Embed Size (px)
Citation preview
ศ.นพ.เกรียง ตั้งสง่า
ภาควชิาอายุรศาสตร์
คณะแพทยศาสตร์ จุฬาลงกรณ์มหาวทิยาลยั
๘ ก.พ. ๒๕๕๕
Update in Delaying Progression of Chronic Kidney Disease
การประชุมวชิาการสัญจร ครั้งที่ 20
ราชวทิยาลยัอายุรแพทย์แห่งประเทศไทย ร่วมกบั โรงพยาบาลแพร่

Scope of Presentation1. ESRD : epidemiology
2. CKD - definition & classification - prevalence
3. Serum creatinine and GFR equation
4. Risk factors for CKD
5. Intervention to delay CKD progression


Prevalence of ESRD - World wide
USRDS report2009


Unique causes of CKD in Thailand
1. RTA (Nephrocalcinosis, renal stone)
2. Nephrolithiasis (obstruction infection, CKD)
3. Cadmium (แม่สอด) B2G’ uria, RTA, CKD
4. Lead poisoning (คลตีี,้ กาญจนบุรี)
5. Fluorosis
6. Herbal medicine (Aristolochic acid, etc.)

Creatinine measurement
- Modified Jaffe’s method ( 10 – 20% ever estimation )
- Enzymatic method

= S.cr
= GFR
S.Cr is a ( poor representative of GFR )

1. Creatinine clearance
- 24h urine colln. Ccr = UV / P- Cockroft & Gault. Ccr = (140 – Age) . BW
72 . S.cr (x 0.85 if female)
2. Isotope clearance
- Plasma clearance : Iothalamate, DTPA-plasma clearance
- Calibrated with serum creatinine [ eGFR ]

Abbreviated MDRD-GFR equations Re-expressed IDMS – traceable 1
= 175 x S.cr-1.154 x Age-0.203 x 0.742 ( female )
MDRD2 = 186 x S.cr-1.154 x Age-0.203 x 0.742 ( female ) x 1.212 (black)
Japanese 3 = 168 x S.cr-1.044 x Age-0.274 x 0.775 ( female )
Chinese 4 = 175 x S.cr-1.234 x Age-0.179 x 0.79 ( female )
Thai 5 re-expressed IDMS traceable MDRD equation.
= 175 x CrEnz-1.154 x Age-0.203 x 0.742 ( female ) x 1.129 ( Thai )
or = 375.5 x CrEnz-0.848 x Age-0.364 x 0.712 ( female )
1. AJKD 2007; 50: 927-37. 2. Ann Intern Med 1999; 130: 461-70.3. Clin Chem 2007; 53: 766-72. 4. JASN 2006; 17: 2937-44.5. Praditpornsilpa K, WCN May 2008.

Levey AS, et al. Ann Intern Med 2009; 150: 604.
S.cr μmol/L ( mg/dL )

Kidney function (GFR, Ccr)
0%
50%
100% Pre-dialysis
CKD
Normal
Dialysis
Time
? CRF

Definition of Chronic Kidney Disease1. Kidney damage >3 months, ( +/- GFR )
defined by a. Pathological abnormalities; orb. Functional abnormalities
Markers of kidney damage include- abnormal blood or urine composition - abnormal imaging tests
2. GFR <60 mL/min/1.73 m2 for >3 months, ( +/- kidney damage )
AJKD 2002; 39 (Suppl 1): S17
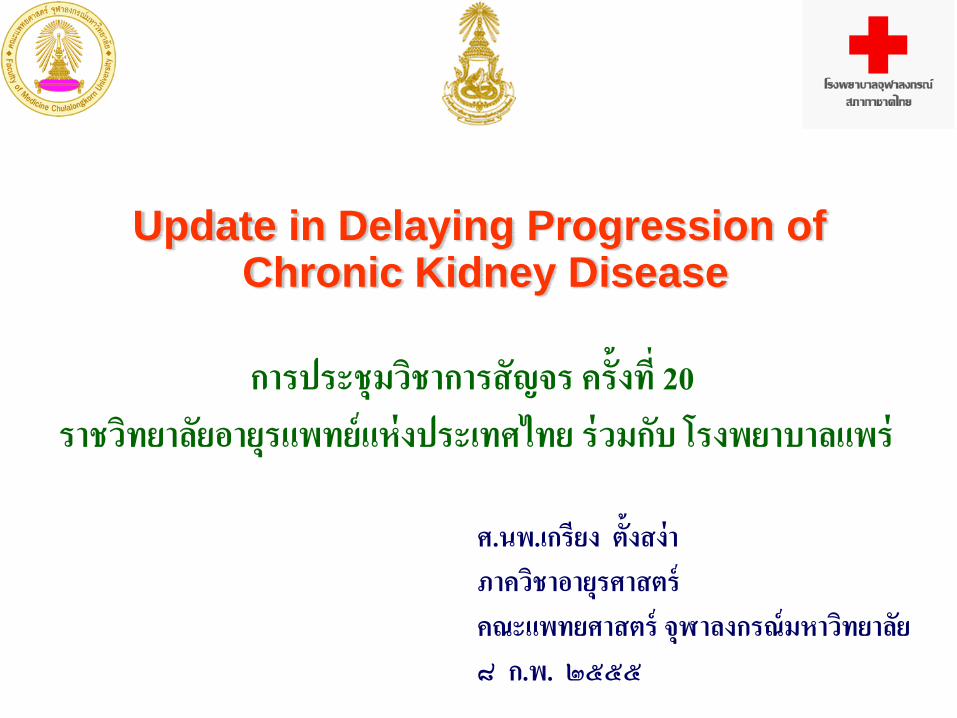
Stages of Chronic Kidney Disease
Stage
1
2
3
4
5ESRD
Kidney Failure
Severely DecreasedFiltration
Moderately DecreasedFiltration
Kidney Damage withMildly Decreased Filtration
Kidney Damage with Normal Filtration
GlomerularFiltration Rate
ml / min / 1.73 m2
> 90
60 – 89
30 – 59
15 – 29
< 15
Prevalence *
64%
31%
4.3%
0.2%
0.2%
RRT
* Prevalence per adult population age > 20 AJKD 2002; 39 ( Suppl 1 ) : S49.
HD, CAPD> Stage 3 = 4,700 PMP


Prevalence studies in ThailandAuthor, year Subject Number CKD stage (%) MDRD
I II III IV VDomrongkitchaiporn S et al, 1997
EGATAge 55(5.1)Male 75.9%
2,967 NA NA 6.4 0.2 0.2
Chittinandana A et al,2002
RTAFAge 45.7(8)Male 82%
15,612 0.8 0.7 2.9 0.1 0.06
InterASIA,2000
General populationAge 50.5(1.5)Male 48%
5,146 NA NA 13.2 0.61 NA
Thai SEEK project,
Ingsathit A, et al, 2009
General populationAge 45.3 (15.4)
Male 45.3%
3,459 3.3 5.6 7.5 0.8 0.3
8.6
CKD awareness = 1.9% among stages 1 - 4
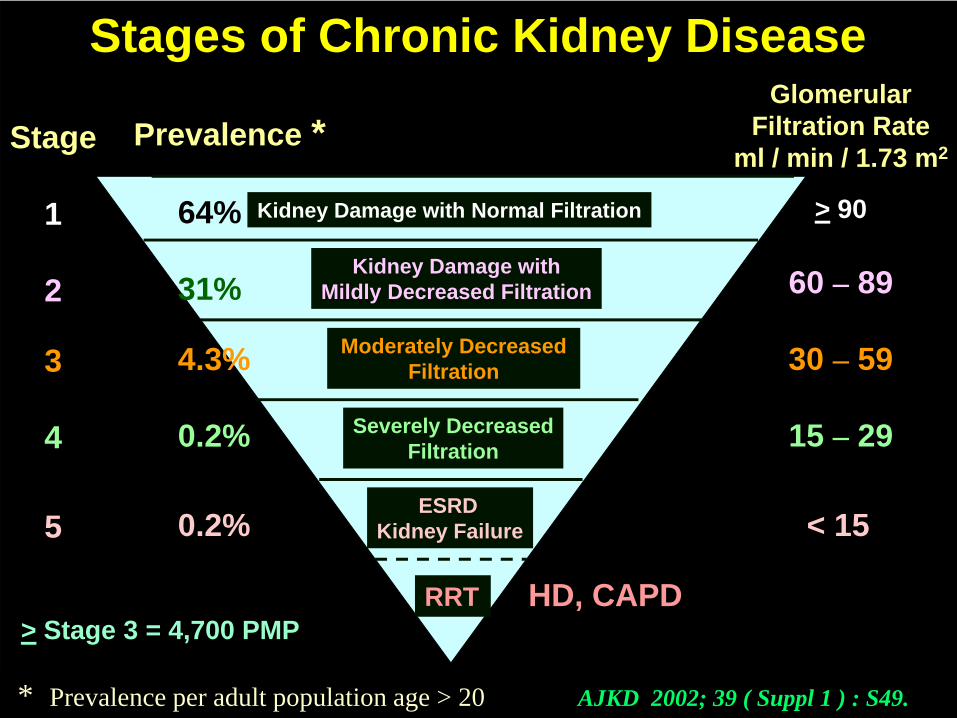
NORMAL
Presence of risk factor
Renal Damage ( Nephropathy )
Primary prevention
Microalbuminuria / proteinuria
GFR
Secondary prevention
Progressive Renal Damage ( CKD progression )
ESRD ( pre-dialysis ) RRT ( HD, PD, KTx )

Levey AS, et al. KI 2005; 67: 2089-100.
Complications
Normal Increasedrisk Damage GFR Kidney
failure Death
Screening for CKD
riskfactors
CKD riskfactor
reduction.Screeningfor CKD.
Dx + Rx ofcomorbid
conditions.Rx to slow
Progression.
Estimaterate of
progression.Treat
complications.Prepare for
replacement.
Replacement by dialysis
& transplant
Conceptual model of thecourse of chronic kidney disease (CKD)

Treatment of primary cause
- Glycemic control in DM- Blood pressure control in hypertensive pts.
-Relieving obstruction - Rx of glomerulonephritis - immunologic damage
- proteinuria- Rx of infection
Overall Risk Factors for CKD Progression
1. Poor glycemic control2. Albuminuria & Proteinuria3. BP control & RAAS inhibition4. Baseline kidney function5. Drugs (ASA, NSAID) & radio-contrast, 6. Metabolic acidosis7. Acute kidney injury8. Diet9. Infection (local & systemic)10. Kidney stones11. Genetics & Races

DCCT / EDIC Group 1441 T1DM F/U 17 yrs.HbA1C : Intensive = 7.4%
Conventional = 9.1%

(10 yrs.) (17 yrs.)

Intensive better
NEJM 2008; 358: 2560.
11,140 T2DM : intensive vs. std. BS control, HbA1C 6.5 vs. 7.3%,F/U 5 yrs.

10,251 T2DM : intensive vs. std. BS control, HbA1C 6.3 vs. 7.2%,F/U 8 yrs.
Lancet 2010; 376: 419.

Trials of glucose control on renal outcome in DM
DMduration
Archivedduration
Microalb.(MA)
eGFR orS.cr
T1DM
DCCT 1-5 yr 7.2 vs. 9.1% risk in IC No. diff.AER < 40 mg/d
T2DM
Advance 8 6.5 vs. 7.3%
Accord 10 6.4 vs. 7.5% risk of MA No. diff.& Mac. A.
VADT 11.5 6.9 vs. 8.4%
IC = Intensive blood sugar control= Early termination of the study due to inc. MR in the arm

Guideline on glycemic control in DM-CKD(NST – CKD guideline, 2552)
- Target FBS = 90 – 130, A1C < 7.0%
- If S.cr > 1.4 mg/dl No. = Metformin, & chlorpropamide
- If S.cr > 3, eGFR < 30 ml / min / 1.73 m2
no glybenclamide, no alpha-glucosidaseinhibitor
no nateglimide
- If S.cr > 5, eGFR < 10 ml / min / 1.73 m2
prefer insulin

Overall Risk Factors for CKD Progression
1. Poor glycemic control2. Albuminuria & Proteinuria3. BP control & RAAS inhibition4. Baseline kidney function5. Drugs (ASA, NSAID) & radio-contrast, 5. Metabolic acidosis6. Acute kidney injury7. Diet8. Infection (local & systemic)9. Kidney stones10. Genetics & Races

Clin Exp Nephrol 2009; 13: 203-204.
Cumulative incidence of ESKD in CKD patients
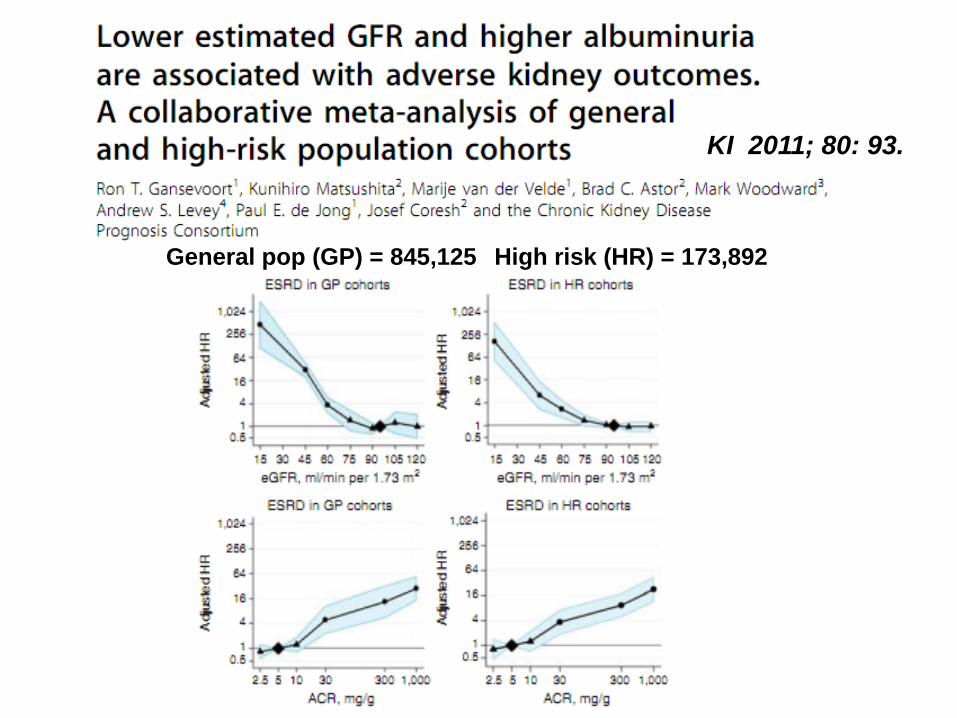
KI 2011; 80: 93.
General pop (GP) = 845,125 High risk (HR) = 173,892

Proportion with renal outcome
Atkins RC, et al. AJKD 2005; 45: 281
>50% decrease
0-50% decrease
>50% Increase
0-50% Increase

Jefferson JA, et al. KI 2008; 74: 22-36.

Schematic summary of some of the pathways and mediators that arebelieved to be involved in proteinuria-induced tubulointerstitial injury.
Zandi-Nejad K, et al. KI 2004; 66 (Suppl 92): S80.
Overall Risk Factors for CKD Progression
1. Poor glycemic control2. Albuminuria & Proteinuria3. BP control & RAAS inhibition4. Baseline kidney function5. Drugs (ASA, NSAID) & radio-contrast, 6. Metabolic acidosis7. Acute kidney injury8. Diet9. Infection (local & systemic)10.Kidney stones11. Genetics & Races

Standard control BP = 140/90 MAP = 105Intensive control BP = <125/75 MAP = 92 Appel LJ, et al. NEJM 2010; 363: 918.
IntensiveUprot./Ucr > 0.22
Uprot./Ucr < 0.22
Standard
Composite IO outcome(Scr x 2, ESRD or Death)

Ann Intern Med 2011; 154: 541.
dose not proveless than 130/80
300 to 1000 mg/d

Hemodynamic changes in Diabetic Nephropathy
- Systemic hypertension
- Glomerular hyperfiltration
- Mechanical stretch of GBM & Mesangial structure
- Tubulo-interstitial hypoperfusion& ischemia
KI 1997; 52: 985.J Pharmacol Sci 2009; 109: 24.
Effect of RASBlockade

Metabolic derangement in diabetic nephropathy
Angiotensinogen
AII synthesis@ podocytes
TGF-β
Mesang. Matrix deposition
Proteinuria
GBM thickening& adhesion to Bowman’s capsuleSlit diaphragm widening
Podocytes : - effacement- apoptosis - HSPG- loss of –ve charge at GBM
- α3β1 integrin- loss of nephrin - Detachment
Semin Nephron 2003: 23: 532.
Am J Physiol Renal Physiol 2006; 291: F1308.
T-I fibrosis
Glomerularsclerosis
ACEI / ARB
X
X
X
X

Progression Risk, Urinary Protein Excretion, and Treatment Effects of Angiotensin-Converting Enzyme Inhibitors in Nondiabetic Kidney Disease
Kent DM, et al. JASN 2007; 18: 1959 – 1965.
ACEi
Risk profiles1. Age2. Genger3. S.cr4. SBP5. Proteinuria
Rate of combinedoutcome (kidney failure or S.cr x 2) per year
30% reduction

80 mg / day10 mg / day
NEJM 2008; 358: 1547 – 1559.
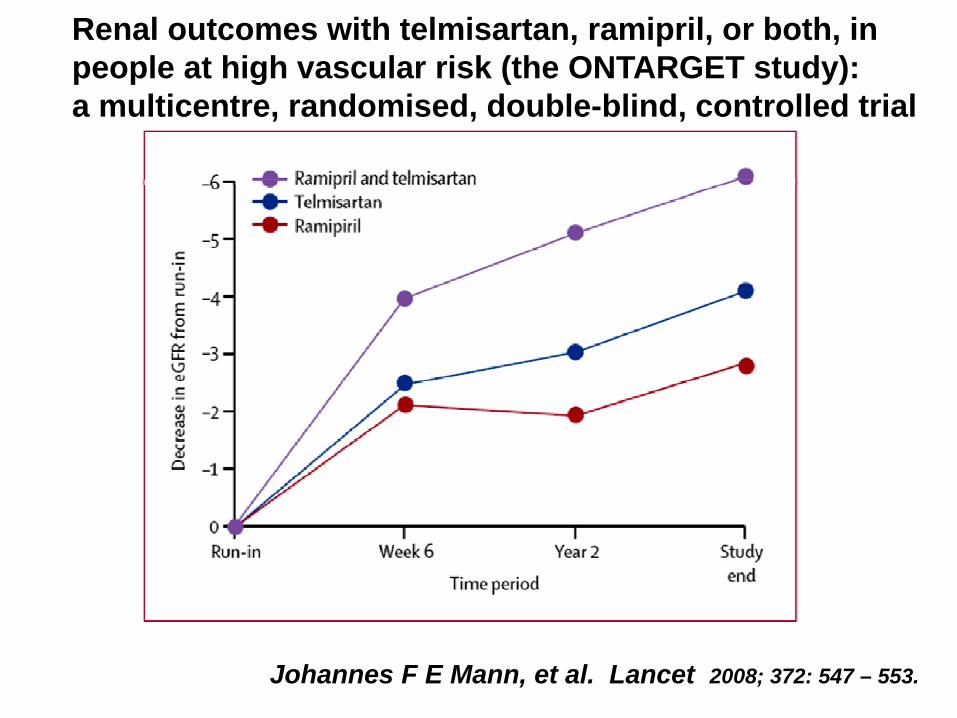
Johannes F E Mann, et al. Lancet 2008; 372: 547 – 553.
Renal outcomes with telmisartan, ramipril, or both, inpeople at high vascular risk (the ONTARGET study):a multicentre, randomised, double-blind, controlled trial

Aldosterone Antagonists for Preventing the Progression ofChronic Kidney Disease: A Systematic Review and Meta-analysis
Navaneethan SD, et al. CJASN 2009; 4: 542 – 551.

Overall Risk Factors for CKD Progression
1. Poor glycemic control2. Albuminuria & Proteinuria3. BP control & RAAS inhibition4. Baseline kidney function5. Drugs (ASA, NSAID) & radio-contrast, 6. Metabolic acidosis7. Acute kidney injury8. Diet9. Infection (local & systemic)10. Kidney stones11. Genetics & Races

KI 2011; 80: 93.
General pop (GP) = 845,125 High risk (HR) = 173,892

NEJM 2006; 354: 131-40.
Scr <3
Scr 3 - 5
20 mg
20 mg
Percentage Not Reaching the Primary End point

Overall Risk Factors for CKD Progression
1. Poor glycemic control2. Albuminuria & Proteinuria3. BP control & RAAS inhibition4. Baseline kidney function5. Drugs (ASA, NSAID) & radio-contrast, 6. Metabolic acidosis7. Acute kidney injury8. Diet9. Infection (local & systemic)10. Kidney stones11. Genetics & Races
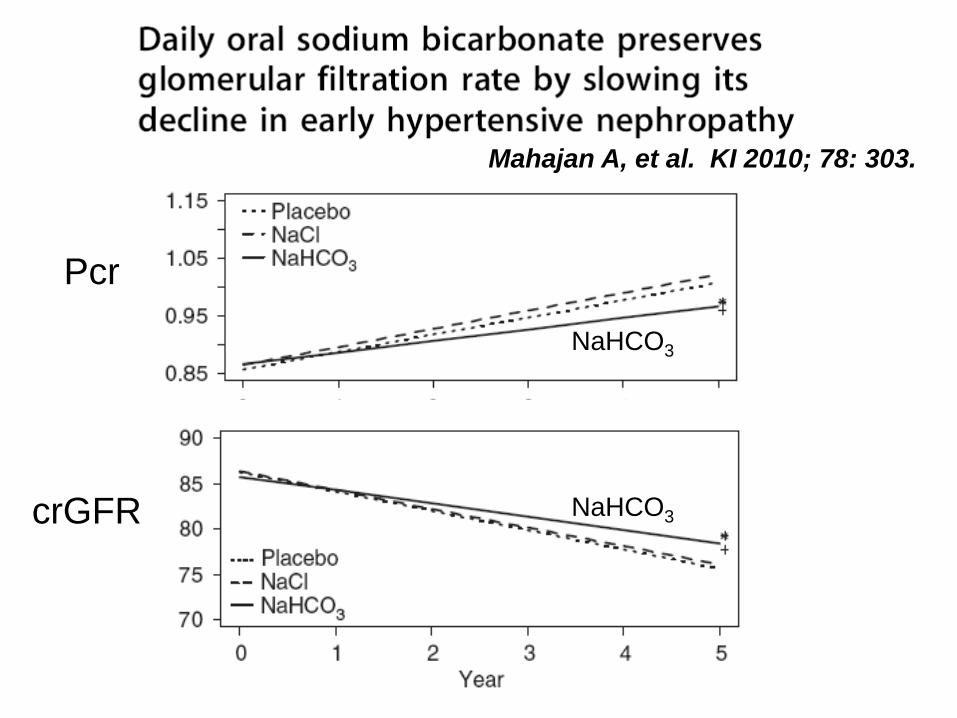
Pcr
crGFR
Mahajan A, et al. KI 2010; 78: 303.
NaHCO3
NaHCO3
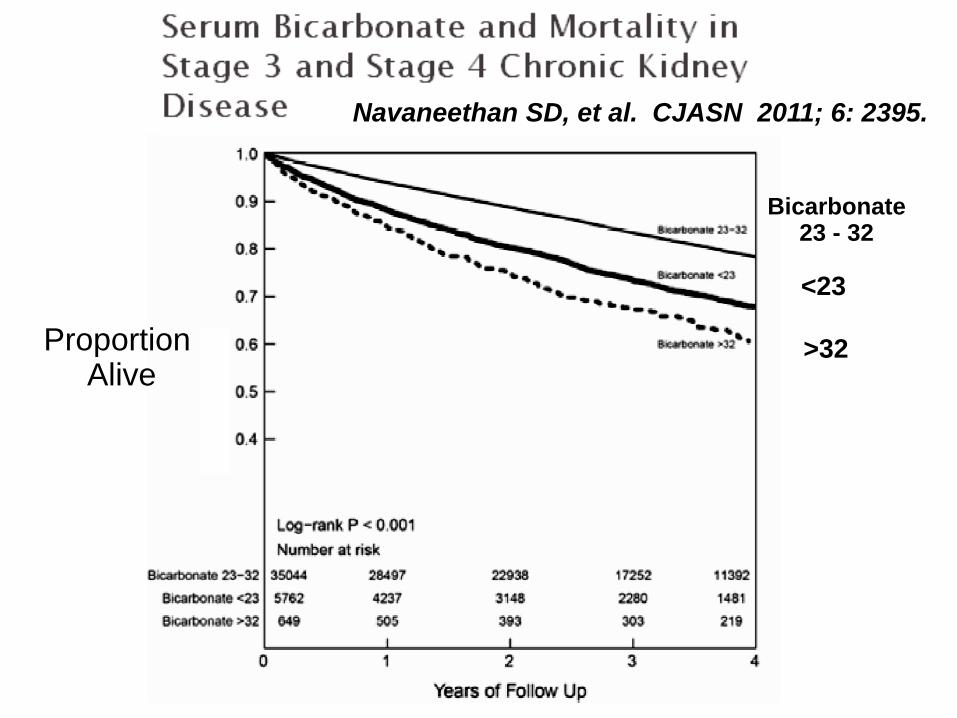
Navaneethan SD, et al. CJASN 2011; 6: 2395.
Proportion Alive
Bicarbonate23 - 32
<23
>32

Acute kidney injury predicts CKD progression
Chawla, et al. KI 2011; 79: 1361
Mean eGFR>79
61-79
<61
Mean eGFR
<61
61-79
>79
Overall Risk Factors for CKD Progression
1. Poor glycemic control2. Albuminuria & Proteinuria3. BP control & RAAS inhibition4. Baseline kidney function5. Drugs (ASA, NSAID) & radio-contrast, 6. Metabolic acidosis7. Acute kidney injury8. Diet ( protein, salt, phosphate )9. Infection (local & systemic)10. Kidney stones11. Genetics & Races

Clin Exp Nephrol 2009; 13: 231-233.
Recommend lifestyle modifications1. Salt intake 6 g / day
2. Vegetables & fruits
3. Cholesterol & saturated fatty acid
4. BMI < 25
5. Exercise
6. Alcohol
7. No smoking

Hypertension2009; 54: 482-8.
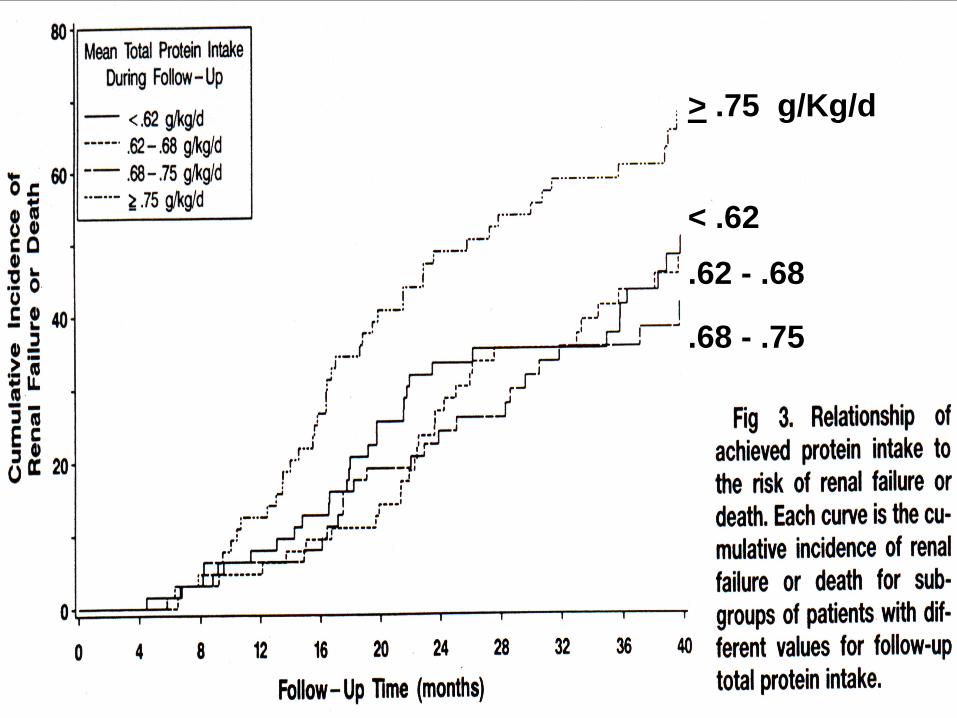
> .75 g/Kg/d
< .62
.62 - .68
.68 - .75

The Cochrane 2009, Issue 3
0.6
0.3-0.6
Less renal death on low protein

KI 2011: 79: 1341.
Adjusted HR
Adjusted HR


Bolland MJ, et al.BMJ 2010; 341: 3691.
AMI Stroke
Calcium
Placebo

Novel risk factors for CKD (2)
- Obesity ( + ) , obstructive sleep apnea
- Periodontal disease
- Low birth weight and nephron numbers.
- Low nephron no. salt-sensitive HT
- Low birth weight and CKD

KI 2011; 80: 1117.Wnt = Wingless + Integrin 1

( resident fibroblasts ) ( epithelial–to–mesenchymal transdifferentiation )
in renal interstitium
KI 2011; 80: 1119.

Promising intervention to delay CKD
- Renin inhibitor (ariskiren) : RAS, U.Alb / cr ratio- Pirfenidone : TGF-beta synthesis,
TNG-alpha signals, ROS scavenger
- Low MW heparin : restore negative charge on cell surfaces
proteininuria, anti-prolifn
- Pentoxifylline : proteinuria, urine TNF-alpha
- Ruboxistaurine mesylate : protein kinase C (PKC) –beta inhibitor
- AVP-receptor antagonists in ADPKD - Sulodexide
CKD system management1. Create awareness (Preventive > Curative)
- health care personnel ? weak- public ? weak
2. Screening - high risk ? late referral- tool ? S.cr
? eGFR? IT
3. Patient counseling & Empowerment - allied personnel ? who ? when
? where ? how? work load
4. Direct clinical care- MD vs. allied personnel
5. Research- IT, Registry

Effectiveness of community-based integrated CKD care program versus standard care program in Thailand.
Teerayut Jiamjariyaporn, Bhumirajanagarindra Kidney Institute, Bangkok.






อบรมผู้ป่วยและผู้ปรุงอาหาร


CKD Team
Will powerKnowledge
IT
Budget
Personnel
- Awareness- Screening- Counseling- Direct care- Research
Home care
อสม.
รพ.สต.