Embed Size (px)
Citation preview

Update:Transcatheter Aortic Valve Implantation
Ganesh ManoharanMBBCh, BAO, MD, FRCP(I), FRCP(Edin), FESC
Consultant Cardiologist, RVH, Belfast
Training Programme Director, Cardiology, NIMDTA
Hon Senior Lecturer, QUB

First clinical insertion of prosthetic valve
Dr Charles A Hufnagel1916 – 1989
Professor of SurgeryGeorgetown University
1952

Do Patients with Valvular Heart Disease Receive Treatment According to Established Guidelines?
The Euro Heart Survey on Valvular Heart Disease
• 92 hospitals from 25 countries• 5001 patients from April – July 2001
Surgery denied in 33% of symptomatic elderly
patients
Age and LV function were key reasons

Aortic Valve Replacement
• General anesthesia
• Sternotomy
• On pump
• Excellent results!
• Increasing mortality with age
• Increased mortality in redo procedures
• Increased mortality with comorbidities
• Increased morbidity in elderly patients:
• Longer ICU stay, hospital stay and recovery

Reference Pt number Pt Characteristics In-HospitalMortality
Filsoufi (2008) 231 ≥80yrs (48% CABG) 5.2
Ferrari (2010) 124 ≥80yrs (Isolated AVR) 5.4
de Vincentis (2008) 345 ≥80yrs (70% CABG) 7.5
Langanay (2006) 442 ≥80yrs (19% CABG) 7.5
Leontyev (2009) 282 ≥80yrs (Isolated AVR) 7.8
Melby (2007) 245 ≥80yrs (57% CABG) 9.0
Kolh (2007) 220 ≥80yrs (26% CABG) 9.0
Gulbins (2008) 236 ≥80yrs (91% CABG) 9.3
Bose (2007) 68 ≥80yrs (46% CABG) 13
Outcome of sAVR or sAVR+CABG in Elderly
9 Studies; Total 2193 patients Range: 5.2 – 13Weighted Av: 8.9%

Mean age 64.8±10.4
Age 70-80 as univariantpredictor
Risk with elderly: Bleeding, infection, wound healing, extended ICU and hospital stay, prolonged recovery,
mental state....

Philipp Bonhoeffer – 1st Pulmonary transcatheter valve implantation
Melody valve
12th of September 2000
Proof of Concept Design

16+ years since first TAVI
Prof Alan Cribier and the 1st TAVR patient
16 April 2002

Medtronic CoreValveSize 23, 26, 29, 31
Annulus: 18 -29mm
Edward SapienSize 23, 26, 29
Annulus: 18-27mm
18F TF for all
TF (16F eS) and TA
TF (18F eS) and TA
TF (20F eS)and TA
eS = e-Sheath
1st Gen Work-Horse TAVI Devices
G Manoharan, Royal Victoria, Belfast

1st TAVI in Ireland: 6th February 2008
Funding secured for 2 years from Ulster Garden Villages, Cardiac Research Funds, RVH and The Heart Trust Fund

Features of New CE Mark Devices
Repositionable
External Skirt
Device Fixation
Conformable Frame
Lower Profile
Delivery System
Improved Outcome

Current Generation TAVI Devices
Images not to scale
Edwards
Sapien
Medtronic
Evolut R
Abbott
PorticoBoston Scientific
Balloon
Expandable
Self
Expanding
Self
Expanding
Mechanically
Expandable
X
SymetisLotus
Self
Expanding
Medtronic
Evolut PRO
Self
Expanding

TAVI Delivery Systems

TAVI Access Options
• Transfemoral
• Subclavian
• Axillary
• Direct Aortic
• Transapical
• Carotid
• Transcaval

Post Procedure Angio

Self-Expanding: Resheatable and Repositionable

TAVI Procedure: Balloon Expandable

Evidence for Suitable Patients
Randomised Clinical Data available:
1. Inoperable patients
2. High risk patients
3. Intermediate risk patients

Inoperable and High Risk


TAVI Superior to Medical Therapy

TAVI = SAVR


TAVI Superior to SAVR


3 yr Follow-UP: TAVI Superior to SAVR

Valve DurabilityThus far, TAVI durability maintained



Intermediate Risk Patients



TAVI (all access) Similar to SAVR in Intermediate Risk Patients

Trans-Femoral TAVI Superior to SAVR in Intermediate Risk Patients



Intermediate Surgical Risk Predicted risk of operative mortality ≥3% and <15%
Heart Team EvaluationAssess inclusion/exclusion
Risk classification
RandomizationStratified by need for revascularization
TAVR SAVR
TAVR + PCI SAVR + CABGTAVR only SAVR only
Baseline neurological assessments
Screening CommitteeConfirmed eligibility
37
SURTAVI Trial Design
Reardon et al; NEJM 2017

n (%) or mean ± SD TAVR (N=864) SAVR (N=796)
Age, years 79.9 ± 6.2 79.7 ± 6.1
Male sex 498 (57.6) 438 (55.0)
Body surface area, m2 1.9 ± 0.2 1.9 ± 0.2
STS PROM, % 4.4 ± 1.5 4.5 ± 1.6
Logistic EuroSCORE, % 11.9 ± 7.6 11.6 ± 8.0
Diabetes mellitus 295 (34.1) 277 (34.8)
Serum creatinine >2 mg/dl 14 (1.6) 17 (2.1)
Prior stroke 57 (6.6) 57 (7.2)
Prior TIA 58 (6.7) 46 (5.8)
Peripheral vascular disease 266 (30.8) 238 (29.9)
Permanent pacemaker 84 (9.7) 72 (9.0)
Baseline Characteristics*
*mITT population; no significant difference in any baseline characteristics 38

0%
5%
10%
15%
20%
25%
30%
0 6 12 18 24
All-
Cau
se M
ort
alit
y o
r D
isab
ling
Stro
ke
Months Post-ProcedureNo. at Risk
796 674 555 407 241
864 755 612 456 272TAVR
SAVR
All-Cause Mortality or Disabling Stroke
24 Months
TAVR SAVR
12.6% 14.0%
39
TAVR = SAVR

0%
2%
4%
6%
8%
10%
0 6 12 18 24
Dis
ablin
g St
roke
Months Post-ProcedureNo. at Risk
796 674 555 407 241
864 755 612 456 272TAVR
SAVR
Disabling Stroke
24 Months
TAVR SAVR95% CI for Difference
2.6% 4.5% -4.0, 0.1
40
TAVR > SAVR

Hemodynamics*
Ao
rtic
Val
ve A
rea,
cm
2
AV
Mean
Grad
ient, m
m H
g
TAVR had significantly better valve performance over SAVR at all follow-up visits
*Core lab adjudicated 41

Total Aortic Regurgitation*
61% 93% 61% 90% 60% 90%
36%
7%
34%
9%
35%
9%3%
1%5%
1%5%
1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
TAVR(N=832)
SAVR(N=707)
TAVR(N=599)
SAVR(N=506)
TAVR(N=299)
SAVR(N=244)
Discharge 12 Months 24 Months
Severe
Moderate
Mild
None/trace
* Implanted population, core lab adjudicated 42
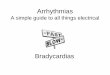
Improved PVL outcome in TAVI compared to High Risk IDE study possibly due to use of CT sizing and adherence to best practice

• TAVR had significantly less 30 day stroke, AKI, atrial fibrillation and transfusion use and a superior quality of life at 30 days.
• TAVR resulted in significantly improved AV hemodynamics with lower mean gradients and larger aortic valve areas than SAVR through 24 months.
• SAVR had less residual aortic regurgitation, major vascular complications and fewer new pacemakers.
• Need for a new pacemaker after TAVR was not associated with increased mortality.
Summary
43

Current Gen TAVI: 30D Moderate/Severe PVL
1213
16.9
24.2
911.5
3.5 4
1 1.7
0
5
10
15
20
25
30
Partner High Risk:Sapien
Advance: CoreValve Partner 2: Sapien Partner 2: XT CoreValve: High Risk CoreValve: ExtremeRisk
Sapien 3 Portico Lotus Direct Flow
Mod/severe (%)
Evolut R Pro = 0 Mod/Severe





SAVR vs TAVI

The US FDA have approved 2 new studies using the new generation TAVI devices (Evolut R and Sapien 3) in low
risk surgical patientsRESULTS: ACC 2019!

TAVI in Clinical Practice Today: Summary 1
• Standard of care for high risk and inoperable patients with symptomatic severe AV disease
• Overall numbers are increasing in each unit
• ‘Moderate risk’ patients are increasingly being offered TAVI
• Further increase expected, being driven by data and patient choice

TAVI in Clinical Practice Today: Summary 2
• Technological advances are impacting positively on TAVI outcome
• Improving outcomes are also due to better patient selection (HEART Team) and operator expertise
• TAVI under local anaesthesia increasing
• Low risk patient - will depend on x2 studies currently ongoing (FDA studies)

Thank You
Ganesh ManoharanMBBCh, BAO, MD, FRCP(I), FRCP(Edin), FESC
Consultant Cardiologist, RVH, Belfast
Training Programme Director, Cardiology, NIMDTA
Hon Senior Lecturer, QUB