Embed Size (px)
Citation preview

Pergamon 0277-9536(94)00169-3
Soc. Sci, Med. Vol. 40, No. 8, pp. 1109 1116, 1995 Copyright ~ 1995 Elsevier Science Ltd
Printed in Great Britain. All rights reserved 0277-9536/95 $9.50+0.00
USEFULNESS OF A NON-EXPERIMENTAL STUDY DESIGN IN THE EVALUATION OF SERVICE DEVELOPMENTS FOR
INFANT FEEDING IN A GENERAL HOSPITAL
NIGEL BRUCE and ANJA GRIFF1OEN Department of Public Health, PO Box 147, University of Liverpool, Liverpool L69 3BX, England
Abstract--There are likely to be many situations in which it is not possible to use a randomized controlled trial (RCT) for the evaluation of local service developments, and the usefulness of non-experimental study designs need to be assessed. This is examined with reference to a study carried out to evaluate the appointment of a baby feeding adviser (BFA) and other policy changes for infant feeding at a district general hospital (DGH). Surveys of Maternity Unit staff attitudes and practices, and of mothers' experiences were carried out in 1988 (prior to the changes) and afterwards in 1990. Service changes were; appointment of a BFA, removal from the postnatal wards of dextrose, seminars on baby feeding for midwifery staff, and a reduction of night-only shifts.There was no change in the initial breast feeding rate of about 80%, but there was an increase in breast feeding at 6 weeks postnatally from 57% (95% CI; 51-64) to 64% (95% CI; 59-69); P=0.15. The percentage of women who stopped breast feeding by 6 weeks fell from 30% in 1988 to 22% in 1990; P = 0.l I. Mothers who did not see the BFA (1990 only) were significantly less likely to begin breast feeding (P = 0.03), independent of social class and age, but a similar association was not seen at 6 weeks. There were significant reductions in the percentage of midwifery staff viewing feeding policy as unimportant (P=0.02), and in the use of supplements for breast-fed babies (P<0.001). Women having Caesarian sections were more likely to give up breast feeding in 1988 and in 1990, and this was partly explained by continued use of supplements.It is concluded that the service initiatives have been associated with some favourable changes in attitudes and practices of staff, and in the outcome for mothers and babies as measured by breast feeding at 6 weeks and satisfaction with advice. The limitations and value of the study design are discussed in the light of the results. While cause and effect will inevitably remain difficult to establish in a non-experimental situation, there are some characteristics of the study which aid interpretation. Of particular importance is the observation that some key social and service factor associations persisted after the intervention, thereby highlighting issues requiring continued attention.
Key words--baby feeding, evaluation, service development, policy, staff practices, study design
INTRODUCTION
There is now considerable pressure to evaluate service and policy developments in heal th services [1]. However, even if the policy in quest ion has been proved to be of benefit in a sound scientific assessment elsewhere, for instance in a randomized trial, there is no guarantee tha t its appl icat ion in any given locality is going to lead to similar results. The major i ty of policy developments tha t are in t roduced into a hospi tal or o ther heal th service uni t will p robab ly never be subjected to randomized trials, and when implemented will be shaped by local interests and
circumstances. So far as local policy implementa t ion is concerned,
there are a n u m b e r of possible opt ions for e v a l u a t i o n - - a t least theoretically. In some circum- stances a randomized control led trial (RCT) can be done, a l though in this case it was not a feasible option. Alternat ively historical controls , or parallel control areas (e.g. one or more other local hospitals) can be employed, but these designs are subject to changed circumstances which can be very difficult to interpret . Wi th historical controls , the invest igator has little
control over the availabili ty and quality of da ta collection, while a control hospital can have many differences which may be unrecognized or difficult to characterize. A n o t h e r opt ion is to carry out a series of studies at intervals of one or more years, relying more on the evidence of a t rend to suppor t inference abou t
cause and effect. This paper describes the evaluat ion of service
development for infant feeding in the materni ty unit of a district general hospital using studies before and after the intervent ion, a l though the design underwent some modif icat ion to facilitate fur ther studies within the hospital. Issues concerning the study design, the context of policy change, and inference abou t cause and effect are examined fur ther in the discussion. The in tervent ion was based on guidelines for good practice in baby feeding [2, 3], the results of the first survey carried out in 1988 [4], and evidence from other studies
[5-81.
Background to baby feeding study
The background to this project and the results of the baseline study have already already been described [4]. The setting was the materni ty unit of a D G H serving
1109
1110 NIOEL BRtJCE and ANJA GRIFFIOEN
an inner London population of 110,000 and parts of the adjacent districts. In this report, the changes occurring over the 18 months following the appointment of a baby feeding adviser (BFA) and other policy developments in the maternity unit are described. The role of the BFA was to work directly with mothers in the antenatal and postnatal periods in hospital [9], and also with maternity unit staff to improve their understanding of baby feeding as well as their advisory skills. The BFA was available to, and visited, all mothers in hospital (Monday-Friday), irrespective of whether they wished to breast or bottle feed.
The input from the BFA to staffon the unit included talks to which almost all of the staffon postnatal wards and the special care baby unit (SCBU) attended during the period of the study, but less from the antenatal clinic and labour ward. All staff were sent a questionnaire (not part of the evaluation study) on baby feeeding advice, to which there was a 47% response; topics covered included practical manage- ment of breast feeding and associated problems, indications for giving fluids, advice on feeding after casesarian section, etc. The results were used as a basis for feedback sessions to unit staff, including the medical staff.
The other policy changes were as follows; the unit policy statement, which already actively supported breast feeding, was revised and re-issued. Dextrose was removed from the postnatal wards, although sterile water and formula were still available. There was no single 'house fourmula', as SMA, Cow and Gate and Farleys products were in use. Independently of the baby feeding initiatives (but at about the same time), a management decision was taken to reduce the number of night-only and night-mainly shifts in the maternity unit because it was felt that night shift staff tended to be more isolated from developments in the unit.
During national breastfeeding week there was a display in the hospital concourse, with input from maternity unit staffincluding the BFA, health visitors, National Childbirth Trust, La Leche League and a local twin club.
The objectives of the study were twofold: first, to study changes in feeding outcomes, maternal satisfaction and staff practices; and second, to analyse where possible the relationships between aspects of the intervention and the specific changes observed. It can be appreciated that the work of the BFA was so inter-related with maternity unit staff and the other policy changes that it would not have been possible to carry out a RCT within the hospital.
METHODS
Two studies were carried out, the first in 1988 prior to the appointment of the BFA and other policy changes, [4] and the second in 1990. Each study
consisted of two surveys; one of staff and one of mothers.
Surveys of staff
A self-administered questionnaire was sent to all non-medical maternity unit staff. Replies were received from 48 (80%) in 1988, and from 65 (87%) in 1990. Apart from a slightly lower response rate, the main reason for the lower numbers in 1988 was a shortage of staff. The questionnaires used were identical in both studies, except that the 1990 version included questions on the role of the BFA. The remaining questions covered time available for talking to mothers, attitudes to policy in the unit, advice on feeding methods and the use of supplements.
Surveys of mothers
The methodology of the two surveys of mothers differed slightly for the following reason. The 1988 survey consisted of an interview (for feeding method, social and demographic data) within the first few days after the birth, followed by a self-administered questionnaire mailed at 6 weeks (for feeding method and views on support). The sample of mothers consisted of all those that could be contacted and interviewed by one member of the research team (ZK) over a period of 2 months, excluding some weekends (n =250, about 80% of the total delivering during that period). This was very time consuming, and we wished to simplify the methodology in such a way that the surveys could be carried out in future more as routine monitoring rather than as research. Accordingly, the 1990 survey consisted only of the 6 week question- naire, and details of the immediate postnatal period had to be recalled by the mothers. The reliability of recall by mothers of feeding practices has been reported as high, even after many years [10].
In 1988, replies to the 6 week questionnaire were received from 202 (81%) of the mothers, with one written reminder. In 1990, a larger sample of mothers was drawn from the district child health computer (from which the hospital code could be identified), and 322 (80%) replied. During piloting of the 1990 study, it was found that if the 6 week questionnaire was sent out without any prior explanation to the mother, there was a response of only about 50%. The BFA and community midwives were therefore asked to briefly explain the study to all mothers during the first week to 10 days after delivery, and to seek their agreement to receiving the questionnaire. This relatively simple action boosted the response to 80%.
The differences in study design in 1988 and 1990 may have influenced the validity of some comparisons between the two surveys. Where relevant, these differences have been pointed out.
Statistical methods
Comparisons between frequencies have been made with Z2 tests, and all P-values quoted include the Yates

Usefulness of a non-experimental study design in service evaluation
Table 1. Staff views on what approach unit policy should adopt
1111
1988 1990
Policy n (%) n (%)
Encourage breast feeding 9 (19) 18 (28) Encourage bottle feeding 0 (0) 0 (0) Not encourage one or other method, but support mother 20 (42) 39 (60) Don't know 4 (8) 0 (0) No policy 15 (31 ) 7 ( 11 ) Missing 0 (0) I (2)
Total 48 (100) 65 (100)
~2 = 8.6 (df= 2), P= 0.013, excluding 'don't know' and 'missing' categories.
continuity correction. The associations between various factors and feeding method at 2 days and at 6 weeks have been examined using logistic regression in the G L M procedure of the Statistical Analysis System. For this purpose, mainly or wholly breast feeding is used as one outcome, and mainly or wholly bottle feeding as the other. Categorical variables with more than two values (e.g. level of support from the BFA) were entered into the model using dummy variables. The odds ratios in Tables 3, 5 and 6 have been derived from the exponent of the logistic regression coefficient (beta), as e ~ ' .
RESULTS
Staff views on policy
Between 1988 and 1990, there was a significant increase in the proport ion of staff agreeing that the unit should have a policy on baby feeding from 52 to 75% (P = 0.02). Staff were asked in both studies about the approach that unit policy should adopt (Table 1). There was an increase in 1990 in the proport ion favouring a policy which actively supported breast feeding, but over half still preferred a 'neutral ' approach, supporting the mother in her decision.
The reasons behind these responses (derived from comments canvassed in this part of the 1990 questionnaire) help us to understand staff attitudes to policy, and these are shown in Table 2. Staffwho were not keen on policy said that it would make women feel pressurized into breast feeding, possibly making them feel guilty. These views were also quite common
among staff who were not sure about unit policy, or were supportive of it. However, almost one third of this group thought that policy could be useful for agreeing guidelines, and would thus help to avoid conflicting advice to mothers.
For advice to the mother of a full-term normally delivered baby, there was an increase in the percentage of staff recommending breast feeding from 50 to 69% and a corresponding reduction in the percentage recommending breast feeding with supplements (P=0.01) . However, when asked about the advice to mothers undecided about which method to use, there was no change in the relatively high percentage who would wish to let the mother make up her own mind (54% in 1988, 59% in 1990; NS).
Role of the baby Jeeding adviser ( BFA )
It might be expected that the appointment of the BFA would influence the perceptions held by staff about who should be advising mothers. Some staff might feel that they no longer had any responsibility for advising, while others might feel resentment about their role being usurped.
Information on staffviews about the role of the BFA and other staff in feeding advice was collected only in 1990, and all unit staff thought that they had some advisory role. The majority thought that responsibility should be shared about equally between them and the BFA, and less than one fifth felt that advising was mainly the responsibility of the BFA. A similar proport ion (19%) suggested that the BFA had a relatively minor role, including a few (5%, mainly in
Table 2. Reasons given by 45 staff for views held about policy, according to whether or not staff believed that there should be a baby feeding policy in the maternity unit; 1990 study.
Reasons n
Should there be a policy'?
No Yes/not sure (%) n (%)
Mother should not be pressurized to follow policy, or made to feel guilty Policy is too rigid, need flexibility Mothers have made up their minds before coming into the hospital Policy is useful for agreeing guidelines, and to avoid conflicting advice Breast is best, but if mother wants to bottle feed, then she should
be supported Desirable to encourage breast feeding as it benefits mother and baby
Total
5 (71) 16 (42) 2 (29) I (3) - I ( 3 )
. . . . 11 (29)
7 (18) - - 6 ( 1 6 )
7 (100) 38 (100)
SSM 408 G
!112 NIGEL BRUCE a n d ANJA GRIFFIOEN
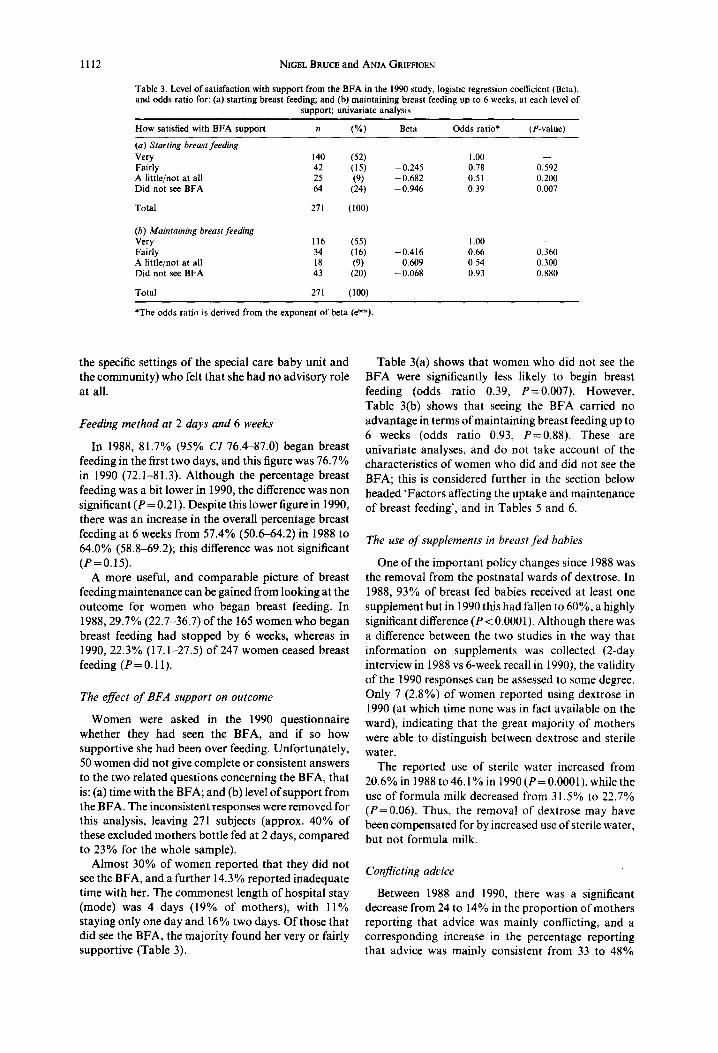
Table 3. Level of satisfaction with support from the BFA in the 1990 study, logistic regression coefficient (Beta), and odds ratio for: (a) starting breast feeding; and (b) maintaining breast feeding up to 6 weeks, at each level of
support; univariate analysis
How satisfied with BFA support n (%) Beta Odds ratio* (P-value)
(a) Starting breast feeding Very 140 (52) 1.00 - - Fairly 42 (15) -0 .245 0.78 0.592 A little/not at all 25 (9) - 0 .682 0.51 0.200 Did not see BFA 64 (24) - 0 . 9 4 6 0.39 0.007
Total 271 (100)
(b) Maintaining breast feeding Very 116 (55) 1.00 - - Fairly 34 (16) -0 .416 0.66 0.360 A little/not at all 18 (9) - 0.609 0.54 0.300 Did not see BFA 43 (20) -0 .068 0.93 0.880
Total 271 (100)
*The odds ratio is derived from the exponent of beta (e~'~).
the specific settings of the special care baby unit and the community) who felt that she had no advisory role at all.
Feeding method at 2 days and 6 weeks
In 1988, 81.7% (95% CI 76.4-87.0) began breast feeding in the first two days, and this figure was 76.7% in 1990 (72.1-81.3). Although the percentage breast feeding was a bit lower in 1990, the difference was non significant (P = 0.21). Despite this lower figure in 1990, there was an increase in the overall percentage breast feeding at 6 weeks from 57.4% (50.6-64.2) in 1988 to 64.0% (58.8-69.2); this difference was not significant (P=0.15).
A more useful, and comparable picture of breast feeding maintenance can be gained from looking at the outcome for women who began breast feeding. In 1988, 29.7% (22.7-36.7) of the 165 women who began breast feeding had stopped by 6 weeks, whereas in 1990, 22.3% (17.1-27.5) of 247 women ceased breast feeding (P=0.11).
The effect o f BFA support on outcome
Women were asked in the 1990 questionnaire whether they had seen the BFA, and if so how supportive she had been over feeding. Unfortunately, 50 women did not give complete or consistent answers to the two related questions concerning the BFA, that is: (a) time with the BFA; and (b) level of support from the BFA. The inconsistent responses were removed for this analysis, leaving 271 subjects (approx. 40% of these excluded mothers bottle fed at 2 days, compared to 23% for the whole sample).
Almost 30% of women reported that they did not see the BFA, and a further 14.3 % reported inadequate time with her. The commonest length of hospital stay (mode) was 4 days (19% of mothers), with 11% staying only one day and 16% two days. Of those that did see the BFA, the majority found her very or fairly supportive (Table 3).
Table 3(a) shows that women who did not see the BFA were significantly less likely to begin breast feeding (odds ratio 0.39, P=0.007). However, Table 3(b) shows that seeing the BFA carried no advantage in terms of maintaining breast feeding up to 6 weeks (odds ratio 0.93, P=0.88). These are univariate analyses, and do not take account of the characteristics of women who did and did not see the BFA; this is considered further in the section below headed 'Factors affecting the uptake and maintenance of breast feeding', and in Tables 5 and 6.
The use of supplements in breast fed babies
One of the important policy changes since 1988 was the removal from the postnatal wards of dextrose. In 1988, 93% of breast fed babies received at least one supplement but in 1990 this had fallen to 60%, a highly significant difference (P < 0.0001). Although there was a difference between the two studies in the way that information on supplements was collected (2-day interview in 1988 vs 6-week recall in 1990), the validity of the 1990 responses can be assessed to some degree. Only 7 (2.8%) of women reported using dextrose in 1990 (at which time none was in fact available on the ward), indicating that the great majority of mothers were able to distinguish between dextrose and sterile water.
The reported use of sterile water increased from 20.6% in 1988 to 46.1% in 1990 (P= 0.0001)~ while the use of formula milk decreased from 31.5% to 22.7% (P=0.06). Thus, the removal of dextrose may have been compensated for by increased use of sterile water, but not formula milk.
Conflicting advice
Between 1988 and 1990, there was a significant decrease from 24 to 14% in the proportion of mothers reporting that advice was mainly conflicting, and a corresponding increase in the percentage reporting that advice was mainly consistent from 33 to 48%

Usefulness of a non-experimental study design in service evaluation
Table 4. Associations with feeding method were examined using univariate logistic regression for the following factors
Social class Mother's age Parity Mode of delivery Previous breast feeding (multips only) Use of supplements Length of hospital stay Conflict in advice Sex of baby Birthweight Support from BFA
1113
(P < 0.001). The 1990 question was made more specific than that used in 1988, referring only to feeding advice from health service staff (1990) rather than feeding advice in general (1988). This change limits the validity of the comparison; however, whether or not there has been a genuine improvement in the consistency of advice, it is notable that in 1990 there were still 37% of mothers who reported that advice from unit staff was mainly or partly conflicting.
Mothers' views on hospital policy
Mothers were asked whether the hospital seemed to support breast feeding, bottle feeding or supported both methods equally. An identical question was asked at 6 weeks in both studies. Between 1988 and 1990 there was an increase in the percentage of mothers who thought that the hospital supported breast feeding from 48.5 to 55.9%, and corresponding reductions in the percentages who felt that the hospital supported bottle feeding (from 4.9 to 1.9%) and that the hospital was neutral (from 35.1 to 28.6%); these changes were significant ( P = 0.034).
It is interesting that, while about half of the mothers thought that the hospital supported breast feeding, only about one third of staff believed that there should be a policy actively encouraging breast feeding (Table 1). This difference may indicate that although staff are comfortable encouraging breast feeding in principle, they are reluctant about working to rigid rules which are seen as (potentially) pressurizing some women with other views or needs.
Factors affecting the uptake and maintenance of breast feeding
(a) Uptake at 2 days. Associations between feeding method and the various factors examined in the 1990
study have been explored using univariate logistic regression for the variables listed in Table 4.
The factors which were significantly associated with a lower chance of starting breast feeding were; lower social class, young maternal age ( < 25 years), length of stay in hospital greater than one week, birth- weight < 2800 g (this cut-off used as numbers below 2500 g were inadequate for analysis), and not seeing the BFA. Among multiparous women, a history of not breast feeding previously (P<0.001) or of breast feeding for less than 6 months (P<0.005) were both strongly associated with a lower chance of breast feeding this child.
It can be expected that some of these factors would be inter-related, for instance social class and birthweight. Table 5 shows the results of multivariate logistic regression, excluding the history of previous breast feeding since the percentage of multiparous mothers in the sample was only 49%, and this would have severely restricted the power of the analysis. Lower social class, younger maternal age and not seeing the BFA remained as the most important factors independently associated with not starting to breast feed.
( b ) Maintenance up to 6 weeks. The factors identified as important in the uptake of breast feeding were also associated with maintenance up to 6 weeks. Thus, lower social class, young maternal age ( < 25 years), longer than average length of stay in hospital (5-7 days), and low birth weight (also birthweight > 3499 g) were all associated with a lower chance of maintaining breast feeding to 6 weeks. The history of breast feeding among multiparous women showed the same relationships. However, there were also a number of factors relating to the service and obstetric experience; the mode of delivery [assisted, e.g. forceps and Ventouse extraction (P=0.011), and Caesarian
Table 5. Factors associated with a lower chance of starting breast feeding in multivariate analysis, showing logistic regression coefficients and odds ratios, 1990 study
Factor Category Beta Odds r a t i o (P-value)
Social class I & II 1.00 III NM - 1.116 0.33 0.002 Manual - 0.355 0.70 0.49 I
Mother's age Continuous 0.057 1.061yr 0.070
BFA supportiveness Very 1.00 Fairly 0.169 1.18 0.759
A little/not at all - 0.546 0.58 0.322 Not seen - 0.839 0.43 0.026
1114 NIGEL BRUCE a n d ANJA GRIFFIOEN
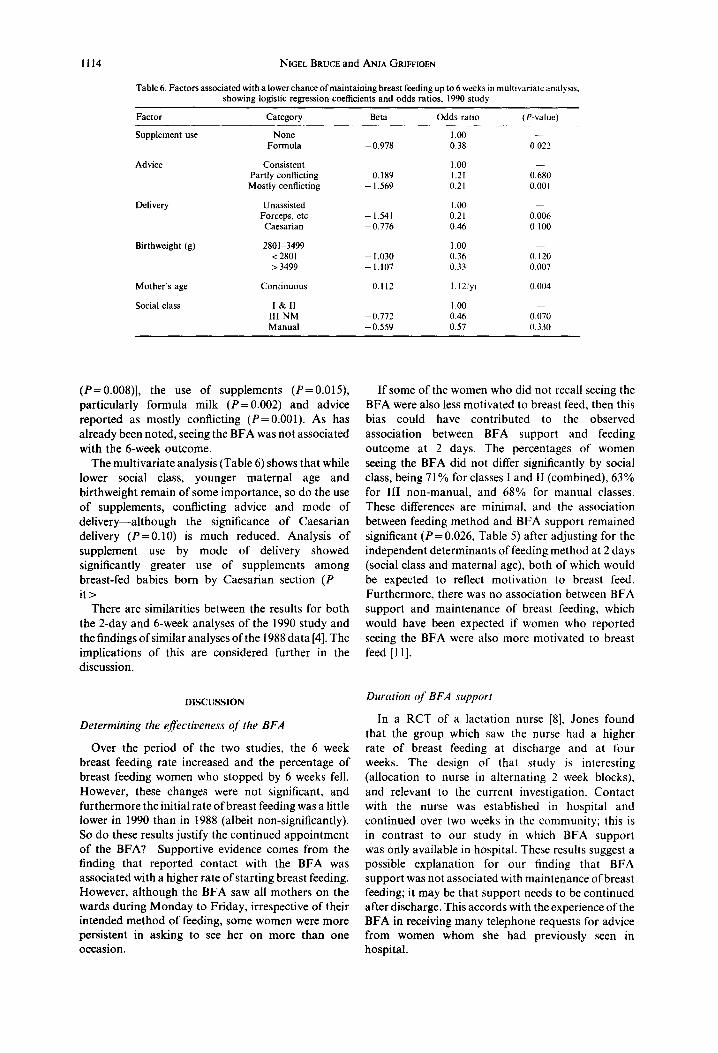
Table 6. Factors associated with a lower chance o f mainta in ing breast feeding up to 6 weeks in mult ivariate analysis, showing logistic regression coefficients and odds ratios, 1990 study
Factor Category Beta Odds ratio (P-value)
Supplement use None 1.00 - Formula - 0.978 0.38 0.022
Advice Consistent 1.00 Partly conflicting 0.189 1.21 0.680 Mostly conflicting - 1.569 0.21 0.001
Delivery Unassisted 1.00 --- Forceps, etc - 1.541 0.21 0.006
Caesar ian - 0.776 0.46 0.100
Birthweight (g) 2801-3499 1.00 <2801 - 1.030 0.36 0.120 > 3499 - 1.107 0.33 0.007
Mother ' s age Cont inuous 0.112 1.12/yr 0.004
Social class I & I1 1.00 - I I I N M - 0 . 7 7 2 0.46 0.070 Manual - 0.559 0.57 0.330
( P = 0.008)], the use of supplements (P=0.015), particularly formula milk (P=0.002) and advice reported as mostly conflicting (P=0.001). As has already been noted, seeing the BFA was not associated with the 6-week outcome.
The multivariate analysis (Table 6) shows that while lower social class, younger maternal age and birthweight remain of some importance, so do the use of supplements, conflicting advice and mode of delivery--although the significance of Caesarian delivery (P=0.10) is much reduced. Analysis of supplement use by mode of delivery showed significantly greater use of supplements among breast-fed babies born by Caesarian section (P i t>
There are similarities between the results for both the 2-day and 6-week analyses of the 1990 study and the findings of similar analyses of the 1988 data [4]. The implications of this are considered further in the discussion.
D I S C U S S I O N
Determining the effectiveness of the BFA
Over the period of the two studies, the 6 week breast feeding rate increased and the percentage of breast feeding women who stopped by 6 weeks fell. However, these changes were not significant, and furthermore the initial rate of breast feeding was a little lower in 1990 than in 1988 (albeit non-significantly). So do these results justify the continued appointment of the BFA? Supportive evidence comes from the finding that reported contact with the BFA was associated with a higher rate of starting breast feeding. However, although the BFA saw all mothers on the wards during Monday to Friday, irrespective of their intended method of feeding, some women were more persistent in asking to see her on more than one occasion.
If some of the women who did not recall seeing the BFA were also less motivated to breast feed, then this bias could have contributed to the observed association between BFA support and feeding outcome at 2 days. The percentages of women seeing the BFA did not differ significantly by social class, being 71% for classes I and II (combined), 63% for III non-manual, and 68% for manual classes. These differences are minimal, and the association between feeding method and BFA support remained significant ( P = 0.026, Table 5) after adjusting for the independent determinants of feeding method at 2 days (social class and maternal age), both of which would be expected to reflect motivation to breast feed. Furthermore, there was no association between BFA support and maintenance of breast feeding, which would have been expected if women who reported seeing the BFA were also more motivated to breast feed [11].
Duration of BFA support
In a RCT of a lactation nurse [8], Jones found that the group which saw the nurse had a higher rate of breast feeding at discharge and at four weeks. The design of that study is interesting (allocation to nurse in alternating 2 week blocks), and relevant to the current investigation. Contact with the nurse was established in hospital and continued over two weeks in the community; this is in contrast to our study in which BFA support was only available in hospital. These results suggest a possible explanation for our finding that BFA support was not associated with maintenance of breast feeding; it may be that support needs to be continued after discharge. This accords with the experience of the BFA in receiving many telephone requests for advice from women whom she had previously seen in hospital.

Usefulness of a non-experimental study design in service evaluation 1115
Identifying the contribution of the BFA
In so far as the contribution of the BFA to the observed rate of breast feeding can be isolated and studied, there is evidence to support continuation of this post. It must be recalled however, that her contribution is not only through direct interaction with the mothers, but also through support and training of maternity unit staff. For example, the BFAs contribution to reduced conflict in advice and supplement use, and the increase in support for breast feeding by the hospital as perceived by mothers, would be extremely difficult to identify and it is necessary to rely more on qualitative accounts of staff and mothers. The current study did not include in-depth qualitative enquiry, but the variety of information that was available has proved useful in the difficult task of interpretation, and this point is considered sub- sequently.
Appropriateness of stud), design
A RCT of the types used by Jones [8] and Frank [12] was not possible for this study because the work of the BFA was much more integrated into the activity of the maternity unit. Indeed, despite the more experimental nature of the interventions in both of those studies [8, 12], some concern was expressed about the influence on the control groups.
A controlled trial of policy changes such as those described here would have required a multicentre study, with hospitals as the units of randomization. It is undoubtably desirable that new health care interventions should be evaluated in controlled trials, but it is also important to distinguish between a definitive controlled trial which assesses the effective- ness (and sometimes the economic efficiency) of a given intervention in a structured research setting, and an evaluation of what happens in practice in a different hospital or district. The importance of this distinction can be appreciated in respect of the unusually high rates of initial breast feeding at this hospital of about 80% at 2 days, compared to 65% nationally [2] and 44% in the controlled study reported by Jones as well as the marked differences in the structures of the interventions [8]; it could not simply be assumed that what has been studied elsewhere would apply here.
There have been a number of other studies of the effect of various interventions on the success of breast feeding [7, 10], and generally a randomized trial design has not been used. Palti studied the outcome of integrating a breast feeding promotion program into routine maternal and child health services [10], an approach which would not have permitted randomiz- ation within the study community. Reference was made to historical controls, and also to a group in a nearby area. Winnikof reported the outcome of a range of hospital initiatives [7], and a nearby hospital was used as a control. We did not feel that the resources required to include a single neighbouring control hospital would have been worthwhile. This
approach is not a substitute for a randomized controlled trial, and if changes occurred in the control hospital during the course of the study (a development over which we could exercise no influence), then interpretation would have been even harder.
Changes in study design
One other important issue was the change to some key elements of the study design, in particular the abandonment of the initial (day 2) questionnaire that was used in 1988. It could be argued that the need for a simpler study design should have been anticipated, and a more consistent design used throughout. However, in programme evaluations, priorities, staff and resources do change, and this may well put pressure on the researcher to adapt the design or discontinue the work. The restrictions on interpret- ation resulting from design change need to be made clear in advance to service and management colleagues (as was done in this case), but if there is a general lesson from this experience it is that the initial design should err towards the most streamlined and efficient possible.
Persisting associations highlight areas jbr action
In this study, we have focused on what can be established from a comparison of the 1988 and 1990 studies, and in particular from studying the issues that have remained as important influences on feeding method in the 1990 study. This latter point is well illustrated by the persisting influence of factors such as assisted and Caesarian delivery, supplement use and conflicting advice in the maintenance of breast feeding.
While recognizing that there are limitations to what can be concluded from a study such as this, we have identified the following additional useful points. The fact of carrying out a local study has focused attention on baby feeding and aroused considerable interest. The two studies have also provided a good deal of information which would not have been available from other sources. The rates of breast feeding at 2 days and 6 weeks are now known to be high, so the service is starting from an above average position. Nevertheless, it is still the case that nearly 25% of breast feeding women stop in the first 6 weeks, and the continuing importance of conflicting advice, sup- plement use, age, social class, mode of delivery and birth weight have been identified.
Another useful outcome of the study is that it has been possible to gain some insight into important observations such as the lower chance of maintaining breast feeding after Caesarian delivery. This was associated with a higher rate of supplement use, which suggests a way forward for further inquiry and possible changes in staff practices.
Variety of data aids interpretation
The surveys yielded valuable insight into the views of maternity unit staff about the development of policy, and this was one area where the variety of

1116 NIGEL BRUCE and ANJA GRIFFIOEN
information helped to interpret the findings and suggest ideas for action. Alongside the changes reported by mothers, midwifery staff in the maternity unit increased their support for a feeding policy and expressed a generally positive and collaborative view of the BFA's role. At the same time however, staff still had concerns about 'pushing' breast feeding too hard, and in coping without the use of supplements in a variety of situations. Furthermore, about half of the stafffelt that supplements of sterile water were justified in a full term normal breast-fed baby, corresponding with the findings for supplement use in practice, The study has provided some information on why staff believed this, and their beliefs must be addressed if constructive change is to be achieved. This ambiva- lence has been recognized in other studies, and may be one important barrier to achieving policy goals in practice [4, 13-14].
CONCLUSIONS
It has been stated that relatively inexpensive investigations (of baby feeding) can be useful in drawing comparisons with national trends, in programme improvement and for targeting high risk groups [15], and our experience with this project would support this conclusion. However, it must be recognized that the study cannot quantify the health or economic outcomes of the intervention or any specific aspect of it. Theoretically, answers to these questions can only be derived from RCTs, but the demands of rigorous experimental design will often mean that the intervention (in this case, the appointment of a BFA) is studied somewhat artificially as a discrete entity and not integrated into the rest of the service as would normally be the case. If the whole 'package' is to be investigated, then randomization of study centres is required which will make the study very complex and expensive. These practical considerations mean that in many instances studies of the type described here will need to be relied upon for the assessment and development of service changes in the day-to-day setting. Although care is required in the interpretation of the findings, it is nevertheless possible to obtain a great deal of useful information that is relevant to policy development.
Acknowledgements--This study was funded by Hampstead Health Authority. The contribution of Dr Zulfia Khan, now Lecturer in Community Medicine at the University of Aligarh, India, is acknowledged. The authors would like to thank the maternity unit staff for all their help and co-operation, in particular the Baby Feeding Advisers Jeanette L'Estrange (1990-) and Alex Dethridge (1988-89), and the Head of Midwifery Mrs Jane Bramley. Thanks also to all of the women who took time to complete and return the questionnaire at such a busy time.
REFERENCES
1. Black N. Quality assurance of medical care. J. Pub. Hlth Med. 12, 97, 1990.
2. DHSS. Present Day Practice in Infant Feeding: Third Report. Report on Health and social subjects 32. HMSO, Oxford, 1988.
3. American Academy of Paediatrics. The promotion of breast feeding. Paediatrics 69, 654, 1992.
4. Bruce N.G., Khan Z. and Olsen N.D.L. Hospital and other influences on the uptake and maintenance of breast feeding: the development of infant feeding policy in a district. Public Hlth 105, 357, 1991.
5. Jenner S. The influence of additional information, advice and support on the success of breast feeding in working class primparas. Child: care, hlth dev. 14, 319, 1988.
6. ReiffM.I. and Essock-Vitale S.M. Hospital influences on early infant feeding practices. Paediatrics 76, 872, 1985.
7. Winnikof B., Myers D., Laukaran V.H. and Stone R. Overcoming obstacles to breast feeding in a large municipal hospital: application of lessons learned. Paediatrics 80, 423, 1987.
8. Jones DA. and West R.R. Lactation nurse increases duration of breast feeding. Arch. Dis. Childhood60, 772, 1985.
9. Levi J. Establishing breast feeding in a hospital. Arch. Dis. Childhood63, 1281, 1988.
10. Palti H., Valderma C., Pogrund R., Jarkoni J. and Kurtzman C. Evaluation of the effectiveness of a structured breast feeding program integrated into a maternal and child health service in Jerusalem. Israel J. Med. Sci. 24, 324, 1988.
11. Jones D.A., West R.R. and Newcombe R.G. Maternal characteristics associated with the duration of breast feeding. Midwifery 2, 141, 1986.
12. Frank D.A., Wirtz S.J., Sorenson J.R. and Heeren T. Commercial discharge packs and breast feeding counseling: effects on infant feeding in a randomised trial. Paediatrics 80, 845, 1987.
13. Beeken S. and Waterston T. Health service support of breast feeding; are we practising what we preach? Br. Med. J. 305, 285, 1992.
14. Waterston T. and Davies J. Could hospital do more to encourage breast feeding? Br. Med. J. 307, 1437, 1993.
15. Labbok M.H. and Simon S.R. A community study of a decade of in-hospital breast feeding: implications for breast feeding promotion. Am. J. Prel,. Med. 4, 62, 1988.





























