Embed Size (px)
Citation preview
10/8/2015
1
Using EHRs to Manage Risk & Improve Quality in Long-Term
Care ( FMDA #105) Rod Baird
October 22, 2015
Disclosures
• Geriatric Practice Management, LLC - President • Developer of LTC Physician EHR software
• ECP Management, LLC - Partner • NC based Provider of LTC Physician services
• AMDA Committee Member • Public Policy & Government Affairs, QM Task Force
• CMS -2012 Innovations Advisor – LTC PCMH
• LTC MD rep. to NASL HIT Committee
[email protected] www.ltcmanagement.com
Rod Baird
2
10/8/2015
2
Acronyms Used In This Presentation • A/I/U – Acquire / Implement / Upgrade • ACO – Accountable Care Organization • APM – Alternative Payment Model • BPCI – Bundled Payment for Care Improvement
• C-CDA – Consolidated Clinical Document Architecture (content of a ‘direct’ message)
• CCM – Chronic Care Management • CEHRT – Certified EHR Technology
• CPOE – Computerized Provider Order Entry
• Direct – secure email protocol (a/k/a direct messaging)
• eCQM – electronic Clinical Quality Measure
• EHR – Electronic Health Record • EMR – Electronic Medical Record • HIE – Health Information Exchange • HISP – Health Info Service Provider
• IMO – Intelligent Medical Objects • LTPAC – Long-Term Post Acute Care
• MDS – Minimum Data Set
• MIPS – Merit Based Incentive Payment System
• MOC – Maintenance of Certification
• MSSP – Medicare Shared Savings Program
• MU – Meaningful Use
• NPP – Non Physician Provider
• ONC – Office of the National Coordinator
• PCMH – Person Centered Medical Home
• PQRS – Physician Quality Reporting System
• SGR – Sustainable Growth Rate
In the past payment was based on your written documentation
Today Payment is based on DATA created by you and others.
10/8/2015
3
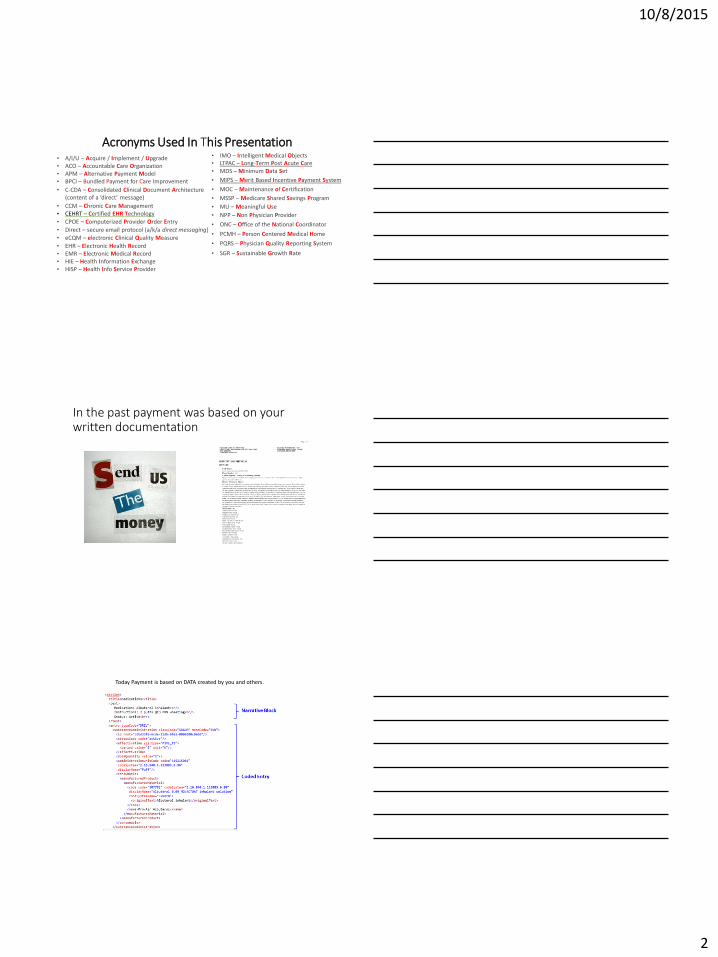
All your Future Medicare Payments are Adjusted by DATA
Electronic Health Records Are YOUR DATA
The Real Objective of today’s Program • We personally know LTPAC Medical Groups that qualified for Over $25,000,000 of
Medicaid A/I/U payments in 30+ state
• That Medicaid Payment is based on acquiring ANY Ambulatory CEHRT – demonstrating MU is not required
• Every Medicare Program assumes you are using an EHR
• Most EHRs simplify the complexities of tracking and reporting Quality Measures
• The Entry Door to the Medicaid EHR Payment Program CLOSES FOREVER at end of 2016
• The Penalties for not using CEHRT continue without end (at least through 2022)
Your text here
10/8/2015
4
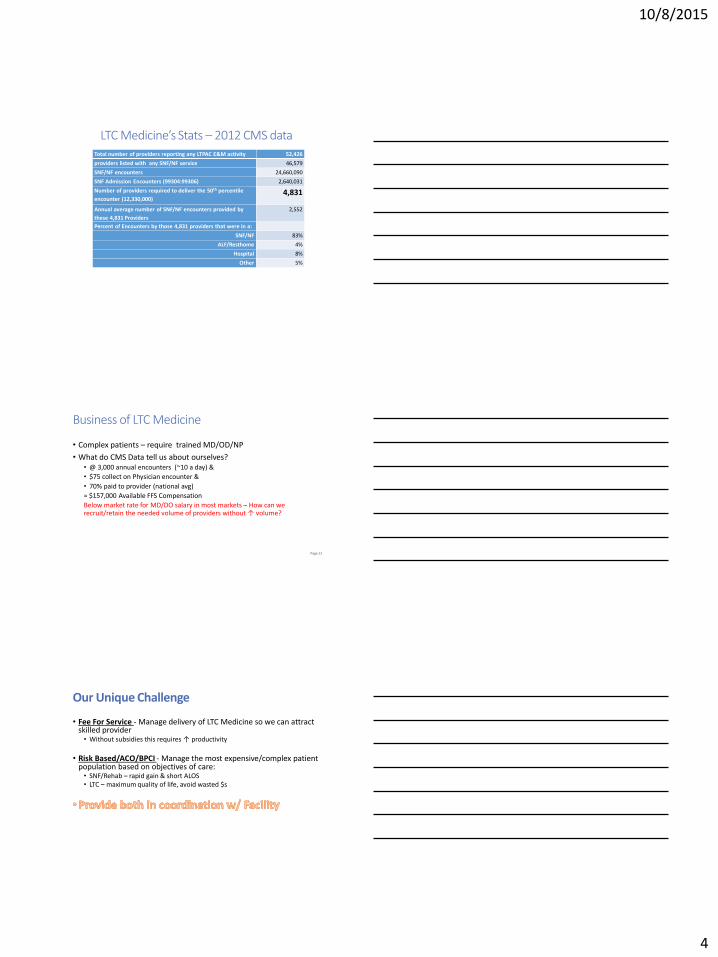
LTC Medicine’s Stats – 2012 CMS data Total number of providers reporting any LTPAC E&M activity 52,426
providers listed with any SNF/NF service 46,579
SNF/NF encounters 24,660,090
SNF Admission Encounters (99304:99306) 2,640,031
Number of providers required to deliver the 50th percentile
encounter (12,330,000) 4,831
Annual average number of SNF/NF encounters provided by
these 4,831 Providers
2,552
Percent of Encounters by those 4,831 providers that were in a:
SNF/NF 83%
ALF/Resthome 4%
Hospital 8%
Other 5%
Business of LTC Medicine
• Complex patients – require trained MD/OD/NP
• What do CMS Data tell us about ourselves? • @ 3,000 annual encounters (~10 a day) &
• $75 collect on Physician encounter &
• 70% paid to provider (national avg)
= $157,000 Available FFS Compensation
Below market rate for MD/DO salary in most markets – How can we recruit/retain the needed volume of providers without ↑ volume?
Page 12
Our Unique Challenge
• Fee For Service - Manage delivery of LTC Medicine so we can attract skilled provider • Without subsidies this requires ↑ productivity
• Risk Based/ACO/BPCI - Manage the most expensive/complex patient population based on objectives of care: • SNF/Rehab – rapid gain & short ALOS • LTC – maximum quality of life, avoid wasted $s
10/8/2015
5
Options for Our Members
•Plan to retire before the pain becomes unbearable
•Minimize PA/LTC work, work in an office setting compliant with changes
•Work for the facility or health system
•Become the leader(s) of a ‘virtual care team’
EHRs – It’s about Time
• Provider pay based on volume
• FFS payments for 3-5+ years
• CPT $ rate reductions likely
• Only Solution - higher volume??
• How to get more done?
Page 15
Can an EHR help with Time?
Paper • Benefits
• Nothing Faster at 1-4 lines
• ‘free’
• Liabilities • Rarely compliant
• Slower beyond minimal
• Fails @PQRS, VBP, MU, ACO etc
• No data or audit access
Electronic Records • Benefits
• Reusable & shareable
• MU$, PQRS, ACO, VBP
• CPOE & CDS
• Shared Quality Measures
• Liabilities • Costs $s
• Time to learn
• Longer than some paper
10/8/2015
6
Educational Objectives
1. Understand statutory requirements met by Ambulatory EHR
2. Recognize office based medical EHR shortcomings for LTPAC Medical Group
5. Importance of integration/connectivity when using a LTPAC Physician’s EHR
3. Recognize shortcomings a LTPAC Facility EHR may present for a LTPAC Physician/Medical Group
4. Understand EHR Contracting Considerations
1. Understand statutory requirements met by Ambulatory EHR
MU is a Requirement in Other Programs • ACOs (Accountable Care Organization) and APMs (Alternative
Payment Model) • Providers in the panel must use CEHRT as part of the quality metric (e.g. >50% of
ACO physicians demonstrate MU to qualify for incentive payments)
• MIPS (Merit Based Incentive Payment System) • Not applicable until beginning of 2019 • All Quality Measurement integrates with EHR eCQMs • MIPS – Combines All 3 Programs, plus ‘clinical practice activities’
#1 – Multiple CMS Programs Require Use of CEHRT
(ONC Certified EHR Technology)
• Meaningful Use (MU) requires CEHRT • Certification requires:
• Testing and approval by a Certification Body to meet ONC standards
• Certification can be full or partial • Most Facility EHRs have ‘partial’ certification (none are fully Ambulatory Certified as of 5/1/2015)
• e.g. ePrescribing, electronic Clinical Quality Measures [a version of PQRS]
• If a fully certified EHR is available in your Ambulatory Practice, use of a facility’s partially certified EHR for CPOE would be acceptable.
• CMS & ONC have 3 Stages of Certification planned. • For 2015 everyone must use a Stage 2 Certified EHR (key point to verify)
10/8/2015
7
How do you Verify CEHRT is up to date?
http://oncchpl.force.com/ehrcert/CHPLHome
Ambulatory EHR software - Can $ incentives help?
• Two Programs – Medicare & Medicaid • Dual eligible patients count as Medicaid
• Medicare for MD only, steep performance tests
• Medicaid is available if 30% of encounters are M’cd
• Medicaid pays MD and NP – attestation only year 1
• 1st year Payment typically @ $21,250/provider
• All LTC MD and NP staff potentially eligible
EHR Meaningful Use Basics
• Thanks to AMDA interventions at CMS, LTC Physicians qualify for a Medicare EHR Meaningful use Hardship Exemption.
• CRITICAL DATE – Must apply for 2015 Medicare exemption by March 31, 2015(date uncertain)
• Most LTC MD, DO, & NP (not PAs) eligible for first year State Medicaid HIT $.
• if >30% of encounters are Medicaid (Dual Eligibles w/ ‘$0 pay’ are included).
• Year 1 $ $21,250.
• Years 2-6 @ $8,500 -Requires actual MU
10/8/2015
8
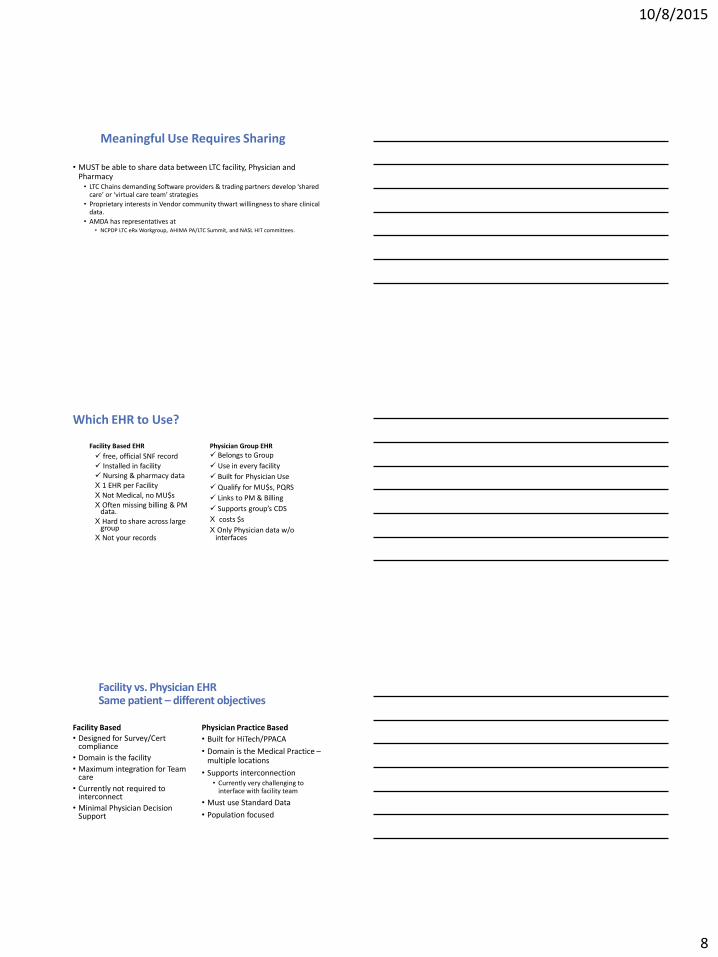
Meaningful Use Requires Sharing
• MUST be able to share data between LTC facility, Physician and Pharmacy • LTC Chains demanding Software providers & trading partners develop ‘shared
care’ or ‘virtual care team’ strategies
• Proprietary interests in Vendor community thwart willingness to share clinical data.
• AMDA has representatives at • NCPDP LTC eRx Workgroup, AHIMA PA/LTC Summit, and NASL HIT committees.
Which EHR to Use?
Facility Based EHR
free, official SNF record Installed in facility Nursing & pharmacy data X 1 EHR per Facility X Not Medical, no MU$s X Often missing billing & PM
data. X Hard to share across large
group X Not your records
Physician Group EHR
Belongs to Group
Use in every facility
Built for Physician Use
Qualify for MU$s, PQRS
Links to PM & Billing
Supports group’s CDS
X costs $s
X Only Physician data w/o interfaces
Facility vs. Physician EHR Same patient – different objectives
Facility Based • Designed for Survey/Cert
compliance
• Domain is the facility
• Maximum integration for Team care
• Currently not required to interconnect
• Minimal Physician Decision Support
Physician Practice Based
• Built for HiTech/PPACA
• Domain is the Medical Practice – multiple locations
• Supports interconnection • Currently very challenging to
interface with facility team
• Must use Standard Data
• Population focused
10/8/2015
9
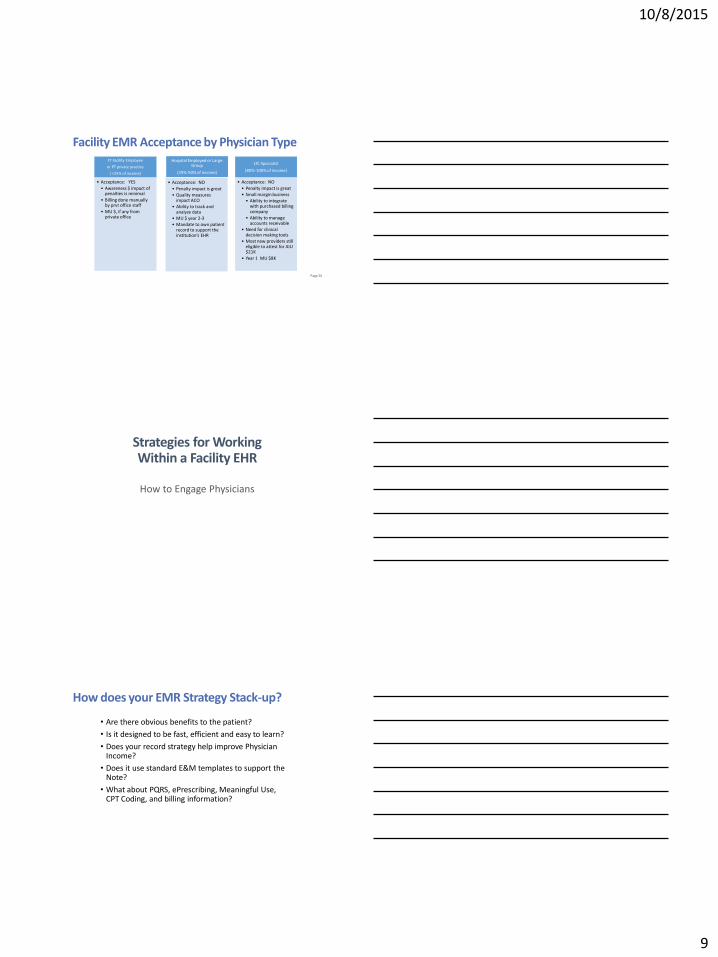
Facility EMR Acceptance by Physician Type FT Facility Employee
or PT private practice
( <25% of income)
• Acceptance: YES
• Awareness $ impact of penalties is minimal
• Billing done manually by prvt office staff
• MU $, if any from private office
Hospital Employed or Large Group
(25%-50% of income)
• Acceptance: NO
• Penalty impact is great
• Quality measures impact ACO
• Ability to track and analyze data
• MU $ year 2-3
• Mandate to own patient record to support the institution’s EHR
LTC Specialist
(80%-100% of income)
• Acceptance: NO
• Penalty impact is great
• Small margin business
• Ability to integrate with purchased billing company
• Ability to manage accounts receivable
• Need for clinical decision making tools
• Most new providers still eligible to attest for AIU $21K
• Year 1 MU $8K
Page 26
Strategies for Working Within a Facility EHR
How to Engage Physicians
How does your EMR Strategy Stack-up?
• Are there obvious benefits to the patient?
• Is it designed to be fast, efficient and easy to learn?
• Does your record strategy help improve Physician Income?
• Does it use standard E&M templates to support the Note?
• What about PQRS, ePrescribing, Meaningful Use, CPT Coding, and billing information?
10/8/2015
10
Why do Physicians resist using your EMR/EHR
• No existing LTPAC EMR/EHR applications create Value for the Attending Physician.
• No obvious benefit to patient in Physicians’ eyes
• Adds time to their day – not designed for physician use
• No economic benefit – reduces productivity
• Fails to provide fundamental features Physicians need to meet CMS mandates
• No data interface to physicians’ practices
What is Your Objective for MD Engagement?
Choose One:
• Perform Order Entry
- OR -
• Select & Electronically Approve Great Orders?
How is your MD connected?
• Community based MD doing some LTPAC work? • LTC ~ 25% of Fee for Service income
• Part of a LTC Specific practice serving multiple facilities? • LTC > 50% of Fee for Service income
• Employed by your facility? • LTC 100% of Salary
10/8/2015
11
Educational Objectives
1. Understand statutory requirements met by Ambulatory EHR
2. Recognize office based medical EHR shortcomings for LTPAC Medical Group
5. Importance of integration/connectivity when using a LTPAC Physician’s EHR
3. Recognize shortcomings a LTPAC Facility EHR may present for a LTPAC Physician/Medical Group
4. Understand EHR Contracting Considerations
2. Recognize office based medical EHR shortcomings for LTPAC Medical Group
Patients Are Stationary, Physicians Are Not; ‘Location’ of Critical Importance
• Clinical notes created by Physician/NPP alone. • Incident to charting is not legal in SNF/NF settings. Does the EHR know this?
• Need for efficient data capture in absence of ancillary staff. • Office based EHRs require Patient pre-registration and a scheduled encounter
• Orders often created by facility staff in its EHR. • How do you manage orders?
• Every Facility – potentially a new interface (usually ↑$s)
• Can Facility communicate with Physician’s EHR? • If you work in Facility’s EHR, how do you get your data into your EHR?
Educational Objectives
1. Understand statutory requirements met by Ambulatory EHR
2. Recognize office based medical EHR shortcomings for LTPAC Medical Group
5. Importance of integration/connectivity when using a LTPAC Physician’s EHR
3. Recognize shortcomings a LTPAC Facility EHR may present for a LTPAC Physician/Medical Group
4. Understand EHR Contracting Considerations
3. Recognize shortcomings a LTPAC Facility EHR may present for a LTPAC Physician/Medical Group
10/8/2015
12
For LTPAC Medicine the
EHR’s Design Features are
Critically Important
LTPAC Facility EHR’s are Designed For Different Objectives – Slide #1
• For Nursing Care management & documentation
• To satisfy SNF/NF regulatory requirements (MDS, etc.)
• Do not include PQRS Measures for MD/NPP • (but does have useful data!)
• No Facility EHR is Certified as ‘Ambulatory CEHRT’ • More are becoming ‘modularly or partially’ Certified
• Use of eCQMs is tricky (nearly impossible) with multiple EHRs. • eCQM use is ‘assumed’ by CMS for MIPS
• Records are owned by Facility not Physician • How do you get access to your notes if MD & Facility part ways?
• ’
• .
• Physician is dependent on the Facility’s IT Dept. to get your data.
• Physicians visiting multiple facilities would have records spread across multiple EHRs.
• Even with well-intentioned facility partners, record access for Payment audits is problematic
• Even if all Facility Records were CEHRT, spanning different vendors would be exceedingly difficult to achieve mandated reporting
• Each facility’s implementation of the same EHR is often different
LTPAC Facility EHR’s are Designed For Different Objectives – Slide #2
10/8/2015
13
Educational Objectives
1. Understand statutory requirements met by Ambulatory EHR
2. Recognize office based medical EHR shortcomings for LTPAC Medical Group
5. Importance of integration/connectivity when using a LTPAC Physician’s EHR
3. Recognize shortcomings a LTPAC Facility EHR may present for a LTPAC Physician/Medical Group
4. Understand EHR Contracting Considerations
4. Understand EHR Contracting Considerations
* http://www.healthit.gov/providers-professionals/ehr-implementation-steps/step-3-select-or-upgrade-certified-ehr#resource_table
• Step 1 – read ONC’s contracting guidance* for an EHR purchase. These are key issues: • Who owns your data? Verify there is a protocol for immediate access to your data at
termination. • Avoid being held Hostage - defining exit strategy in advance is key - (there may be a
fee)! • Clarify implementation services/plan. Confirm contract specifies exactly what you
will receive… who does what, what training is required, etc. • Require that the contract specifies how key considerations are addressed – e.g.
patient registration – a tricky issue if patient preregistration & scheduling is required prior to beginning the encounter.
LTC Medical Group EHR Contracting Considerations - slide #1
LTC Medical Group EHR Contracting Considerations - slide #3
• How does the provider using the EHR actually capture data for eCQMs (electronic clinical quality measures)? List the installed measures. Does the EHR Vendor support Registry Reporting for Quality Measures? Is there a cost?
• Connectivity – provisions to the Internet, facilities, labs, etc.
• Does the Vendor support a fax or secure email solution for transmitting encounter notes to the facility? What if anything is the charge for this service?
10/8/2015
14
LTC Medical Group EHR Contracting Considerations - slide #2
• How a copy of your note actually finds its way to the Facility paper or electronic chart.
• Hardware requirements (cloud based?, server purchase?, user hardware, what operating system limitations, support availability, printing capabilities, etc.)
• Software features – does it manage patients based on multiple locations? How are encounters conveyed to the facilities (get a demonstration)?
• What is the EHR’s capability to track and record PQRS measures? Do they have a strategy specific to LTC Medical Groups?
LTC Medical Group EHR Contracting Considerations - slide #4
• Interface with Billing Systems – if there is not an installed PM system with the software, what does it cost for a bidirectional interface. Why is bidirectional required? Are there any existing examples of billing system interfaces?
• What are the fees for establishing an interface with 3rd party billing systems?
• How does the practices patient/problem list get imported into the EHR?
LTC Medical Group EHR Contracting Considerations - slide #5
• If the practice has an existing EHR, what are the costs (and success rates) for importing clinical data from the old EHR and into the new one?
• General interface issues – are there interface costs to any other system? This can be quite costly in some contracts. LTPAC requires multiple interfaces (one to each facility)
• What provisions does the EHR have for supporting ePrescribing (how do orders get back to the facility?
• Enumerate all add-on costs – Dragon, IMO, etc. How are 3rd party fees handled?
10/8/2015
15
Educational Objectives
1. Understand statutory requirements met by Ambulatory EHR
2. Recognize office based medical EHR shortcomings for LTPAC Medical Group
5. Importance of integration/connectivity when using a LTPAC Physician’s EHR
3. Recognize shortcomings a LTPAC Facility EHR may present for a LTPAC Physician/Medical Group
4. Understand EHR Contracting Considerations
5. Importance of integration/connectivity when using a LTPAC Physician’s EHR
The Biggest Challenge – Getting Connected
• In 2015 ‘Connectivity’ is a concept in most markets, not reality
• Dumping Data into an HIE is not connectivity • You have to leave your EHR and hunt for patient Data - ??
• Look for either: • HISP – directly connects providers (like email), or • Partial Integration with Facility’s EHR
• (e.g. PointClick, Matrix, AmericanHealth-Tech, HealthMedx, etc.)
Are Your Facilities On-Board? • Enlist your Facility As a Partner – explain the benefits of your EHR use
• Legible, Accessible, and Timely Notes • Patient Summaries are standard features – benefit to PR for facility? • Reduces Staff Clerical Time • Supports Transitions of Care back to Community and PCP • Enables connecting to ACOs & other provider Networks
• Internet Connectivity is often a Challenge
• Ask for access to dedicated WiFi.
• Facility EHR vendor is a Partner for Connectivity
• Many Facilities don’t have fully enabled interfaces or on-site IT Staff • Finding a Vendor Contact can be a major challenge
10/8/2015
16
Nursing Facility Chains Want Solutions Read Their White Paper
http://www.ahcancal.org/facility_operations/hit/Documents/2013-06-12%20CIOC-NEC_EHR_WhitePaper_FINAL.pdf
‘Virtual Care Teams’ = ‘Shared Care’
ePrescribing - Most Important Integration For Patients’ Benefit
• ePrescribing standardizes Medication lists for Physician, Facility, & Pharmacy
• DHHS-OIG; Feb., 2014 • Adverse Events in SNFs
• During Aug., 2011 • 22% of patients in sample had adverse event • Additional 11% suffered harm • 1/3 of all events were Medication Related
10/8/2015
17
Connectivity & Integration
• Use an EHR as a standalone application for E&M notes & PQRS reporting.
• Receive Patient Census Messages from Facility EHR/EMR • File your encounter notes at facility electronically • Send Transition of Care documents at Discharge to community PCP
• Share CPOE for ePrescribing, Labs, Consultations • Receive data created by Facility RNs to improve your care and satisfy MU requirements
to avoid Medicare Penalties and earn Medicaid MU $s
Start with Paying Yourself • Take advantage of Medicaid EHR incentives in your
state – If you are >30% Medicaid (Dual Eligible Patients count!) you can receive $21,250 upon executing a contract
• Shop wisely – all solutions are not equal. Check with ONC Website to verify Certification.
• Avoid Penalties from Medicare – claim a hardship exemption
• Verify your EHR supports PQRS reporting
Understand your Own Workflow • Require Vendor to walk-you through their models and verify EVERY step
works in your practice • Remember some EHRs require a Front Desk, Patient Preregistration & scheduling
• How do your Charges flow to Billing?
• Verify process for Note distribution to EACH facility – automatic vs. manual
• Can your Partners manage your patients/see your schedule w/o support?
• Remember, you are not stationary, workflow needs to support moving from one facility to another
10/8/2015
18
EHR Implementation is a Team Effort
• Success requires full support of the majority of the group • A few naysayers can poison the well
• Every implementation will have potholes on road to Success
• Plan in extra time – if implementation is quicker Celebrate!
• Try to enlist facilities as collaborators
Reference Materials •How to Implement an EHR – http://healthit.gov/providers-professionals/ehr-implementation-steps/step-1-assess-your-practice-readiness
•Regional Extension Centers - http://healthit.gov/providers-professionals/get-ehr-implementation-support
•Medicaid EHR Incentive Program – The Basics http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/MedicaidStateInfo.html
• 2015 EHR hardship exemption application http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/paymentadj_hardship.html
Quality Reporting 2015-2019
The View from 10,000 feet
10/8/2015
19
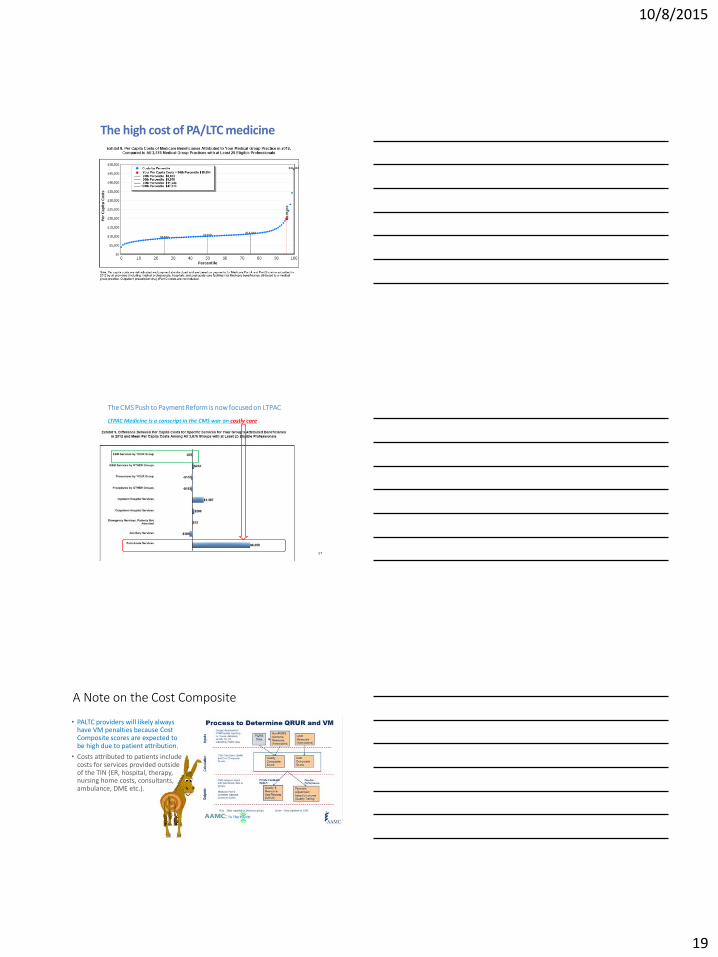
The high cost of PA/LTC medicine
The CMS Push to Payment Reform is now focused on LTPAC LTPAC Medicine is a conscript in the CMS war on costly care
57
A Note on the Cost Composite
• PALTC providers will likely always have VM penalties because Cost Composite scores are expected to be high due to patient attribution.
• Costs attributed to patients include costs for services provided outside of the TIN (ER, hospital, therapy, nursing home costs, consultants, ambulance, DME etc.).
10/8/2015
20
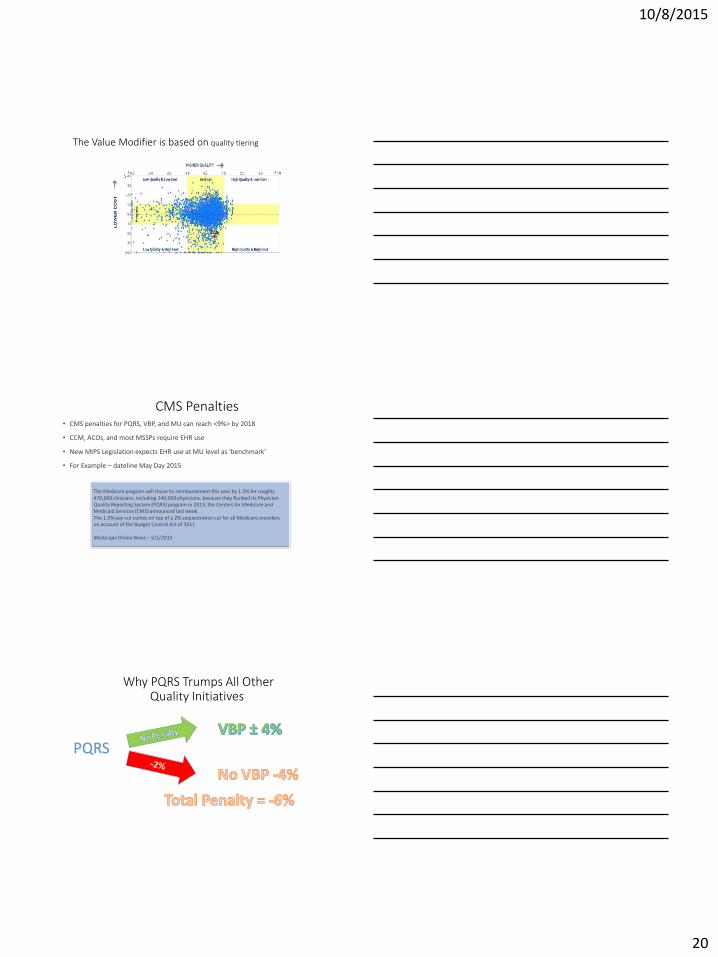
The Value Modifier is based on quality tiering
CMS Penalties • CMS penalties for PQRS, VBP, and MU can reach <9%> by 2018
• CCM, ACOs, and most MSSPs require EHR use
• New MIPS Legislation expects EHR use at MU level as ‘benchmark’
• For Example – dateline May Day 2015
The Medicare program will shave its reimbursement this year by 1.5% for roughly 470,000 clinicians, including 240,000 physicians, because they flunked its Physician Quality Reporting System (PQRS) program in 2013, the Centers for Medicare and Medicaid Services (CMS) announced last week. The 1.5% pay cut comes on top of a 2% sequestration cut for all Medicare providers on account of the Budget Control Act of 2011 Medscape Online News – 5/1/2015
Why PQRS Trumps All Other Quality Initiatives
PQRS
10/8/2015
21
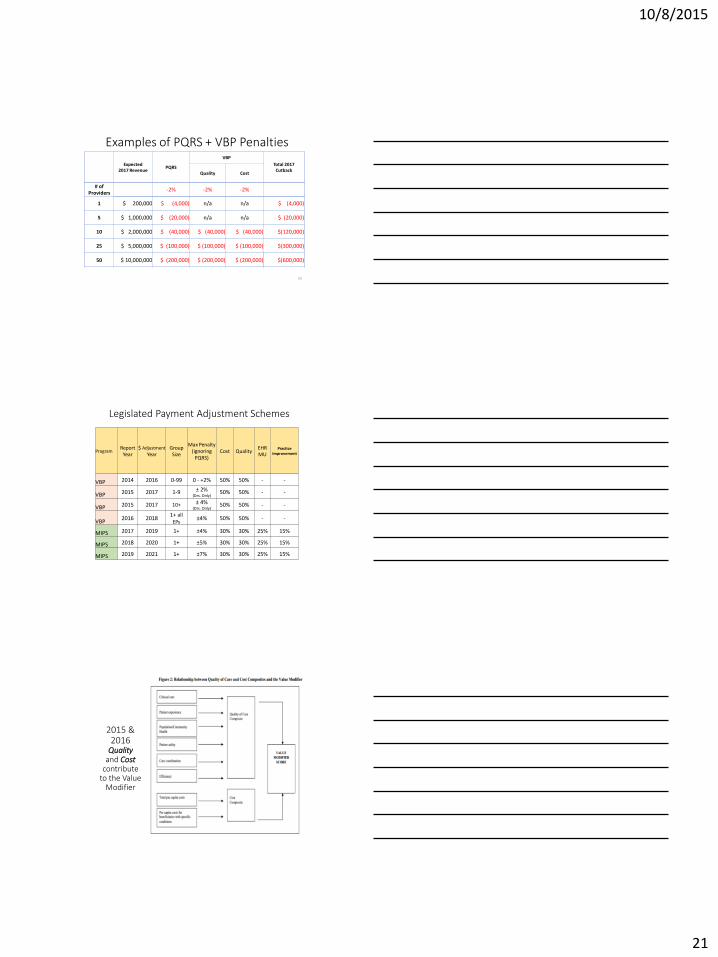
Examples of PQRS + VBP Penalties
Expected 2017 Revenue
PQRS
VBP
Total 2017 Cutback
Quality Cost
# of Providers
-2% -2% -2%
1 $ 200,000 $ (4,000) n/a n/a $ (4,000)
5 $ 1,000,000 $ (20,000) n/a n/a $ (20,000)
10 $ 2,000,000 $ (40,000) $ (40,000) $ (40,000) $(120,000)
25 $ 5,000,000 $ (100,000) $ (100,000) $ (100,000) $(300,000)
50 $ 10,000,000 $ (200,000) $ (200,000) $ (200,000) $(600,000)
62
Legislated Payment Adjustment Schemes
Program Report
Year $ Adjustment
Year Group
Size
Max Penalty (ignoring
PQRS) Cost Quality
EHR MU
Practice Improvement
VBP 2014 2016 0-99 0 - +2% 50% 50% - -
VBP 2015 2017 1-9 ± 2% (Drs. Only)
50% 50% - -
VBP 2015 2017 10+ ± 4% (Drs. Only)
50% 50% - -
VBP 2016 2018
1+ all
EPs ±4% 50% 50% - -
MIPS 2017 2019 1+ ±4% 30% 30% 25% 15%
MIPS 2018 2020 1+ ±5% 30% 30% 25% 15%
MIPS 2019 2021 1+ ±7% 30% 30% 25% 15%
2015 & 2016
Quality and Cost
contribute to the Value
Modifier
10/8/2015
22
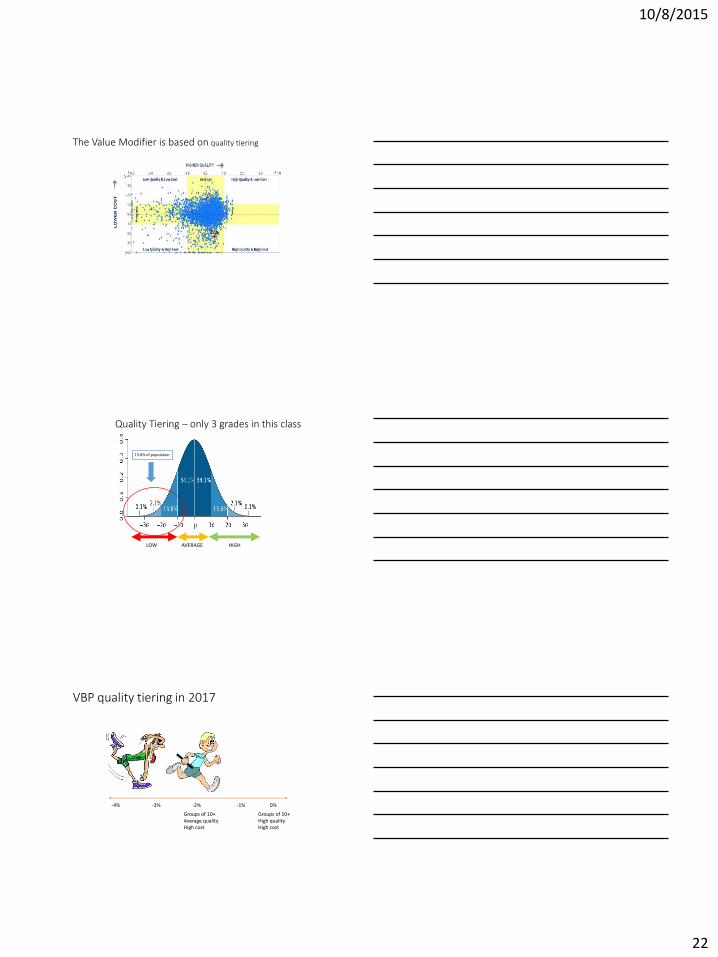
The Value Modifier is based on quality tiering
15.8% of population
LOW
Quality Tiering – only 3 grades in this class
AVERAGE HIGH
VBP quality tiering in 2017
COST
-4% -3% -2% -1% 0%
Groups of 10+ Average quality High cost
Groups of 10+ High quality High cost
10/8/2015
23
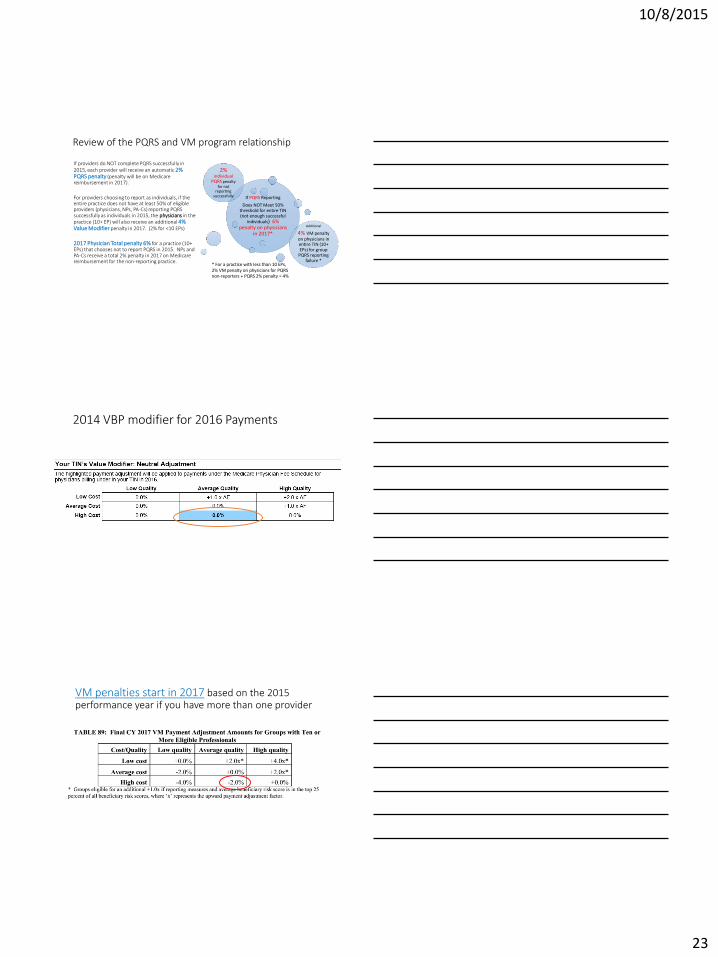
Review of the PQRS and VM program relationship
If providers do NOT complete PQRS successfully in 2015, each provider will receive an automatic 2% PQRS penalty (penalty will be on Medicare reimbursement in 2017).
For providers choosing to report as individuals, if the entire practice does not have at least 50% of eligible providers (physicians, NPs, PA-Cs) reporting PQRS successfully as individuals in 2015, the physicians in the practice (10+ EP) will also receive an additional 4% Value Modifier penalty in 2017. (2% for <10 EPs)
2017 Physician Total penalty 6% for a practice (10+ EPs) that chooses not to report PQRS in 2015. NPs and PA-Cs receive a total 2% penalty in 2017 on Medicare reimbursement for the non-reporting practice.
If PQRS Reporting
Does NOT Meet 50% threshold for entire TIN (not enough successful
individuals) 6% penalty on physicians
in 2017*
2% individual
PQRS penalty for not
reporting successfully
Additional
4% VM penalty on physicians in entire TIN (10+ EPs) for group
PQRS reporting failure *
* For a practice with less than 10 EPs, 2% VM penalty on physicians for PQRS non-reporters + PQRS 2% penalty = 4%
2014 VBP modifier for 2016 Payments
VM penalties start in 2017 based on the 2015 performance year if you have more than one provider
10/8/2015
24
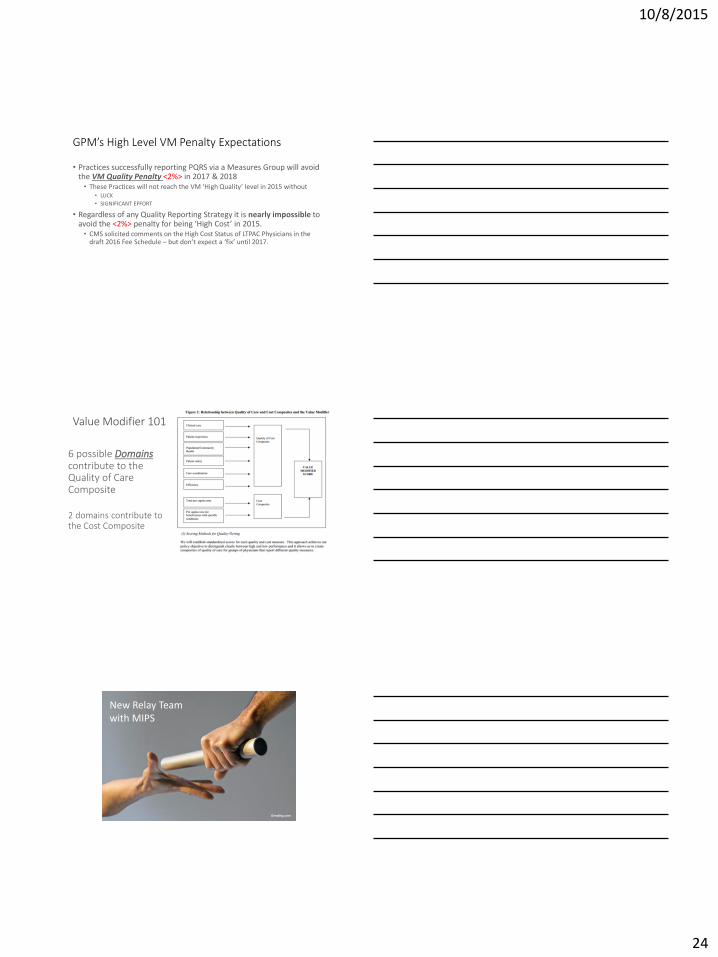
GPM’s High Level VM Penalty Expectations
• Practices successfully reporting PQRS via a Measures Group will avoid the VM Quality Penalty <2%> in 2017 & 2018 • These Practices will not reach the VM ‘High Quality’ level in 2015 without
• LUCK
• SIGNIFICANT EFFORT
• Regardless of any Quality Reporting Strategy it is nearly impossible to avoid the <2%> penalty for being ‘High Cost’ in 2015. • CMS solicited comments on the High Cost Status of LTPAC Physicians in the
draft 2016 Fee Schedule – but don’t expect a ‘fix’ until 2017.
6 possible Domains contribute to the Quality of Care Composite
2 domains contribute to the Cost Composite
Value Modifier 101
Oreablog.com
New Relay Team with MIPS
10/8/2015
25
2017 – MIPS Scoring Begins 2019 – MIPS Payment Adjustments WEIGHTING OF CATEGORIES
• COST – 30%
• QUALITY – 30%
• MEANINGFUL USE – 25%
• PRACTICE IMPROVEMENT – 15%
CMS Regualtions imply that scores in each category are hierarchial (every individual element adds/subtracts value.
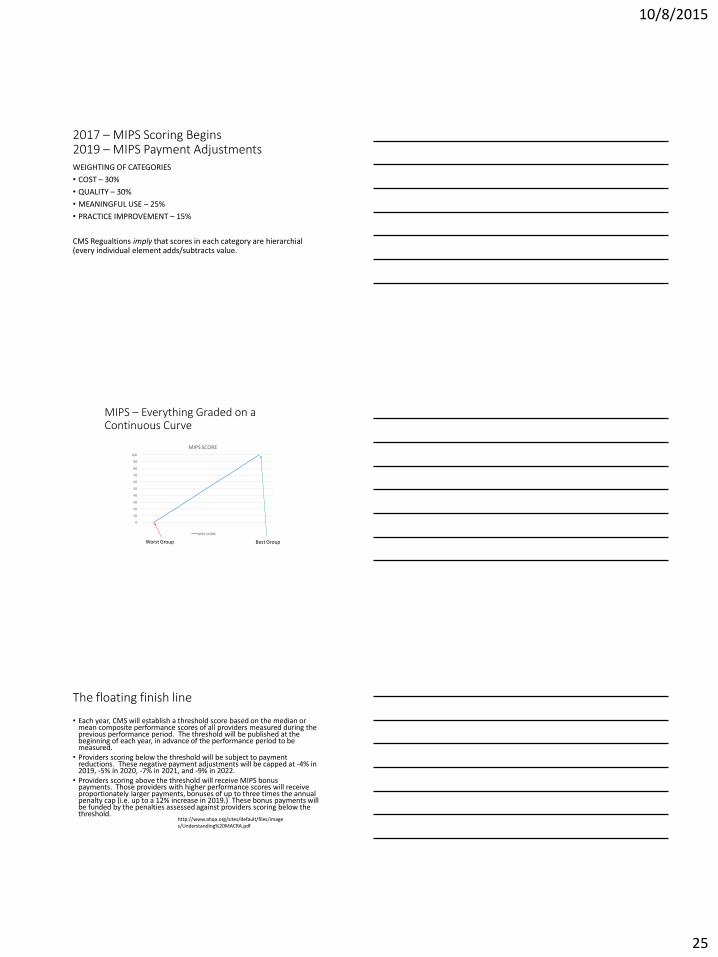
MIPS – Everything Graded on a Continuous Curve
0
10
20
30
40
50
60
70
80
90
100
MIPS SCORE
MIPS SCORE
Worst Group Best Group
The floating finish line
• Each year, CMS will establish a threshold score based on the median or mean composite performance scores of all providers measured during the previous performance period. The threshold will be published at the beginning of each year, in advance of the performance period to be measured.
• Providers scoring below the threshold will be subject to payment reductions. These negative payment adjustments will be capped at -4% in 2019, -5% in 2020, -7% in 2021, and -9% in 2022.
• Providers scoring above the threshold will receive MIPS bonus payments. Those providers with higher performance scores will receive proportionately larger payments, bonuses of up to three times the annual penalty cap (i.e. up to a 12% increase in 2019.) These bonus payments will be funded by the penalties assessed against providers scoring below the threshold.
http://www.ahqa.org/sites/default/files/images/Understanding%20MACRA.pdf
10/8/2015
26
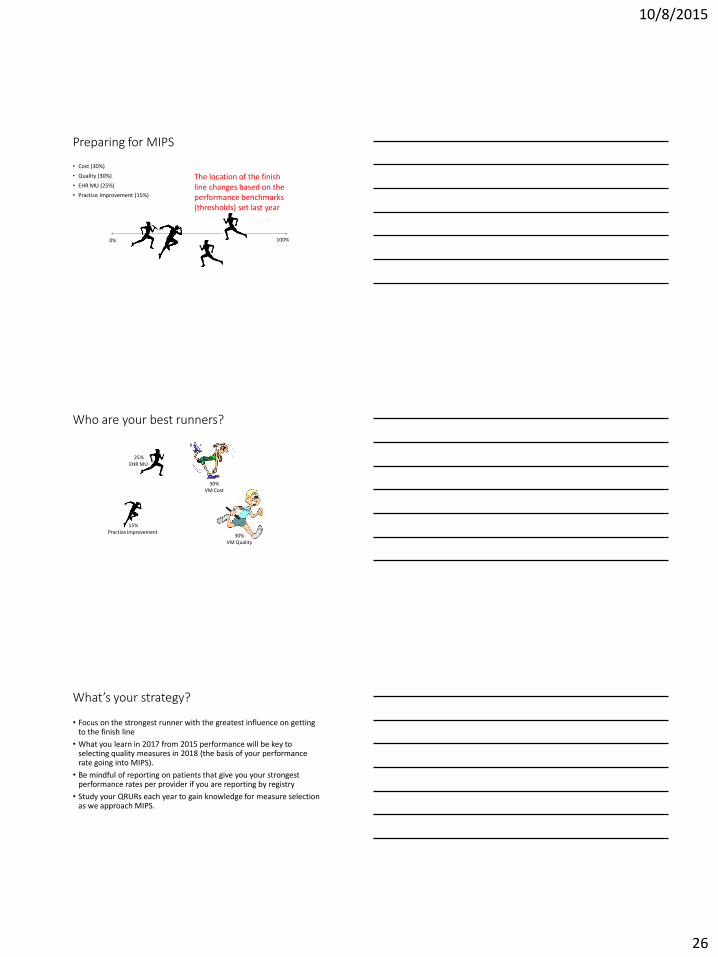
Preparing for MIPS
• Cost (30%)
• Quality (30%)
• EHR MU (25%)
• Practice Improvement (15%)
0% 100%
The location of the finish line changes based on the performance benchmarks (thresholds) set last year
Who are your best runners?
COST 25% EHR MU
15% Practice Improvement
30% VM Cost
30% VM Quality
What’s your strategy?
• Focus on the strongest runner with the greatest influence on getting to the finish line
• What you learn in 2017 from 2015 performance will be key to selecting quality measures in 2018 (the basis of your performance rate going into MIPS).
• Be mindful of reporting on patients that give you your strongest performance rates per provider if you are reporting by registry
• Study your QRURs each year to gain knowledge for measure selection as we approach MIPS.
10/8/2015
27
Strategies to Implement now!
• QUALITY – to be discussed at Lunch Break-Out Session. • QRUR Reports are the bible for Quality – too bad they are written in
иероглифический
• COST – Plan for MIPS, VBP is lost cause! • HCC – code all the ACUITY Possible (covered in ICD-10)
• Hospitalization Rates – under MIPS any improvement is beneficial. This is when ‘CARE MANAGEMENT’ counts.
• PRACTICE IMPROVEMENT – T/B/D in final rule
• MEANINGFUL USE – Interface Strategy (PCC, etc)
Groups in an Alternate Payment Model are not subject to MIPS • APMs include ACOs, MSSP, PCMH, etc.
• BPCI is a MSSP but regulations unclear on how it applies
• APM participants have +5% higher fee schedule • Percent of revenue covered in APM increases each year
• All APM programs include Quality and Cost today. • Assume that MU will become part of regulations in future to align with MIPS.
MIPS and AMPs are Endurance Events, not sprints!
10/8/2015
28
QUESTIONS
?
10/8/2015
1
Confidential ©MDI Achieve 2013
Focus on Outcomes: Using EHRs to Manage Risk &
Improve Quality in Long-Term Care
Denise Wassenaar, RN, MS, LNHA October 22, 2015
Confidential ©MDI Achieve 2013
1. What is your credential?
A. Physician
B. Advanced Practice Nurse
C. Physician Assistant
D. Registered Nurse
E. Pharmacist
F. Directors of Nursing
G. Allied medical professional
H. Nursing home administrator
I. Other
Question
Confidential ©MDI Achieve 2013
1. Discuss The Impending Changes To Healthcare Delivery and
Reimbursement
2. Describe the role of outcome management within the changing
reimbursement paradigm
3. Explain expectations in the use of EHR data in quality reporting
requirements
Objectives
10/8/2015
2
Confidential ©MDI Achieve 2013
New Regulations
Affecting Reimbursement
& Quality
Manage Outcomes Manage Quality
Interoperability Data analytics
Focus on Three Areas
Confidential ©MDI Achieve 2013
We always overestimate the
change that will occur in
the next two years and
underestimate the change
that will occur in the next
ten years.
- Bill Gates
5
Confidential ©MDI Achieve 2013
Objective 1
Discuss The Impending Changes To Healthcare
Delivery and Reimbursement
6
New Regulations Affecting Reimbursement & Quality

10/8/2015
3
Confidential ©MDI Achieve 2013
1. Clinical Outcomes will be part of the foundation for
future reimbursement.
A.True
B.False
Question
Confidential ©MDI Achieve 2013
1. Clinical Outcomes will be part of the foundation for
future reimbursement.
A.True
B.False
Question
Confidential ©MDI Achieve 2013
What will it look like?
The Future of Healthcare Reimbursement
Volume
• Fragmented providers and payments
• No uniform quality
• Fees for volume
• Demand increasing
Value
• Collaboration, connectivity
• Clinical, financial data, analysis
• Optimize outcomes
• Accountable care
10/8/2015
4
Confidential ©MDI Achieve 2013
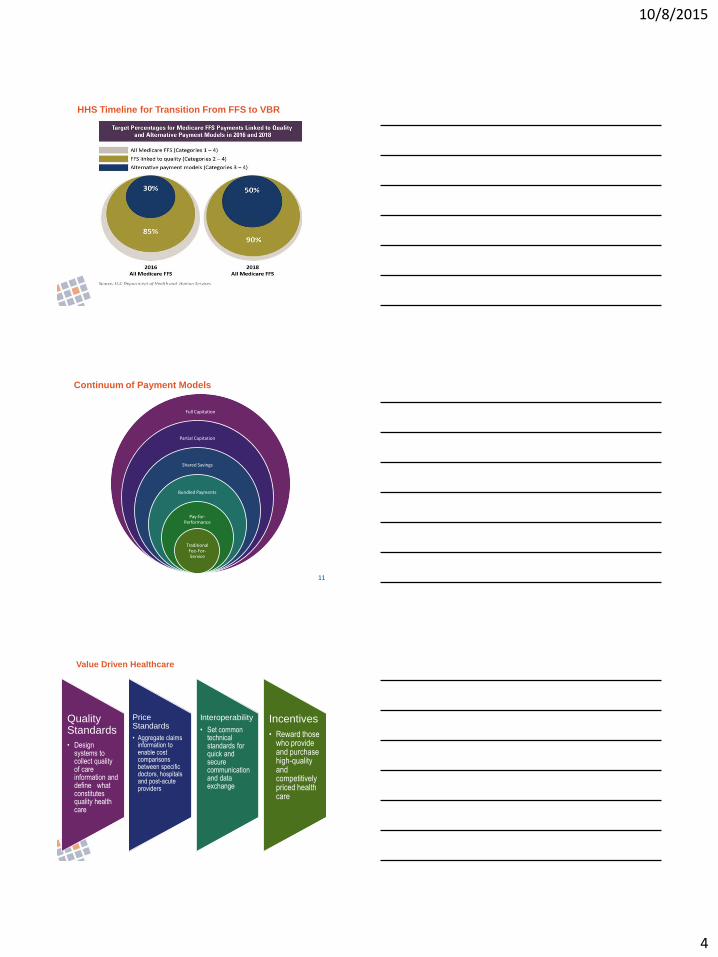
HHS Timeline for Transition From FFS to VBR
Full Capitation
Partial Capitation
Shared Savings
Bundled Payments
Pay-for-Performance
Traditional Fee-For-Service
Continuum of Payment Models
11
Confidential ©MDI Achieve 2013
Quality Standards
• Design systems to collect quality of care information and define what constitutes quality health care
Price Standards
• Aggregate claims information to enable cost comparisons between specific doctors, hospitals and post-acute providers
Interoperability
• Set common technical standards for quick and secure communication and data exchange
Incentives
• Reward those who provide and purchase high-quality and competitively priced health care
Value Driven Healthcare
10/8/2015
5
Confidential ©MDI Achieve 2013
Outcome Driven Care
IMPACT Act
ACOs
VBP BPCI
CMS Quality
Measures
Outcome Driven Care
Confidential ©MDI Achieve 2013
Illustrate Outcome Management using Data Analytics
• Case:
•Facility Hospital Readmission rate is greater than the national level at 30%
•The facility goal is 15%
Confidential ©MDI Achieve 2013
Hospital Readmission rate is an outcome measure of which
Regulation?
A. IMPACT Act
B. VBP
C.New Proposed CMS Quality Measures
D.All the above
Question
10/8/2015
6
Confidential ©MDI Achieve 2013
Hospital Readmission rate is an outcome measure of which
Regulation?
A. IMPACT Act
B. VBP
C.New Proposed CMS Quality Measures
D.All the above
Question
Confidential ©MDI Achieve 2013
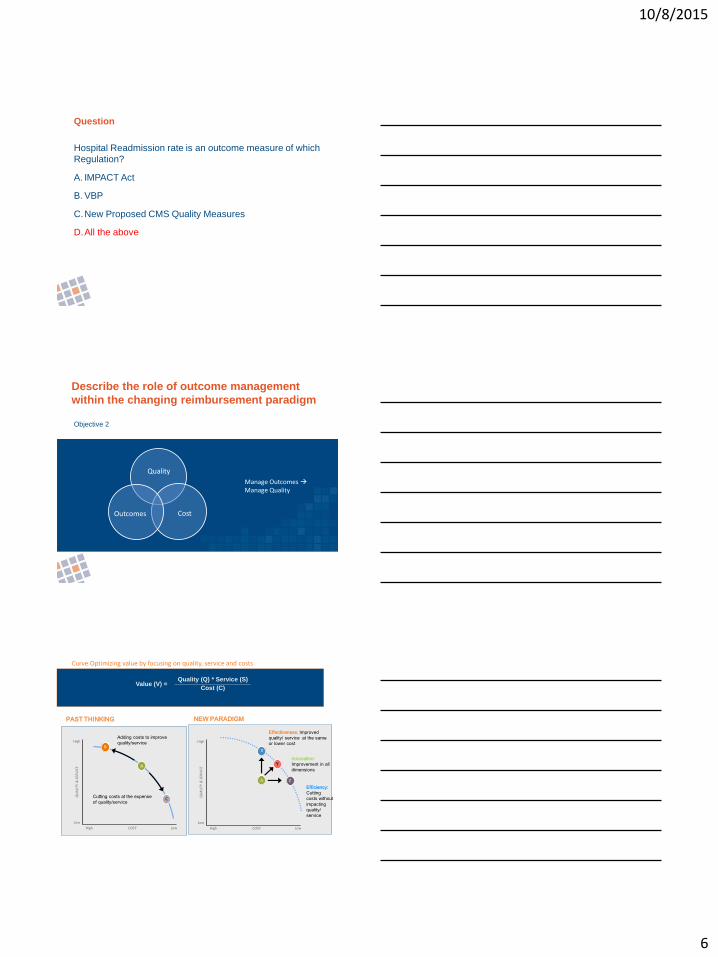
Objective 2
Describe the role of outcome management
within the changing reimbursement paradigm
Manage Outcomes Manage Quality
Quality
Cost Outcomes
Curve Optimizing value by focusing on quality, service and costs
Value (V) = Quality (Q) * Service (S)
Cost (C)
A
X
Y
Z
QU
ALI
TY &
SER
VIC
E
High
Low
Low High COST
Adding costs to improve
quality/service
Cutting costs at the expense
of quality/service
B
A
C
QU
ALI
TY &
SER
VIC
E
High
Low
Low High COST
Effectiveness: Improved
quality/ service at the same
or lower cost
Innovation:
Improvement in all
dimensions
Efficiency:
Cutting
costs without
impacting
quality/
service
PAST THINKING NEW PARADIGM
10/8/2015
7
Confidential ©MDI Achieve 2013
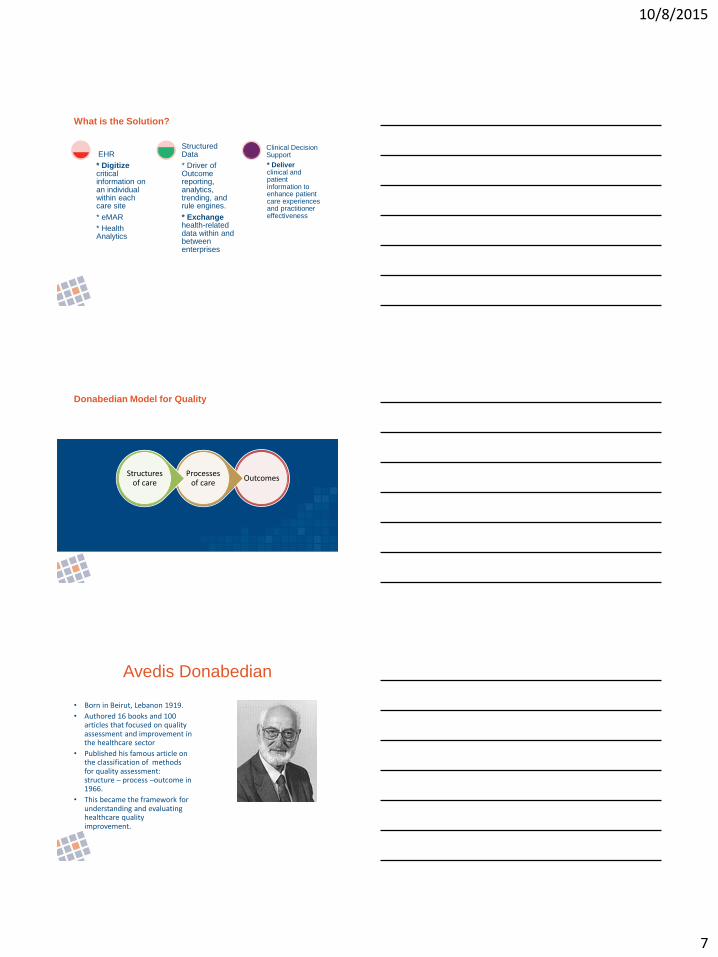
* Digitize critical information on an individual within each care site
* eMAR
* Health Analytics
EHR
* Driver of Outcome reporting, analytics, trending, and rule engines.
* Exchange health-related data within and between enterprises
Structured Data
* Deliver clinical and patient information to enhance patient care experiences and practitioner effectiveness
Clinical Decision Support
What is the Solution?
Confidential ©MDI Achieve 2013
Donabedian Model for Quality
Outcomes Processes
of care Structures
of care
Confidential ©MDI Achieve 2013
Avedis Donabedian
• Born in Beirut, Lebanon 1919.
• Authored 16 books and 100 articles that focused on quality assessment and improvement in the healthcare sector
• Published his famous article on the classification of methods for quality assessment: structure – process –outcome in 1966.
• This became the framework for understanding and evaluating healthcare quality improvement.
10/8/2015
8
Confidential ©MDI Achieve 2013
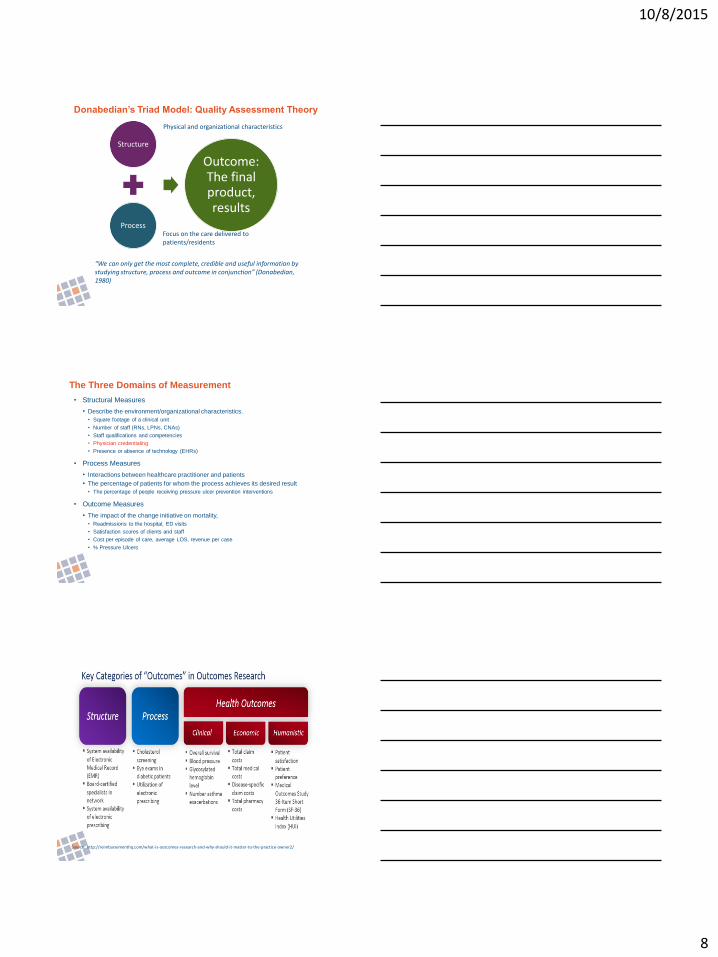
Donabedian’s Triad Model: Quality Assessment Theory
“We can only get the most complete, credible and useful information by studying structure, process and outcome in conjunction” (Donabedian, 1980)
Structure
Process
Outcome: The final product, results
Physical and organizational characteristics
Focus on the care delivered to patients/residents
Confidential ©MDI Achieve 2013
• Structural Measures
• Describe the environment/organizational characteristics.
• Square footage of a clinical unit
• Number of staff (RNs, LPNs, CNAs)
• Staff qualifications and competencies
• Physician credentialing
• Presence or absence of technology (EHRs)
• Process Measures
• Interactions between healthcare practitioner and patients
• The percentage of patients for whom the process achieves its desired result
• The percentage of people receiving pressure ulcer prevention interventions
• Outcome Measures
• The impact of the change initiative on mortality,
• Readmissions to the hospital, ED visits
• Satisfaction scores of clients and staff
• Cost per episode of care, average LOS, revenue per case
• % Pressure Ulcers
The Three Domains of Measurement
Confidential ©MDI Achieve 2013 Source: http://reimbursementhq.com/what-is-outcomes-research-and-why-should-it-matter-to-the-practice-owner2/
10/8/2015
9
Confidential ©MDI Achieve 2013
Staffing during times of fall is an example of:
A. Structure
B. Process
C.Outcome
Applying the Donebedian Framework to Managing
Readmissions: Question
Confidential ©MDI Achieve 2013
Staffing during times of fall is an example of:
A. Structure
B. Process
C.Outcome
Applying the Donebedian Framework to Managing
Readmissions: Question
Confidential ©MDI Achieve 2013
Adherence to a fall risk protocol is an example of:
A. Structure
B. Process
C.Outcome
Applying the Donebedian Framework to Managing
Readmissions: Question
10/8/2015
10
Confidential ©MDI Achieve 2013
Adherence to a fall risk protocol is an example of:
A. Structure
B. Process
C.Outcome
Applying the Donebedian Framework to Managing
Readmissions: Question
Confidential ©MDI Achieve 2013
Objective 3
Explain expectations in the use of EHR data in quality
reporting requirements
Interoperability Data analytics
Confidential ©MDI Achieve 2013
Learning high risk patients
Quality Compliance
Learning which patients are ”motivated”
Sharing health information
Ways to use technology for data analytics and quality
10/8/2015
11
Confidential ©MDI Achieve 2013
Interoperability
• “INTEROPERABILITY”:
– the ability of different
information technology
systems and software
applications to:
• communicate,
• exchange data, and
• use the information that
has been exchanged.
Confidential ©MDI Achieve 2013
• Data with a high degree of organization
• Searchable using algorithms
Structured Data
Confidential ©MDI Achieve 2013
Structured Data
Interoperability Now what?
10/8/2015
12
Confidential ©MDI Achieve 2013
• The process by which an organization manages large amounts of
data, extracting pertinent information, and turning that information
into knowledge upon which actions can be taken.
• Becoming the norm rather than the exception.
What is Business Intelligence?
Confidential ©MDI Achieve 2013
Measure
Analysis Insight
Plan
Business Intelligence
Confidential ©MDI Achieve 2013
Improved performance based upon timely and accurate information
Elimination of guesswork
Expedited decision making
Early visibility of changes:
Improved outcomes
Enhanced compliance
Benefits of BI
36
10/8/2015
13
Confidential ©MDI Achieve 2013
1
Best Care Practices
24th Annual Conference
Using EHRs to Manage Risk &
Improve Quality in Long-Term Care
Thursday, October 22, 2015
2:30 p.m. – 5:45 p.m.
Gregory A. Chaires, Esq. Board Certified in Health Law
Chaires, Brooderson & Guerrero, P.L.
283 CRANES ROOST BLVD., SUITE 165
ALTAMONTE SPRINGS, FLORIDA 32701
(407) 834-2777
www.chlawyers.com
Session Overview
Electronic health care/ medical
recordkeeping certainly has its challenges.
The onset of issues and hurdles associated
with electronic medical records will be
discussed. It is hopeful that participants
will become more informed about
potential pitfalls so to facilitate risk
prevention as it relates to electronic
documentation.
Topics for discussion:
- Relevant Law
- Purpose
- Meaningful Use
- Benefits of EHR
- Patient care
- Incentives
- Penalties
- Practical Issues with Electronic Recordkeeping
- Risk Prevention
2
Relevant Law
Why are we here?
Pursuant to the American Recovery and
Reinvestment Act of 2009 (“ARRA”), as of
January 1, 2014, all public and private
healthcare providers and other eligible
professionals (EP) must have adopted and
demonstrated “meaningful use” of electronic
medical records (EMR) in order to maintain
their existing Medicaid and Medicare
reimbursement levels.
EHR vs. EMR
EHR is certainly more comprehensive than
EMR. With an EMR, a patient’s medical
history from one provider or practice is at
issue. However, the goal of the federal
mandate for EHR is significant. EHR are
built to reach out beyond the health
organization that collected and compiled the
patient information.
3
What is “Meaningful Use?”
As defined by HealthIT.gov, “Meaningful use” is using
certified EHR technology to
Improve quality, safety, efficiency, and reduce health
disparities
Engage patients and family
Improve care coordination, and population and public
health
Maintain privacy and security of patient health
information
The goal…
It is hoped that meaningful use compliance
will result in:
• Better clinical outcomes
• Improved population health outcomes
• Increased transparency and efficiency
• Empowered individuals
• More robust research data on health
systems.
From healthit.gov
Stage 1: Meaningful use criteria focus on:
Stage 2: Meaningful use criteria focus on:
Stage 3: Meaningful use criteria focus on:
Electronically capturing health information in a standardized format
More rigorous health information exchange (HIE)
Improving quality, safety, and efficiency, leading to improved health outcomes
Using that information to track key clinical conditions
Increased requirements for e-prescribing and incorporating lab results
Decision support for national high-priority conditions
Communicating that information for care coordination processes
Electronic transmission of patient care summaries across multiple settings
Patient access to self-management tools
Initiating the reporting of clinical quality measures and public health information
More patient-controlled data Access to comprehensive patient data through patient-centered HIE
Using information to engage patients and their families in their care
Improving population health
4
On March 20, 2015, the proposed rule for Stage 3 of the Medicare and
Medicaid Electronic Health Record Incentive Programs went on
display. It was published in the Federal Register on March 30, 2015
and the comment period will close on May 29, 2015. It is intended for
the rule to provide more flexibility and to simplify requirements for
providers by focusing upon advanced use of EHRs and eliminating
irrelevant requirements.
To view the proposed rule, visit:
https://www.federalregister.gov/articles/2015/03/30/2015-06612/2015-
edition-health-information-technology-health-it-certification-criteria-
2015-edition-base
healthit.gov
Benefits
How can EHRs help me as a
provider?
Improve provider care by having patient health
information available in one place
Facilitate efficient and appropriate decisions regarding
patient care.
– Built-in safeguards against adverse events
– Clinical reminders and alerts
– Improved communication of patient information
– Support provider decision-making
– Condition-specific order sets
– Focused patient data reports/summaries
– Documentation templets
5
Eligible Professional Core Objectives
Computerized Physician Order Entry (CPOE) for Medication, Laboratory and Radiology Orders
D1 - Improve Quality, Safety, Efficiency
e-Prescribing (eRx) D1 - Improve Quality, Safety, Efficiency
Record Demographics D1 - Improve Quality, Safety, Efficiency
Record Vital Signs D1 - Improve Quality, Safety, Efficiency
Record Smoking Status D1 - Improve Quality, Safety, Efficiency
Clinical Decision Support Rule D1 - Improve Quality, Safety, Efficiency
Patient Ability to Electronically View, Download & Transmit (VDT) Health Information D2 -
Engage Patients & Family
Clinical Summaries D2 - Engage Patients & Family
Protect Electronic Health Information D5 - Ensure Privacy & Security for Personal Health
Information
Clinical Lab - Test Results D1 - Improve Quality, Safety, Efficiency
Patient Lists D1 - Improve Quality, Safety, Efficiency
Preventative Care D1 - Improve Quality, Safety, Efficiency
Patient-Specific Education Resources D2 - Engage Patients & Families
Medication Reconciliation D3 - Improve Care Coordination
Summary of Care D3 - Improve Care Coordination
Immunization Registries D4 - Improve Public & Population Health
Use Secure Electronic Messaging
From healthit.gov
Did you know?
The ARRA includes financial incentives for
healthcare providers who prove meaningful
use of electronic health records (EHR).
There are two EHR Incentive Programs. CMS oversees the Medicare Program, whereas State Medicaid agencies manage Medicaid Incentive Program. (see healthit.gov)
Medicare EHR Incentive Program Medicaid EHR Incentive Program
Run by CMS Run by Your State Medicaid Agency
Maximum incentive amount is $44,000 Maximum incentive amount is $63,750
Payments over 5 consecutive years Payments over 6 years, does not have to be consecutive
Payment adjustments will begin in 2015 for providers who
are eligible but decide not to participate
No payment adjustments for providers who are only
eligible for the Medicaid program
Providers must demonstrate meaningful use every year to
receive incentive payments.
In the first year providers can receive an incentive
payment for adopting, implementing, or upgrading EHR
technology. Providers must demonstrate meaningful use in
the remaining years to receive incentive payments.
6
To determine if you are eligible to
participate in the incentive programs,
please visit:
http://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentiveProgram
s/MedicaidStateInfo.html
Helpful Links
For information regarding
EHR Incentive programs, visit
http://www.healthit.gov/provi
ders-professionals/ehr-
incentive-programs
REMEMBER!
Covered entities under HIPAA are required
to conduct a risk assessment of their
healthcare organization to ensure the CE is
compliance with HIPAA safeguards.
Information regarding risk assessment is
available at:
http://www.healthit.gov/providers-
professionals/security-risk-assessment
7
Penalties
What if I don’t comply?
If EP’s have not implemented EMR/EHR
systems and demonstrated meaningful use,
such providers will have a 1% reduction in
Medicare reimbursements. It is anticipated
that rates of reduction will rise annually
thereafter.
Don’t forget HIPAA
and breach!
The Breach Notification Rule
Requires covered providers to promptly notify individuals and the
Secretary of the HHS of the loss, theft, or certain other
impermissible uses or disclosures of unsecured PHI.
Covered providers must also promptly notify the Secretary of HHS
if there is any breach of unsecured protected health information if
the breach affects 500 or more individuals.
Covered providers must notify the media if the breach affects more
than 500 individuals of a State or jurisdiction
8
More than forty states have passed their own
information and protection acts, including
Alaska (PIPA), Florida (FIPA), Maryland
(PIPA), California, Texas, Massachusetts
and Wisconsin.
Let’s take a look at Florida…
Welcome to FIPA!
On June 20, 2014, Governor Rick Scott
signed, “The Florida Information and
Protection Act of 2014” into law and it went
into effect on July 1, 2014.
Things to know about FIPA
1. Under FIPA, a “covered entity” is much more expansive than the
definition of a covered entity under HIPAA.
Why? FIPA CEs include any business that acquires, maintains, stores,
or uses personal information, not just those in the healthcare
industry. The FIPA definition of “personal information” also includes
more information than the definition of protected health information
under HIPAA.
Did you know that under FIPA, a name with credit card number
qualifies as “personal information?”
9
Things to know about FIPA
Under FIPA, covered entities and third-party agents (similar to business
associates) are required to take reasonable measures to protect and secure data
in electronic form containing personal information.
Therefore, you will either need to create a FIPA policy and procedure or add the
FIPA provisions to your HIPAA policies and procedures.
Though your organization may be carefully safeguarding programs containing
medical information, such as EMR, practitioners need to examine all programs
storing identifying information that may amount to “personal information.”
A Breach under FIPA
There are additional obligations under FIPA in the event of a breach.
1. The covered entity will need to provide written notice to the Department of Legal
Affairs (AKA Attorney General) within thirty (30) days if more than 500 people are
involved in the breach. The notice must contain very specific elements. The CE
should be prepared to be asked for a copy of its breach policies.
2. If greater than 1,000 individuals are affected by the breach, the covered entity must
notify all consumer reporting agencies.
3. If the third-party agent (similar to a business associate) has a breach, it must notify
the covered entity with ten (10) days. (HIPAA required notice in up to sixty (60)
days).
4. Affected individuals must be notified of the breach within thirty (30) days. (HIPAA
requires 60 day notification and there is an exception that may enable providers to
notify individuals in accordance with HIPAA.)
FIPA
Did you know that under FIPA, CEs and third-party agents
are required to take all reasonable measures to dispose of
customer records containing personal information?
More specifically, shredding, erasing, or making the
personal information unreadable or undecipherable. Make
sure your organization creates a FIPA policy and procedure
on this or add to your HIPAA policy and procedure.
10
Civil Penalties
The U.S. Department of Health and Human Services’ Office for Civil
Rights (OCR) is responsible for administering and enforcing the HIPAA
Privacy and Security Rules. Thus, the OCR conducts associated complaint
investigations, compliance reviews, and audits.
If a covered provider is found to have failed to comply with HIPAA, the
OCR may impose fines. State Attorneys General may also enforce
provisions of the HIPAA Rules.
Under FIPA, a violation by either a covered entity or a third-party agent will
be treated as an unfair or deceptive trade practice and could result in a civil
penalty of up to $500,000. As FIPA does not create a private right of action
for individuals to file suit, the Department of Legal Affairs will be the
enforcing body in the state of Florida.
Criminal Penalties
Again, the U.S. Department of Justice (DOJ)
may enforce criminal penalties for HIPAA
violations.
Practical Issues with Electronic Recordkeeping
11
Practical Issues with Electronic Recordkeeping
It takes so much more time to document!
Some of the templates are not pertinent to my
practice area.
I accidentally pushed the wrong button and
now I have to amend the record.
My records are less detailed.
What other issues can you identify? Discuss!
Case # 1
Documentation &
Electronic Medical
Records.
Case # 1
Synopsis
Practitioner at nursing home copied the prior progress notes for patients and re-dated them to reflect the current date. No changes were made to each patients’ prior vital signs, but the Practitioner did evaluate each patient.
Allegations
A two-count Administrative Complaint was filed, alleging that the Practitioner violated s. 458.331(1)(m), Fla. Stat. (2007) by failing to keep legible medical records that justified the course and care and treatment accurately with regard to the patients and also alleged that Practitioner violated 458.331(1)(k), Fla. Stat. (2007) by making deceptive, untrue or fraudulent representations in or related to the practice of medicine.
Case is currently pending.
12
Case # 1 Details
Practitioner completes rounds at nursing home and was experiencing reported visual issues. Upon noting that the symptoms and statuses of a few patients were unchanged from a the previous evaluation, the practitioner copied the prior progress notes for those patients and re-dated them to reflect the current date. No changes were made to each patients’ prior vital signs
Nursing home staff corroborated that the practitioner did in fact evaluate each patient on the date in question.
Does this conduct violate the law?
Case # 1 Details
Ultimately, the Department filed a two-count Administrative Complaint, where it was alleged that the Practitioner violated s. 458.331(1)(m), Fla. Stat. (2007) by failing to keep legible medical records that justified the course and care and treatment accurately with regard to the patients. It was further alleged that the Practitioner violated 458.331(1)(k), Fla. Stat. (2007) by making deceptive, untrue or fraudulent representations in or related to the practice of medicine.
Case # 1 Details
How does this apply to you in your field?
How could the practitioner protect himself
in this situation?
Will EMR help or hurt?
13
Case # 2
Continuity of Care
Case # 2
Synopsis:
Nursing facility practitioner did not order accuchecks because he did not find any indication in the Patient’s medical record that the Patient was diabetic or taking any medications for diabetes. Additionally, the hospital transfer form did not include any indication of an accucheck order. The Practitioner only saw the Patient on one occasion, at the time of admission. Nine days later, the Patient was subsequently found unresponsive by a nursing home nurse. Patient subsequently expired due to Cerebrovascular Accident.
Allegation:
DOH filed a two-count Administrative Complaint, alleging that the Practitioner violated s. 458.331(1)(t) Fla. Stat., by committing medical malpractice and violated s. 458.331(1)(m), Fla. Stat. (2005), by failing to keep legible medical records justifying the course of treatment of the Patient.
Outcome:
Letter of Concern; $8,000.00 administrative fine, $4,596.66 in administrative costs, five (5) hours of CME in “Risk Management.”
Case # 2 Details
Patient was discharged from hospital following issues with his blood sugars at home, which caused him to fall out of a chair, be combative, etc. He was ordered to have accuchecks done three (3) times daily. Laboratory studies performed during his hospital admission did not show any abnormal blood sugar levels and the Patient’s hospital physician at the hospital never ordered a Hemoglobin A1C. Even with a normal glucose, however, the Patient still had a decreased level of responsiveness. At the time of transfer to a nursing facility, the Patient was lethargic and non-responsive and the Practitioner was unable to obtain any information from him and no family members were present for to discuss the Patient’s past medical history or condition. Upon examination, the Practitioner noted that the Patient had weakness and swelling in his right arm and right leg, and had multiple decubitus ulcers. Otherwise, his examination was unremarkable. The Practitioner closely reviewed all of the documentation from the hospital that was made available to him at the time of admission. This limited information in the medical record indicated the onset of the patient’s illness and EMS transfer to the hospital; and the transfer form provided the patient’s admission diagnosis of Altered Mental Status as a Primary Diagnosis, and Dehydration and Elevated Liver Enzymes as a Secondary Diagnosis. The hospital attending physician had ordered Aleve, one tablet twice a day and Physical Therapy Evaluation and Dietary Consult with fair rehabilitation potential. The nursing facility practitioner also reviewed the laboratory studies in the medical record, which showed a blood sugar of 70 on one day and a blood sugar of 114 two days later. A CT scan report also indicated a borderline abdominal aneurysm. The foregoing was the only information that was provided to the Practitioner at the time of the Patient’s admission to the nursing home.
14
Case # 2 Details
The Practitioner did not order accuchecks because he did not find any indication in the Patient’s medical record that the Patient was diabetic or taking any medications for diabetes. Additionally, the hospital transfer form did not include any indication of an accucheck order. In consideration of the limited information available to him, the Practitioner believed that the Patient had suffered an isolated hypoglycemic attack at the time of admission due to his poor nutritional status and dehydration. Therefore, he admitted the Patient to the nursing home with a diagnosis of cerebrovascular accident with right hemiparesis, renal insufficiency, dementia and multiple decubitus ulcers. The Practitioner only saw the patient on one occasion, at the time of admission.
Nine days later, the Patient was subsequently found unresponsive by a nursing home nurse. The on-call physician was contacted, and ordered that the patient be transferred to the hospital for evaluation. The Practitioner was never informed by the nursing home or the hospital of this incident. Days later, the Practitioner received a call from a local funeral home requesting that he sign the Certificate of Death, as an autopsy had been denied by the Medical Examiner. The Practitioner complied, and indicated Cerebrovascular Accident as the immediate cause of death, and senile arteriosclerosis as a secondary cause.
DOH Expert’s Criticisms
Patient was not stable enough to go to a
nursing facility
Acceptance of Patient without acquiring
necessary details from patient’s
hospitalization
Failure to order necessary tests and
consultations.
Case # 2 is especially
frightening because…
The physician was held responsible,
arguably for failing to order testing, based
upon information that was not provided to
him at the time of admission to the nursing
facility.
15
Discuss….
Liability?
– What could you have done to avoid this result?
Should the Practitioner have rounded on the Patient more
frequently than once in nine days?
What was the responsibility of the medical director?
– What could the nursing home have done to facilitate
information during the transfer of care?
Legal Issues: Use of EHR/EMR in
Nursing Homes
Application & Analysis
Medical Directors
16
Why would a physician want to become a medical director?
Financial challenges for physicians. Some
may wish to seek an additional source of
income.
Duties of Medical Director
Pursuant to 400.9935, Fla. Stat.,
(1) Each clinic shall appoint a medical director or clinic director who shall agree in writing to accept legal
responsibility for the following activities on behalf of the clinic. The medical director or the clinic director shall:
(a) Have signs identifying the medical director or clinic director posted in a conspicuous location within the clinic
readily visible to all patients.
(b) Ensure that all practitioners providing health care services or supplies to patients maintain a current active and
unencumbered Florida license.
(c) Review any patient referral contracts or agreements executed by the clinic.
(d) Ensure that all health care practitioners at the clinic have active appropriate certification or licensure for the level
of care being provided.
(e) Serve as the clinic records owner as defined in s. 456.057.
(f) Ensure compliance with the recordkeeping, office surgery, and adverse incident reporting requirements of chapter
456, the respective practice acts, and rules adopted under this part and part II of chapter 408.
(g) Conduct systematic reviews of clinic billings to ensure that the billings are not fraudulent or unlawful. Upon
discovery of an unlawful charge, the medical director or clinic director shall take immediate corrective action. If the
clinic performs only the technical component of magnetic resonance imaging, static radiographs, computed
tomography, or positron emission tomography, and provides the professional interpretation of such services, in a fixed
facility that is accredited by a national accrediting organization that is approved by the Centers for Medicare and
Medicaid Services for magnetic resonance imaging and advanced diagnostic imaging services and if, in the preceding
quarter, the percentage of scans performed by that clinic which was billed to all personal injury protection insurance
carriers was less than 15 percent, the chief financial officer of the clinic may, in a written acknowledgment provided to
the agency, assume the responsibility for the conduct of the systematic reviews of clinic billings to ensure that the
billings are not fraudulent or unlawful.
Duties of Medical Director
(h) Not refer a patient to the clinic if the clinic performs magnetic resonance imaging, static radiographs, computed
tomography, or positron emission tomography. The term “refer a patient” means the referral of one or more patients of
the medical or clinical director or a member of the medical or clinical director’s group practice to the clinic for
magnetic resonance imaging, static radiographs, computed tomography, or positron emission tomography. A medical
director who is found to violate this paragraph commits a felony of the third degree, punishable as provided in s.
775.082, s. 775.083, or s. 775.084.
(i) Ensure that the clinic publishes a schedule of charges for the medical services offered to patients. The schedule
must include the prices charged to an uninsured person paying for such services by cash, check, credit card, or debit
card. The schedule must be posted in a conspicuous place in the reception area of the urgent care center and must
include, but is not limited to, the 50 services most frequently provided by the clinic. The schedule may group services
by three price levels, listing services in each price level. The posting may be a sign that must be at least 15 square feet
in size or through an electronic messaging board that is at least 3 square feet in size. The failure of a clinic to publish
and post a schedule of charges as required by this section shall result in a fine of not more than $1,000, per day, until
the schedule is published and posted.
(2) Any contract to serve as a medical director or a clinic director entered into or renewed by a physician or a licensed
health care practitioner in violation of this part is void as contrary to public policy. This subsection shall apply to
contracts entered into or renewed on or after March 1, 2004.
(3) A charge or reimbursement claim made by or on behalf of a clinic that is required to be licensed under this part
but that is not so licensed, or that is otherwise operating in violation of this part, regardless of whether a service is
rendered or whether the charge or reimbursement claim is paid, is an unlawful charge and is noncompensable and
unenforceable. A person who knowingly makes or causes to be made an unlawful charge commits theft within the
meaning of and punishable as provided in s. 812.014.
17
Duties of Medical Director
(4)(a) Regardless of whether notification is provided by the agency under s. 408.812, a person commits a felony of the
third degree, punishable as provided in s. 775.082, s. 775.083, or s. 775.084, if the person knowingly:
1. Establishes, owns, operates, manages, or maintains an unlicensed clinic required to be
licensed under this part or part II of chapter 408; or
2. Offers or advertises services that require licensure as a clinic under this part or part II of
chapter 408 without a license.
(b) If the agency provides notification under s. 408.812 of, or if a person is arrested for, a violation of subparagraph
(a)1. or subparagraph (a)2., each day during which a violation of subparagraph (a)1. or subparagraph (a)2. occurs
constitutes a separate offense.
(c) A person convicted of a second or subsequent violation of subparagraph (a)1. or subparagraph (a)2. commits a
felony of the second degree, punishable as provided in s. 775.082, s. 775.083, or s. 775.084. If the agency provides
notification of, or if a person is arrested for, a violation of this paragraph, each day that this paragraph is violated
thereafter constitutes a separate offense. For purposes of this paragraph, the term “convicted” means a determination of
guilt which is the result of a trial or the entry of a plea of guilty or nolo contendere, regardless of whether adjudication
is withheld.
(d) In addition to the requirements of part II of chapter 408, a health care provider who is aware of the operation of an
unlicensed clinic shall report the clinic to the agency. The agency shall report to the provider’s licensing board a failure
to report a clinic that the provider knows or has reasonable cause to suspect is unlicensed.
(e) A person commits a felony of the third degree, punishable as provided in s. 775.082, s. 775.083, or s. 775.084, if
the person knowingly:
1. Files a false or misleading license application or license renewal application or files false or
misleading information related to such application or agency rule; or
2. Fails to report information to the agency as required by s. 408.810(3).
Duties of Medical Director
(5) Any licensed health care provider who violates this part is subject to discipline in accordance
with this chapter and his or her respective practice act.
(6) Any person or entity providing health care services which is not a clinic, as defined under s.
400.9905, may voluntarily apply for a certificate of exemption from licensure under its exempt status
with the agency on a form that sets forth its name or names and addresses, a statement of the reasons
why it cannot be defined as a clinic, and other information deemed necessary by the agency. An
exemption is not transferable. The agency may charge an applicant for a certificate of exemption in an
amount equal to $100 or the actual cost of processing the certificate, whichever is less. An entity
seeking a certificate of exemption must publish and maintain a schedule of charges for the medical
services offered to patients. The schedule must include the prices charged to an uninsured person
paying for such services by cash, check, credit card, or debit card. The schedule must be posted in a
conspicuous place in the reception area of the entity and must include, but is not limited to, the 50
services most frequently provided by the entity. The schedule may group services by three price levels,
listing services in each price level. The posting must be at least 15 square feet in size. As a condition
precedent to receiving a certificate of exemption, an applicant must provide to the agency
documentation of compliance with these requirements.
Duties of Medical Director
(7)(a) Each clinic engaged in magnetic resonance imaging services must be accredited by a national
accrediting organization that is approved by the Centers for Medicare and Medicaid Services for
magnetic resonance imaging and advanced diagnostic imaging services within 1 year after licensure. A
clinic that is accredited or that is within the original 1-year period after licensure and replaces its core
magnetic resonance imaging equipment shall be given 1 year after the date on which the equipment is
replaced to attain accreditation. However, a clinic may request a single, 6-month extension if it
provides evidence to the agency establishing that, for good cause shown, such clinic cannot be
accredited within 1 year after licensure, and that such accreditation will be completed within the 6-
month extension. After obtaining accreditation as required by this subsection, each such clinic must
maintain accreditation as a condition of renewal of its license. A clinic that files a change of ownership
application must comply with the original accreditation timeframe requirements of the transferor. The
agency shall deny a change of ownership application if the clinic is not in compliance with the
accreditation requirements. When a clinic adds, replaces, or modifies magnetic resonance imaging
equipment and the accrediting agency requires new accreditation, the clinic must be accredited within
1 year after the date of the addition, replacement, or modification but may request a single, 6-month
extension if the clinic provides evidence of good cause to the agency.
(b) The agency may deny the application or revoke the license of any entity formed for the purpose
of avoiding compliance with the accreditation provisions of this subsection and whose principals were
previously principals of an entity that was unable to meet the accreditation requirements within the
specified timeframes. The agency may adopt rules as to the accreditation of magnetic resonance
imaging clinics.
18
Duties of Medical Director
(8) The agency shall give full faith and credit pertaining to any past variance and waiver
granted to a magnetic resonance imaging clinic from rule 64-2002, Florida Administrative
Code, by the Department of Health, until September 2004. After that date, such clinic
must request a variance and waiver from the agency under s. 120.542.
(9) In addition to the requirements of part II of chapter 408, the clinic shall display a
sign in a conspicuous location within the clinic readily visible to all patients indicating
that, pursuant to s. 626.9892, the Department of Financial Services may pay rewards of
up to $25,000 to persons providing information leading to the arrest and conviction of
persons committing crimes investigated by the Division of Insurance Fraud arising from
violations of s. 440.105, s. 624.15, s. 626.9541, s. 626.989, or s. 817.234. An authorized
employee of the Division of Insurance Fraud may make unannounced inspections of a
clinic licensed under this part as necessary to determine whether the clinic is in
compliance with this subsection. A licensed clinic shall allow full and complete access to
the premises to such authorized employee of the division who makes an inspection to
determine compliance with this subsection.
59A-33.008, F.A.C.
(1) A licensed health care clinic may not operate or be maintained without the day-to-day supervision of a single
medical or clinic director as defined in Section 400.9905(5), F.S. The health care clinic responsibilities under Sections
400.9935(1)(a)-(i), F.S., cannot be met without an active, appointed medical or clinic director. Failure of an appointed
medical or clinic director to substantially comply with health care clinic responsibilities under Rule 59A-33.012, F.A.C.
and Sections 400.9935(1)(a)-(i), F.S., shall be grounds for the revocation or suspension of the license and assessment of
a fine pursuant to Section 400.995(1), F.S.
(2) By statutory definition in Section 400.9905(5), F.S., a medical director is a health care practitioner that holds an
active and unencumbered Florida physician’s license in accordance with Chapters 458 (medical physician), 459
(osteopathic physician), 460 (chiropractic physician) or 461 (podiatric physician), F.S. A suspended or non-renewed
license is considered an encumbered license, as is a license that restricts the license holder from performing health care
services in a manner or under supervision different from a license holder without board or Department of Health
restrictions.
(3) The Agency shall issue an emergency order suspending the license of any health care clinic operated or maintained
without a medical or clinic director as required by Sections 400.990-400.995, F.S., and this rule for such period of time
as the health care clinic is without a medical or clinic director. The Agency shall assess a civil fine of up to $5,000 for
operating or maintaining a health care clinic without a medical or clinic director. Each day of operation following
receipt of Agency notice is considered a separate offense. Operation and maintenance of a health care clinic without a
medical or clinic director shall be grounds for revocation of the license in addition to the assessment of fines pursuant to
Section 400.995(1), F.S.
59A-4.106, F.A.C.
(2) Each nursing home facility shall adopt, implement, and
maintain written policies and procedures governing all
services provided in the facility.
(3) All policies and procedures shall be reviewed at least annually and revised as needed with
input from, at
minimum, the facility Administrator, Medical Director, and Director of Nursing.
(4) Each facility shall maintain policies and procedures in the following areas:
(a) Activities;
(b) Advance directives;
(c) Consultant services;
(d) Death of residents in the facility;
(e) Dental services;
(f) Staff education, including hiv/aids Training;
(g) Diagnostic services;
(h) Dietary services;
(i) Disaster preparedness;
(j) Fire prevention and control;
19
59A-4.106, F.A.C. (k) Housekeeping;
(l) Infection control;
(m) Laundry service;
(n) Loss of power, water, air conditioning or heating;
(o) Medical director/consultant services;
(p) Medical records;
(q) Mental health;
(r) Nursing services;
(s) Pastoral services;
(t) Pharmacy services;
(u) Podiatry services;
(v) Resident care planning;
(w) Resident identification;
(x) Resident’s rights;
(y) Safety awareness;
(z) Social services;
(aa) Specialized rehabilitative and restorative services;
(bb) Volunteer services; and
(cc) The reporting of accidents or unusual incidents involving any resident, staff member,
volunteer or visitor. This policy shall include reporting within the facility and to the AHCA.
59A-4.1075, F.A.C.
(1) Each facility will have only one physician who is designated as Medical Director.
(2)(a) The Medical Director must be a physician licensed under Chapters 458 or 459, F.S., the nursing home
administrator may require that the Medical Director be certified or credentialed through a recognized
certifying or credentialing organization.
(b) A Medical Director who does not have hospital privileges shall be certified or credentialed through a
recognized certifying or credentialing body, such as the Joint Commission on Accreditation of Healthcare
Organizations (JCAHO), the American Medical Directors Association, the Healthcare Facilities
Accreditation Program of the American Osteopathic Association, the Bureau of Osteopathic Specialists of
the American Osteopathic Association, the Florida Medical Directors Association or a Health maintenance
organization licensed in Florida.
(c) A physician must have his/her principal office within 60 miles of all facilities for which he/she serves as
Medical Director. Principal office is the office maintained by a physician pursuant to Sections 458.351 or
459.026, F.S., and where the physician delivers the majority of medical services. The physician must specify
the address of his/her principal office at the time of becoming Medical Director. The agency may approve a
request to waive this requirement for rural facilities that exceed this distance requirement. A rural facility is a
facility located in a county with a population density of no greater than 100 persons per square mile, which is
at least 30 minutes of travel time, on normally traveled roads under normal traffic conditions, from any other
nursing home facility within the same county.
59A-4.1075, F.A.C.
(d) The facility shall appoint a Medical Director who shall visit the facility at least once a month. The
Medical Director shall review all new policies and procedures; review all new incident and new accident
reports from the facility to identify clinical risk and safety hazards. The Medical Director shall review the
most recent grievance logs for any complaints or concerns related to clinical issues. Each visit must be
documented in writing by the Medical Director.
(3) A physician may be Medical Director of a maximum of 10 nursing homes at any one time. The Medical
Director, in an emergency where the health of a resident is in jeopardy and the attending physician or
covering physician cannot be located, may assume temporary responsibility of the care of the resident and
provide the care deemed necessary.
(4) The Medical Director appointed by the facility shall meet at least quarterly with the quality assessment
and assurance committee of the facility.
(5) The Medical Director appointed by the facility shall participate in the development of the comprehensive
care plan for the resident when he/she is also the attending physician of the resident.
20
Random provisions re: medical director
The facility shall maintain an Emergency Medication Kit, the contents of which shall be determined in
consultation with the Medical Director, Director of Nursing and Pharmacist, and it shall be in accordance
with facility policies and procedures. The kit shall be readily available and shall be kept sealed. All items in
the kit shall be properly labeled. The facility shall maintain an accurate log of receipt and disposition of each
item in the Emergency Medication Kit. An inventory of the contents of the Emergency Medication Kit shall
be attached to the outside of the kit. If the seal is broken, the kit must be resealed the next business day after
use. See 59A-4.112(10), F.A.C.
(d) Residents may not be retained in the facility who require services beyond those for which the facility is
licensed or has the functional ability to provide as determined by the Medical Director and the Director of
Nursing in consultation with the facility administrator. See 59A-4.106(1)(d)
(5) The following must be completed for each child. An RN shall be responsible for ensuring these tasks are
accomplished:
(a) Informing the attending physician and medical director of beneficial and untoward effects of the
therapeutic interventions;
See 59A-4.1295Additional Standards for Homes That Admit Children 0 Through 20 Years of Age
Liabilities of Medical Directors
Must ensure compliance with regulatory
laws!
Watch out for referral violations!
– Anti-kickback Statute
– Stark Law
– Florida Patient Brokering Act
Liabilities of Medical Directors
Fines and civil monetary penalties can range
from $10,000 to $50,000 PER occurrence!
You can be excluded from Medicare and
Medicaid programs!
Disciplinary action against medical license
Jail!
21
Liabilities of Medical Directors
Medical Malpractice Actions
- Direct and vicarious liability claims
Professional Liability Matters
Why?
- Supervision of personnel
- Many medical directors are required to review
policies and procedures which relate to risk
management, clinical care and patient care.
Liabilities of Medical Directors
Do you have a medical director
agreement? Are there indemnification
provisions?
What does your insurance policy have to
say?
Liabilities of Medical Directors
Don’t forget about billing regulations!!!!
Medicare and Medicaid regulations often require certain
levels of supervision by a physician to allow for billing
of services provided by an ancillary provider. If
appropriate supervision is not provided, you may face
an issue of FALSE CLAIMS.
Yes….claims have been asserted by government
agencies against medical directors.

22
United States ex rel. Beaujon
v.
Hebrew Homes Health Network, Inc., et al.,
Case No. 12-20951 CIV (S.D. Fla.).
Announced June 16, 2015
From 2006 through 2013, Hebrew Homes allegedly operated a
sophisticated kickback scheme in which they hired numerous
physicians ostensibly as medical directors pursuant to contracts that
specified numerous job duties and hourly requirements.
The various facilities had several such medical directors under
contract at any given time, paying each several thousand dollars
monthly. The United States alleged that in reality these were ghost
positions, and that most of the medical directors were required to
perform few, if any, of their contracted job duties.
Instead, they were allegedly paid for their patient referrals to the
Hebrew Homes facilities, which increased exponentially once the
medical directors were put on the payroll.
Hebrew Homes Health Network Inc., its operating subsidiaries and
affiliates, and William Zubkoff, the former president and executive
director of Hebrew Homes Health Network Inc. (collectively
Hebrew Homes), have agreed to pay $17 million to resolve
allegations that Hebrew Homes violated the False Claims Act by
improperly paying doctors for referrals of Medicare patients
requiring skilled nursing care.
Hebrew Homes provided skilled nursing services at seven
rehabilitation and skilled nursing facilities in Miami-Dade County,
Florida.
This is the largest settlement involving alleged violations of the
Anti-Kickback Statute by skilled nursing facilities in the United
States.
23
“The record settlement announced today demonstrates this office’s commitment
to rooting out all forms of illegal kickback schemes,” said U.S. Attorney Wifredo
A. Ferrer of the Southern District of Florida. “And that is certainly true in the
context of nursing homes, where the Department of Justice will not allow
healthcare decisions for elderly Medicare patients to be influenced by kickback
payments to physicians. The integrity of our public health care program requires
that such decisions be based on quality of care.”
“Hebrew Homes’ intricate kickback scheme in this record-setting case threatened
the impartiality of physician referrals, the financial integrity of Medicare and the
public’s trust in the health care system,” said Special Agent in Charge Shimon R.
Richmond of the U.S. Department of Health and Human Services’ Office of
Inspector General (HHS-OIG). “Our agency will continue to investigate nursing
homes and other health care providers that seek to illegally boost profits at the
expense of federal health care programs.”
As part of the settlement, Mr. Zubkoff has agreed to resign as Hebrew
Homes’ Executive Director and to no longer be an employee of the
company. Also, as part of the settlement announced today, Hebrew
Homes has entered into a five-year corporate integrity agreement with
HHS-OIG, and has agreed to change its policies on hiring and
maintaining medical directors.
The settlement resolves allegations made in a lawsuit filed by Stephen
Beaujon, a former CFO of Hebrew Homes, under the qui tam, or
whistleblower, provisions of the False Claims Act, which permit private
individuals to sue on behalf of the government for false claims and to
share in any recovery. Mr. Beaujon will receive $4.25 million.
The Implementation of the Health Care
Clinic Act in Chapter 400, Fla. Stat. has
raised the bar as to supervision and liability
for medical directors in those settings.
24
Where the medical director has no involvement with the patient…
In November 2013, the Georgia Supreme Court considered a case where liability was alleged against the medical
director of an emergency department who was not involved in providing care to the patient. It was alleged that the
medical director negligently failed to ensure that emergency room physicians and nurses had adequate training. The
appellate court had previously held that the medical director owed a duty to the patient such that the failure to
adequately supervise emergency room staff can “result in liability for any damages resulting from such failure by one
whose responsibility it is to provide such supervision.”
However, the Georgia Supreme Court disagreed with this determination and instead, ruled that the medical director was
entitled to summary judgment, and held:
(1) A medical director cannot be liable for merely undertaking to supervise medical staff. However, the medical
director may be liable if that individual undertakes to direct the method and manner in which care is provided by the
medical staff. In the instant case, the medical director did not treat the patient and was uninvolved and was not
responsible to control or direct the method or manner in which care was rendered. Thus, the Georgia Supreme Court
determined that he owed no duty to the patient and therefore, was not liable for medical malpractice as claimed.
(2) The medical director did not increase the risk to the patient of harm through any alleged failure to adequately
supervise the ER staff and physicians. The Georgia Supreme Court determined that at worst, the medical director failed
to resolve a misunderstanding amongst the medical staff regarding the specifics of a particular treatment protocol.
Where the medical director has no involvement with the patient…
REMEMBER:
This does not rule out the possibility of medical director liability! Rather, it serves to
limit the circumstances of liability.
This makes it even more important for medical directors to ensure that they review
agreements with their facilities to ensure that it is crystal clear as to whether the provider
has the responsibility or authority to control or direct the method or manner in which care
is provided by the medical staff the medical director is supervising.
If there is such responsibility or authority, the potential for medical director liability
exists concerning the actions of medical staff. However, if there is no such responsibility
or authority, then the medical director is likely protected from liability for injuries to
patients with who he or she was not involved in providing care to, UNLESS the medical
director did something to escalate a risk to the patient.
Protect yourself!
Do you have a medical director agreement?
Is it comprehensive?
Check with your health care attorney!
25
Risk Prevention
Templates
If you find that the EHR template is not
relevant/has extraneous data sets not
pertinent to your practice, etc.; immediately
contact the EHR manager to have the
template changed to meet your needs. One
size does not fit all. This will ensure more
detailed records and better prompts to
improve documentation and will save time.
Slow down!
Our firm recently represented a practitioner who
was investigated by the Florida Department of
Health based upon a patient’s complaint that her
record inaccurately reflected that she had
endoscopy and celiac disease, when she in fact did
not. This resulted from a simple error by the
physician, who pressed the incorrect stereo marker
during EHR documentation and also resulted in the
patient seeking unnecessary further care.
26
Check your defaults!
We represented a radiologist whose default was
inadvertently set to “no hydrocephalus.” Guess
what? The Patient had hydrocephalus and the
result was death. Be careful!
In another matter, the patient was documented as
having great circulation/pulses/appropriate
extensive nerve testing/response in his left arm.
The patient’s left arm had been amputated
following Vietnam.
Less detailed documentation
Our firm handles hundreds of Department of
Health investigations each year. Due to the
onset of EHR, we have observed a
significant absence of detail within patient
medical records.
Less detailed documentation
Remember: If it is not documented, it did
not happen. If you would have documented
a finding in a non-EHR record, it needs to be
in the EHR record.
If necessary, use a blank sheet of paper and
attach it as an addendum! Be sure to timely
date the record!
27
Remember
Poor, scant or limited documentation impacts
patient care drastically.
It also impacts you and your license. Your records
are your sword and shield when it comes to
defending investigations by licensing or
governmental authorities and specialty boards, as
well as billing audits.
Going mobile?
Use extra care!
Mobile health devices, such as iPads, laptops,
phones and so forth. While convenient, be careful!
Take extra precautions to prevent:
loss
theft
downloading a virus
Is your wi-fi secured? Confirm!
Do you share devices? Consider ramifications!
When you think about
practice issues, consider
Liability Issues?
What could the practitioner have done to avoid
disciplinary action?
Could this situation apply to your practice?
How could you protect yourself?
28
What can I do to protect
my license?
Check your insurance!
– Do you have broadform coverage? Some new carriers may not! In addition to coverage in the event of a malpractice claim, broadform provides coverage for your attorney fees should you be investigated by the Department of Health and sometimes, FMQIA, etc.
– Remember: It will cover your attorney fees, but it will not cover any potential fine or costs assessed against you by your licensing board.
What can I do to protect
my license?
Remember that the mere occurrence of an investigation of your license, even if it is dismissed without a finding of probable cause or any filing of an Administrative Complaint, can potentially impact you in terms of credentialing. Contact your attorney to discuss how best to respond on applications for licenses, reapplications/applications for privileges at hospitals and ASCs, to specialty boards and so forth.
Example: History of license being “investigated” vs. “disciplined”
Board of Medicine
http://doh.state.fl.us/mqa/medical/index.html
Board of Nursing
http://doh.state.fl.us/mqa/nursing/index.html
Board of Nursing Home Administrators
http://doh.state.fl.us/mqa/nurshome/index.html
Board of Osteopathic Medicine
http://doh.state.fl.us/mqa/osteopath/index.html
Board of Pharmacy
http://doh.state.fl.us/mqa/pharmacy/index.html
29
For more information or to access
newsletters and developing news in
the field of health care law, please
visit our website at:
www.chlawyers.com
Gregory A. Chaires, Esq.
Board Certified in Health Law
JoAnn M. Guerrero, Esq., LHRM A special thanks for her assistance
CHAIRES, BROODERSON & GUERRERO, P.L.
283 Cranes Roost Blvd., Suite 165
Altamonte Springs, Florida 32701
Telephone (407) 834-2777
Fax (407) 834-2778
www.chlawyers.com
Email: [email protected]