Embed Size (px)
Citation preview

University of Groningen
Identifying therapeutic targets by elucidating signaling pathways in pediatric lymphoidleukemiasvan der Sligte, Naomi Eline
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2015
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):van der Sligte, N. E. (2015). Identifying therapeutic targets by elucidating signaling pathways in pediatriclymphoid leukemias. [Groningen]: University of Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 21-10-2020

General introduction and Scope of the thesis
Chapter 1

Chapter 1
10
GENERAL INTRODUCTIONNormal and malignant hematopoiesis
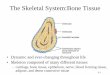
The biological process of blood cell formation is called hematopoiesis. All types of blood cells originate from a small pool of pluripotent stem cells, known as hematopoietic stem cells (HSC). The maintenance, commitment, proliferation, and differentiation of HSCs is dependent on the bone marrow microenvironment.1 In the bone marrow, bone marrow stromal cells (including stromal fibroblasts, osteoblasts, endothelial cells, and adipocytes) support the production of blood cell maturation by producing growth factors, direct stromal cell-blood cell contact, and the production of the extracellular bone marrow matrix.1 In this bone marrow niche, HSCs are multipotent and have the capacity to differentiate towards all types of mature blood cells. Before differentiating into various mature blood cells, the committed HSC will first differentiate into lineage-specific progenitor cells; the common myeloid progenitor and the common lymphoid progenitor (Figure 1).2,3
Genetic alterations in hematopoietic stem and progenitor cells disturb the regulation of normal hematopoiesis leading to a clonal proliferation of hematopoietic progenitor cells in the bone marrow.4,5 Accumulation of subsequent genetic changes can lead to leukemia formation. Leukemia is characterized by an uncontrolled proliferation of immature blood cells, accompanied by a block in maturation and frequently escape from apoptosis, resulting in an excess of malignant cells.6
Figure 1 Hematopoiesis

General introduction and scope of the thesis
11
1Leukemias can be stratified according to the affected lineage into either lymphoid or myeloid.7
When the differentiation block occurs in the myeloid lineage the disease is called ‘myeloid leukemia’, whereas a blocked lymphoid lineage differentiation is called ‘lymphoid leukemia’. Leukemias can also be classified based on clinical presentation and disease development in ‘acute’ or ‘chronic’. In total we can classify four main categories: Acute Lymphoblastic Leukemia (ALL), Acute Myeloid leukemia (AML), Chronic Lymphoblastic Leukemia (CLL), and Chronic Myeloid Leukemia (CML).7 This thesis will focus on therapeutic targets in the context of pediatric ALL and a progressed phase of pediatric CML (lymphoid blast crisis CML).
Acute Lymphoblastic Leukemia
Epidemiology and clinical presentation
With approximately 25% of all pediatric malignancies diagnosed, ALL is the most common type of cancer among children (<15 years).8 The peak incidence occurs between two and five years of age with a male:female prevalence of 1.3:1.9
The symptoms of ALL are mainly nonspecific e.g. fatigue, pale skin, fever, bleeding, hematoma, petechiae, bone pain, and lymphadenopathy. Symptoms occur by displacement of normal bone marrow cells by immature blasts, resulting in anemia, thrombocytopenia, and granulocytopenia or lymphocytopenia.7,10 Bone pain, most frequently affecting the long bones, is caused by leukemic involvement of the periosteum. Mediastinal mass, testicular enlargement, and focal neurological signs are rare.7,10
Pathobiology
In general, ALL arises from various genetic, epigenetic, and environmental lesions in a lymphoid progenitor cell leading to an uncontrolled cell proliferation and stage-specific development arrest.9,11 Historically, ALL was classified based on morphology using the French-American-British (FAB) system incorporating information regarding the size, amount of cytoplasm, and prominence of nucleoli of tumor cells from the bone marrow.12 The World Health Organization (WHO) published a classification system for tumors and leukemias incorporating immunophenotypic, genetic, and clinical information to define a clinically and biologically relevant disease nomenclature.13 According to the immunophenotype, ALL is first classified into B-cell progenitor ALL (BCP-ALL) and T-cell ALL (T-ALL) and secondly subclassified according to cytogenetic and molecular genetic abnormalities.14 The complete WHO classification is shown in Table 1.
A minority of all ALL cases (<5%) is associated with inherited, predisposing genetic syndromes as for example Down’s syndrome.11 Cytogenetic and molecular genetic abnormalities are known in approximately 75% of the cases.15 In BCP-ALL these abnormalities include hyperdiploidy

Chapter 1
12
(>50 chromosomes), hypodiploidy (<44 chromosomes), and the translocations t(12;21)(p13;q22) encoding ETV6-RUNX1, t(1;19)(q23;p13) encoding TCF3-PBX1, t(9;22)(q34;q11) encoding BCR-ABL1, and MLL rearrangements (Figure 2).9 Dysregulation of the T-cell receptor (TCR) genes TLX1, TLX3, HOXA, TAL1, TAL2, LMO1, LMO2, and LYL1 often occurs in T-ALL (Figure 2).9,16 However, these translocations alone do not induce leukemia in experimental mouse models and in 25% of the cases no chromosomal alteration are known, suggesting additional genetic alterations contributing to leukemogenesis.9 High-resolution microarray profiling revealed the presence of more genetic alterations involved in prognosis and development of leukemia and defined new leukemia subtypes (e.g. IKZF1, PAX5, and CDKN2A/B deletions in BCP-ALL, and CDKN2A deletions, activating NOTCH1 mutations, and PTEN loss in T-ALL).9,17 Similarly, gene-expression profiling revealed new ALL subtypes based on gene-expression signatures such as BCR-ABL1-like in BCP-ALL (also known as Philadelphia-like), a subtype of precursor BCP-ALL with a similar gene expression profile compared to Philadelphia-positive ALL, and early T-cell precursor (ETP) ALL in T-ALL.18-20
Table 1 WHO classification of acute lymphoblastic leukemias (World Health Organization 2008)
Acute lymphoblastic leukemia
1. B lymphoblastic leukemia
B lymphoblastic leukemia, not otherwise specified
B lymphoblastic leukemia with recurrent genetic abnormalities
B lymphoblastic leukemia with t(9;22)(q34;q11.2); BCR-ABL1
B lymphoblastic leukemia with t(v;11q23); MLL-rearranged
B lymphoblastic leukemia with t(12;21)(p13;q22); TEL-AML1 (ETV6-RUNX1)
B lymphoblastic leukemia with hyperdiploidy
B lymphoblastic leukemia with hypodiploidy
B lymphoblastic leukemia with t(5;14)(q31;q32); IL3-IGH
B lymphoblastic leukemia with t(1;19)(q23;p13.3) E2A-PBX1 (TCF3-PBX1)
2. T lymphoblastic leukemia
Prognostic factors and prognosis
Clinical and biological factors are important prognostic predictors of outcome. Age (infant or ≥ 10 years of age), leukocyte count (≥ 50x109/L), race (black and Hispanic), and male sex are unfavorable clinical prognostic factors.9,11 Unfavorable biological prognostic factors include T-ALL, hypodiploidy, MLL-translocations, and BCR-ABL fusion.9,11 Recently, IKZF1 deletions are identified as an unfavorable prognostic factor.19,21,22 The most relevant prognostic factor is

General introduction and scope of the thesis
13
1the early response to therapy e.g. minimal residual disease (MRD).9 The prognosis of patients with ≥1% leukemic cells after remission-induction therapy is almost as poor as those who fail to achieve complete clinical remission (≥5% leukemic cells).8,11
Since the introduction of chemotherapy, and especially the introduction of combination chemotherapy, overall 5-year event-free and overall survival rates for ALL have increased dramatically.8 Current overall survival rates are approaching 90%.9 Nevertheless, despite intensive chemotherapy, still about 20% of ALL patients struggle with ALL relapse.23
Figure 2 Frequencies of key subtypes of childhood ALLData were modified from Mullighan et al.9 Abnormalities that are exclusively seen in T-ALL are shown in blue.
Chronic Myeloid Leukemia
Epidemiology and clinical presentation
With an annual incidence of 0.6-1.2 per million children/year, accounting for approximately 2-3% of all pediatric leukemia cases, CML is very rare among children.24-26 With age, the incidence of CML increases with a median age at diagnosis of 65 years.24 The median age at presentation in children is 11 years. At initial presentation, 85% of pediatric CML patients is diagnosed in the chronic phase (CP).25,26 CML has historically been a triphasic disease. Without treatment, CML can rapidly progress to accelerated phase (AP) and blast crisis (BC), which in adults involves either myeloid (67%) or lymphoid (33%) transformation.27
As with acute lymphoblastic leukemia, the most frequent symptoms of CML are nonspecific, including fatigue, night sweats, malaise and weight loss, left upper quadrant pain, and splenomegaly.28

Chapter 1
14
Pathobiology
CML is a clonal hematopoietic stem cell disorder characterized by the presence of the Philadelphia chromosome translocation t(9;22)(q34;q11), generating the BCR-ABL1 fusion gene which is giving rise to the constitutively active tyrosine kinase BCR-ABL.27,28 The initial chronic phase is characterized by a clonal expansion of the granulocytic cell lineage, even though theoretically all hematopoietic lineages can be produced from the CML stem cell.29
The transition of CML chronic phase into blast crisis is not completely understood. Currently it is hypothesized that BCR-ABL activity cause genomic instability, resulting in the accumulation of genetic abnormalities activating oncogenic factors and / or mutations required for disease progression to blast phase.30,31 This phase is characterized by a block in cell differentiation of the myeloid or lymphoid lineage known as myeloid blast crisis (MyBC) or lymphoid blast crisis (LyBC), respectively.29
Prognosis
With the introduction of tyrosine kinase inhibitors (TKIs), like imatinib (Gleevec ®), CML has transformed from a fatal disease to a leukemia subtype with a favorable prognosis.24,26 Estimated progression-free survival rates are 98% among children with chronic phase CML at 36 months, which is comparable to the results achieved in adults.25,32,33 Unfortunately, when CML has progressed to blast crisis, treatment options are limited to only a few months.34
Signal transduction pathways in cancer
The transformation from a normal cell to a malignant cell is a highly complex process and involves multiple genetic, epigenetic, and environmental events.35 Hanahan and Weinberg have defined specific characteristics of malignant cells, known as the hallmarks of cancer, which are: sustaining proliferative signaling, evading growth suppressors, avoiding immune destruction, enabling replicative immortality, tumor-promoting inflammation, activating invasion and metastasis, inducing angiogenesis, genome instability and mutation, resisting cell death, and deregulating cellular energetics.5,36 These characteristics are acquired through complex genetic changes including the activation of oncogenes by mutations, translocations, and amplifications resulting in enhanced cell signaling, which in turn leads to oncogenic transformation.37,38 Mutations in tumor suppressor genes, such as loss of function deletions, similarly contribute to oncogenesis.38 In addition to oncogenes and tumor suppressor genes, aberrations in proapoptotic and antiapoptotic genes as well as genes that control cell proliferation and differentiation contribute to cancer formation and metastasis.37
Genetic alterations can lead to or coincide with epigenetic changes including loss of DNA methylation and alterations in the histone acetylation patterns.39 Many of the genetic and

General introduction and scope of the thesis
15
1epigenetic abnormalities which are at the basis of oncogenic transformation, maintenance, and tumor progression ultimately influence the activation of signal transduction pathways.37
Signal transduction pathways are intracellular signaling cascades traditionally initiated by an extracellular stimulus e.g. binding of ligand by a transmembrane receptor that transfers the signal through a series of phosphorylation events until finally reaching regulatory molecules in the nucleus, such as transcription factors. Cellular signal transduction activity is controlled by protein phosphorylation. Therefore, the balance of kinase and phosphatase activity, responsible for protein phosphorylation and dephosphorylation, respectively, regulate many key aspects of intracellular processes. In the human body, 518 unique human protein kinases and 58 receptor tyrosine kinases have been identified.39,40 Malignant transformation of cells is highly dependent on the deregulation of protein kinases responsible for the activation of signal transduction pathways.41 In this regard, protein kinases are highly interesting targets to be investigated by pharmaceutical companies.
Signal transduction for the identification of druggable targets
Over the past decade, molecular profiling of the genome, epigenome, transcriptome, and proteome has markedly increased our knowledge of the molecular background underlying cancer development. As a consequence, treatment strategies have changed from a “one size fits all” principle to a more personalized approach.42 The dictionary of cancer terms from the National Cancer Institute (NCI) defines personalized medicine as “A form of medicine that uses information about a person’s genes, proteins, and environment to prevent, diagnose, and treat disease” (www.cancer.gov/dictionary). A breakthrough for targeted therapy was the introduction of the tyrosine kinase inhibitor imatinib (Gleevec ®) for the treatment of CML. Imatinib blocks the ATP binding site on the constitutively activated protein kinase BCR-ABL1 and thereby inhibits the phosphorylation of downstream substrates.43 To date, 29 small molecule inhibitors have received US Food and Drug Administration (FDA) approval for cancer indications. Currently, targeted therapy is also used in clinical practice for patients with non-small cell lung cancer (NSCLC) harboring ALK-rearrangements, EGFR-mutated NSCLC, KIT-mutated gastrointestinal stroma tumors, and melanoma harboring BRAF V600 mutations.44-47
From the clinical point of view, in pediatric lymphoid leukemias, kinase inhibitors only have a revolutionary impact to the treatment of Philadelphia-positive (Ph+) ALL and CML.48 However, genomic profiling of high risk BCP-ALL identified several subgroups sensitive to kinase inhibitors.49,50 Genomic profiling of the BCR-ABL1-like ALL subtype identified rearrangements involving EBF1 and PDGFRB giving rise to the constitutively active PDGFRB kinase which is sensitive to FDA-approved ABL1 inhibitors as imatinib and dasatinib.50-52 Additionally, characterization of the signaling consequences of CRLF2-rearrangements in ALL showed increased basal levels of pSTAT5 and pJAK2 which can be targeted with JAK inhibitors.53 In addition to CRLF2-rearranged ALL, JAK inhibitors are interesting for the treatment of human

Chapter 1
16
leukemic cells with JAK2 rearrangements as well as erythropoietin receptor (EPOR) rearranged ALL.49
In T-ALL the rationale for the use of kinase inhibitors is less intensively studied compared to BCP-ALL. Genomic profiling of early T cell precursor (ETP) ALL, an aggressive subtype of T-ALL, showed activating mutations in genes regulating cytokine receptor, RAS, and JAK/STAT signaling in more than 60% of the cases, thus suggesting the use of targeted therapy for this specific T-ALL subtype.54,55 Unfortunately, intensive genome profiling has not yet resulted in the widely implementation of kinase inhibitors for the treatment of ALL and CML-LyBC.
SCOPE OF THE THESISAlthough the survival of pediatric leukemias, in particular acute lymphoblastic leukemia, has improved remarkably over the last decades, ALL relapse remains a leading cause of cancer death among children and the survival of lymphoid blast crisis CML is limited in terms of months.23,34 Major improvements in outcome for ALL are the result of improved scheduling and dosing of combination chemotherapies. However, these improvements in clinical outcome have reached a plateau, mostly due to chemotherapy related toxicity.56 Furthermore, treatment options for lymphoid blast crisis CML are limited due to tyrosine kinase inhibitor resistance.34 Therefore, new treatment options are needed to cure all children with lymphoid leukemia.
Since genomic, epigenomic, and environmental alterations affect components of signaling pathways that lead to critical cellular processes such as proliferation and differentiation, the aim of this thesis is to identify therapeutic targets by elucidating signal transduction pathways in pediatric lymphoid leukemias.
We are currently facing significant limitations in implementing newly designed kinase inhibitors in the clinic for the treatment of pediatric malignancies. As many hallmarks of cancer are known to be regulated by intracellular protein signaling networks, we suggest to focus on these networks to improve the implementation of kinase inhibitors. Chapter 2 will provide a short overview of currently used strategies for the implementation of kinase inhibitors as well as reasons why kinase inhibitors has unfortunately not yet resulted in the widespread use for the treatment of pediatric cancer. Furthermore, we will propose a personalized medicine strategy, combining kinomics, proteomics, and drug screen approaches attempting to bridge the gap between pediatric cancers and the use of kinase inhibitors.
ALL arises after the occurrence of several known and unknown abnormalities.9 Previously we have shown that kinome profiling is an elegant approach to generate insight into active signal transduction pathways and is able to identify new potential druggable targets for future treatment

General introduction and scope of the thesis
17
1strategies.57-59 In Chapter 3 we used kinome profiling to study active signal transduction pathways in pediatric ALL and investigated known and unknown signaling proteins relevant to ALL and of potential interest for future targeted therapy approaches.
Subsequently, our kinase activity profiles showed a significantly elevated phosphorylation of a peptide derived from cyclic (c)-AMP response element binding protein_Y134/S133 (CREB_Y134/S133) compared to normal bone marrow.58 The applicability of CREB as a potential druggable target in ALL is described in Chapter 4. We studied the effects of a loss of CREB function on ALL cell survival and gene expression profiles using shRNA mediated knockdown of CREB and a CREB inhibitor. Moreover, we correlated CREB expression in primary ALL patients to outcome.
Genome wide approaches in ALL have increased the list of risk predictors and added IKZF1 deletions as an unfavorable prognostic factor.19,21,22 Although in adults IKZF1 deletions are most frequently identified in Philadelphia chromosome positive (Ph+) ALL, in pediatric BCP-ALL 80% of the IKZF1 deletions are found in a Philadelphia negative background. Effects of IKZF1 deletions on signaling pathways in this Philadelphia negative group is largely unknown. In Chapter 5 we studied the effect of IKZF1 deletions on active signal transduction pathways using kinome profiling and western blot analysis.
Since treatment options for CML are limited once the disease has progressed to lymphoid blast crisis, early recognition of patients at risk of disease progression to CML-LyBC is desirable. In Chapter 6 we used Multiplex Ligation-dependent Probe Amplification (MLPA) to determine whether B-cell lymphoid leukemia-specific copy number alterations (CNAs), including IKZF1, PAX5, and CDKN2A deletions, could be detected in CML-CP and used to predict disease progression to CML-LyBC.
The activation of signaling pathways, independent of BCR-ABL1 activity, might be involved in disease progression to CML-LyBC and CML-LyBC cell survival. Therefore, inhibition of signaling hubs of these pathways might be of potential interest as new targets for the treatment of lymphoid blast crisis CML. In Chapter 7 we have studied the role of Akt, STAT3, and FAK for the survival of CML-LyBC cells to identify new potential therapeutic targets.
Finally, Chapter 8 will summarize the results of the studies described in this thesis and the results will be discussed in a broader perspective. In Chapter 9 a summary of the thesis in Dutch is given.

Chapter 1
18
REFERENCES
1. Taichman RS. Blood and bone: two tissues whose fates are intertwined to create the hematopoietic stem-cell niche. Blood 2005; 105: 2631-2639.
2. Morrison SJ, Wandycz AM, Hemmati HD, Wright DE, Weissman IL. Identification of a lineage of multipotent hematopoietic progenitors. Development 1997; 124: 1929-1939.
3. Uchida N, Fleming WH, Alpern EJ, Weissman IL. Heterogeneity of hematopoietic stem cells. Curr Opin Immunol 1993; 5: 177-184.
4. Passegue E, Jamieson CH, Ailles LE, Weissman IL. Normal and leukemic hematopoiesis: are leukemias a stem cell disorder or a reacquisition of stem cell characteristics? Proc Natl Acad Sci U S A 2003; 100 Suppl 1: 11842-11849.
5. Hanahan D and Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011; 144: 646-674. 6. Warner JK, Wang JC, Hope KJ, Jin L, Dick JE. Concepts of human leukemic development. Oncogene
2004; 23: 7164-7177. 7. Davis AS, Viera AJ, Mead MD. Leukemia: an overview for primary care. Am Fam Physician 2014; 89:
731-738. 8. Pui CH. Recent research advances in childhood acute lymphoblastic leukemia. J Formos Med Assoc
2010; 109: 777-787. 9. Inaba H, Greaves M, Mullighan CG. Acute lymphoblastic leukaemia. Lancet 2013; 381: 1943-1955. 10. Margolin J, Steuber C, Poplack D. Acute Lymphoblastic Leukemia. In: Principles and Practice of
Pediatric Oncology. 4th ed. Pizzo PA, Poplack DG, Philadelphia, Lippincott-Raven 2001; 489. 11. Pui CH, Robison LL, Look AT. Acute lymphoblastic leukaemia. Lancet 2008; 371: 1030-1043. 12. Bennett JM, Catovsky D, Daniel MT, et al. Proposals for the classification of the acute leukaemias.
French-American-British (FAB) co-operative group. Br J Haematol 1976; 33: 451-458. 13. Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO)
classification of myeloid neoplasms and acute leukemia: rationale and important changes. Blood 2009; 114: 937-951.
14. Jaffe ES, Harris NL, Stein H, Isaacson PG. Classification of lymphoid neoplasms: the microscope as a tool for disease discovery. Blood 2008; 112: 4384-4399.
15. Pui CH, Carroll WL, Meshinchi S, Arceci RJ. Biology, risk stratification, and therapy of pediatric acute leukemias: an update. J Clin Oncol 2011; 29: 551-565.
16. Grabher C, von Boehmer H, Look AT. Notch 1 activation in the molecular pathogenesis of T-cell acute lymphoblastic leukaemia. Nat Rev Cancer 2006; 6: 347-359.
17. Tosello V and Ferrando AA. The NOTCH signaling pathway: role in the pathogenesis of T-cell acute lymphoblastic leukemia and implication for therapy. Ther Adv Hematol 2013; 4: 199-210.
18. Den Boer ML, van Slegtenhorst M, De Menezes RX, et al. A subtype of childhood acute lymphoblastic leukaemia with poor treatment outcome: a genome-wide classification study. Lancet Oncol 2009; 10: 125-134.
19. Mullighan CG, Su X, Zhang J, et al. Deletion of IKZF1 and prognosis in acute lymphoblastic leukemia. N Engl J Med 2009; 360: 470-480.
20. Coustan-Smith E, Mullighan CG, Onciu M, et al. Early T-cell precursor leukaemia: a subtype of very high-risk acute lymphoblastic leukaemia. Lancet Oncol 2009; 10: 147-156.
21. van der Veer A, Waanders E, Pieters R, et al. Independent prognostic value of BCR-ABL1-like signature and IKZF1 deletion, but not high CRLF2 expression, in children with B-cell precursor ALL. Blood 2013; 122: 2622-2629.

General introduction and scope of the thesis
19
122. Kuiper RP, Waanders E, van der Velden VH, et al. IKZF1 deletions predict relapse in uniformly treated
pediatric precursor B-ALL. Leukemia 2010; 24: 1258-1264. 23. Mullighan CG. The molecular genetic makeup of acute lymphoblastic leukemia. Hematology Am Soc
Hematol Educ Program 2012; 2012: 389-396. 24. Hehlmann R, Hochhaus A, Baccarani M, European LeukemiaNet. Chronic myeloid leukaemia. Lancet
2007; 370: 342-350. 25. Suttorp M, Eckardt L, Tauer JT, Millot F. Management of chronic myeloid leukemia in childhood. Curr
Hematol Malig Rep 2012; 7: 116-124. 26. de la Fuente J, Baruchel A, Biondi A, et al. Managing children with chronic myeloid leukaemia (CML):
recommendations for the management of CML in children and young people up to the age of 18 years. Br J Haematol 2014; 167: 33-47.
27. Faderl S, Kantarjian HM, Talpaz M. Chronic myelogenous leukemia: update on biology and treatment. Oncology (Williston Park) 1999; 13: 169-80; discussion 181, 184.
28. Apperley JF. Chronic myeloid leukaemia. Lancet 2014. 29. Ren R. Mechanisms of BCR-ABL in the pathogenesis of chronic myelogenous leukaemia. Nat Rev
Cancer 2005; 5: 172-183. 30. Calabretta B and Perrotti D. The biology of CML blast crisis. Blood 2004; 103: 4010-4022. 31. Mullighan CG, Miller CB, Radtke I, et al. BCR-ABL1 lymphoblastic leukaemia is characterized by the
deletion of Ikaros. Nature 2008; 453: 110-114. 32. Millot F, Baruchel A, Guilhot J, et al. Imatinib is effective in children with previously untreated chronic
myelogenous leukemia in early chronic phase: results of the French national phase IV trial. J Clin Oncol 2011; 29: 2827-2832.
33. Druker BJ, Guilhot F, O’Brien SG, et al. Five-year follow-up of patients receiving imatinib for chronic myeloid leukemia. N Engl J Med 2006; 355: 2408-2417.
34. Cortes J, Kim DW, Raffoux E, et al. Efficacy and safety of dasatinib in imatinib-resistant or -intolerant patients with chronic myeloid leukemia in blast phase. Leukemia 2008; 22: 2176-2183.
35. Bishop JM. Molecular themes in oncogenesis. Cell 1991; 64: 235-248. 36. Hanahan D and Weinberg RA. The hallmarks of cancer. Cell 2000; 100: 57-70. 37. Vogelstein B and Kinzler KW. Cancer genes and the pathways they control. Nat Med 2004; 10: 789-
799. 38. Lodish H, Berk A, Lawrence Zipursky S, et al. Section 24.2. In: Molecular Cell Biology. 4th ed. Freeman
WH, New York, Media Connected 2000. 39. Lemmon MA and Schlessinger J. Cell signaling by receptor tyrosine kinases. Cell 2010; 141: 1117-
1134. 40. Manning G, Whyte DB, Martinez R, Hunter T, Sudarsanam S. The protein kinase complement of the
human genome. Science 2002; 298: 1912-1934. 41. Blume-Jensen P and Hunter T. Oncogenic kinase signalling. Nature 2001; 411: 355-365. 42. Kalia M. Biomarkers for personalized oncology: recent advances and future challenges. Metabolism
2015; 64: S16-21. 43. Breccia M, Efficace F, Alimena G. Imatinib treatment in chronic myelogenous leukemia: What have
we learned so far? Cancer Lett 2011; 300: 115-121. 44. Shaw AT, Yeap BY, Solomon BJ, et al. Effect of crizotinib on overall survival in patients with advanced
non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis. Lancet Oncol 2011; 12: 1004-1012.

Chapter 1
20
45. Sequist LV, Martins RG, Spigel D, et al. First-line gefitinib in patients with advanced non-small-cell lung cancer harboring somatic EGFR mutations. J Clin Oncol 2008; 26: 2442-2449.
46. Heinrich MC, Corless CL, Demetri GD, et al. Kinase mutations and imatinib response in patients with metastatic gastrointestinal stromal tumor. J Clin Oncol 2003; 21: 4342-4349.
47. Flaherty KT, Puzanov I, Kim KB, et al. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med 2010; 363: 809-819.
48. Ohno R. Changing paradigm of the treatment of Philadelphia chromosome-positive acute lymphoblastic leukemia. Curr Hematol Malig Rep 2010; 5: 213-221.
49. Roberts KG, Li Y, Payne-Turner D, et al. Targetable kinase-activating lesions in Ph-like acute lymphoblastic leukemia. N Engl J Med 2014; 371: 1005-1015.
50. Roberts KG, Morin RD, Zhang J, et al. Genetic alterations activating kinase and cytokine receptor signaling in high-risk acute lymphoblastic leukemia. Cancer Cell 2012; 22: 153-166.
51. Weston BW, Hayden MA, Roberts KG, et al. Tyrosine kinase inhibitor therapy induces remission in a patient with refractory EBF1-PDGFRB-positive acute lymphoblastic leukemia. J Clin Oncol 2013; 31: e413-6.
52. Lengline E, Beldjord K, Dombret H, et al. Successful tyrosine kinase inhibitor therapy in a refractory B-cell precursor acute lymphoblastic leukemia with EBF1-PDGFRB fusion. Haematologica 2013; 98: e146-8.
53. Tasian SK, Doral MY, Borowitz MJ, et al. Aberrant STAT5 and PI3K/mTOR pathway signaling occurs in human CRLF2-rearranged B-precursor acute lymphoblastic leukemia. Blood 2012; 120: 833-842.
54. Zhang J, Ding L, Holmfeldt L, et al. The genetic basis of early T-cell precursor acute lymphoblastic leukaemia. Nature 2012; 481: 157-163.
55. Maude SL, Dolai S, Delgado-Martin C, et al. Efficacy of JAK/STAT pathway inhibition in murine xenograft models of early T-cell precursor (ETP) acute lymphoblastic leukemia. Blood 2015; 125: 1759-1767.
56. Roberts KG and Mullighan CG. How new advances in genetic analysis are influencing the understanding and treatment of childhood acute leukemia. Curr Opin Pediatr 2011; 23: 34-40.
57. Sikkema AH, Diks SH, den Dunnen WF, et al. Kinome profiling in pediatric brain tumors as a new approach for target discovery. Cancer Res 2009; 69: 5987-5995.
58. Ter Elst A, Diks SH, Kampen KR, et al. Identification of new possible targets for leukemia treatment by kinase activity profiling. Leuk Lymphoma 2011; 52: 122-130.
59. Kampen KR, Ter Elst A, Mahmud H, et al. Insights in dynamic kinome reprogramming as a consequence of MEK inhibition in MLL-rearranged AML. Leukemia 2014; 28: 589-599.









![Bi Journal of Bioengineering & Biomedical Science...Medicine [46]. Adult bone marrow include two well defined populations of stem cells: hematopoietic stem cells (HSCs) that give rise](https://img.pdfslide.net/doc/110x75/60e09ab44a39df492a73ab8f/bi-journal-of-bioengineering-biomedical-science-medicine-46-adult-bone.jpg)