Embed Size (px)
Citation preview
- 2 -
USAID Kenya (APHIAplus HCM Program) Quarterly Progress Report
(January-March 2014)
REPORT: As at March 31, 2014

i
APHIAplus Health Communication and Marketing Program
Year 3, Quarter 2 Progress Report
(January –March 31, 2014)
Submitted to:
Chief of Party
USAID APHIAplus HCM Program
PS/Kenya.
C/O American Embassy
United States Agency for International Development/Kenya
United Nations Avenue, Gigiri
P.O. Box 629, Village Market 00621
Nairobi, Kenya
Prepared by:
KMET
Prime Award Number : AIDS -615-A-12-00002
P. O. Box 6805-40103,
Kisumu.
The authors’ views expressed in this report do not necessarily reflect the views of the United
States Agency for International Development or the United States Government.

ii
Table of Contents
ACRONYMS AND ABBREVIATIONS ............................................................................................................... IV
1.0 EXECUTIVE SUMMARY .................................................................................................................................... 2
2.0 KEY ACHIEVEMENTS (QUALITATIVE AND QUALITATIVE IMPACT) ............................................. 3
2.1 EVENT DAYS ........................................................................................................................................................................... 3 2.2 COMMUNITY MOBILIZATION ............................................................................................................................................... 4 2.3 BUILDING CAPACITY OF CHWS ....................................................................................................................................... 12 2.4 BUILDING CAPACITY OF MEMBERS ..................................................................................................................................... 13
2.4.1 Contraceptive Technology .................................................................................................................. 13
2.4.2 Integrated Management of Childhood illnesses ............................................................................. 13
2.5 FACILITATIVE SUPERVISION ................................................................................................................................................. 15 2.5.1 Observations from the facilitative supervisions ............................................................................. 15
2.6 PERFORMANCE REVIEW MEETINGS ..................................................................................................................................... 16 2.6.1 Provider performance review meetings ........................................................................................... 16
2.6.2 Achievements ......................................................................................................................................... 19
2.6.3 Performance review meeting Community Health Workers ...................................................... 19
3.0 PROGRAMPROGRESS ................................................................................................................................... 20
IR 1.1: INCREASE ACCESS TO AND DEMAND FOR HIGH QUALITY HEALTH PRODUCTS AND
SERVICES ................................................................................................................................................................................... 20 3.1 FAMILY PLANNING (FP) SERVICES ...................................................................................................................................... 20 3.2 HIV TESTING AND COUNSELLING (HTC) AND COUPLE COUNSELLING SERVICES ..................................................... 21 3.3 CERVICAL CANCER SCREENING SERVICES ......................................................................................................................... 21 3.4 PERFORMANCE MANAGEMENT PLAN ............................................................................................................................... 21
4.0 PERFORMANCE MONITORING ................................................................................................................ 25
5.0 PROGRESS ON LINKS WITH GOK AND OTHER AGENCIES .................................................. 27
5.1 STAKEHOLDERS’ MEETINGS ................................................................................................................................................. 27
6.0 YEAR 3 QUARTER 2 WORK PLAN STATUS ......................................................................................... 27
7.0 HUMAN INTEREST STORIES ....................................................................................................................... 30
7.1 WORKING WITH RURAL COMMUNITIES: BEATRICE’S EXPERIENCES AND LESSONS ....................... 30 7.2 CHALLENGES OF ACCESS TO CONTRACEPTIVE SERVICES AND INFORMED CHOICE .................... 32 7.3 LACK OF FAMILY PLANNING KNOWLEDGE MADE MY LIFE MISERABLE, MOTHER SAYS ................. 33

iii
LIST OF TABLES
Table 1: Event days’ achievements .......................................................................................................................... 3 Table 2: Community mobilizations sessions......................................................................................................... 5 Table 3: Provider performance review meeting ................................................................................................ 16 Table 4: FP service provision ................................................................................................................................. 21 Table 5: HIV testing and counseling (HTC) services ........................................................................................ 21 Table 6: PMTCT service provision ....................................................................................................................... 21 Table 7: Cervical Cancer screening services ...................................................................................................... 21 Table 8: Performance Management Plan ............................................................................................................. 22 Table 9: Actual work plan status (Jan-March, 2014) ........................................................................................ 27

iv
ACRONYMS AND ABBREVIATIONS
CBO Community Based Organization
CHEWs Community Health Extension Workers
CHWs Community Health Workers
COCs Combined Oral Contraceptives
SCHMTs Sub-County Health Management Teams
FP Family Planning
HTC HIV counseling and testing
HCM Health Communications and Marketing
IMCI Integrated Management of Childhood illnesses
HIV Human Immunodeficiency Virus
LARCs Long Acting and Reversible Contraceptives
MoH Ministry of Health
POPs Progesterone Only Pills
PBCC Provider Behavior Change Communication
PMTCT Prevention of Mother-to-Child Transmission of HIV/AIDS
USAID United States Agency for International Development
USG United States Government
VIA Visual Inspection by Acetic Acid
VILI Visual Inspection by Lugos Iodine

2
1.0 EXECUTIVE SUMMARY
KMET implements Health Communication and Marketing (HCM) activities through Huduma Poa social
franchise. The social franchising approach offers a significant opportunity to integrate health services with
the aim of improving availability and access to high quality, affordable health products and services.
During the quarter (January-March 2014), a number of activities were implemented:
facilitation of 38 event days and 84 community mobilization activities at different social franchise
and community units respectively
orientating of 106 Community Health Workers on key messages on HIV testing and counselling
and cervical cancer
Production and distribution of IEC materials for demand creation
building capacity of 22 social franchise providers on contraceptive technology; and 24 providers on
integrated Management of childhood illnesses (IMCI)
conduct provider and CHWs performance review meetings
participate in the stakeholders meetings
provision of facilitative supervision to providers in the social franchise
forging linkages between franchise facilities with local Ministry of Health (MoH)
There has been a challenges in the roll out of ART services across selected franchise facilities. The
process has been slow.

3
2.0 KEY ACHIEVEMENTS (Qualitative and Qualitative Impact)
RESULT 1: Increased Use of Quality Health Services, Products and Information.
IR 1.1: Increase Access To and Demand for High Quality Health Products and Services
2.1 Event days
Within the reporting period, KMET conducted thirty eight (38) Huduma Poa days ( 36 facility based event
days and 2 outreaches) aimed at improving access to quality health products and services, 504 clients
received contraceptive services (333 implant insertions, 61 IUCDs insertions, 86 Injectables, 24 oral
contraceptives) during event days.
These data is exclusive of data generated
from daily service provision across
franchised facilities between January-
March 2014. The utilization rate of
contraceptive services through event days
improved by 338% compared to the
previous quarter when only 115 clients
received family planning services.
Considerably, 356 clients were counseled
and tested on HIV, of whom, 13 tuned
positive and referred to patient support
canters for initiation of care and
treatment.
The table below illustrations achievements of event days held during the reporting period.
Table 1: Event days’ achievements
January –March, 2014
Integrated reproductive health Services during Huduma Poa days #= 38 Huduma Poa days
Implants IUCDs Injectables Oral
contraceptives
Cervical
cancer
screening
Suspicious
for cancer
Via/Vili
Positives
Cervical
polyps
Referred
for
treatment
HTC HIV Positive
clients
333
61
86
24
461
14
25
0
29
356
13
Figure 1: A provider and CHWs giving Health Education during event day

4
Up to 461 women who turned for event days were screened for cervical cancer in an effort to enhance
integration of reproductive health services. Among them, 25 turned positive for VIA/VILI whereas 14
exhibited suspicious signs for cancer of the cervix. Significantly, 29 of the clients screened clients were
appropriately referred for treatment.
Community Health Workers (CHWs) Workers have continued to mobilize, create demand and forge
linkages between communities and Huduma Poa network.
There were more event days conducted
within the reporting period compared to
the previous quarter at which, only 15 event
days were conducted. Community Health
Workers have actively engaged themselves
in creating demand for supported services
offered across franchise facilities.
Huduma Poa days have continued to
promote accelerated uptake of the much
desired method – mix in family planning and
created an opportunity to mentor
providers to acquire prerequisite
competence and skills for insertion of LARCs, interpreting VIA/VILI cervical cancer screening results, and
improved contraceptive cancelling.
2.2 Community mobilization
Mobilization activities intensified within the reporting period. Up to 85 community mobilizations sessions
were conducted at community units, youth groups, community barazas and CBO reaching out to 5866
clients (2118 males and 3728 females)-The figure is 29.3% higher than that of the previous quarter when
only 4536 persons were reached through mobilization activities. This may be attributed to increased
mobilization activities geared towards behavior change .Community Health Workers (CHWs) Workers
continued to mobilize, create demand and forge linkages between communities and Huduma Poa network
facilities in line with the in line with the MoH community strategy synergistically linked both to IR 1.1 and
IR 1.2 (increase access to and demand for high quality health products and services; and improve adoption
and maintenance of healthy behavior.
Figure 2: Clients queue at Huduma poa facility with
referral forms from CHWs
5
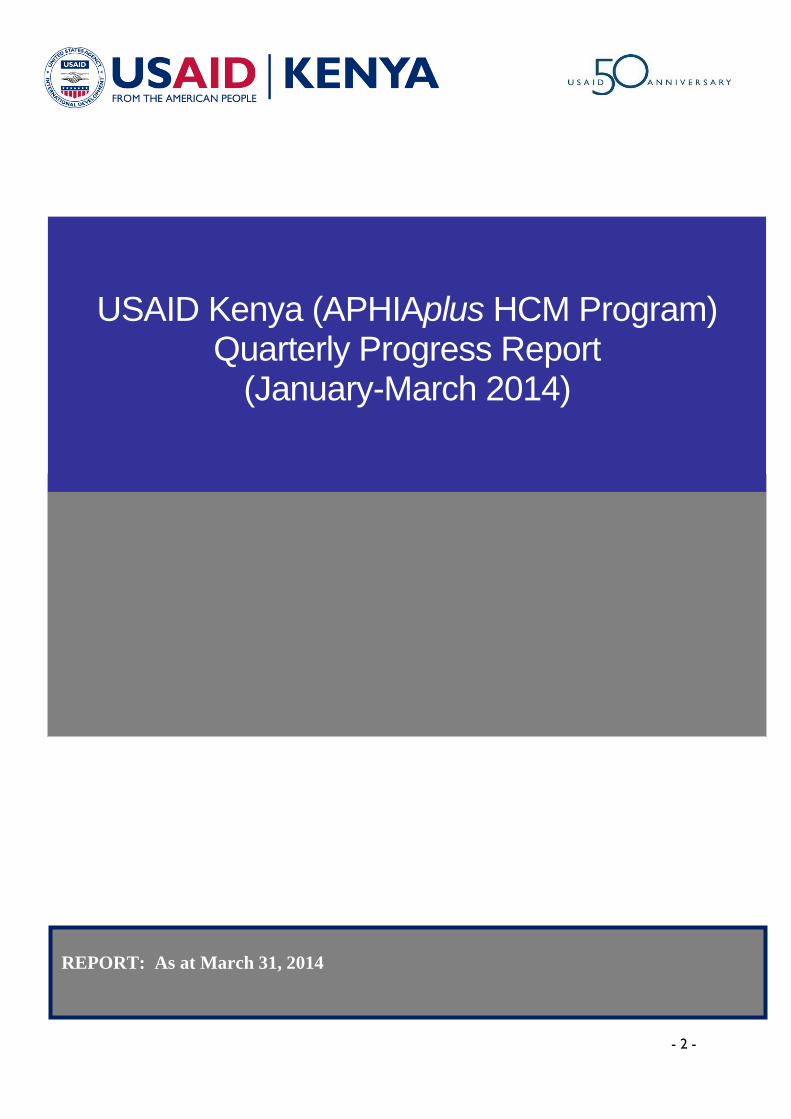
Men constitute only 36% of the
attendees. Majority (64%) of
attendees were women. The sessions
were aimed at equipping target
communities with accurate and
reliable information on family
planning, cervical screening and
HIV/AIDS. This has been deemed
appropriate in demystifying myths and
misconceptions that have profoundly
hindered the utilization integrated
reproductive health services.
Similar to previous quarter, efforts
have been put in place to promote utilization of IUCDs, whose utilization level has been low (3% in the
previous quarter-July-September, 2013). Most of mobilization communications focused on repositioning
IUCD as a highly effective, safe, and convenient FP method with unique benefits. Similar repositioning is
expected to continue in the subsequent quarters. We anticipate to facilitate this through emphasizing to
potential users and influential individuals about the benefits of IUCD, and engage current users to convey
the messages on how the method has been highly satisfying. The same current users will be engaged to
dispel common myths related to the method.
Table 2: Community mobilizations sessions
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Borabu
Sub-county
Mwongori chiefs
Baraza,
32 50 Benefits and limitations of modern
methods of contraception
Simbau Farm 41 48 Benefits of integrated reproductive
health services at the social franchise
facility
Importance of cervical cancer screening
Figure 3: Huduma Poa CHW educating women on modern
contraceptive methods during an outreach

6
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Borasa 16 63 Modern contraceptive Methods and
client medical eligibility based on the
WHO eligibility criteria
Keremas 29 82 Benefits of FP
Chepilat market 47 127 Why do we plan our family
Rongo Sub
County
Kodero Bara 31 41 Advantages of Long Term methods
Kanying’ombe 27 122 Addressing myths on IUCD and
implants
Kosiri 17 59 Modern contraceptive Methods and
client medical eligibility based on the
WHO eligibility criteria
Kosodo 24 67
Trans Mara
East
Town Centre 18 24 Family planning & Cervical cancer
screening.
Naikuyan 35 47 Modern contraceptive Methods and
client medical eligibility based on the
WHO eligibility criteria
Oloiborsoita 27 32 Benefits of integrated reproductive
health services at the social franchise
facility
Importance of cervical cancer screening
Oldonyokosha 11 15 Feedback Meeting to community
stakeholders
Leporosi (chiefs
Meeting)
36 18 Benefits and limitations of modern
methods of contraception
Manga Ogango Chiefs
Baraza,
17 38 Counselling on various FP methods and
their importance

7
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Tinga Villages, 11 31 Advantages of non-hormonal methods
of FP
Bondeni Village 25 48 Benefits and limitations of modern
methods of contraception
Kisumu
East
Kasawino 3 23 Benefits of long term family planning
methods
Magadi 25 51 Experience sharing on FP use
Kuoyo Konunga 21 52 Importance of FP and HTC: experience
sharing
Suna East Giribe 21 43 Methods of FP advantages and
disadvantages.
Manyera 37 57 Benefits of long term family planning
methods
Nyamaraga 25 63 Non Hormonal
Bondo Nyironge 14 26 Importance of FP and HTC: experience
sharing
Bungoma
South
Tuuti
4 68 Benefits of long term family planning
methods
Bukembe
Nzoia Med.
Centre
34 80 Addressing myths on IUCD and
implants
Bungoma
East
Mihuu
Jaggary Clinic
29 98 Benefits of Family Planning and HTC
Bungoma
Central
Chwele
Bewa Med. Clinic
65 87 Experience sharing on FP use
Sabatia
Wanondi 23 57 Benefits of Implants and HTC
Chavogere 48 75 Importance of FP and HTC: experience
sharing

8
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Chavakali 42 97 Benefits and limitations of modern
methods of contraception
Bungoma
South
Halaba Jordan
Med. Clinic
23 45 Addressing myths on IUCD and
implants
Halaba Lumboka
Hospital
15 23 Non hormonal methods of family
planning
Halaba Musico
Med. Clinic
38 85 Advantages of Long acting
contraceptives
Bukembe 32 39 Debunking myths on family planning
methods
Bungoma
East
Marinda 39 52 Advantages of family planning and
cancer screening
Mihuu 42 73 Discussing myths on IUCD
Bungoma
Central
Chwele 42 80 Benefits of Implants, HTC and cancer
screening
Sabatia
Wanondi 32 46 Experience sharing on FP use and
cancer screening
Chavakali 36 87 Benefits of Implants and HTC
Kakamega
East
Shinyalu 12 36 Importance of FP and Couple HTC
Kambiri 22 67 Advantages of long acting FP methods
Bungoma
South
Halaba 11 15 Services offered at Lumboka and
charges
Halaba
12 18 Addressing myths on IUCD and
implants
Halaba
20 48 Benefits of early screening of Cervical
cancer
Tuuti
18 62 Experience sharing on FP use and
Couple HTC
Bukembe
18 51 Benefits of Cervical cancer screening
and HTC

9
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Bungoma
East
Marimba
23 42 Importance of FP and HTC
Mihuu
15 23 Advantages of long acting FP methods
and Clinic charges
Bungoma
Central
Sabatia
Chwele
35 52 Advantages of IUCD/Services offered at
Bewa
Wanondi Carol
12 15 Advantages of long acting FP methods
and cancer screening
Kakamega
East
Chavogere
19 52 FP methods and Cancer screening
Shinyalu,
12 35 Importance of Family planning/ Couple
HTC
Kambiri
32 63 Importance of couple HTC and Family
Planning
Emuhaya
Ebusikhale
(Makutano Med
Clinic)
11 16 Addressing myths on Family planning
Chavakali
32 48 Non hormonal Family planning
methods.
Mumias Township
14 21 Advantages of Long acting
contraceptives and cancer screening
Siaya Ngi’ya Chiefs
Camp
87 68 Importance HIV Testing and counselling
Siaya Compassion
Mothers Group
1 22 Importance cervical cancer screening
Family Planning Methods mix
Siaya Gulf Pri.School
(Ng’iya C.U)
28 37 Types of FP methods
Importance of knowing your HIV status
Gem Ndere
Dispensary
97 108 Importance of Cervical cancer
screening
Long term FP methods
Gem Nyabeda Village 13 24 Importance of Family planning

10
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Gem Nyabeda Youth
Group
19 14 HTC
Benefits of long term FP methods
Types of FP- Lactation amenorrhea
method
Gem Ndere Sda
Church
18 23 Importance of cervical cancer screening
Couple testing in HTC
Gem Ndere Ack
Church
30 45 Counselling in FP and cervical cancer
screening
Mbita Kogalo Beach
(Waware)
32 16 HTC and contraceptive use.- Female
and Male condoms
Mbita Waware
Dispensary
19 38 Importance CA screening
Family Planning Methods
Kisumu
west
Bidii Youth
Group
12 16 Importance HIV Testing and counselling
Gem Ukulima Group 11 4 Benefits of long term FP methods over
short term FP methods
Kisumu
west
Lela Chiefs Camp 20 30 Importance CA screening
Family Planning Methods-implants.
Kisumu
east
Obunga Village 15 25 Long term FP methods
Importance of knowing your HIV status
Kisumu
east
Kasarani Village 8 20 Importance of CA cancer screening
Siaya Karemo Chiefs
Camp
30 16 Long term FP methods
Bondo Gobei Health
Centre (Bar
Chando)
20 15 Importance of early Cervical Cancer
screening
Ugunja Ambira Market 22 30 Benefits of long term FP methods

11
SUB-
COUNTY
COMMUNITY
UNIT
NUMBER OF
PEOPLE
REACHED
HEALTH EDUCATION AREAS
COVERD
Male Female
Ugenya Sihay Self Help
Group
13 23 HTC importance of couple testing
Mbita Kasgunga Central
CU
13 24 Importance of cervical cancer screening
Gem Kodiaga Village 24 18 Importance of knowing your HIV status
Rarieda Omia Diere.E Cu 17 23 Introduction of the and the HCM
program & CHWs to the group
Bondo Mahanga Village 14 11 Importance of cervical cancer screening
Bondo Kabarua Village 15 21 Long term FP methods (IUCD)
Bondo Magare Island 13 24 Knowing your HIV status
Bondo Gobei Youth
Group (Bar
Chando)
6 24 Importance of early cervical cancer
screening
Homabay Piki Piki
Associates Group
63 1 Benefits of HIV testing and counselling
Homabay Wakianga
Polytechnic
(Rusinga)
6 45 Types of Family Planning methods
Total number of clients
reached
2118
3748
Demand creation activities have helped raise awareness on reproductive health issues at the community
level and mitigate on social and cultural issues that promote or inhibit use of reproductive health products
and services. Furthermore we focused on and will continue to improve clients’ understanding of various
contraceptive methods enabling them draw distinctions between facts and myths associated to the specific
methods.
Within the reporting period, 1112 clients were directly referred from the community to access services at
the social franchise. There has been more men (2118) coming out to participate reproductive health event
days- a domain that has previously been regarded as women’s sole responsibility.

12
Target communities around Huduma Poa clinics (both men and women) can now freely discuss reproductive
health issues at community barazas, dialogue days and during other forms of mobilization sessions. It is no
longer a sole affair for women. This been evident across all the 85 community mobilizations held during
the reporting period.
Demand creation and community mobilization activities will continue in the subsequent quarter as key a
key strategy for increasing access to and demand for high quality health products and services.
2.3 Building capacity of CHWs
Forty 106 community health workers (CHWs) underwent a 2 days’ orientation on HIV testing and
counseling and cervical cancer to enhance their understanding and capacity to proficiently engage
communities during demand creation on integrated reproductive health services. This is aimed at improving
facility-community linkages in promoting sustainable demand and utilization of quality healthcare services.
This complements previous orientations that have been given to Community Health Workers on
community strategy, modern family planning methods, contraceptive counseling and Tiahrt Amendment
To date, there are 120 CHWs have been
engaged and trained for efficacious
program implementation across 60 social
franchise facilities in line with the Ministry
of Health Community Strategy.
Two (2) CHWs are assigned per social
franchise outlet to forge linkages between
the facilities and target communities in line
with the MOH community strategy; and
mobilize surrounding communities in
ensuring sustainable demand and
utilization of quality health care services
that are accessible and affordable to consumers of health services accessing care. Within the reporting
period 1112clients were referred from the community to access services at the social franchise.
In the subsequent quarters, CHWs will be oriented in child health in order to improve their proficiency in
correctly identifying giving health messages and referring children with childhood illness for effective
management.
Figure 4: Community Health Workers undergoing
capacity building session

13
2.4 Building capacity of members
2.4.1 Contraceptive Technology
Within the reporting period, KMET collaborated with the local Ministry of Health in Migori to train 23
healthcare providers on contraceptive technology to strengthen their capacity to offer comprehensive
contraceptive services; and accelerate quality integration of HIV testing and counselling (HTC) and cervical
cancer screening services.
Integrating cervical cancer and HIV
counseling and testing services to family
services across franchise facilities
guarantees prudent utilization of scarce
resources while ensuring clients receive
integrated services under one roof
without placing an undue burden on
health care service provision. It creates
opportunities for clients to access
multiple services simultaneously resulting
to more efficient services, better
treatment adherence, and more holistic care.
Social franchise providers were trained on contraceptive method mix (Permanent, Long Acting and
Reversible Contraceptives; and short term Methods). The training focused in ensuring providers correctly
provide balanced contraceptive information to their clients to enable them choose methods that best suits
them. Making a wide range of methods available improves quality of care.
2.4.2 Integrated Management of Childhood illnesses
Order to strengthen the ability of Huduma Poa health facilities to offer improved prevention and
management of childhood illnesses, KMET collaborated with the MoH-Kisumu to train 26 providers on
Integrated Management of Childhood illnesses (IMCI). The training focused on equipping providers with
desirable knowledge and skills to accurately assess, classify, identify treatment and treat ill children using
the IMCI protocol, The strategy provides an integrated approach for standard management of major causes
of childhood morbidity and mortality like Pneumonia, Diarrhoea, Malnutrition, Neonatal problems, Measles
and Malaria. The approach offers simple and effective methods to comprehensively prevent and manage
the leading causes of serious illness and mortality in children. This is expected to greatly contribute reducing
child mortality and avert significant child disability.
Figure 5: Providers practicing insertion of IUCDs
during skills session

14
In the subsequent quarters, Huduma
Poa facilities trained are expected
implement what they learnt; and to
go beyond managing single
childhood diseases, but instead
address the overall health of a child.
KMET will work closely with social
franchise providers and community
health workers attached to the
social franchise to reduce childhood
mortality and morbidity by
improving family and community
practices for the home
management of illness, and
improving case management skills of
health workers across the social franchise. Providers will be mentored, given technical support and linked
with MoH and other partners
to access commodities
including: Zinc Sulphate, ORS
sachets, Vitamin A
supplements, Anti-Malaria
Drugs and appropriate
antibiotics.
IMCI has been shown to
improve health worker
performance, but constraints
have been identified in
achieving sufficient coverage to
improve child survival, and implementation remains sub-optimal. At the core of the IMCI strategy is a
clinical guideline whereby health workers use a series of algorithms to assess and manage a sick child, and
give counselling to care givers.
Health workers found the training interesting, informative and empowering, and there was consensus that
it improved their skills in managing sick children. They appreciated the variety of learning methods
employed, and felt that repetition was important to reinforce knowledge and skills. Facilitators were rated
highly for their knowledge and commitment, as well as their ability to identify problems and help participants
as required. Providers’ increased confidence in managing sick children was identified at the
Figure 1: Huduma Poa IMCI participants assessing a child at the
outpatient department during their practicum sessions
Figure 7: IMCI participants keenly follow the sessions as they refer
to guide booklet charts

15
practicum/clinical areas. There is going to be joint KMET-MoH follow-up visits to all providers trained to
ensure acquired knowledge and skills are implemented; and that providers perfect their counselling skills
in an effort to accelerate quality roll out of the services.
2.5 Facilitative supervision
Joint KMET-MoH structured support supervisions were conducted in 5 facilities. In addition, the quality
assurance team conducted 11 monthly facilitative supervisions across 11 facilities in the social franchise to
identify quality gaps and bridge them. These included provision of on job training to inculcate required skills
in implant and IUD insertions, infection prevention, and accurate documentation and reporting. Providers
have continued to benefit from coaching, mentorship and dissemination of appropriate IEC materials
including FP counselling charts and bags to systematically provide information to clients and improve their
competencies essential in the provision integrated quality health care services that meet the demand of
target communities. Support supervision visits focus on adherence to MOH quality standards, improvement
of provider skills and promoting a balanced method mix of contraceptive options that emphasizes on the
use of LARCs and therefore changing the current pattern of predominantly short-acting methods.
2.5.1 Observations from the facilitative supervisions
Profoundly, facilities have improved their monthly reporting of service provision to the ministry. Utilization
of implants has largely increased compared to Intra-Uterine Devices (IUDs). There is
1. Improved provider behavior and attitude regarding provision of integrated reproductive health
services without discriminating any method
2. Enhanced provider knowledge and skills in offer integrated reproductive health services as a result
of provider trainings in Contraceptive Technology, IMCI, HTC and cervical cancer screening.
3. Improved documentation in the service delivery registers ‘
4. Increased client flow to social franchise facilities compared to the period before. This has been
attributed to demand creation and community mobilization facilitated by CHWs attached to social
franchise facilities.
5. success in the integration of family planning, cervical cancer screening and HIV testing and
counselling services across franchise facilities

16
2.6 Performance review meetings
2.6.1 Provider performance review meetings
Within the quarter, Huduma Poa providers conducted performance review meetings intended to review
quarterly social franchise performances, identify gray areas and suggest new methodologies in heightening
quality service provision across social franchise facilities.
Providers had the opportunity to review their joint effort and progress in the provision of FP, cervical
cancer and HTC services. In addition, they shared experiences, success, challenges and possible solutions
to perceived and expressed challenges. This was aimed at establishing and putting in place mechanisms that
will accelerate demand and access for quality integrated services at franchised facilities.
Service data generated from various franchised
facilities was discussed, a line drawn between
providers who are performing exemplary well
and those performing fairly low. Best practices
and strategies used by well performing
providers were discussed, creating a perfect
opportunity for low preforming provides to
learn.
Provider review meetings elicited different
challenges which include: inadequate
equipment for key procedures i.e. insertion
kits; staff turnover, occasional commodities stock out, inadequate space for service integration. Facilities
have improved in monthly reporting of service provision to the ministry.
Table 3: Provider performance review meeting
Provider performance review meeting
Areas discussed Challenges identified Agreed solutions
Equipment and
Commodities
1. Inadequate IUD
insertion equipment at
some franchise facilities
2. Occasional commodity
stock-outs
KMET to identify and link facilities to
a supplier who could sell autoclave
and insertion equipment at a lower
cost and if possible, a supplier who
would allow them pay for the items in
installments
Figure 8: Community Health Workers participate in
their demand creation review meeting

17
3. Lack of autoclave in
some facilities thus
affecting their routine
sterilization of
equipment
Franchise providers agreed to
purchase autoclave and additional
insertion equipment
Franchise facilities to continue
strengthening their forged linkages
with MoH to easy acquisition of FP
commodities and reporting tools
Inter-facility borrowing of
commodities in case one has surplus
i.e. HIV rapid test kits and FP
commodities.
KMET to supply IUCD startup kits to
the new facilities; recently trained
Service Delivery
Low numbers of client
flow at some franchise
facilities
Inadequate space for
reproductive health
service integration in
some facilities
Cost- a barrier to
utilization of services at
some communities
Regular structured joint meetings
between providers and community
health workers to discuss and plan
mobilization sessions.
KMET to design standard form to
evaluate client satisfaction across
franchise facilities
Providers to motivate CHWS to make
them work better
Occasionally, providers to join CHWs
during health promotions and
mobilization sessions to be able to
help them in sharing health messages
with community
Providers urged to charge affordable
costs to enable the communities
access services at the franchised
facility
Providers to continue using
suggestion box to track client
satisfaction

18
Facility providers were tasked to marshal resource and either buy disposable speculums or utilize high level
disinfection and chemical sterilization to ensure equipment are sterilized and service provision is not
impeded. Inaccurate filling of registers by a few service providers was also identified as an area that need
capacity building. In the subsequent quarters, integration of services will continue including HTC and
integrated management of Childhood illnesses (IMCI).
Satisfied clients to be utilized as media
during mobilizations; they act as
advocates for services utilized.
Linkages and
Partnerships
Lack of a joint online
platform for sharing
among franchised clinics
Weak ties between
MoH and some of the
newly recruited
facilities.
Providers to be circulated with
contacts of one another to ease
communication within the franchise
and if possible facilitate sharing of
resources.
KMET establish a common mail to
enable franchise providers to
constantly share best practices
KMET to assist in strengthening
linkages between new facilities and the
MoH
Providers to support CHWs attached
to their facilities in perfecting linkages
with the surrounding communities
Staffing
Staff turnovers at
franchise facilities
infrequently affecting
continuity of quality
services
Inadequate on job
training (OJT) to other
franchise staff by
trained providers
Providers who have trained in
contraceptive Technology, HTC,
IMCI, Cervical Cancer screening to
ensure that the rest at the franchise
facilities are trained.
KMET to continue offering OJT for
the trained staff who have challenges
in service provision

19
2.6.2 Achievements
During the performance review meeting, providers expressed success in the following areas:
1. Increased awareness on services offered at the social franchise facilities as a result of continuous
Huduma poa days
2. Increased client flow to social franchise facilities compared to the period before the start of the
program. This has been attributed to demand creation and community mobilization facilitated by
CHWs attached to social franchise facilities.
3. Enhanced provider knowledge and skills to offer integrated reproductive health services as a result
of provider trainings
4. Improved documentation and monthly reporting to MoH through support supervisions
5. Improved linkages to the community and MoH through demand creation and forged linkages with
the ministry of health
6. Improved supply of contraceptive commodities from the Ministry of Health stores following
fostered linkages and adequate monthly reporting
7. Successful integration of family planning, cervical cancer screening and HIV testing and counselling
services across franchise facilities
8. MOH support for cryo-therapy services in some sub-counties thus facilitating service provision for
VIA/VILI positive clients.
2.6.3 Performance review meeting Community Health Workers
KMET conducted 3 performance review meetings with CHWs attached to social franchise facilities to
review program performance, experiences, success, challenges and possible solutions to perceived and
expressed challenges.
The review meeting provided an opportunity for CHWs to ventilate a number of thematic areas including:
community linkages and partnerships, community-facility referrals and documentation, other avenues of
mobilization including the church, markets and organized groups, client satisfaction and social franchise
service delivery, missed opportunities and
joint provider-CHWs meetings. Staff
turnover and cost were cited as major
challenges at the franchise facility that
occasionally affects provision long acting
and reversible contraceptive services.
Evidentially, clients prefer free services as
opposed to subsidized as it is the case at
the Huduma Poa facilities. During the
review meetings meeting, CHWs were
Figure 2: Program staff demonstrates the use of family
planning counseling bag to the CHWs

20
issued with relevant IEC materials necessary for
their community and household mobilizations.
These included: Family planning counseling bags,
Umbrellas with relevant health promotion
messages, demand creation registers, posters, daily
activity registers and referral forms.
3.0 PROGRAMPROGRESS IR 1.1: INCREASE ACCESS TO AND DEMAND FOR HIGH QUALITY HEALTH PRODUCTS AND
SERVICES
3.1 Family planning (FP) services
Up to 3920 clients received family planning services up from 3271 in the previous quarter (19.84%
higher).Significantly, 800 implants and 169 IUCDs were inserted through the social franchise and two
outreaches conducted in Migori. Up to 2251 clients accessed injectable contraceptives up from 1869
in the previous quarter, 262 received condoms whereas 292 were issued with (combined oral
contraceptives and progesterone only) pills.
Compared to previous quarter, utilization of implants improved by 21.58% whereas utilization of
IUCDs slightly improved by of 8.33%.
Evidently, in some remote rural communities particularly South Nyanza, the unmet needs for family
planning services and other reproductive health services remains acute because clinics or hospitals are
scarce, distant apart (approximately 10 Km apart), hard to reach and / or unable to meet the needs of
all clients because of a limited number of skilled staff or the limited availability of essential health
commodities. Consequently, KMET has now put in place an additional strategy to conduct community
based outreaches – to deliver integrated reproductive health services by a mobile team of trained
providers with the support of Quality Assurance Teams. This is invaluably critical service delivery
option for KMET and service providers to reach underserved communities. Within the reporting
period, the strategy was tried at two sites in Migori at which point 139 clients were attended to
(72contraceptive implant insertions, 25 Intrauterine Device insertions and Injectables administered).
Figure 3: CHWs display their FP counselling
bags after the review meeting
21
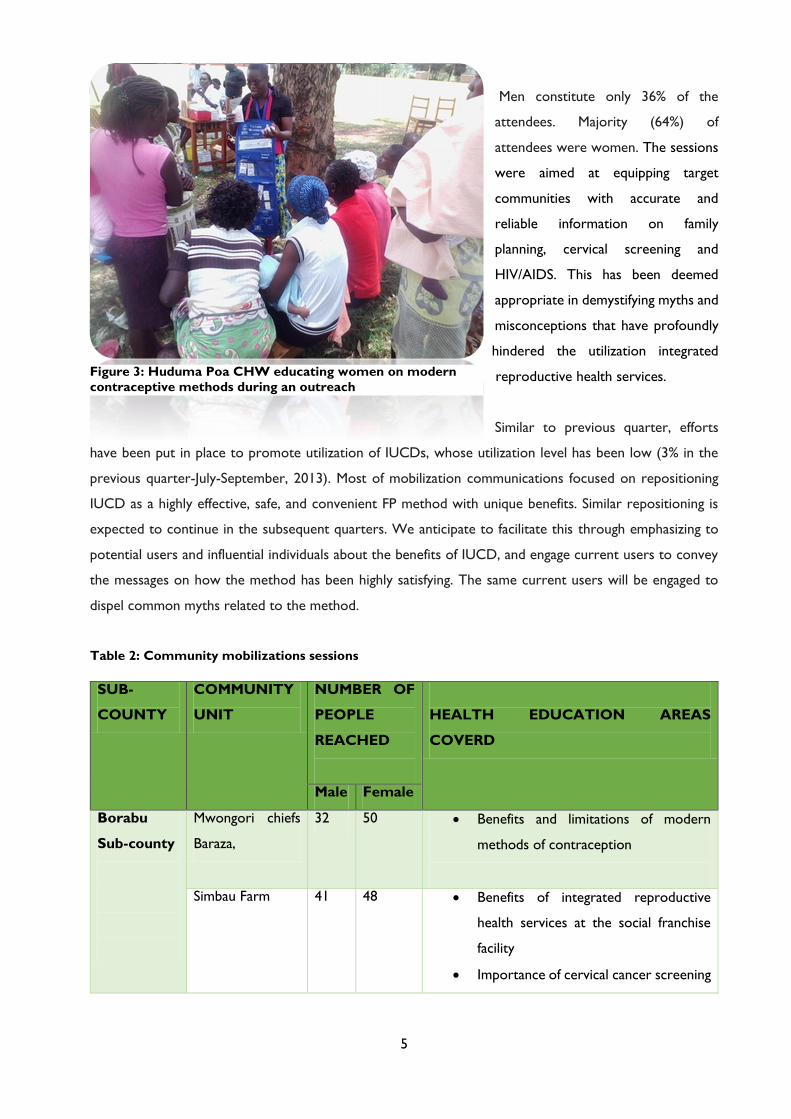
Table 4: FP service provision
Social Franchise FP service provision (Jan-March 2014)
# Social franchise facilities = 51
# outreaches=2
CONTRACEPTIVE METHOD
Month
IUCD
Implants
EC Pills
Injections
Condoms
POPs
COCs
# Insertions
# Removals
# Insertions # Removals # Clients # Clients # Clients # Clients # Clients
Jan- 2014 48 8 197 23 8 726 85 11 72
Feb -2014 57 4 263 30 4 664 58 7 66
Mar-2014 39 5 268 41 1 841 119 28 108
2 outreaches 25 19 72 3 0 20 0 0 0
Total
169
36 800 97
13
2,251
262
46 246
3.2 HIV testing and counselling (HTC) and couple counselling services
In the previous two quarters, KMET has initiated integration of HIV testing and counselling services to
other services offered at facilities in the social franchise as an entry point to prevention, diagnosis and
management of HIV and AIDS.
Throughout the reporting period, up to 5276 clients (4,948 individuals and 328 couples) were
counseled and tested on HIV through the social franchise. A total of 423 individual clients and 20 couples
(both) tested HIV positive whereas 20 couples tested discordant.
Table 5: HIV testing and counseling (HTC) services
HIV testing and counselling (HTC) services (Jan-March 2014)
# Social franchise facilities = 51
Month HTC - Individuals
HTC – Couples
Counsele
d
Tested HIV
+ve
Referral
s
Counsel
ed
Tested Both HIV
+ve
Discorda
nt
Jan 2014 1533 1532 142 108 120 118 8 7
Feb 2014 1653 1651 160 90 101 100 5 6
March
2014 1769 1765 121 41 111 110 7 7
Total
4,955
4,948
423
239
332
328 20 20

21
Considerably, 482 pregnant women accessing antenatal services were counseled and tested for HIV as the
start point for PMTCT interventions, out of whom 37 turned positive. Women who turned postive were
referred to PMTCT service providers to access comprehensive PMTCT intervention services
Table 6: PMTCT service provision
PMTCT Infants
Counseled Tested HIV +ve Total Referrals Tested HIV +ve
Jan 2014 209 170 13 1 4 0
Feb 2014 229 155 11 1 2 0
Mar 2014 214 157 13 3 15 1
Total 652 482 37 5 21 1
3.3 Cervical cancer screening services
Efforts have been put in place to facilitate integration of family planning, HIV testing and counselling, and
cervical cancer screening to all women seeking reproductive health services across franchise facilities.
Within the reporting period, 632 women of reproductive age got screened for cervical cancer, out of
whom 30 turned VIA/VILI positive whereas 21 exhibited positive findings for suspicious for cervical cancer.
A total of 50 clients were referred through the social franchise for treatment at various central sites.
Among those referred included clients with VIA/VILI positives results and suspicious for cervical cancer
cases.
Table 7: Cervical Cancer screening services
Month Cervical Cancer Screening Jan-March 2014
# Social franchise facilities =51
# Clients Screened # Positive # Suspicious # Referrals
Jan 2014 223 8 8 16
Feb 2014 246 15 8 23
Mar 2014 163 7 5 11
Total 632 30 21 50
3.4 Performance Management Plan
Table 6 below presents basic data on project progress towards the achievement of targets set for year 3.

22
Table 8: Performance Management Plan
AO
P
Acti
vit
y
Refe
ren
ce Output
So
urc
e
Indicator
Year 3
October 2013- September 2014)
Oct
-
Dec
Jan -
Mar Apr - Jun Jul- Sep
Ach
ievem
en
t
Yr
3
(12 m
on
ths)
Yr
3 T
arg
et
Ach
ievem
en
t
Yr
3 %
Achievement
Yr 1 Yr 2 Yr 3 Yr
4
FP services
Provided
KMET
HCM
Reports
Percent of USG supported service delivery
that provide FP counseling/or services 48 51 0 0 51 60 85% N/A 90%
85%
Capacity
building of
social
franchise
members
KMET
HCM
Reports
Number of health care workers who
successfully complete an in-service training
program through a social franchise
24 49 0 0 73 119 61% N/A 76%
61%
Health
workers
trained
KMET
HCM
Reports
Number of Health Care workers trained in
child health 0 26 0 0 26 60 43.3% N/A N/A
43,3%
Services
provided in
affiliated
franchise
facilities
KMET
HCM
Reports
Number of individuals
receiving services
(disaggregated by sex and
health area) through
social franchise
FP 3271 3920 0 7191 21960 32.74% N/A N/A 32.74%
PMTCT 1 1 0 0 2 240 0.83% N/A N/A 0.83%
Preg. women
C&T 576 482 0 0 1058 4896 21.6% N/A N/A
21.6.8%
HTC 4729 4948 0 0 9677 20304 47.7% N/A N/A 47.7%
Diarrhoea 0 0 0 4020 0% N/A N/A 0%
Malaria 0 0 0 0 2820 N/A N/A N/A 0%
Pneumonia 0 0 0 0 1680 N/A N/A N/A 0%
HTC
services
provided
KMET
HCM
Reports
Number of individuals who received HTC
services for HIV and received their test
results (PEPFAR P11.1.D) through a social
franchise
4729 4948 0 0
9677
20304
47.7%
N/A
N/A
47.7%

23
AO
P
Acti
vit
y
Refe
ren
ce Output
So
urc
e
Indicator
Year 3
October 2013- September 2014)
Oct
-
Dec
Jan -
Mar Apr - Jun Jul- Sep
Ach
ievem
en
t
Yr
3
(12 m
on
ths)
Yr
3 T
arg
et
Ach
ievem
en
t
Yr
3 %
Achievement
Yr 1 Yr 2 Yr 3 Yr
4
PMTCT
services
provided
KMET
HCM
Reports
Number of pregnant women with known
HIV status (PEPFAR P1.1.D) through a
social franchise
576 482 0 0 1058 4896 21.6% N/A N/A
21.6%
PMTCT
services
provided
KMET
HCM
Reports
Number of HIV-positive pregnant women
who received anti-retrovirals to reduce
risk of mother-to-child-transmission
through a social franchise
1 1 0 0 2 180 1.11% N/A N/A
1.11%
ART
services
provided
KMET
HCM
Reports
Number of HIV-positive adults and
children receiving a minimum of one
clinical service (PEPFAR C 2.1D) through a
social franchise
20 32 0 0 32 640 5% N/A N/A
5%
ART
services
provided
KMET
HCM
Reports
Number of adults and children with
advanced HIV infection newly enrolled on
ART (PEPFAR T 1.1 D) through a social
franchise
6 8 0 0 14 400 3.5% N/A N/A
3.5%
ART
services
provided
KMET
HCM
Reports
Number of adults and children with
advanced HIV infection receiving ART
(PEPFAR T 1.2 D) through a social
franchise
6 8 0 0 14 240 5.8% N/A N/A
5.8%
ORT
services
provided
KMET
HCM
Reports
Percentage of children under 5 years with
diarrhea treated with ORT 0 0 0 0 0 80% N/A N/A N/A
0%

25
4.0 PERFORMANCE MONITORING Program quarterly review meetings with both community health worker and providers were
conducted. These meeting were well attended with participant who were willing to learn from their
colleagues, understand the dynamic of service delivery and demand creation in diverse communities.
The teams generally agreed that:
a) Overly, family planning services was still low in most facilities and communities
b) New and well thought approaches needed to be designed to create more demand
c) There was need to dispel growing myths and misconception about family planning
d) There was need to fully address commodities stock out in the MOH.
e) Health facilities proprietors needed to see RH service as a way of improving their revenue
and not to discriminate any aspect of it
f) Continuous updates need to be conducted to both community health workers and service
providers
The teams discussed service delivery and demand creation success, challenges and way forward using
a prepared format with focus areas like: Facility Preparedness, service Delivery, Infection Prevention,
documentation & Reporting and staffing.
Success witnessed over the project period:
a) Creation of awareness through mobilization in Baraza, house to house and medical camps
b) Increase in referral through facility volunteer
c) Most of the facilities offer IUCD at cost effective price.
d) Continuous supervisions by the project staff to offer mentorship to both service providers
and community health workers
e) Availability of both FP and HTC commodities in most health facilities
f) Creation of strong linkages and partnership with MOH and other like- minded organization
g) Growing acceptance and uptake of family planning services including LTMs from STMs
h) Drive towards low cost service provision in most health facilities has increased uptake
i) Increased and growing male involvement in family planning issues have increased demand
j) Growing number of satisfied clients in the community who act as willing and good
ambassadors for family planning services
k) There is increase awareness of the need for facility planning in most communities
l) Increase number of trained service providers and CHWs who offer FP, HTC, cancer screening
and IMCI services
m) Focus on service integration where clients are able to get more than one service offered by
the same provider or within the same facility.

26
Providers and CHWs suggested the following solutions to issues raised:
a) Possibility of exchange program where CHWs could work in different places.
b) Program officers to accompany CHWs in various communities, barazas and in villages.
c) Continuous awareness creation for the community to know the importance/benefits of family
planning.
d) The need for health facilities to improve in quality service provision
e) More involvement of males on issues of reproductive health and family planning.
f) CHWs to be well equipped and informed on issues of RH and FP
g) Continuous creation of linkages with the MoH and other like-minded partners
h) Branding of all health facilities that have met the minimum standards for branding as a way of
positioning the new facilities
i) Enhance integration of services to reached all clients who visit the health facility for any service
j) Conduct outreaches in every facility at least once a month
k) Continuous motivation of CHWs as they do their work
l) Improving documentation through registers, books and forms provided by both KMET and
MOH for evidence of work done
m) Reporting to be done monthly by every CHWs and Health Provider.
Different or new demand creation approaches were also discussed which include: utilization of
satisfied clients, moving door to door, full integration of services to reach women and men who visit
other department within the hospitals, conducting outreaches, collaboration between service
providers and the demand creation team. Community health workers resolved to find better
approaches of creating demand for family planning, HIV Testing and counselling, cervical cancer
screening and other services. This is expected to be evident from next quarter moving forward.

27
5.0 PROGRESS ON LINKS WITH GOK AND OTHER AGENCIES
5.1 Stakeholders’ meetings
The HCM program participated in stakeholders’ meetings in 5 sub-counties (Migori, Homabay,
Rarieda, Kisumu and Siaya). The meetings
brought together partners implementing
different aspects of reproductive health
among other services in respective
counties to discuss health indicators and
individual partner contributions to the sub-
counties. It was also a perfect opportunity
for partners to lobby for MoH support
geared towards improving service
provision at private facilities. KMET had
the chance to showcase the magnitude of
what they have managed to deliver in family planning; cervical cancer screening and HTC in the facilities
supported by the HCM program. The MoH in Migori and Siaya offered to support KMET with
cryotherapy services for VIA/VILI positive cases requiring management by use of cryotherapy.
Evidently, there were expressed commitments from the MoH to continue supporting Huduma Poa
facilities to access FP commodities from MoH stores and KEMSA
6.0 YEAR 3 QUARTER 2 WORK PLAN STATUS
Table 9: Actual work plan status (Jan-March, 2014)
Key Planned Activities Achievements
Facilitate capacity building of 22 new
HP facilities on CTU
23 providers were trained on contraceptive method mix
(Permanent, Long Acting and Reversible Contraceptives;
and short term Methods). The training focused in ensuring
providers correctly provide balanced contraceptive
information to their clients to enable them choose methods
that best suits them. Making a wide range of methods
available improves quality of care.
Figure 4: KMET presenting their performance at
the stakeholders' meeting in Rarieda

28
Key Planned Activities Achievements
Facilitate capacity building of 30
Huduma poa Health Network on
IMCI
KMET collaborated with the MoH-Kisumu to train 26
providers on Integrated Management of Childhood illnesses
(IMCI). The training focused on equipping providers with
desirable knowledge and skills to accurately assess, classify,
identify treatment and treat ill children using the IMCI
protocol. In the subsequent quarter, there is going to be
joint KMET-MoH follow-up visits to all providers trained to
ensure acquired knowledge and skills are implemented; and
that providers perfect their counselling skills in an effort to
accelerate quality roll out of the services.
Quality assessments of facilities in
30 Huduma Poa Health Network
• 11 Quality assessments were done in 11 Huduma Poa
facilities;
• 5 Joint supervisions (MOH-KMET) were done to to social
franchise facilities-Asembo bay, Ngiya, Ahero Medical, Jawabu
Medical, Alphond Medical
Conduct 18 Provider Behavior
Change Communication (PBCC) to
improve provision of integrated RH
services
• 13 facilities were taken through PBCC adoption stairway.
• Some of the providers were assisted to set up their FP
room, acquire commodities and reporting tools
• Most providers have commenced to hold joint discussions
with CHWs to plan for franchise performance and improve
demand and access to reproductive health services.
Conduct 3 performance review
meetings with franchise providers
and provide updates
2 performance review meetings were conducted by
franchise providers. The meetings were intended to review
previous quarter’s performances, identify gray areas and
suggest new methodologies in heightening quality service
provision across social franchise facilities.
Providers had the opportunity to review their joint effort
and progress in the provision of FP, cervical cancer and
HTC services. In addition, they shared experiences, success,
challenges and possible solutions to perceived and
expressed challenges
Facilitate 30 HP Health facilities to
access health commodities from
MOH & OR other stakeholders
18 facilities had commodity linkages strengthened. There
was inter-county borrowing of reporting tools in areas that
had shortages.
29
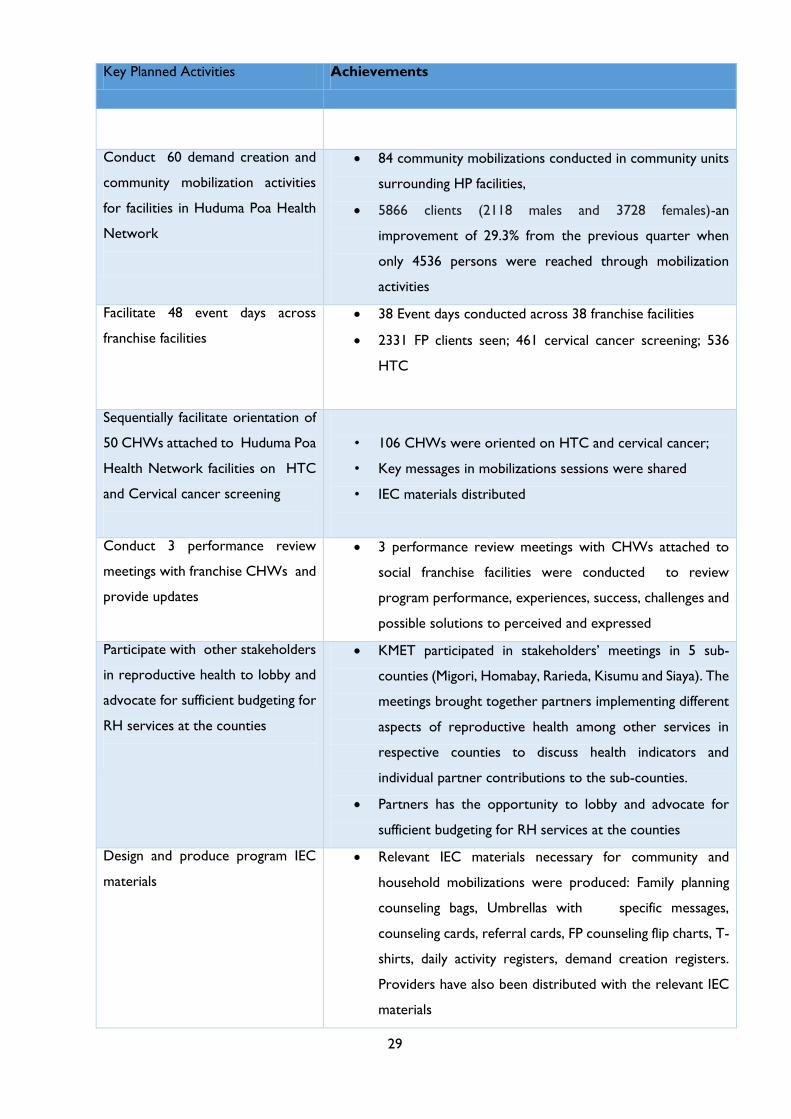
Key Planned Activities Achievements
Conduct 60 demand creation and
community mobilization activities
for facilities in Huduma Poa Health
Network
84 community mobilizations conducted in community units
surrounding HP facilities,
5866 clients (2118 males and 3728 females)-an
improvement of 29.3% from the previous quarter when
only 4536 persons were reached through mobilization
activities
Facilitate 48 event days across
franchise facilities
38 Event days conducted across 38 franchise facilities
2331 FP clients seen; 461 cervical cancer screening; 536
HTC
Sequentially facilitate orientation of
50 CHWs attached to Huduma Poa
Health Network facilities on HTC
and Cervical cancer screening
• 106 CHWs were oriented on HTC and cervical cancer;
• Key messages in mobilizations sessions were shared
• IEC materials distributed
Conduct 3 performance review
meetings with franchise CHWs and
provide updates
3 performance review meetings with CHWs attached to
social franchise facilities were conducted to review
program performance, experiences, success, challenges and
possible solutions to perceived and expressed
Participate with other stakeholders
in reproductive health to lobby and
advocate for sufficient budgeting for
RH services at the counties
KMET participated in stakeholders’ meetings in 5 sub-
counties (Migori, Homabay, Rarieda, Kisumu and Siaya). The
meetings brought together partners implementing different
aspects of reproductive health among other services in
respective counties to discuss health indicators and
individual partner contributions to the sub-counties.
Partners has the opportunity to lobby and advocate for
sufficient budgeting for RH services at the counties
Design and produce program IEC
materials
Relevant IEC materials necessary for community and
household mobilizations were produced: Family planning
counseling bags, Umbrellas with specific messages,
counseling cards, referral cards, FP counseling flip charts, T-
shirts, daily activity registers, demand creation registers.
Providers have also been distributed with the relevant IEC
materials

30
7.0 HUMAN INTEREST STORIES 7.1 WORKING WITH RURAL COMMUNITIES: BEATRICE’S EXPERIENCES
AND LESSONS
Beatrice Akinyi has served as a Demand Creation Officer at the APHIAplus Health Communications
and Marketing Program for 2 years now. She shares experiences, challenges and lessons she has
encountered in the field as she carries out demand creation and health promotion in the remote
areas of Kenya.
“As a Demand Creation Officer covering parts of Southern Nyanza and South Rift Valley, I
have come into contact with different communities whose diverse cultures influence their
mindset on reproductive health and family planning.
The most common communities I interact with include the Luo, Abagusii, Kalenjins and Maasai
thus giving me quite a vast understanding of the diverse cultures and their attitudes towards
family planning.
In Giribe, Migori County we noted that most of Huduma Poa mobilization meetings would
be attended majorly by men and the same was noted by health workers during house visits
where only the men would speak and even discuss family planning on behalf of their wives.
The men have the ultimate say and therefore, all decisions are made by men even those that
do concern the woman.
It was heart wrenching to
find that girls as young as 14
are married and by age 18,
most of them have about 2
to 3 children. On event days,
the women would show up
late in the afternoon because
their husbands are not for
the idea of family planning
and would therefore double
their duties at home before
they are finally released.
Every societal group is
fighting to have a piece of the Kenyan political power pie. It came to our attention that to
most communities numbers are a visible proof of political power and they improperly believe
that family planning stands in the way of having a key political figures elected from their region.
This we found to be a tough wall to crumble since it had been etched in their minds for so
long, that it was a practice that gradually got absorbed into their cultural ways. With such
kind of mentality, it takes extra effort and patience to change community attitudes towards
family planning.
Figure 5: Beatrice Akinyi, reaching out to tea pickers in
Nyamira during a community mobilization in March 2014

31
These communities
operate under set down
rules; for example, in the
Maasai community, one is
not allowed to question a
woman on the number of
children she has therefore
posing quite a challenge in
extraction of information
during counseling.
Women in these areas
tend to be quite
submissive and loyal to
the laws of the land making counseling more difficult.
Well, there’s a silver lining in every dark cloud, in some of the communities, we receive heroic
reception when they finally realize the benefits opening up to contraceptive information has
had in their families and the community at large.
Community Health
Workers have come in
handy in achieving such
results as they continually
do follow ups and
information sharing even
in the rigid communities;
helping women and men
to gradually embrace
family planning.
As a Program Officer, I
have learnt that it is
fruitful to reach out to community members through the Ministry of Health and local leaders
as one is able to work along with other development partners and have the goodwill of the
government.
Participating in activities such as community meetings and dialogue and stakeholders’ action
days also gives one an upper hand in winning the community’s trust.
Finally, organizing a series of health talks helps communities to gradually open up to new ideas
and share their views on each. This kind of healthy discussion builds trust between community
and the field officers as well as among themselves”
Author: Beatrice Akinyi
Program Officer-KMET
Figure 2: CHWs in Nyamira mobilizing women for integrated
reproductive health services
Figure 3: CHWs on an information sharing mission at community
unit

32
7.2 CHALLENGES OF ACCESS TO CONTRACEPTIVE SERVICES AND
INFORMED CHOICE
Meet Colleta Awuor Oluoch, a 38 year old mother of 8, living in Rural Bondo. Having raised
8 children she did not wish to give birth anymore so she sought for a family planning method
at a nearby government hospital, and there she was put on a 5 year implant.
Immediately after one week, Colleta learnt from friends that she could get access to other
forms of contraceptives including a permanent method. She went back to the same facility for
a successful tubal ligation but says that she could not get the previously inserted implant
removed.
“Without giving a clear reason, the attending doctor sent me back home on instruction that
I come on another day and when I came back later as instructed, I found a different provider
who, this time, informed me that the doctor who inserted the implant wasn’t around the
facility but he could remove the implant at a fee of 200 shillings,” recalls Colleta.
As is the common scenario in low income rural settings, Colleta did not have that amount of
money and was sent back home a second time, disappointed. “I was psychologically disturbed”
she says “I didn’t understand why they could not just remove the implant and whether it
would have any negative effect on me. I continued visiting that hospital, as it was the nearest
to my home, over and over in vain.”
Luck set in two years later. On 15/11/2013, she met a community health worker attached to
one of KMET’s Huduma Poa Health network facilities. The community health worker (CHW)
referred her to Aro Medical Clinic, a Huduma Poa medical clinic in Bondo.
Here, she was counseled, attended to and
her choice of method respected.
Expressing her relief afterwards, Colleta
couldn’t stop thanking the healthcare
provider: “Asante sana Daktari, Asante
(thank you Doctor)”. She and her family
now get treated at Aro Medical Clinic.
Even though, family planning programs in
Kenya have long endorsed the principle of
informed choice as a way of ensuring that
clients select a method that best meets
their needs providers seldom tailor their
discussion of contraceptive methods to the client's reproductive intentions, prior knowledge
of family planning, contraceptive preferences, personal circumstances or health risks
(International Family Planning Perspectives, 1998).
Author: Pamela Nyagol
Quality Assurance Officer-KMET
Figure 4: Colleta Awuor on the right after the
implant removal procedure.

33
7.3 LACK OF FAMILY PLANNING KNOWLEDGE MADE MY LIFE
MISERABLE, MOTHER SAYS
38 year old Jerusa Peters believes she is one of the biggest benefactors of Huduma Poa Heath
Network services in Nyamira County. The mother of four who turned into a grandmother
two years ago, confesses that family planning information has changed her life.
Jerusa has been married for 21 years and is a mother of four children, three boys and a girl.
Like many other women, she says she was ignorant on how to space child bearing a fact that
she points out to have made her formative days miserable.
Jerusa and her spouse Joram Nyalika, 50 years old, got married at an early age while Jerusa
was still in her teens. The two lived in Meru for a shortwhile before they decided to come
back to Joram’s ancestral home in Bobangi Village in Nyamira since they did not have any
meaningful source of income in Meru.
During this period the two were expecting their first born and life in the village was challenging
as they had neither a house nor a steady source of income and had to put up in relative’s
houses.
Jerusa says the situation got even worse when she gave birth to twin baby boys, now 24. “I
was overwhelmed, I realized I had two young children, I could barely afford food and was yet
to move out to start building my home,” she sombrely recalls.
Jerusa and her
husband decided to
erect and move out
in a makeshift
structure in the
husband’s piece of
land as they
purposed to build a
home later. The
husband had to take
odd jobs in the
village to make ends
meet.
Just a year later the couple learnt that they were expecting another child which they confess
gave them mixed reactions: one they could barely sustain their basic needs and two they were
happy to have a baby girl join the family.
Juggling between being a mother, casual labourer and small scale farmer Jerusa’s health
deteriorated so much and says she even thought she was HIV positive and just when she was
recovering, the inevitable happened, she got another baby, a boy.
One concerned relative advised her to visit any hospital for a family planning method and six
months after delivery she was put on injectable contraceptive; which she confesses to have
had adverse effects on her weight and bleeding.
Figure 5: Jerusa leads a team of CHWs and KMET field officer to her
home after a community outreach in March 2014

34
“For a year I went for injections which were costing me 150 KES after every 3 months, I grew
bigger and gained weight but I didn’t have any other alternative,” she explains.
This was however to change
when she met a neighbor who
works as a Huduma Poa
Community Health Worker
in Nyamira. They had a chat
and invited the CHW to talk
to her husband too.
After couple counselling the
two settled for a long term
method and were referred
for IUCD insertion and for
cervical cancer screening at
no fee.
Speaking to KMET field officers last month, Jerusa was delighted saying that she since lives
with peace of mind knowing she has control of when to give birth and can focus on building
a better life for herself and family.
Her parting shot went to her daughter 23 who is a mother to a two year old baby boy: “if
you want to live a better life than your father and I follow these Huduma Poa people and get
a family planning method.”
Author: Beatrice Akinyi
Program Officer-KMET
Figure 6: From left, Mayaka, the CHW who introduced Jerusa
to Huduma Poa Services. Right; Jerusa with her grandson at
her home in Bobangi Village