Embed Size (px)
Citation preview

Usefulness of Speckle Tracking Echocardiography in HypertensiveCrisis and the Effect of Medical Treatment
Mahboob Alam, MDa, Lily Zhang, MDa, Mark Stampehl, MDa, Nasser Lakkis, MDa,and Hisham Dokainish, MDb,*
The acute impact of hypertensive crisis, and changes after treatment, on left ventricular
aDivision of CMedicine, HoustoMedicine, McMasreceived SeptembMarch 8, 2013.
See page 264*CorrespondinE-mail address
0002-9149/13/$ -http://dx.doi.org/1
(LV) systolic and diastolic function using comprehensive echocardiography, includingspeckle tracking, has not been well characterized. Thirty consecutive patients admitted tothe hospital from the emergency room with hypertensive crisis underwent Doppler echo-cardiography at baseline and after blood pressure optimization. The mean age of thepatients was 54 – 13 years, with 19 men (63%). The most common presenting symptomsincluded dyspnea (70%), chest pain (43%), and altered mental status (13%). Mean systolicand diastolic blood pressures at presentation were 198 – 12 and 122 – 12 mm Hg,decreasing to 143 – 15 and 77 – 12 mm Hg (p <0.001 for both) after treatment. There wasno significant change in LV ejection fraction between baseline and follow-up (48 – 18% vs46 – 18%, p [ 0.50); however, global longitudinal LV systolic strain (L10 – 4% to L12 –4%, p [ 0.01) and global systolic strain rate (L1.0 – 0.4 vs L1.4 – 0.6 sL1, p [ 0.01)significantly improved. Mean global early diastolic strain (L7.2 – 4.0% to L9.4 – 2.9%,p [ 0.004) and early diastolic strain rate (0.3 – 0.2 to 0.5 – 0.4 sL1, p [ 0.05) alsoimproved after treatment. On multivariate analysis, the independent predictors of LVlongitudinal strain at follow-up were LV ejection fraction (p <0.001), heart rate (p[ 0.005),systolic blood pressure (p[ 0.04), and left atrial volume index (p[ 0.05). In conclusion, asopposed to LV ejection fraction, LV systolic strain and strain rate were depressed duringhypertensive crisis and significantly improved after medical treatment. LV diastolic func-tion, assessed using conventional and speckle-tracking parameters, was also depressed andsignificantly improved after treatment. � 2013 Elsevier Inc. All rights reserved. (Am JCardiol 2013;112:260e265)
Hypertensive crisis, including urgency and emergency, isan important cause of hospital visits to the emergency room.1
Yet there are few data on the impact of acute worsening ofblood pressure on left ventricular (LV) systolic and diastolicfunction using conventional and advanced Doppler echo-cardiographic parameters. One study assessed the impact ofacute hypertensive crisis with pulmonary edema on LVejection fraction (LVEF) but did not find a significant changein LVEF after the optimization of blood pressure.2 Severalreports have demonstrated reduced longitudinal andcircumferential systolic strain (e) as well as early and latediastolic e in patients with hypertension in various stages,3e7
and myocardial global longitudinal e has been reported to bea superior predictor of mortality compared with LVEF andwall motion systolic index.8 It has further been demonstratedthat speckle-tracking imaging may be more sensitive than LVvolumetric changes, as speckle-tracking e and strain rate (SR)(correlating with myocardial deformation and the rate ofdeformation, respectively) may be more sensitive to
ardiology, Department of Medicine, Baylor College ofn, Texas; and bDivision of Cardiology, Department ofter University, Hamilton, Ontario, Canada. Manuscripter 26, 2012; revised manuscript received and accepted
for disclosure information.g author: Tel: 905-527-4322 ext 40327; fax: 905-577-1474.: [email protected] (H. Dokainish).
see front matter � 2013 Elsevier Inc. All rights reserved.0.1016/j.amjcard.2013.03.025
pathologic changes than LVEF.9e13 However, it is unknownif hypertensive crisis is associated with LV systolic and dia-stolic abnormalities as assessed by speckle-tracking imagingand if acute treatment of hypertensive crisis results insignificant improvement in function. Therefore, we hypoth-esized that speckle-tracking echocardiography would iden-tify LV systolic and diastolic abnormalities associated withhypertensive crisis that would improve with treatment and,furthermore, that these abnormalities and subsequentimprovement would not necessarily be detected by changesin LVEF.
Methods
This study was conducted at a tertiary-level academicpublic hospital in Houston, Texas. All patients presenting tothe emergency room with symptoms or signs consistent withhypertensive emergency or urgency (hypertensive crisis)were eligible for inclusion in this study. Patients wereincluded in the study if they had presenting blood pressures�180 mm Hg systolic or �120 mm Hg diastolic (recordedby emergency room medical staff members on presentation)in addition to clinical evidence of chest pain, shortness ofbreath, altered mental status, cerebrovascular accident(including transient ischemic attack and stroke), or acuterenal failure.1 All patients who were included in this studyunderwent 2 separate transthoracic echocardiographicexams, first at initial screening in the emergency room whileblood pressure was still elevated within the aforementioned
www.ajconline.org

Table 1Baseline demographic and clinical variables (n ¼ 30)
Variable Value
Age (yrs) 54 � 13Body mass index (kg/m2) 33 � 9.6Body surface area (m2) 2.0 � 0.3Men 19 (63%)African American 19 (63%)Asian 1 (3%)European American 2 (7%)Hispanic/Latino 8 (27%)Hypertension 30 (100%)Diabetes mellitus 16 (53%)Dyslipidemia* 27 (90%)Coronary artery disease† 6 (20%)Cardiomyopathyz 16 (53%)Tobacco 17 (57%)Myocardial infarction 6 (20%)Congestive heart failure 15 (50%)Previous hypertensive crisis 3 (10%)Cerebrovascular accident 6 (20%)Chronic renal insufficiency 12 (40%)Dyspnea 21 (70%)Heart failure 20 (67%)Chest pain 13 (43%)Acute coronary syndromes 2 (7%)Altered mental status/encephalopathy 4 (13%)Cerebrovascular accident 5 (17%)Acute renal failure 12 (40%)Cocaine intoxication 2 (7%)
Data are expressed as mean � SD or as number (percentage).* Documented total cholesterol �240 mg/dl or low-density lipoprotein
�160 mg/dl or currently taking lipid-lowering medication.† Documented myocardial infarction, coronary artery bypass surgery, or
percutaneous coronary intervention or diameter coronary stenosis �70% in�1 major epicardial coronary artery.
z Documented hypertensive heart disease (LV mass index >115 g/m2) ora documented LVEF <50%.
Table 2Baseline and follow-up hemodynamic and conventional echocardiographicdata (n ¼ 30)
Variable Baseline Follow-Up p Value
Systolic blood pressure (mm Hg) 199 � 12 143 � 15 <0.001Diastolic blood pressure (mm Hg) 123 � 12 77 � 12 <0.001Heart rate (beats/min) 82 � 14 76 � 14 0.005Angiotensin-converting enzyme
inhibitors13 (43%) 24 (80%) 0.004
b blockers 7 (23%) 26 (87%) <0.001Calcium channel blockers 11 (37%) 16 (53%) 0.19Statins 5 (17%) 21 (70%) <0.001Aspirin 7 (23%) 16 (53%) 0.02Nitrates 2 (7%) 7 (23%) 0.07Diuretics 14 (47%) 19 (63%) 0.20Vasodilators 6 (20%) 7 (23%) 0.70Angiotensin-converting enzyme
inhibitors13 (43%) 24 (80%) 0.004
Left atrial volume (ml) 74 � 30 64 � 24 0.004Left atrial volume index (ml/m2) 37 � 13 32 � 11 0.005Right atrial volume (ml) 51 � 26 40 � 20 <0.001Right atrial volume index (ml/m2) 25 � 12 20 � 9 <0.001LV end-diastolic dimension (cm) 4.8 � 0.8 4.7 � 0.8 0.30LV end-systolic dimension (cm) 3.6 � 1.2 3.3 � 1.0 0.09LV end-diastolic volume (ml) 127 � 56 125 � 61 0.70LV end-diastolic volume index
(ml/m2)62 � 22 61 � 25 0.70
LV end-systolic volume (ml) 70 � 47 70 � 46 1.00LV end-systolic volume index
(ml/m2)34 � 20 35 � 21 0.90
LV fractional shortening (%) 28 � 15 31 � 14 0.20LVEF (%) 48 � 18 46 � 18 0.50Mitral deceleration time (ms) 175 � 63 204 � 70 0.04E velocity (m/s) 0.9 � 0.2 0.8 � 0.2 0.40A velocity (m/s) 0.7 � 0.3 0.8 � 0.3 0.10Mitral E/A ratio 1.4 � 0.7 1.0 � 0.6 0.09Tissue Doppler lateral annular
velocity (e0) (m/s)0.06 � 0.03 0.07 � 0.03 0.40
Tissue Doppler septal annularvelocity (e0) (m/s)
0.05 � 0.2 0.05 � 0.2 0.30
Mitral E/e0 lateral annularvelocity ratio
15 � 9 12 � 5 0.04
Mitral E/e0 septal annular velocityratio
20 � 7 15 � 7 0.04
Data are expressed as mean � SD or as number (percentage).
Systemic Hypertension/Echocardiography in Hypertensive Crisis 261
parameters, with follow-up echocardiography performed�48 hours after hospital admission when medical optimi-zation of blood pressure had been achieved.
Baseline and follow-up echocardiographic exams wereperformed using a GE Vivid 7 ultrasonographic machine(GE Medical Systems, Milwaukee, Wisconsin). Two-dimensional measurements were performed according to theAmericanSociety of Echocardiography14 and includedLVEFby the biplane method of discs, maximal left atrial volume bythe method of discs, and LV mass by the area-length method;the latter 2 variables were indexed to body surface area.Studies were analyzed by echocardiologists blinded to allclinical data. Mitral inflowmeasurements included peak early(E) and peak late (A) velocities, the E/A ratio, and thedeceleration time of E.15 Three cardiac cycles were measuredand averaged for all Doppler measurements. For 2-dimen-sional speckle tracking, images of LV myocardium wereobtained with a frame rate �60 frames/s (mean framerate 82 � 9).
Measurements of 2-dimensional e and SR were per-formed by off-line analysis. The endocardial border wasmanually traced, and a myocardial region of interest wasthen automatically identified by the software package
(EchoPAC Dimension ’06; GE Medical Systems).As previously described,13 systolic, early diastolic, and latediastolic event timing was based on the timing of theserespective events on SR imaging; in this way, the time frompeak QRS to these events was measured with SR imagingand the same time intervals were used to identify theserespective events for e imaging. In systole, e and SR weremeasured in the parasternal short-axis views at the papillarymuscle level to determine circumferential e and SR and inthe 3 apical views (which were then averaged) to determinelongitudinal e and SR. Similarly, in diastole, early and latediastolic e and SR were determined in the circumferentialand longitudinal vectors.
Continuous data are presented as mean � SD and cate-gorical data as number (percentage). For continuous vari-ables, Student’s t test was performed, and for dichotomous

Table 3Speckle-tracking strain analysis in patients presenting with hypertensivecrisis (n ¼ 30)
Variable Baseline Follow-Up p Value
Mean global longitudinal systolice (%)
�10 � 4 �12 � 4 0.01
Mean global longitudinal systolic SR(s�1)
�1.0 � 0.4 �1.4 � 0.6 0.01
Mean global longitudinal earlydiastolic e (%)
�7.2 � 4.0 �9.4 � 2.9 0.004
Mean global early diastolic SR (s�1) 0.3 � 0.2 0.5 � 0.4 0.05Mitral E/early longitudinal diastolic
e ratio�0.2 � 0.1 �0.09 � 0.04 <0.001
Mitral E/early longitudinal diastolicSR ratio
1.9 � 1.4 1.4 � 0.6 0.04
Mean systolic circumferential e (%) �6.0 � 3.2 �11.3 � 5.4 0.03Mean systolic circumferential SR
(s�1)�0.6 � 0.3 �0.7 � 0.5 0.49
Mean early diastolic circumferentiale (%)
�4.9 � 2.7 �9.4 � 5.0 0.05
Mean early diastolic circumferentialSR (s�1)
0.4 � 0.2 0.7 � 0.3 0.03
Data are expressed as mean � SD.
262 The American Journal of Cardiology (www.ajconline.org)
variables, the chi-square test was used. Linear regressionwas performed to determine the correlation betweencontinuous variables, and multivariate regression was per-formed to determine independence. A p value �0.05 wasconsidered significant. Analyses were performed with SPSSversion 16.0 (IBM, Armonk, New York).
Results
A total of 30 patients with hypertensive crisis, consecu-tively enrolled from June 2008 to July 2009, were includedin the study. Table 1 lists details of baseline demographicand clinical variables, and Table 2 lists vital signs, medi-cations, and comprehensive echocardiographic measure-ments at baseline and follow-up. At the time of follow-upechocardiography, more patients were receiving angio-tensin-converting enzyme inhibitors and b blockers, meansystolic and diastolic blood pressures were significantlylower, and baseline left atrial volume index was significantlydecreased; in contrast, LVEF and LV fractional shorteningat baseline and follow-up were similar. There were nosignificant differences in lateral and septal annular tissueDoppler myocardial velocities at baseline and follow-up;however, there was a significant decrease in lateral andseptal E/e0 ratios.
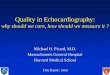
Table 3 lists systolic and diastolic speckle-trackingvariables. In contrast to LVEF, global LV longitudinalsystolic e improved from baseline to follow-up. There wasalso significant improvement in mean global systolic SR andmean global circumferential systolic e. Mean global earlydiastolic e improved from baseline to follow-up, as didmean global early diastolic SR and early circumferentialdiastolic e and SR. Ratios of mitral valve E-wave velocity toearly diastolic longitudinal e decreased from baseline tofollow-up, as did the ratio of mitral E-wave velocity to earlydiastolic SR. Left ventricular ejection fraction and e vari-ables at baseline and follow-up are depicted in Figure 1.
Among continuous variables, significant univariate corre-lates of global LV longitudinal e were LVEF (R ¼ 0.70,p ¼ 0.01), systolic blood pressure (R ¼ 0.52, p ¼ 0.02), leftatrial volume index (R ¼ 0.49, p ¼ 0.03), E/A ratio (R ¼0.47, p ¼ 0.04), and heart rate (R ¼ 0.41, p ¼ 0.05). Onmultivariate analysis, the independent predictors of LVlongitudinal e at follow-up were LVEF (p <0.001), heartrate (p ¼ 0.005), systolic blood pressure (p ¼ 0.04), and leftatrial volume index (p ¼ 0.05). Because most patients in thisstudy (20 of 30 [67%]) presented with clinical diagnoses ofcongestive heart failure, the study cohort was divided intopatients with and without clinical congestive heart failure,with the results listed in Table 4. The patients with clinicalcongestive heart failure at presentation were more likely todemonstrate improvement in systolic and diastolic speckle-tracking e parameters after treatment compared with thosewithout congestive heart failure.
Discussion
This study is the first to demonstrate, using speckle-tracking echocardiography, significant LV systolic anddiastolic abnormalities associated with hypertensive crisisthat improve with medical treatment. In contrast, there wasno significant change in LVEF or LV fractional shorteningfrom baseline to follow-up. These findings of improvementin LV systolic e could be related to the fact that speckle-tracking e analysis is more sensitive at detecting subtlemyocardial abnormalities compared with LVEF before andafter therapy.
Hypertension is characterized by a gradual increase inLV mass, which may result in concentric hypertrophy anddiastolic dysfunction due to LV stiffness with impairedrelaxation.16 The mechanism behind the impairment of LVsystolic and diastolic function during hypertensive crisis, asassessed by speckle-tracking echocardiography, may be dueto increased transmyocardial wall stress, which can producesubendocardial ischemia, thus increasing myocardial stiff-ness and reducing myocardial deformation in systole anddiastole. In a previous study using myocardial resonanceimaging, it was demonstrated that that intramural circum-ferential and longitudinal myocardial shortening weredepressed in hypertensive patients with LV hypertrophy.17
It has also been demonstrated by echocardiography that LVmidwall shortening is depressed in patients with hyperten-sion, indicating that systolic dysfunction may be present inhypertension even with a preserved LVEF.18,19 As bloodpressure decreases after medical treatment, LV wall stressalso decreases, thus decreasing LV stiffness and improvingmyocardial systolic and diastolic function. Our findingsshowed that changes in myocardial systolic function weredetected by speckle-tracking imaging but not by 2-dimen-sional measurements of LV systolic function (LVEF andfractional wall shortening), consistent with several studiesindicating that speckle-tracking imaging (as well as tissueDoppler imaging) can detect myocardial abnormalitiesearlier in the pathophysiologic cascade of heart failure thanLV fractional shortening and LVEF.9e13 This may be thecase because speckle-tracking more sensitively detectsregional changes in myocardial deformation, because oflocalized myocyte dysfunction, that temporally precede

Figure 1. Echocardiographic variables before and after treatment for hypertensive crisis. *p <0.05.
Table 4Baseline and follow-up variables in patients with hypertensive crisis and heart failure
Variable Heart Failure (n ¼ 20) No Heart Failure (n ¼ 10)
Baseline Follow-Up p Value Baseline Follow-Up p Value
Systolic blood pressure (mm Hg) 196 � 18 146 � 22 <0.001 202 � 23 137 � 17 <0.001Diastolic blood pressure (mm Hg) 110 � 20 80 � 16 <0.001 101 � 19 67 � 17 <0.001Heart rate (beats/minute) 80 � 13 74 � 12 0.01 83 � 14 77 � 17 0.07Left atrial volume index (ml/m2) 38 � 13 33 � 10 0.05 34 � 14 29 � 12 0.05Right atrial volume index (ml/m2) 27 � 11 22 � 9 0.001 21 � 11 16 � 7 0.03LV fractional shortening (%) 23 � 13 28 � 14 0.08 38 � 14 36 � 13 0.60LVEF (%) 43 � 16 43 � 16 0.90 59 � 18 53 � 20 0.30Mitral deceleration time (ms) 178 � 64 206 � 68 0.20 170 � 20 199 � 76 0.14E velocity (m/s) 0.9 � 0.3 0.9 � 0.2 0.90 0.7 � 0.1 0.6 � 0.2 0.02A velocity (m/s) 0.7 � 0.3 0.8 � 0.3 0.10 0.7 � 0.2 0.8 � 0.2 0.80Mitral E/A ratio 1.5 � 0.8 1.3 � 0.6 0.30 1.1 � 0.5 0.9 � 0.2 0.20Tissue Doppler lateral annular velocity (e0) (m/s) 0.06 � 0.03 0.07 � 0.02 0.20 0.06 � 0.03 0.05 � 0.02 0.20Tissue Doppler septal annular velocity (e0) (m/s) 0.05 � 0.02 0.05 � 0.02 0.20 0.05 � 0.02 0.05 � 0.02 0.90Mitral E/e0 lateral annular velocity ratio 17 � 5 13 � 5 0.08 15 � 10 12 � 9 0.17Mitral E/e0 septal annular velocity ratio 20 � 6 15 � 5 0.05 18 � 9 14 � 9 0.11Mean global longitudinal systolic e (%) �10 � 4 �12 � 5 0.02 �11 � 5 �12 � 3 0.30Mean global longitudinal systolic SR (s�1) �0.8 � 0.2 �1.1 � 0.4 0.20 �1.4 � 0.4 �2.0 � 0.6 0.15Mean global longitudinal early diastolic e (%) �8.4 � 3.7 �9.2 � 3.2 0.30 �7.0 � 4.4 �10 � 3.0 0.08Mean global early diastolic SR (s�1) 0.6 � 0.3 0.8 � 0.4 0.10 0.5 � 0.2 0.5 � 0.1 0.50Mitral E/early longitudinal diastolic e ratio �0.2 � 0.1 �0.1 � 0.04 0.01 �0.2 � 0.1 �0.07 � 0.02 0.02Mitral E/early longitudinal diastolic SR 1.7 � 0.8 1.3 � 0.5 0.03 2.2 � 0.8 1.6 � 0.8 0.50Mean systolic circumferential e (%) �5.2 � 3.0 �11.4 � 6.2 0.04 �16 � 6.9 �16 � 7.3 0.90Mean systolic circumferential SR (s�1) �0.5 � 0.3 �0.6 � 0.6 0.50 �1.0 � 0.2 �1.1 � 0.5 0.30Mean early diastolic circumferential e (%) �4.5 � 2.9 �9.9 � 5.6 0.01 �9.2 � 5.1 �10.7 � 5.7 0.50Mean early diastolic circumferential SR (s�1) 0.3 � 0.2 0.7 � 0.3 0.01 1.0 � 0.5 0.8 � 0.3 0.40Mean global longitudinal systolic e (%) �10 � 4 �12 � 4 0.02 �11 � 5 �12 � 3 0.30Mean global longitudinal systolic SR (s�1) �0.8 � 0.2 �1.1 � 0.4 0.20 �1.4 � 0.4 �2.0 � 0.6 0.15Mean global longitudinal early diastolic e (%) �8.3 � 3.6 �9.2 � 3.2 0.30 �7.0 � 4.5 �10 � 3.0 0.08
Data are expressed as mean � SD.
Systemic Hypertension/Echocardiography in Hypertensive Crisis 263

264 The American Journal of Cardiology (www.ajconline.org)
global changes in LV dimension or volume.20 Recent datahave also shown that speckle-tracking longitudinal e moresensitively detects improvement in myocardial functionafter aortic valve replacement compared with LVEF.21 Thislatter study, similar to ours, demonstrates the effects ofincreased afterload on the left ventricle, with improvementsin these speckle-tracking parameters after aortic valvereplacement (as afterload decreases). Another recent studyperformed in African subjects demonstrated that LV twistusing speckle tracking was reduced in LV systolicdysfunction.22 In our study, in predominately AfricanAmerican patients with clinical congestive heart failure atpresentation, LV twist was also depressed, consistent withthese findings.
LV diastolic function also showed improvement withacute therapy in these patients. These improvements weredetected by traditional Doppler, including reduction inmitral E/e0 ratio, prolongation of mitral deceleration time,and reduction in left atrial volume. This is consistent withprevious findings, showing that reductions in blood pressureand afterload can reduce myocardial wall stress and improveLV diastolic function.23 A novel feature of our study wasthat 2D speckle-tracking diastolic longitudinal e and SR—and derived ratios using E in the numerator and diastolice and SR in the denominator, as previously published24—also showed improvements after treatment in patients withhypertensive crisis.
There are few data on the acute effects of hypertensivecrises on LV systolic function. A previous study did notdemonstrate a significant change in LV systolic functionduring hypertensive crisis causing pulmonary edemacompared with after treatment; however, this study onlyassessed systolic function using 2-dimensional LVEF andwall motion score.2 In contrast, a previous case reportdescribed acute and reversible LV systolic dysfunction(by LVEF) in a patient with hypertensive crisis.25 With theuse of speckle-tracking e analysis, we were able todemonstrate significant abnormalities in LV systolic anddiastolic function in patients presenting with hypertensivecrisis that improved with medical therapy, whereas theseabnormalities and subsequent changes were not detected byLVEF. Therefore, these data from speckle tracking point tothe importance of early blood pressure control in hyper-tensive crisis that may mitigate more permanent myocardialabnormalities from developing. In addition, future studiesmay be useful to determine if these LV systolic and dia-stolic abnormalities by speckle-tracking imaging influencepatient prognosis in terms of admission for heart failure ordeath.
This study included 30 patients; however, because eachpatient served as his or her own comparator (before andafter treatment for hypertensive crisis), we were able todemonstrate significant differences in several parameters.The patients were not followed for clinical outcomes(readmission for clinical events, death, or stroke), whichwould permit associations to be assessed between thesespeckle-tracking parameters and outcomes. Newer3-dimensional speckle-tracking technology is now availablethat may permit more comprehensive assessments ofmyocardial e and SR in all 3 axes, which would be attractivein future studies.
Disclosures
The authors have no conflicts of interest to disclose.
1. Rodriguez MA, Kumar SK, De Caro M. Hypertensive crisis. CardiolRev 2010;18:102e107.
2. Gandhi SK, Powers JC, Nomeir AM, Fowle K, Kitzman DW, RankinKM, Little WC. The pathogenesis of acute pulmonary edema associ-ated with hypertension. N Engl J Med 2001;344:17e22.
3. Atilgan D, Bilge AK, Onur I, Pamukcu B, Ozcan M, Adalet K.Assessment of longitudinal left ventricular systolic function bydifferent echocardiographic modalities in patients with newly diag-nosed mild-to-moderate hypertension. Anadolu Kardiyol Derg2009;10:247e252.
4. Bilge AK, Atilgan D, Onur I, Pamukcu B, Ozcan M, Adalet K. Rela-tionship between left ventricular hypertrophy, hypertensive retinopathy,microalbuminuria and echocardiographic modalities in newly diag-nosed hypertensive patients. Int J Cardiovasc Imaging 2010;26:405e412.
5. Galderisi M, Lomoriello VS, Santoro A, Esposito R, Olibet M,Raia R, Di Minno MN, Guerra G, Mele D, Lombardi G. Differ-ences of myocardial systolic deformation and correlates of diastolicfunction in competitive rowers and young hypertensives: a speckle-tracking echocardiography study. J Am Soc Echocardiogr 2010;23:1190e1198.
6. Mizuguchi Y, Oishi Y, Miyoshi H, Iuchi A, Nagase N, Oki T.Concentric left ventricular hypertrophy brings deterioration of systoliclongitudinal, circumferential, and radial myocardial deformation inhypertensive patients with preserved left ventricular pump function.J Cardiol 2010;55:23e33.
7. Mizuguchi Y, Oishi Y, Miyoshi H, Iuchi A, Nagase N, Oki T. Bene-ficial effects of telmisartan on left ventricular structure and function inpatients with hypertension determined by two-dimensional strainimaging. J Hypertens 2009;27:1892e1899.
8. Stanton T, Leano R, Marwick TH. Prediction of all-cause mortalityfrom global longitudinal speckle strain: comparison with ejectionfraction and wall motion scoring. Circ Cardiovasc Imaging 2009;2:356e364.
9. DokainishH, SenguptaR, PillaiM,Bobek J, LakkisN.Assessment of leftventricular systolic function using echocardiography in patients withpreserved ejection fraction and elevated diastolic pressures.Am JCardiol2008;101:1766e1771.
10. Park SJ, Miyazaki C, Bruce CJ, Ommen S, Miller FA, Oh JK. Leftventricular torsion by two-dimensional speckle tracking echocardiog-raphy in patients with diastolic dysfunction and normal ejection frac-tion. J Am Soc Echocardiogr 2008;21:1129e1137.
11. Wang J, Khoury DS, Yue Y, Torre-Amione G, Nagueh SF. Preservedleft ventricular twist and circumferential deformation, but depressedlongitudinal and radial deformation in patients with diastolic heartfailure. Eur Heart J 2008;29:1283e1289.
12. Wang J, Khoury DS, Yue Y, Torre-Amione G, Nagueh SF. Leftventricular untwisting rate by speckle tracking echocardiography.Circulation 2007;116:2580e2586.
13. Nguyen JS, Lakkis NM, Bobek J, Goswami R, Dokainish H. Systolicand diastolic myocardial mechanics in patients with cardiac disease andpreserved ejection fraction: impact of left ventricular filling pressure.J Am Soc Echocardiogr 2010;23:1273e1280.
14. LangR, BierigM,DevereuxRB, Flachskamp FA, Foster E, Pellikka PA,Picard MH, Roman MJ, Seward J, Shanewise JS, Solomon SD,Spencer KT, St John Sutton M, Stewart WJ. Recommendations forchamber quantification: a report from the American Society ofEchocardiography’s Guidelines and Standards Committee and theChamber Quantification Writing Group. J Am Soc Echocardiogr2005;18:1440e1463.
15. Lester SJ, Tajik AJ, Nishimura RA, Oh JK, Khandheria BK,Seward JB. Unlocking the mysteries of diastolic function: deci-phering the Rosetta stone 10 years later. J Am Coll Cardiol2008;51:679e689.
16. Bountioukos M, Schinkel AF, Bax JJ, Lampropoulos S, Poldermans D.The impact of hypertension on systolic and diastolic left ventricularfunction. A tissue Doppler echocardiographic study. Am Heart J2006;151:1323.e7e1323.e12.
17. Palmon LC, Reichek N, Yeon SB, Clark NR, Brownson D, Hoffman E,Axel L. Intramural myocardial shortening in hypertensive left

Systemic Hypertension/Echocardiography in Hypertensive Crisis 265
ventricular hypertrophy with normal pump function. Circulation1994;89:122e131.
18. Wachtell K, PapademetriouV, SmithG, Gerdts E, Dahlöf B, EngblomE,Aurigemma GP, Bella JN, Ibsen H, Rokkedal J, Devereux RB. Relationof impaired left ventricular filling to systolic midwall mechanics inhypertensive patients with normal left ventricular systolic chamberfunction: the Losartan Intervention for Endpoint Reduction in Hyper-tension (LIFE)study. Am Heart J 2004;148:538e544.
19. de Simone G, Ganau A, Roman MJ, Devereux RB. Relation of leftventricular longitudinal and circumferential shortening to ejectionfraction in the presence or in the absence of mild hypertension.J Hypertens 1997;15:1011e1077.
20. Gorcsan J III, Tanaka H. Echocardiographic assessment of myocardialstrain. J Am Coll Cardiol 2011;58:1401e1413.
21. Kempny A, Diller GP, Kaleschke G, Orwat S, Funke A, Radke R,Schmidt R, Kerckhoff G, Ghezelbash F, Rukosujew A, Reinecke H,Scheld HH, Baumgartner H. Longitudinal left ventricular 2D strain is
superior to ejection fraction in predicting myocardial recovery andsymptomatic improvement after aortic valve implantation. Int J Car-diol. Epub Jul 3, 2012.
22. Maharaj N, Khandheria BK, Peters F, Libhaber E, Essop MR. Time totwist: marker of systolic dysfunction in Africans with hypertension.Eur Heart J Cardiovasc Imaging 2013;13:358e365.
23. Eryonucu B, Guler N, Guntekin U, Tuncer M. Comparison of the effectsof nitroglycerin and nitroprusside on transmitral Doppler flow parame-ters in patients with hypertensive urgency. Ann Pharmacother 2005;39:997e1001.
24. Dokainish H, Sengupta R, Pillai M, Bobek J, Lakkis N. Useful-ness of new diastolic strain and strain rate indexes for the esti-mation of left ventricular filling pressure. Am J Cardiol 2008;101:1504e1509.
25. D’Aloia A, Fiorina C, Vizzardi E, Faggiano P, Dei Cas L. Hypertensivecrisis and acute, reversible, left ventricular systolic dysfunction: a casereport. Eur J Heart Fail 2002;4:655e660.