Embed Size (px)
Citation preview
ACOFP 54th Annual Convention & Scientific Seminars
Urgency vs. Emergency: Pearls for the Urgent Care Physician
Lindsay Saleski, DO, MBA, FACOEP
3/9/2017
1
Urgency vs. Emergency
Pearls for the Urgent Care
PhysicianLINDSAY TJIATTAS-SALESKI DO, MBA, FACOEP
FAMILY PRACTICE/EMERGENCY MEDICINE
MIDLANDS EMERGENCY PHYSICIANS
PALMETTO HEALTH TUOMEY
Objectives
To provide the urgent care physician with evidence based
information regarding common outpatient presentations, initial
treatment strategies and potential need for more emergent care.
3/9/2017
2
Outline
Head trauma evaluation – PECARN and Canadian Head CT Rules
Human Bite
Evaluation of Hypertension
Supracondylar Fracture
Pharyngitis
Headache
Scaphoid Fracture
Allergy versus Anaphylaxis
Cervical spine trauma
Pulmonary Embolism Clinical Prediction Rules
Doc… my kid fell off the bed and
hit their head!
Pediatric Emergency Care Applied Research Network – PECARN
Federally-funded multi-institutional network for research in pediatric
emergency medicine in the United States
Pediatric Head Injury Prediction provides factors to identify those
at very low risk of clinically important traumatic brain injuries for
whom CT might be unnecessary
Prospective cohort study of 42,412 children
Children (<18 years) presenting within 24 hours of head trauma, with
Glasgow Coma Scale scores of 14 to 15
3/9/2017
3
Pediatric Head Injury/Trauma
Algorithm
Children younger than 2 years
Normal mental status
No scalp hematoma except frontal
No loss of consciousness or loss of
consciousness for <5 seconds
Non–severe injury mechanism
No palpable skull fracture
Acting normally according to the parents
Children ages 2 years and older
Normal mental status
No loss of consciousness
No vomiting
Non–severe injury mechanism
No signs of basilar skull fracture
No severe headache
Doc…I fell and hit my head!
Traumatic brain injury (TBI) = brain function impairment that results from external force
Mild: GCS 14-15 (Most Common)
Moderate: GCS 9-13
Severe: GCS 3-8
History and Physical Exam
Pupillary response
Altered motor function
Age of patient
Comorbidities (anticoagulant use?)
Decision rules attempt to limit unnecessary CT imaging & identify surgical emergencies
3/9/2017
4
Canadian CT Head Injury/Trauma
Rule
Can clear a head injury without imaging
Apply to patients with:
GCS 13-15 and LOC
Amnesia to the event
Confusion
Excludes:
Age <16
Seizure after injury
Blood thinner use
Canadian Head CT Rule
High Risk Criteria: Rules out need for neurosurgical intervention
GCS <15 at 2 hours post-injury
Suspected open or depressed skull fracture
Any sign of basilar skull fracture?
Hemotympanum, raccoon eyes, Battle’s Sign, CSF oto-/rhinorrhea
≥ 2 episodes of vomiting
Age ≥ 65
Medium Risk Criteria: In addition to above, rules out “clinically important” brain injury (positive CT's that normally require admission)
Retrograde amnesia to the event ≥ 30 minutes
“Dangerous” mechanism?
Pedestrian struck by motor vehicle, occupant ejected from motor vehicle, or fall from > 3 feet or > 5 stairs.
3/9/2017
5
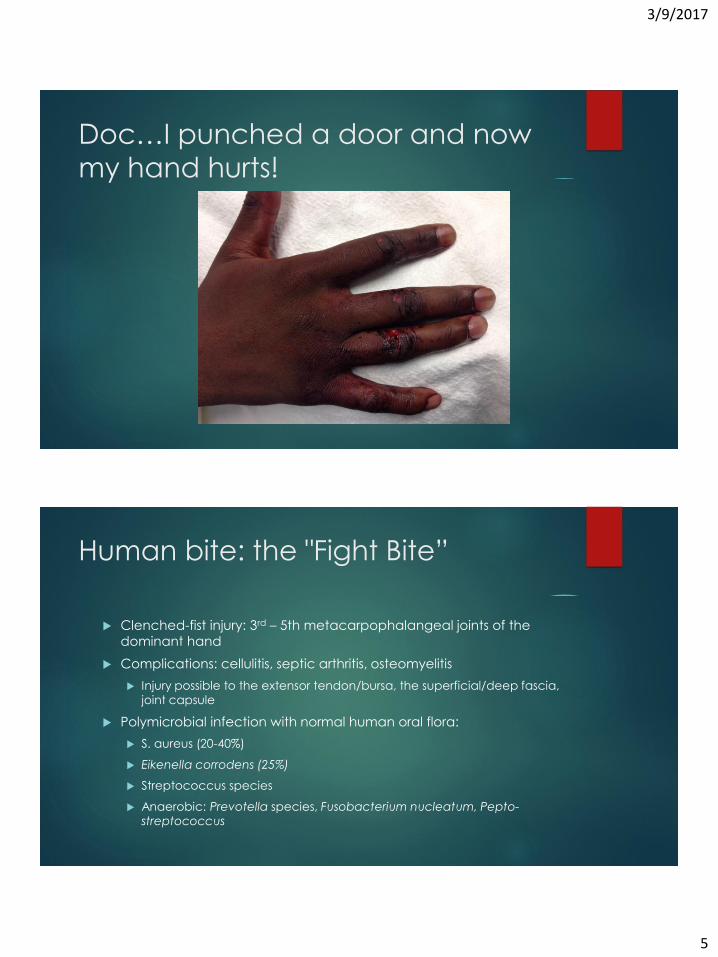
Doc…I punched a door and now
my hand hurts!
Human bite: the "Fight Bite”
Clenched-fist injury: 3rd – 5th metacarpophalangeal joints of the
dominant hand
Complications: cellulitis, septic arthritis, osteomyelitis
Injury possible to the extensor tendon/bursa, the superficial/deep fascia,
joint capsule
Polymicrobial infection with normal human oral flora:
S. aureus (20-40%)
Eikenella corrodens (25%)
Streptococcus species
Anaerobic: Prevotella species, Fusobacterium nucleatum, Pepto-
streptococcus
3/9/2017
6
Treatment
Neurovascular evaluation of the hand & plain radiographs to rule out fracture
Copious irrigation and debridement
DO NOT close the wound (exceptions cosmetic)
Wound culture
Antibiotics ISDA and Tintinalli
Amoxicillin/clavulanic acid 875/125 mg PO BID
Ampicillin-sulbactam 1.5-3 gm Q 6 hours or cefoxitin 2gm Q 8 hours or piperacillin-tazobactam 3.375 grams Q6 hours
PCN allergy – clindamycin plus moxifloxacin or TMP-SMX and metronidazole
Clindamycin 300 mg tid or 600 mg every 6–8 h plus Cipro 500–750 mg bid 400 mg every 12 h
Doc….My blood pressure is
210/115!
First thing…Recheck it!
HTN defined as SBP>140 mm Hg and DBP > 90 mm Hg
Primary (essential) vs. Secondary
ED Classification:
Asymptomatic elevated BP without hx HTN
Uncontrolled HTN
Hypertensive emergency
3/9/2017
7
Hypertensive Emergency
Hypertensive emergency = HTN with evidence of ACUTE end organ
dysfunction
Heart: Chest pain, Acute MI, Pulmonary edema
Brain: Hypertensive encephalopathy/CVA/Hemorrhage
Cerebral autoregulation
Kidney: Ischemia and Renal impairment
Vascular: Aortic Dissection
Other: Eclampsia, Retinal Hemorrhage, drug abuse (cocaine,
amphetamine)
Sx: SOB, CP, HA, MS change, vision changes
Hypertensive Emergency
Management
Immediate treatment
Reduce MAP 10-20% in 30-60 minutes
Addition reduction 5-15% over next 23 hours
Reduction beyond this risks end organ ischemia due to relative
hypotension
Exception: Aortic dissection acute goal = 100-120mm Hg
Drugs of choice:
IV Meds Nicardipine, Labetalol, Esmolol
Disposition admission
3/9/2017
8
Asymptomatic Hypertension
2013 ACEP Clinical Policy on Asymptomatic Hypertension
Asymptomatic HTN PCP f/u, no acute tx, labs may be helpful in select patients
Should I screen for target-organ injury?
Routine lab screening not required
If patients have poor follow-up, screening may identify acute kidney injury
Should I treat the blood pressure?
Medical intervention not required
If poor follow-up can treat in the ED and rx meds
Patel KK, et al. Characteristics and Outcomes of Patients Presenting With Hypertensive Urgency in the Office Setting. JAMA Intern Med. 2016 Jul 1;176(7):981-8
“Hypertensive urgency is common, but the rate of MACE in asymptomatic patients is very low. Visits to the ED were associated with more hospitalizations, but not improved outcomes. Most patients still had uncontrolled hypertension 6 months later.”
Asymptomatic Hypertension
Management - Outpatient
JNC 8 BP tx threshold of 150/90 mm Hg in the >60 age group and 140/90 mm Hg in <60 age group, DM and CKD
JNC7: chemistry, EKG, chest xray, UA, prior to therapy initiation
Medical treatment:
Non-black: thiazide type diuretics, ACEIs, ARBs, CCBs
Black: thiazide type diuretics, CCB
Chronic kidney disease: ACE or ARB (do they have a PCP)
AHA/ACA/CDC 2014 Science Advisory:
Stage 1: lifestyle modifications and HCTZ
Stage 2: lifestyle modifications plus thiazide in combo with ACEI, ARB, CCB
3/9/2017
9
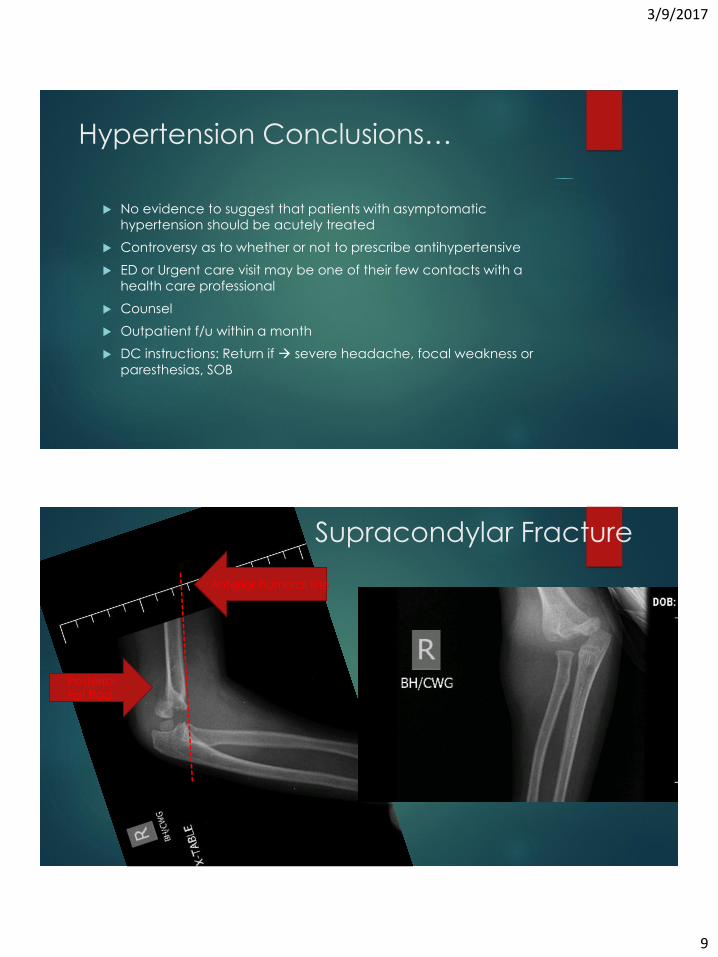
Hypertension Conclusions…
No evidence to suggest that patients with asymptomatic
hypertension should be acutely treated
Controversy as to whether or not to prescribe antihypertensive
ED or Urgent care visit may be one of their few contacts with a
health care professional
Counsel
Outpatient f/u within a month
DC instructions: Return if severe headache, focal weakness or
paresthesias, SOB
Supracondylar Fracture
Posterior
Fat Pad
Anterior humeral line
3/9/2017
10
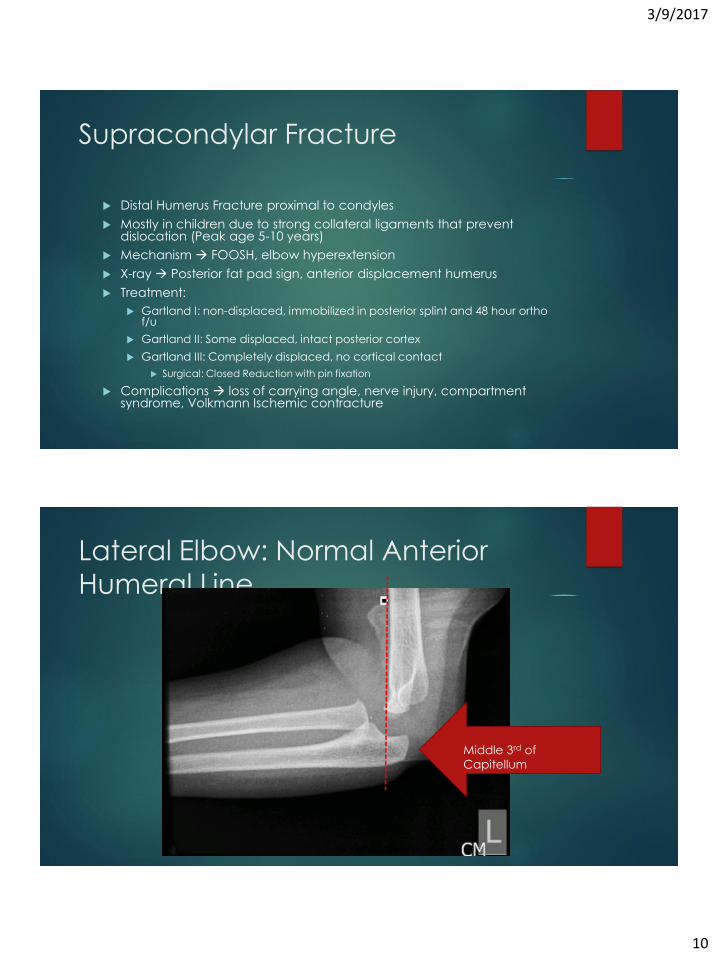
Supracondylar Fracture
Distal Humerus Fracture proximal to condyles
Mostly in children due to strong collateral ligaments that prevent dislocation (Peak age 5-10 years)
Mechanism FOOSH, elbow hyperextension
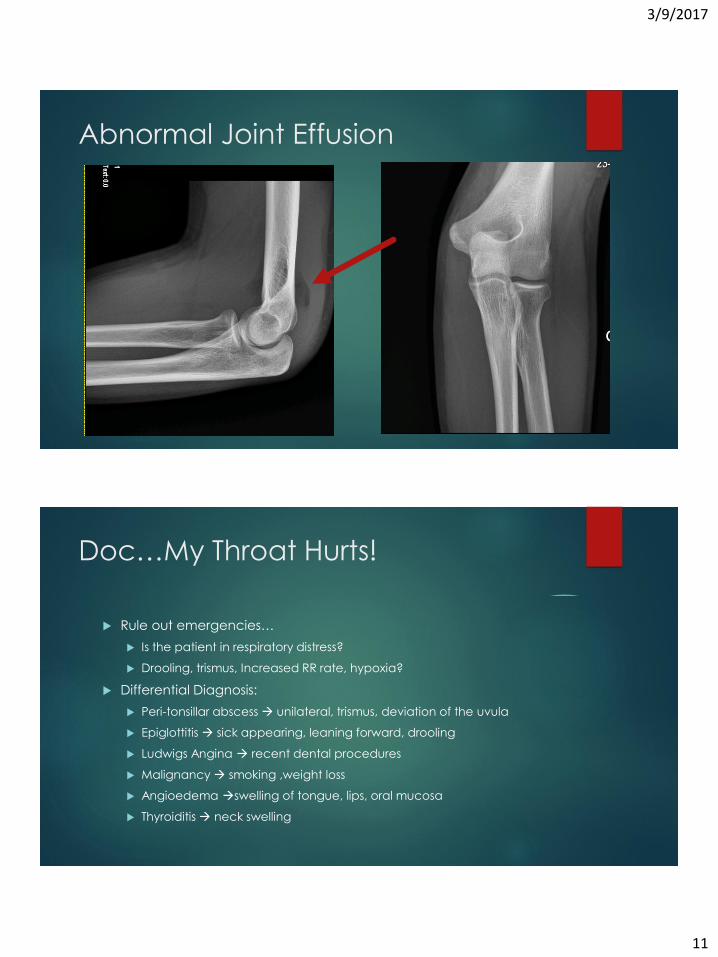
X-ray Posterior fat pad sign, anterior displacement humerus
Treatment:
Gartland I: non-displaced, immobilized in posterior splint and 48 hour ortho f/u
Gartland II: Some displaced, intact posterior cortex
Gartland III: Completely displaced, no cortical contact
Surgical: Closed Reduction with pin fixation
Complications loss of carrying angle, nerve injury, compartment syndrome, Volkmann Ischemic contracture
Lateral Elbow: Normal Anterior
Humeral Line
Middle 3rd of
Capitellum
3/9/2017
11
Abnormal Joint Effusion
Doc…My Throat Hurts!
Rule out emergencies…
Is the patient in respiratory distress?
Drooling, trismus, Increased RR rate, hypoxia?
Differential Diagnosis:
Peri-tonsillar abscess unilateral, trismus, deviation of the uvula
Epiglottitis sick appearing, leaning forward, drooling
Ludwigs Angina recent dental procedures
Malignancy smoking ,weight loss
Angioedema swelling of tongue, lips, oral mucosa
Thyroiditis neck swelling
3/9/2017
12
Bacterial Vs. Viral Pharyngitis
Viral vesicular or petechial pattern on the soft palate and tonsils and is associated with rhinorrhea
16% have tonsillar exudate
55% have cervical adenopathy
64% lack cough
Diagnostic testing not necessary except: influenza, mononucleosis, & acute retroviral syndrome
Bacterial Group A β-hemolytic Streptococcus: adults (15%), children (30%)
Incubation period of 2 to 5 days
Sudden onset of sore throat, painful swallowing, chills, and fever
Signs and symptoms:
Erythema of the tonsils (62%)
Exudate (32%)
Enlarged, tender cervical lymph nodes (76%)
Diagnostic Testing
Centor and Modified Centor Criteria
Original article in 1981: exudates, anterior cervical adenopathy, no cough, fever
Modified in 1998: Age qualifier added
Age 3-14 years (+1)
Age 15-44 years (+0)
Age >45 years (-1)
Rapid Antigen Detection Testing (RADT) or Throat culture (gold standard)
Guidelines:
ISDA 2012 2+, perform RADT
AHA/AAP 2009 2+, perform RADT
CDC/AAFP/ACP 2, perform RADT, 3+ RADT or treat empirically
If viral sx (coryza, cough, diarrhea, ulcerative stomatitis) and score 0-1 no testing/no treating
3/9/2017
13
Treatment
Decrease: symptom duration, infectivity
Complications:
Suppurative peritonsillar abscess, OM, sinusitis
Non-suppurative complications acute rheumatic fever, PSGM
Antibiotics
First Line (CDC recommendations):
Penicillin VK: Children: 250 mg twice daily or 3 times daily; adolescents and adults: 250 mg 4 times daily or 500 mg twice daily x 10 days
Amoxicillin: 50 mg/kg once daily (max = 1000 mg); alternate:25 mg/kg (max = 500 mg) twice daily x 10 days
Penicillin G benzathine: <27 kg: 600,000 U; ≥27 kg: 1,200,000 U IM x 1
PCN Allergy (not severe): Cephalexin PO, Cefadroxil PO
Severe PCN Allergy: Clindamycin PO, Azithromycin PO, Clarithromycin PO
Pain Relief
NSAIDS, Acetaminophen, throat lozenges
https://www.cdc.gov/groupastrep/diseases-hcp/strep-throat.html
Steroids?
Cochrane Review from 2012 of 8 trials involving 743 patients
showed:
“Oral or intramuscular corticosteroids, in addition to antibiotics, increase
the likelihood of both resolution and improvement of pain in participants
with sore throat. Further trials assessing corticosteroids in the absence of
antibiotics and in children are warranted.”
ISDA 2012 Guidelines recommends against use for symptoms
Dosing:
Dexamethasone 0.6mg/kg, maximum 10mg
Prednisone 60mg PO for 1-2 days
3/9/2017
14
Doc…my head hurts!
Typical of previous headaches?
Worst headache of your life?
How did it onset? (sudden versus gradual)
Fevers and chills?
Meningeal signs?
Characterize the headache?
Associated symptoms?
Surrounding events? (trauma, pregnancy, recent infection)
Hypercoagulable or on anticoagulants?
Age?
Differential Diagnosis
Differential Diagnosis
Migraine
Meningitis
Cluster headache
Hypertension, hypertensive encephalopathy
Temporal (giant cell) arteritis
Tumor
Caffeine, alcohol or drug withdrawal
Carbon monoxide poisoning
Venous sinus thrombosis
Pseudotumor cerebri
Post-Lumbar Puncture
• Tension Headache
• Sinusitis
• Cervical arthritis
• Acute angle closure glaucoma
• Dental Abscess
• Otitis Media
• TMJ
• Trigeminal neuralgia
• Depression• Cerebral ischemia
• Post LP Headache
• Subarachnoid hemorrhage
3/9/2017
15
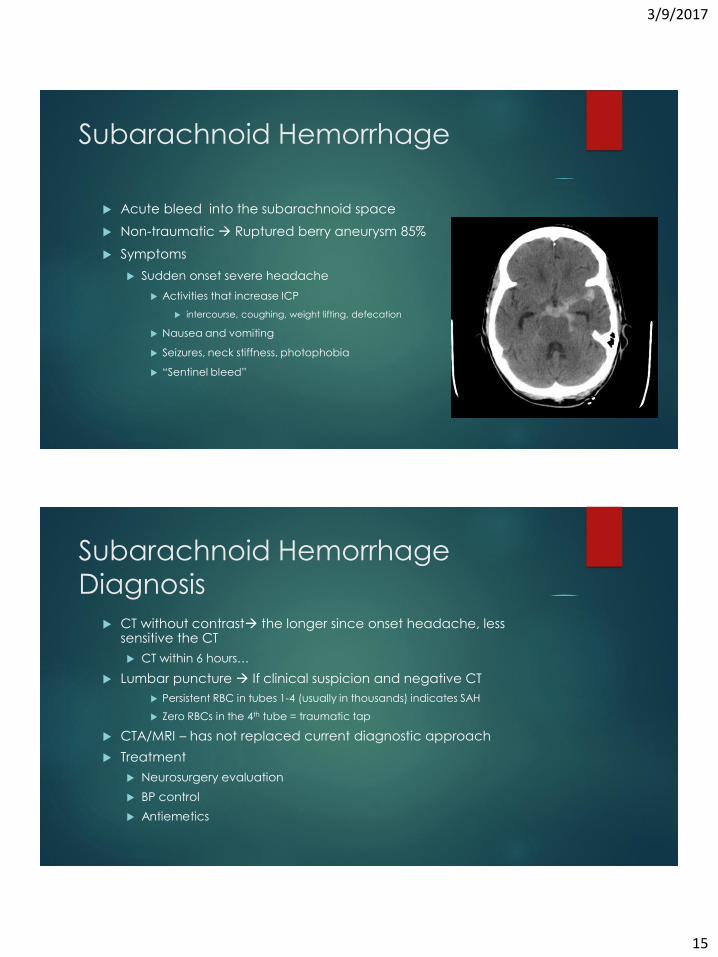
Subarachnoid Hemorrhage
Acute bleed into the subarachnoid space
Non-traumatic Ruptured berry aneurysm 85%
Symptoms
Sudden onset severe headache
Activities that increase ICP
intercourse, coughing, weight lifting, defecation
Nausea and vomiting
Seizures, neck stiffness, photophobia
“Sentinel bleed”
Subarachnoid Hemorrhage
Diagnosis
CT without contrast the longer since onset headache, less sensitive the CT
CT within 6 hours…
Lumbar puncture If clinical suspicion and negative CT
Persistent RBC in tubes 1-4 (usually in thousands) indicates SAH
Zero RBCs in the 4th tube = traumatic tap
CTA/MRI – has not replaced current diagnostic approach
Treatment
Neurosurgery evaluation
BP control
Antiemetics
3/9/2017
16
Meningitis
1.38 out of 100,000 people with fatality rate 14.3%
Inflammation of membranes covering spinal cord or brain due to
bacterial, viral or fungal infection
Causes
Recent otitis, sinusitis, pneumonia or immunocompromised, trauma,
neurosurgery, indwelling medical devices
Bacterial S. pneumoniae (MC), N. meningitides, L. monocytogenes
Viral Enteroviruses (MC, summer), Herpes simplex
Fungal Cryptococcus, Toxoplasma
Non-infectious Lupus, Vasculitis, Sarcoidosis etc.
Meningitis Diagnosis
Symptoms & Exam
Fever, headache, neck stiffness, altered MS, photophobia, vomiting, seizures, petechial/purpuric rash, Kernig/Brudzinski
CT head without contrast
Before LP IDSA recommends for patients who meet any criteria:
Immunocompromised state
History of CNS disease (mass lesion, stroke, or focal infection)
New-onset seizure within 1 week of presentation
Papilledema
Abnormal level of consciousness
Focal neurologic deficit
LP
Contraindications coagulopathy
Disposition Admission and monitoring
3/9/2017
17
Chemoprophylaxis
Exposure increases risk by 500-800x normal population
Close contacts:
Housemates
Secretion exposure (kissing, shared utensils or toothbrush, person who
intubated without a facemask)
Can decrease transmission by 89% in N. menengitidis
Initiate within 24 hours, but no later than 2 weeks
Rifampin 10 mg/kg (max 600mg) Q 12 hours x 4 doses
Cipro 500mg PO once
Ceftriaxone 250mg IM once
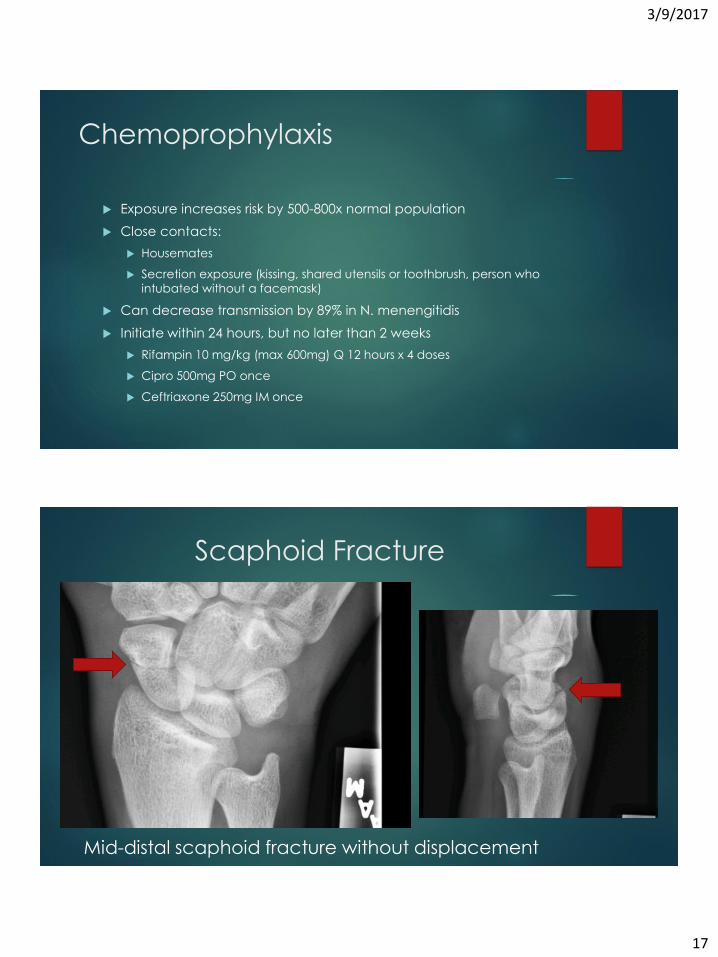
Scaphoid Fracture
image
Mid-distal scaphoid fracture without displacement
3/9/2017
18
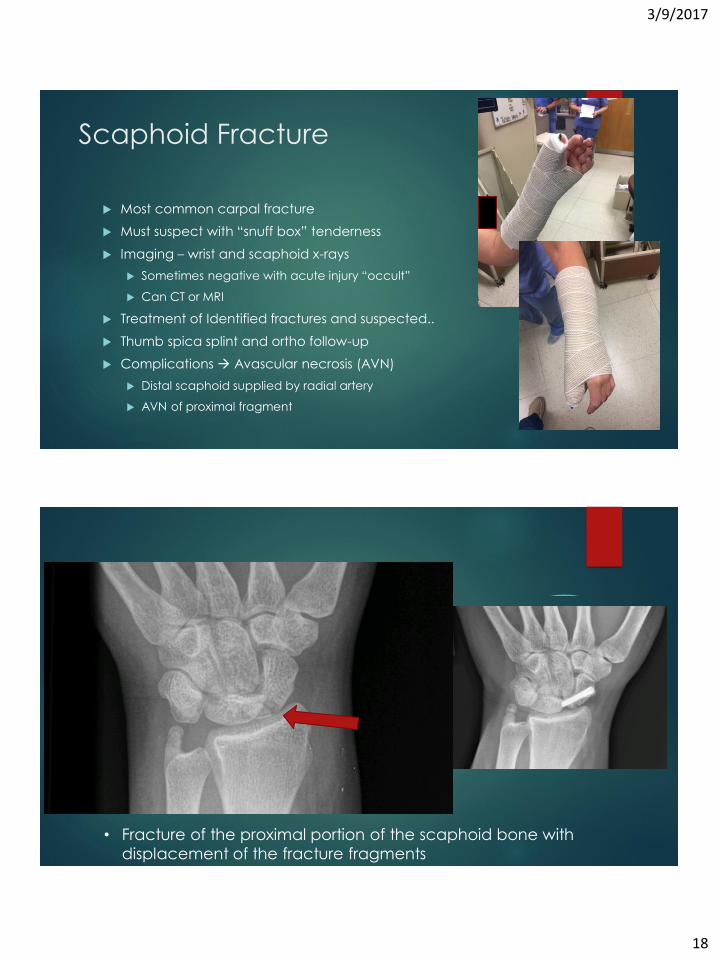
Scaphoid Fracture
Most common carpal fracture
Must suspect with “snuff box” tenderness
Imaging – wrist and scaphoid x-rays
Sometimes negative with acute injury “occult”
Can CT or MRI
Treatment of Identified fractures and suspected..
Thumb spica splint and ortho follow-up
Complications Avascular necrosis (AVN)
Distal scaphoid supplied by radial artery
AVN of proximal fragment
Picture Thumb Spica
• Fracture of the proximal portion of the scaphoid bone with
displacement of the fracture fragments
3/9/2017
19
Doc, I’m itchy and my tongue is
swollen…
What is “just” an Allergic Reaction vs. Anaphylaxis?
Vital signs?
Causes: medications, foods, insect stings, environmental allergens,
latex, exercise, and other unknown factors
Differential Diagnosis:
MI, arrhythmia, PE, Asthma, COPD
Vasovagal response, anxiety, septic shock
Scromboid poisoning, monosodium glutamate syndrome
Ace inhibitor or hereditary induced angioedema
Definition of Anaphylaxis from
NIAID/FAAN
1. “Acute onset of an illness (minutes to several hours) with
involvement of the skin, mucosal tissue, or both” AND one of the
following:
Respiratory compromise or reduced BP
2. Two or more of the following that occur rapidly after exposure to a
likely allergen for that patient
Involvement of skin-mucosal tissue, respiratory compromise,
hypotension, GI symptoms
3. Reduced BP after exposure to known allergen for that patient
30% decrease in systolic BP in children or adults
Campbell, Ronna L. et al.Evaluation of National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network criteria for the diagnosis of anaphylaxis in emergency department
patients. Journal of Allergy and Clinical Immunology , Volume 129 , Issue 3 , 748 - 752
3/9/2017
20
Treatment of Anaphylaxis
Prehospital
Evaluate VS and ABCs/monitor
Supplemental O2
Large bore IV access
IV fluids, supine position with elevation of legs
Remove hymoneptera stinger
B-agonists – 2.5mg via nebulizer
Steroids
Medications to Initiate
Epinephrine 0.3 to 0.5mL (0.01mg/kg in children max 0.3 dosage) of
epinephrine in a 1:1000 dilution
IM, lateral aspect of the thigh
Every 5-10 minutes as necessary
Antihistamines:
Diphenhydramine 25-50mg
H1 and H2: Ranitidine 50mg (adult) 1mg/kg (children)
Corticosteroids
Prednisone 1mg/kg PO
Methylprednisolone 125mg IV
3/9/2017
21
Disposition
Admission
Limited access to phone or emergency services
Prior history of anaphylaxis
Underlying asthma, renal disease, CHF, B-blocker usage
Discharge after Observation
AAAI and AI Joint Task force – observation time based on individual
patients
NIAID &FARE – observation time of 4-6 hours
Biphasic reaction in 5-20%
Doc…my neck hurts after an MVA
Low risk trauma patients: Alert, stable, adult trauma patient w/o neurologic deficits
National Emergency X-Radiography Utilization Study (NEXUS) - 1998
Plain cervical spine injury unnecessary if patients lack 5 criteria
99.6% sensitive, 12.9% specific, negative predictive value 99.9%
Limitations: Age >60
Canadian Cervical Spine Rule for Radiography (CCR)
3 assessments asked in sequential order
If any answer is positive imaging
100% sensitive, 42.5% specific
Limitations: Complexity compared to NEXUS
3/9/2017
22
NEXUS Criteria
1. Absence of midline cervical tenderness
2. Normal level of alertness
3. No evidence of intoxication
4. Absence of focal neurologic deficit
5. Absence of painful distracting injury
If any of the above criteria are present, the C-Spine cannot be
cleared clinically by these criteria, consider imaging
Canadian C-Spine Rule
Assessments
1. There are no high risk factors that
mandate radiography
2. There are low risk factors that
allow for a safe assessment of
range of motion
3. The patient is able to actively
rotate the neck
Definitions
Age 65 or older
A dangerous mechanism of injury
Paresthesias in extremities
Simple rear-end MVA
Patient able to sit up
Ambulatory
Delayed onset of pain
Absence of midline TTP
Can rotate neck 45 degrees bilaterally
3/9/2017
23
Cervical Spine Imaging
Plain radiography
3 views: Lateral, anterior-posterior, odontoid
Clinically acceptable study: all 7 vertebrae and superior border first
thoracic
Benefits: Cost- effective, bedside, small amount of radiation
Disadvantages: C1 & C2, Visualizing spine due to body habitus
Cervical Spine CT
More sensitive and specific than plain X-rays
Consider for moderate & high risk patients
Thoracic and Lumbar Spine Imaging
Doc…it hurts when I take a deep
breath!
History
Duration?
Location?
Associated symptoms?
Constant or intermittent?
Aggravating or alleviating factors?
Differential:
Pneumonia
Bronchitis
Pulmonary embolism
Pneumothorax
Pericarditis
Rib fracture
Esophageal spasm/rupture
Atypical CP/MI
3/9/2017
24
Pulmonary Embolism
650,000 - 900,000 PEs each year in the US 200,000 deaths
Pulmonary Embolism:
Thrombus forms in the venous system (MC LE DVT) and embolizes to the lung
Causes acute obstruction of the pulmonary arterial system and pulmonary ischemia/infarction
Large emboli obstruction of right ventricular outflow and circulatory collapse
Risk Factors: THROMBOSIS
Trauma, travel
Hypercoagulable, hormone replacement
Relatives, recreational drugs
Old (age >60)
Malignancy
Birth control
Obesity, obstetrics
Surgery, smoking
Immobilization
Sickness
Pulmonary Embolism
Symptoms
Hemoptysis
Shortness of breath
Pleuritic chest pain
Exam: SOB, tachy, clear lungs, hypoxia, unilateral leg swelling, +/-unstable VS
Diagnosis
EKG ST, S1Q3T3, new RBBB
CXR Hampton Hump, Westermark sign
D-dimer
CTA/VQ Scan
3/9/2017
25
PERC Rule for Pulmonary Embolism
Rules out PE if no criteria are present and pre-test probability is ≤15%
If all are negative, no need for further workup, <2% chance of PE
ACEP 2011 Clinical Policy: “Level B recommendations. In patients
with a low pretest probability for suspected pulmonary embolism,
consider using the PERC to exclude the diagnosis based on historical
and physical examination data alone.”
D-dimer:
D-dimer if low-risk, but not PERC negative
D-dimer negative and pre-test probability is <15% then no further
testing
D-dimer positive then CT-angiography or V/Q
Criteria for PERC Rule
Clinical low probability (<15% probability of PE based on gestalt
assessment)
Age < 50
HR < 100
O2 sat on room air > 94% at near sea level
No prior hx DVT or PE
Recent trauma or surgery
No Hemoptysis
No estrogen use
No unilateral leg swelling (asymmetrical calves on visual inspection)
3/9/2017
26
Wells Clinical Prediction Rule for PE
Risk stratifies patients for PE & provides an estimated pre-test
probability
Based on risk, physician chooses next diagnostic study
D-dimer
CTA
3 tiers: low, moderate, high
2 tiers: unlikely, likely (supported by ACEP’s 2011 clinical policy on
PE)
Main criticism: has a “subjective” criterion in it “PE #1 diagnosis or
equally likely”
Wells Clinical Prediction Rule for PE
Point Score
Suspected DVT 3
Alt dx less likely than PE 3 points
Heart rate > 100 bpm 1.5
Prior venous thrombus 1.5
Immobilization w/in 4 wks 1.5
Active malignancy 1
Hemoptysis 1
Risk Score Interpretation
3- Tier model
Low risk (<2 points): 1.3%
Mod risk (2-6 points): 16.2%
High risk (>6 points): 37.5%
2-Tier model
PE unlikely (0-4 points): 12.1%
PE likely (>4 points): 37.1%
3/9/2017
27
D-dimer
Clots contain fibrin, degraded by plasmin yields D-dimer
Half-life of approximately 8 hours, can be elevated for at least 3 days
Sensitivity: 94-98%, Specificity: 50-60%
Factors known to give false positive D-dimer level
Age > 70
Pregnancy
Malignancy
Recent surgical procedure
Liver disease
RA
Trauma
Potential false negatives: Lipemia, symptoms > 5 days, warfarin, small pulmonary infarction, isolated calf vein thrombosis
Closing Points…
3/9/2017
28
References Pediatric Head Trauma
Kupperman N, Holmes J, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. The Lancet. Volume 374, Issue 9696, 3–9 October 2009, Pages 1160–1170
Goldman R. Decision rules can identify children at very low risk of clinically important traumatic brain injury. Journal of Pediatrics, The, 2010-03-01, Volume 156, Issue 3, Pages 509-510, Copyright © 2010 Mosby, Inc.
Schonfeld D1, Bressan S, et al. Pediatric Emergency Care Applied Research Network head injury clinical prediction rules are reliable in practice. Arch Dis Child. 2014 May;99(5):427-31. doi: 10.1136/archdischild-2013-305004. Epub 2014 Jan 15.
Easter JS, Bakes K et al. Comparison of PECARN, CATCH, and CHALICE rules for children with minor head injury: a prospective cohort study. Ann Emerg Med. 2014 Aug;64(2):145-52, 152.e1-5. doi: 10.1016/j.annemergmed.2014.01.030. Epub 2014 Mar 11.
PECARN Pediatric Head Injury/Trauma Algorithmhttps://www.mdcalc.com/pecarn-pediatric-head-injury-trauma-algorithm
Kupperman N, Holmes J, et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. The Lancet. Volume 374, Issue 9696, 3–9 October 2009, Pages 1160–1170
Goldman R. Decision rules can identify children at very low risk of clinically important traumatic brain injury. Journal of Pediatrics, The, 2010-03-01, Volume 156, Issue 3, Pages 509-510, Copyright © 2010 Mosby, Inc.
Schonfeld D1, Bressan S, et al. Pediatric Emergency Care Applied Research Network head injury clinical prediction rules are reliable in practice. Arch Dis Child. 2014 May;99(5):427-31. doi: 10.1136/archdischild-2013-305004. Epub 2014 Jan 15.
Easter JS, Bakes K et al. Comparison of PECARN, CATCH, and CHALICE rules for children with minor head injury: a prospective cohort study. Ann EmergMed. 2014 Aug;64(2):145-52, 152.e1-5. doi: 10.1016/j.annemergmed.2014.01.030. Epub 2014 Mar 11.
PECARN Pediatric Head Injury/Trauma. Algorithmhttps://www.mdcalc.com/pecarn-pediatric-head-injury-trauma-algorithm
Canadian Head CT References
Stiell IG, Wells GA, et al. The Canadian CT Head Rule for patients
with minor head injury. Lancet. 2001 May 5;357(9266):1391-6.
Stiell IG, Clement CM, et al. Comparison of the Canadian CT Head
Rule and the New Orleans Criteria in patients with minor head injury.
JAMA. 2005 Sep 28;294(12):1511-8.
Easter JS, Hakoos JS, et al. Traumatic intracranial injury in intoxicated
patients with minor head trauma. Acad Emerg Med. 2013
Aug;20(8):753-60. doi: 10.1111/acem.12184.
3/9/2017
29
References Fight Bite
Goldstein E, Abrahamian F. Human Bites. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition. 320, 3510-3515.e1. Eighth Edition. Copyright © 2015 by Saunders, an imprint of Elsevier Inc.
Stevens D, Bisno A, Chambers H, et. al. Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. CID 2014:59 (15 July).
Germann CA. Germann C.A. Germann, Carl A.Nontraumatic Disorders of the Hand. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli J.E., Stapczynski J, Ma O, Yealy D.M., Meckler G.D., Cline D.M. Eds. Judith E. Tintinalli, et al.eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.vcom.idm.oclc.org/content.aspx?bookid=1658§ionid=109447692. Accessed February 13, 2017.
Hypertension References
Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure – The JNC 7 Report. JAMA. 2003; 289 (19):2560-2572.
James PA, Oparil S, Carter BL, et al. 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eigth Joint National Committee (JNC 8). JAMA. 2014;311(5):507-520.
Goldberg E. An Evidence-Based Approach to Managing Asymptomatic Elevated Blood Pressure in the Emergency Department. Emergency Medicine Practice. February 2015. Volume 17, Number 2.
Patel KK, et al. Characteristics and Outcomes of Patients Presenting With Hypertensive Urgency in the Office Setting. JAMA Intern Med. 2016 Jul 1;176(7):981-8.
Wolf et al. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients in the Emergency Department with Asymptomatic Elevated Blood Pressure. Ann Emergency Medicine;62:59-68
3/9/2017
30
Supracondylar Fracture References
Blok B, Cheung D, Platts-Mills T. Elbow Injuries: Supracondylar Fracture. First Aid for the Emergency Medicine Boards. Copyright 2016 by McGraw-Hill Education. P215-16
The Treatment of Pediatric Supracondylar Humerus Fractures: Evidence Based Guideline and Evidence Report. American Academy of Orthopedic Surgeons. Published in 2011. http://www.aaos.org/research/guidelines/SupracondylarFracture/SupConFullGuideline.pdf
Chow YC. Chow Y.C. Chow, Yvonne C.Elbow and Forearm Injuries. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli J.E., Stapczynski J, Ma O, Yealy D.M., Meckler G.D., Cline D.M. Eds. Judith E. Tintinalli, et al.eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.vcom.idm.oclc.org/content.aspx?bookid=1658§ionid=109446609. Accessed March 08, 2017.
References for PERC/PE
Kline JA, Mitchell AM et al. Clinical criteria to prevent unnecessary diagnostic testing in emergency department patients with suspected pulmonary embolism. J Thromb Haemost. 2004 Aug;2(8):1247-55.
Kline JA, Courtney DM et al. Prospective multicenter evaluation of the pulmonary embolism rule-out criteria. J Thromb Haemost. 2008 May;6(5):772-80. doi: 10.1111/j.1538-7836.2008.02944.x. Epub2008 Mar 3.
Dachs R, Endres J, Garber M. Pulmonary Embolism Rule-Out Criteria: A Clinical Decision Rule That Works. Am Fam Physician. 2013 Jul 15;88(2):98-100.
Fesmire, Francis MD. ACEP News Contributing Writer. June 1, 2011. ACEP Clinical Policy Review: Suspected Pulmonary Embolism. http://www.acepnow.com/article/acep-clinical-policy-review-suspected-pulmonary-embolism/2/?singlepage=1
Critical Issues in the Evaluation and Management of Adult Patients Presenting to the ED with suspected PE. ACEP Clinical Policy. Ann Emerg Med 2011;57:628-652
Kline JA. Kline J.A. Kline, Jeffrey A.Venous Thromboembolism. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli J.E., Stapczynski J, Ma O, Yealy D.M., Meckler G.D., Cline D.M. Eds. Judith E. Tintinalli, et al.eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.vcom.idm.oclc.org/content.aspx?bookid=1658§ionid=109429015. Accessed March 08, 2017.
3/9/2017
31
Pharyngitis References
Hildreth A, Takhar S. Evidence Based Evlauation and Mangement of Patients with Pharyngitis in the Emergency Department. Emergency Medicine Practice. September 2015. Volume 17, Number 9.
Hayward G, Thompson MJ, Perera R, Et al. Corticosteroids as a standalone or add-on treatment for sore throat. Cochrane Database Syst Rev. 2012;10:CD008268.
Schams SC, Goldman RD. Steroids as adjuvant treatment of sore throat in acute bacterial pharyngitis. Can Fam Physician. 2012;58(1):52-54
Hartman ND. Hartman N.D. Hartman, Nicholas D.Neck and Upper Airway. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli J.E., Stapczynski J, Ma O, Yealy D.M., Meckler G.D., Cline D.M. Eds. Judith E. Tintinalli, et al.eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.vcom.idm.oclc.org/content.aspx?bookid=1658§ionid=109387281. Accessed February 13, 2017.
Evaluation of Pharyngitis. Urgent Care RAP. April 2015: Volume 1, Issue 2. Accessed 3/7/17.
Group A Streptococcal Disease, For Clinicians. CDC. https://www.cdc.gov/groupastrep/diseases-hcp/index.html. Accessed 3/7/17.
Shulman et al. Clinical Practice Guideline for the Diagnosis and Management of Group A Streptococcal Pharyngitis: 2012 Update by the Infectious Diseases Society of America. CID. https://www.idsociety.org/uploadedFiles/IDSA/Guidelines-Patient_Care/PDF_Library/2012%20Strep%20Guideline.pdf
Headache References
Blok B, Cheung D, Platts-Mills T. Subarachnoid Hemorrhage. First Aid for the Emergency Medicine Boards. 3rd Edition. p846-848.
Blok B, Cheung D, Platts-Mills T. CNS Infections: Meningitis. First Aid for the Emergency Medicine Boards. 3rd Edition. p840-843.
Based Approach to Diagnosis and Management of Subarachnoid Hemorrhage in the ED. Emergency Medicine Practice: October 2014, Vol. 16, Number 10
Blok KM, Rinkel GJ et al. CT within 6 hours of headache onset to rule out subarachnoid hemorrhage in nonacademic hospitals. Neurology. 2015 May 12;84(19):1927-32. doi: 10.1212/WNL.0000000000001562. Epub 2015 Apr 10.
Carpenter C, Hussain A et al. Spontaneous Subarachnoid Hemorrhage: A Systematic Review and Meta-analysis Describing the Diagnostic Accuracy of History, Physical Examination, Imaging, and Lumbar Puncture With an Exploration of Test Thresholds. Academic Emergency Medicine. Volume 23, Issue 9, pages 963–1003, September 2016
Perry J et al. Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. BMJ 2011;343:d4277
Nicole M. Dubosh, M. Fernanda Bellolio, Alejandro A. Rabinstein and Jonathan A. Edlow. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage. Stroke. 2016;STROKEAHA.115.011386, originally published January 21, 2016
Bamberger D. Diagnosis, Initial Management, and Prevention of Meningitis. Am Fam Physician. 2010 Dec 15;82(12):1491-1498.
Erin N. Quattromani, MD, and Amer Z. Aldeen, MD. Focus On: Emergent Evaluation and Management of Bacterial Meningitis. ACEP News May 2008. https://www.acep.org/clinical---practice-management/focus-on--emergent-evaluation-and-management-of-bacterial-meningitis.
Tiffee A, Zosky M. Meningitis: Clinical Pearls an Pitfalls. Feb 4, 2015. http://www.emdocs.net/meningitis-clinical-pearls-pitfalls/
Hackman JL, Nelson AM, Ma O. Hackman J.L., Nelson A.M., Ma O Hackman, Jeffrey L., et al.Spontaneous Subarachnoid and Intracerebral Hemorrhage. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli J.E., Stapczynski J, Ma O, Yealy D.M., Meckler G.D., Cline D.M. Eds. Judith E. Tintinalli, et al.eds. Tintinalli’sEmergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.vcom.idm.oclc.org/content.aspx?bookid=1658§ionid=109436521. Accessed March 08, 2017.
3/9/2017
32
Scaphoid References
Boyd A, Benjamin H, Apslund C, Splints and Casts: Indications and
Methods. Am Fam Physician. 2009 Sep 1;80(5):491-499.
Jones B, MD, Rozental T. Ortho Info: Scaphoid Fracture of the Wrist.
American Academy of Orthopedics. Last reviewed March of 2016.
http://orthoinfo.aaos.org/topic.cfm?topic=A00012
Phillips G, Reibach A, Slomiany P. Diagnosis and Management of
Scaphoid Fractures. Am Family Physician. 2004 Sep 1;70(5):879-884.
Allergic Reaction References
Singer E, Zodda D. Allergy and Anaphylaxis: Principles of Acute Emergency Management. Emergency Medicine Practice. August 2015. Volume 17. Number 8.
Campbell, Ronna L. et al.Evaluation of National Institute of Allergy and Infectious Diseases/Food Allergy and Anaphylaxis Network criteria for the diagnosis of anaphylaxis in emergency department patients. Journal of Allergy and Clinical Immunology , Volume 129 , Issue 3 , 748 - 752
Sampson HA, Munoz-Furlong A, Bock SA, et al. Symposium on the definition and management of anaphylaxis: summary report. J Allergy Clinical Immunology. 2005;115(3):584-591
Liebman P, Nicklas RA, Oppenheimer J, et al. The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clinical Immunology. 2010;126 (3)477-480.
Liebman P. Biphasic anaphylactic reactions. Ann Allergy Asthma Immunology. 2005;95 (3):217-226
3/9/2017
33
Neck Pain References
Go S. Go S Go, Steven.Spine Trauma. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. Tintinalli J.E., Stapczynski J, Ma O, Yealy D.M., Meckler G.D., Cline D.M. Eds. Judith E. Tintinalli, et al.eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.vcom.idm.oclc.org/content.aspx?bookid=1658§ionid=109387434. Accessed March 02, 2017.
Pullen, Lara. Imaging Not a Necessity for Spine Evaluation in Trauma Patients. http://www.acepnow.com/article/imaging-necessity-spine-evaluation-trauma-patients/
Brunk, Doug. ACEP News June 2008. Studies Challenge Spine Injury Criteria for Children. https://www.acep.org/Clinical---Practice-Management/Studies-Challenge-Spine-Injury-Criteria-for-Children/
Updated Guidelines For Management Of Acute Cervical Spine And Spinal Cord Injury In Pediatric Patients. September 2014. EB Medicine.
Current Guidelines For Assessment Of Cervical Spine And Vertebral Artery Injuries In Adults Following Blunt Trauma. July 2014. EB Medicine.
Cervical Spine Injury: An Evidence-Based Evaluation Of The Patient With Blunt Cervical Trauma. April 2009. EB Medicine.