Embed Size (px)
Citation preview
Rev Mex Urol 2010;70(3):187-192 187
CLINICAL CASE
Corresponding author: Dr. Víctor Alfonso Francolugo Vélez. Pericón esquina Angélica 5º piso-502. Colonia Miraval. Cuernavaca, Mor. Telephone and Fax: (777) 314 0555. Email: [email protected]
1 Urologist. Sanatorio Henri Dunant, Professor at the Universidad Au-tónoma del Estado de Morelos. Mexico.
2 Pathologist. Hospital Carlos Calero Elorduy, ISSSTE. Cuernavaca, Morelos. Mexico.
Urinary tract infection from Schistosoma haematobium: a case in Cuernavaca, Morelos, MexicoFrancolugo-Vélez VA,1 Zarzosa-Alguiar J.2
•ResumenLa Esquistosomiasis, llamada también Bilhariasis o Bilhar-siosis, es una enfermedad que puede causar cistitis hemo-rrágica y asociarse a cáncer vesical. La esquistosomiasis es causada por Schistosoma haematobium, es más frecuente en África y en el medio Oriente y es de alta contagiosidad para el ser humano durante la fase larual del platelminto.
Caso clínico: Masculino de raza negra, de 24 años de edad originario de Nigeria, con hematuria discreta de un año de evolución. La urotac reveló microlitiasis renal en el cá-liz medio del riñón derecho y tumoraciones vesicales. La biopsia por cistoscopia reportó cistitis aguda y crónica con hemorragia y metaplasia epidermoide, lesión consecutiva a infección por huevos de Schistosoma haematobium. Se administró tratamiento con prazicuantel.
Palabras clave: Schistosoma haematobium, hematuria, México.
•AbstRActSchistosomiasis, also known as Bilharziasis or Bilharsiosis, is a disease that can cause hemorrhagic cystitis and be associated with bladder cancer. Schistosomiasis is caused by Schistosoma haematobium. It is more frequent in Africa and the Middle East and is highly contagious for humans in the larual stage miracidia phase of the platyhelminth worm.
Clinical case: The patient is a 24-year-old Nigerian man presenting with mild hematuria of 1 year progression. Kidney microlithiasis in the middle calyx of the right kidney and bladder polyps were revealed by 64-slice computerized tomography. Cystoscopic biopsy reported acute and chronic cystitis with hemorrhage and epidermoid metaplasia, a lesion following Schistosoma haematobium egg deposition. Patient was treated with praziquantel.
Key words: Schistosoma haematobium, hematuria, Mexico.

188 Rev Mex Urol 2010;70(3):187-192
Francolugo-Vélez VA, et al. Urinary tract infection from Schistosoma haematobium: a case in Cuernavaca, Morelos, Mexico
•IntRoductIonSchistosomiasis, originally known as Bilharziasis (or Bilharsiosis) is a parasitic disease produced by the platyhelminth worm of the class Trematoda, genus Schistosoma (commonly known as blood-flukes and bilharzia) and is relatively common in developing countries, especially on the continent of Africa1 and in central rural zones of Egypt and China.2
It dates from ancient times, as bilharzia eggs have been found in mummies and hematuria (principal symptom) has been registered in ancient papyri from Kahun in Egypt.
In 1851, Theodor Maximilian Bilharz discovered parasites in portal circulation and associated them with being causal agents of cystitis. 1-3 Pirajá da Silva first described the pathogenic agent in 1908.1 In 1911, Ferguson was the first to report the high frequency of bladder cancer and its etiological relation to urinary bilharziasis.3
There are 5 species of Schistosoma parasites that produce schistosomiasis in humans and each of them has its respective clinical manifestations: 4,2
• Schistosoma mansoni and Schistosoma intercalatum cause intestinal schistosomiasis.
• Schistosoma japonicum and Schistosoma mekongi cause the Asian variety of intestinal schistosomiasis.
• Schistosoma haematobium causes urinary schistosomiasis 5 and is most frequent in Africa, the Middle East and the Mediterranean.1
The disease is the result of the granulomatous response of the definitive host to the Schistosoma egg and pathophysiology is related to the life cycle of the parasite. Parasite eggs hatch upon contact with fresh water, releasing free-swimming miracidia. The miracidia infect the Bulinus snail which acts as an intermediary host. Here the miracidia undergo asexual reproduction and are transformed into cercariae which are the larval form of the parasite that is capable of infecting mammals. Cercariae are released into the water as free-swimming organisms with tails. They attach to humans and penetrate the skin (penetration can take place after only 10 seconds of contact of human skin with contaminated water). They lose their tails during penetration and become schistosomulae that then enter into the circulatory system. 6
Schistosomulae migrate to portal blood in the liver and mature into adults. After fertilization, females reach the bladder plexes through the portal system.
Adult worm: The adult worm is from 10-15 mm in length and 2 mm wide. It releases its eggs in blood vessels adjacent to the bladder. The eggs pass
through the bladder wall and exit the body in urine. Adult worms can live in the body from 2-18 years. The worms themselves do not cause inflammatory vascular reaction. Pathology is the result of the progressive immune response. 7
Egg: Parasite eggs cause the first disease manifestations. They are rarely taken into account and are the cause of later chronic Schistosomiasis.
Principle damage is the formation of granulomas caused by the immunological response to the eggs and the parasite. Inactive schistosomiasis may occur after adult worms have died and viable eggs are not presented in tissue or urine, resulting in the so-called bilharzial granulomas found in the bladder wall and containing calcified eggs.7
When viable eggs are released in fresh water they hatch, producing a miracidium embryo. It swims towards the Bulinus snail and penetrates its tissue where it transforms into the larval form of the parasite, infesting the snail, and the cycle is repeated.
Clinical manifestations: The acute form is called Katayama syndrome or fever and it is rarely identified since it occurs 3-9 weeks after infection. It is characterized by fever, lymphadenopathy, splenomegaly, eosinophilia, urticaria, dermatitis in the penetration zone, headache and general malaise.
Chronic form due to the presence of eggs in the bladder wall, ureter or genital organs and its accompanying inflammatory granulomatous reaction occurs at 2-7 months after infection. It is characterized by discontinuous hematuria with bright red blood that can be accompanied by dysuria, frequent urination, reduced bladder capacity, pain in the lower back, pelvic pain and urinary incontinence. Bladder ulcerations may present and it is possible for this disease to lead to epidermoid bladder carcinoma.
Diagnosis: Diagnosis is made through the study of urinary sediment in the search for eggs. Urine should be collected between 11:00 and 14:00 hours, considered to be the hours in which there is maximum parasite expulsion.8 Infection is classified as mild when there are less than or equal to 50 eggs per 10mL and serious when there are more than 50 eggs per 10mL.5 Recount of the amount of eggs in urine sample enables the severity of the infection to be evaluated.
Analysis of the same urine sample determines the presence of proteinuria or hematuria and urinary cytology can reveal the presence of tumor cells.
An enzyme-linked immunosorbent assay (ELISA) test in Gimvi, India, has been reported that uses antigens derived from S. haematobium and S. mansoni
Rev Mex Urol 2010;70(3):187-192
Francolugo-Vélez VA, et al. Urinary tract infection from Schistosoma haematobium: a case in Cuernavaca, Morelos, Mexico
189
adult worms. It has been pointed out that patients that excrete schistosomiasis eggs in urine, test positive for ELISA titers. 2
Eosinophil cationic protein (ECP) measurement in urine will be much higher, the greater the urinary tract invasion, since it can combined with both bladder and upper urinary tract lesions.2, 9,10
In the United Kingdom there are a variety of serological methods for diagnosing schistosomiasis. The Hospital of Tropical Diseases in London uses an ELISA with raw Schistosoma mansoni, soluble egg antigens (SEA), with 97% specificity and 96% sensitivity (S mansoni).11
Simple abdominal X-ray can show fine, more or less continuous, lineal calcifications in the bladder wall, total bladder wall calcification, porcelain bladder or calcification of the distal segment of the ureter. Ultrasound (US) has been shown to be useful in the diagnosis of Schistosomiasis haematobium infection of the urinary tract by revealing data such as thick mamelonated bladder wall, sessile or pedunculated bladder polyps or pyelocaliceal dilatation with irregular cavities. Unfortunately only severe pathology can be visualized and mild bladder lesions cannot be detected with this method. 9 Excretory urography can localize ureteral stricture and identify hydronephrosis as consequences of this type of parasite.
Cystoscopy is carried out in cases in which egg recount is not conclusive and enables a biopsy sample to be taken in order to rule out neoplastic degeneration.
As concluded by da Silva,12 cystoscopy is an important procedure for detecting schistosomiasis in cases of hematuria and other bladder affectations in the study of disease from S. haematobium, particularly in cases in which non-invasive semiological evaluation has not been able to establish diagnosis.
Control studies should be carried out every 6 months and should be complemented with bladder biopsy in cases in which alterations of the bladder mucosa have been observed. Immunological studies should be repeated and when necessary new treatment should be administered with cystoscopy follow-up. 12
Treatment of choice: Praziquantel is active for all clinical forms and disease stages at a single dose of 40 mg per kg of weight.
•cAse pResentAtIonThe patient is a 24-year-old black man born in Nigeria. He has been studying at the university level for 3 years in Cuernavaca, Morelos, Mexico with a scholarship from his native country. He had no previous medical history of importance.
Patient sought medical attention in July 2008 for mild, colicky pain in the upper left abdominal quadrant that also presented occasionally upon deep breathing. Nausea of 15-second duration presented once or twice a week. Patient had no urinary discomfort but occasionally presented with mild hematuria when beginning to urinate, a symptom which had a 1-year
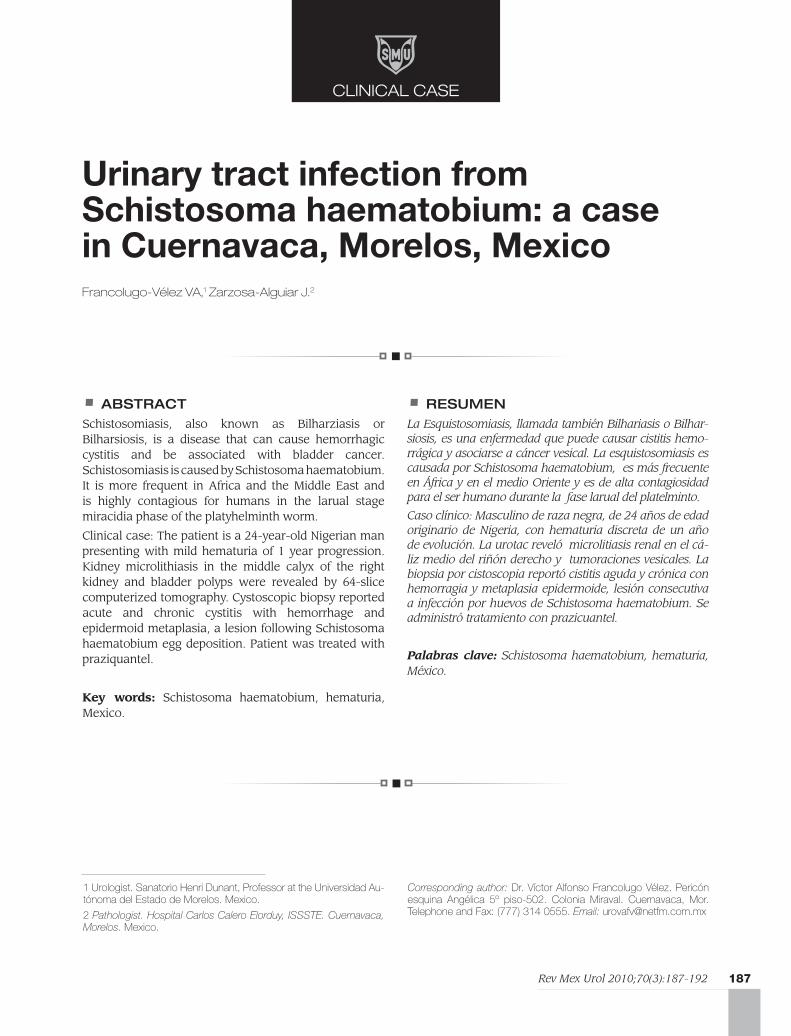
Image 1. Bladder level URO-CT study. Arrows show two small tumors; the one at the bladder dome measures approximately 8.6 mm.
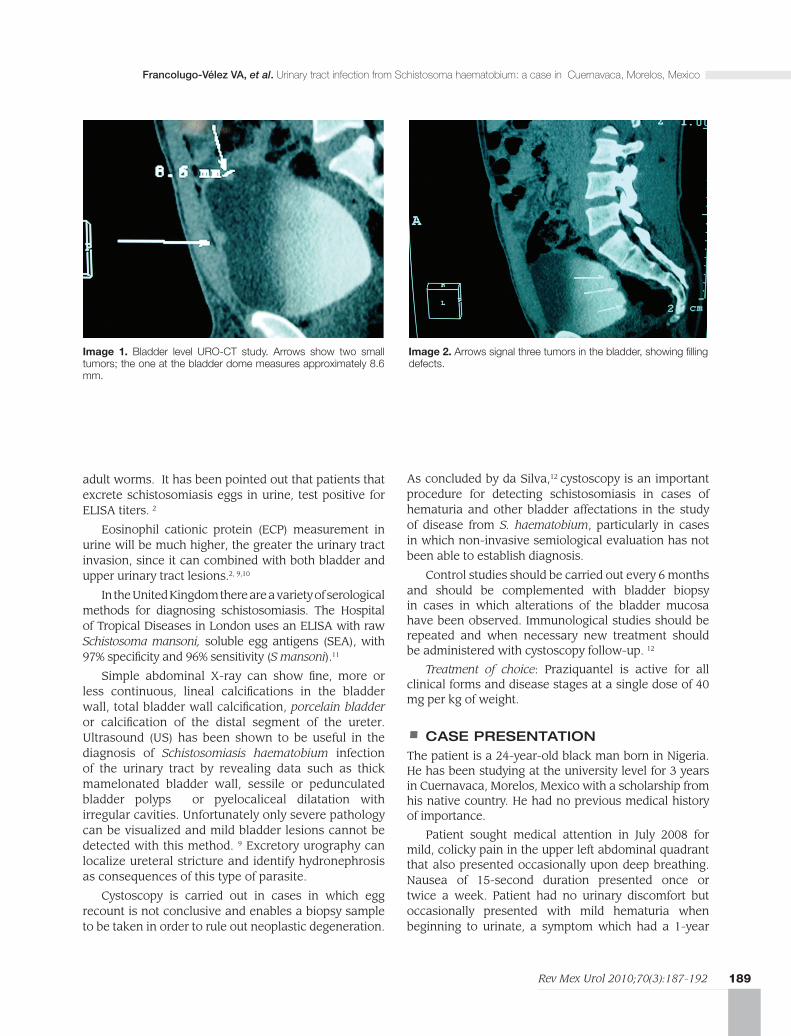
Image 2. Arrows signal three tumors in the bladder, showing filling defects.
190 Rev Mex Urol 2010;70(3):187-192
Francolugo-Vélez VA, et al. Urinary tract infection from Schistosoma haematobium: a case in Cuernavaca, Morelos, Mexico
progression. Renal US reported an approximately 5 mm calculus in the mid-calyx of the left kidney.
Simple kidney tomography results were doubtful in regard to the presence of the calculus seen with the previous US. Urinalysis reported some bacteria, 1-2 erythrocytes per field and protein traces. URO-CT was ordered and revealed non-obstructive microlithiasis in the mid-calyx of the right kidney of approximately 3 mm as well as multiple bladder polyps (Images 1 and 2).
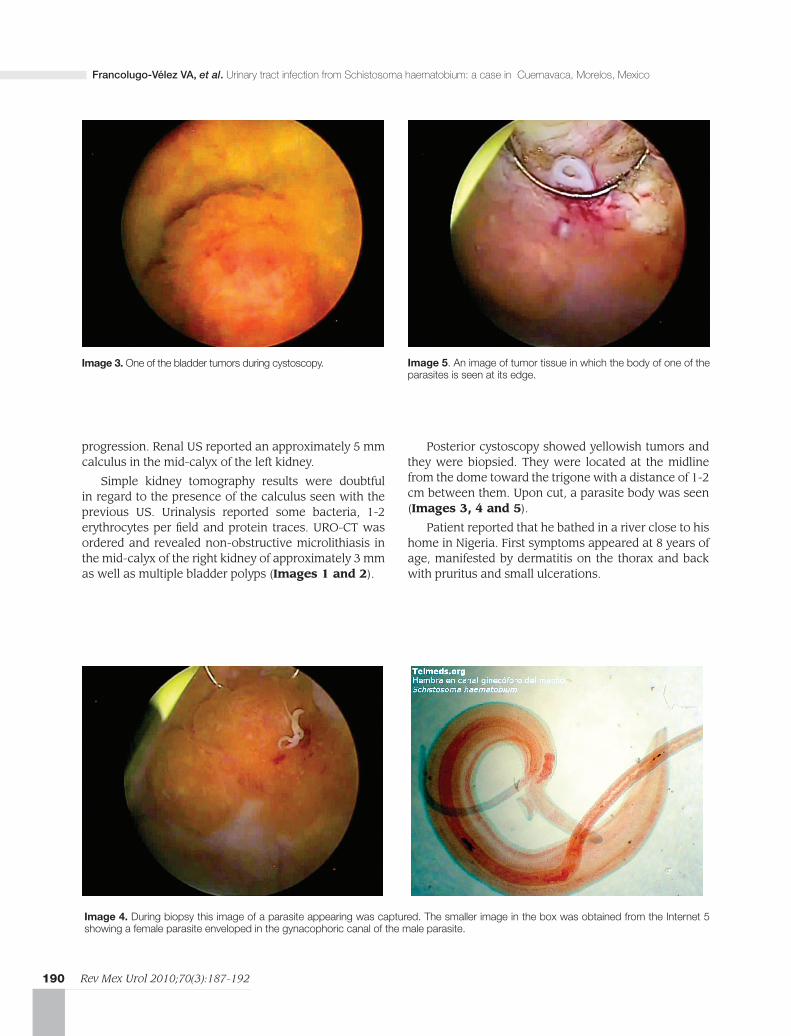
Posterior cystoscopy showed yellowish tumors and they were biopsied. They were located at the midline from the dome toward the trigone with a distance of 1-2 cm between them. Upon cut, a parasite body was seen (Images 3, 4 and 5).
Patient reported that he bathed in a river close to his home in Nigeria. First symptoms appeared at 8 years of age, manifested by dermatitis on the thorax and back with pruritus and small ulcerations.
Image 3. One of the bladder tumors during cystoscopy.
Image 4. During biopsy this image of a parasite appearing was captured. The smaller image in the box was obtained from the Internet 5 showing a female parasite enveloped in the gynacophoric canal of the male parasite.
Image 5. An image of tumor tissue in which the body of one of the parasites is seen at its edge.

Rev Mex Urol 2010;70(3):187-192
Francolugo-Vélez VA, et al. Urinary tract infection from Schistosoma haematobium: a case in Cuernavaca, Morelos, Mexico
191
Schistosomiasis was suspected and patient was given a single dose of 40 mg per kg of weight of praziquantel. Biopsy histopathological report confirmed diagnosis of acute cystitis and chronic hemorrhage with epidermoid metaplasia as a consequent lesion of S. haematobium (Image 6).
A month and a half after treatment, repeat cystoscopy and laboratory exams were carried out to detect eggs or parasites in urine. Urine cytology was negative for malignant cells and there was no evidence of parasites.
Patient experienced intense headache and an episode of lipothymia as secondary effects of treatment. Cystoscopy revealed pale mucosa with reddened zones and small granulomas without tumor. Biopsy was taken of this tissue and histopathological study reported three 5-7 mm light brown, slightly softened, malleable fusiform fragments. Microscopically, chronic inflammatory process with lymphocyte and plasmatic cell formation with intermediary cytoplasmic histiocytes was observed. No parasites were identified. Diagnosis was: subacute and chronic cystitis with no observation of malignant neoplastic elements.
Two more studies were carried out in March and October 2009 with normal results and no hematuria.
•dIscussIonMore than 200 million people in the world in tropical regions suffer from schistomsomiasis.11 Its urinary presentation is caused by Schistosoma haematobium which is endemic in 54 cities of Africa. Studies on school-age children show high prevalence of S. haematobium infection. Humans can become infected by coming into contact with contaminated water. The worms install themselves in the vesical plexus and pelvic veins where females deposit from 20-290 eggs per day. The lower urinary tract, ureters and seminal vesicles are the most affected organs. Lesions are characterized by granulomas caused by tissue response to eggs. 13
Schistosoma haematobium is the most common cause of hematuria in endemic cities.5 In women the uterus, cervix and vagina are most commonly affected. Principal symptoms are hematuria, dysuria, lumbar pain, bacterial infection data, dysmenorrhea, leukorrhea, abdominal pain and intermenstrual bleeding. 13
Identification of S. haematobium infection cases meriting treatment is generally based on microscopic detection of eggs in urine in endemic populations, especially in children. From data of 45 studies that included 74 schools and 28 communities, detected microhematuria prevalence was evaluated. Its presence was found to be slightly lower in communities (16%) than
in schools (24%) and the evaluation of 4 techniques for detecting S. haematobium pathology or morbidity was focused on: US for bladder pathology, reactive strips for microhematuria, interrogation for macrohematuria or macroscopic urine examination. It was concluded that more cases of the same degree of pathology were detected by US in children than in adults and that reactive strip was superior to interrogation.14
There is a lack of knowledge and information in the population about schistosomiasis. Only 0.78% has knowledge of the disease and 16 out of 133 children (in Mina, Nigeria) reported having blood in urine for which they sought medical attention.8 It has been documented that there is a greater infection frequency in children than in adults.5
In a retrospective study by the University of Cairo in Egypt, carried out over a 37-year period (1970-2007) on the analysis and time tendency of 9843 patients with bladder cancer caused by schistosomiasis, it was found that the disease was more common in men with a mean age of 46.7 years. The most common histological type was squamous cell carcinoma. There was muscle layer invasion in advanced stage cases and therefore the principal line of treatment was radical cystectomy. 3
It was noted in this study that patients treated from 2003-2007 showed a significant reduction in bladder cancer frequency that was associated with a reduction in egg frequency of this parasite, reduction of squamous cell cancer and an increase in transitional cell carcinoma. Mean age of patients was 60.5 years.
Image 6. Schistosoma haematobium egg.

192 Rev Mex Urol 2010;70(3):187-192
Francolugo-Vélez VA, et al. Urinary tract infection from Schistosoma haematobium: a case in Cuernavaca, Morelos, Mexico
There was also a reduction in prevalence among men from 5.4-3.3%.3
In the present case, cystoscopy was very important since this disease has been demonstrated in patients who are not living in endemic populations but who have been in them. Results, even after a second treatment, have shown the continued presence of granulomas and viable eggs in 33% of patients, despite negative urine tests. 3 In addition, the possibility of therapeutic failure with praziquantel exists, underlining the need for research on new alternative therapeutics.6 Control cystoscopy must be carried out every six months or every year. This is still pending in the present case, but the patient is currently asymptomatic.
BIBLIogrAphy
1. Internet Wikipedia; http://en.wikipedia.org/wiki/Schistosomiasis 2009; pag. www.sci-ntds.org.
2. Viroj Wiwanitkit. Overview of clinical reports on urinary schistoso-miasis in the tropical Asia. Pak J Med Sci 2005;21(4):499-501.
3. Gouda I, Mokhtar N, Bilal D. Bilharziasis and bladder cancer: a time trend analysis of 9843 patients. J Egypt Natl Canc Inst 2007;19(2):158-162.
4. Lopes RI, Leite KR, Prando D. Testicular schistosomiasis caused by Schistosoma mansoni: a case report from Brazil. Braz J Infect Dis 2007;11(5):523-524.
5. Nmorsi OP, Ukwandu NC, Ogoinja S. Urinary tract pathology in Schis-tosoma haematobium infected rural Nigerians. Southeast Asian J Trop Med Public Health 2007;38(1):32-37.
6. Silva IM, Pereira Filho E, Thiengo R. Schistosomiasis haematobia: Histopatological course determined by cystoscopy in patient in whom praziquantel treatment failed. Rev Inst Med Trop Sao Paulo 2008;50(6):343-346.
7. Murra Atlas de Videoendoscopía. El Salvador 2009. http://www.gas-trointestinalatlas.com/Espanol/Colon_y_Recto/Parásitos/parásitos.html
8. Chidozie EU, Daniyan SY. Urinary schistosomiasis epidemiological survery of urinary schistosomiasis among children in selected schools: A preliminary study in Minna, Nigeria. African J.of Biotech-nology 2008;7(16):2773-2776.
9. Leutscher PD, Reimert CM, Vennervald BJ. Morbidity assessment in urinary schistosomiasis infection through ultrasonography and mea-surement of eosinophil cationic protein (ECP)in urine. Trop Med Int Health 2000;5(2):88-93.
10. Reimert CM, Mshinda HM, Hatz CF. Quantitative assessment of eosi-nophiluria in schistosoma haematobium infections: A new marker of infection and bladder morbidity. Am J Trop Med Hyg 2000;62(1):19-28.
11. Turner P, Lalloo K, Bligh J. Serological speciation of human schistoso-me infections by ELISA with a panel of three antigens. J Clin Pathol 2004;57(11):1193-1196.
12. Silva IM, Thiengo R, Conceição MJ. Cystoscopy in the diagnosis and fo-llow-up of urinary schistosomiasis in Brazilian soldiers returning from Mozambique, Africa. Rev Inst Med Trop Sao Paulo 2006;48(1):39-42.
13. Tzanetou K, Adamis G, Andipa E. Urinari Tract Schistosoma Haema-tobium Infection: A case Report . J Travel Med 2007;14(5):334-337.
14. van der Werf MJ, de Vlas SJ. Diagnosis of urinary schistosomiasis: a novel approach to compare bladder pathology measured by ultra-sound and three methods for hematuria detection. Am J Trop Med Hyg 2004;71(1):98-106.











![Deep, multi-stage transcriptome of the schistosomiasis vector … · 2017. 8. 28. · schistosomiasis - Schistosoma mansoni [7], Schistosoma japonicum [53] and Schistosoma haematobium](https://img.pdfslide.net/doc/110x75/60f8a53e7bdd0764ad39282d/deep-multi-stage-transcriptome-of-the-schistosomiasis-vector-2017-8-28-schistosomiasis.jpg)

















