Embed Size (px)
Citation preview
DesignforNext
12thEADConferenceSapienzaUniversityofRome
12-14April2017
Copyright©2016.Thecopyrightofeachpaperinthisconferenceproceedingsisthepropertyoftheauthor(s).Permissionisgrantedtoreproducecopiesoftheseworksforpurposesrelevanttotheaboveconference,providedthattheauthor(s),sourceandcopyrightnoticeareincludedoneachcopy.Forotherusespleasecontacttheauthor(s).
User-DesignedDementiaCarePathwaysAdisruptiveapproachtomappingdementiasupportservices
[AuthorNamesAffiliationnamesCorrespondingauthoremail]
Abstract:This paper reports on the first author’s ongoing Arts and Humanities ResearchCouncil (AHRC) fundedPhD research exploring thepotential for disruptive designinterventionswithinthecontextofhealthandsocialcare.Thispaperdescribesanongoing project tomap the services available to peoplewith dementia and theircarers,withaspecificemphasisontheservicesavailablebeforethepatientreceivesaformaldiagnosisofdementia.Manyserviceusersaresimplyunawareof thesupportavailable to them,andarelefttonavigatetheirownpathsthroughtheunfamiliarandintimidatinglandscapeofdementiaservices.Thispaperreportsonthedevelopmentoftwotoolsforusebycarers,patients,anddementiaserviceproviders.Thesetoolsofferinnovativewaysofenablingserviceuserstovisualisethepathwayoftheircurrentandfuturecare,whilst alsoallowing serviceproviders to identify the strengthsandweaknesses inthetypeofsupporttheyprovide.
Keywords:disruption,dementia,innovation,mapping,servicedesign
1.IntroductionAround850,000peopleintheUKsufferfromsomeformofdementia(Judd&Alzhiemer’sSociety,2007)-acomplexandunpredictablebraindisorderassociatedwithprogressivecognitiveandphysicaldegeneration.Dementiamanifestsinmanydifferentways-therearemorethan200differenttypesofdementia-anditssymptomscanhaveawide-rangingimpactonpeoples’health,independence,andtheirrelationshipswithfriendsandfamilymembers.Typicalsymptomsinclude“communicationandlanguageproblemsandchangesinpersonality”(UnforgettableFoundation,2015).Dementiacanalsobringabout,orexacerbate,physicalproblems,suchasfrailtyandpoorself-care.In2015,dementia(andphysicalconditionsarisingdirectlybecauseofdementia)becametheleadingcauseofdeathintheUK(OfficeforNationalStatistics,2016).Thereisnoknowncurefordementia.
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
2
TheUKspends£14.7bnondementiacareserviceseachyear,withafurther£11.6bnvalueofunpaidcareprovidedby“informalcarers”(Alzhiemer’sSociety,2015).Thereare670,000informalcarersintheUKwhoprovideunpaidcareforfriendsandfamilymemberswithdementia.Informalcarersoftenfeelmarginalizedastheyarelefttocopealoneastheirlovedoneundergoesasignificantdeteriorationinphysicalstateand/orpersonalitychanges.Thisleadstoa“biographicaldisruption”(Bury,2982)aspatientsandcarersstruggletocometotermswiththenewlifecircumstancesforceduponthem.Thiscanleavebothpartiesdisorientatedandupsetas“agradual,terrible,horribleprogression”(Newkirk&Lui,2016)unfoldsbeforethem.Carersforpeoplewithdementiareporthigherthannormallevelsofstressanddepressionthanthosewhocareforolderpeoplewhodonotsufferfromdementia(WillsandSoliman,2001;Moiseetal,2004).
Informalcarersplayavitalroleinsupportingpeoplewithdementia.Becauseofthenatureofthecondition,manypatients(particularlythoseintheadvancedstagesofdementia)areunabletounderstandinformationputtothem,andinsomecaseslackthementalorphysicalcapacitytoexpressevenbasicwishes.Informalcarers–manyofwhomhavespentalifetimewiththepatient–areuniquelypositionedtobridgethecommunicationgapbetweenserviceprovidersandserviceusers.
ThispaperwilldescribeanongoingArtsandHumanitiesResearchCouncil(AHRC)fundedcollaborationwithNewcastleCarers,anindependentcharitythatprovidesexpertandimpartialassistancetoinformalcarers.Thisassistanceincludespracticaladvice,emotionalsupportandcounselling,andcomplementarytherapy.Theauthors’previousresearchinthisareaexploredtheexperiencesofinformaldementiacarersandtheirinteractionswithacomplexwebofhealthandsocialcareservices,aswellhowtheydesignedtheirownmethodsofmeetingthechallengestheyfaced.
Ourearlierprojects(Author,2015)highlightedalackofclarityinwhatarecollectivelyreferredtoas“dementiasupportservices”.TheseservicesarespreadacrosstheNationalHealthService(NHS),whichprovides“healthcare”(i.e.clinicaltreatment),andlocalauthoritiesandcharitieswhichprovide“socialcare”–althoughinpracticetheseservicesoverlapinnumerousways.Collectively,dementiasupportservicesincluderespitecare,medication,hospitalin-patienttreatment,andmanyotherformsofinterventionforbothpatientsandcarers.Carersuniversallyexpressedtheviewthattheyrequiredmoreassistanceinidentifyingthemostsuitablepaththroughwhatis,fromtheirperspective,anewandunclearlandscape.Furthermore,theyinformedusthatsuchassistancewouldbemostvaluableintheearlystagesoftheircaringrole–priorto,orimmediatelyafter,dementiaisdiagnosed.Theyalsocomplainedofalackofguidanceastowhichspecificinterventionsmightassist(orhinder)theircaringrole–leadingsometomisstheseservicesaltogether.
TheongoingprojectdescribedinthispaperseekstoaddressthislackofclaritythroughthedevelopmentofmappingtoolswhichproposeaphysicaltopographyofdementiaservicesacrosstwolocationsinNorthEastEngland.Thephysicalartefactsdesignedintheseworkshopsarethefirststepstowardsestablishinganewapproachforengagingwithcarersandpeoplewithdementia.Inacceptingthat“socialinnovationinvolves—indeed,requires—redistributingpower”(Westley,Zimmerman,&Patton,2007),theseinnovativemethodsofvisualisingdementiasupportservicesseektoplacegreaterpowerinthehandsofcarersandpeoplewithdementiawhoknowlittleifanythingaboutwhatchallengesawaitthemandwhichservicesarebestpositionedtoassistthemontheirindividualjourneys.

Articletitle[STYLE:_DfNRunningheadodd]
3
2.AimsandObjectives 2.1DesignDisruptioninContext Theaimofthisresearchistodevelopdisruptivedesigninterventionsthatchallengethestatusquoandprovokenewresponsestothechallengesfacedbyinformalcarers.Theworkhereadoptsalargelyinterventionistapproach,whichisbasedonanumberoftheoriesemanatingfromresearchineconomic,business,anddesign(Christensen,1997;Christensen&Overdorf,2000;Scharmer,2011;RodgersandTennant,2012).Theterm“DesignDisruption”wellestablishedacrossthecommercialsector,whereeconomiceffectsareoftenconcreteandmeasurable(Druker,1985).Bycontrast,publicservicesoperatewithinamorenuancedenvironmentandamorecomplexremit.YeeandWhite(2015)extensivelydiscussthe“goalsandvalues[ofpublicservicedesign]thataremoreambiguousanddifficulttoquantify”,andofferexamplesofbarriersincluding“ariskaverse…performancedrivencultureandlackofincentives”1(Mulgan&Albury,2003).
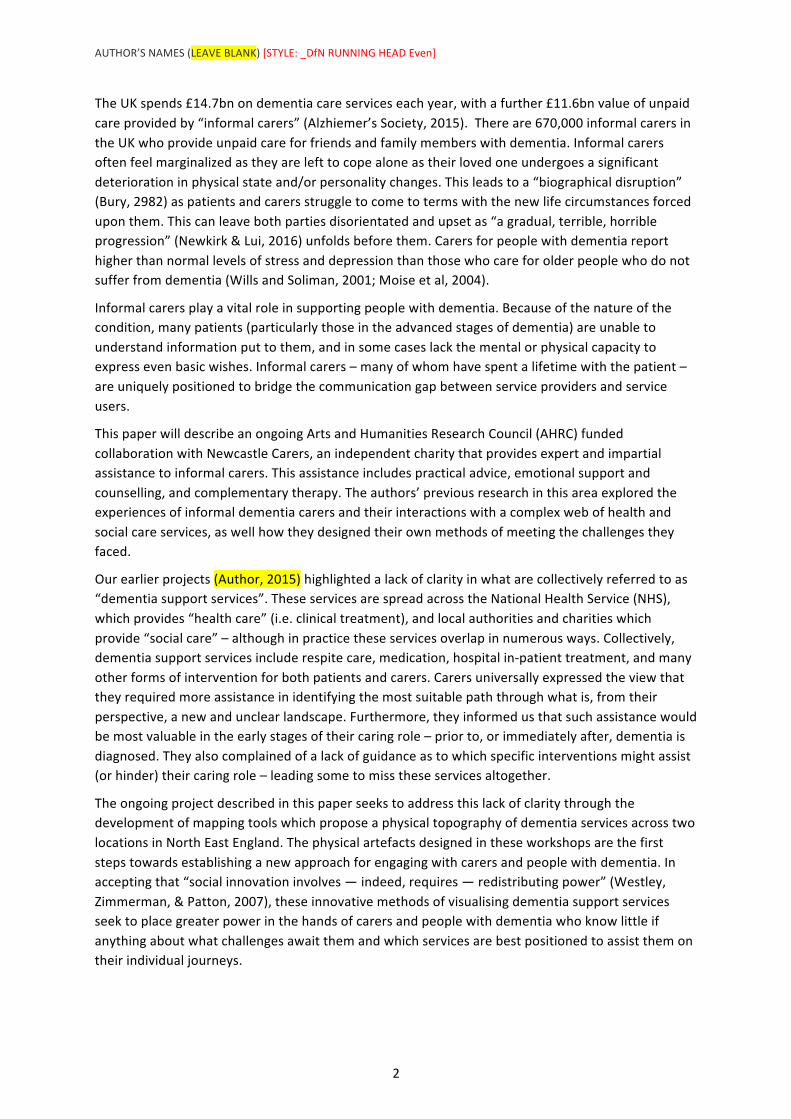
ChristianBasonoftheDanishDesignCentrevisualisedtheroleofdesigninpublicservicewithinalinearprocessofexploration,policydevelopment,implementation,andassessmentofintendedandunintendedoutcomes.Thisapproach,however,situatesdesignwithinacomplexandever-changingpoliticallandscapeof“disjointedincrementalism”(DesignCommission,2014)inwhichtheurgentneedsofserviceusersclashwiththeglacialpaceofinstitutionalchange.DesignDisruption,bycontrast,declinestofollowtraditionalmodelsofpublicservicedesign.Instead,itplacesanemphasisonactionandreflection,“trialanderror,hunchesandexperiments”(Mulganetal,2007),embracesfailureasavitalpartofthelearningprocess,andseekstodirectlyaddressasocietalchallengethroughadvocacy,provocation,andunearthingnewinsightsthatcanleadtofurtherinnovativeanddynamicinterventionsinpeoples’lives.
DesignDisruptionsharesaconceptualspacewithCriticalDesigninthatitisarguably“moreofanattitudethananythingelse,apositionratherthanamethodology”(Dunne&Raby,2014).Thetermhasbeencriticisedasapotentialhindrancewithinthefieldofdesign,an“unnecessary”(Tonkinwise,2015)orpotentially“unhelpful”qualification(Green,Rodgers,&Tennant2016).Throughoutourresearch,however,ithasofferedausefulvocabularytoestablishathemeofenergeticactivismandaspecificfocusonactionandimpact.Adoptingtheprefixof“disruption”hasassistedusinhelpingnon-designerstounderstandandbuyintotheexperimentalnatureoftheprojects.
Disruptionarises“viaanintensejourney,aformativeevent…[leadingdirectlytoa]discomfortordissatisfactionwiththeeverydaywayofworking”(Celaschi,2013).Howeveritisreached,theoverallgoalistocreateacounter-narrativeinfavourofpositivesocialandinstitutionalchange(Faud-Luke,2009)whilstrecognisingtheinherentriskthatsuchanarrativecanbemarginalised,“reducedtoexhibitionmaterialorusedtomaintainthestatusquo”(Green,Rogers,&Tennant,2016),whensubsumedwithincomplexorganisations.Thedesignermusttreadcarefullytoengageproductivelywithhealthandsocialcareorganisationswhilstretainingtheindependencetoconstructivelycritique,provoke,andchallengeestablishedwaysofdoing(CostaandKallick,1993).
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
4
Figure1.ChristianBason’svisualisationoftheprocessofservicedesign(black).Bycontrast,DesignDisruption(green)eschewsthedrawn-outpoliticalprocessofpolicydevelopmentinfavourofswiftactiontodirectlyaddresssocialchallenges.
Thisresearchaimstoofferaspacefor“highlightingpotential…transformativevisions”(Jégou,2010)withinpublicservices,wheretheever-presentpressuresofexpandinguserbasesanddwindlingfinancialresourcesmeanthat“innovationhasbecomenothinglessthanasurvivalstrategy”(Brown,2009).InGuiBonsiepe’s1997lecture“DesignbeyondDesign”,presentedattheJanvanEyckAkademie,heproposedsixvirtuesfordesignbasedonItaloCalvino’s“SixMemosfortheNextMillennium”.Bonsiepe’ssecondvirtue,“Intellectuality”,calledforamorecriticalstanceindesign.Thatis,designmustrocktheboat,critique‘whatis’andimagine‘whatcouldbe’,andcontinuallycontestthelegitimisationofestablishedpowerbases.Theworkwepresentherestrivestofulfiltheseambitions.
2.2ResearchQuestions • Howcandisruptivedesigninterventionshelpensurethatcarersandpeoplewithdementia
developagreaterunderstandingoftheoptionsavailabletothemasearlyaspossible?
• Howcanthesedesigninterventionsdevelopandremainusefultousersastheircircumstanceschange?
• Cantheseinterventionsbeofuseto,andbemaintainedby,dementiacaresupportservices?
• Canthisapproachaffectpositivechangeinhowcarersandpeoplewithdementiainteractwithdementiasupportservices?
Articletitle[STYLE:_DfNRunningheadodd]
5
3.DementiaServiceMappingProject 3.1BackgroundIn2015wewereapproachedbytheNationalHealthService(NHS)EnglandfollowingtheinceptionofitsNorthernEnglandDementiaAdvisoryGroup(NEDAG),ataskforcecomprisedofseveralNHStrusts,PublicHealthEngland,localauthorities,andcharitableservices.Werecognisedthisasanopportunitytoworkwitha“suitablegroupofpartnersand[theopportunityto]buildwiththemasetofsharedvaluesandconverginginterests”(Manzini,2015)necessaryforsuccessfulandsustainablecollaborativedesign.Weagreedtoexploretheoverlapbetweensocialservices-typicallyprovidedbycharitiesandlocalauthorities-andtheclinicalservicesoftheNHS.Inparticular,wewishedtoinvestigatethepossibilityofclarifyingapathway(oramultitudeofpathways)forpositiveinterventionswithcarersandpeoplewithdementiaatthepre-diagnosisstage,whentheytypicallyreceivelittleornosupport.
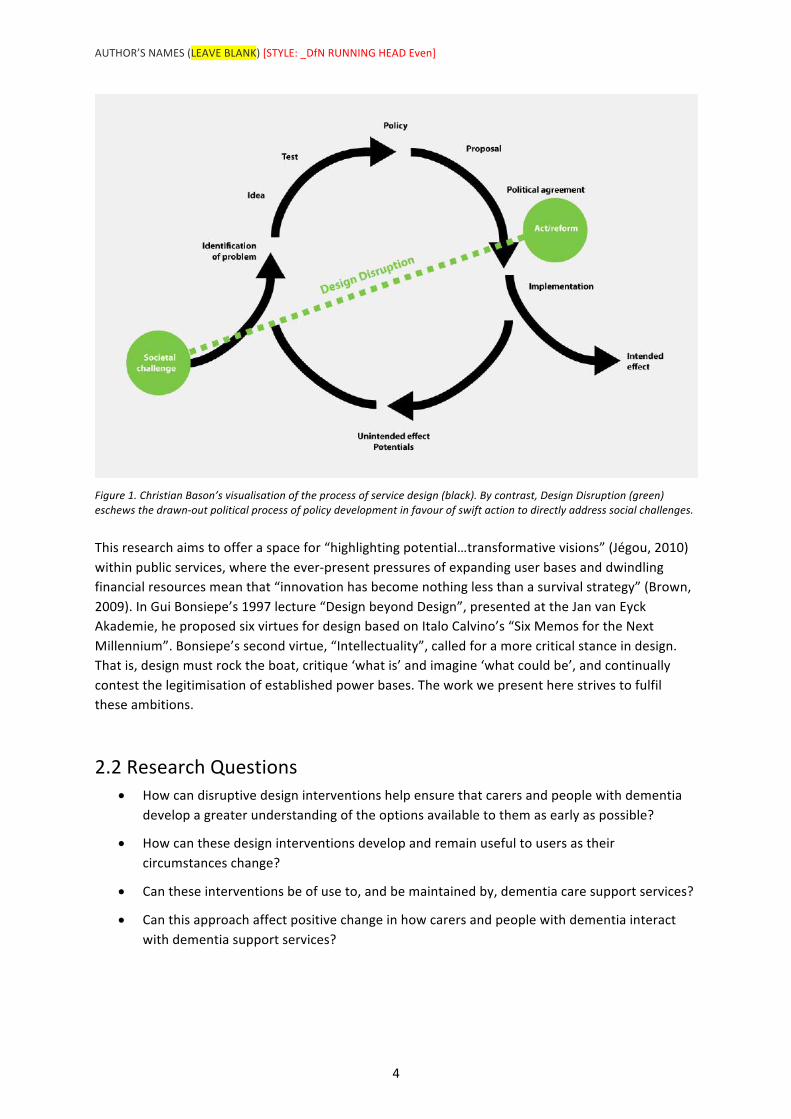
TheNationalInstituteforClinicalExcellence(NICE)publisha“DementiaOverview”-acomprehensiveandregularlyupdatedonlinesupporttoolforusebycliniciansspecialisingindementiacare.Itoutlinesbest-practicetreatmentpathwaysandoverarchingguidingprinciplesforNHSstaffinprovidingcareforpeoplewithdementia.TheNICEDementiaPathwaydoesnot,however,provideanyassistanceforthemanypeoplewithdementiaandtheircarerswhodealwiththeconditionformanyyearsbeforeadiagnosisisestablished.Bytakingstepstoidentify,intervene,andassistcarersandpatientsearlier,theNEDAGaimtomitigateorentirelyavoidcrisesinthefuture,andtherebyrelievefinancialpressureontheirservicesaswellastheemotionaltollontheserviceusers.
Figure2.DetailoftheNationalInstituteforClinicalExcellence(NICE)DementiaOverviewonlinesupporttool.
Weproposedtoexplorethepotentialforcreatingartefactsthatinvestigatedtheexperiencesofpre-diagnosiscarersandpatientsandwhethertheirgoalsareassistedbyexistingservices.WeagreedtopilotthisprojectintwoareasoftheNorthEastofEngland.ThefirstisStockton-on-Tees,whichin2014wonrecognitionforitsworkindevelopinga“DementiaFriendlyCommunity”(StocktonBoroughCouncil,2014).ThesecondisNorthTyneside,aconurbationclosetoNewcastleuponTyne,
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
6
whichhascomparativelylittleinthewayofdementiasupportservices.Separatedgeographicallybyaround35miles,thesetwoareasconsistofbroadlysimilarpopulationsize(eacharound200,000people)andage/racedemographics(OfficeforNationalStatistics,2012),whichwillallowforavalidcomparisontobedrawnbetweentheservicesavailableinthetwolocations.
ThispaperreportsonthedevelopmentoftheprojectinStockton-on-Tees,withtheNorthTynesideprojectduetocommenceinearly2017.
4.Methodology Themethodologyadoptedforthisprojectwasthatofadisruptiveapproach(seeabove)manifestedviaActionResearch(Lewin,1946),involvingasequenceofplanning,acting,observing,andreflectingontheintendedandunintendedoutcomes.Astheprojectisongoing,thismethodologyisnotaclosedcirclebutaspiral(CarrandKemis,1986)wheretheprocessofreflectiondirectlyinformsthenextstageofplanning,andsoon.WeorganisedtwoworkshopstoinvestigatethedementiaservicelandscapeinStockton-on-Tees.
Workshop1,19thOctober2016
Theparticipantsinthisfirstworkshopwere15carersandpeoplewithdementia.Thiswasaninformalsessionwhereweaskedparticipantstorespondtosimpleprobesabouttheirlives,theirhopesforthefuture,andtheirexperienceswithdementiacareservices.Whipple’s(1987)CommunityofPracticemodelespousedthat“knowledgeiscreatedandnotsimplytransferredandisconsideredtobelocatedinthe‘community’ratherthantheindividual”;likewise,theseaccumulatedresponsesprovideduswithinsightsintotheindividualexperienceswhichwerethenusedasthebasisforasemi-structuredgroupdiscussionabouttheirexperiencesandconcernsuniquetotheStocktonarea.
ThisworkshopgeneratednumerousinsightsintotheexperiencesofpeopleinStockton,including:
• Ageneralsatisfactionwiththelevelofpost-diagnosissupportreceived,butfrustrationanduncertaintypriortothis.Someparticipantsexplicitlystatedthattheyfelt“lost”whenattemptingtonavigateservicesofwhichtheyhadnopriorknowledge;
• Aconsensusthatthecarersandpatientsfeeloverwhelmedanddisorientatedwhenthepatient’sneedsrequirethemtomoveoutoftheirownhomesandintostaffedcarehomes.Theprocesswasdescribedas“labyrinthine”andallpartieswhohadexperiencedthistransitionfelttheydidnothaveavoiceinthisprocess;
• Theexperiencesofsomecarerswildlydifferedfromothers,eventhoughtheyaccessedthesameorganisations;
• Thevastmajorityofcaretakesplaceinanon-medicalcontext(suchasthefamilyhome)ratherthanamedicalcontext(suchasahospital).
• Whendescribingtheirexperiences,participantsusedavocabularywhichechoedthatofaphysicaljourney.Theyfelt“lost”,theytook“wrongturns”alonga“longanddifficultroad”,andattimesfelt“trapped”.
Articletitle[STYLE:_DfNRunningheadodd]
7
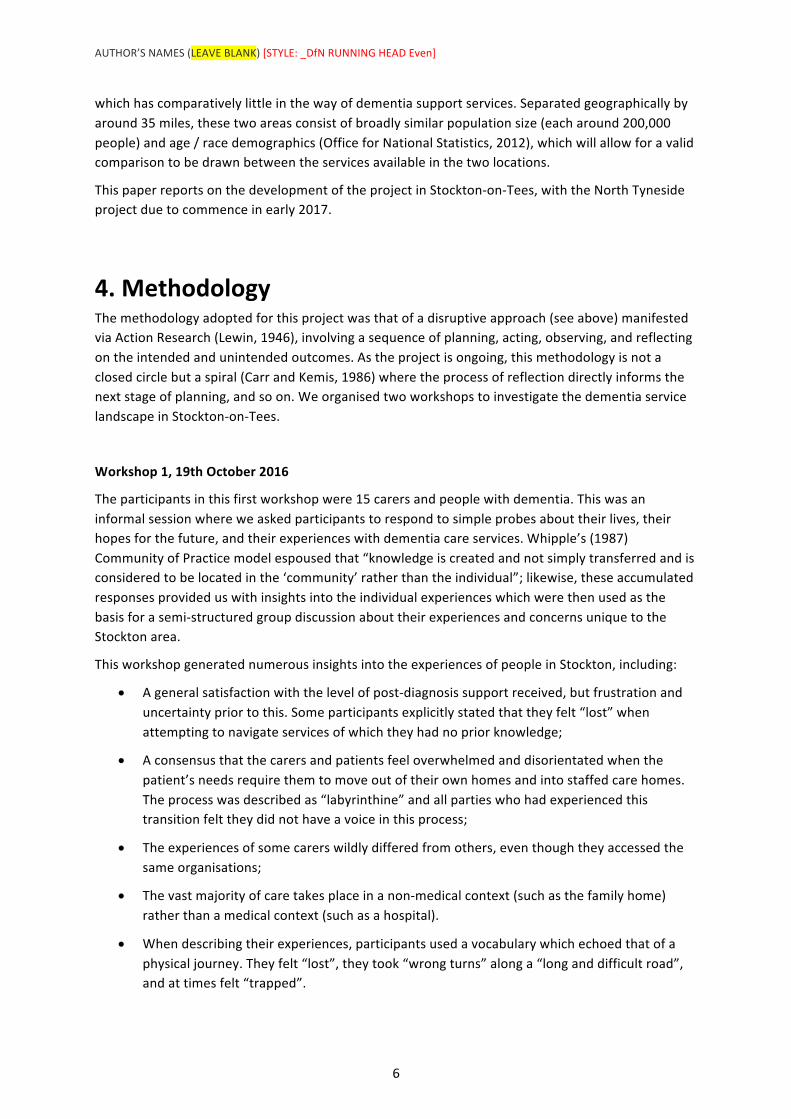
Figure3.Imagesoftheoutcomescreatedatthefirstworkshop.(right)Oneoftheresponsesofawomancaringforherhusbandwhohasdementia.Thisgivessomeindicationoftheissueswhichareimportanttothiscarer–forexample,theimportanceofstrongfamilyties,balancingherownhealththeneedsofherhusband,andherdesireenjoylifeoutsidethe“caringrole”.
Thisworkshopwasfollowedbyareflectioncycle(McNiff&Whitehead,2006)duringwhichtheauthorsconsideredtheoutcomesoftheworkshopandhowbesttousethemasthebasisforthesecondworkshopduetotakeplacethefollowingmonth.Duringthisperiodofreflection,wedistilledtheoutcomesintoeightdistinctgoalssharedbycarersandpeoplewithdementia.Thegoalswere:
• Tobehappy;
• Tofeeluseful;
• Tobeabletoplanahead;
• Toknowwhattheyareentitledto;
• Tofeellistenedto;
• Tochoosetolivethewaytheywished;
• Tohaveassistanceincopingwithcrises;
• Tolivehealthyandactivelives.
Thisledustoconsiderhowdementiaserviceproviders,whotypicallyhaveverynarrowremits,helppeopletofulfiltheseabstractgoals.Werecognisedaninterestingtensionbetweentheserviceproviders’approachoffocussingonveryspecificoutcomes,andthecomparativelyabstractnatureoftheabovegoals.ThistensionwasconsideredbyBurnsetalintheir2006REDPaper:
“Here,emotionalconsiderationsareequaltopracticalones,andthisdemandstheabilitytolookataproblemfromaperspectivethatmaybefundamentallydifferentfromthatofthebusiness-ownerorservice-provider.”
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
8
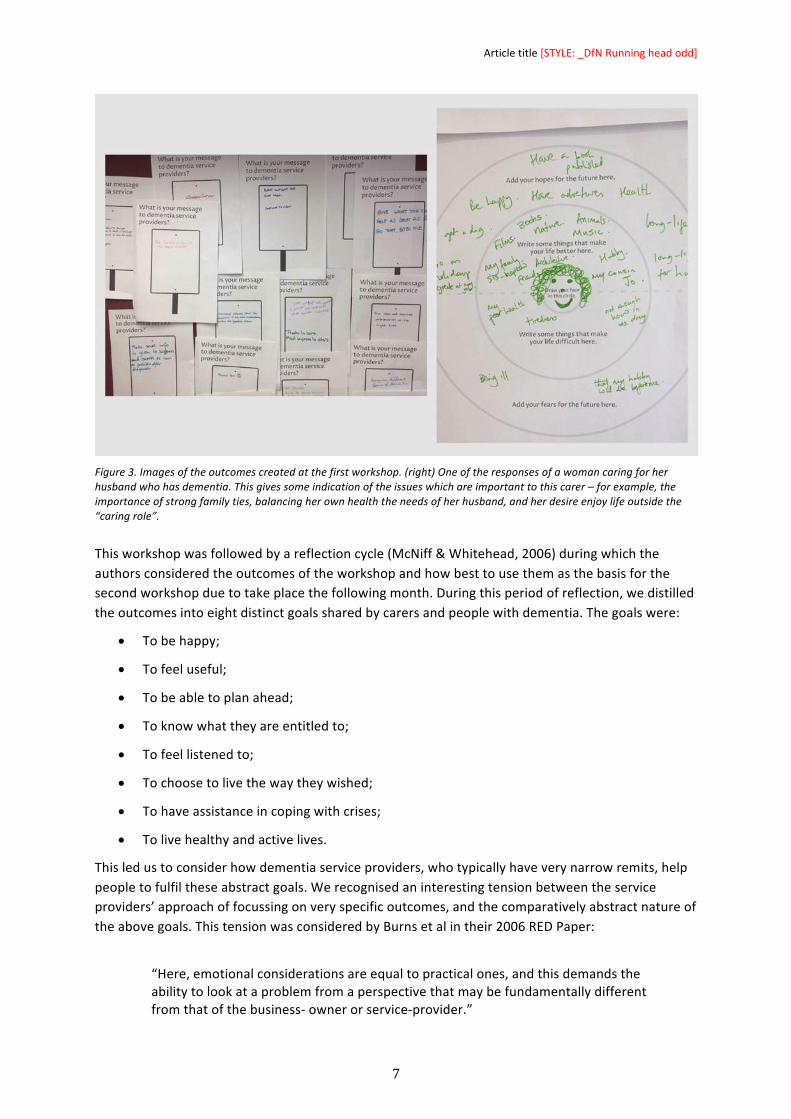
Toencouragethisnewperspective,weadoptedthefamiliarvisualdeviceofatransitmapwiththeserviceuserplacedfirmlyinthecentreoftheprocess.
Figure4.Thegoalsofpeoplewithdementiaandtheircarers,visualisedaseightdistinctpathstheycouldtake.
Workshop2,23rdNovember2016
Thissecondworkshopwasattendedby18participants,eachofwhomrepresentedanorganisationprovidingsupportfordementiapatientsandorcarers.Theywerejoinedbyhusbandandwife(whowerealsoapatientandcarerrespectively),whoalsoparticipatedinthefirstworkshop.Theyrequestedtocontinuetoparticipateinthedesignprocessandgivetheirviewsontheoutcomesproducedattheworkshop.
Weaskedtheparticipantstoconsiderthemanyinterventionseachoftheirservicesprovide-frominformationleafletstodementiacafés,employmentsupporttohealthylivingadvice–andtoplacethemonthemapaccordingtothegoalstheyhelpedusersfulfil.Eachorganisationfoundthattheirdifferentinterventionsoccupiednumerouspaths,andthustheycouldidentifythatseveralorganisationsoverlappedsignificantly,withsomepursuingsimilarinterventionswithidenticalgoals.Thishighlightedspaceforpotentialcollaborationbetweentheirservices.
Articletitle[STYLE:_DfNRunningheadodd]
9
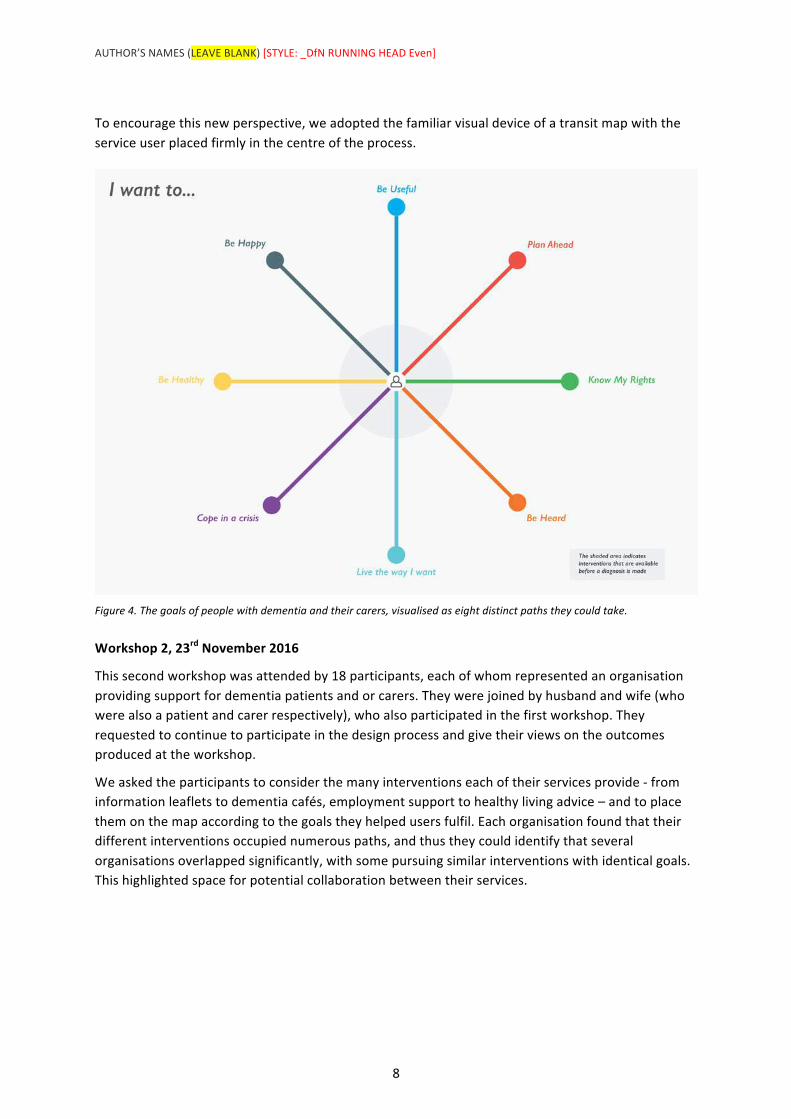
Figure5.Thecompleted“InterventionsMap”.
Pre-diagnosisserviceswerehighlightedatthecentreofthemap,allowingustofocusonthesespecificinterventionswithintheirwidercontext.Itisclearthatonlyasmallproportionofdementiaservicesprovideanyassistanceatthisstage,withthevastmajoritybeing‘passive’informationgatheringservicessuchasfactsheets,ratherthanproviding‘active’planningandassistance.Thishighlightstheuntappedpotentialforprovidingassistanceatanearlierstage.
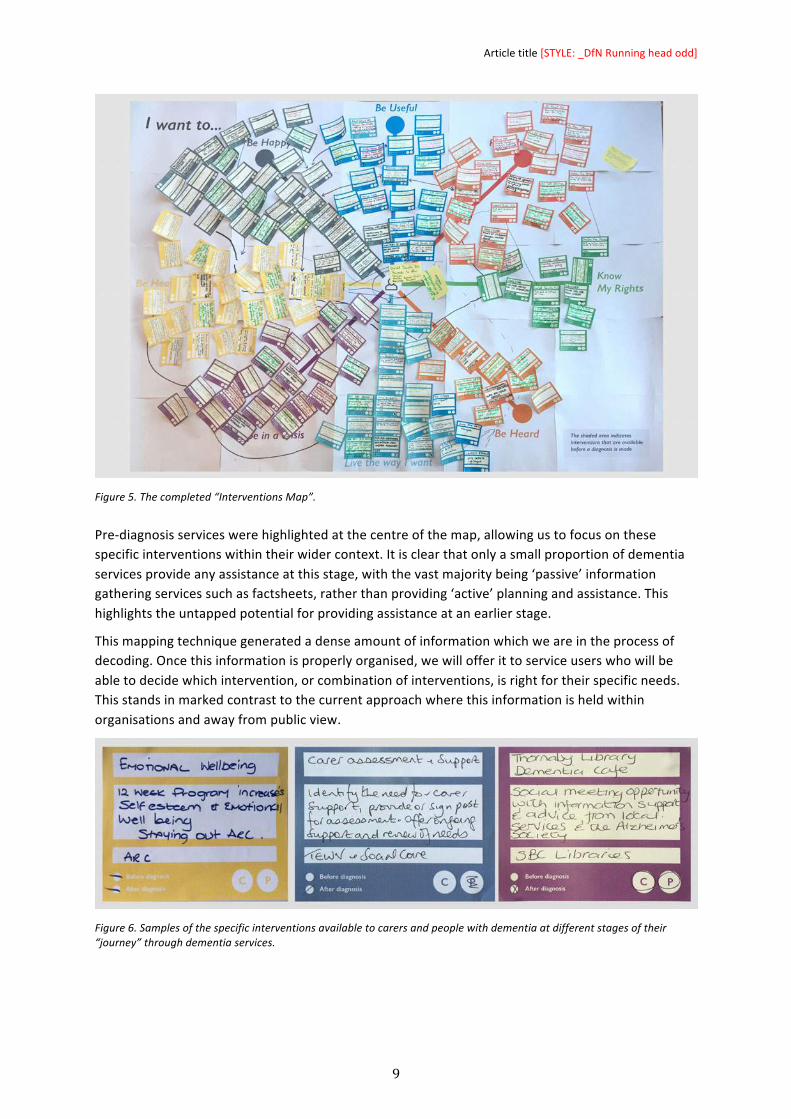
Thismappingtechniquegeneratedadenseamountofinformationwhichweareintheprocessofdecoding.Oncethisinformationisproperlyorganised,wewillofferittoserviceuserswhowillbeabletodecidewhichintervention,orcombinationofinterventions,isrightfortheirspecificneeds.Thisstandsinmarkedcontrasttothecurrentapproachwherethisinformationisheldwithinorganisationsandawayfrompublicview.
Figure6.Samplesofthespecificinterventionsavailabletocarersandpeoplewithdementiaatdifferentstagesoftheir“journey”throughdementiaservices.
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
10
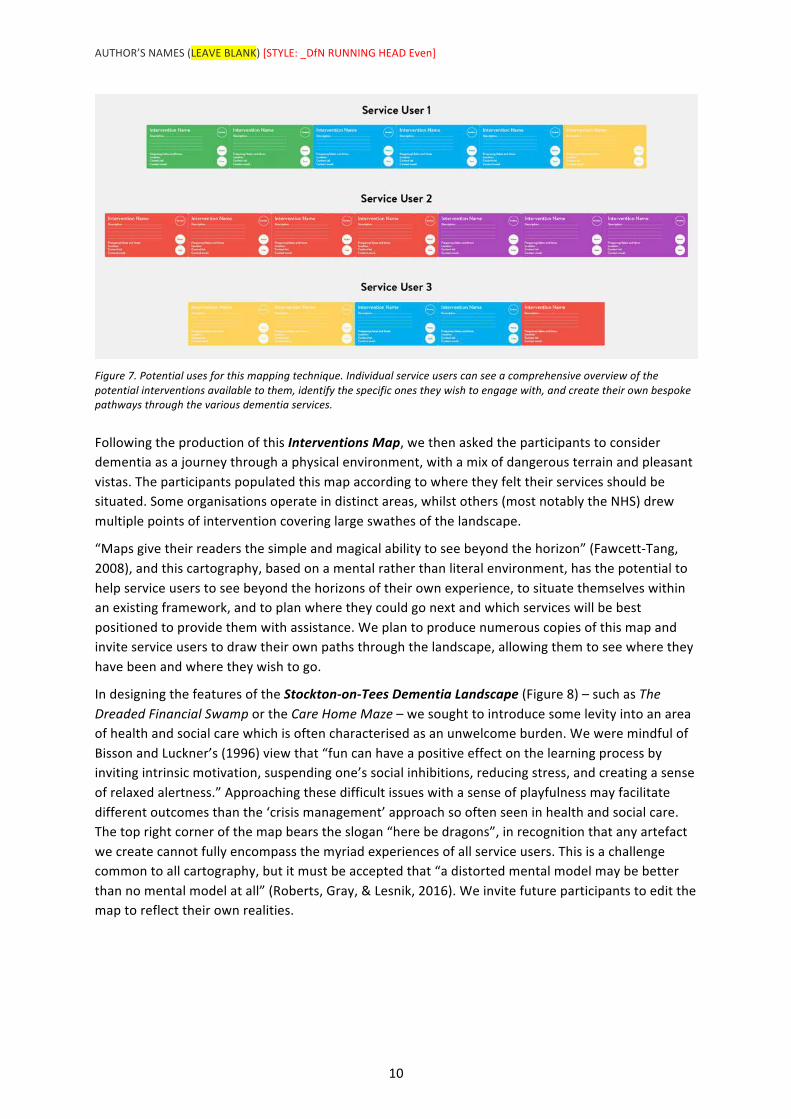
Figure7.Potentialusesforthismappingtechnique.Individualserviceuserscanseeacomprehensiveoverviewofthepotentialinterventionsavailabletothem,identifythespecificonestheywishtoengagewith,andcreatetheirownbespokepathwaysthroughthevariousdementiaservices.
FollowingtheproductionofthisInterventionsMap,wethenaskedtheparticipantstoconsiderdementiaasajourneythroughaphysicalenvironment,withamixofdangerousterrainandpleasantvistas.Theparticipantspopulatedthismapaccordingtowheretheyfelttheirservicesshouldbesituated.Someorganisationsoperateindistinctareas,whilstothers(mostnotablytheNHS)drewmultiplepointsofinterventioncoveringlargeswathesofthelandscape.
“Mapsgivetheirreadersthesimpleandmagicalabilitytoseebeyondthehorizon”(Fawcett-Tang,2008),andthiscartography,basedonamentalratherthanliteralenvironment,hasthepotentialtohelpserviceuserstoseebeyondthehorizonsoftheirownexperience,tosituatethemselveswithinanexistingframework,andtoplanwheretheycouldgonextandwhichserviceswillbebestpositionedtoprovidethemwithassistance.Weplantoproducenumerouscopiesofthismapandinviteserviceuserstodrawtheirownpathsthroughthelandscape,allowingthemtoseewheretheyhavebeenandwheretheywishtogo.
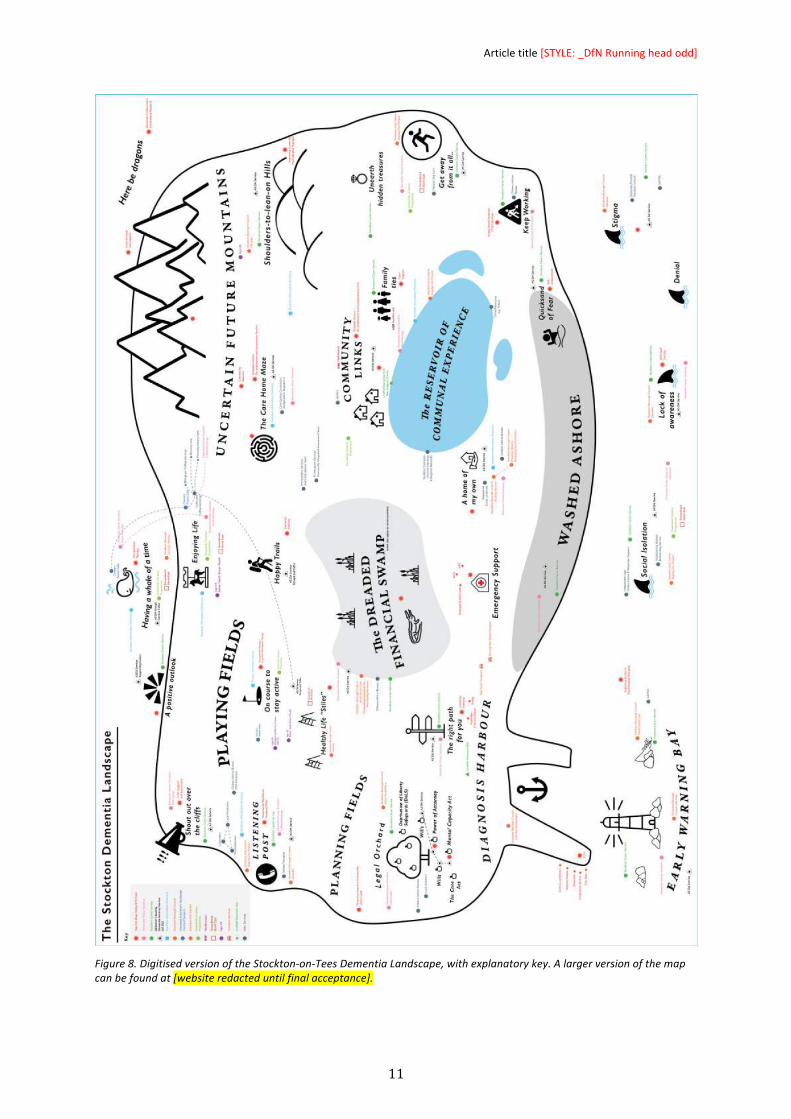
IndesigningthefeaturesoftheStockton-on-TeesDementiaLandscape(Figure8)–suchasTheDreadedFinancialSwamportheCareHomeMaze–wesoughttointroducesomelevityintoanareaofhealthandsocialcarewhichisoftencharacterisedasanunwelcomeburden.WeweremindfulofBissonandLuckner’s(1996)viewthat“funcanhaveapositiveeffectonthelearningprocessbyinvitingintrinsicmotivation,suspendingone’ssocialinhibitions,reducingstress,andcreatingasenseofrelaxedalertness.”Approachingthesedifficultissueswithasenseofplayfulnessmayfacilitatedifferentoutcomesthanthe‘crisismanagement’approachsooftenseeninhealthandsocialcare.Thetoprightcornerofthemapbearstheslogan“herebedragons”,inrecognitionthatanyartefactwecreatecannotfullyencompassthemyriadexperiencesofallserviceusers.Thisisachallengecommontoallcartography,butitmustbeacceptedthat“adistortedmentalmodelmaybebetterthannomentalmodelatall”(Roberts,Gray,&Lesnik,2016).Weinvitefutureparticipantstoeditthemaptoreflecttheirownrealities.
Articletitle[STYLE:_DfNRunningheadodd]
11
Figure8.DigitisedversionoftheStockton-on-TeesDementiaLandscape,withexplanatorykey.Alargerversionofthemapcanbefoundat[websiteredacteduntilfinalacceptance].

AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
12
5.InitialFindings/Contribution Inthisproject,wedevelopedtwoverydifferentmethodsofquicklygatheringdatatocreatephysicalmapsofdementiaserviceswithinaspecificregion.Wecollectedsignificantamountsofrawdatathroughaprocessofobservation,reflection,andswiftaction.Theoutcomescanbeinterpretedinmanywaysandfordifferentpurposes,andweareintheprocessofrefiningthehandmadeartefactsintowell-structured,understandableproductswhichcanbedistributedwidely.
Fordementiaserviceproviders,themapsofferanovelwaytovisualisetheirinterventionsinpeoples’lives,toseewheretherearegapsinthesupporttheyoffer,andtohighlightcommongroundandpotentialspacesforfuturecollaboration.Indoingso,thisprojectisasteptowardsconfronting“institutionalandprofessionalborders”(Ehn,Nilsson,&Topgaard,2014)whichmaypreventserviceusersfromreceivingtherightsupportattherighttime.Byengagingtheminacollaborative,co-designprocess,weofferedthemspaceto“jointlyexploreandarticulatetheirlatentneedsandjointlyexploreandmakesolutions”(Steed,Manschot,&DeKoning,2011)tothoseneeds.Nowthetopographyofcarehasbeenmadevisible,thereisafurtherchallengetoexplorewhetherthisresearchcanformpartofaprocessof“continuouslearningandredesigning”(Fuad-Luke,2009),orwhetheritisasinglesnapshotofalandscapethatwillinevitablyshift.
Forcarersandpeoplewithdementia,theyoffernewwaystointeractwithdementiaservices,helpthemtoplanforthefuture,andtoarticulatetheirexperiencesinnewways.Aswithallmaps,these“redescribetheworld”(Harley,2002)inwayswhichchallengetheexistingstructuresofpowerandpractice.Atthisproject’sinception,wewereaskedtoconsiderwhetherwecoulddesignapathwayforserviceusersintheveryearlystagesofdementiacare.Thesemapsreflectthelivedreality–thatthereisnosinglepathwayforeveryonetofollow–butinvitesthemtocreatetheirownpathwaystomeettheirspecificchallenges.
TheseworkshopswillberepeatedinNorthTynesideinJanuaryandFebruary2017.Oncethesemapsarecompleted,wewillbeabletodrawcomparisonsbetweenthetypeofdementiacareservicesavailableineachoftheseareas.Thismayfurtherassistserviceprovidersineachlocationtoconsidertheneedsoftheirserviceusersandthelevelofsupportthey,inturn,provide.
“Wethinkthatwe’reintheartefactbusiness,butwe’renot;we’reintheconsequencebusiness”(Chocinov,n.d.)–andthetruevalueofthesedesigninterventionscomesinwhethertheyresultinoutcomeswhicharevaluabletoallstakeholders.Wedonotproposethatthesemapsshouldreplaceface-to-facediscussions,butbeusedtoaddvaluetothemasatooltoencouragenewinsights.Wewishtoempowerdementiaserviceprovidersandtheirserviceuserstofeelabletopointtoamapandask‘andwhataboutthis…?’
Articletitle[STYLE:_DfNRunningheadodd]
13
ReferencesAuthor(2015)–namesandtitleremovedAlzheimerSociety(2014)DefiningDementia.Retreived24thOctober2015fromwww.alzheimers.org.uk/infographic(Accessed3rdFebruary2016)Bason,C.(2016)ServiceDesignasavehicleforexploringnewgeographies[Powerpointslides]Retrievedfromhttp://www.slideshare.net/servdes/keynote-opening-presentation-at-servdes-2016-christian-bason-ddcon1stJuly2016Bisson,C.andLuckner,J.,“FuninLearning:ThePedagogicalRoleofFuninAdventureEducationPerspectives”,JournalofExperientialEducation,19(2),1996,pp.108-112.Bonsiepe,G.(1999).Interface–AnApproachtoDesign,JanvanEyckAkademie,Maastricht,TheNetherlands.Brown,T.(2009).Changebydesign:Howdesignthinkingcreatesnewalternativesforbusinessandsociety.NewYork,NY:HarperCollinsPublishers.Burns,C.,Cottam,H.,Vanstone,C.,&Winhall,J.(2006).REDpaper02:TransformationDesign.Design(Vol.44).London:DesignCouncil.Bury,M.(1982).Chronicillnessasbiographicaldisruption,SociologyofHealth&Illness,Vol.4,No.2,pp.167-182Celaschi,F.,Formia,E.,&Lupo,E.(2013).Fromtrans-disciplinarytoundisciplineddesignlearning:educatingthrough/todisruption.StrategicDesignResearchJournal,6(1),1-10.Costa,A.,&Kallick,B.(1993).ThroughtheLensofCriticalFriends.EducationalLeadership,51(2),49–51.Carr,W.,&Kemmis,S.(2003).Becomingcritical:educationknowledgeandactionresearch.Routledge.ChicagoChochinov,A.1.000wordsmanifesto.RetrievedNovember01,2016,fromhttp://www.manifestoproject.it/allan-chochinov/Christensen,C.M.(1997).Theinnovator’sdilemma:Whennewtechnologiescausegreatfirmstofail.Boston,MA:HarvardBusinessSchoolPress.Christensen,C.andOverdorf,M.(2000).“MeetingtheChallengeofDisruptiveChange”,HarvardBusinessReview,Vol.78,No.2,pp.66-76.
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
14
DesignCommission."RestartingBritain2:DesignandPublicServices."AnnualReviewofPolicyDesign2.1(2014):1-10.Druker,P.(1985).InnovationandEntrepreneurship:PracticesandPrinciples.NewYork,NY:HarperandRowDunne,A.,&Raby,F.(2014)Speculativeeverything:Design,fiction,andsocialdreaming.Cambridge:TheMITPressEhn,P,Nilsson,E.M.,&Topgaard,R.(Eds.).(2014).Makingfutures:Marginalnotesoninnovation,design,anddemocracy.Cambridge,MA,UnitedStates:MITPressFuad-Luke,A.(2009).Designactivism:Beautifulstrangenessforasustainableworld.London:EarthscanPublications.Fawcett-Tang,R.(2008)Mappinggraphicnavigationalsystems.Switzerland:RotovisionGreen,M.,Rodgers,P.,&Tennant,A.(2016).DisruptingServiceDesign.Retrievedfromhttp://www.ep.liu.se/ecp/125/015/ecp16125015.pdfHarley,J.B.(2002).Thenewnatureofmaps:Essaysinthehistoryofcartography.Baltimore,MD:TheJohnsHopkinsUniversityPress.Lewin,K.(1946).Actionresearchandminorityproblems.JournalofSocialIssues,2(4),34–46.doi:10.1111/j.1540-4560.1946.tb02295.xJégou,F.(2010)“SocialInnovationsandRegionalAcupunctureTowardsSustaainability”Zhuangshi,Beijing.Retreivedon7thMarch2015fromwww.strategicdesignscenarios.net/social-innovations-and-regional-acupuncture-towards-sustainability/J.B.Harley,"TextandContextsintheInterpretationofEarlyMaps"inTheNewNatureofMaps:EssaysintheHistoryofCartography.BaltimoreandLondon:JohnHopkinsUniversityPress,2001,p.35]Manzini,E.(2015).Design,wheneverybodydesigns:Anintroductiontodesignforsocialinnovation.UnitedStates:MITPress.McNiff,J.&Whitehead,J.(2006)AllyouneedtoknowaboutActionResearch.London:SAGEPublicationsLtd.Moise,P,Schwarzinger,MandUm,M-Y(2004),DementiaCarein9OECDCountries:AComparativeAnalysis(Paris,OECDHealthWorkingPaperNo.13,OECD).Mulgan,G.,&Albury,D.(2003).Innovationinthepublicsector.Retrieved1stOctober2016fromhttp://www.sba.oakland.edu/faculty/mathieson/mis524/resources/readings/innovation/innovation_in_the_public_sector.pdf
Articletitle[STYLE:_DfNRunningheadodd]
15
Mulgan,G.,Tucker,S.,Ali,R.,&Sanders,B.(2007).Socialinnovation:whatitis,whyitmattersandhowitcanbeaccelerated.London:TheBasingstokePress.NationalInstituteforClinicalExcellence(2015)DementiaOverview.RetrievedinMarch2015fromhttps://pathways.nice.org.uk/pathways/dementiaNewkirk,B.,&Lui,R.(2016,April2).Whendementiaupendsamarriage:Insidetheemotionaljourney..Retrievedon4thNovember2016fromhttp://www.desertsun.com/story/news/health/2016/03/30/when-dementia-upends-marriage-inside-emotional-journey/82255036/OfficeforNationalStatistics(16July2012)CensusresultshowsincreaseinpopulationofNorthEast.Retreivedon1stNovember2016fromhttp://webarchive.nationalarchives.gov.uk/20160105160709/http://www.ons.gov.uk/ons/rel/mro/news-release/census-result-shows-increase-in-population-of-the-north-east/censusnortheastnr0712.htmlOfficeforNationalStatistics.(2016,November).DeathsregisteredinEnglandandwales(seriesDR):2015.Retrievedon1stDecember2016fromhttps://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredinenglandandwalesseriesdr/2015#dementia-and-alzheimer-disease-was-the-leading-cause-of-death-in-2015Rodgers,P.A.andTennant,A.,“ImprovingHealthandWellbeingthroughDisruptiveDesignInterventions”,Proceedingsofthe8thSwissDesignNetworkConference2012:“DisruptiveInteraction”,9thNovember2012,Lugano,Switzerland.Roberts,M.J.,Gray,H.,&Lesnik,J.(2016).Preferenceversusperformance:Investigatingthedissociationbetweenobjectivemeasuresandsubjectiveratingsofusabilityforschematicmetromapsandintuitivetheoriesofdesign.InternationalJournalofHuman-ComputerStudies,98,109–128.doi:10.1016/j.ijhcs.2016.06.003Scharmer,C.O.(2011).“LeadingfromtheEmergingFuture”,MindsforChange–FutureofGlobalDevelopmentCeremonytomarkthe50thAnniversaryoftheBMZFederalMinistryforEconomicCooperationandDevelopment,Berlin,November13th,2011.Steen,M.,Manschot,M.,&DeKoning,N.(2011).BenefitsofCo-designinServiceDesignProjects.InternationalJournalofDesign,5(2),53–61.Retrievedon31stJuly2016fromhttp://www.ijdesign.org/ojs/index.php/IJDesign/article/view/890StocktonBoroughCouncil(2014,January23).Stocktonachievesdementia-friendlycommunityrecognition.RetrievedOctober31st2016,fromhttps://www.stockton.gov.uk/news/2014/january/stockton-achieves-dementia-friendly-community-recognition/
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
16
Tonkinwise,C.(2015,August21).Justdesign.RetrievedAugust25,2015,fromhttps://medium.com/@camerontw/just-design-b1f97cb3996f#.cclhxdz1hUnforgettableFoundation(2015),DementiaExplainedPartOne:TheTypesandCausesofDementia(p2)Retreived4thJanuary2016fromhttp://e-unforgettable.org/p/2U5V-PO/dementia-explained-pt-1Westley,F.,Zimmerman,B.,&Patton,M.Q.(2007).Gettingtomaybe:Howtheworldischanged.Toronto:RandomHouseofCanada.Whipple,W.R."CollaborativeLearning:RecognizingItWhenWeSeeIt."AAHEBulletin(October1987):4-6.(ED289396).Wills,WandSoliman,A,(2001)“Understandingtheneedsofthefamilycarersofpeoplewithdementia”,MentalHealthReviewJournal,6,2,pp25–28.Yee,J.,&White,H.(2015).”TheGoldilocksConundrum:The‘justright’conditionsfordesigntoachieveimpactinpublicandthirdsectorprojects.”InternationalJournalofDesign,10(1),7-19.
Articletitle[STYLE:_DfNRunningheadodd]
17
AUTHOR’SNAMES(LEAVEBLANK)[STYLE:_DfNRUNNINGHEADEven]
18
AbouttheAuthors:
Author1addanauthorbiothatdescribesresearchinterestsandmainachievementsinamaximumof40words.[LEAVEBLANKUNTILFINALACCEPTANCE][_DfNAuthorBioandAcknowledgements]
Author2addanauthorbiothatdescribesresearchinterestsandmainachievementsinamaximumof40words.[LEAVEBLANKUNTILFINALACCEPTANCE]
Acknowledgements:thissectionisoptional.Youcanusethissectiontoacknowledgesupportyouhavehadforyourresearchfromyourcolleagues,student’sparticipation,internalorexternalpartners’contributionorfundingbodies.[LEAVEBLANKUNTILFINALACCEPTANCE]





























