Embed Size (px)
Citation preview

PEER-REVIEW REPORTS
Use of External Lumbar Cerebrospinal Fluid Drainage and Lumboperitoneal Shunts with
Strata NSC Valves in Idiopathic Normal Pressure Hydrocephalus: A Single-CenterExperienceMadoka Nakajima, Masakazu Miyajima, Ikuko Ogino, Hidenori Sugano, Chihiro Akiba, Naoko Domon,Kostadin L. Karagiozov, Hajime Arai
-OBJECTIVE: In Japan, idiopathic normal pressure hydrocephalus (iNPH)currently is treated mainly with lumboperitoneal (LP) shunts. Our aim was toevaluate whether LP shunting via the use of Medtronic Strata NSC programmablevalveswas as effective as ventriculoperitoneal shunting in the treatment of patientswith iNPH from the perspectives of safety and symptomatic improvement rate.
-METHODS: The clinical records of 51 iNPH patients (mean age, 75 years;males, 29), who underwent placement of Medtronic Strata NSC LP shunt systemswere reviewed retrospectively as a cohort. LP shunting was evaluated with themodified Rankin Scale, the Japan Normal-Pressure Hydrocephalus GradingScale, the Mini-Mental State Examination, the Frontal Assessment Battery, andthe Trail-Making Test A as outcome measures.
-RESULTS: Modified Rankin Scale scores improved from 3.2 to 2.2 (P < 0.01),indicating a 64% response rate 12 months after treatment. Total Japan Normal-Pressure Hydrocephalus Grading Scale scores decreased from 6.5 to 4.0 (P <0.01), indicating a response rate of 81%. Mini-Mental State Examination scoresimproved from 22.2 to 25.4 (P < 0.01), Frontal Assessment Battery scores improvedfrom 11.7 to 13.4 (P < 0.05), and Trail-Making Test A scores improved from 122.3 to112.7 (P [ 0.60). During the 12-month follow-up period, complications requiringsurgery were observed in 6 cases (11.8%).
-CONCLUSION: LP shunts showed effectiveness rates that were similar tothose of ventriculoperitoneal shunts. Despite the relatively high complicationrate, LP shunts can be recommended for the treatment of patients with iNPHbecause of their minimal invasiveness and lack of lethal complications.
Key words- Cerebrospinal fluid- Dementia- Idiopathic normal pressure hydrocephalus
Abbreviations and AcronymsCSF: Cerebrospinal fluidDESH: Disproportionately enlarged subarachnoid-space hydrocephalusELD: External lumbar drainageFAB: Frontal Assessment BatteryiNPH: Idiopathic normal-pressure hydrocephalusJNPHGS: Japan Normal-Pressure HydrocephalusGrading ScaleLP: LumboperitonealMMSE: Mini-Mental State ExaminationMRI: Magnetic resonance imagingmRS: modified Rankin ScaleSINPHONI: Study of iNPH on NeurologicalImprovementTUG: 3-minute up-and-go testVP: Ventriculoperitoneal
Department of Neurosurgery, Juntendo University School ofMedicine, Tokyo, Japan
To whom correspondence should be addressed:Madoka Nakajima, M.D., Ph.D.[E-mail: [email protected]]
Citation: World Neurosurg. (2015) 83, 3:387-393.http://dx.doi.org/10.1016/j.wneu.2014.08.004
Supplementary digital content available online.
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
ª 2015 The Authors. Published by Elsevier Inc. This is anopen access article under the CC BY-NC-SA license (http://
INTRODUCTION
Idiopathic normal-pressure hydrocephalus(iNPH) (1), a condition of uncertain etiologythat characteristically afflicts elderlypatients, is treated by cerebrospinal fluid(CSF) shunting. iNPH is characterizedby the classical triad of symptoms: gaitdisturbance, dementia, and urinary incon-tinence. Recent reports of prevalence ratesof 0.51% and 1.4% in community-dwellingelderly people have suggested that iNPHis more common than previously thought(9, 18). The accurate diagnosis and
creativecommons.org/licenses/by-nc-sa/3.0/).
WORLD NEUROSURGERY 83 [3]: 387-393
treatment of this disease are expected toreduce the burden on patients’ families andsociety as a whole (3).Because of the current emphasis on
minimally invasive treatments, in JapaniNPH is treated mainly with lumboper-itoneal (LP) shunts (2) (Table 1); however,in Western countries, ventriculoperitoneal(VP) shunts are used to treat iNPH in mostcases partially because there is currently noestablished evidence for the use of LPshunts as a treatment for iNPH (3).Regarding the shunt device, many shuntsystems are designed for VP shunting;therefore, surgeons adapt systems for LPshunting according to their actual needs.In this situation, we have chosen the LPshunt kit 44421 (Medtronic, Inc., Goleta,
, MARCH 2015 ww
California, USA), which includes a small-lumen peritoneal catheter and a Strata NSCLP programmable valve, the only LP shuntprogrammable valve approved by the Foodand Drug Administration in the UnitedStates. Because there are no reports on theuse of this device in patients with iNPH, wewould like to provide the present reportas an important base for establishing LPshunts as a treatment for this condition.The purpose of this study was to examine
the improvement rates of symptoms in pa-tients who were suspected of having iNPHor so-called “possible iNPH” (15) based ontheir neurologic manifestations and theresults of tests and imaging 12months aftertreatment with Strata NSC LP programma-ble shunts. We compared the outcome of
w.WORLDNEUROSURGERY.org 387

Table 1. Treatment of IdiopathicNormal-Pressure Hydrocephalus inJapan According to the QuestionnaireSurveys
2007 2011
Number of facilities 251 289
iNPH patients 1211 1608
VP shunts 855 761
LP shunts 324 846
VA shunts 13 15
Others 5 14
Arai et al., 2009 (2).Neurosurgery centers: 1108; Recovery rate: 39% (289
centers). The number of cases that were treatedincreased by approximately 400 from those reportedin the survey performed 4 years earlier; the totalnumber of cases of treated iNPH was 1608. Notably,more cases were treated with LP shunts than withVP shunts. Currently, iNPH is mainly treated with LPshunts in Japan. The category of interest is theboldface figures.
iNPH, idiopathic normal pressure hydrocephalus; VP,ventriculoperitoneal; LP, lumboperitoneal; VA,ventriculoatrial.
Figure 1. Comparison of images acquired before and after lumboperitoneal (LP) shunting; theshunting pressure was reduced stepwise over the course of approximately 3 months to thepostoperative benchmark, at which diagnostic imaging showed cancellation of the compression inhigh convexity. Top: comparison of high convexity (computed tomography) before and after the LPshunting; the sulcus in high convexity is unclear before the operation, whereas it is depicted after theoperation. Bottom: callosal angle in magnetic resonance imaging (T1-weight image, coronal section);the angle between the white lines is acute (<90�) before the LP shunting, whereas it becomes anobtuse angle (>90�) after the operation.
PEER-REVIEW REPORTS
MADOKA NAKAJIMA ET AL. EXTERNAL LUMBAR CSF DRAINAGE AND LP SHUNTS WITH STRATA NSC VALVES IN INPH
patients treated with LP shunts with theoutcome of patients previously treated withVP shunts in other published series. Ouraim was to verify whether LP shunts whenused with our approach to treatment are aseffective as VP shunts in themanagement ofpatients with iNPH regarding safety andsymptomatic improvement rate.
METHODS
The subjects of this study (N ¼ 51) werereviewed retrospectively as a cohort of pa-tients who received LP shunts, afterconsulting our department. They weresuspected of having iNPH based on theirneurologic manifestations and findings onmagnetic resonance imaging (MRI) scans.Tap tests evaluation criteria was consistentwith Japanese guidelines for iNPH (15). Theresult was deemed positive if, within 1 weekafter removal of CSF, any of the followingwere found: 1) improvement of any item onthe “Japanese normal pressure hydroceph-alus grading scale revised” (JNPHGS) (16);2) �10% improvement on the 3-minuteup-and-go test (TUG); or 3) �3-pointimprovement on the Mini-Mental State
388 www.SCIENCEDIRECT.com
Examination (MMSE) (6). The JNPHGS is aclinician-rated scale that is used to rateseparately the severity of each of the triadsymptoms of iNPH gait (disturbance,cognition, and urination). The score oneach domain ranges from 0 to 4. Grade 0 isnormal, and grade 1 indicates subjectivesymptoms with an absence of objectivedisturbances. Grades 2, 3, and 4 indicatemild, moderate, and severe disturbances,respectively. The evaluation was performedby a single, third-party neuropsychologist.Forty-six patients were selected on
the basis of their positive TTs, and another5 patients with negative TTs wereselected after an additional external lumbardrainage (ELD), as described in the section“Drainage Test.” All 51 patients diagnosedwith iNPH were considered indicated for
WORLD NEUROSURGERY, http://
shunting and had LP shunts inserted. Weused the same type of shunt componentsfor LP shunting in all patients.The spinal catheter was a commonly
used one, with 0.7 mm internal diameterand 1.5 mm outer diameter, whereasthe small-lumen peritoneal catheter hadthe same 0.7-mm internal diameter asthe spinal catheter and a 2.5-mm outerdiameter. All were components of theMedtronic Strata NSC LP shunt system.The lengths of the small lumen peritonealcatheters could influence the overalloutflow resistance of the shunt system.The valves had the full range of perfor-mance levels: 0.5 (15e35 mmH2O), 1.0(35e55 mmH2O), 1.5 (90e110 mmH2O),2.0 (145e165 mmH2O), and 2.5 (200e220mmH2O). Therefore, we used 30-cm long
dx.doi.org/10.1016/j.wneu.2014.08.004

Figure 2. Changes in the scores of the Normal-Pressure Hydrocephalus Grading Scale (NPHGS; left)and modified Ranking Scale (mRS; right) 12 months after the shunting compared with those recordedbefore shunting. In the first year after surgery, approximately 80% of cases exhibited animprovement of at least 1 point in NPHGS score, which was similar to the findings of Study of iNPHon Neurological Improvement (SINPHONI). An evaluation performed using the mRS showedimprovement by 1 grade or more in 64% cases, which was a little lower than the 69% observed inthe European Study and SINPHONI.
Video available atWORLDNEUROSURGERY.org
PEER-REVIEW REPORTS
MADOKA NAKAJIMA ET AL. EXTERNAL LUMBAR CSF DRAINAGE AND LP SHUNTS WITH STRATA NSC VALVES IN INPH
peritoneal catheters in all patients, whichwere shortened from the original 120 cmlength provided by the manufacturer.
LP Shunting and ManagementThe clinical records of iNPH patients whounderwent placement of Medtronic StrataNSCLP shunt systemsbetween July 2010andApril 2012 were reviewed retrospectively.iNPH was clinically diagnosed in thesepatients according to the classical triad ofgait impairment, urinary incontinence, andimpairedmental function, and supported byventricular dilation, dilation of Sylvian fis-sures and narrowing of sulci and subarach-noid spaces over the high convexity withoutsignificant cerebral atrophy as seen oncomputed tomography or MRI. The evalua-tion criteria were consistent with Japaneseguidelines for iNPH (15).To date, 51 cases have been followed-up
for 12 months or longer. The average agewas 75.0 � 6.4 years (mean � standarddeviation), and the male-to-female ratiowas 29:22, with male patients beingslightly more prevalent. MRI showed thepresence of the so-called disproportion-ately enlarged subarachnoid-space hydro-cephalus (DESH) (7, 13) type in 80% of thepatients, with the remaining 20% havingother types. The deep white matter lesionsobserved were mild in approximately 60%of the patients, and moderate to severe inabout 40% of the cohort.The valves were adjusted before implan-
tation to an initial performance level of 2.5for all patients. The reason for the use of thegreatest settingwas thatwe aimed to reducethe rate of overdrainage symptoms (e.g.,low-pressure headache and subdural he-matoma), caused by CSF leakage from thepenetration of the dura into the epiduralspace immediately after surgery (12). Theproper pressure setting of the LP shunt wasdetermined around 1 month after theoperation by reference not only to theremaining neurological symptoms relatedto iNPH but also to neuroimaging (post-shunting computed tomography and MRI)criteria (depiction of sulci in the high con-vexity and change of the callosal angle toobtuse) (10) in diagnostic head images(Figure 1). At 1, 3, 6, 9, and 12 months aftersurgery, the patients attended an outpatientfollow-up consultation, during which apuncture of the shunt valve reservoir wasconducted using a 27-gauge needle andCSFwas aspirated using negative pressure, to
WORLD NEUROSURGERY 83 [3]: 387-393
check for the smooth outflow of CSF andthe presence or absence of shunt occlusion.The LP shunting was evaluated 12
months after surgery using the modifiedRankin Scale (mRS), JNPHGS, MMSE, theFrontal Assessment Battery (FAB) (5), theTrail-Making Test A (17), and the Wechs-ler Adult Intelligence Scale III symbolsearch (5) as outcome measures.
Drainage TestFive elderly people (2 men and 3 women;age range, 72e83 years; average age, 77.4years) were categorized as having possibleiNPH on the basis of their clinical symp-toms and MRI findings despite their TTsbeing negative. The patients were sub-jected to a 5-day drainage test, which was
performed as follows: while thepatient was under local anes-thesia, a 14-gauge Tuohy needlewas introduced into the lumbarsubarachnoid space at theL2eL3 or L3eL4 intervertebralspace. Next, a spinal catheterwas inserted through the Tuohy needle into the lumbar subarachnoid space, MARCH 2015 ww
and directed 20 cm cephalad. Before andafter ELD, all patients were evaluated usingthe JNPHGS, the MMSE, and the TUG. Theresponse to the ELD was predefined by the3 following major scales: JNPHGS, TUG,and MMSE. Improvements consisting of 1point or more on the iNPH grading scale(total), a greater than 10% improvement intime on the TUG, or more than 3 pointson the MMSE were regarded as a positiveresult.
Surgical Technique of LP Shunting (Video 1)Lumbar spinal anesthesia combined withlocal anesthesia was standard. A rightlateral position was used after confirmingthe anesthetized level in the supine posi-tion. The paramedian approach usually
w.WORLDNEU
was chosen for lumbarpunctures to avoid cathetertroubles because, in elderlypatients, the interlaminarspace might be narrow. Forparamedian punctures, theTuohy needle was insertedpointing at an angle of 45
degrees cranially, and the lumbar catheter
ROSURGERY.org 389
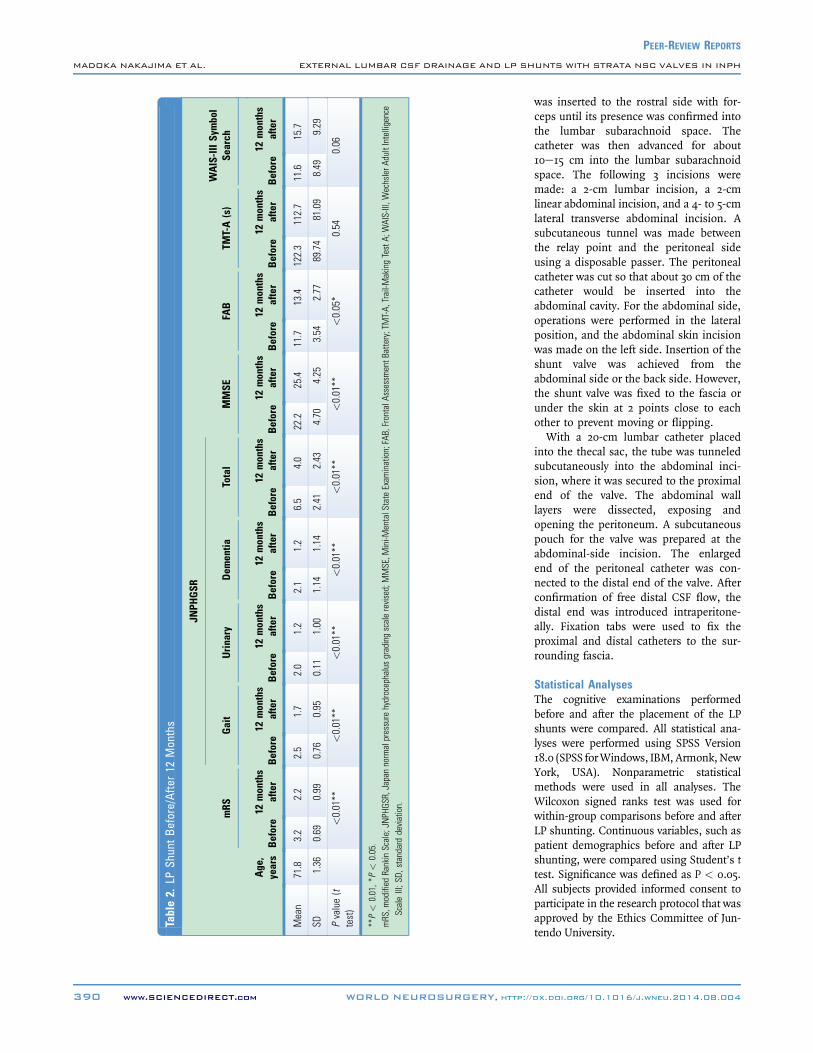
Table2.
LPSh
untBefore/Afte
r12
Mon
ths
Age
,years
mRS
JNPH
GSR
MMSE
FAB
TMT-A(s)
WAIS-IIISymbol
Search
Gait
Urinary
Dem
entia
Total
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Before12
mon
ths
after
Mean
71.8
3.2
2.2
2.5
1.7
2.0
1.2
2.1
1.2
6.5
4.0
22.2
25.4
11.7
13.4
122.3
112.7
11.6
15.7
SD1.36
0.69
0.99
0.76
0.95
0.11
1.00
1.14
1.14
2.41
2.43
4.70
4.25
3.54
2.77
89.74
81.09
8.49
9.29
Pvalue(t
test)
<0.01**
<0.01**
<0.01**
<0.01**
<0.01**
<0.01**
<0.05*
0.54
0.06
**P<
0.01,*
P<
0.05.
mRS,m
odified
RankinScale;JN
PHGS
R,Japannormalpressurehydrocephalusgradingscalerevised;MMSE,M
ini-M
entalStateExam
ination;FAB,FrontalA
ssessm
entB
attery;TMT-A,
Trail-M
akingTestA;
WAIS-III,W
echslerA
dultIntelligence
ScaleIII;S
D,standard
deviation.
390 www.SCIENCEDIRECT.com WORLD NEUROSURGERY, http://
PEER-REVIEW REPORTS
MADOKA NAKAJIMA ET AL. EXTERNAL LUMBAR CSF DRAINAGE AND LP SHUNTS WITH STRATA NSC VALVES IN INPH
was inserted to the rostral side with for-ceps until its presence was confirmed intothe lumbar subarachnoid space. Thecatheter was then advanced for about10e15 cm into the lumbar subarachnoidspace. The following 3 incisions weremade: a 2-cm lumbar incision, a 2-cmlinear abdominal incision, and a 4- to 5-cmlateral transverse abdominal incision. Asubcutaneous tunnel was made betweenthe relay point and the peritoneal sideusing a disposable passer. The peritonealcatheter was cut so that about 30 cm of thecatheter would be inserted into theabdominal cavity. For the abdominal side,operations were performed in the lateralposition, and the abdominal skin incisionwas made on the left side. Insertion of theshunt valve was achieved from theabdominal side or the back side. However,the shunt valve was fixed to the fascia orunder the skin at 2 points close to eachother to prevent moving or flipping.With a 20-cm lumbar catheter placed
into the thecal sac, the tube was tunneledsubcutaneously into the abdominal inci-sion, where it was secured to the proximalend of the valve. The abdominal walllayers were dissected, exposing andopening the peritoneum. A subcutaneouspouch for the valve was prepared at theabdominal-side incision. The enlargedend of the peritoneal catheter was con-nected to the distal end of the valve. Afterconfirmation of free distal CSF flow, thedistal end was introduced intraperitone-ally. Fixation tabs were used to fix theproximal and distal catheters to the sur-rounding fascia.
Statistical AnalysesThe cognitive examinations performedbefore and after the placement of the LPshunts were compared. All statistical ana-lyses were performed using SPSS Version18.0 (SPSS forWindows, IBM,Armonk,NewYork, USA). Nonparametric statisticalmethods were used in all analyses. TheWilcoxon signed ranks test was used forwithin-group comparisons before and afterLP shunting. Continuous variables, such aspatient demographics before and after LPshunting, were compared using Student’s ttest. Significance was defined as P < 0.05.All subjects provided informed consent toparticipate in the research protocol that wasapproved by the Ethics Committee of Jun-tendo University.
dx.doi.org/10.1016/j.wneu.2014.08.004
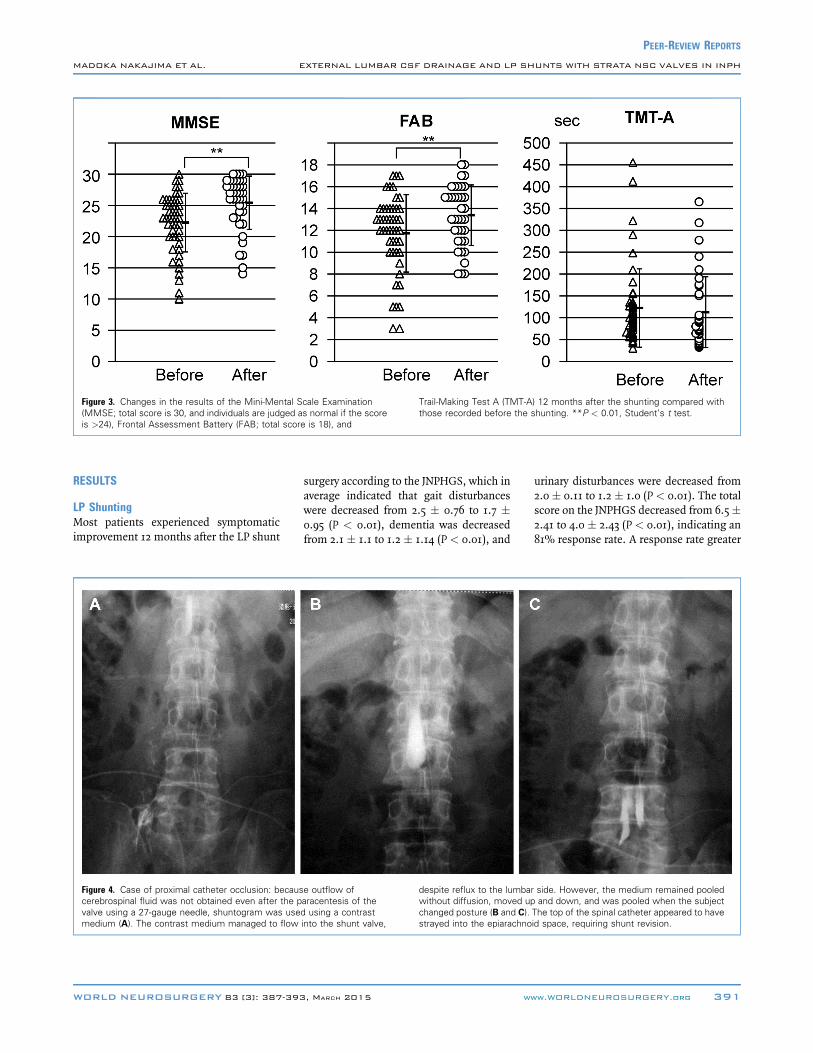
Figure 3. Changes in the results of the Mini-Mental Scale Examination(MMSE; total score is 30, and individuals are judged as normal if the scoreis >24), Frontal Assessment Battery (FAB; total score is 18), and
Trail-Making Test A (TMT-A) 12 months after the shunting compared withthose recorded before the shunting. **P < 0.01, Student’s t test.
PEER-REVIEW REPORTS
MADOKA NAKAJIMA ET AL. EXTERNAL LUMBAR CSF DRAINAGE AND LP SHUNTS WITH STRATA NSC VALVES IN INPH
RESULTS
LP ShuntingMost patients experienced symptomaticimprovement 12 months after the LP shunt
Figure 4. Case of proximal catheter occlusion: becauscerebrospinal fluid was not obtained even after the pvalve using a 27-gauge needle, shuntogram was usemedium (A). The contrast medium managed to flow
WORLD NEUROSURGERY 83 [3]: 387-393
surgery according to the JNPHGS, which inaverage indicated that gait disturbanceswere decreased from 2.5 � 0.76 to 1.7 �0.95 (P < 0.01), dementia was decreasedfrom 2.1 � 1.1 to 1.2 � 1.14 (P < 0.01), and
e outflow ofaracentesis of thed using a contrastinto the shunt valve,
despite reflux to the lumbawithout diffusion, moved upchanged posture (B and C).strayed into the epiarachno
, MARCH 2015 ww
urinary disturbances were decreased from2.0� 0.11 to 1.2 � 1.0 (P < 0.01). The totalscore on the JNPHGS decreased from 6.5�2.41 to 4.0 � 2.43 (P < 0.01), indicating an81% response rate. A response rate greater
r side. However, the medium remained pooledand down, and was pooled when the subject
The top of the spinal catheter appeared to haveid space, requiring shunt revision.
w.WORLDNEUROSURGERY.org 391

Table 3. Response and Complications: Comparison of the Results Between VP Shunting(European Study Performed in 2012 and SINPHONI) and LP Shunting (Ours), Operated1 Year After
VP Shunting (Klingeet al. (14), Europeanstudy n [ 115)
VP Shunting(Hashimoto et al. (7),SINPHONI n [ 100)
LP Shunting (thisstudy Nakajimaet al.; n [ 51)
Responserate
mRS 69% 69% 64%
NPHGS 84% 80% 81%
Complicationrate
Complicationsrequiring shuntsurgery (total)
15% 1% 11.8%
Complications notrequiring shuntsurgery (total)
13% 13% 11.8%
Hematoma andhygroma requiringevacuation
1% 1% 2.0%
Subduralhematomas
6% 6% 2.0%
Infection (fever þcell count)
1% N/A 2.0%
Valve failure 4% N/A N/A
Proximal catheterfailure
4% 1% 3.9%
Distal catheterfailure
4% N/A 2.0%
SINPHONI, The Study of INPH on Neurological Improvement; mRS, modified Rankin Scale; NPHGS, Normal-PressureHydrocephalus Grading Scale; N/A, not available.
PEER-REVIEW REPORTS
MADOKA NAKAJIMA ET AL. EXTERNAL LUMBAR CSF DRAINAGE AND LP SHUNTS WITH STRATA NSC VALVES IN INPH
than 90% was observed in DESH-type pa-tients. In addition, mRS scores exhibited astatistically significant improvement, from3.2 � 0.69 to 2.2 � 0.99 (P < 0.01), whichindicated a 64% response rate 12 monthsafter treatment (Figure 2).The testing of higher brain functions at 12
months after treatment revealed that MMSEscores improved from 22.2 � 4.70 (DESHtype, 21.7 � 4.73) preoperatively to 25.4 �4.25 (24.9� 4.62) postoperatively (P< 0.01),FAB scores improved from 11.7 � 3.54 (11.3� 3.51) to 13.4� 2.77 (13.5� 3.18) (P< 0.05),Trail-Making Test A scores improved from122.3� 89.74 (125.2� 81.3) to 112.7� 81.09(110.2 � 71.35) (P ¼ 0.61), and WechslerAdult Intelligence Scale III symbol searchesimproved from 11.64 � 8.49 to 15.7 � 9.29(P ¼ 0.06) (Table 2). The comparison ofpreoperative and postoperative cognitivefunctions revealed a statistically significantincrease in the MMSE and FAB scores(Figure 3).
392 www.SCIENCEDIRECT.com
In addition, during the 12-month follow-up period, complications requiring surgerywere observed in 6 cases (11.8%): shuntinfection was observed in 1 case (2.0%),subdural hematoma was observed in 1 case,spinal (proximal) catheter occlusions wereobserved in 2 cases (3.9%) (Figure 4), pro-cedure-related radiculopathy was observed 1case, and prolapse of the peritoneal (distal)catheter was observed in 1 case. Over-drainagewas observed in 7 cases (13.7%). Allof these complications were improved byadjustment of the valve performance level,with the exception of 1 case (2.0%), with asubdural hematoma requiring evacuation.
DISCUSSION
LP shunts are seldom used for iNPHtreatment in Europe and North America.Among the various conceivable reasons forthis low usage, the high complication ratethat has been reported for LP shunts is the
WORLD NEUROSURGERY, http://
most important. Toma et al. (19) per-formed LP shunts in 20 patients aged 40.3years on average using a Strata NSC pro-grammable valve and reported that 7 oftheir patients (35%) required shunt revi-sion. The majority of these reports wereon patients with idiopathic intracranialhypertension and slit-ventricle syndromewho were young and active in their dailylife. We believe that high CSF pressureand trunk motion could be the cause fordisplacement of the proximal/distal shuntcatheters. However, although there is alow number of reports on the use of LPshunts for the treatment of iNPH, Blochand McDermott performed LP shunts in 33patients with iNPH using the Integra H/Vvalve systems (Integra LifeSciences Cor-poration), resulting in 9 patients (27%)requiring re-operation during the follow-up period, which averaged 19 months (4).Although the follow-up period of ourcases was short, the rate of complicationsrequiring shunt revision was 6 of 51 cases(11.8%). We cannot simply compare ourresults with those listed previouslybecause elderly iNPH patients with LPshunts are characterized by poor activityand lower CSF pressure, which are prob-ably related to fewer complications.In contrast, studies of iNPH treatment
with VP shunts include a multicenter studythat used a programmable valve (11) in allpatients diagnosed with possible iNPHbased on their neurologic manifestationsand imaging studies. An evaluation using aJNPH grading scale and mRS (for theassessment of daily activities) performed 1year after treatment revealed that approxi-mately 80% and 69% of improvement wasseen, respectively (Table 3). In addition,according to Klinge et al. (14), who pub-lished an European multicenter study in2012, symptomatic improvement in iNPHwas observed, with 69% and 84% responserates on the mRS and iNPH scales,respectively; whereas 17 of 115 subjects(15%) required shunt revision during a1-year period (Table 3) (8). The rates ofintracranial bleeding requiring surgery andinfection were both 1%. Within the firstyear after surgery, approximately 80% ofcases showed an improvement of 1 point orgreater on the JNPHGS, which was similarto the findings of the Study of iNPH onNeurological Improvement (SINPHONI).An evaluation performed using the mRSshowed improvement of 1 grade or more in
dx.doi.org/10.1016/j.wneu.2014.08.004

PEER-REVIEW REPORTS
MADOKA NAKAJIMA ET AL. EXTERNAL LUMBAR CSF DRAINAGE AND LP SHUNTS WITH STRATA NSC VALVES IN INPH
64% of the cases, which was a little lowerthan the 69% observed in the EuropeanStudy and in SINPHONI. We consideredthat VP shunts tend to have lower rates ofrevision caused by occlusion, displace-ment, and other complications related tothe shunt catheter compared with those ofLP shunts.However, although VP shunts are not
associated with such greater rates of de-vice-related complications, they tend tobe a more invasive surgery (requiringgeneral anesthesia and brain interven-tion) and yield complications with agreater impact on the general conditionof the patient. Patients with iNPH areelderly, with relatively higher rates ofamyloid angiopathy and AD comorbidity.An increased risk of intracranial hemor-rhage has been associated with VP shuntplacement. MRI T2* can be used toassess coexisting amyloid angiopathy (20)and eventually avoid shunt treatmentbased on the anticipated risks. Incontrast, there are also specific compli-cations of the LP shunt, the aberrantspinal catheter (Figure 4) and the proce-dure-related radiculopathy, which usuallyimproves with removing the catheter un-der local anesthesia. As an elderly popu-lation, patients with iNPH tend to have arelatively high incidence of lumbar ste-nosis. The optimal evaluation to avoidcomplications requires a “whole-spine”MRI examination to confirm adequacy ofthe lumbar subarachnoid space and itscontinuity with the rest of the CSFspaces.
CONCLUSION
Although our data are based on a retro-spective survey at a single center, LPshunts showed effectiveness rates similarto those of VP shunts. Despite the highcomplication rate inherent to this proce-dure, LP shunting can be recommendedfor the treatment of patients with iNPHbecause of their minimal invasivenessand lack of the lethal complications seenwith VP shunts. A multi-institutional trialwould definitely be of need.
WORLD NEUROSURGERY 83 [3]: 387-393
REFERENCES
1. Adams RD, Fisher CM, Hakim S, Ojemann RG,Sweet WH: Symptomatic occult hydrocephaluswith “normal” cerebrospinal fluid pressure. Atreatable syndrome. N Engl J Med 273:117-126,1965.
2. Arai H, Hashimoto M, Miyajima M: Results of aquestionnaire survey on idiopathic normal pressurehydrocephalus—Toward establishment of pro-spective clinical observation study of idiopathicnormal pressure hydrocephalus. In: FY 2008Summary Report of the Shared Research “Studieson Epidemiology, Disease State and Treatment ofNormal Pressure Hydrocephalus,” Research Projectfor the Measures for Intractable Diseases supportedby Ministry of Health Labour and Welfare Grant-in-Aid for Scientific Research 2009:57.
3. Bergsneider M, Black PM, Klinge P, Marmarou A,Relkin N: Surgical management of idiopathicnormal-pressure hydrocephalus. Neurosurgery 57(3 Suppl):S29-S39; discussion ii-v, 2005.
4. Bloch O, McDermott MW: Lumboperitonealshunts for the treatment of normal pressure hy-drocephalus. J Clin Neurosci 19:1107-1111, 2012.
5. Dubois B, Slachevsky A, Litvan I, Pillon B: TheFAB: a Frontal Assessment Battery at bedside.Neurology 55:1621-1626, 2000.
6. Folstein MF, Folstein SE, McHugh PR: “Mini-mental state.” A practical method for grading thecognitive state of patients for the clinician.J Psychiatr Res 12:189-198, 1975.
7. Hashimoto M, Ishikawa M, Mori E, Kuwana N:Study of INPH on neurological improvement(SINPHONI). Diagnosis of idiopathic normalpressure hydrocephalus is supported by MRI-based scheme: a prospective cohort study. Cere-brospinal Fluid Res 7:18, 2010.
8. Hellstrom P, Klinge P, Tans J, Wikkelsø C: A newscale for assessment of severity and outcome iniNPH. Acta Neurol Scand 126:229-237, 2012.
9. Iseki C, Kawanami T, Nagasawa H, Wada M,Koyama S, Kikuchi K, Arawaka S, Kurita K,Daimon M, Mori E, Kato T: A symptomatic ven-triculomegaly with features of idiopathic normalpressure hydrocephalus on MRI (AVIM) in theelderly: a prospective study in a Japanese popu-lation. J Neurol Sci 277:54-57, 2009.
10. Ishii K, Kanda T, Harada A, Miyamoto N,Kawaguchi T, Shimada K, Ohkawa S, Uemura T,Yoshikawa T, Mori E: Clinical impact of the cal-losal angle in the diagnosis of idiopathic normalpressure hydrocephalus. Eur Radiol 18:2678-2683,2008.
11. Ishikawa M: Guideline Committee for IdiopathicNormal PressureHydrocephalus, Japanese Society ofNormal Pressure Hydrocephalus. Clinical guidelines
, MARCH 2015 ww
for idiopathic normal pressure hydrocephalus.Neurol Med Chir (Tokyo) 44:222-223, 2004.
12. Kaijima M, Fukuda H, Yamamoto K: Post-opera-tive complications peculiar to lumboperitonealshunt: possible consequences due to side leakageof CSF from around the inserted spinal tube intothe lumbar epidural space. No Shinkei Geka 39:497-504, 2011.
13. Kitagaki H, Mori E, Ishii K, Yamaji S, Hirono N,Imamura T: CSF spaces in idiopathic normalpressure hydrocephalus: morphology and volu-metry. AJNR Am J Neuroradiol 19:1277-1284, 1998.
14. Klinge P, Hellstrom P, Tans J, Wikkelsø C: Euro-pean iNPH Multicentre Study Group: One-yearoutcome in the European multicentre study oniNPH. Acta Neurol Scand 126:145-153, 2012.
15. Mori E, Ishikawa M, Kato T, Kazui H, Miyake H,Miyajima M, Nakajima M, Hashimoto M,Kuriyama N, Tokuda T, Ishii K, KaijimaM,Hirata Y,Saito M, Arai H: Guidelines for management ofidiopathic normal pressure hydrocephalus: secondedition. Neurol Med Chir (Tokyo) 52:775-809, 2012.
16. Mori K: Management of idiopathic normal-pressurehydrocephalus: amultiinstitutional study conductedin Japan. J Neurosurg 95:970-973, 2001.
17. Reitan RM: Relationships between measures ofbrain functions and general intelligence. J ClinPsychol 41:245-253, 1985.
18. Tanaka N, Yamaguchi S, Ishikawa H, Ishii H,MeguroK: Prevalence of possible idiopathic normal-pressure hydrocephalus in Japan: The Osaki-Tajiriproject. Neuroepidemiology 32:171-175, 2009.
19. Toma AK, Dherijha M, Kitchen ND, Watkins LD:Use of lumboperitoneal shunts with the StrataNSC valve: a single-center experience. J Neurosurg113:1304-1308, 2010.
20. Yates PA, Villemagne VL, Ellis KA, Desmond PM,Masters CL, Rowe CC: Cerebral microbleeds: areview of clinical, genetic, and neuroimaging as-sociations. Front Neurol 4:205, 2014.
Conflict of interest statement: Madoka Nakajima andMasakazu Miyajima have received honoraria for lecturingand consulting by Medtronic Japan. The remaining authorshave no conflicts to report.
Received 21 September 2013; accepted 1 August 2014;published online 7 August 2014
Citation: World Neurosurg. (2015) 83, 3:387-393.http://dx.doi.org/10.1016/j.wneu.2014.08.004
Journal homepage: www.WORLDNEUROSURGERY.org
Available online: www.sciencedirect.com
ª 2015 The Authors. Published by Elsevier Inc. This is anopen access article under the CC BY-NC-SA license (http://creativecommons.org/licenses/by-nc-sa/3.0/).
w.WORLDNEUROSURGERY.org 393