Embed Size (px)
Citation preview
Urinary System I: Kidneys and Urine Formation
Functions of the Urinary System
Organs of the Urinary System
The Kidney
• Coverings and Regions
• Blood Flow
• Nephrons: Glomeruli and Renal Tubules
• Urine Formation
Urinalysis
Ureters, Bladder, and Urethra
Functions of the Urinary System: Blood Filtration Elimination of waste products
• Nitrogenous wastes (amino groups from amino acids)
• Toxins
• Drugs
Regulate aspects of homeostasis
• Water balance
• Electrolytes
• Acid-base balance in the blood
• Blood pressure
• Red blood cell production (erythropoietin)
• Activation of vitamin D
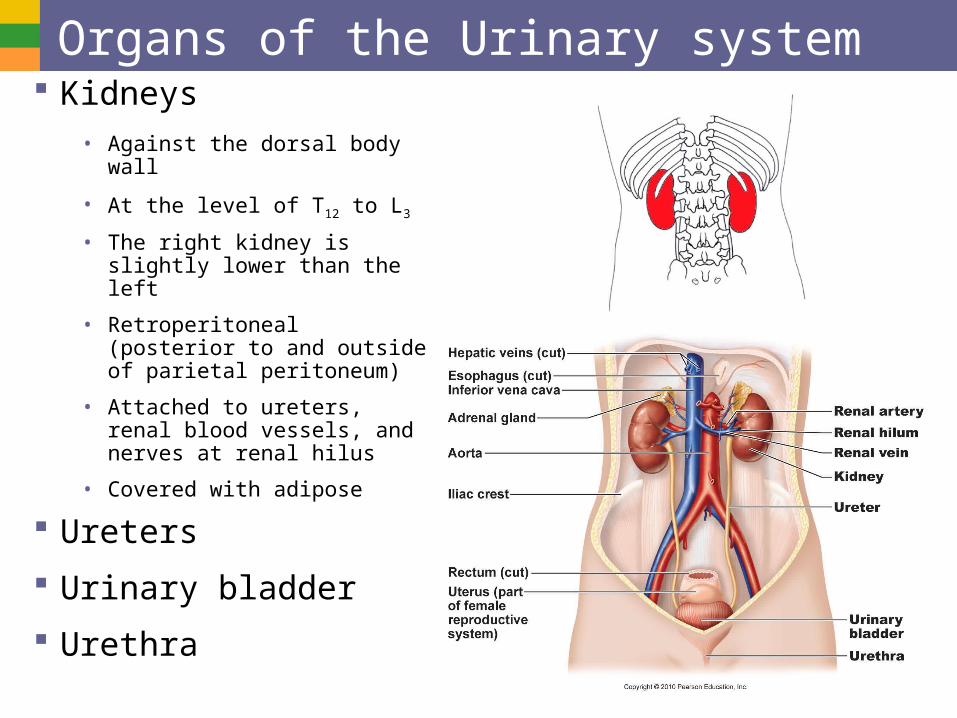
Organs of the Urinary system Kidneys
• Against the dorsal body wall
• At the level of T12 to L3
• The right kidney is slightly lower than the left
• Retroperitoneal (posterior to and outside of parietal peritoneum)
• Attached to ureters, renal blood vessels, and nerves at renal hilus
• Covered with adipose
Ureters
Urinary bladder
Urethra
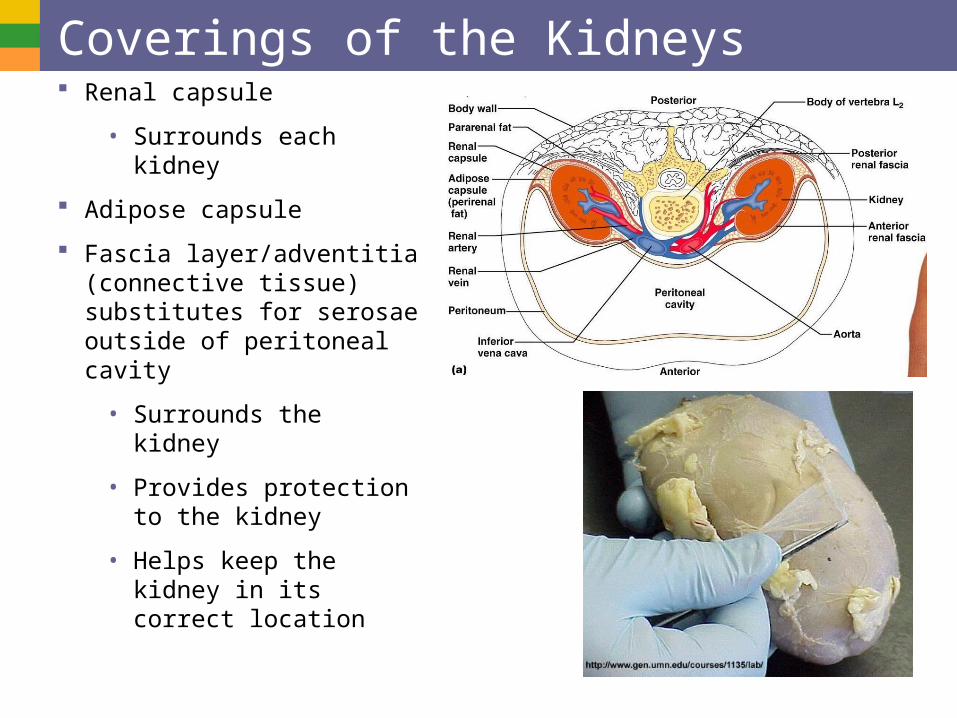
Coverings of the Kidneys Renal capsule
• Surrounds each kidney
Adipose capsule
Fascia layer/adventitia (connective tissue) substitutes for serosae outside of peritoneal cavity
• Surrounds the kidney
• Provides protection to the kidney
• Helps keep the kidney in its correct location
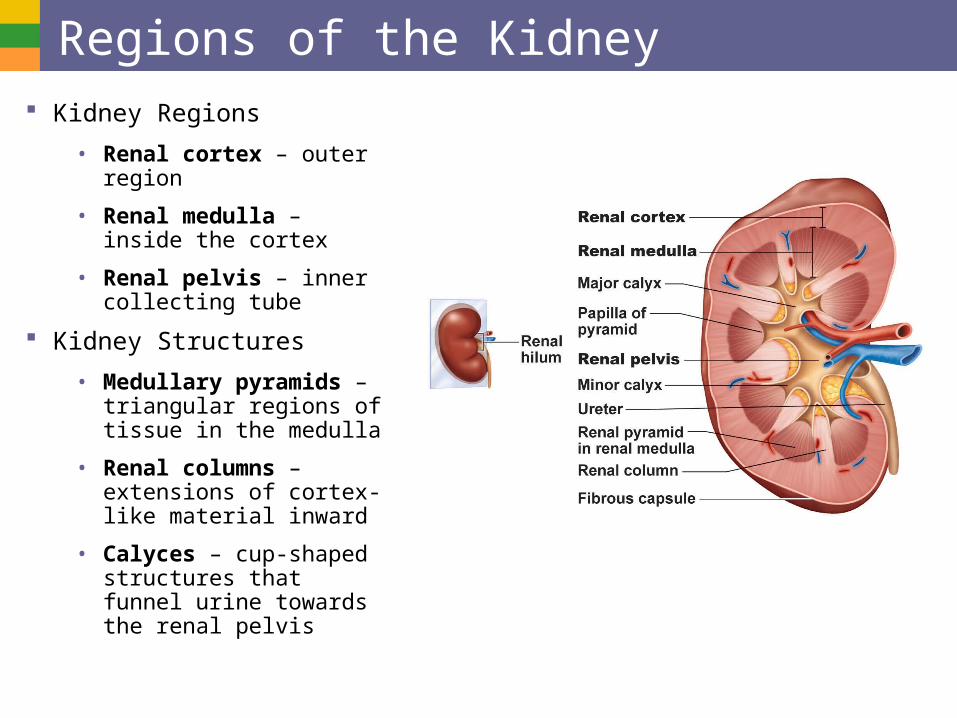
Regions of the Kidney Kidney Regions
• Renal cortex – outer region
• Renal medulla – inside the cortex
• Renal pelvis – inner collecting tube
Kidney Structures
• Medullary pyramids – triangular regions of tissue in the medulla
• Renal columns – extensions of cortex-like material inward
• Calyces – cup-shaped structures that funnel urine towards the renal pelvis
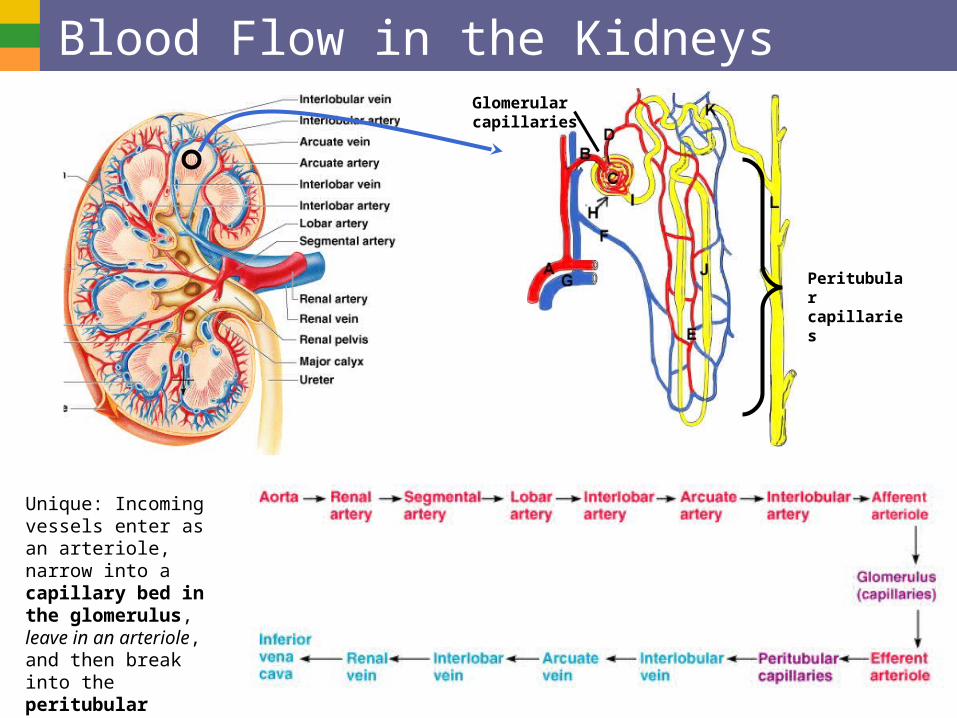
Blood Flow in the Kidneys
Unique: Incoming vessels enter as an arteriole, narrow into a capillary bed in the glomerulus, leave in an arteriole, and then break into the peritubular capillary bed before leaving as venus blood.
Peritubular capillaries
Glomerular capillaries
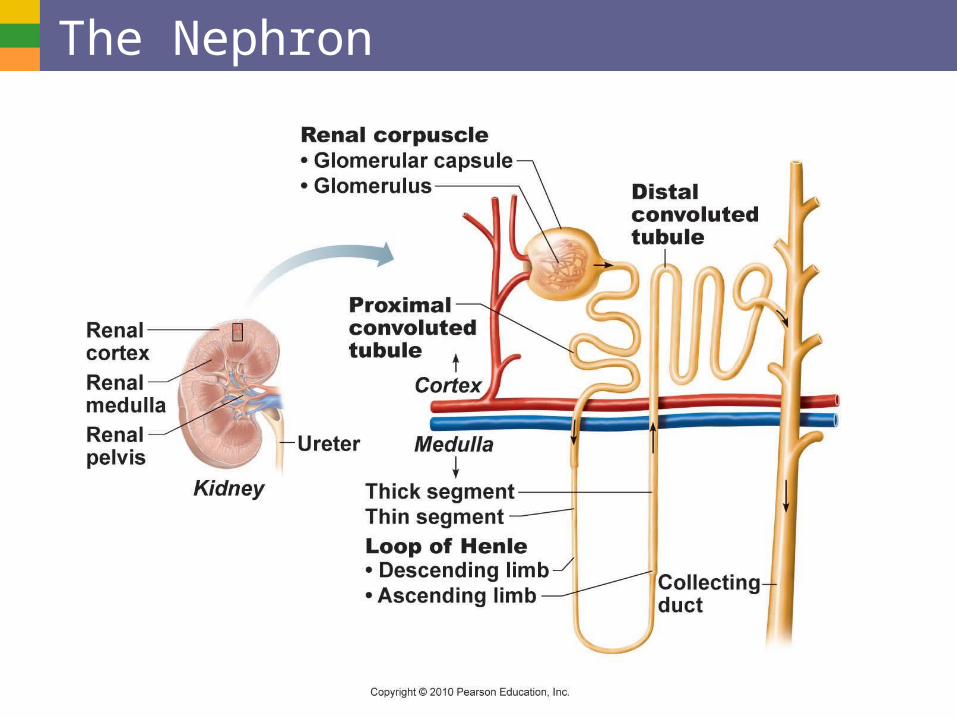
The Nephron
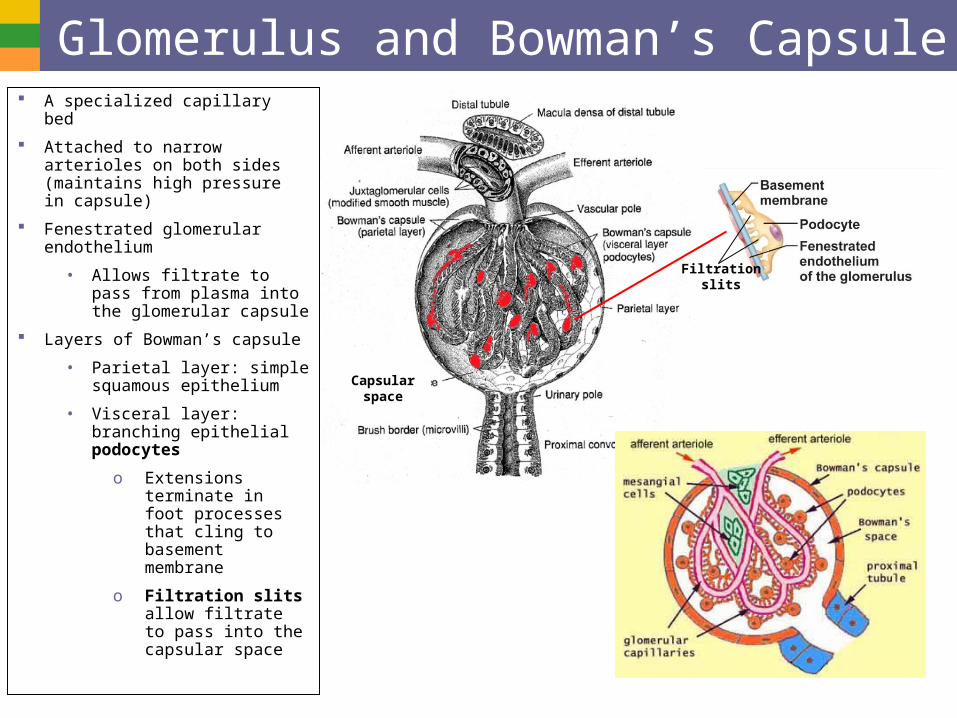
Glomerulus and Bowman’s Capsule A specialized capillary bed
Attached to narrow arterioles on both sides (maintains high pressure in capsule)
Fenestrated glomerular endothelium
• Allows filtrate to pass from plasma into the glomerular capsule
Layers of Bowman’s capsule
• Parietal layer: simple squamous epithelium
• Visceral layer: branching epithelial podocytes
o Extensions terminate in foot processes that cling to basement membrane
o Filtration slits allow filtrate to pass into the capsular space
Capsular space
Filtrationslits
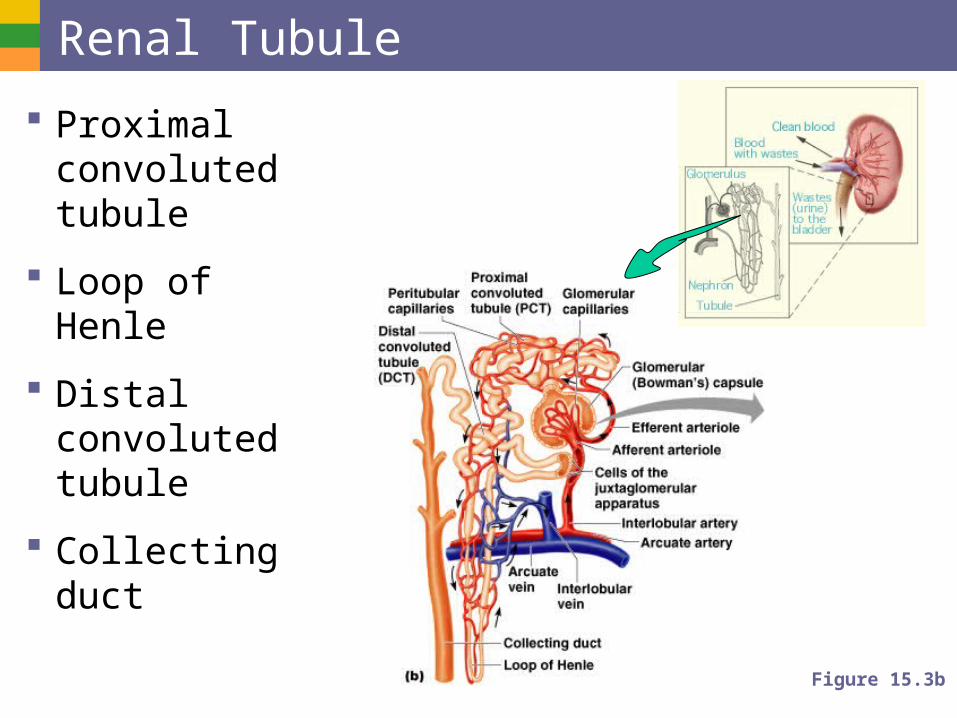
Renal Tubule
Proximal convoluted tubule
Loop of Henle
Distal convoluted tubule
Collecting duct
Figure 15.3b
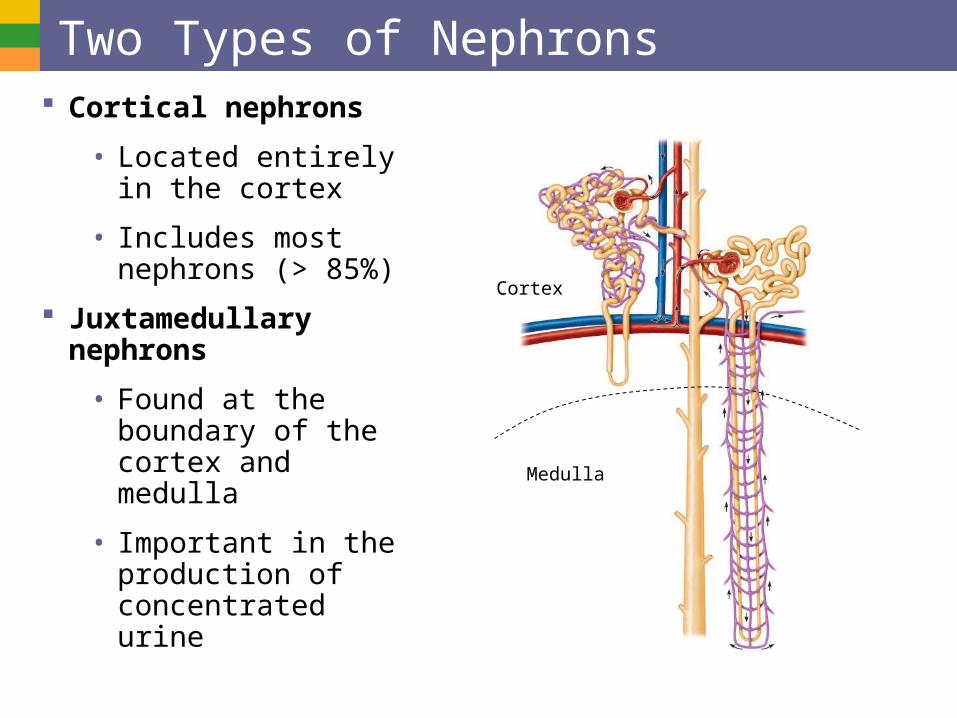
Two Types of Nephrons Cortical nephrons
• Located entirely in the cortex
• Includes most nephrons (> 85%)
Juxtamedullary nephrons
• Found at the boundary of the cortex and medulla
• Important in the production of concentrated urine
Medulla
Cortex
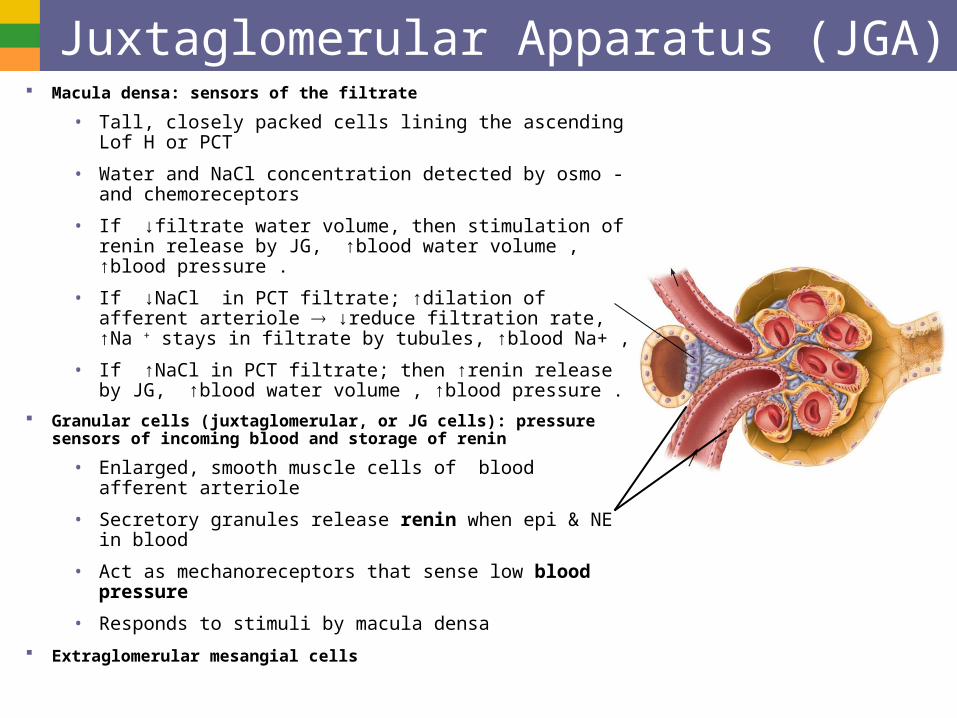
Juxtaglomerular Apparatus (JGA) Macula densa: sensors of the filtrate
• Tall, closely packed cells lining the ascending Lof H or PCT
• Water and NaCl concentration detected by osmo -and chemoreceptors
• If ↓filtrate water volume, then stimulation of renin release by JG, ↑blood water volume , ↑blood pressure .
• If ↓NaCl in PCT filtrate; ↑dilation of afferent arteriole ↓reduce filtration rate, ↑Na + stays in filtrate by tubules, ↑blood Na+ ,
• If ↑NaCl in PCT filtrate; then ↑renin release by JG, ↑blood water volume , ↑blood pressure .
Granular cells (juxtaglomerular, or JG cells): pressure sensors of incoming blood and storage of renin
• Enlarged, smooth muscle cells of blood afferent arteriole
• Secretory granules release renin when epi & NE in blood
• Act as mechanoreceptors that sense low blood pressure
• Responds to stimuli by macula densa
Extraglomerular mesangial cells
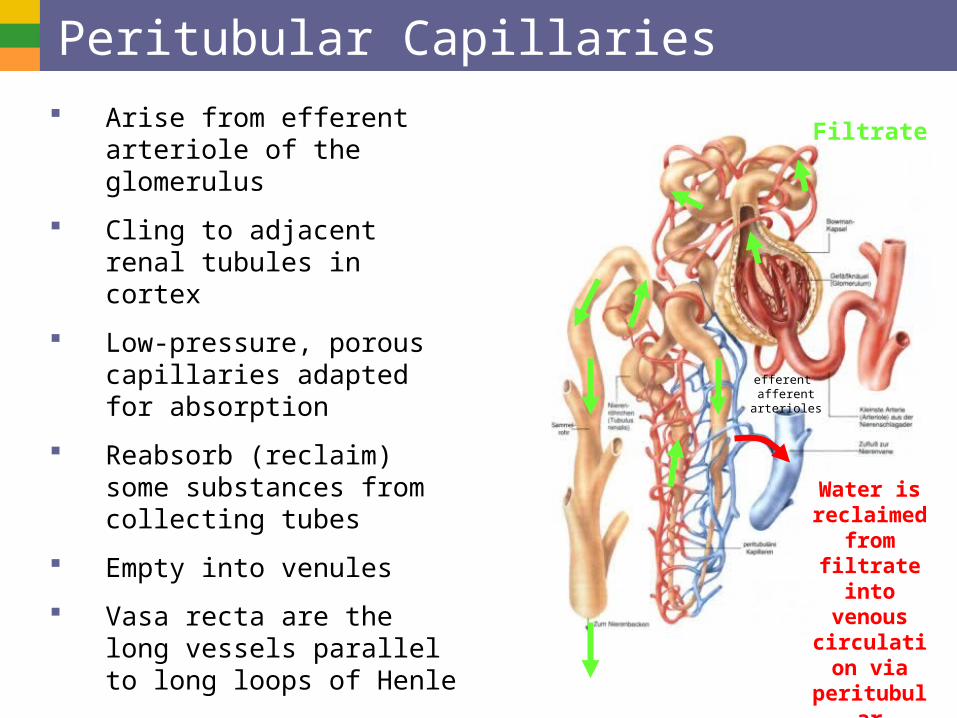
Peritubular Capillaries
Arise from efferent arteriole of the glomerulus
Cling to adjacent renal tubules in cortex
Low-pressure, porous capillaries adapted for absorption
Reabsorb (reclaim) some substances from collecting tubes
Empty into venules
Vasa recta are the long vessels parallel to long loops of Henle
efferent afferent arterioles
Water is reclaimed
from filtrate into venous
circulation via
peritubular
capillaries
Filtrate
Fenestratedendotheliumof the glomerulus
Microvilli
Cortex
Medulla
Podocyte
Basementmembrane
Mitochondria
Highly infolded plasmamembrane
Proximalconvolutedtubule
Distalconvolutedtubule
• Descending limbLoop of Henle
• Ascending limb
• Glomerular capsule
Renal corpuscle
• Glomerulus
Thick segment
Collectingduct
Intercalated cellPrincipal cell
Thin segment
Proximal convoluted tubule cells
Glomerular capsule: parietal layer
Glomerular capsule: visceral layer
Distal convoluted tubule cells
Loop of Henle (thin-segment) cells
Collecting duct cells
Renal cortex
Renal medulla
Renal pelvis
Ureter
Kidney
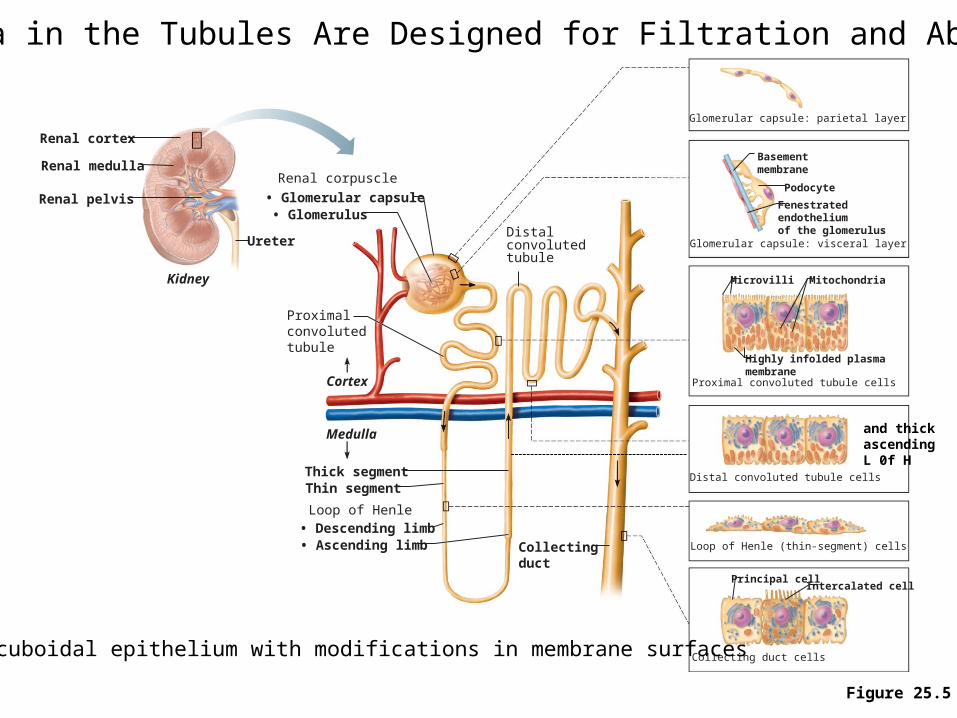
Epithelia in the Tubules Are Designed for Filtration and Absorption
Figure 25.5
Mostly cuboidal epithelium with modifications in membrane surfaces
and thick ascendingL 0f H
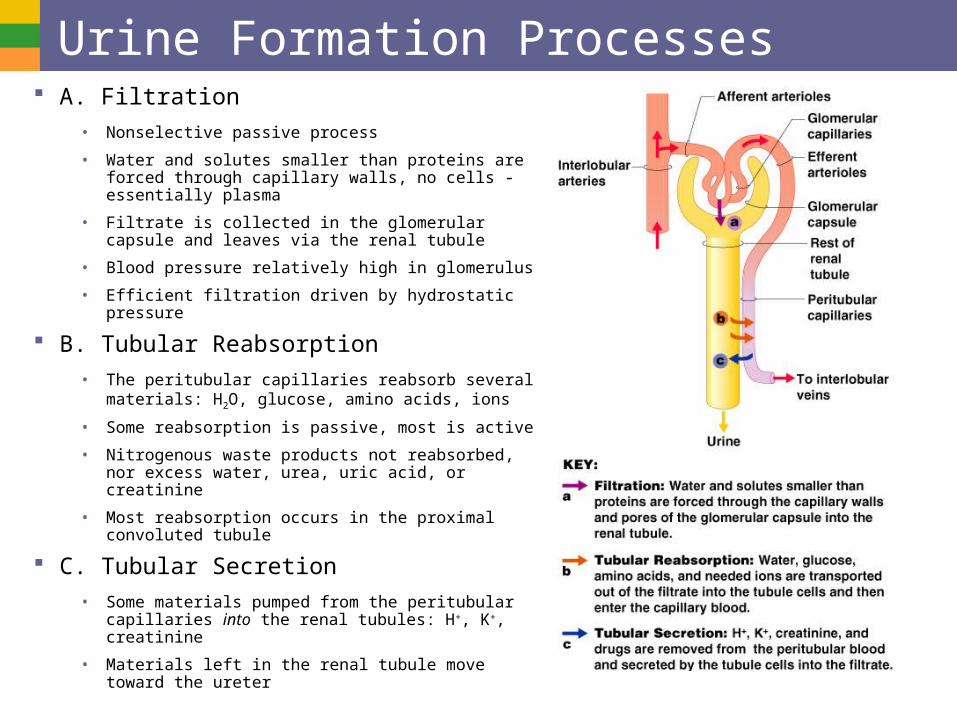
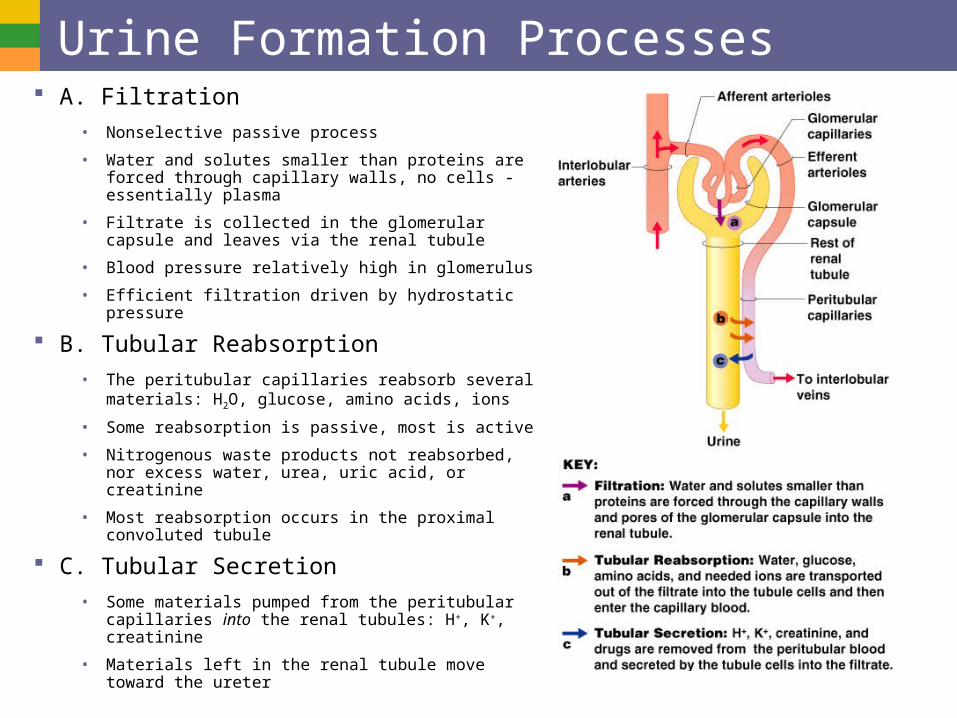
Urine Formation Processes A. Filtration
• Nonselective passive process
• Water and solutes smaller than proteins are forced through capillary walls, no cells - essentially plasma
• Filtrate is collected in the glomerular capsule and leaves via the renal tubule
• Blood pressure relatively high in glomerulus
• Efficient filtration driven by hydrostatic pressure
B. Tubular Reabsorption
• The peritubular capillaries reabsorb several materials: H2O, glucose, amino acids, ions
• Some reabsorption is passive, most is active
• Nitrogenous waste products not reabsorbed, nor excess water, urea, uric acid, or creatinine
• Most reabsorption occurs in the proximal convoluted tubule
C. Tubular Secretion
• Some materials pumped from the peritubular capillaries into the renal tubules: H+, K+, creatinine
• Materials left in the renal tubule move toward the ureter
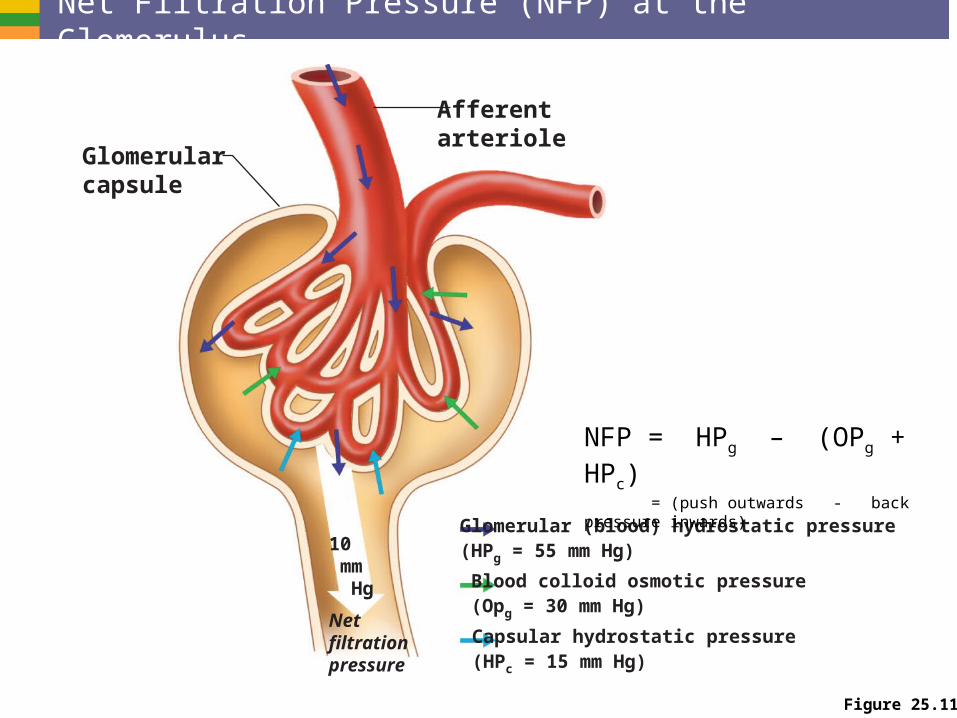
Figure 25.11
Glomerularcapsule
Afferentarteriole
10 mm Hg
Netfiltrationpressure
Glomerular (blood) hydrostatic pressure(HPg = 55 mm Hg)
Blood colloid osmotic pressure(Opg = 30 mm Hg)
Capsular hydrostatic pressure(HPc = 15 mm Hg)
NFP = HPg – (OPg + HPc) = (push outwards - back pressure inwards)
Net Filtration Pressure (NFP) at the Glomerulus
Glomerular Filtration Rate
Volume of filtrate formed per minute by the kidneys (120–125 ml/min)
Governed by (and directly proportional to)
• Total surface area available for filtration
• Filtration membrane permeability
• Flow rate (GFR) is tightly controlled by two types of mechanisms
o Intrinsic controls (renal autoregulation)
o Extrinsic controls (nervous and endocrine regulation
Intrinsic Controls (Renal Autoregulation) of GFR
Local action within the kidney
• Myogenic mechanism
BP constriction of afferent arterioles
Helps maintain normal GFR
Protects glomeruli from damaging high BP
BP dilation of afferent arterioles
Helps maintain normal GFR
• Tubuloglomerular feedback mechanism, which senses changes in the juxtaglomerular apparatus
o Flow-dependent mechanism directed by the macula densa cells
o If GFR increases, filtrate flow rate increases in the tubule
o Filtrate NaCl concentration will be high because of insufficient time for reabsorption
o Macula densa cells of the JGA respond to NaCl by releasing a vasoconstricting chemical that acts on the afferent arteriole GFR
Extrinsic controls of GFR Nervous and endocrine mechanisms that maintain
blood pressure, but affect kidney function
Under normal conditions at rest
• Renal blood vessels are dilated
• Renal autoregulation mechanisms prevail
Under extreme stress
• Norepinephrine is released by the sympathetic nervous system; epinephrine is released by the adrenal medulla
• NE and Epi cause constriction of afferent arterioles, inhibiting filtration and triggering the release of renin from JGA cells leading to renin-angiotensin cascade
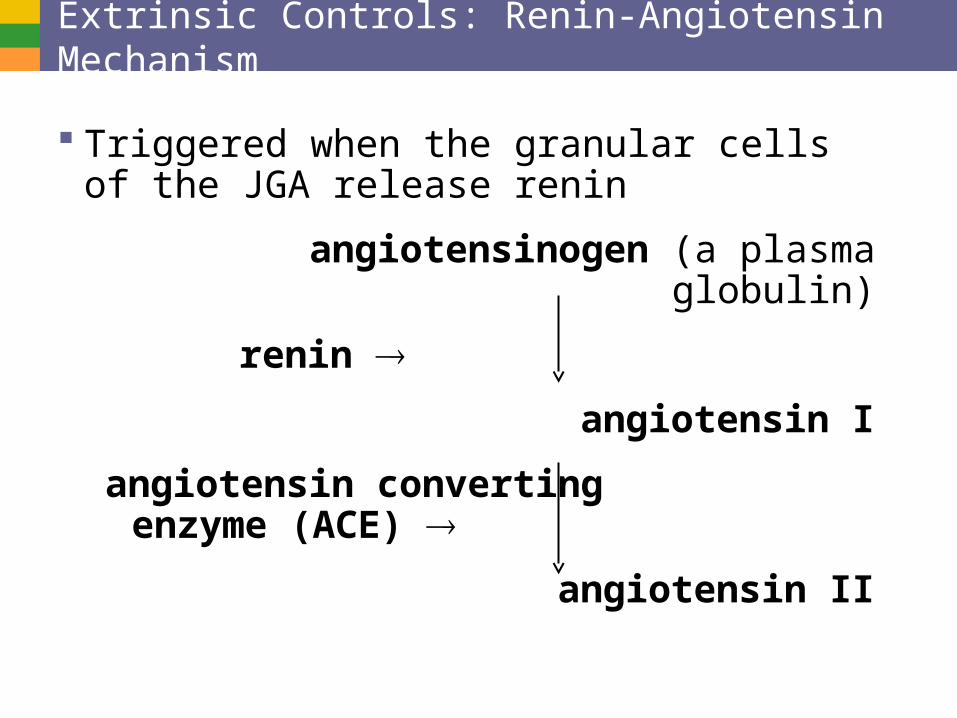
Extrinsic Controls: Renin-Angiotensin Mechanism
Triggered when the granular cells of the JGA release renin
angiotensinogen (a plasma globulin)
renin
angiotensin I
angiotensin converting enzyme (ACE)
angiotensin II
Effects of Angiotensin II1. Constricts arteriolar smooth muscle, causing mean arterial
pressure to rise (hypertensive)
2. Stimulates the reabsorption of Na+
• Acts directly on the renal tubules
• Triggers adrenal cortex to release aldosterone (hypertensive
3. Stimulates the hypothalamus to release ADH and activates the thirst center (increases hydration)
4. Constricts efferent arterioles, decreasing peritubular capillary hydrostatic pressure and increasing fluid reabsorption (saves water)
5. Causes glomerular mesangial cells to contract, decreasing the surface area available for filtration (saving water)
Extrinsic Controls: Renin-Angiotensin Mechanism
Triggers for renin release by granular cells
• Reduced stretch of granular cells (MAP below 80 mm Hg)
• Stimulation of the granular cells by activated macula densa cells
• Direct stimulation of granular cells via 1-adrenergic receptors by renal nerves
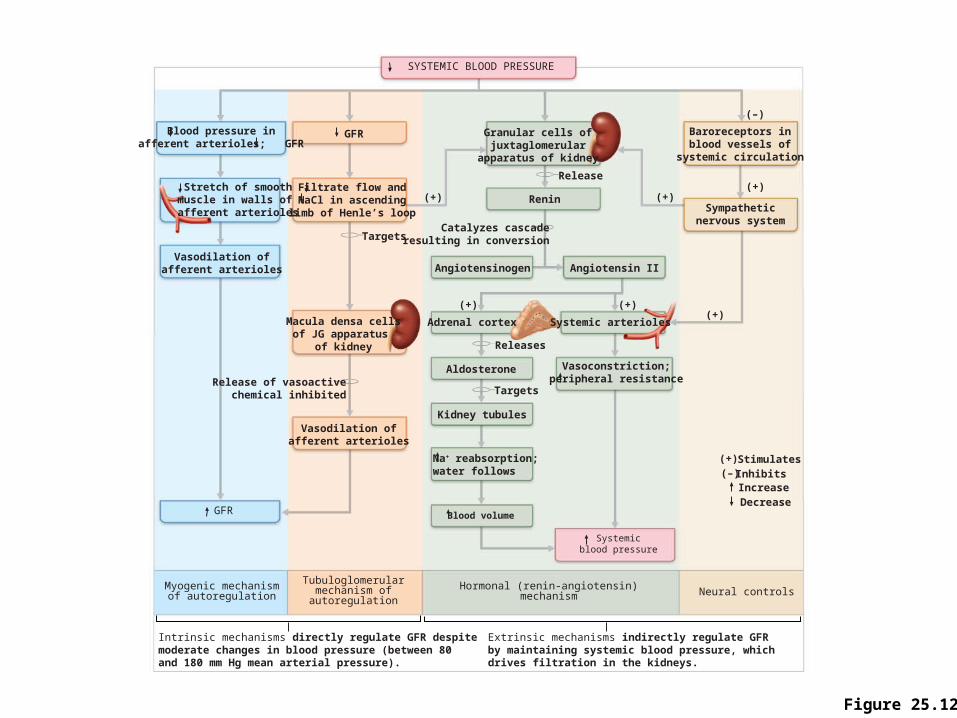
Figure 25.12
Stretch of smoothmuscle in walls of afferent arterioles
Blood pressure inafferent arterioles; GFR
Vasodilation ofafferent arterioles
GFR
Myogenic mechanismof autoregulation
Release of vasoactive chemical inhibited
Intrinsic mechanisms directly regulate GFR despitemoderate changes in blood pressure (between 80 and 180 mm Hg mean arterial pressure).
Extrinsic mechanisms indirectly regulate GFRby maintaining systemic blood pressure, whichdrives filtration in the kidneys.
Tubuloglomerularmechanism ofautoregulation
Hormonal (renin-angiotensin)mechanism Neural controls
SYSTEMIC BLOOD PRESSURE
GFR
Macula densa cellsof JG apparatus
of kidney
Filtrate flow andNaCl in ascending
limb of Henle’s loop
Targets
Granular cells ofjuxtaglomerular
apparatus of kidney
Angiotensinogen Angiotensin II
Adrenal cortex Systemic arterioles
(+) Renin
Release
Catalyzes cascaderesulting in conversion
(+)
(+)
(+)
Kidney tubules
Aldosterone
Releases
Targets
Vasoconstriction;peripheral resistance
Blood volume
Na+ reabsorption;water follows
Systemicblood pressure
(+)
(+) (–)
IncreaseDecrease
StimulatesInhibits
Baroreceptors inblood vessels of
systemic circulation
Sympatheticnervous system
(+)
(–)
Vasodilation ofafferent arterioles
Urine Formation Processes A. Filtration
• Nonselective passive process
• Water and solutes smaller than proteins are forced through capillary walls, no cells - essentially plasma
• Filtrate is collected in the glomerular capsule and leaves via the renal tubule
• Blood pressure relatively high in glomerulus
• Efficient filtration driven by hydrostatic pressure
B. Tubular Reabsorption
• The peritubular capillaries reabsorb several materials: H2O, glucose, amino acids, ions
• Some reabsorption is passive, most is active
• Nitrogenous waste products not reabsorbed, nor excess water, urea, uric acid, or creatinine
• Most reabsorption occurs in the proximal convoluted tubule
C. Tubular Secretion
• Some materials pumped from the peritubular capillaries into the renal tubules: H+, K+, creatinine
• Materials left in the renal tubule move toward the ureter
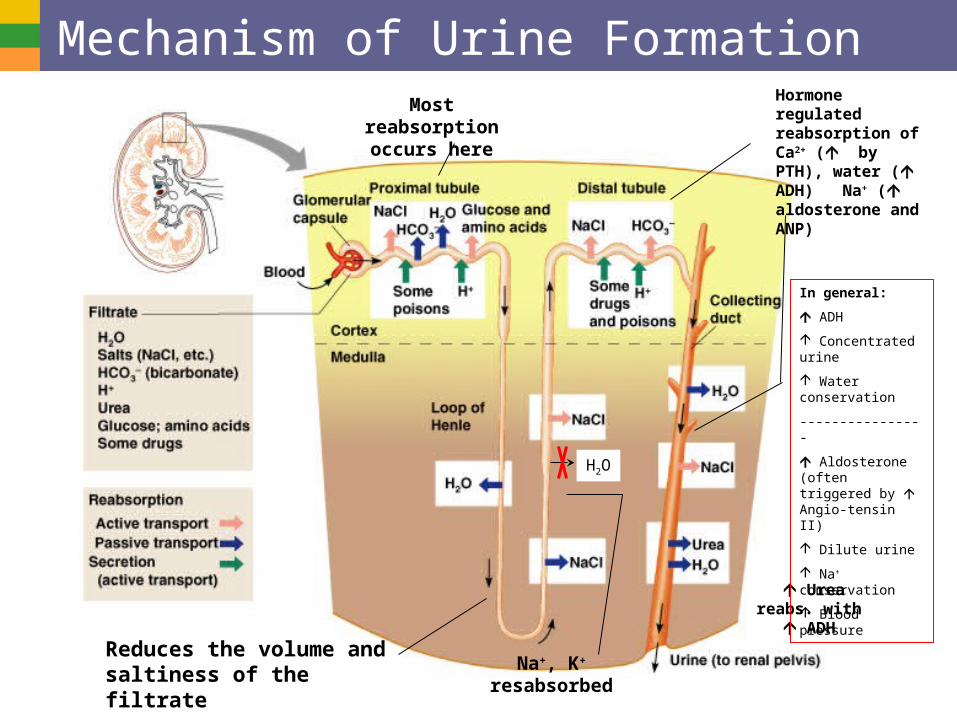
Mechanism of Urine FormationMost
reabsorption occurs here
Na+, K+ resabsorbed
Hormone regulated reabsorption of Ca2+ ( by PTH), water ( ADH) Na+ ( aldosterone and ANP)
H2O
Urea reabs. with ADH
In general:
ADH
Concentrated urine
Water conservation
----------------
Aldosterone (often triggered by Angio-tensin II)
Dilute urine
Na+ conservation
Blood pressure
Reduces the volume and saltiness of the filtrate
Countercurrent Mechanism Occurs when fluid flows in opposite directions in
two adjacent segments of the same tube
• E.g. Filtrate flow in the loop of Henle (countercurrent multiplier)
• E.g. Blood flow in the vasa recta (countercurrent exchanger)
Role of countercurrent mechanisms
• Establish and maintain an osmotic gradient
• Allow the kidneys to vary urine concentration (but especially make dilute urine)
• Allow for more efficient exchange of ions or gases
Countercurrent Multiplier: Loop of Henle Descending limb
• Freely permeable to H2O, which passes out of the filtrate into the hyperosmotic medullary interstitial fluid
• Filtrate osmolality increases to ~1200 mOsm
Ascending limb
• Impermeable to H2O
• Selectively permeable to solutes
o Na+ and Cl– are passively reabsorbed in the thin segment, actively reabsorbed in the thick segment
• Filtrate osmolarity decreases to 100 mOsm
Loop of Henle
Osmolalityof interstitialfluid(mOsm)
Innermedulla
Outermedulla
Cortex Active transport
Passive transport
Water impermeable
(a) Countercurrent multiplier. The long loops of Henle of the juxtamedullary nephrons create the medullary osmotic gradient.
H2O
H2O
H2O
H2O
H2O
H2O
H2O
NaCI
NaCI
NaCI
NaCI
NaCI
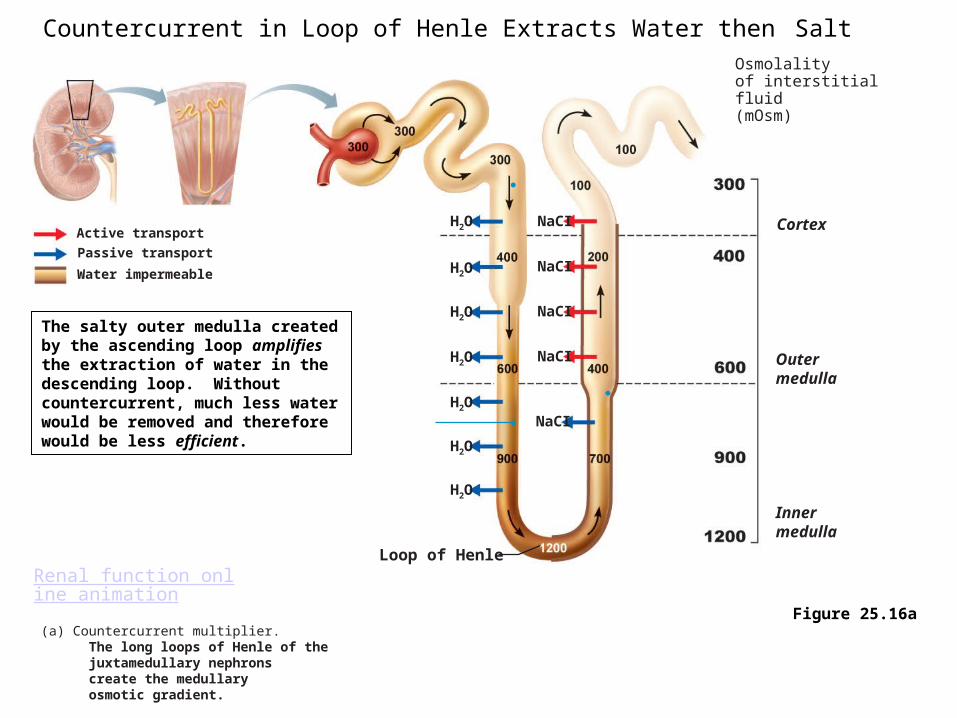
Countercurrent in Loop of Henle Extracts Water then Salt
Figure 25.16a
Renal function online animation
The salty outer medulla created by the ascending loop amplifies the extraction of water in the descending loop. Without countercurrent, much less water would be removed and therefore would be less efficient.
Countercurrent Exchanger: Vasa Recta The Vasa Recta (peritubular
capillaries parallel to the Loop of Henle
• Maintain the osmotic gradient
• Deliver blood to the medullary tissues
• Protect the medullary osmotic gradient by preventing rapid removal of salt, and by removing reabsorbed H2O
NaCIH2O
NaCIH2O
NaCIH2O
NaCIH2O
NaCIH2O
NaCIH2O
NaCIH2O
NaCIH2O
Vasa recta
To vein
Osmolalityof interstitialfluid(mOsm)
Blood fromefferent arteriole
Innermedulla
Outermedulla
Cortex
Passive transport
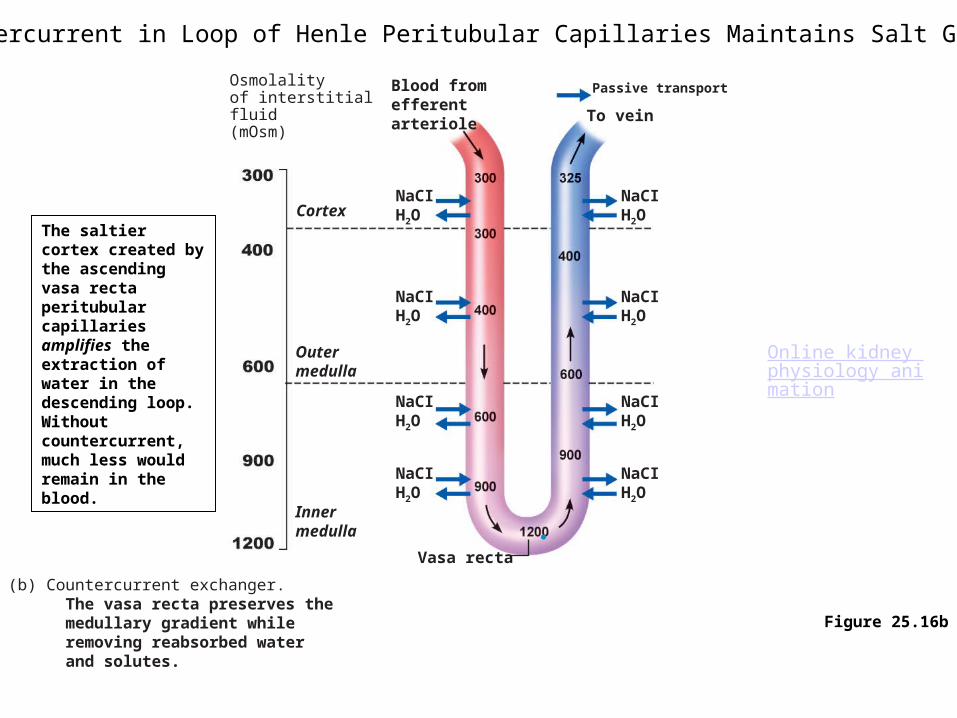
(b) Countercurrent exchanger. The vasa recta preserves the medullary gradient while removing reabsorbed water and solutes.
Figure 25.16b
Countercurrent in Loop of Henle Peritubular Capillaries Maintains Salt Gradient
Online kidney physiology animation
The saltier cortex created by the ascending vasa recta peritubular capillaries amplifies the extraction of water in the descending loop. Without countercurrent, much less would remain in the blood.
Urea Recycling Urea moves between the collecting ducts and
the loop of Henle
• Secreted into filtrate by facilitated diffusion in the ascending thin segment
• Reabsorbed by facilitated diffusion in the collecting ducts deep in the medulla
• More collecting duct reabsorption if ADH present
Contributes to the high osmolality in the medulla
Diuretics Chemicals that enhance the urinary output
• Osmotic diuretics: substances not reabsorbed, (e.g., high glucose in a diabetic patient) causes increased water and urine volume
• ADH inhibitors such as alcohol
• Substances that inhibit Na+ reabsorption and obligatory H2O reabsorption such as caffeine and many drugs
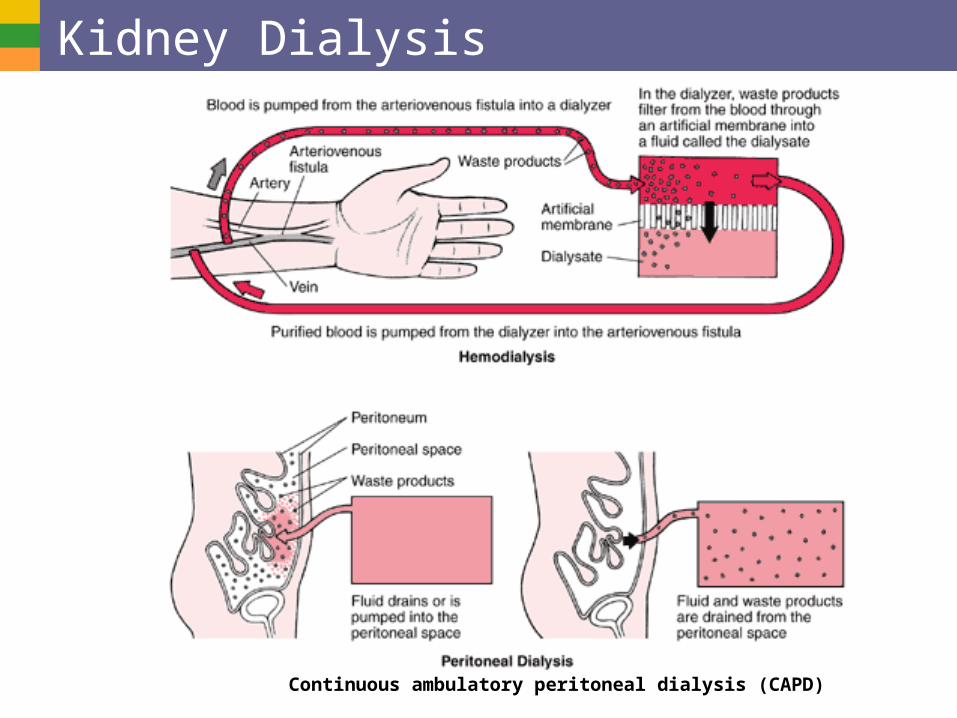
Kidney Dialysis
Continuous ambulatory peritoneal dialysis (CAPD)