Embed Size (px)
Citation preview

Updates in Neonatal
Resuscitation:
Out-of-hospital deliveries 2014
E. Preka, S. Redant, D. Biarent
Service des Urgences Pediatriques HUDERFsemina
ires i
ris
Overview
• Introduction
• Physiology of birth
• Considerations in every delivery
– Cord clamping (time, sterile procedure)
– Temperature management
– Pulse oxymetry : Air VS 100%Oxygen
• Basic NLS instructions
• Particular cases (meconium, therapeutic hypothermia)semina
ires i
ris
Introduction
• Out-of-hospital Delivery (OHD) : Planned or unplanned deliveries
(home, road, out-of-bloc arrival in the hospital)
• Is it often?
0,6% in USA, 0,5% in France, 0,8% in italy,
0,15% in Finland
Peoples’ needs change….
30% in Netherlands, 3% in UK, 1% in USA
• Who’s more at risk ?
• Is it more dangerous ?
K. Viisainen, Acta Obstet Gynecol Scand 1999
Lancet 2010
semina
ires i
ris
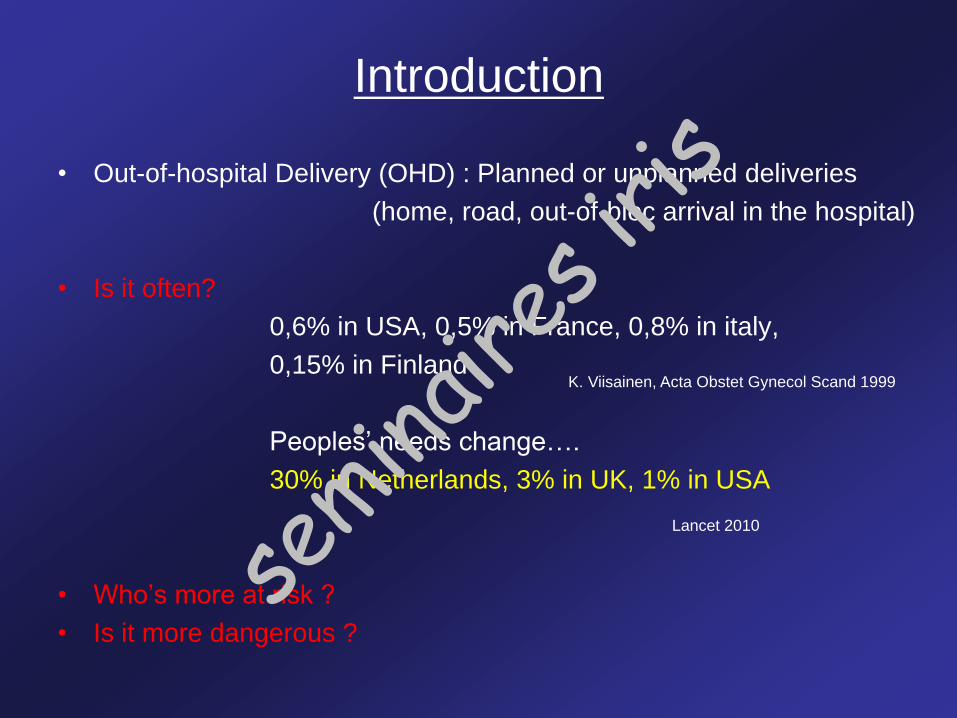
• France : retrospective case-
control study 2007-2009
• Inclusion criteria : a live birth
and no planned home birth
• Exclusion criteria : GA < 22w
and BW < 500gr
• 4 independent risk factors :
- multiparity
- unemployement
- lack/poor antenatal care
- a travel time > 45 min
Background characteristics of OHD (2)
I. Renesme, Acta Pediatrica 2013
semina
ires i
ris
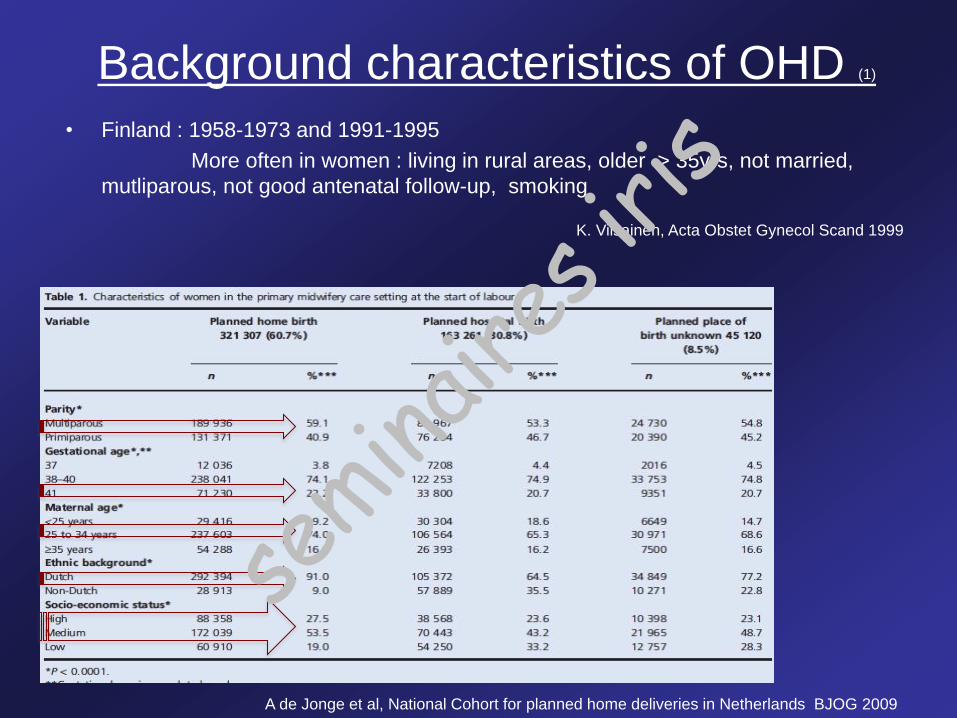
• Finland : 1958-1973 and 1991-1995
More often in women : living in rural areas, older > 35yrs, not married,
mutliparous, not good antenatal follow-up, smoking
Background characteristics of OHD (1)
K. Viisainen, Acta Obstet Gynecol Scand 1999
A de Jonge et al, National Cohort for planned home deliveries in Netherlands BJOG 2009
semina
ires i
ris
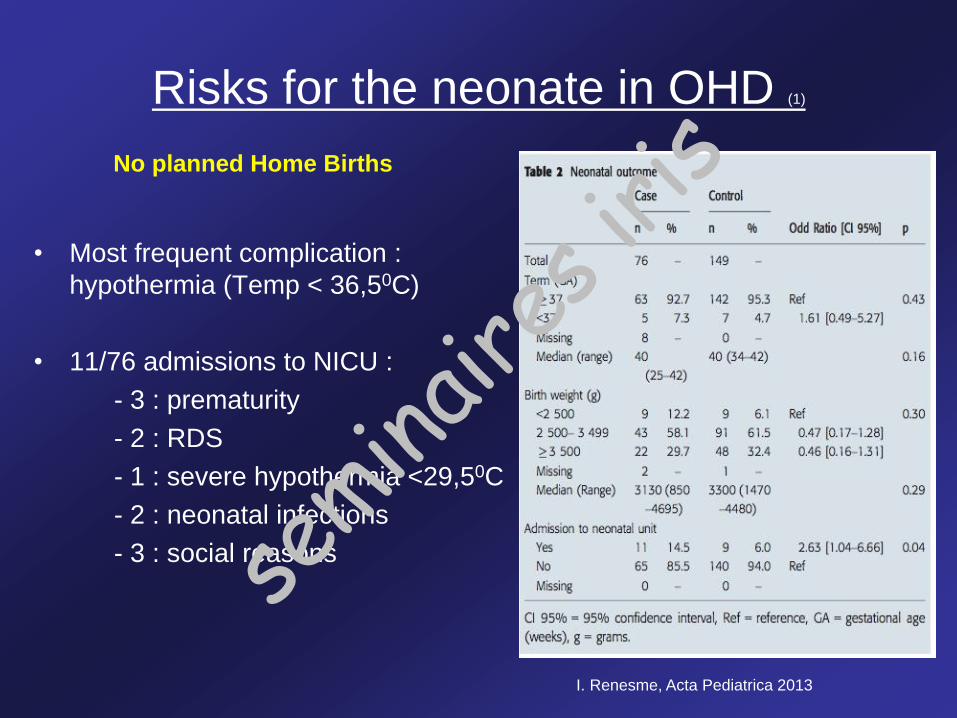
Risks for the neonate in OHD (1)
• Most frequent complication :
hypothermia (Temp < 36,50C)
• 11/76 admissions to NICU :
- 3 : prematurity
- 2 : RDS
- 1 : severe hypothermia <29,50C
- 2 : neonatal infections
- 3 : social reasons
I. Renesme, Acta Pediatrica 2013
No planned Home Births
semina
ires i
ris
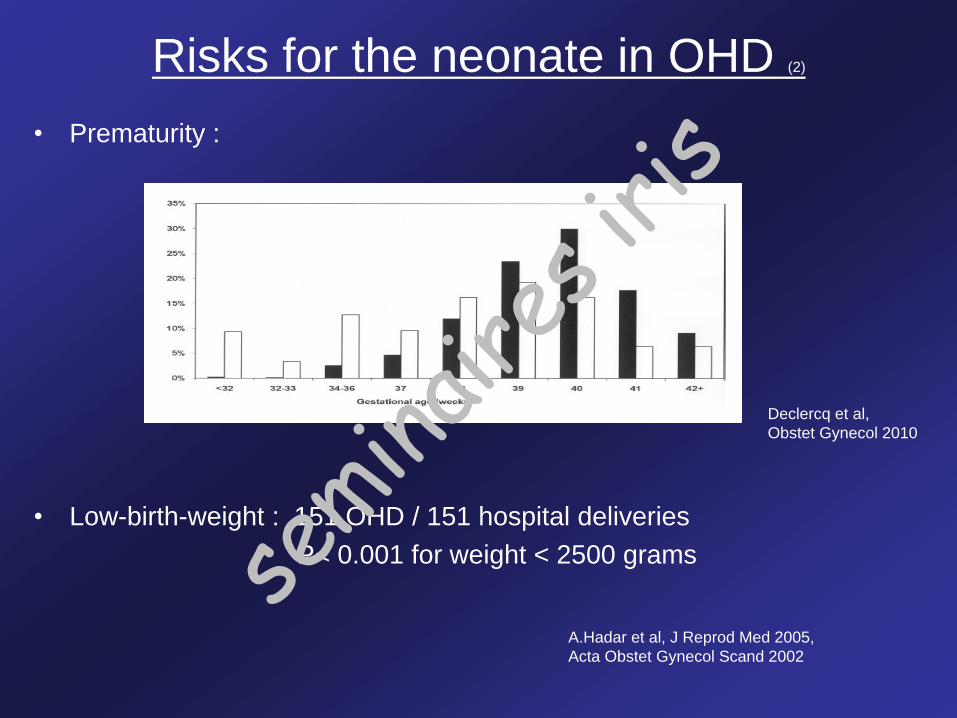
Risks for the neonate in OHD (2)
• Prematurity :
• Low-birth-weight : 151 OHD / 151 hospital deliveries
P< 0.001 for weight < 2500 grams
Declercq et al,
Obstet Gynecol 2010
A.Hadar et al, J Reprod Med 2005,
Acta Obstet Gynecol Scand 2002
semina
ires i
ris
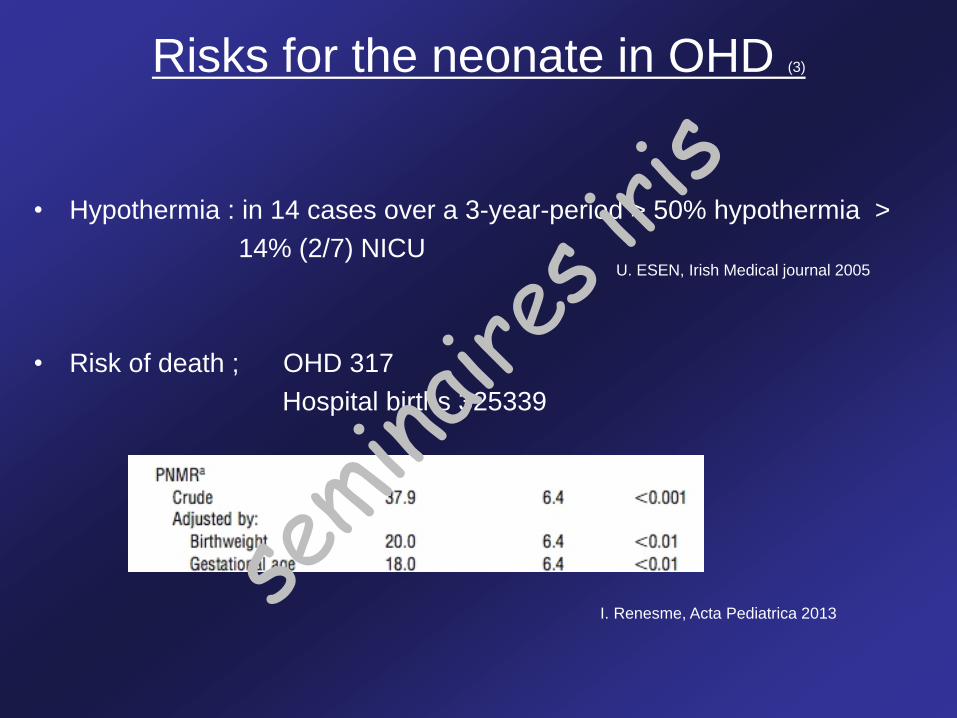
Risks for the neonate in OHD (3)
• Hypothermia : in 14 cases over a 3-year-period > 50% hypothermia >
14% (2/7) NICU
• Risk of death ; OHD 317
Hospital births 325339
I. Renesme, Acta Pediatrica 2013
U. ESEN, Irish Medical journal 2005
semina
ires i
ris
Results……
Perinatal Mortality> no significant differences
Admission to the NICU> less for the group ‘’Planned Home Birth’’
Risks for the neonate in OHD (4)
semina
ires i
ris
Overview• Introduction
• Physiology of birth
• Considerations in every delivery
– Cord clamping (time, sterile procedure)
– Temperature management
– Pulse oxymetry : Air VS 100%Oxygen
• Basic NLS instructions
• Particular cases (meconium, therapeutic hypothermia)semina
ires i
ris
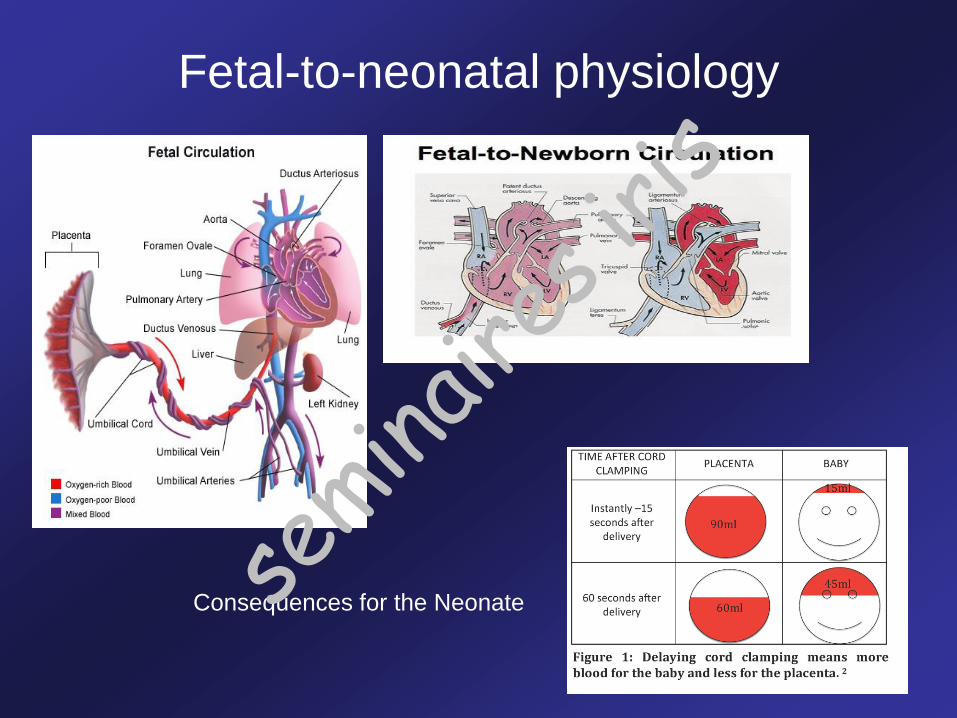
Fetal-to-neonatal physiology
Consequences for the Neonate semina
ires i
ris
Considerations
• Cord clamping
• Temperature control
• Air or 100% oxygen
semina
ires i
ris
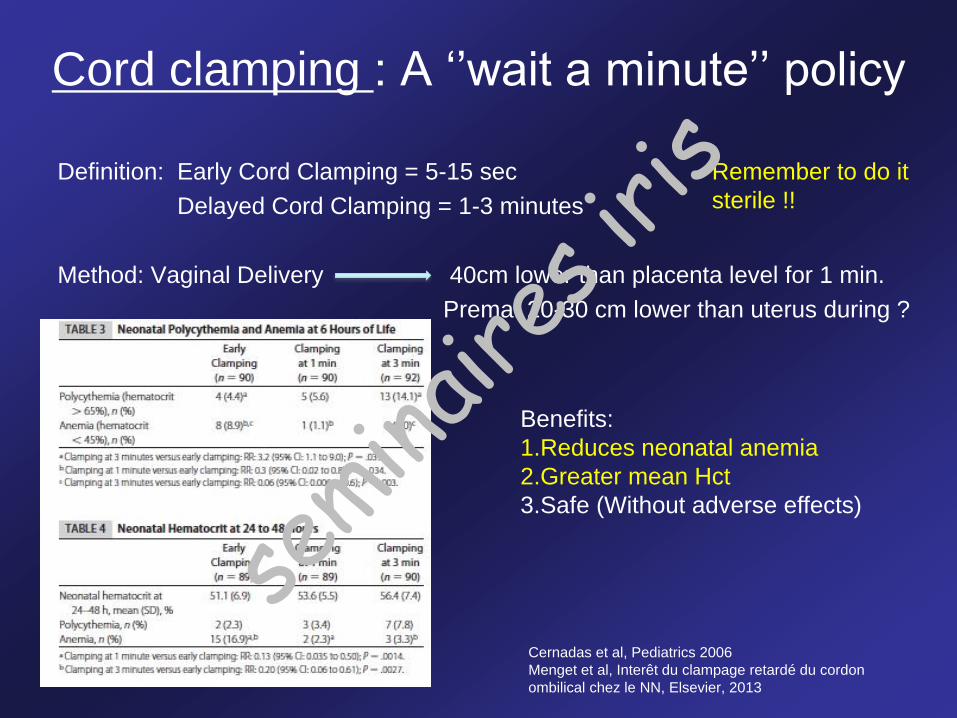
Definition: Early Cord Clamping = 5-15 sec
Delayed Cord Clamping = 1-3 minutes
Method: Vaginal Delivery 40cm lower than placenta level for 1 min.
Prema: 20-30 cm lower than uterus during ?
45-60s.
Cord clamping : A ‘’wait a minute’’ policy
Cernadas et al, Pediatrics 2006
Menget et al, Interêt du clampage retardé du cordon
ombilical chez le NN, Elsevier, 2013
Benefits:
1.Reduces neonatal anemia
2.Greater mean Hct
3.Safe (Without adverse effects)
Remember to do it
sterile !!
semina
ires i
ris
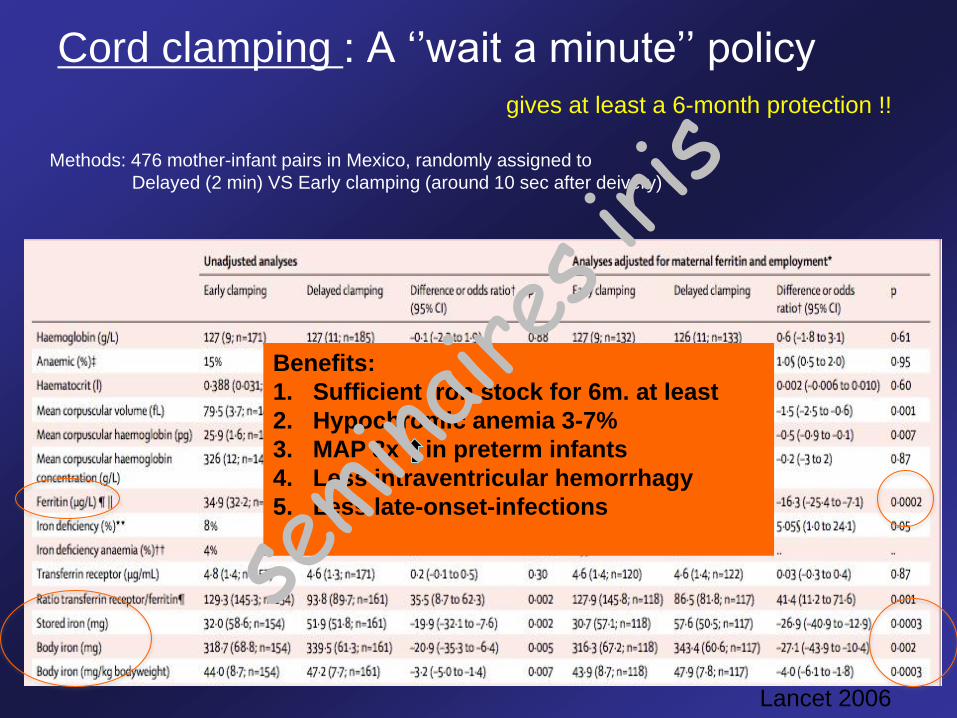
Cord clamping : A ‘’wait a minute’’ policy
gives at least a 6-month protection !!
Lancet 2006
Methods: 476 mother-infant pairs in Mexico, randomly assigned to
Delayed (2 min) VS Early clamping (around 10 sec after deivery)
Benefits:
1. Sufficient iron stock for 6m. at least
2. Hypochromic anemia 3-7%
3. MAP 3x in preterm infants
4. Less intraventricular hemorrhagy
5. Less late-onset-infections
semina
ires i
ris
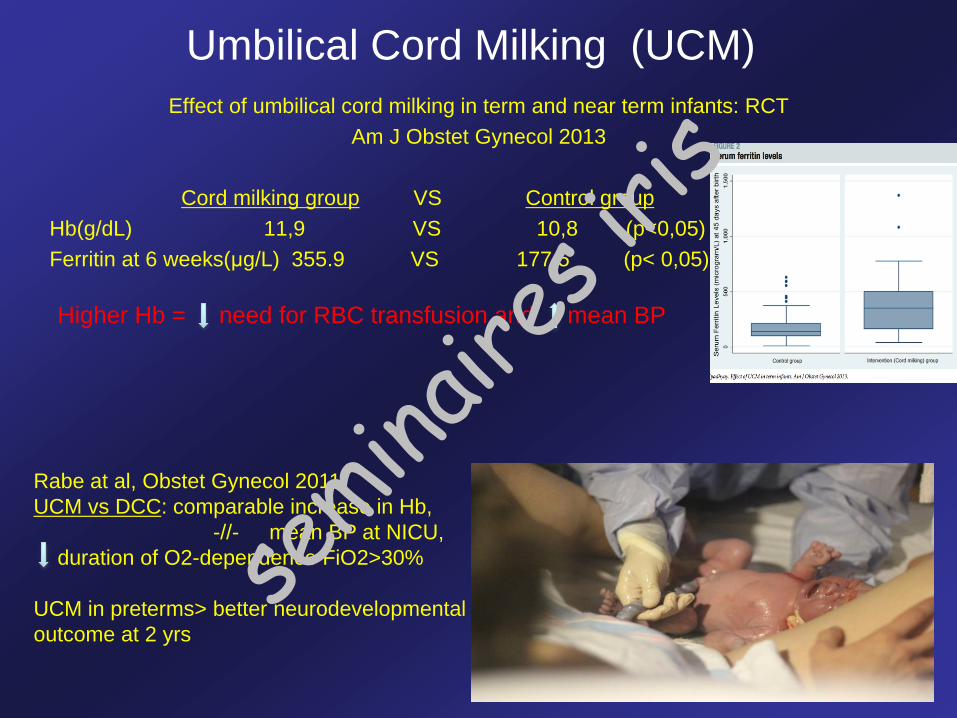
Umbilical Cord Milking (UCM)
Effect of umbilical cord milking in term and near term infants: RCT
Am J Obstet Gynecol 2013
Cord milking group VS Control group
Hb(g/dL) 11,9 VS 10,8 (p<0,05)
Ferritin at 6 weeks(μg/L) 355.9 VS 177,5 (p< 0,05)
Higher Hb = need for RBC transfusion and mean BP
Rabe at al, Obstet Gynecol 2011
UCM vs DCC: comparable increase in Hb,
-//- mean BP at NICU,
duration of O2-dependence FiO2>30%
UCM in preterms> better neurodevelopmental
outcome at 2 yrs
semina
ires i
ris
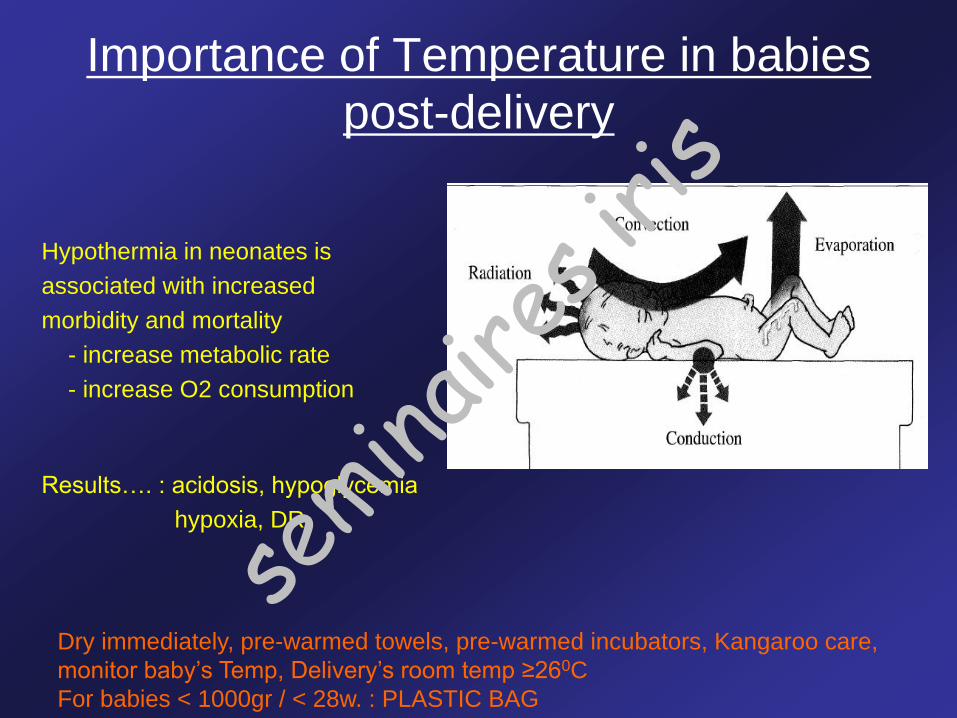
Importance of Temperature in babies
post-delivery
Hypothermia in neonates is
associated with increased
morbidity and mortality
- increase metabolic rate
- increase O2 consumption
Results…. : acidosis, hypoglycemia
hypoxia, DR
Dry immediately, pre-warmed towels, pre-warmed incubators, Kangaroo care,
monitor baby’s Temp, Delivery’s room temp ≥260C
For babies < 1000gr / < 28w. : PLASTIC BAG
semina
ires i
ris
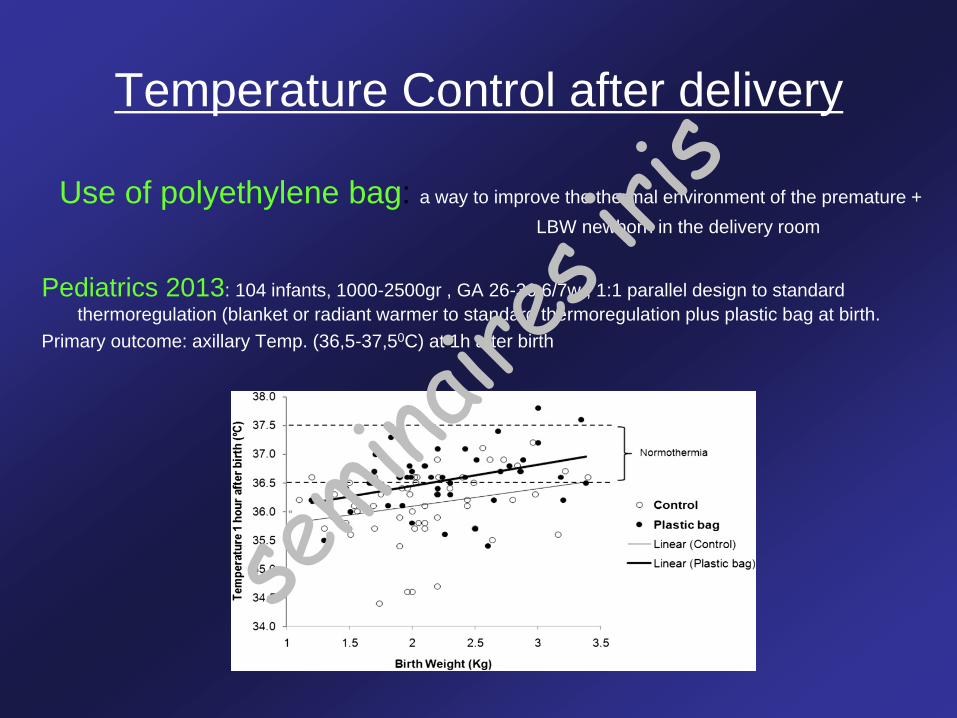
Temperature Control after delivery
Use of polyethylene bag: a way to improve the thermal environment of the premature +
LBW newborn in the delivery room
Pediatrics 2013: 104 infants, 1000-2500gr , GA 26-36 6/7w., 1:1 parallel design to standard
thermoregulation (blanket or radiant warmer to standard thermoregulation plus plastic bag at birth.
Primary outcome: axillary Temp. (36,5-37,50C) at 1h after birth
semina
ires i
ris
Air or 100% Oxygen
Successful REA at delivery = rapid establishment of pulmonary gas exchange
• Oxygen Paradox : oxidative stress !!
• RCT in asphyxiated newborn babies: Air = 100% O2
Air more effective in short term and less deleterious effects on immature
human brain
• Put Sat.O2 (wait 2 min…)
• Don’t trust the color
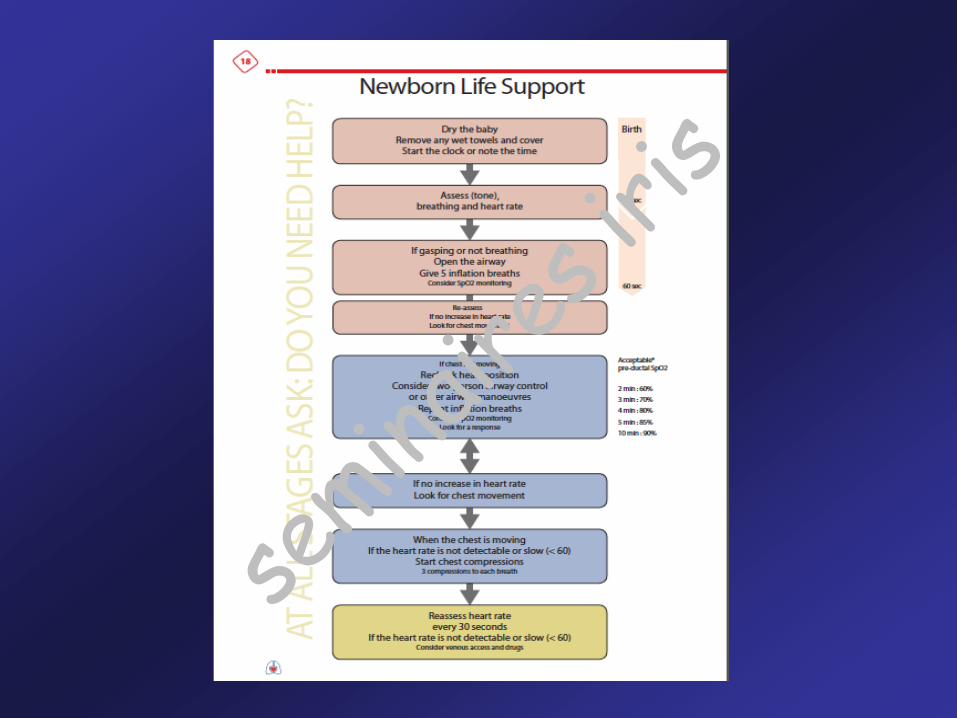
ERC 2010: 2 min : 60%
3 min : 70%
4 min : 80%
5 min : 85%
10 min : 90%
Koch et al, Cereb Blood Flow Metab 2008
semina
ires i
ris
Air or 100% Oxygen
Recommendation ERC 2010 :
Term infants: Start with Air (FiO2 21%)
if despite effective ventilation, no increase in HR/O2 ->>>> Air+Oxygen
Premature babies < 32weeks: Start with Oxygen (FiO2 21-30%)
and then adjust depending on the Sat.O2
Method: 5 first inflations
Pression: start with +/- 20 cm H2O
semina
ires i
ris
Intubate or not? Indications
• Meconium Aspiration Syndrome
• If bag-mask ventilation is ineffective or prolonged
• When Chest Compressions are performed
• Special circumstance: Congenital Diaphragmatic Hernia,
BW < 1000gr
ERC for babies at birth, 2010
Depends on the
experience of the person
responsible…
semina
ires i
ris
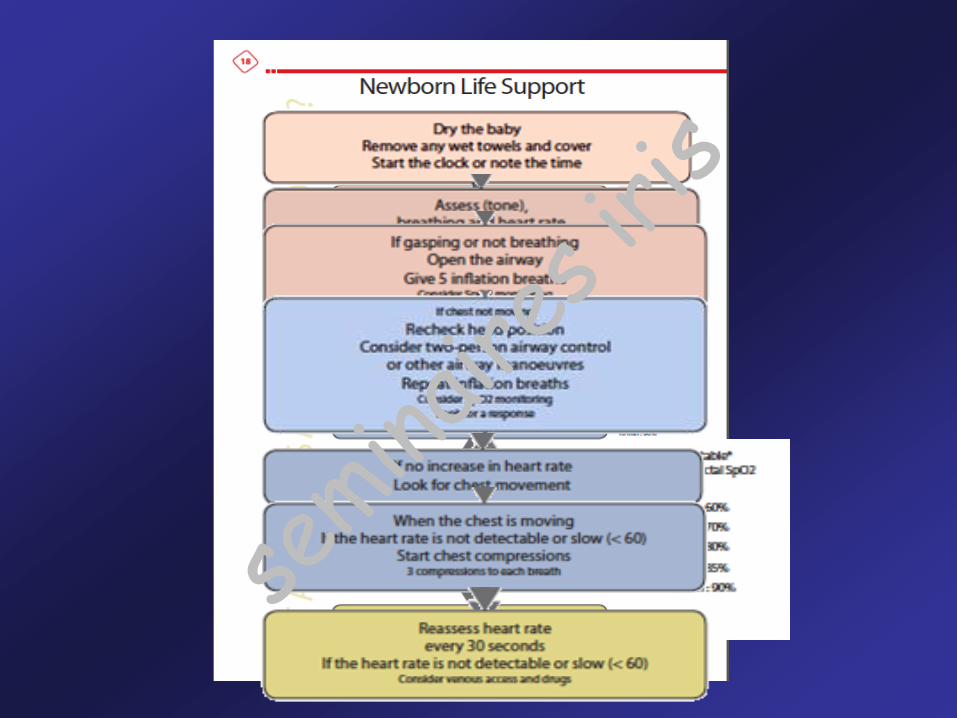
European Resuscitation Council
Resuscitation of babies at birth 2010
1. Preparation
1. Planned Home Deliveries
1. Equipment and environment PREPARATION !!!!
1. Temperature control
1. Initial assessment (FC, FR/Satu, Colour, Tone)
Acta Paediatr 1992, Methods of resuscitation in low-Apgar-
score newborn infants--a national survey in Sweden
of 100,000 babies in 1yr, only 1% needed resuscitation at
delivery and only 0,2% needed IT
( limitations, awareness of mother, at least 2
persons: one fully trained in mask ventilation and
chest compressions)
(exposure of the newborn to cold stress -> lower
SatO2%, metabolic acidosis!)
APGAR does not identify babies that
need resuscitation !!!!!!
semina
ires i
ris
Initial assessment :
- Breathing : rate, depth, symmetry, gasp?, grunting?
- Heart rate : USE your stethoscope !
- Colour : poor means of judjing oxygenation
- Tone
European Resuscitation Council
Resuscitation of babies at birth 2010
semina
ires i
ris

Classification according to initial assessment :
1. Vigorous breathing/crying
Good tone
HR > 100bpm
2. Breathing inadequaly or apnoeic
Normal or reduced tone
HR < 100 bpm
3. Breathing inadequaly or apnoeic
Floppy, often pale (poor perfusion)
Low/ indetectable HR
European Resuscitation Council
Resuscitation of babies at birth 2010
Dry only, wrap
Skin-to-skin
Dry-wrap
Mask inflation
+/- chest compressions
Dry-wrap
Airway control (air inflation and ventilation)
+/- chest compressions
+/- drugssemina
ires i
ris
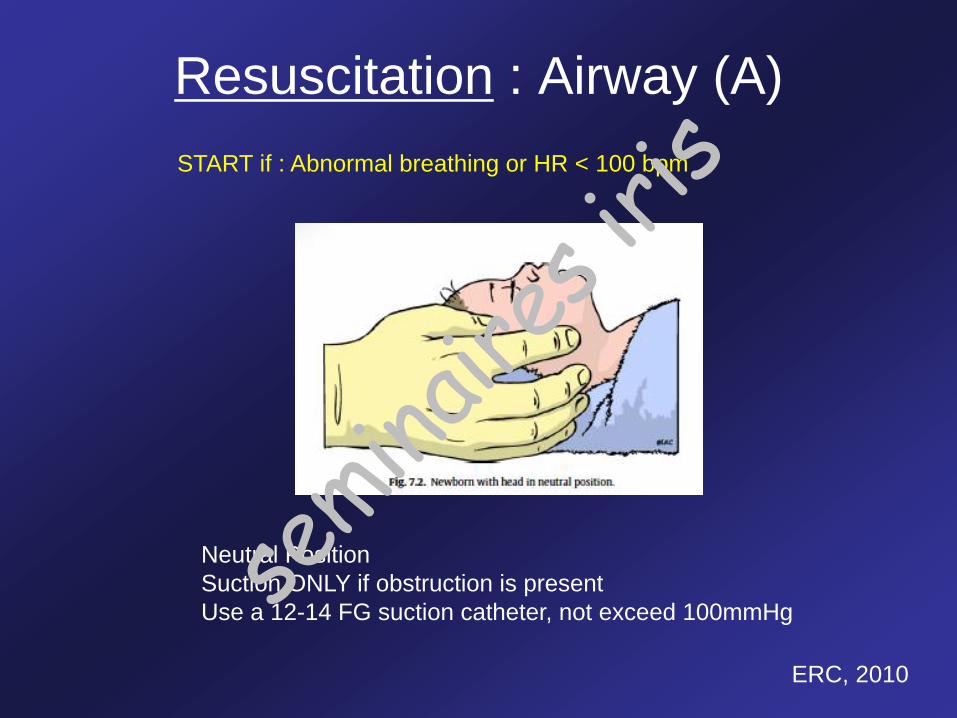
Resuscitation : Airway (A)
Neutral Position
Suction ONLY if obstruction is present
Use a 12-14 FG suction catheter, not exceed 100mmHg
ERC, 2010
START if : Abnormal breathing or HR < 100 bpm
semina
ires i
ris
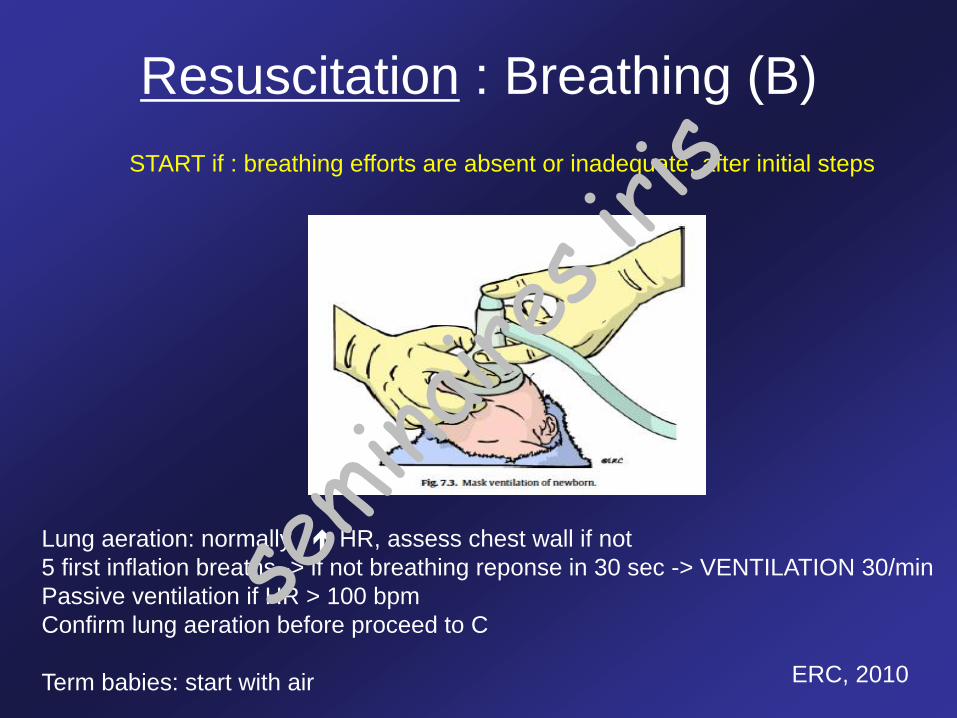
Resuscitation : Breathing (B)
START if : breathing efforts are absent or inadequate, after initial steps
Lung aeration: normally HR, assess chest wall if not
5 first inflation breaths -> if not breathing reponse in 30 sec -> VENTILATION 30/min
Passive ventilation if HR > 100 bpm
Confirm lung aeration before proceed to C
Term babies: start with air ERC, 2010
semina
ires i
ris
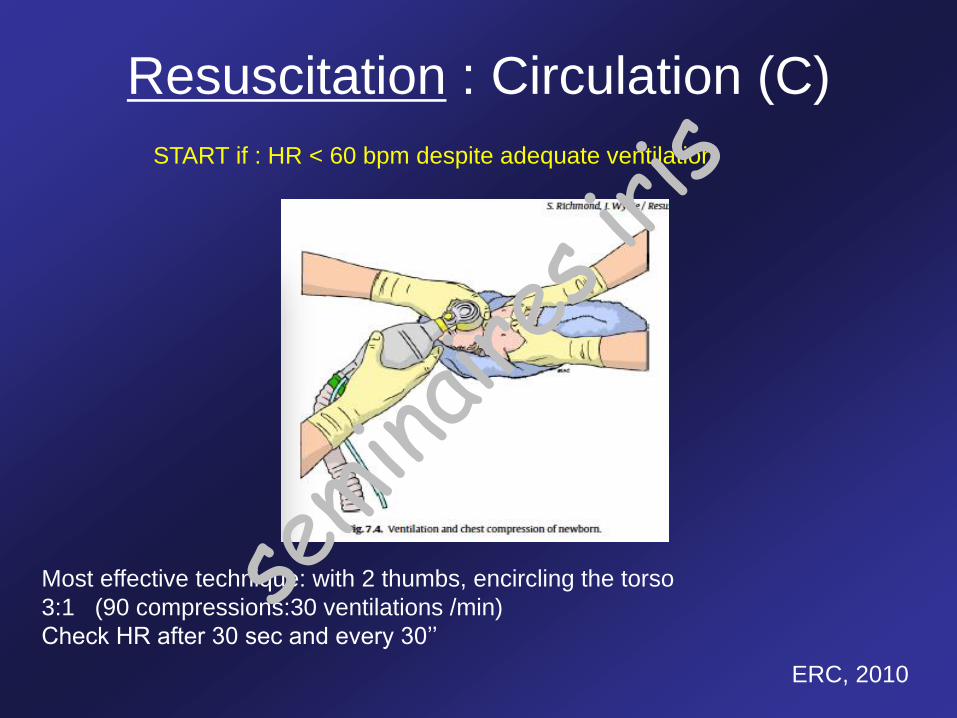
Resuscitation : Circulation (C)
START if : HR < 60 bpm despite adequate ventilation
Most effective technique: with 2 thumbs, encircling the torso
3:1 (90 compressions:30 ventilations /min)
Check HR after 30 sec and every 30’’
ERC, 2010
semina
ires i
ris
• STOP Resuscitation if :
- HR not detectable for 10 minutes
- desicion is often much more complex…
• Communication with the parents
Resuscitation : Until when ?
semina
ires i
ris
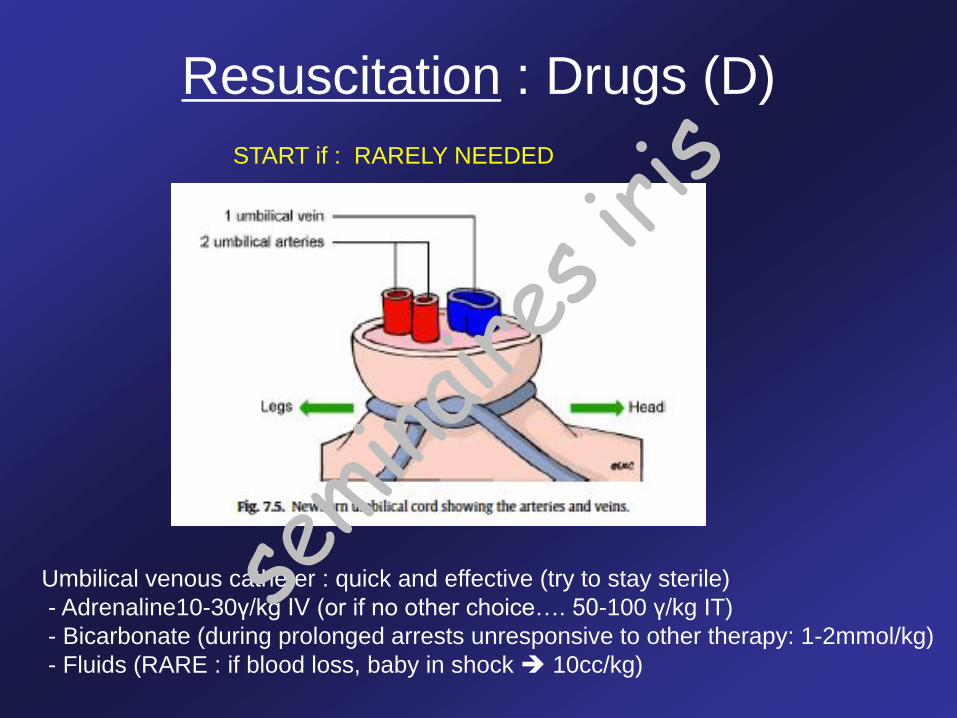
Resuscitation : Drugs (D)
START if : RARELY NEEDED
Umbilical venous catheter : quick and effective (try to stay sterile)
- Adrenaline10-30γ/kg IV (or if no other choice…. 50-100 γ/kg IT)
- Bicarbonate (during prolonged arrests unresponsive to other therapy: 1-2mmol/kg)
- Fluids (RARE : if blood loss, baby in shock 10cc/kg)
semina
ires i
ris
semina
ires i
ris
semina
ires i
ris

PARTICULAR CASES
Meconium
Induced hypothermia.
semina
ires i
ris
Meconium
• 12-15% of all newborn infants : 3-10% of those develop MAS
• Since mid-1970s (and for 25 years): Intubation in order to suction out the trachea
• Wiswell TE et al, Pediatrics 2002
RCT with 2000 infants: Intubation+trachea suctioning OR expectant management
Vigorous immediately (HR >100bpm, good respiratory effort, normal tone)
No differences in outcome
• ERC 2010
If feasible: direct oropharyngeal + tracheal aspiration of non-vigorous babies.
If intubation prolonged/unsuccessful : mask ventilation !!!!
TRUTH : Not enough data (RCT studies…clinical arguments…)
Wiswell ET, Respiratory Care 2011
semina
ires i
ris
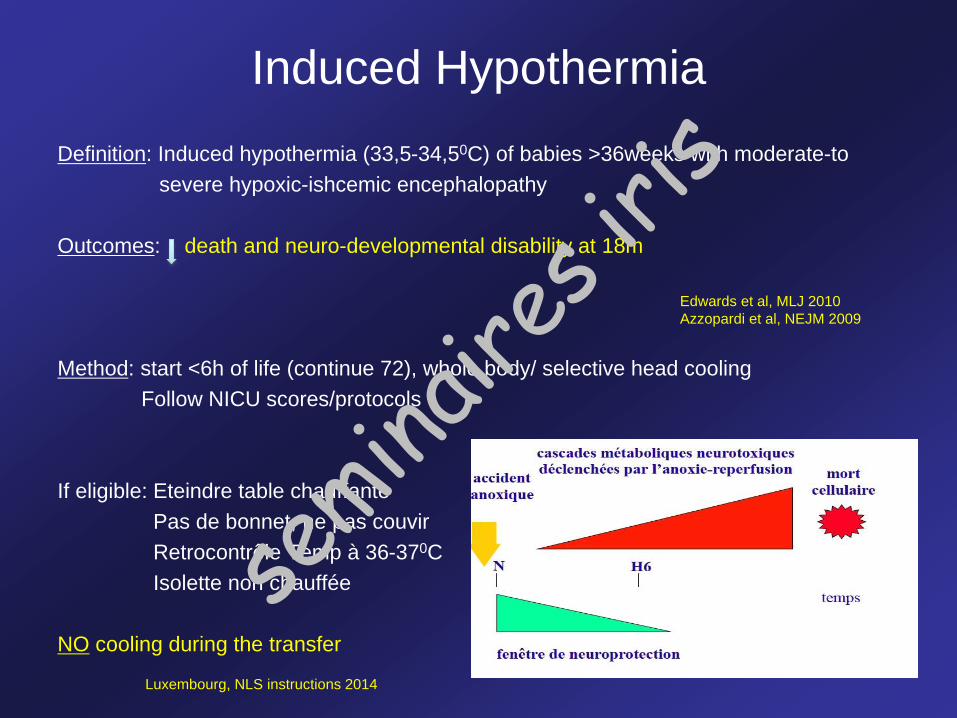
Induced Hypothermia
Definition: Induced hypothermia (33,5-34,50C) of babies >36weeks with moderate-to
severe hypoxic-ishcemic encephalopathy
Outcomes: death and neuro-developmental disability at 18m
Method: start <6h of life (continue 72), whole body/ selective head cooling
Follow NICU scores/protocols
If eligible: Eteindre table chauffante
Pas de bonnet, ne pas couvir
Retrocontrôle Temp à 36-370C
Isolette non chauffée
NO cooling during the transfer
Edwards et al, MLJ 2010
Azzopardi et al, NEJM 2009
Luxembourg, NLS instructions 2014
semina
ires i
ris
Take Home Message
• An out-of-hospital delivery becomes the more and more usual in our
societies
- Safe for low-risk-pregnancies
- Unsafe for all the rest…
• Remind regurarly your NLS skills
• Remember:
- A ‘wait-a-minute’’ policy for cord clamping
- Keep the baby’s temperature 36,5-37,50C
semina
ires i
ris
Merci pour votre attention…
Questions ?semina
ires i
ris
![hernia of the umbilical cord [وضع التوافق] of the umbilical cord.pdf · Umbilical cord hernia…cont Conclusion: ¾Hernia of the umbilical cord is a rare entityy, of the](https://img.pdfslide.net/doc/110x75/5ea7ce695a148409cd011fd0/hernia-of-the-umbilical-cord-of-the-umbilical-cordpdf.jpg)