Embed Size (px)
Citation preview

Usefulness of External Counterpulsation EarlyPostoperatively After the Fontan Procedure in Children
William Ma, MD, Matthew S. Lemler, MD, Hisashi Nikaidoh, MD,Steven R. Leonard, MD, Gwendoline Y. Shang-Feaster, MD, Brett P. Giroir, MD, and
Daniel Stromberg, MD
External counterpulsation (EC) is a noninvasive circu-latory assistance technique that improves coronary
blood flow and myocardial performance, augments sys-temic venous return, and reduces ventricular afterload.1–3
We hypothesized that EC could benefit patients whounderwent the Fontan procedure by improving cardiacoutput in the early postoperative period. EC had not beenstudied in the postoperative setting, and had never pre-viously performed in the pediatric population. Therefore,this investigation sought to provide preliminary evidenceof EC safety and short-term efficacy in children afterFontan surgery.
• • •We performed a prospective, within-patient, con-
trolled investigation of EC in children who underwentthe Fontan procedure (fenestrated and nonfenestrated)at Children’s Medical Center, Dallas, from May 1999to June 2001. Children were considered for participa-tion in the study if they were consecutive pediatricpatients for whom parental consent was obtained, ifthere was an EC machine available, and if EC cuffsizes were deemed appropriate (pediatric-sized cuffstraps able to be tightened over a sheepskin barrier toprevent excessive movement and skin irritation duringEC). Patients were excluded from study for the fol-lowing reasons: significant intraoperative surgicalcomplications that may have compromised postoper-ative neurologic status (defined as �10 minutes ofhypotension off bypass with blood pressure less thanthe fifth percentile for age), extubation before or im-mediately upon arrival to the cardiac intensive careunit, presence of a cardiac arrhythmia or paced heartrhythm, invasive line(s) in the femoral or lower ex-tremities, peripheral vascular disease, musculoskeletalanomaly involving the lower extremities, significantand prolonged postoperative hemorrhage (�3 ml/kg/hour persisting for �10 hours after arrival to thecardiac intensive care unit), or aortic insufficiency.
After admission to the cardiac intensive care unit,each patient was assessed for clinical stability. Bloodproducts and/or volume (5% albumin) were adminis-tered and inotropes were adjusted at the discretion ofthe attending physician based on hemodynamic status,chest tube drainage, hemoglobin level, and degree of
anticoagulation. Intravenous fluid was administeredbefore the investigation if systemic perfusion wasdetermined to be clinically poor, or if systolic bloodpressure decreased below the fifth percentile for age atany time. The study protocol was initiated while pa-tients were sedated and anesthetized with midazolamand fentanyl, before extubation, and after mediastinalblood loss was controlled (�3 ml/kg/hour). Inotropesand vasoactive medications were unchanged duringthe period of investigation.
The study protocol was divided into 3 10-minuteperiods. During the first period, baseline parameterswere measured before initiation of EC. This was im-mediately followed by a 10-minute EC period, anddirectly thereafter, a postintervention period. The he-modynamic parameters obtained during all 3 periodsincluded cardiac index (CI) by ascending aortic pulseDoppler echocardiography (averaged over 8 cardiaccycles),4 vital signs (heart rate, blood pressure), andcentral venous pressure (CVP). Each parameter wasmeasured every minute during the 3 study intervals,except ascending aortic Doppler flow, which wasevaluated every 2 minutes. Echocardiographic deter-minations of CI were made off-line by a single inter-preter who was blinded to the period of testing.Blinded interpretation was feasible because EC doesnot alter ascending aortic Doppler flow patterns.5Chest tube output and oxygen saturation were re-corded throughout the investigation.
EC was performed using the Cardiomedics Cardi-Assist 3000 EC system (Irvine, California). Pediatriccuffs were applied over a sheepskin barrier to preventskin irritation during counterpulsation. The patient’selectrocardiographic signal directed timing of distal-to-proximal cuff inflation at the onset of diastole, anddeflation at the onset of systole. Cuff pressures andinflation delay after inscription of the QRS complexwere adjusted during EC to achieve maximal diastolicaugmentation using the lowest applied external force.Finger plethysmography was used for arterial waveform monitoring.
Tukey’s repeated-measures analysis of variancewas used for comparison of serially collected datafrom each patient. Chi-square testing was used todetermine relations between categorical variables.Data are presented as median with associated range, ormean � SEM unless otherwise specified.
Consent for study participation was obtained pre-operatively from 26 patients who underwent the Fon-tan procedure and their parents/guardians. Fourteenchildren were excluded from the investigation in thepostoperative period for the following reasons: 8 had
From the University of Texas, Southwestern Medical Center at DallasChildren’s Medical Center of Dallas, Dallas, Texas. This study waspartially funded by a grant from Cardiomedics, Inc., Irvine, California.Dr. Stromberg’s address is: Department of Pediatrics, Cardiology,University of Texas, Southwestern Medical Center at Dallas, 1935Motor Street, Dallas, Texas 75235. E-mail: [email protected]. Manuscript received April 24, 2002; revised manuscriptreceived and accepted June 25, 2002.
1029©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 90 November 1, 2002 PII S0002-9149(02)02696-6
lower extremity/femoral arterial indwelling catheters,2 required temporary pacing due to cardiac arrhyth-mias, 3 had prolonged postoperative bleeding, and 1was extubated upon arrival to the cardiac intensivecare unit. Thus, 12 patients began the EC protocol.However, 2 were excluded from the final analysis.One patient underwent EC lacking complete equip-ment for the study (no buttock cuff was available).The other child did not complete the EC testing pro-tocol due to a hospital electrical malfunction. Thus, 10extracardiac Fontan patients completed the EC proto-col within 4 hours of intensive care unit admission(Table 1). The median age of the patients was 4.1years (range 2.4 to 8.4), and the median weight was17.6 kg (range 11.9 to 25.9).
There were no complications or morbidities asso-ciated with EC use. Mediastinal chest tube outputremained minimal (mean 0.6 ml/kg) throughout thestudy period. Irritation at sites of cuff placement (legsand buttock skin) was insignificant. All patients weresuccessfully extubated shortly after conclusion of theEC protocol (median 3.3 hours, range 1.5 to 8.8).
Study subjects were transferred outof the intensive care unit expedi-tiously (median 44 hours, range 28to 93), and all patients survived untilhospital discharge without neuro-logic sequelae.
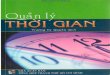
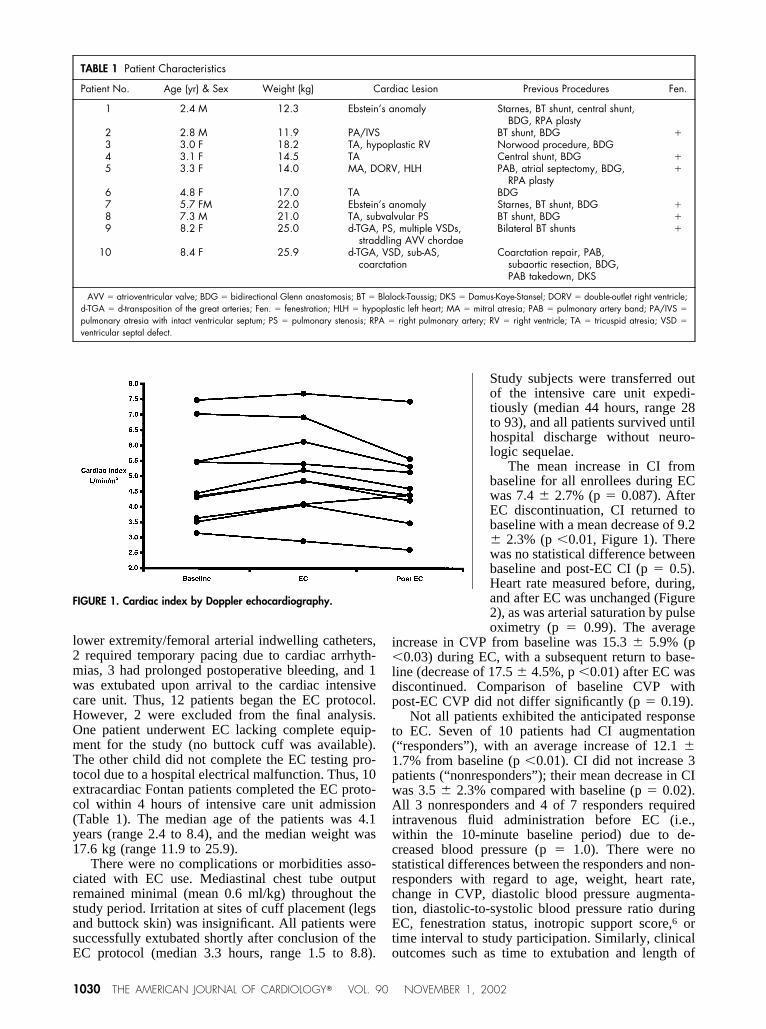
The mean increase in CI frombaseline for all enrollees during ECwas 7.4 � 2.7% (p � 0.087). AfterEC discontinuation, CI returned tobaseline with a mean decrease of 9.2� 2.3% (p �0.01, Figure 1). Therewas no statistical difference betweenbaseline and post-EC CI (p � 0.5).Heart rate measured before, during,and after EC was unchanged (Figure2), as was arterial saturation by pulseoximetry (p � 0.99). The average
increase in CVP from baseline was 15.3 � 5.9% (p�0.03) during EC, with a subsequent return to base-line (decrease of 17.5 � 4.5%, p �0.01) after EC wasdiscontinued. Comparison of baseline CVP withpost-EC CVP did not differ significantly (p � 0.19).
Not all patients exhibited the anticipated responseto EC. Seven of 10 patients had CI augmentation(“responders”), with an average increase of 12.1 �1.7% from baseline (p �0.01). CI did not increase 3patients (“nonresponders”); their mean decrease in CIwas 3.5 � 2.3% compared with baseline (p � 0.02).All 3 nonresponders and 4 of 7 responders requiredintravenous fluid administration before EC (i.e.,within the 10-minute baseline period) due to de-creased blood pressure (p � 1.0). There were nostatistical differences between the responders and non-responders with regard to age, weight, heart rate,change in CVP, diastolic blood pressure augmenta-tion, diastolic-to-systolic blood pressure ratio duringEC, fenestration status, inotropic support score,6 ortime interval to study participation. Similarly, clinicaloutcomes such as time to extubation and length of
FIGURE 1. Cardiac index by Doppler echocardiography.
TABLE 1 Patient Characteristics
Patient No. Age (yr) & Sex Weight (kg) Cardiac Lesion Previous Procedures Fen.
1 2.4 M 12.3 Ebstein’s anomaly Starnes, BT shunt, central shunt,BDG, RPA plasty
2 2.8 M 11.9 PA/IVS BT shunt, BDG �3 3.0 F 18.2 TA, hypoplastic RV Norwood procedure, BDG4 3.1 F 14.5 TA Central shunt, BDG �5 3.3 F 14.0 MA, DORV, HLH PAB, atrial septectomy, BDG,
RPA plasty�
6 4.8 F 17.0 TA BDG7 5.7 FM 22.0 Ebstein’s anomaly Starnes, BT shunt, BDG �8 7.3 M 21.0 TA, subvalvular PS BT shunt, BDG �9 8.2 F 25.0 d-TGA, PS, multiple VSDs,
straddling AVV chordaeBilateral BT shunts �
10 8.4 F 25.9 d-TGA, VSD, sub-AS,coarctation
Coarctation repair, PAB,subaortic resection, BDG,PAB takedown, DKS
AVV � atrioventricular valve; BDG � bidirectional Glenn anastomosis; BT � Blalock-Taussig; DKS � Damus-Kaye-Stansel; DORV � double-outlet right ventricle;d-TGA � d-transposition of the great arteries; Fen. � fenestration; HLH � hypoplastic left heart; MA � mitral atresia; PAB � pulmonary artery band; PA/IVS �
pulmonary atresia with intact ventricular septum; PS � pulmonary stenosis; RPA � right pulmonary artery; RV � right ventricle; TA � tricuspid atresia; VSD �
ventricular septal defect.
1030 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 90 NOVEMBER 1, 2002
cardiac intensive care unit stay were not differentbetween groups.
• • •Previous indications for EC have been directed
toward relief of symptomatic coronary artery diseasein adults who have failed maximal medical therapy,and are not acceptable candidates for surgical inter-vention.7,8 Such patients theoretically benefit from theability of EC to raise diastolic blood pressure andimprove retrograde coronary perfusion either throughnative vessels or recruited collateral vasculature.9,10 Incontrast, we sought to take advantage of EC’s abilityto increase CI by way of simultaneous afterload re-duction and augmentation of systemic venous return.2Patients who have undergone the Fontan procedureoften have elevated pulmonary vascular resistance andventricular dysfunction in the early postoperative pe-riod. Both of these conditions diminish cardiac output,particularly because output is dependent on passiveflow through the Fontan circuit. Thus, EC’s potentialto lower systemic afterload and increase preload to afunctional single ventricle was hypothesized to bedesirable. The prevalence of preexisting coronary ar-tery disease or coronary insufficiency in our studycohort of children between 2.4 and 8.4 years of age,although not determined specifically, was presumed tobe low. Therefore, EC effects on coronary arterialflow, while potentially beneficial, were unmeasuredand considered secondary in importance.
The average increase in CI from baseline duringEC in all children tested was 7.4%. This effect issimilar to that which has been observed in normaladults (11% increase),11 and adults after myocardialinfarction (9.1% increase after 15 minutes).2 If the 7 of10 patients whose CI was augmented during EC areconsidered separately (i.e., the responder subgroup),the magnitude of the CI increase was 12.1% comparedwith baseline. Whether the increase in CI achievedwith EC is clinically significant is beyond the scope
and design of this study. Not surpris-ingly, in our limited sample in whichEC was used for only 10 minutes, nooutcome differences were observedbetween EC responders and nonre-sponders. In addition, all patientswere expeditiously extubated (within4 to 14 hours of surgery) and trans-ferred out of the cardiac intensivecare unit. Future studies are neededto determine the optimal length ofpostoperative counterpulsation andthe clinical utility of the intervention.
In conclusion, this investigationdemonstrates for the first time thatEC can be used safely immediatelyafter cardiac surgery, can be safelyapplied to a pediatric population,and can increase CI in patients
who underwent the Fontan procedure.
Acknowledgment: The investigators wish to thankDeborah Town, RN, Hollie Carron, RDCS, KatherineHarris, BS, RDCS, Keith Dixon, RDCS, the staff ofthe Cardiac Intensive Care Unit at Children’s MedicalCenter, Dallas, Texas, and Cardiomedics, Inc. for theirsupport and assistance in conducting this investiga-tion.
1. Lawson WE, Hui JCK, Zheng ZS, Oster Z, Katz JP, Diggs P, Burger L, CohnCD, Soroff HS, Cohn PF. Three-year sustained benefit from enhanced externalcounterpulsation in chronic angina pectoris. Am J Cardiol 1995;75:840–841.2. Taguchi I, Ogawa K, Oida A, Abe S, Kaneko N, Sakio H. Comparison ofhemodynamic effects of enhanced external counterpulsation and intra-aorticballoon pumping in patients with acute myocardial infarction. Am J Cardiol2000;86:1139–1141.3. Urano H, Ikeda H, Ueno T, Matsumoto T, Murohara T, Imaizumi T. Enhancedexternal counterpulsation improves exercise tolerance, reduces exercise-inducedmyocardial ischemia and improves left ventricular diastolic filling in patients withcoronary artery disease. J Am Coll Cardiol 2001;37:93–99.4. Snider AR, Serwer GA, Ritter SB. Echocardiography in pediatric heart disease.St. Louis: Mosby, 1997:190–191.5. Kern MJ, Henry RH, Lembo N, Park RC, Lujan MS, Ferry D, O’Rourke RA.Effects of pulsed external augmentation of diastolic pressure on coronary andsystemic hemodynamics in patients with coronary artery disease. Am Heart J1985;110:727–735.6. Rosenzweig EB, Starc TJ, Chen JM, Cullinane S, Timchak DM, Gersony WM,Landry DW, Galantowicz ME. Intravenous arginine-vasopressin in children withvasodilatory shock after cardiac surgery. Circulation 1999;100(suppl II):II-182–II-186.7. Soran O, Crawford LE, Schneider VM, Feldman AM. Enhanced externalcounterpulsation in the management of patients with cardiovascular disease. ClinCardiol 1999;22:173–178.8. Barsness G, Feldman AM, Holmes DR Jr, Holubkov R, Kelsey SF, KennardED, The International EECP Patient Registry (IEPR). Design, methods, baselinecharacteristics, and acute results. Clin Cardiol 2001;24:435–442.9. Watson JT, Platt MR, Rogers DE, Sugg WL, Willerson JT. Similarities incoronary flow between external counterpulsation and intra-aortic balloon pump-ing. Am J Physiol 1976;230:1616–1621.10. Masuda D, Nohara R, Hirai T, Kataoka K, Chen LG, Hosokawa R, InubushiM, Tadamura E, Fujita M, Sasayama S. Enhanced external counterpulsationimproved myocardial perfusion and coronary flow reserve in patients withchronic stable angina: evaluation by (13)N-ammonia positron emission tomog-raphy. Eur Heart J 2001;22:1451–1458.11. Cohen LS, Mullins CB, Mitchell JH. Sequenced external counterpulsationand intraaortic balloon pumping in cardiogenic shock. Am J Cardiol 1973;32:656–661.
FIGURE 2. Heart rate. bpm � beats/min.
BRIEF REPORTS 1031




![Intra-aortic balloon pump counterpulsation [IABP] for ...Intervention Review] Intra-aortic balloon pump counterpulsation (IABP) for myocardial infarction complicated by cardiogenic](https://img.pdfslide.net/doc/110x75/5b0c16167f8b9a8b038b916c/intra-aortic-balloon-pump-counterpulsation-iabp-for-intervention-review-intra-aortic.jpg)