

- Human CMV increases alloreactivity by effector T cell proliferation -
predispose to a high level of HCMV reactivation in HCMV-seropositive lung graft recipients.
It is striking that in a number of patients who did not demonstrate a persistent HCMV viral load a high proportion of CD8+CD45RA+CD2T T cells developed and persisted in the peripheral blood. An explanation for this phenomenon could be that HCMV reactivation after lung transplantation involves a low grade, but continuous process of local tissue infection with a high degree of abortive infections. This may not result in HCMV pp65 production and, consequently, positive HCMV pp-65 antigenemia tests. It is likely that the observed effector CD8+ T cells in our patients are contributing to the abortion of the virus reactivation, possibly by reacting to HCMV IE antigens. In support of this notion, Kern et al. (184) showed that frequencies of HCMV IE-specific T cells can be much higher than frequencies of T cells directed against HCMV pp65. Also, (large) expansions of HCMV pp65-specific T cells were not commonly seen in our patients. The occurrence of low grade and, possibly, abortive infection in lung transplant patients is further supported by data of Greijer et al. (185) who demonstrated CMV IE mRNA in peripheral blood samples in 69% (primary infections) and 43% (secondary infections) of CMV-carrying lung transplant patients with negative CMV pp65 antigenemia test results.
The lung transplant recipients included in this study did not receive ganciclovir prophylaxis. This treatment, however, is at present more commonly applied in lung transplantation centers (20), including recently our center, since it reduces the incidence of HCMV disease. This raises the question if ganciclovir prophylaxis would inhibit HCMV-induced effects on the immune system and, in general, on the development of acute and chronic rejection. In this respect, it has been shown that human HCMVinduced ICAM-1 and HCMV-IE antigen expression and immune activation of T cells by HCMV-infected allogeneic cells could not be inhibited by ganciclovir (146, 147). On the other hand, antiviral prophylaxis with ganciclovir did prevent rat CMV infection enhanced obliteration of rat trachea transplants (186). In recent studies in lung transplant recipients, however, a beneficial effect of ganciclovir prophylaxis on the development of BOS and survival was not found (187, 188). This underlines the importance of HCMV-matching on lung transplant survival. As suggested by Zamora (20), ganciclovir may only delay infection or reactivation. This indicates that HCMV-mediated effects on graft-directed immune responses could evolve also after an initial period with ganciclovir prophylaxis, a notion which necessitates further investigation.
9 1

- Chapter 6
In this study, we postulated that HCMV enhances graft-directed responses through its effect on the generation of T cell subsets with an increased effector function together with an enhanced cross-reactivity towards alloantigens. Lung recipient CD8+CD2T T cell more efficiently produced IFN-y than CD8+CD27+ T cells, a finding in agreement with reports showing an inverse correlation between quantitative CD27 expression and cytotoxic effector function (189). Besides a higher effector function, an enhanced crossreactivity of T cells may be induced by HCMV infection, this through the expression of NKG2D on T cells and (graft) tissue cell expression of its ligand MICA. NKG2D expression could be acquired when CDS+ T cells enter (inflamed) tissue. For example, increased expression of NKG2D by tissue-expressed IL-15 has been demonstrated for intra-epithelial T cells ( 190). This may similarly apply to graft-infiltrating CDS+ T cells as well. IL-15 expression is shown to be induced by viral infection-induced type I interferons (160), which probably also occurs in HCMV infection. In our in vitro experiments IL-15, however, appeared not to be involved in CDS proliferation and upregulation of NKG2D upon coculture with HCMV-infected HUVEC (Fig. 6). In contrast, signalling activity by IL-2 appeared to be essential in this respect (Fig. 6). It is unknown whether activated and IL-2 producing CD4+ T cells were involved in the in vitro potentiation of CDS proliferation into effector cells, since unfractionated T cell preparations were used in these experiments.
HCMV-infection of HUVEC resulted in an increased ICAM-1 expression and only a slight upregulation of MICA (Fig. 5). It is noted that HUVEC already had some low level expression of MICA which is in agreement with others (191 ). Blocking experiments suggested that, besides ICAM-1-LFAl interactions, the NKG2D-MICA interaction contributed to CDS proliferation as well. In this respect, it is likely that both ICAM-1 and MICA ligands contribute to CDS+ T cell activation and proliferation through their contribution to the formation of ring junctions in the immunological synaps (192). The simultaneous activity oflCAM and MICA will reduce the treshold for CDS+ T cell activation allowing also weakly alloreactive CDS+
T cells (with high tresholds for activation) to participate in the response, thus allowing a more broad recognition of allogeneic cells. Importantly, a role for MICA in graft-directed immune responses is further supported by recent studies showing the development of (graft-expressed) MICA-specific antibodies in patients with acute rejection of kidney grafts and in vivo
92

- Human CMV increases alloreactivity by effector T cell proliferation -
expression of MICA on kidney tubulus epithelial cells in acute and chronic rejection (193, 194).
In conclusion, HCMV may enhance graft-directed responses by supporting the proliferation of effector type CD8+CD2T T cells that express NKG2D together with the induction of expression of ICAM-1 and the NKG2D ligand MICA on graft tissue cells.
93

94

Chapter 7
General discussion

- Chapter 7 -
During recent years, lung transplantation has become an accepted treatment option for patients suffering from end-stage pulmonary diseases, as a result of improvements in operation techniques and newly developed immunosuppressive drugs. Loss of graft function, however, remains a major problem after lung transplantation. The survival rates at 5 and 10 years after transplantation are 49% and 24%, respectively, according to the Registry of the International Society of Heart and Lung Transplantation ( 6). An important cause of graft loss beyond the first year after transplantation is chronic rejection of the lungs. Chronic rejection of the lungs is predominantly characterized by an ongoing fibroproliferative process of the airways, with inflammation and fibrosis of the lamina propria and lumen. This process, called bronchiolitis obliterans (BO), is considered to be the major and leading threat for long-term function and survival of clinical lung grafts. It is reported to be the cause of death in over 30% of the lung transplant patients (6). Although, many factors have been suggested to be involved in the development of chronic rejection, a complete insight in the etiology and pathophysiology of chronic rejection after lung transplantation is lacking.
In Chapter 1 of this thesis risk factors contributing to chronic rejection are reviewed. Possible pre-transplant risk factors for the development of chronic rejection are brain death and ischemia-reperfusion injury. Also, post-transplant factors such as infections and acute rejection are assumed to be involved.
The aim of this thesis, described in Chapter 2, was to study whether damage before, during, or early after transplantation has an effect on the development of chronic rejection after lung transplantation. This knowledge is mandatory in order to design means to overcome chronic rejection. Therefore, we studied some essential factors in the development of chronic rejection in the lung after transplantation in both experimental animals and in humans.
Chronic rejection and brain death
In Chapter 3 we investigated whether the pre-transplant factor brain death has an effect on the development of chronic rejection. Our study shows that brain death increases inflammatory mediators in the donor lung (increased number of PMNs and macrophages and VCAM-1 expression) and aggravates chronic rejection (a decreased lung function, heavy
96

- General discussion -
perivascular, peribronchiolar, and interstitial leukocyte infiltration, severe intimal hyperplasia in the transplant's blood vessels, and increased IL-2 mRNA expression) after lung transplantation. Previous studies have already shown that brain death has a detrimental effect on donor organs: brain death increases inflammatory mediators in lungs, kidneys, and livers from braindead rats (53-57). Upon transplantation of organs from these brain-dead donors, acute rejection of heart and kidney rat allografts was accelerated (58, 59). Those studies, however, focussed on the early post-operative period. Our study is the first to investigate the long-term effects and to show that brain death is a risk factor for chronic rejection in lung transplantation.
Our observations indicate that the pathophysiology of the process leading to chronic rejection is already initiated before transplantation in the donor, instead of in the recipient, by an inflammatory response in the lungs from brain-dead donors. This inflammatory response can contribute to increased immunogenicity of transplanted organs, which will intensify the process of acute rejection. This may well be a central factor in the mechanism of chronic rejection, as it has been shown convincingly in lung transplant recipients that the number and severity of acute rejection episodes is the most important risk factor for the development of chronic rejection (79, 80). Thus, brain death has a detrimental effect in the donor lung affecting transplant outcome not only on the short, but also on the long-term after lung transplantation.
Different strategies can be developed to treat or avoid the effects of brain death leading to chronic rejection. Most efforts are aiming at reducing the negative effects of brain death on the donor organ. In experimental models, it has been shown that treatment of brain-dead donor rats with steroids decreased the early inflammatory changes (195), decreased expression of pro-inflammatory mediators, decreased acute rejection, and prolonged survival of transplanted kidneys ( 196). In a clinical study, it has been shown that treatment with steroids of brain-dead human donors before organ harvest significantly decreased tissue and serum expression of proinflammatory cytokines in livers (197). A similar treatment of donor lungs resulted in improved oxygenation and increased donor lung recovery after brain death (198). Furthermore, a clinical study shows that application of catecholamines to brain-dead donors is associated with improved graft survival after transplantation of kidneys (199). In addition to the reduction of brain-dead induced inflammation, treatment of donors with steroids could also lead tot the generation of donor-derived tolerogenic dendritic cells. These cells could, upon transplantation, induce regulatory T cells which
97

- Chapter 7 -
contribute to graft acceptance and favorable long-term outcome (200). Thus, above results show that treatment of the brain-donor can improve the quality of the donor organ and can have a beneficial effect on acceptance, function, and survival of the organ after transplantation. Therefore, it is important that donor-related therapeutic treatments should be developed.
To avoid the negative effects of brain death on the donor organ completely, lungs can be transplanted from living donors. Clinical data have shown that the incidence of chronic rejection in pediatric lungs transplanted from living donors is lower compared with brain-dead donors (108, 109). The negative effects of brain death on the donor lung found in our study may therefore explain the clinical difference in long-term function between lungs from cadaveric donors and living donors. From this point of view, living donor lung transplantation seems to be preferable over cadaveric transplantation. It has, however, major obstacles preventing widespread application. One significant problem is the risk to the donors, mostly relatives of the patients. Nevertheless, this option might continue to be used under properly selected circumstances. It needs to be awaited if the absence of bronchiolitis obliterans in lungs transplanted from living donors remains if more patients are observed and patients are monitored for a longer postoperative period.
A recent development is the use of non-heart beating donors (NHBD) for lung transplantation. This is a possible solution for the shortage of suitable donor organs. This procedure, in which donors had a cardiac arrest, but were not brain-dead, possibly effects the development of chronic rejection. So, it would be interesting if results of transplantation of lungs from NHBDs are superior to those of brain-dead donors. At present, NHBDs are used mainly in kidney transplantation. Results so far show that kidneys transplanted from NHBDs have a high rate of delayed function, but the long-term function appears to be similar to kidneys transplanted from brain-dead donors (201-203 ). Thus, kidneys from NHBDs are an acceptable alternative to those from brain-dead donors. In lung transplantation also some succesful transplantations have been performed from NHBDs, but these are few compared with renal transplantation and results on the long-term remain to be seen (204-206).
98

- General discussion -
Chronic rejection and viral infections
The most obvious post-transplant risk factors for chronic rejection are virus infections in the recipients which frequently occur in lung transplantation patients. In this thesis we studied two types of virus infections in the pathophysiology of chronic rejection, namely a respiratory virus infection with Sendai virus, which locally infects epithelial cells of the airways and a virus infection which disseminates systemically, i.e. cytomegalovirus (CMV) infection.
In Chapter 4 we investigated whether a local respiratory infection with Sendai virus can abrogate acceptance of the lung after transplantation in rats. Our study shows that despite the slightly increased peribronchiolar infiltration and an increased infiltration of CD3+ T cells in lung grafts after Sendai infection, no other, more evident symptoms of increased graft rejection were found. Thus, a local viral infection with Sendai virus in lung allografts did not consistently abrogate acceptance of the lung graft. The absent effect of Sendai infection on graft rejection seen in our study might be explained by several factors, including the presence of regulatory T cells. Previous studies already showed the development of regulatory T cells when a short-term low dose cyclosporin-A (CsA) treatment is used in rat recipients of hearts transplants (122). Therefore, it is possible that in our study regulatory T cells were present and that these cells may have counteracted the cytotoxic activity of alloreactive T cells that entered the graft as a result of the pro-inflammatory response induced by the Sendai virus infection.
Although not confirmed in our study, the findings that respiratory virus infections are associated with acute and chronic rejection after lung transplantation (30, 67, 68, 73, 75) warrants further exploration for example by investigating the effects of treatment. In this respect, the treatment of respiratory virus infections with antiviral drugs in lung transplant recipients remains rather empirical (28, 29). In addition to the use of antiviral drugs, vaccination may be used to limit infection with influenza virus. Influenza vaccines have been regularly used in immunocompromised hosts, however, there has been concern that immunosuppressive therapy reduces the antibody response to the vaccine when compared to immunocompetent hosts. Indeed, antibody responses upon influenza vaccination were found to be decreased in lung transplant recipients (207, 208). Furthermore, influenza vaccination does not stimulate a cell-mediated immune response in lung
99

- Chapter 7
transplant recipients (209). Therefore, more research needs to be performed to investigate the usefullness of vaccination of influenza virus in lung transplant recipients, and possible effects on the long-term outcome of lung transplants.
Besides a respiratory virus we also investigated a more systemically disseminating virus, i.e. CMV, in rats (Chapter 5) and humans (Chapter 6). CMV is not directly deleterious for the lung tissue but causes a more systemic inflammatory response. The exact role of CMV enhancing acute and chronic rejection is subject of a long-lasting debate. Many studies show that CMV is associated with the development of chronic rejection in lung transplant patients (61, 62), while others claim an absence of effect (65, 66).
Our studies in rats and humans showed that CMV infection modulates both the recipient's immune system and the immunogenicity of allogeneic (transplant) tissue cells, which activities may act in concert to enhance the graft-reactive response.
Because CMV is associated with acute and chronic rejection, it is important that therapeutic strategies are developed to prevent CMV infection. At present, ganciclovir prophylaxis is used to prevent CMV infection and is commonly applied in lung transplantation centers (20), including recently our center. It has been shown that ganciclovir prophylaxis reduces the incidence of HCMV disease. Therefore, it is important to know if ganciclovir prophylaxis would inhibit the development of chronic rejection. A previous study showed that enhanced obliteration of rat trachea transplants in rats infected with rat CMV is prevented by antiviral prophylaxis with ganciclovir (186). However, it has been shown that human HCMV-induced ICAM-1 and HCMV-IE antigen expression and immune activation of T cells by HCMV-infected allogeneic cells could not be inhibited by ganciclovir (146, 14 7). In recent studies in lung transplant recipients, no beneficial effect of ganciclovir prophylaxis on the development of BOS and survival was found (187, 188). Furthermore, it has been suggested that ganciclovir may only delay infection or reactivation (20). Thus, HCMV-mediated effects on graft-directed immune responses could evolve also after an initial period with ganciclovir prophylaxis. Therefore, more research needs to be performed to investigate therapeutic strategies to treat or prevent CMV infection.
A virus that may also contribute to chronic rejection in lung transplant recipients is the Epstein-Barr virus (EBV). EBV is related to the
1 00

- General discussion -
development of post-transplant lymphoproliferative disease (PTLD) in immunocompromised patients. PTLD is characterized by uncontrolled B lymphocyte proliferation after transplantation. The incidence of PTLD after lung and heart-lung transplant recipients ranges from 1.5-9%. In the University Medical Center Groningen the activity of EBY is monitored in patients based on viral DNA load in blood. Guided by this DNA load the immunosuppressive treatment is changed. If the DNA load is high the immunosuppresion is reduced. Since the EBY-guided stepwise reduction of immunosuppression was introduced the incidence of BO was decreased. This reduction of the incidence of BO can be a result of this program, but more factors may have helped to improve the outcome, because at that period also CMY prophylaxis was introduced and the induction therapy was changed (from A TG to anti-CD25). Nevertheless, the data strongly supports the idea that viral infections play a role in the induction of chronic rejection.
In summary, different factors can contribute to the development of chronic rejection. In this thesis we studied some of these factors, namely the pre-transplant factor brain death and the post-transplant factor viral infection. The results show that both factors contribute to chronic rejection by a dual effect: on the one hand on the recipient's immune system with enhancement of it's alloreactive potential and on the other hand on transplant tissue cells with enhancement of their immunogenicity. So, it can be concluded that early damage before (brain death) and early damage after transplantation (viral infection) contribute to chronic rejection. Thus, it is not a single factor, but a combination of factors that plays a role in the development of chronic rejection.
101

102

Chapter 8
Summary

- Chapter 8
Chronic rejection of the lungs, characterized by bronchiolitis obliterans (BO), is the major threat for long-term function and survival of clinical lung grafts. BO is an ongoing fibroproliferative process of the airways with inflammmation and fibrosis of the lamina propria and obliteration of the lumen as a consequence and affects about 50% of recipients within 5 years after lung transplantation. Many factors have been suggested to be involved in the development of chronic rejection, but a complete insight in the etiology and pathophysiology of chronic rejection is still lacking.
Chapter 1 gives an overview of the current status of lung transplantation and of the clinical and histopathological hallmarks of chronic rejection after lung transplantation. Moreover, it describes risk factors for the development of chronic rejection. The pre-transplant risk factors such as brain death and ischemia-reperfusion injury and the early post-transplant risk factors such as infections and acute rejection are assumed to be involved in the development of chronic rejection. Based on the review of risk factors we hypothesize that early damage before, during, or early after transplantation can cause an inflammatory response which can have an effect on the development of chronic rejection after lung transplantation. Chapter 2 presents the aim of the research described in this thesis, which is analyzing the effects of the early risk factors brain death and viral infections such as Sendai virus and cytomegalovirus (CMV) on the initiation of chronic rejection.
In Chapter 3 we investigated the hypothesis that brain death increases inflammatory mediators in the donor lung and subsequently aggravates chronic rejection of the lungs after transplantation in rats. Therefore, donor lungs of brain-dead rats were investigated for influx of leukocytes, expression of cell adhesion molecules, and cytokine mRNA expression. Transplanted lungs of brain-dead rats were investigated for lung function, histologic symptoms of chronic rejection and cytokine mRNA expression. This study shows that brain death induces an inflammatory response in the donor lung and subsequently aggravates chronic rejection after transplantation. This may explain the clinical difference in long-term function between lungs from cadaveric donors and living donors.
In Chapter 4 we investigated whether a local Sendai virus infection could abrogate the acceptance of rat allografted lungs that, despite inflammation peaking at day 28, are accepted due to a short-term cyclosporin-A (CsA) treatment after transplantation. Therefore, transplanted rats with CsA immunosuppression were infected intratracheally with Sendai
104

- Summary -
virus. The effects of Sendai infection on cellular infiltration and epithelial changes as well as infiltration of inflammatory cells and cytokines were investigated. The overall data support the view that, despite inflammation peaking at day 28, acceptance of the lung is not abrogated by a local Sendai virus infection after lung transplantation in rats.
In Chapter 5 we tested the hypothesis that one mechanism by which CMV could enhance rejection of lung grafts is through generation of immune effector cells during CMV infection and immunosuppression. These effector cells may have the capacity to promiscuously recognize CMV-infected tissue cells, including CMV-infected allogeneic tissue cells, leading to an increased lung graft infiltration. Therefore, transplanted rats were immunosuppressed with CsA and, subsequently, infected with rat cytomegalovirus (RCMV). The effects of RCMV infection on leukocyte subsets in peripheral blood and inflammatory responses in the grafted lung with local expression of cytokines were analyzed, as well as the capacity of the immunocompromised and RCMV-exposed recipient's immune system to respond to (allogeneic) RCMV-infected tissue cells in vitro. The overall data support the view in the rat an interplay between the recipient's immune system system ( accumulation of NK cells and CD8�KRP 1 + T cells) and CMV-induced effects on the levels of the allogeneic (transplant) tissue cells with increased immunogenicity, may result in an enhanced transplant reactive immune response.
In Chapter 6 we tested the hypothesis that human CMV has dual effects, both on the recipient's immune system as well as on transplant tissue cells: HCMV induces recipient effector type CD8+ T cells that, via expression of NKG2D, broadly recognise HCMV-infected and MICA-expressing donor target cells. These effects, acting in concert, may enhance graft reactive responses. Therefore, peripheral blood samples from HCMV-carrying and non-HCMV-carrying lung transplant recipients were analyzed for CD8+ T cell expression of CD45RA and CD27. CD2T and CD27+ CD8+ T cells were investigated for intracellular IFN-y production and expression of NKG2D. Also, the capacity of HCMV-infected HUVEC expressing ICAM-1 and MICA, to stimulate the proliferation of T cells was analyzed. This study shows that HCMV may enhance graft-directed responses by supporting the proliferation of effector type CD8+CD2T T cells that express NKG2D together with the induction of expression of ICAM-1 and the NKG2D ligand MICA on graft tissue cells.
1 05

- Chapter 8
In Chapter 7 the results described in this thesis are discussed. It can be concluded that early damage before (brain death) and early damage after transplantation (viral infection) can contribute to chronic rejection. We conclude that a combination of factors and not a single factor are causative for the initiation and progression of chronic rejection of lung allografts.
1 06

Chapter 9
Nederlandse samenvatting (voor niet-ingewijden)

- Chapter 9
lnleiding
Longtransplantatie is in de afgelopen jaren een succesvolle tberapie geworden voor patienten die lijden aan verscbillende vormen van longziekten zoals COPD ( chroniscbe obstructieve longziekten) en taaislijmziekte. De eerste longtransplantaties werd uitgevoerd in de periode 1963 tot 1973, maar deze waren niet succesvol als gevolg van incomplete onderdrukking van bet afweersysteem. Het duurde tot 1983 voordat de eerste succesvolle longtransplantatie werd uitgevoerd.
In bet ideale geval kunnen longen getransplanteerd worden tussen een donor en ontvanger die niet genetiscb van elkaar verscbillen, een zogenaamde syngene transplantatie, zoals bet geval is bij een eeneiige tweeling. Bij zo'n transplantatie zullen de longen na transplantatie in bet algemeen goed functioneren en niet worden afgestoten. Alleen komen deze transplantaties in de praktijk niet vaak voor. De meeste longtransplantaties vinden plaats tussen een donor en ontvanger die wel genetiscb van elkaar verscbillen, een zogenaamde allogene transplantatie. Bij deze transplantaties kan er wel een afstotingsreactie plaatsvinden. Het afweersysteem van de ontvanger zal namelijk de getransplanteerde long zien als licbaamsvreemd en zal proberen deze te vemietigen. Om deze afstotingsreactie te voorkomen wordt er gebruik gemaakt van medicijnen om bet afweersysteem van de ontvanger te onderdrukken, de zogenaamde immunosuppressie. Ondanks bet gebruik van immunosuppressie is de overleving na longtransplantatie op lange termijn beperkt. Volgens de wereldwijde registratie van transplantatiegegevens is de overleving na 1 jaar 80%, terwijl die na 5 en 10 jaar respectievelijk 49% en 24% bedraagt.
De voomaamste oorzaak van de beperkte overleving van longen na transplantatie op lange termijn is bet ontstaan van cbroniscbe rejectie. Chronische rejectie kan gezien worden als een sluimerende ontstekingsreactie dat tot uiting komt als een voortdurende achteruitgang van de functie van longen na transplantatie. Dit is onomkeerbaar met als uiteindelijke gevolg dat longen zo slecht functioneren dat patienten opnieuw getransplanteerd moeten worden. In longen wordt chronische rejectie gekarakteriseerd door bronchiolitis obliterans. Histologische tekenen van bronchiolitis obliterans in de longen zijn ontstekingsreacties gevolgd door fibrose (toename van bindweefsel) in de luchtwegen, wat uiteindelijk resulteert in het dichtgroeien van de luchtwegen waardoor de longen niet meer kunnen functioneren. Ongeveer 50% van de longtransplantatie-
108

- Nederlandse samenvatting
patienten ontwikkelen bronchiolitis obliterans binnen 5 jaar na transplantatie. Op dit moment kan bronchiolitis obliterans niet voorkomen of behandeld worden met de huidige immunosuppressie.
De oorzaak waarom chronische rejectie, gekarakteriseerd als bronchiolitis obliterans, zich uiteindelijk ontwikkelt is niet geheel duidelijk. Hoewel er in de afgelopen jaren verschillende risicofactoren beschreven zijn die bijdragen aan de ontwikkeling van chronische rejectie, is het precieze mechanisme dat hieraan ten grondslag ligt nog grotendeels onbekend. Zowel factoren die gericht zijn tegen de lichaamsvreemde long als andere factoren blijken een rol te spelen bij het ontstaan van chronische rejectie.
Dit proefschrift
De doelstelling van het onderzoek beschreven in dit proefschrift was het onderzoeken van het effect van een aantal vroege risicofactoren op het ontstaan van chronische rejectie na longtransplantatie.
Hoof dstuk 1 gee ft een algemene inleiding over longtransplantatie waarin de klinische en histologische kenmerken van chronische rejectie na longtransplantatie beschreven zijn. Daamaast worden risicofactoren voor het ontstaan van chronische rejectie besproken. De pre-transplantatie factoren zoals hersendood en ischemie-reperfusieschade en de vroege posttransplantatie factoren infectie en acute rejectie lijken een rol te spelen in de ontwikkeling van chronische rejectie. Verder wordt de hypothese van het onderzoek gepresenteerd. De hypothese is <lat vroege schade voor, tijdens of na transplantatie een ontstekingsreactie veroorzaakt die van invloed is op het ontstaan van chronische rejectie na longtransplantatie.
In hoofdstuk 2 wordt de doelstelling van het onderzoek beschreven. Deze doelstelling was het onderzoeken van het effect van vroege risicofactoren op het ontstaan van chronische rejectie na longtransplantatie.
In hoofdstuk 3 is het effect beschreven van de pre-transplantatie factor hersendood op het ontstaan van chronische rejectie na longtransplantatie in ratten. In dit hoofdstuk is de hypothese onderzocht dat hersendood een ontstekingsreactie veroorzaakt in de donorlong en vervolgens chronische rejectie van de longen verergert na transplantatie. Voor dit onderzoek zijn ratten hersendood gemaakt waama de donorlongen onderzocht zijn op de toename van leukocyten (witte bloedcellen), expressie van celadhesie moleculen en cytokine mRNA expressie. Vervolgens zijn longen van
109

- Chapter 9
bersendode ratten getransplanteerd waama ze 100 dagen na transplantatie onderzocbt zijn op longfunctie, weefselkenmerken van cbroniscbe rejectie en cytokine mRNA expressie. Het onderzoek laat zien dat bersendood een ontstekingsreactie veroorzaakt in de donorlong die vervolgens na transplantatie resulteert in een verergering van chronische rejectie. Deze resultaten kunnen bet kliniscbe verschil in functioneren van longen op lange termijn verklaren tussen hersendode donoren en levende donoren.
In hoofdstuk 4, 5 en 6 is het effect van de post-transplantatie factor virusinfectie op bet ontstaan van chroniscbe rejectie na longtransplantatie onderzocht. In hoofdstuk 4 is onderzocbt of een locale Sendaivirusinfectie ( een luchtweginfectie) de acceptatie van getransplanteerde allogene longen in ratten kan doorbreken. De getransplanteerde longen zijn geaccepteerd middels een kortdurende bebandeling met immunosuppressie ( cyclosporine) na transplantatie. Voor dit onderzoek zijn getransplanteerde ratten behandeld met immunosuppressie en vervolgens via de luchtpijp ge'infecteerd met Sendaivirus. Daama zijn zowel de effecten van Sendaivirusinfectie op celinfiltratie en epitheelveranderingen als infiltratie van ontstekingscellen en cytokines onderzocbt. De resultaten laten zien dat, ondanks een versterkte ontsteking op dag 28, de acceptatie van longen niet doorbroken wordt door een Sendaivirusinfectie na longtransplantatie in ratten.
In hoof dstuk 5 en 6 is bekeken wat bet effect van cytomegalovirusinfectie is na transplantatie. In hoofdstuk 5 is het onderzoek uitgevoerd in ratten en in hoofdstuk 6 is gebruik gemaakt van humaan materiaal. In hoofdstuk 5 is gekeken wat bet effect van cytomegalovirus (CMV) op het afweersysteem van de ontvanger is en op de getransplanteerde weefselcellen. Voor dit onderzoek zijn getransplanteerde ratten behandeld met immunosuppressie en vervolgens ge'infecteerd met ratcytomegalovirus. De resultaten laten zien dat CMV-infectie een toename veroorzaakt van effectorcellen en dat CMV-ge'infecteerde allogene weefselcellen een verboogde capaciteit hebben om door het aan CMV blootgestelde afweersysteem van de ontvanger herkend te worden. Verder is in de long een verhoogde toename van cellen gevonden. De effecten van CMV op het afweersysteem van de ontvanger en op de getransplanteerde weefselcellen in de rat kunnen resulteren in een verhoogde afweerreactie tegen de getransplanteerde long.
In vervolg op de rattenstudie is in hoofdstuk 6 bet effect van CMV onderzocht in longtransplantatiepatienten. Hierbij is gekeken of ook humaan CMV een tweeledig effect heeft, op zowel bet afweersysteem van de
1 10

- Nederlandse samenvatting -
ontvanger als op getransplanteerde weefselcellen. De resultaten laten zien dat humaan CMV een toename van effectorcellen veroorzaakt die een activerende receptor (NKG2D) op hun celoppervlak tot expressie brengen. Verder veroorzaakt humaan CMV een toename van de expressie van ICAM-1 en NKG2D ligand MICA op getransplanteerde weefselcellen. Door deze effecten kan humaan CMV de afweerreactie tegen getransplanteerde longen verhogen.
In hoofdstuk 7 worden de resultaten uit dit proefschrift bediscussieerd. Er kan geconcludeerd worden dat vroege schade die al ontstaat voor (hersendood) of kort na transplantatie (virusinfectie) een ontstekingsreactie teweegbrengt die uiteindelijk resulteert in de ontwikkeling van chronische rejectie. We concluderen dat een combinatie van factoren en niet een factor bijdraagt aan het ontstaan en progressie van chronische rejectie van longen na transplantatie.
1 1 1


References
Abbreviations
Dankwoord

- References
References
1. Hardy JD, Webb WR, Dalton ML, Jr., Walker GR, Jr. Lung Homotransplantation in Man. Jama 1963; 186: 1065.
2. Reitz BA, Wallwork JL, Hunt SA, et al. Heart-lung transplantation: successful therapy for patients with pulmonary vascular disease. N Engl J Med 1982; 306 (10): 557.
3. Unilateral lung transplantation for pulmonary fibrosis. Toronto Lung Transplant Group. N Engl J Med 1986; 314 (18): 1140.
4. Studer SM, Levy RD, McNeil K, Orens JB. Lung transplant outcomes: a review of survival, graft function, physiology, healthrelated quality of life and cost-effectiveness. Eur Respir J 2004; 24 (4): 674.
5. Smeritschnig B, Jaksch P, Kocher A, et al. Quality of life after lung transplantation: a cross-sectional study. J Heart Lung Transplant 2005; 24 (4): 474.
6. Trulock EP, Edwards LB, Taylor DO, Boucek MM, Keck BM, Hertz Ml. Registry of the International Society for Heart and Lung Transplantation: twenty-second official adult lung and heart-lung transplant report--2005. J Heart Lung Transplant 2005; 24 (8): 956.
7. DeMeo DL, Ginns LC. Lung transplantation at the tum of the century. Annu Rev Med 2001; 52: 185.
8. Starnes VA, Lewiston NJ, Luikart H, Theodore J, Stinson EB, Shumway NE. Current trends in lung transplantation. Lobar transplantation and expanded use of single lungs. J Thorac Cardiovasc Surg 1992; 104 ( 4): 1060.
9. Date H, Aoe M, Sano Y, et al. Improved survival after living-donor lobar lung transplantation. J Thorac Cardiovasc Surg 2004; 128 (6): 933.
1 14

- References -
10. Bowdish ME, Pessotto R, Barbers RG, Schenkel FA, Starnes VA, Barr ML. Long-term pulmonary function after living-donor lobar lung transplantation in adults. Ann Thorac Surg 2005; 79 (2): 418.
1 1. Kotloff RM, Ahya VN. Medical complications of lung transplantation. Eur Respir J 2004; 23 (2): 334.
12. Alexander BD, Tapson VF. Infectious complications of lung transplantation. Transpl Infect Dis 2001; 3 (3): 128.
13. Knoop C, Haverich A, Fischer S. Immunosuppressive therapy after human lung transplantation. Eur Respir J 2004; 23 (1): 159.
14. Chaparro C, Chamberlain D, Maurer J, De Hoyos A, Winton T, Kesten S. Acute lung injury in lung allografts. J Heart Lung Transplant 1995; 14 (2): 267.
15. Christie JD, Bavaria JE, Palevsky HI, et al. Primary graft failure following lung transplantation. Chest 1998; 114 ( 1 ): 51.
16. Khan SU, Salloum J, O'Donovan PB, et al. Acute pulmonary edema after lung transplantation: the pulmonary reimplantation response. Chest 1999; 116 (1): 187.
17. Kubak BM. Fungal infection in lung transplantation. Transpl Infect Dis 2002; 4 Suppl 3: 24.
18. Maurer JR, Tullis DE, Grossman RF, Vellend H, Winton TL, Patterson GA. Infectious complications following isolated lung transplantation. Chest 1992; 101 (4): 1056.
19. Kramer MR, Marshall SE, Starnes VA, Gamberg P, Amitai Z, Theodore J. Infectious complications in heart-lung transplantation. Analysis of 200 episodes. Arch Intern Med 1993; 153 (17): 2010.
20. Zamora MR. Cytomegalovirus and lung transplantation. Am J Transplant 2004; 4 (8): 1219.
1 1 5

- References -
2 1 . Duncan AJ, Dummer JS, Paradis IL, et al. Cytomegalovirus infection and survival in lung transplant recipients. J Heart Lung Transplant 1 991 ; 1 0 (5 Pt 1 ): 638.
22. Smyth RL, Scott JP, Borysiewicz LK, et al. Cytomegalovirus infection in heart-lung transplant recipients: risk factors, clinical associations, and response to treatment. J Infect Dis 1 99 1 ; 1 64 ( 6): 1 045.
23. Aris RM, Maia DM, Neuringer IP, et al. Post-transplantation lymphoproliferative disorder in the Epstein-Barr virus-naive lung transplant recipient. Am J Respir Crit Care Med 1996; 1 54 (6 Pt 1 ): 17 12.
24. Montone KT, Litzky LA, Wurster A, et al. Analysis of Epstein-Barr virus-associated posttransplantation lymphoproliferative disorder after lung transplantation. Surgery 1 996; 1 19 (5): 544.
25. Tsai DE, Hardy CL, Tomaszewski JE, et al. Reduction in immunosuppression as initial therapy for posttransplant lymphoproliferative disorder: analysis of prognostic variables and long-term follow-up of 42 adult patients. Transplantation 2001 ; 7 1 (8): 1 076.
26. Niedermeyer J, Hoffmeyer F, Hertenstein B, Hoeper MM, Fabel H. Treatment of lympho-proliferative disease with rituximab. Lancet 2000; 355 (9202): 499.
27. Verschuuren EA, Stevens SJ, van Imhoff GW, et al. Treatment of posttransplant lymphoproliferative disease with rituximab: the remission, the relapse, and the complication. Transplantation 2002; 73 ( 1 ): 1 00.
28. Palmer SM, Jr., Henshaw NG, Howell DN, Miller SE, Davis RD, Tapson VF. Community respiratory viral infection in adult lung transplant recipients. Chest 1 998; 1 13 (4): 944.
1 1 6

- References -
29. Billings JL, Hertz MI, Wendt CH. Community respiratory virus infections following lung transplantation. Transpl Infect Dis 2001; 3 (3): 138.
30. Billings JL, Hertz MI, Savik K, Wendt CH. Respiratory viruses and chronic rejection in lung transplant recipients. J Heart Lung Transplant 2002; 21 (5): 559.
31. Chakinala MM, Trulock EP. Acute allograft rejection after lung transplantation: diagnosis and therapy. Chest Surg Clin N Am 2003; 13 (3): 525.
32. Yousem SA, Berry GJ, Cagle PT, et al. Revision of the 1990 working formulation for the classification of pulmonary allograft rejection: Lung Rejection Study Group. J Heart Lung Transplant 1996; 15 (1 Pt 1): 1.
33. Burke CM, Theodore J, Dawkins KD, et al. Post-transplant obliterative bronchiolitis and other late lung sequelae in human heart-lung transplantation. Chest 1984; 86 (6): 824.
34. Estenne M, Hertz MI. Bronchiolitis obliterans after human lung transplantation. Am J Respir Crit Care Med 2002; 166 (4): 440.
35. Boehler A, Estenne M. Post-transplant bronchiolitis obliterans. Eur Respir J 2003; 22 (6): 1007.
36. Valentine VG, Robbins RC, Berry GJ, et al. Actuarial survival of heart-lung and bilateral sequential lung transplant recipients with obliterative bronchiolitis. J Heart Lung Transplant 1996; 15 ( 4 ): 3 71.
37. Boehler A, Kesten S, Weder W, Speich R. Bronchiolitis obliterans after lung transplantation: a review. Chest 1998; 114 (5): 1411.
38. Cooper JD, Billingham M, Egan T, et al. A working formulation for the standardization of nomenclature and for clinical staging of chronic dysfunction in lung allografts. International Society for Heart and Lung Transplantation. J Heart Lung Transplant 1993; 12 (5): 7 13.
1 1 7

- References -
39. Estenne M, Maurer JR, Boehler A, et al. Bronchiolitis obliterans syndrome 2001: an update of the diagnostic criteria. J Heart Lung Transplant 2002; 21 (3): 297.
40. Corris PA. Lung transplantation. Bronchiolitis obliterans syndrome. Chest Surg Clin N Am 2003; 13 (3): 543.
41. Scott AI, Sharples LD, Stewart S. Bronchiolitis obliterans syndrome: risk factors and therapeutic strategies. Drugs 2005; 65 (6): 761.
42. Yousem SA, Burke CM, Billingham ME. Pathologic pulmonary alterations in long-term human heart-lung transplantation. Hum Pathol 1985; 16 (9): 911.
43. Yousem SA, Paradis IL, Dauber JH, et al. Pulmonary arteriosclerosis in long-term human heart-lung transplant recipients. Transplantation 1989; 47 (3): 564.
44. van den Berg JWK. Allograft vasculopathy precedes bronchiolitis obliterans syndrome after lung transplantation. In: Thesis, Bronchiolitis obliterans syndrome after lung transplantation, 2000: 111.
45. de Perrot M, Liu M, Waddell TK, Keshavjee S. Ischemiareperfusion-induced lung injury. Am J Respir Crit Care Med 2003; 167 (4): 490.
46. Hirt SW, You XM, Moller F, et al. The influence of ischemia on the severity of chronic rejection in a rat lung transplant model. Transplant Proc 1999; 31 (1-2): 189.
47. Fiser SM, Tribble CG, Long SM, et al. Ischemia-reperfusion injury after lung transplantation increases risk of late bronchiolitis obliterans syndrome. Ann Thorac Surg 2002; 73 (4): 1041.
48. Novitzky D, Wicomb WN, Cooper DK, Rose AG, Fraser RC, Barnard CN. Electrocardiographic, hemodynamic & endocrine changes occuring during experimental brain death in the chacma baboon. J Heart Transplant 1984; 4: 63.
1 1 8

- References -
49. Herijgers P, Leunens V, Tjandra-Maga TB, Mubagwa K, Flameng W. Changes in organ perfusion after brain death in the rat and its relation to circulating catecholamines. Transplantation 1996; 62 (3): 330.
50. Chen EP, Bittner HB, Kendall SW, Van Trigt P. Hormonal and hemodynamic changes in a validated animal model of brain death. Crit Care Med 1996; 24 (8): 1352.
51. Cooper DK, Novitzky D, Wicomb WN. The pathophysiological effects of brain death on potential donor organs, with particular reference to the heart. Ann R Coll Surg Engl 1989; 71 (4): 261.
52. Shivalkar B, Van Loon J, Wieland W, et al. Variable effects of explosive or gradual increase of intracranial pressure on myocardial structure and function. Circulation 1993; 87 (1): 230.
53. Fisher AJ, Donnelly SC, Hirani N, et al. Enhanced pulmonary inflammation in organ donors following fatal non-traumatic brain injury. Lancet 1999; 353 (9162): 1412.
54. Takada M, Nadeau KC, Hancock WW, et al. Effects of explosive brain death on cytokine activation of peripheral organs in the rat. Transplantation 1998; 65 (12): 1533.
55. van der Hoeven JA, Ploeg RJ, Postema F, et al. Induction of organ dysfunction and up-regulation of inflammatory markers in the liver and kidneys of hypotensive brain dead rats: a model to study marginal organ donors. Transplantation 1999; 68 ( 12): 1884.
56. van Der Hoeven JA, Ter Horst GJ, Molema G, et al. Effects of brain death and hemodynamic status on function and immunologic activation of the potential donor liver in the rat. Ann Surg 2000; 232 (6): 804.
57. Avlonitis VS, Fisher AJ, Kirby JA, Dark rn. Pulmonary transplantation: the role of brain death in donor lung injury. Transplantation 2003; 75 (12): 1928.
1 19

- References
58 . Wilhelm MJ, Pratschke J, Beato F, et al. Activation of the heart by donor brain death accelerates acute rejection after transplantation. Circulation 2000; 102 ( 19) : 2426.
59. Pratschke J, Wilhelm MJ, Kusaka M, et al. Accelerated rejection of renal allografts from brain-dead donors. Ann Surg 2000; 232 (2): 263 .
60. Cainelli F, Vento S. Infections and solid organ transplant rejection: a cause-and-effect relationship? Lancet Infect Dis 2002; 2 (9) : 539.
6 1 . Keenan RJ, Lega ME, Dummer JS, et al. Cytomegalovirus serologic status and postoperative infection correlated with risk of developing chronic rejection after pulmonary transplantation. Transplantation 1 99 1 ; 5 1 (2): 433 .
62. Keller CA, Cagle PT, Brown RW, Noon G, Frost AE. Bronchiolitis obliterans in recipients of single, double, and heart-lung transplantation. Chest 1 995; 1 07 (4) : 973 .
63 . Humar A, Gillingham KJ, Payne WD, Dunn DL, Sutherland DE, Matas AJ. Association between cytomegalovirus disease and chronic rejection in kidney transplant recipients. Transplantation 1 999; 68 ( 1 2) : 1 879.
64. Koskinen PK, Nieminen MS, Krogerus LA, et al. Cytomegalovirus infection accelerates cardiac allograft vasculopathy: correlation between angiographic and endomyocardial biopsy findings in heart transplant patients. Transpl Int 1 993; 6 (6) : 34 1 .
65. Ettinger NA, Bailey TC, Trulock EP, et al. Cytomegalovirus infection and pneumonitis. Impact after isolated lung transplantation. Washington University Lung Transplant Group. Am Rev Respir Dis 1993; 1 47 (4): 1 0 1 7.
66. Luckraz H, Sharples L, McNeil K, Wreghitt T, Wallwork J. Cytomegalovirus antibody status of donor/recipient does not influence the incidence of bronchiolitis obliterans syndrome in lung transplantation. J Heart Lung Transplant 2003; 22 (3): 287.
120

- References -
67. Vilchez RA, McCurry K, Dauber J, et al. The epidemiology of parainfluenza virus infection in lung transplant recipients. Clin Infect Dis 200 1 ; 33 ( 12): 2004.
68. Vilchez R, McCurry K, Dauber J, et al. Influenza and parainfluenza respiratory viral infection requiring admission in adult lung transplant recipients. Transplantation 2002; 73 (7): 1 075 .
69. Arnold R, Humbert B, Werchau H, Gallati H, Konig W. Interleukin-8, interleukin-6, and soluble tumour necrosis factor receptor type I release from a human pulmonary epithelial cell line (A549) exposed to respiratory syncytial virus. Immunology 1 994; 82 ( 1 ): 1 26.
70. Subauste MC, Jacoby DB, Richards SM, Proud D. Infection of a human respiratory epithelial cell line with rhinovirus. Induction of cytokine release and modulation of susceptibility to infection by cytokine exposure. J Clin Invest 1 995; 96 ( 1 ) : 549.
7 1 . Matsukura S, Kokubu F, Noda H, Tokunaga H, Adachi M. Expression of IL-6, IL-8, and RANTES on human bronchial epithelial cells, NCI-H292, induced by influenza virus A. J Allergy Clin Immunol 1 996; 98 (6 Pt 1 ) : 1 080.
72. Skoner DP, Gentile DA, Patel A, Doyle WJ. Evidence for cytokine mediation of disease expression in adults experimentally infected with influenza A virus. J Infect Dis 1 999; 1 80 ( 1 ): 1 0.
73 . Husain S, Singh N. Bronchiolitis obliterans and lung transplantation: evidence for an infectious etiology. Semin Respir Infect 2002; 1 7 (4): 3 1 0.
74. Vilchez RA, Dauber J, Kusne S. Infectious etiology of bronchiolitis obliterans: the respiratory viruses connection - myth or reality? Am J Transplant 2003 ; 3 (3): 245 .
75 . Khalifah AP, Hachem RR, Chakinala MM, et al. Respiratory viral infections are a distinct risk for bronchiolitis obliterans syndrome and death. Am J Respir Crit Care Med 2004; 170 (2): 1 8 1 .
121

- References
76. Le Moine A, Goldman M, Abramowicz D. Multiple pathways to allograft rejection. Transplantation 2002; 73 (9): 1373.
77. De Hoyos A, Chamberlain D, Schvartzman R, et al. Prospective assessment of a standardized pathologic grading system for acute rejection in lung transplantation. Chest 1993; 103 (6): 1813.
78. Hopkins PM, Aboyoun CL, Chhajed PN, et al. Prospective analysis of 1,235 transbronchial lung biopsies in lung transplant recipients. J Heart Lung Transplant 2002; 21 (10): 1062.
79. Banda K, Paradis IL, Simila S, et al. Obliterative bronchiolitis after lung and heart-lung transplantation. An analysis of risk factors and management. J Thorac Cardiovasc Surg 1995; 110 (1): 4.
80. Kroshus TJ, Kshettry VR, Savik K, John R, Hertz MI, Bolman RM, 3rd. Risk factors for the development of bronchiolitis obliterans syndrome after lung transplantation. J Thorac Cardiovasc Surg 1997; 114 (2): 195.
81. Husain AN, Siddiqui MT, Holmes EW, et al. Analysis of risk factors for the development of bronchiolitis obliterans syndrome. Am J Respir Crit Care Med 1999; 159 (3): 829.
82. Sharples LD, McNeil K, Stewart S, Wallwork J. Risk factors for bronchiolitis obliterans: a systematic review of recent publications. J Heart Lung Transplant 2002; 21 (2): 271.
83. Boehler A, Chamberlain D, Kesten S, Slutsky AS, Liu M, Keshavjee S. Lymphocytic airway infiltration as a precursor to fibrous obliteration in a rat model of bronchiolitis obliterans. Transplantation 1997; 64 (2): 311.
84. Adams BF, Brazelton T, Berry GJ, Morris RE. The role of respiratory epithelium in a rat model of obliterative airway disease. Transplantation 2000; 69 (4): 661.
122

- References -
85. Hele DJ, Yacoub MH, Belvisi MG. The heterotopic tracheal allograft as an animal model of obliterative bronchiolitis. Respir Res 2001; 2 (3): 169.
86. Hertz MI, Jessurun J, King MB, Savik SK, Murray JJ. Reproduction of the obliterative bronchiolitis lesion after heterotopic transplantation of mouse airways. Am J Pathol 1993; 142 ( 6): 1945.
87. King MB, Pedtke AC, Levrey-Hadden HL, Hertz MI. Obliterative airway disease progresses in heterotopic airway allografts without persistent alloimmune stimulus. Transplantation 2002; 74 (4): 557.
88. Uusitalo MH, Salminen US, Ikonen TS, et al. Alloimmune injury preceding airway obliteration in porcine heterotopic lung implants: a histologic and immunohistologic study. Transplantation 1999; 68 (7): 970.
89. Qu N, de Vos P, Schelfhorst M, de Haan A, Timens W, Prop J. Integrity of airway epithelium is essential against obliterative airway disease in transplanted rat tracheas. J Heart Lung Transplant 2005; 24 (7): 882.
90. Ikonen TS, Brazelton TR, Berry GJ, Shorthouse RS, Morris RE. Epithelial re-growth is associated with inhibition of obliterative airway disease in orthotopic tracheal allografts in nonimmunosuppressed rats. Transplantation 2000; 70 (6): 857.
91. Neuringer IP, Mannon RB, Coffman TM, et al. Immune cells in a mouse airway model of obliterative bronchiolitis. Am J Respir Cell Mol Biol 1998; 19 (3): 379.
92. Neuringer IP, Walsh SP, Mannon RB, Gabriel S, Aris RM. Enhanced T cell cytokine gene expression in mouse airway obliterative bronchiolitis. Transplantation 2000; 69 (3): 399.
93. Higuchi T, Jaramillo A, Kaleem Z, Patterson GA, Mohanakumar T. Different kinetics of obliterative airway disease development in heterotopic murine tracheal allografts induced by CD4+ and CD8+ T cells. Transplantation 2002; 74 (5): 646.
123

- References -
94. Boehler A, Bai XH, Liu M, et al. Upregulation of T-helper 1 cytokines and chemokine expression in post-transplant airway obliteration. Am J Respir Crit Care Med 1999; 159 (6): 1910.
95. Suga M, Maclean AA, Keshavjee S, Fischer S, Moreira JM, Liu M. RANTES plays an important role in the evolution of allograft transplant-induced fibrous airway obliteration. Am J Respir Crit Care Med 2000; 162 (5): 1940.
96. Farivar AS, Krishnadasan B, Naidu BV, Woolley SM, Mulligan MS. The role of the beta chemokines in experimental obliterative bronchiolitis. Exp Mol Pathol 2003; 75 (3): 2 10.
97. Ikonen T, Uusitalo M, Taskinen E, et al. Small airway obliteration in a new swine heterotopic lung and bronchial allograft model. J Heart Lung Transplant 1998; 17 (10): 945.
98. Maasilta P, Salminen US, Taskinen E, Hietala EM, Ikonen T, Harjula A. Obliterative airway disease in a porcine heterotopic bronchial allograft model. Transpl Int 2000; 13 (3): 2 18.
99. Maasilta PK, Salminen US, Lautenschlager IT, Taskinen EI, Harjula AL. Immune cells and immunosuppression in a porcine bronchial model of obliterative bronchiolitis. Transplantation 2001; 72 (6): 998.
100. al-Dossari GA, Kshettry VR, Jessurun J, Bolman RM, 3rd. Experimental large-animal model of obliterative bronchiolitis after lung transplantation. Ann Thorac Surg 1994; 58 (1): 34.
101. Marek KW, Wildevuur CR. Lung transplantation in the rat: I. Technique and survival. Ann Thorac Surg 1982; 34 (1): 74.
102. Prop J, Nieuwenhuis P, Wildevuur CR. Lung allograft rejection in the rat. I. Accelerated rejection caused by graft lymphocytes. Transplantation 1985; 40 ( 1): 25.
124

- References -
103. Tazelaar HD, Prop J, Nieuwenhuis P, Billingham ME, Wildevuur CR. Airway pathology in the transplanted rat lung. Transplantation 1988; 45 (5): 864.
104. Matsumura Y, Marchevsky A, Zuo XJ, Kass RM, Matloff JM, Jordan SC. Assessment of pathological changes associated with chronic allograft rejection and tolerance in two experimental models of rat lung transplantation. Transplantation 1995; 59 (11): 1509.
105. Hirt SW, You XM, Moller F, et al. Development of obliterative bronchiolitis after allogeneic rat lung transplantation: implication of acute rejection and the time point of treatment. J Heart Lung Transplant 1999; 18 (6): 542.
106. Yasufuku K, Heidler KM, Woods KA, et al. Prevention of bronchiolitis obliterans in rat lung allografts by type V collageninduced oral tolerance. Transplantation 2002; 73 (4): 500.
107. Hertz MI, Taylor DO, Trulock EP, et al. The registry of the international society for heart and lung transplantation: nineteenth official report-2002. J Heart Lung Transplant 2002; 21 (9): 950.
I 08. Starnes VA, Woo MS, MacLaughlin EF, et al. Comparison of outcomes between living donor and cadaveric lung transplantation in children. Ann Thorac Surg 1999; 68 (6): 2279.
109. Woo MS, MacLaughlin EF, Hom MV, Szmuszkovicz JR, Barr ML, Starnes VA. Bronchiolitis obliterans is not the primary cause of death in pediatric living donor lobar lung transplant recipients. J Heart Lung Transplant 2001; 20 (5): 491.
110. Prop J, Ehrie MG, Crapo JD, Nieuwenhuis P, Wildevuur CR. Reimplantation response in isografted rat lungs. Analysis of causal factors. J Thorac Cardiovasc Surg 1984; 87 (5): 702.
111. Segel LD, vonHaag DW, Zhang J, Follette DM. Selective overexpression of inflammatory molecules in hearts from brain-dead rats. J Heart Lung Transplant 2002; 21 (7): 804.
125

- References
112. Pratschke J, Wilhelm MJ, Laskowski I, et al. Influence of donor brain death on chronic rejection of renal transplants in rats. J Am Soc Nephrol 2001; 12 (11): 2474.
113. Hayashi M, Martinez OM, Garcia-Kennedy R, So S, Esquivel CO, Krams SM. Expression of cytokines and immune mediators during chronic liver allograft rejection. Transplantation 1995; 60 (12): 1533.
114. Nadeau KC, Azuma H, Tilney NL. Sequential cytokine dynamics in chronic rejection of rat renal allografts: roles for cytokines RANTES and MCP-1. Proc Natl Acad Sci U S A 1995; 92 (19): 8729.
115. Kouwenhoven EA, JN IJ, de Bruin RW. Etiology and pathophysiology of chronic transplant dysfunction. Transpl Int 2000; 13 (6): 385.
1 16. Hayry P, Isoniemi H, Yilmaz S, et al. Chronic allograft rejection. Immunol Rev 1993; 134: 33.
117. Winter JB, Gouw AS, Groen M, Wildevuur C, Prop J. Respiratory viral infections aggravate airway damage caused by chronic rejection in rat lung allografts. Transplantation 1994; 57 (3): 418.
118. Uyama T, Winter JB, Groen G, Wildevuur CR, Monden Y, Prop J. Late airway changes caused by chronic rejection in rat lung allografts. Transplantation 1992; 54 (5): 809.
119. Gudmundsdottir H, Turka LA. T cell costimulatory blockade: new therapies for transplant rejection. J Am Soc Nephrol 1999; 10 (6): 1356.
120. Wekerle T, Kurtz J, Bigenzahn S, Takeuchi Y, Sykes M. Mechanisms of transplant tolerance induction using costimulatory blockade. Curr Opin Immunol 2002; 14 (5): 592.
126

- References -
121. Schmidt H, Filantenkov A, Reutzel-Selke A, et al. Adoptive transfer of regulatory T cells following chronic allograft rejection induces tolerance for secondary allografts. Transplant Proc 2002; 34 (7): 2893.
122. Kawai M, Kitade H, Mathieu C, Waer M, Pirenne J. Inhibitory and stimulatory effects of cyclosporine A on the development of regulatory T cells in vivo. Transplantation 2005; 79 (9): 1073.
123. Zuo XJ, Matsumura Y, Prehn J, et al. Cytokine gene expression in rejecting and tolerant rat lung allograft models: analysis by RT-PCR. Transpl Immunol 1995; 3 (2): 151.
124. Kingsley CI, Karim M, Bushell AR, Wood KJ. CD25+CD4+ regulatory T cells prevent graft rejection: CTLA-4- and IL- I 0-dependent immunoregulation of alloresponses. J Immunol 2002; 168 (3): 1080.
125. Josien R, Douillard P, Guillot C, et al. A critical role for transforming growth factor-beta in donor transfusion-induced allograft tolerance. J Clin Invest 1998; 102 (11 ): 1920.
126. Punch JD, Tono T, Qin L, Bishop DK, Bromberg JS. Tolerance induction by anti-CO2 plus anti-CD3 monoclonal antibodies: evidence for an IL-4 requirement. J Immunol 1998; 161 (3): 1 156
127. Welsh RM, Markees TG, Woda BA, et al. Virus-induced abrogation of transplantation tolerance induced by donor-specific transfusion and anti-CD154 antibody. J Virol 2000; 74 (5): 2210.
128. Williams MA, Onami TM, Adams AB, et al. Cutting edge: persistent viral infection prevents tolerance induction and escapes immune control following CD28/CD40 blockade-based regimen. J Immunol 2002; 169 ( 10): 5387.
129. Romaniuk A, Prop J, Petersen AH, Wildevuur CR, Nieuwenhuis P. Expression of class II major histocompatibility complex antigens by bronchial epithelium in rat lung allografts. Transplantation 1987; 44 (2): 209.
1 27

- References -
130. Hall BM, Pearce NW, Gurley KE, Dorsch SE. Specific unresponsiveness in rats with prolonged cardiac allograft survival after treatment with cyclosporine. III. Further characterization of the CD4+ suppressor cell and its mechanisms of action. J Exp Med 1990; 171 (1): 141.
131. Meloni F, Vitulo P, Bianco AM, et al. Regulatory CD4+CD25+ T cells in the peripheral blood of lung transplant recipients: correlation with transplant outcome. Transplantation 2004; 77 (5): 762.
132. Zhou J, Carr RI, Liwski RS, Stadnyk AW, Lee TD. Oral exposure to alloantigen generates intragraft CD8+ regulatory cells. J Immunol 2001; 167 (1): 107.
133. Sundaresan S, Alevy YG, Steward N, et al. Cytokine gene transcripts for tumor necrosis factor-alpha, interleukin-2, and interferon-gamma in human pulmonary allografts. J Heart Lung Transplant 1995; 14 (3): 512.
134. Dai Z, Lakkis FG. The role of cytokines, CTLA-4 and costimulation in transplant tolerance and rejection. Curr Opin Immunol 1999; 11 (5): 504.
135. Pirenne J, Kitade H, Kawai M, et al. Regulatory cells, TH1/TH2 unbalance, and antibody-induced chronic rejection in operational tolerance induced by donor-specific blood transfusion. Transplantation 2005; 79 (3 Suppl): S25.
136. Rowshani AT, Florquin S, Bemelman F, Kummer JA, Hack CE, Ten Berge IJ. Hyperexpression of the granzyme B inhibitor PI-9 in human renal allografts: a potential mechanism for stable renal function in patients with subclinical rejection. Kidney Int 2004; 66 (4): 1417.
137. Borchers AT, Perez R, Kaysen G, Ansari AA, Gershwin ME. Role of cytomegalovirus infection in allograft rejection: a review of possible mechanisms. Transpl Immunol 1999; 7 (2): 75.
1 28

- References -
138. Lautenschlager I, Soots A, Krogerus L, et al. Effect of cytomegalovirus on an experimental model of chronic renal allograft rejection under triple-drug treatment in the rat. Transplantation 1997; 64 (3): 391.
139. Lemstrom K, Koskinen P, Krogerus L, Daemen M, Bruggeman C, Hayry P. Cytomegalovirus antigen expression, endothelial cell proliferation, and intimal thickening in rat cardiac allografts after cytomegalovirus infection. Circulation 1995; 92 (9): 2594.
140. Koskinen PK, Kallio EA, Bruggeman CA, Lemstrom KB. Cytomegalovirus infection enhances experimental obliterative bronchiolitis in rat tracheal allografts. Am J Respir Crit Care Med 1997; 155 (6): 2078.
141. Johnson PC, Lewis RM, Golden DL, et al. The impact of cytomegalovirus infection on seronegative recipients of seropositive donor kidneys versus seropositive recipients treated with cyclosporine-prednisone immunosuppression. Transplantation 1988; 45 (1): 116.
142. Sharples LD, Caine N, Mullins P, et al. Risk factor analysis for the major hazards following heart transplantation--rejection, infection, and coronary occlusive disease. Transplantation 1991; 52 (2) : 244.
143. van Dam JG, Damoiseaux JG, Van der Heijden HA, Grauls G, Van Breda Vriesman PJ, Bruggeman CA. Infection with rat cytomegalovirus (CMV) in the immunocompromised host is associated with the appearance of a T cell population with reduced CD8 and T cell receptor (TCR) expression. Clin Exp Immunol 1997; 110 (3): 349.
144. van Dam JG, Damoiseaux JG, Christiaans MH, Bruggeman CA. Acute primary infection with cytomegalovirus (CMV) in kidney transplant recipients results in the appearance of a phenotypically aberrant CD8+ T cell population. Microbiol Immunol 2000; 44 (12): 1011.
129

- References -
145. Kuijpers TW, Vossen MT, Gent MR, et al. Frequencies of circulating cytolytic, CD45RA+CD27-, CD8+ T lymphocytes depend on infection with CMV. J Immunol 2003 ; 1 70 (8): 4342.
146. Craigen JL, Grundy JE. Cytomegalovirus induced up-regulation of LFA-3 (CD58) and ICAM-1 (CD54) is a direct viral effect that is not prevented by ganciclovir or foscamet treatment. Transplantation 1996; 62 (8): 1 102.
1 47. Waldman WJ, LeClaire JD, Knight DA. T-cell activation response to allogeneic CMV-infected endothelial cells is not prevented by ganciclovir or foscamet: implications for transplant vascular sclerosis. Transplantation 2002; 73 (2): 3 14.
148. Yagyu K, Steinhoff G, Duijvestijn AM, Bruggeman CA, Matsumoto H, van Breda Vriesman PJ. Reactivation of rat cytomegalovirus in lung allografts: an experimental and immunohistochemical study in rats. J Heart Lung Transplant 1 992; 1 1 ( 6): 1 03 1 .
1 49. Balthesen M, Messerle M, Reddehase MJ. Lungs are a major organ site of cytomegalovirus latency and recurrence. J Virol 1 993 ; 67 (9): 5360.
1 50. Reinke P, Prosch S, Kem F, Volk HD. Mechanisms of human cytomegalovirus (HCMV) (re)activation and its impact on organ transplant patients. Transpl Infect Dis 1999; 1 (3): 1 57.
1 5 1 . Bruggeman CA, Debie WM, Grauls G, Majoor G, van Boven CP. Infection of laboratory rats with a new cytomegalo-like virus. Arch Virol 1 983; 76 (3): 1 89.
1 52. Ross PS, Van Loveren H, de Swart RL, et al. Host resistance to rat cytomegalovirus (RCMV) and immune function in adult PVG rats fed herring from the contaminated Baltic Sea. Arch Toxicol 1 996; 70 (1 0): 661 .
130

- References
153. van der Werf N, Hillebrands JL, Klatter FA, Bos I, Bruggeman CA, Rozing J. Cytomegalovirus infection modulates cellular immunity in an experimental model for autoimmune diabetes. Clin Dev Immunol 2003; 10 (2-4): 153.
154. Bukowski JF, Woda BA, Welsh RM. Pathogenesis of murine cytomegalovirus infection in natural killer cell-depleted mice. J Virol 1984; 52 (1): 119.
155. Biron CA, Byron KS, Sullivan JL. Severe herpesvirus infections in an adolescent without natural killer cells. N Engl J Med 1989; 320 (26): 1731.
156. Dokun AO, Chu DT, Yang L, Bendelac AS, Yokoyama WM. Analysis of in situ NK cell responses during viral infection. J Immunol 2001; 167 (9): 5286.
157. Nguyen KB, Salazar-Mather TP, Dalod MY, et al. Coordinated and distinct roles for IFN-alpha beta, IL-12, and IL-1 5 regulation of NK cell responses to viral infection. J Immunol 2002; 169 (8): 4279.
158. Eloranta ML, Sandberg K, Alm GV. The interferon-alpha/beta responses of mice to herpes simplex virus studied at the blood and tissue level in vitro and in vivo. Scand J Immunol 1996; 43 (4): 356.
159. Bogdan C. The function of type I interferons in antimicrobial immunity. Curr Opin Immunol 2000; 12 (4): 419.
160. Durbin JE, Fernandez-Sesma A, Lee CK, et al. Type I IFN modulates innate and specific antiviral immunity. J Immunol 2000; 164 (8): 4220.
161. Mattei F, Schiavoni G, Belardelli F, Tough DF. IL- 15 is expressed by dendritic cells in response to type I IFN, double-stranded RNA, or lipopolysaccharide and promotes dendritic cell activation. J Immunol 2001; 167 (3): 1179.
1 3 1

- References
162. Carson WE, Giri JG, Lindemann MJ, et al. Interleukin (IL) 15 is a novel cytokine that activates human natural killer cells via components of the IL-2 receptor. J Exp Med 1994; 180 (4): 1395.
163. Petersson E, Hedlund G. Proliferation and differentiation of alloselective NK cells after alloimmunization-evidence for an adaptive NK response. Cell Immunol 1999; 197 (1): 10.
164. Petersson E, Holmdahl R, Butcher GW, Hedlund G. Activation and selection of NK cells via recognition of an allogeneic, non-classical MHC class I molecule, RTl -E. Eur J Immunol 1999; 29 (11): 3663.
165. Beijleveld LJ, Groen H, Broeren CP, et al. Susceptibility to clinically manifest cyclosporine A (CsA)-induced autoimmune disease is associated with interferon-gamma (IFN-gamma)producing CD45RC+RT6- T helper cells. Clio Exp Immunol 1996; 105 (3): 486.
166. Hylkema MN, van der Deen M, Pater JM, Kampinga J, Nieuwenhuis P, Groen H. Single expression of CD45RC and RT6 in correlation with T-helper 1 and T-helper 2 cytokine patterns in the rat. Cell Immunol 2000; 199 (2): 89.
167. Groh V, Rhinehart R, Randolph-Habecker J, Topp MS, Riddell SR, Spies T. Costimulation of CD8alphabeta T cells by NKG2D via engagement by MIC induced on virus-infected cells. Nat Immunol 2001; 2 (3): 255.
168. Berg SF, Dissen E, Westgaard IH, Fossum S. Molecular characterization of rat NKR-P2, a lectin-like receptor expressed by NK cells and resting T cells. Int Immunol 1998; 10 (4): 379.
169. Sharples LD, Tamm M, McNeil K, Higenbottam TW, Stewart S, Wallwork J. Development of bronchiolitis obliterans syndrome in recipients of heart-lung transplantation--early risk factors. Transplantation 1996; 61 (4): 560.
132

- References
170. Bando K, Paradis IL, Komatsu K, et al. Analysis of time-dependent risks for infection, rejection, and death after pulmonary transplantation. J Thorac Cardiovasc Surg 1995; 109 (1): 49.
171. Heng D, Sharples LD, McNeil K, Stewart S, Wreghitt T, Wallwork J. Bronchiolitis obliterans syndrome: incidence, natural history, prognosis, and risk factors. J Heart Lung Transplant 1998; 17 (12): 1255.
172. Orloff SL, Strehlow DN, Soderberg-Naucler C, et al. Elimination of donor-specific alloreactivity prevents cytomegalovirus-accelerated chronic rejection in rat small bowel and heart transplants. Transplantation 2002; 73 (5): 679.
173. Helantera I, Koskinen P, Tornroth T, Loginov R, Gronhagen-Riska C, Lautenschlager I. The impact of cytomegalovirus infections and acute rejection episodes on the development of vascular changes in 6-month protocol biopsy specimens of cadaveric kidney allograft recipients. Transplantation 2003; 75 (11 ): 1858.
174. Hamann D, Roos MT, van Lier RA. Faces and phases of human CD8 T-cell development. Immunol Today 1999; 20 (4): 177.
175. Raulet DH. Roles of the NKG2D immunoreceptor and its ligands. Nat Rev Immunol 2003; 3 (10): 781.
176. van der Bij W, Torensma R, van Son WJ, et al. Rapid immunodiagnosis of active cytomegalovirus infection by monoclonal antibody staining of blood leucocytes. J Med Virol 1988; 25 (2): 179.
177. de Haan A, van der Gun I, Hepkema BG, et al. Decreased donorspecific cytotoxic T cell precursor frequencies one year after clinical lung transplantation do not reflect transplantation tolerance: a companson of lung transplant recipients with or without bronchiolitis obliterans syndrome. Transplantation 2000; 69 (7): 1434.
133

- References -
1 78 . Gamadia LE, Rentenaar RJ, Baars PA, et al. Differentiation of cytomegalovirus-specific CD8( +) T cells in healthy and immunosuppressed virus carriers. Blood 200 1 ; 98 (3): 754.
179. Sinzger C, Knapp J, Plachter B, Schmidt K, Jahn G. Quantification of replication of clinical cytomegalovirus isolates in cultured endothelial cells and fibroblasts by a focus expansion assay. J Virol Methods 1 997; 63 (1 -2): 1 03 .
1 80. Alves NL, Hooibrink B, Arosa FA, van Lier RA. IL- 1 5 induces antigen-independent expansion and differentiation of human naive CD8+ T cells in vitro. Blood 2003; 1 02 (7): 254 1 .
1 8 1 . Appay V, Dunbar PR, Callan M , et al. Memory CD8+ T cells vary in differentiation phenotype in different persistent virus infections. Nat Med 2002; 8 (4): 379.
1 82. Yagyu K, Takeshita M, Otsuka T, Kubota H, Furuse A, van Breda Vriesman PJ. Reactivation of latent cytomegalovirus in allografts: comparison of lung graft and kidney graft in rats. Transplant Proc 1 994; 26 (4): 2343 .
1 83 . Tamura K, Oka T, Ohsawa K, e t al. Allogeneic cell stimulation enhances cytomegalovirus replication in the early period of primary infection in an experimental rat model. J Heart Lung Transplant 2003 ; 22 (4): 452.
1 84. Kem F, Surel IP, Faulhaber N, et al. Target structures of the CD8( + )-T-cell response to human cytomegalovirus: the 72-kilodalton major immediate-early protein revisited. J Virol l 999; 73 ( 1 0) : 8 1 79.
1 85 . Greijer AE, Verschuuren EA, Harmsen MC, et al. Direct quantification of human cytomegalovirus immediate-early and late mRNA levels in blood of lung transplant recipients by competitive nucleic acid sequence-based amplification. J Clin Microbiol 200 l ; 39 ( 1 ) : 25 1 .
1 34

- References -
186. Tikkanen JM, Kallio EA, Bruggeman CA, Koskinen PK, Lemstrom KB. Prevention of cytomegalovirus infection-enhanced experimental obliterative bronchiolitis by antiviral prophylaxis or immunosuppression in rat tracheal allografts. Am J Respir Crit Care Med 2001; 164 (4): 672.
187. Bonatti H, Tabarelli W, Ruttmann E, et al. Impact of cytomegalovirus match on survival after cardiac and lung transplantation. Am Surg 2004; 70 (8): 710.
188. Perreas KG, McNeil K, Charman S, Sharples LD, Wreghitt T, Wallwork J. Extended ganciclovir prophylaxis in lung transplantation. J Heart Lung Transplant 2005; 24 (5): 583.
189. Tomiyama H, Takata H, Matsuda T, Takiguchi M. Phenotypic classification of human CD8+ T cells reflecting their function: inverse correlation between quantitative expression of CD27 and cytotoxic effector function. Eur J Immunol 2004; 34 (4): 999.
190. Roberts AI, Lee L, Schwarz E, et al. NKG2D receptors induced by IL-15 costimulate CD28-negative effector CTL in the tissue microenvironment. J Immunol 2001; 167 (10): 5527.
191. Zwimer NW, Dole K, Stastny P. Differential surface expression of MICA by endothelial cells, fibroblasts, keratinocytes, and monocytes. Hum Immunol 1999; 60 (4): 323.
192. Somersalo K, Anikeeva N, Sims TN, et al. Cytotoxic T lymphocytes form an antigen-independent ring junction. J Clin Invest 2004; 113 (1): 49.
193. Zwimer NW, Marcos CY, Mirbaha F, Zou Y, Stastny P. Identification of MICA as a new polymorphic alloantigen recognized by antibodies in sera of organ transplant recipients. Hum Immunol 2000; 61 (9): 917.
194. Hankey KG, Drachenberg CB, Papadimitriou JC, et al. MIC expression in renal and pancreatic allografts. Transplantation 2002; 73 (2): 304.
1 35

- References
195. Gasser M, Waaga AM, Kist-Van Holthe JE, et al. Normalization of brain death-induced injury to rat renal allografts by recombinant soluble P-selectin glycoprotein ligand. J Am Soc Nephrol 2002; 13 (7): 1937.
196. Pratschke J, Kofla G, Wilhelm MJ, et al. Improvements in early behavior of rat kidney allografts after treatment of the brain-dead donor. Ann Surg 2001; 234 (6): 732.
197. Kuecuek 0, Mantouvalou L, Klemz R, et al. Significant reduction of proinflammatory cytokines by treatment of the brain-dead donor. Transplant Proc 2005; 37 (1): 387.
198. Follette DM, Rudich SM, Babcock WD. Improved oxygenation and increased lung donor recovery with high-dose steroid administration after brain death. J Heart Lung Transplant 1998; 17 (4): 423.
199. Schnuelle P, Berger S, de Boer J, Persijn G, van der Woude FJ. Effects of catecholamine application to brain-dead donors on graft survival in solid organ transplantation. Transplantation 2001; 72 (3): 455.
200. Adorini L, Giarratana N, Penna G. Pharmacological induction of tolerogenic dendritic cells and regulatory T cells. Semin Immunol 2004; 16 (2): 127.
201. Alvarez J, del Barrio MR, Arias J, et al. Kidney transplantation from non-heart-beating donors: short- and long-term results. Transplant Proc 2002; 34 (7): 2591.
202. Gok MA, Buckley PE, Shenton BK, et al. Long-term renal function in kidneys from non-heart-beating donors: A single-center experience. Transplantation 2002; 74 (5): 664.
203. Arias-Diaz J, Alvarez J, del Barrio MR, Balibrea JL. Non-heartbeating donation: current state of the art. Transplant Proc 2004; 36 (7): 1891.
136

- References -
204. Steen S, Sjoberg T, Pierre L, Liao Q, Eriksson L, Algotsson L. Transplantation of lungs from a non-heart-beating donor. Lancet 2001; 357 (9259): 825.
205. Nunez JR, Varela A, del Rio F, et al. Bipulmonary transplants with lungs obtained from two non-heart-beating donors who died out of hospital. J Thorac Cardiovasc Surg 2004; 127 (1): 297.
206. Van Raemdonck DE, Rega FR, Neyrinck AP, Jannis N, Verleden GM, Lerut TE. Non-heart-beating donors. Semin Thorac Cardiovasc Surg 2004; 16 (4): 309.
207. Mazzone PJ, Mossad SB, Mawhorter SD, Mehta AC, Schilz RJ, Maurer JR. The humeral immune response to influenza vaccination in lung transplant patients. Eur Respir J 2001; 18 ( 6): 971.
208. Hayney MS, Welter DL, Francois M, Reynolds AM, Love RB. Influenza vaccine antibody responses in lung transplant recipients. Prog Transplant 2004; 14 (4): 346.
209. Mazzone PJ, Mossad SB, Mawhorter SD, Mehta AC, Mauer JR. Cell-mediated immune response to influenza vaccination in lung transplant recipients. J Heart Lung Transplant 2004; 23 (10): 1175.
1 37

- Abbreviations
Abbreviations
AEC APC BN BO BOS CF CFSE CMV Con-A COPD CsA dps EBY FCS FEVl HCMV HES HUVEC ICAM-1 IE genes IFN-y IL iNOS i.p. IPF LCMV LEW LFA MAP MCP MHC MIC MoAb NCS NK OAD
3-amino-9-ethyl-carbazole antigen presenting cell Brown Norway bronchiolitis obliterans bronchiolitis obliterans syndrome cystic fibrosis 5-(and-6)-carboxyfluorescein diacetate succinimidyl ester cytomegalovirus Concanavalin-A chronic obstructive pulmonary disease cyclosporin-A desintergrations per second Epstein-Barr virus fetal calf serum forced expiratory volume in one second human cytomegalovirus hydroxyethyl starch human umbilical vein endothelial cell intercellular adhesion molecule- I immediate-early genes interferon-y interleukin inducible nitric oxide synthase intraperitoneal idiopathic pulmonary fibrosis lymphocytic choriomeningitis virus Lewis leukocyte function-associated antigen mean arterial pressure monocyte chemotactic protein major histocompatibility complex MHC class I related chain monoclonal antibody newborn calf serum natural killer obliterative airway disease
138

PBMNC PBS PCR pfu PI-9 PMN PPH pp65 PTLD RANTES RCMV REF RPMI RT-PCR TCID TCR TGF-� TNF-a VCAM-1 WKY
- Abbreviations -
peripheral blood mononuclear cell phosphate buffered saline polymerase chain reaction plaque forming units protease inhibitor 9 polymorphonuclear primary pulmonary hypertension phosphoprotein 65 post-transplant lymphoproliferative disease regulated on activation, normal T cell expressed and secreted rat cytomegalovirus rat embryonic fibroblast Roswell Park Memorial Institute, culture medium reverse transcriptase-polymerase chain reaction tissue culture infectious dose T cell receptor transforming growth factor-� tumor necrosis factor-a vascular cell adhesion molecule- I Wistar Kyoto
139

- Dankwoord
Dankwoord
Het heeft even geduurd, maar uiteindelijk is het dan toch zover. Het boekje is af en ik ga promoveren! Het onderzoek heb ik natuurlijk niet alleen gedaan en daarom wil ik graag een aantal mensen bedanken in en buiten het lab die een bijdrage hebben geleverd aan de totstandkoming van dit proefschrift.
Allereerst mijn co-promotor en begeleider Jochum Prop. Beste Jochum, bedankt dat ik de mogelijkheid heb gekregen om dit onderzoek te doen en om daarop te kunnen promoveren. Verder wil ik je bedanken voor alle hulp die je hebt geboden tijdens mijn promotieonderzoek.
Verder wil ik Aalzen de Haan bedanken. Beste Aalzen, met je creativiteit en kennis heb je een grote bijdrage geleverd aan het totstandkomen van dit proefschrift. Ik wil je dan ook enorm bedanken voor alle hulp die je hebt geboden bij het onderzoek zoals je ideeen, het opzetten van experimenten, bediscussieren van de resultaten en het corrigeren van mijn proefschrift. Daamaast kon ik altijd bij je binnenlopen voor een vraag of een praatje. Zonder al je hulp had ik het proefschrift niet kunnen afronden.
lk wil mijn promotor Prof. L.F.M.H. de Leij bedanken voor het vertrouwen dat je in me hebt gesteld en verder voor je inbreng en opbouwende kritieken.
Het onderzoek had ik niet kunnen doen zonder hulp te hebben bij het uitvoeren van de longtransplantaties. Arjen, ik wil je dan ook enorm bedanken dat je voor en samen met mij vele uurtjes hebt doorgebracht op het CDL om al die longtransplantaties uit te voeren. Zonder deze transplantaties en je enthousiasme, gezelligheid en opbeurende woorden als er weer een experiment mislukt was, was er geen proefschrift geweest. En naast het werk hebben we regelmatig wat ontspanning gezocht zoals een drankje, etentje of squashen waarbij we over van alles en nog wat gepraat hebben. Dit heb ik als zeer aangenaam ervaren. Hopelijk houden we deze traditie in stand ook na mijn promotie. Arjen, bedankt dat je mij op deze belangrijke dag wilt bijstaan als paranimf.
Ik wil heel graag Paul de Vos bedanken voor de hulp en steun die hij heeft gegeven bij het schrijven van een aantal hoofdstukken. Paul, bedankt dat je me uit de dip hebt weten te halen en mij weer de motivatie hebt gegeven om het proefschrift af te schrijven.
Prof. dr. G.H. Koeter, Prof. dr. C.G.M. Kallenberg en Prof. dr. R.J. Ploeg wil ik graag bedanken voor de beoordeling van mijn proefschrift.
140

- Dankwoord -
Mijn ( ex-) kamergenootjes (Ning, Jasper, Daniel, Susanne, Caroline en Maaike) wil ik allemaal ontzettend bedanken voor jullie steun, gezelligheid, de vele onderzoek-gerelateerde en niet-gerelateerde gesprekken en de kilo's snoep.
Ik wil de mensen op bet kleine lab of die daar gewerkt hebben (Anita, Bart-Jan, Berber, Caba, Douwe, Elinda, Ieneke, Linda, Marian, Marijke, Pamela, Susan en Wijnand) en de rest van de Medische Biologie bedanken voor alle hulp bij het labwerk, de leuke sfeer en voor de ontspanning naast het werk (etentjes, borrelen, labdagen en inline-skaten). Wat uitgebreider wil ik Greetje Groen bedanken voor het kleuren van de vele histologische coupes. Henk Moorlag wil ik bedanken voor het uitvoeren van een aantal immunokleuringen. Verder wil ik Geert Mesander en Henk Moes bedanken voor de hulp bij de FACS analyses. Naomi Werner en Bart de Haan wil ik bedanken voor de hulp op bet DNA-lab en bij de real-time PCR. Jelleke wil ik bedanken voor de ondersteuning bij het kweken. Ingrid Molema wil ik bedanken voor het geven van steun en hulp om door te gaan met mijn onderzoek.
Ik wil de (ex)-AIO's van de Medische Biologie en Klinische Immunologie (Agnieszka, Alja, Andre, Astrid, Caroline, Daniel, Edwin, Eliane, Esther, Hannie, Jan-Stefan, Jasper, Maaike, Machteld, Martine, Monica, Namkje, Sandrine, Shanti en Susanne) bedanken voor de leuke tijd en het delen van de frustraties van het AIO zijn.
Medewerkers van bet CDL, bedankt voor het verzorgen van mijn ratten. Verder wil ik de secretaresses Henriette, Diny en Annet bedanken voor de ondersteuning.
Ik heb het onderzoek niet alleen op het lab van de Medische Biologie gedaan. Daarom wil ik Nienke van de Werf en Flip Klatter bedanken voor de hulp bij de CMV studie. Verder wil ik de mensen van ander labs zoals het DNA-lab, Isotopenlab en Pathologie bedanken voor de hulp bij het onderzoek.
Agnes; bedankt dat je mijn paranimf wilt zijn en natuurlijk oak bedankt voor de gezelligheid de afgelopen jaren. Als een totale vreemdeling in Groningen heb jij me ruim 6 jaar geleden wegwijs gemaakt in Groningen waarbij ik a.a. leuke restaurantjes en kroegjes heb ontdekt. Daamaast heb je altijd een luisterend oor en sta je voor me klaar, bedankt daarvoor.
Tijdens een zogenaamde AIO-borrel wat eigenlijk geen AIO-borrel was, is een kolonistenclubje (Astrid, Elinda, Susan, Jasper en Daniel) ontstaan. Onder het mom van een spelletje lekker kunnen bijkletsen over het lab,

- Dankwoord
onderzoek en andere dingen. Bedankt voor jullie steun, gezelligheid en de vele zakken chips.
lk wil Usha en Willy en de rest van de familie bedanken voor jullie steun en alle goede zorgen. En ja Oma, ik ga eindelijke promoveren waar u het al zo lang over heeft. lk ben er trots op dat ik kan zeggen dat mijn 97-jarige Oma bij mijn promotie is geweest.
lk heh gemerkt dat sporten een erg belangrijke manier is om het werk even te kunnen vergeten. lk wil daarom de mensen van mijn inlinehockeyclub Vikings en Dames 3 team van veldhockey bedanken dat ik mijn werkstress en frustraties kon afreageren door tegen een balletje te slaan tijdens trainingen en wedstrijden.
lk wil al mijn vrienden bedanken voor de nodige ontspanning naast het werk (hockeyen, skaten, etentjes, borrelen, weekendjes weg, concerten, bioscoop, skieen en vakanties). Ondanks dat jullie niet altijd begrepen wat voor onderzoek ik nou precies deed, ja iets met ratten en longen, jullie hebben er in ieder geval voor gezorgd dat ik regelmatig mijn werk even kon vergeten en kon genieten van iets anders.
Tenslotte mijn ouders. Lieve pap en mam, ontzettend bedankt voor al jullie liefde, steun, begrip en zorgzaamheid. Ondanks dat jullie niet altijd begrepen waar mijn onderzoek over ging, waren jullie zeker geinteresseerd in mijn onderzoek en hadden jullie altijd een luisterend oor. Bedankt voor alles wat jullie voor mij gedaan hebben. lk ben er trots op dat jullie mijn ouders zijn !
Bedankt!!
Noelle
142