Embed Size (px)
Citation preview

Using the New GAIN Patient Placement Summary to Support Individual Treatment
Planning, Placement and Program Evaluation
Marc Fishman, M.D., Johns Hopkins University and Maryland Treatments Center, Baltimore, MD
Laverne Hanes Stevens, Ph.D., Chestnut Health Systems, Atlanta, GA
Michael L. Dennis, Ph.D., Chestnut Health Systems, Bloomington, IL
Workshop at the Joint Meeting on Adolescent Treatment Effectiveness, Baltimore, MD, March 28, 2006. Preparation of this manuscript was supported by funding from the Center for Substance Abuse Treatment (CSAT Contract no. 270-2003-00006) and
several individual grants. The content of this poster are the opinions of the author and do not reflect the views or policies of the government. Available on line at
www.chestnut.org/LI/Posters or by contacting Joan Unsicker at 720 West Chestnut, Bloomington, IL 61701, phone: (309) 827-6026, fax:(309) 829-4661, e-Mail:

This workshop will..
• Provide an overview of the evolution, strengths and limits of ASAM’s patient placement criteria (Fishman)
• Outline the GAIN approach to integrating treatment planning and placement, including the expanded recommendations we are developing (Stevens)
• Summarize Chestnut’s work to developing real time placement recommendations for line clinicians using the CSAT adolescent treatment data set (Dennis)

Introduction the American Society of Addiction Medicine’s (ASAM) Patient Placement Criteria (PPC)
Marc Fishman MD
Johns Hopkins University
Maryland Treatment Centers

Evolution of the APC
PPC-1 (1991)
PPC-2 (1996)
PPC-2R (2001)

ASAM PPC-2: Assessment Dimensions
1: Intoxication / Withdrawal Potential2: Biomedical Conditions3: Emotional / Behavioral / Cognitive Conditions4: Readiness to Change5: Relapse / Continued Use / Continued Problem
Potential6: Recovery Environment
ASAM PPCLevels of Care
Level 0.5: Early Intervention
Level I: Outpatient
Level II: Intensive Outpatient and Partial Hospital
Level III: Residential / Inpatient
(includes therapeutic communities)
Level IV: Hospital
(based on services – NOT length of stay)

ASAM PPC-2R Adolescent Criteria
• Level II– II.1: Intensive Outpatient (IOP)– II.5: Partial Hospital / Day Program
• Level III– III.1: Clinically Managed Low Intensity
Residential (e.g.., halfway houses)
– III.5: Clinically Managed Medium Intensity Residential (moderate –long term treatment)
– III.7: Medically Monitored High Intensity Residential/Inpatient (short term treatment)

ASAM PPC-2R Crosswalk
I. OutpatientII. Intensive Outpatient III. Residential
IV. Medically Managed Inpatient
Withdrawal No risk Minimal Some risk Severe risk
Medical No risk Manageable Medical monitoring required
24 hr acute medical care required
Emotional/ Behavioral
No risk Mild severity Moderate 24 hr psychiatric care required
Readiness To Change
Cooperative Cooperative but requires structure
High resistance, needs 24 hr monitoring
Relapse Potential
Maintains abstinence
More symptoms, needs close monitoring
Unable to control use in outpatient care

ASAM PPC: General Principles
• Unidimensional --> Multidimensional assessment• Program driven --> Clinically / individually
driven treatment• Fixed length --> Variable length of treatment• Fragmentation --> Integration of treatment
services• Discrete Types --> Continuum of care

Strengths of PPC
• Real time placement decisions
• Justification of placement (regulatory, reimbursement)
• Guide to common language for organizing assessment data
• Guide to treatment needs and plan
• Shift to a more chronic model of care that recognizes most people go through treatment multiple times over a period of several years before reaching sustained recovery.

Evaluation First and Continuous
ProformaAssessment
Treatment StandardizedAssessment
Treatment

Local Implementation
• Local variations in– Availability of continuum of services
• Availability of certain levels of care• Characteristics and services of actual local
programs in each levels of care– Needs and expectations of client, referrors,
payors, regulators, and others (e.g. judges) – Variation in provider programs, services,
capacity, culture

Limitations to PPC
• Inconsistency of interpretation and complex nature making training and reliable implementation difficult
• Reliability of assessment data without standardized instrumentation
• Operationalization of decision rules for placement• Services are NOT consistently bundled by level of care• Some services not level of care dependent • Face valid, but limited outcome research• Need to integrate with treatment planning for specific
services

The GAIN approach to integrating treatment planning and placement
Laverne Hanes Stevens, Ph.D.,
Chestnut Health Systems, Atlanta, GA

How the GAIN Views Problem Sets
Recency
Prevalence
Breadth

Interpreting Problem Sets
Factor #1
Recency:– Has this problem ever occurred and, if so, when
did it last occur?– Things that happened in the past week or 90 days
will typically play a greater role in current treatment than those that happened 4-12 months or 1+ years ago.

Interpreting Problem Sets
Factor #2Breadth:• How widespread/diverse is the presentation of
clinical symptoms or pattern of service utilization? • Typically more diverse presentations are associated
with higher severity. • For clinical problems, the focus is on the past year
(or since the last interview in follow-up assessments).
• For services, the focus is on the lifetime pattern of service utilization.
Interpreting Problem Sets
Factor #3Current Prevalence:• How often has this happened in the past 90 days? • Typically things that happen more frequently
(particularly if they interfere with responsibilities at home, work/school or socially) are going to be more important than those that happened only once or twice.

GAIN Approach to ASAM Level of Care Placement
• Rate the “Problem Recency” and “Treatment History”– Three time perspectives: None, past or current
• First -- Determine treatment planning and service needs based on the above rating.
• Then --Identify the level of care and/or local program that best matches the cluster of service needs that are identified.
• Lastly -- Use information from average performance of different levels of care with similar populations to make choices where there is more than one possibility or trade-off.

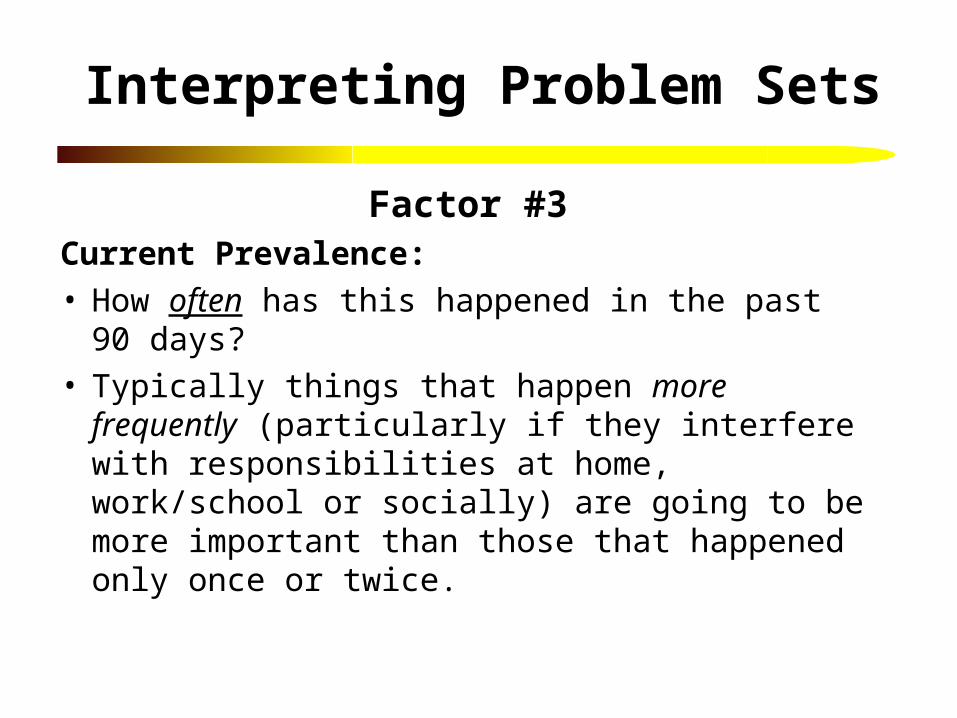
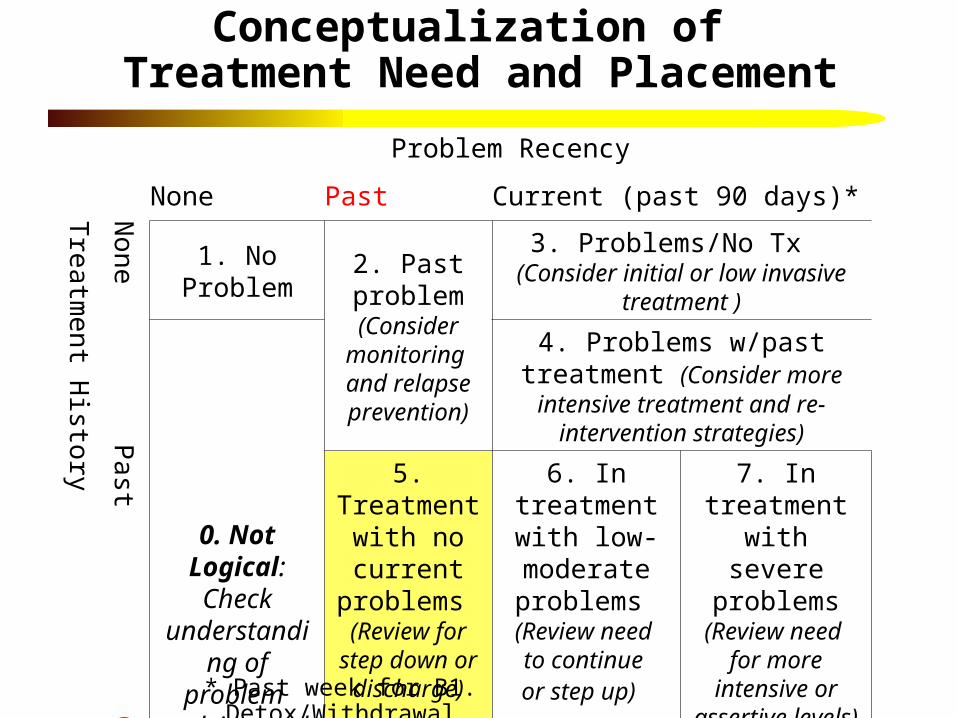
Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal
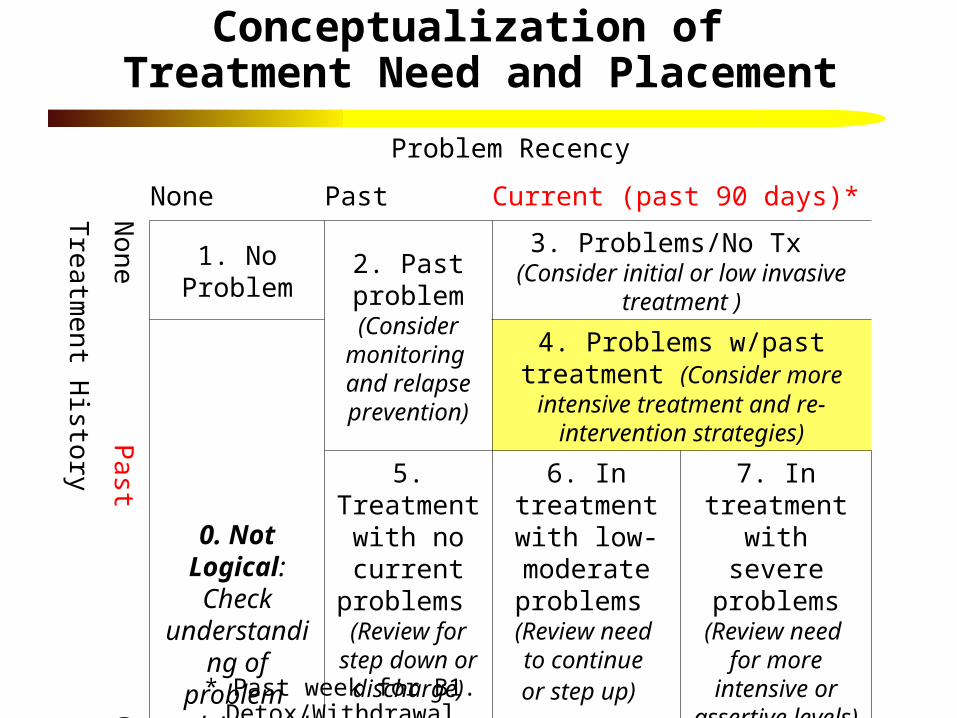
Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal
Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Supplemental ASAM
Worksheet (GAIN I page 100)
Can document impression here so it prints out in GRRS
SA treatment used for A, B4, B5, and (if IOP/residential) B6
Can record problem recency by treatment history rating
Can record comment to help with treatment planning
Record preliminary placement recommendations and any comments about placement to include at the end of the GRRS

The GAIN Recommendation and Referral Summary (GRRS)
A text-based narrative in MS Word designed to be edited and shared with specialists, clinical staff from other agencies, insurers and lay people.

G-RRS Organization & Content(See Appendix F)
1. Presenting Concerns and Identifying Information
2. DSM-IV/ICD-9 Diagnoses
3. Evaluation Procedure
4. Substance Use Diagnoses and Treatment History (ASAM criteria A)
5. Level of Care and Service Needs (ASAM Six Dimensional Criteria B)
6. Summary Recommendation
7. Staff Notes from Assessment (should be used and removed during editing)

G-RRS Organization & Content(See Appendix F)
1. Presenting Concerns and Identifying Information
2. DSM-IV/ICD-9 Diagnoses
3. Evaluation Procedure
4. Substance Use Diagnoses and Treatment History (ASAM criteria A)
5. Level of Care and Service Needs (ASAM Six Dimensional Criteria B)
6. Summary Recommendation
7. Staff Notes from Assessment (should be used and removed during editing)

Level of Care and Service Needs
Arranged by six dimensions of ASAM Criteria B:
1. Acute Alcohol/Drug Intoxication and Withdrawal Potential
2. Biomedical Conditions and Complications
3. Emotional, Behavioral, or Cognitive Conditions and Complications
4. Readiness to Change
5. Relapse, Continued Use, or Continued Problem Potential
6. Recovery Environment

Prior Treatment Options Built into the GAIN Recommendation & Referral Summary
B1 Intoxication/Withdrawal: Need for Detox Services– Monitoring for change in intoxication or withdrawal symptoms– Ambulatory detoxification services related to withdrawal– Inpatient detoxification services related to current intoxication and withdrawal
B2 – Biomedical: Need for Medical Services– Monitoring for change in physical health (and medication compliance)– The following specific accommodations for medical conditions required to
participate in treatment: List out– A more detailed medical assessment (including nutritional guidance)– Referral for the following specific medical services: List out
B3 Emotional/Behavioral: Need for Psychological Services– Monitoring for change in mental health (and medication compliance)– The following specific accommodations for psychological conditions required
to participate in treatment: List out– A more detailed psychological assessment– Referral for the following specific psychological services: List out

Prior Treatment Options… (Continued)B4 Readiness to Change: Need for Motivational Services,
Coordination of Pressure and/or Access/Resistance Issues– Monitoring for change in readiness for change– The following assistance to help address treatment resistance: list out– Individual motivational enhancement sessions– The following specific services to help maintain motivation to stay in recovery: list out
B5 Relapse/Continued Use Potential: Need for Risk Management– Monitoring for change in relapse potential– Relapse prevention skills groups– Increased structure to reduce environmental risks of relapse– The following specific steps to reduce continued use/relapse potential: list out
B6 Recovery Environment: Need for Environmental Interventions and Risk management
– Monitoring for change in recovery environment– A residential or more structured treatment setting to temporarily control environmental risks– the following specific steps to reduce recovery environment risks: list out– The following specific steps to take further advantages of sources of support/personal
strengths: list out

NEW Recommendation Summary for
Supporting Clinical Decisions

Dimension B-1: Intoxication / Withdrawal
Problem
No Problem• No past / current
Past Problems• Lifetime history of withdrawal
symptoms and no current problems
Current - Low/Mod Problems• Any past week symptoms of withdrawal
and no current high severity problems
Current High Severity• High on Current Withdrawal Scale in the
past week• Any past week withdrawal symptoms
with daily opioid use or physiological symptoms of withdrawal
Treatment
No Treatment History• No past / current treatment
Past (Lifetime) Treatment History• Lifetime history of detoxification
services and no current treatment
Currently in Treatment• 1 or more of the past 90 days in
detoxification

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Example: Dimension B-1 / Cell 6 Text
The GRRS will print:
[NAME] has received detoxification services in the past 90 days but is still using at a low frequency or having some withdrawal symptoms in the past week. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0
SPECIFIC NEEDS AND CLINICAL INDICATIONS>> • Discussing the current and/or prior detoxification episodes with
[NAME] to review the experience (e.g., Did [he/she/name] complete the prior detoxification program? follow-up recommendation to go to treatment? achieve a period of initial abstinence (at least 90 days)? Are there things that might be adjusted to make it work as well or better this time? What is [he/she/name] willing/able to do differently this time?)

• Requesting records from most recent detoxification episode and reviewing those records to determine the services previously provided, recommendations and outcomes.
• Discuss [NAME]’s progress with current treatment team to discuss areas of responsiveness and unresponsiveness; compliance and noncompliance; and possible impact of any physical or emotional problems that may be posing challenges for detoxification.
• A review to determine whether to continue with current detoxification services, re-admit or step-up to next level of care.
• Restart or continue ambulatory or residential/inpatient detoxification services

Dimension B-2: Biomedical Conditions
Problem
No Problem• No past / currentPast Problems• Past year mod/high on Health Distress
Scale; any disabilities; female w/history of pregnancy; history of infectious diseases; or any lifetime report of health problems/issues
Current - Low/Mod Problems• Any disabilities; female who became
pregnant in past 90 days (regardless of outcome) or is currently pregnant, past 90 day infectious diseases or health problems or need medical attention to attend treatment
Current High Severity• Had any health problems daily (45+/90)
or functional impairment weekly (13+/90)
Treatment
No Treatment History• No past / current treatmentPast (Lifetime) Treatment History• Any physical health treatment, or
current medication, or ever having seen a doctor)
Currently in Treatment• Any physical health treatment in the
past 90 days or currently being treated

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Example: Dimension B-2 / Cell 2 Text
The GRRS will print:
[NAME] reported a history of prior health problems, but not having problems or treatment in the past 90 days. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0 SPECIFIC NEEDS AND CLINICAL INDICATIONS>>
• Discussing prior health problems and any prior medical care
with [NAME] to review the problem, the care received, and potential impact upon treatment (e.g., Is there a relationship between [NAME]’s medical issues and [his/her/Name’s] substance use? To what extent might these health issues pose challenges for the treatment of the substance use disorder? Are there special needs that must be considered in order to participate in substance use treatment?)

• Monitoring for change in physical health (and medication compliance)
• Review of plan for what to do if these health problems re-occur in the future

Dimension B-3: Emotional-Cognitive-Behavioral
Problem
No Problem• No past / currentPast Problems• Reported lifetime history of being
bothered by emotional, trauma or behavior problems, or diagnoses
Current - Low/Mod Problems• Bothered by MH problems, functional
impairment, memories from the past, attention problems or self-injury, at any time in the past 90 days.
Current High Severity• Had any emotional, trauma or behavioral
problems daily (45+ /90) or functional impairment or self-harm weekly (13+/90) or suicide plans/ means/attempts with any functional impairment or self-harm
Treatment
No Treatment History• No past / current treatmentPast (Lifetime) Treatment History• Any mental health treatment, or
current medication, or ever having seen a doctor
Currently in Treatment• Any mental health treatment in the
past 90 days or currently being treated

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Example: Dimension B-3 / Cell 5 Text
The GRRS will print:
[NAME] has received mental health treatment for emotional, behavioral or cognitive problems in the past 90 days, but reports not having problems in the past 90 days. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0 SPECIFIC NEEDS AND CLINICAL INDICATIONS>>
• Discussing past emotional, behavioral or cognitive problems with [NAME] to review the need for future mental health services, barriers to accessing them and any accommodations needed to participate in treatment.

• Discussing how past emotional, behavioral or cognitive problems and substance use problems may be related
• Develop follow-up plans related to mental health care (e.g. Were arrangements made for continuing care? Does [NAME] express willingness, have a plan and means, and/or taken initial steps toward adhering to the follow-up recommendations? Does [NAME] know what to do if problems re-emerge?)
• Monitoring for change in emotional, behavioral or cognitive condition, linkage to treatment, and treatment/medication compliance
• The following specific accommodations for emotional, behavioral or cognitive problems required to participate in treatment: <list out>

Dimension B-4: Readiness for Change
Problem
No Problem• No past / currentPast Problems• Lifetime substance dependence, abuse,
induced disorders, weekly substance use, hiding use or substance related family problems
Current - Low/Mod Problems• Using in the past 90 days and one of the
following (mod/high resistance, low/mod motivation, few reasons for quitting, not completely ready to stop)
Current High Severity• (Using in the past 48 hours, daily (45+/90)
or using opioids weekly (13+/90)) and one of the following (high resistance, low motivation, no reasons for quitting, not completely ready to stop)
Treatment
No Treatment History• No past / current treatment
Past (Lifetime) Treatment History• Lifetime substance use disorder
treatment, current medication, any recent treatment
Currently in Treatment• Currently taking substance use disorder
meds; in substance use disorder treatment in the past 90 days; currently in substance use disorder treatment; or others are putting on pressure to change.

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Example: Dimension B-4 / Cell 7 Text
The GRRS will print:
[NAME] has received treatment for substance use problems in the past 90 days, but is still experiencing severe problems. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0 SPECIFIC NEEDS AND CLINICAL INDICATIONS>>
• Discussing the current and/or prior treatment episodes with [NAME] to review the experience (e.g., Did [he/she/name] achieve a period of sustained abstinence? What is [he/she/name] willing/able to do differently?)

• Discussing the Personal Feedback Report with [NAME], (e.g. Use Motivational Interviewing to explore consequences of [NAME]'s substance use? What are some of [NAME]’s reasons for wanting to quit? What things are a part of [NAME]’s typical pattern of use? When does [NAME] have the most situational confidence for avoiding substances?)
• Discussing with [NAME] the way substance use functions in [his/her/name’s] life, (e.g. What things are usually going on just prior to the decision to use drugs or alcohol? What thoughts and feelings precede using? What effect does substance use have on those thoughts/feelings? What people, situations, or activities are associated with using drugs or alcohol? What things might impact the likelihood of continued use?)

• Discussing [NAME]'s goals, present level of motivation for treatment and resistance to change, (e.g. Use Motivational Interviewing to explore [NAME]’s goals for substance use? What are some important reasons for those goals? What steps are necessary to achieve those goals? What things could prevent being able to attain those goals? What are [NAME]’s points of ambivalence about quitting?)
• Discussing [NAME]’s progress with current treatment team to discuss areas of responsiveness and unresponsiveness; compliance and noncompliance; and areas of resistance and ambivalence; and any barriers to treatment retention and compliance
• A review to determine whether to continue with current level of care or step-up to next level of care.
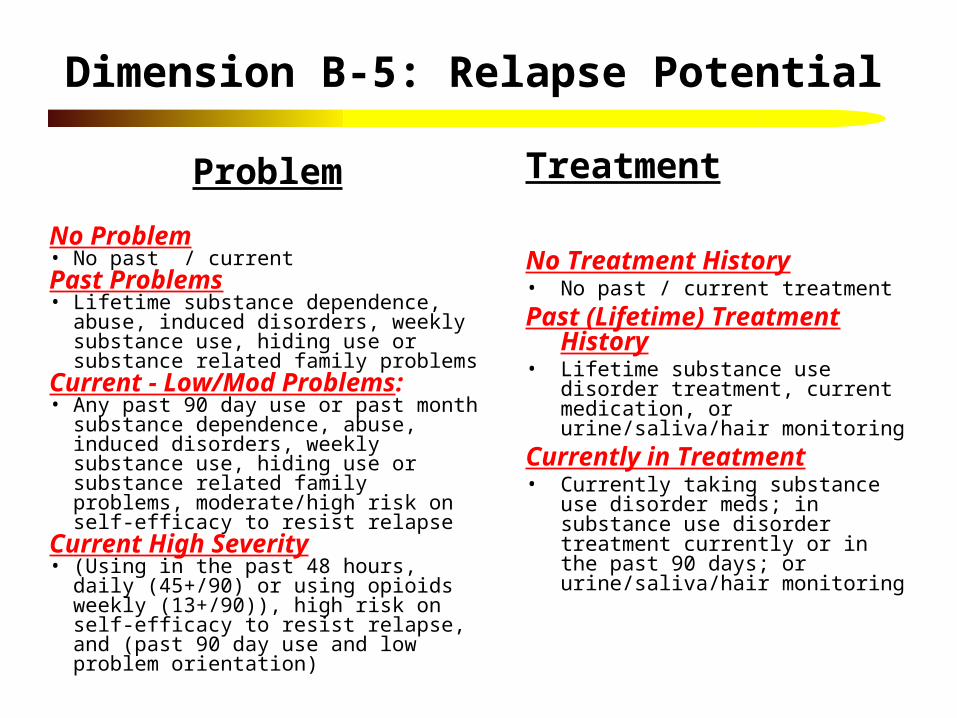
Dimension B-5: Relapse Potential
Problem
No Problem• No past / currentPast Problems• Lifetime substance dependence, abuse, induced
disorders, weekly substance use, hiding use or substance related family problems
Current - Low/Mod Problems:• Any past 90 day use or past month substance
dependence, abuse, induced disorders, weekly substance use, hiding use or substance related family problems, moderate/high risk on self-efficacy to resist relapse
Current High Severity• (Using in the past 48 hours, daily (45+/90) or
using opioids weekly (13+/90)), high risk on self-efficacy to resist relapse, and (past 90 day use and low problem orientation)
Treatment
No Treatment History• No past / current treatment
Past (Lifetime) Treatment History• Lifetime substance use disorder
treatment, current medication, or urine/saliva/hair monitoring
Currently in Treatment• Currently taking substance use disorder
meds; in substance use disorder treatment currently or in the past 90 days; or urine/saliva/hair monitoring

Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Example: Dimension B-5 / Cell 3 Text
The GRRS will print:
[NAME] reported substance use problems in the past 90 days and no prior history of treatment for those problems. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0 SPECIFIC NEEDS AND CLINICAL INDICATIONS>>
• Referral to relapse prevention group or counseling intervention to identify relapse triggers, develop a plan for minimizing triggers, coping with those that do occur, and what to do if [NAME] does relapse, (e.g. Does [NAME] understand the nature of relapse and its triggers? What people, places, things, thoughts or emotions are associated with initiating substance use? What things might impact the likelihood of relapse? Who will [NAME] call to help get back on track?)
• Referral to cognitive-behavior therapy to develop skills for coping with stress, managing thoughts and behaviors and avoiding relapse
• Discuss with [NAME] the situations that pose a risk of relapse, (e.g. Who are the people, places and things that put [NAME] at high risk? How can high-risk situations be avoided? What refusal skills does [NAME] already have or need to develop? What will be [NAME]’s plan for handling emergency risk situations?)

• Discussing [NAME]’s willingness to participate in a 12-step or other recovery program (e.g. including getting and actively working with a sponsor; working the 12 steps; establishing a relationship with a home group; performing a service at meetings such as set-up, literature, chairing a meeting; or sharing their story at a meeting)
• Developing and discussing options for [NAME] to build or enhance a non-using social support network; engage in substance-free recreational activities; build situational confidence; strengthen refusal skills; and cope with relapse

Dimension B-6: Recovery Environment
Problem
No Problem• No past / currentPast Problems• Lifetime history of homelessness, environmental risk
for home, school/work peers, or social peers, victimization, drug related illegal activities.
Current - Low/Mod Problems• Past 90 day homelessness, unable to stay in the same
home, trouble at home, arguing/violence, victimization, structured activities involving alcohol or drugs, or any illegal activity to get substances or under their influences.
Current High Severity• Past 90 day illegal activity to get substances or under
their influences, victimization; or weekly (13+/90 days) homeless, with substance use in the home, or structured activities involving alcohol or drugs; or daily (45+/90 days) trouble with family or arguing.
Treatment
No Treatment History• No past / current treatment
Past (Lifetime) Treatment History• Lifetime history of environmental
interventions targeting substance use including: self help, recovery homes, IOP, residential treatment, probation, parole, detention, jail, electronic monitoring, or house arrest.
Currently in Treatment• Past 90 day history of environmental
interventions targeting substance use including: self help, recovery homes, IOP, residential treatment, other controlled environment where they could not come & go as they please or being on probation, parole, detention, jail, electronic monitoring or house arrest.
Conceptualization of Treatment Need and Placement
Problem Recency
None Past Current (past 90 days)*
Treatm
ent History
None P
ast Current .
1. No Problem
2. Past problem (Consider
monitoring and relapse prevention)
3. Problems/No Tx (Consider initial or low invasive
treatment )
0. Not Logical:Check
understanding of problem or lying and
recode
4. Problems w/past treatment (Consider more intensive treatment
and re-intervention strategies)
5. Treatment with no current
problems (Review for
step down or discharge)
6. In treatment with low-moderate problems
(Review need to continue or step up)
7. In treatment with severe problems
(Review need for more
intensive or assertive levels)
* Past week for B1. Detox/Withdrawal

Example: Dimension B-6 / Cell 4 Text
The GRRS will print:
NAME] reported current (past 90 days) recovery environment problems and also reported receiving intervention for those problems in the past. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0 SPECIFIC NEEDS AND CLINICAL INDICATIONS>>
• Discussing the prior times in a controlled environment to review the experience (e.g., Did [he/she/name] make changes in the recovery environment or supports? Were other family members involved in making changes? Did they have a follow-up recommendation? achieve a period of initial abstinence (at least 90 days)? Are there things that might be adjusted to make more permanent changes this time? What is [he/she/name] willing/able to do differently this time?)

• Requesting records from prior service providers and reviewing those records to determine the services previously provided, recommendations and outcomes.
• Increased structure of environment to reduce exposure to relapse triggers and increase support for recovery (e.g. Placement in IOP or residential treatment; involvement in substance-free structured activities in the community; increased monitoring; substance-free vocational activities)

Dimension Recommendation Text
For each dimension, the GRRS will print text addressing 4 areas:
1. Client’s self-report summarized
2. Client Requests
3. Cell-specific Recommendations
4. General Recommendations for the Dimension

Self-Report Summarized
• Problems: Things the client reported in terms of symptoms and problems in that dimension
• Treatment history: Lifetime service-utilization in that dimension
• Beliefs: Client attitudes, perceptions of problem severity and need for help

List of Client Requests (Example from B-4)
[NAME] specifically asked for assistance with:
• Getting Treatment [S10a6]
• Making transportation arrangements [B9a1]
• Making child care arrangements [B9a2]
• Scheduling around work, school or family responsibilities [B9a3]
• Paying for treatment [B9a4]
• Language, religious, ethnic or cultural issues [B9a5]
• Clothing [B9a6]
• Food [B9a7]
• Other issues:_________ [B9a99v]

Cell-Specific Recommendations (Example from B-4, cell 5)
[NAME] is currently receiving treatment for substance use, but reports no substance use problems in the past 90 days. Based on the information provided, the evaluator recommends: <<PROMPT: REVIEW, DELETE OR EDIT ACCORDING T0 SPECIFIC NEEDS AND CLINICAL INDICATIONS>>
• Developing and discussing post-discharge or step-down plans with [NAME], (e.g. Does [NAME] express willingness, have a plan and means, and/or taken initial steps for adhering to follow-up recommendations?)
• Discussing past substance use problems with [NAME] to review the need for future services, barriers to accessing them and the motivation to stay in recovery…..

General Recommendations for the Dimension(Based on problems endorsed)
• Other: [ [XASB4v]; <list out others> / <list out others>]
• Refer to wrap-around or case management services [If [B9a1-99>0] or [B7=4, 5 or 6] or [B7a>59]]
• Discuss the external pressure for treatment, the consequences of continued use or treatment drop-out, and potential need for coordination of care w/external sources of pressure [If B4a-j>0]
• Discuss and set realistic expectations for how long [NAME] will need to be in treatment and the potential need for continuing care [If [B6<4] and [max of S9c-u>2]]
• Pair [NAME] with program graduate or experienced client to help them understand the treatment process and expectations [If [E5=0 or E5f=4] and [E6=0 or E6f=4] and [E7=0 or E7f=4] and [S7=0]]

Developing Real Time Placement Recommendations for
Line Clinicians
Michael L. Dennis, Ph.D.,
Chestnut Health Systems, Bloomington, IL

Current Summary Recommendation
• Summary of current systems client is involved in and with which treatment needs to be coordinated
• Any level of care recommendation from GAIN placement worksheet
• Prompt to :– enter level of care recommendation – comment on any special barriers to placement and what
might be done about them – comment on need to coordinate care with other treatment
or agencies• Signatures• Staff notes from assessment

Strengths and Limits of Current Approach
• Strengths:– Keeps decisions in the hand of clinicians and avoids risk
of regulator/funders questioning differences– Recognizes the lack of evidence base for forcing several
decisions
• Weaknesses:– Difficult to train and get staff to reliably implement– Staff want advice– Supervisors want tools for training/managing staff,
particularly when there is turn over– It is difficult to do the needed outcome research on
placement rules unless they are made reliably/consistently

Learning from Practice
• Used data collected from 7,269 adolescents interviewed with GAIN version 5 as part of 89 CSAT adolescent treatment grants since 2002
• Created a variable for each of the 8 cells in the GAIN approach and reflected by the text we are developing for the expanded GRRS
• Examined the distribution of the variables overall and by level of care
• Used discriminant function analysis to predict the probability of being in each level of care for similar clients.
• Used to combine information into a level of care recommendation for line clinicians
• Characteristics of CSAT vs. TEDS public 2003 admissions

Geographic Location of Sites
ART
EATSCYTCEYORP
AK
AL
ARAZ
CA CODC
DE
FL
GA
HI
IA
ID
IN
KS
LA
MD
ME
MI
MN
MO
MS
MT
NC
ND
NE
NH
NJ
NM
NV
NY
OH
OK
OR
PA
RI
SC
SD
TN
TX
UTVA
WA
WV
WY
PR
VT
WI
IL
KY
MA
CT
DC
Program

Demographics
30%
19%
58%
16%
6%
17%
83%
18%
42%
17%
23%
20%
73%
29%0% 10
%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Female
African American
Caucasian
Hispanic
Mixed/Other
12 to 14 years old
15 to 17 years old
TEDS (n=153,251)
CSAT (n=7,226)

Clinical Severity
82%
33%
50%
48%
53%
37%
61%
53%
68%
74%0% 10
%
20%
30%
40%
50%
60%
70%
80%
90%
100%
First used underage 15
Prior Treatment
Weekly use atintake
Past YearDependence
Criminal JusticeSystem
TEDS (n=153,251)
CSAT (n=7,226)
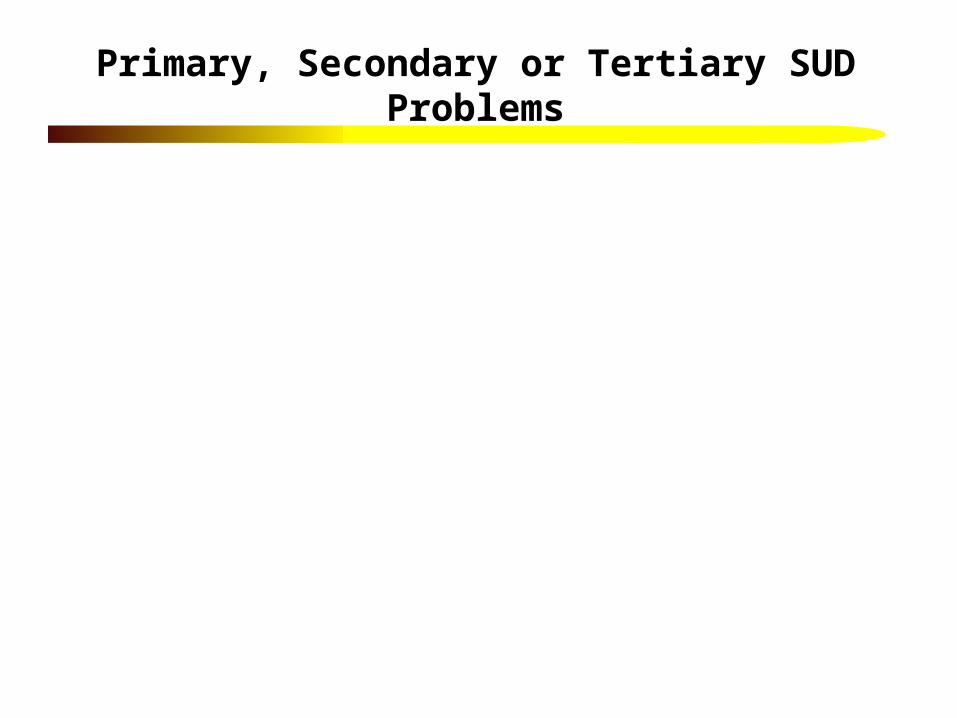
Primary, Secondary or Tertiary SUD Problems
57%
82%
8%
4%
7%
6%
60%
5%
3%
7%
2%
25%
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Alcohol
Marijuana/Hash
Cocaine/Crack
Heroin/Opiates
Meth/amphetamines
Any Other
TEDS (n=153,251)
CSAT (n=7,226)
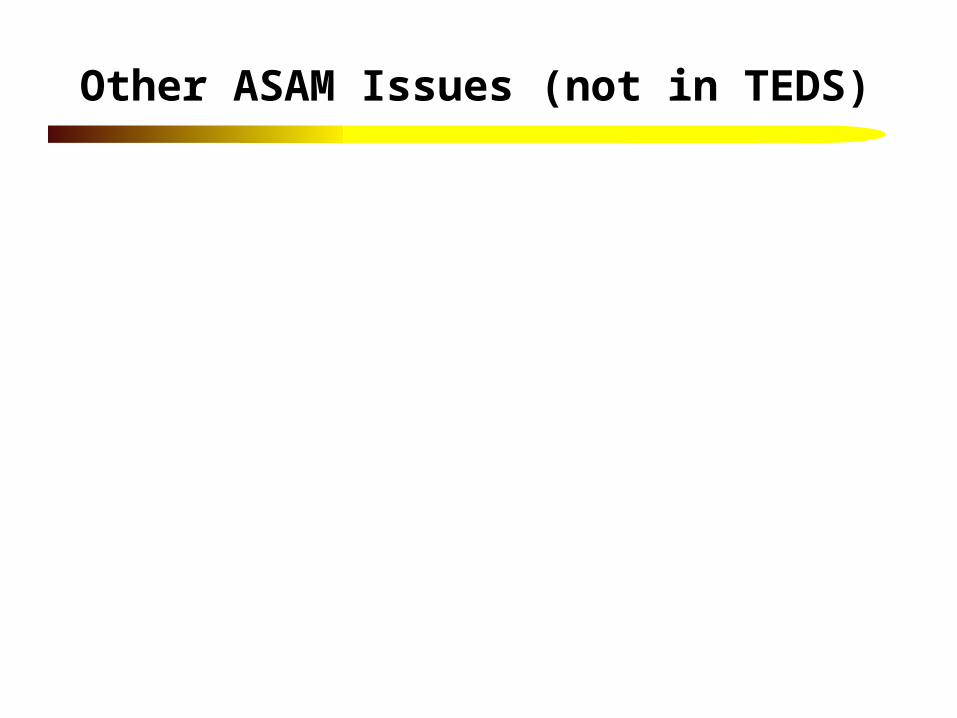
Other ASAM Issues (not in TEDS)
0.31
0.08
0.84
0.27
0.79
0.59
0.70
0.76
0.70
0.81
0.82
0.45
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Any withdrawal symptoms past week
Severe withdrawal (11+ symptoms)
Sexually active in past 90 days
Major health problems
Any co-occurring psychiatric
Ever physical, sexual or emotional victimization
Doesn't acknowledge AOD problem
Doesn't acknowledges need for treatment
Regular alcohol use in recovery environment
Regular drug use in recovery environment
Any violence or illegal activity
Any past year violent crime

Level of Care
68%
14%
18%
8%
21%
71%
0% 10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Outpatient
Intensive Outpatient
Residential TEDS (n=153,251)
CSAT (n=7,226)
Includes 9% in continuing care after residential
treatment or detention

68%
14%
9%
9%
8%
2%
19%
71%0% 10
%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Outpatient
Intensive Outpatient
Short Term Resid(<30 days)
Long Term ResidTEDS (n=153,251)
CSAT (n=7,226)
Level of Care
Includes 9% in continuing care outpatient (CCOP) after
residential treatment or detention

Proportion of Adolescents in Each Cell*
0% 20% 40% 60% 80% 100%
B1 Intox and Withdrawal
B2 Bio-Medical
B3 Psych-Behavioral
B4 Readiness for Change
B5 Relapse Potential
B6 Recovery Environment
0. Inconsistent 1. No Problem
2. Past Problem 3. Cur Prob. w/o Tx Hx
4. Cur Prob. w/ Tx Hx 5. Past Prob w/ Cur Tx
6. Lo/mod Prob w/ Cur Tx 7. High Cur Prob w/ Cur Tx

Diagnostic Severity by Level of Care
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
No/
Pas
t use
Lif
etim
e S
UD
inpa
st m
onth
rem
issi
on
Lif
etim
e S
UD
but
in C
E 4
5+/9
0 pa
stda
ys
Pas
t mon
th a
nyab
use/
depe
nden
cesy
mpt
om
Pas
t mon
th 3
+de
pend
ence
sym
ptom
s
CCOP
LTR
STR
IOP
OP

B1. Intox & Withdrawal Severity by LOC
0%10%20%30%40%50%60%70%80%90%
100%0.
Inc
onsi
sten
t
1. N
o P
robl
em
2. P
ast P
robl
em
3. C
ur P
rob.
w/o
Tx
Hx
4. C
ur P
rob.
w/ T
x H
x
5. P
ast P
rob
w/ C
ur T
x
6. L
o/m
od P
rob
w/ C
ur T
x
7. H
igh
Cur
Pro
b w
/ Cur
Tx
CCOP
LTR
STR
IOP
OP

B2. Biomedical Severity by LOC
* Insufficient data (n<25)
0%10%20%30%40%50%60%70%80%90%
100%0.
Inc
onsi
sten
t
1. N
o P
robl
em
2. P
ast P
robl
em
3. C
ur P
rob.
w/o
Tx
Hx*
4. C
ur P
rob.
w/ T
x H
x
5. P
ast P
rob
w/ C
ur T
x
6. L
o/m
od P
rob
w/ C
ur T
x
7. H
igh
Cur
Pro
b w
/ Cur
Tx
CCOP
LTR
STR
IOP
OP
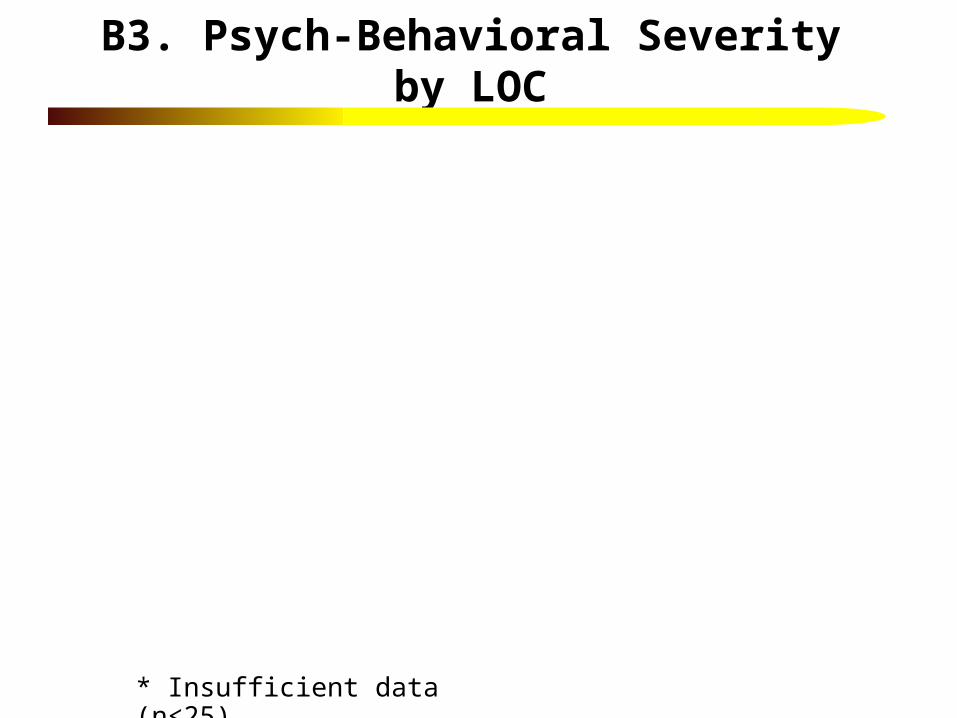
B3. Psych-Behavioral Severity by LOC
* Insufficient data (n<25)
0%10%20%30%40%50%60%70%80%90%
100%0.
Inc
onsi
sten
t*
1. N
o P
robl
em
2. P
ast P
robl
em
3. C
ur P
rob.
w/o
Tx
Hx
4. C
ur P
rob.
w/ T
x H
x
5. P
ast P
rob
w/ C
ur T
x
6. L
o/m
od P
rob
w/ C
ur T
x
7. H
igh
Cur
Pro
b w
/ Cur
Tx
CCOP
LTR
STR
IOP
OP

B4. Readiness for Change Severity by LOC
* Insufficient data (n<25)
0%10%20%30%40%50%60%70%80%90%
100%0.
Inc
onsi
sten
t*
1. N
o P
robl
em*
2. P
ast P
robl
em
3. C
ur P
rob.
w/o
Tx
Hx
4. C
ur P
rob.
w/ T
x H
x*
5. P
ast P
rob
w/ C
ur T
x
6. L
o/m
od P
rob
w/ C
ur T
x
7. H
igh
Cur
Pro
b w
/ Cur
Tx
CCOP
LTR
STR
IOP
OP

B5. Relapse Potential Severity by LOC
* Insufficient data (n<25)
0%
20%
40%
60%
80%
100%0.
Inc
onsi
sten
t
1. N
o P
robl
em
2. P
ast P
robl
em
3. C
ur P
rob.
w/o
Tx
Hx
4. C
ur P
rob.
w/ T
x H
x
5. P
ast P
rob
w/ C
ur T
x
6. L
o/m
od P
rob
w/ C
ur T
x
7. H
igh
Cur
Pro
b w
/ Cur
Tx
CCOP
LTR
STR
IOP
OP

B6. Recovery Environment Severity by LOC
* Insufficient data (n<25)
0%10%20%30%40%50%60%70%80%90%
100%0.
Inc
onsi
sten
t*
1. N
o P
robl
em*
2. P
ast P
robl
em*
3. C
ur P
rob.
w/o
Tx
Hx
4. C
ur P
rob.
w/ T
x H
x
5. P
ast P
rob
w/ C
ur T
x
6. L
o/m
od P
rob
w/ C
ur T
x
7. H
igh
Cur
Pro
b w
/ Cur
Tx
CCOP
LTR
STR
IOP
OP

Predicting Level of Care
• Discriminant Function Analysis using stepwise analysis of the cells we have just reviewed, the GAIN psychopathology scales & change measures, and variables from Rand’s case mix study (Morral et al., 2005).
• Final solution with 42 variables (see next slides) allows us to predict where counselors around the country would place a similar client in terms of the best fit, and the probability of being in each level of care.

Most Influential Cells
-0.80
-0.30
0.20
0.70
1.20B
5.2
Pas
t Rel
apse
Pro
blem
B4.
7 H
igh
Sev
erity
Rea
dine
ss f
or c
hang
eis
sues
/cur
rent
TX
B4.
6 L
ow/m
odR
eadi
ness
for
Cha
nge
prob
lem
/cur
rent
TX
B5.
7 H
i Sev
erity
Rel
apse
pote
ntia
l/cur
rent
TX
B2.
1 N
o B
io-M
edP
rob
B6.
5 P
ast R
ecov
ery
envi
ronm
ent P
rob
B2.
2 P
ast B
io-M
edpr
ob
OP
IOP
STR
LTR
CCOP

Past Month (PM)/Past Year Psychopathology/ Psychopathy
-0.80
-0.30
0.20
0.70
1.20
SubstanceProblem Scale
(PM)
SubstanceDependence Scale
(PY)
Crime & ViolenceScale (PY)
BehaviorComplexity Scale
(PY)
OP
IOP
STR
LTR
CCOP

Past 90 Day/ Week/ Current Change Scores
-0.80
-0.30
0.20
0.70
1.20S
ubst
ance
Fre
quen
cy S
cale
(P90
)
Pro
blem
Ori
enta
tion
Sca
le
Em
otio
nal P
robl
ems
Sca
le(P
90)
Nee
dle
Fre
quen
cy S
cale
(P
90)
Tre
atm
ent M
otiv
atio
n In
dex
Sel
f-E
ffic
acy
Sca
le
Cur
rent
Wit
hdra
wal
Sca
le (
PW
)
Doe
sn't
Ack
nolw
edge
AO
Dpr
ob
Tre
atm
ent R
esis
tanc
e In
dex
Hea
lth
Pro
blem
s S
cale
(P
90)
OP IOPSTR LTRCCOP

Pattern of Substance Use
-0.80
-0.30
0.20
0.70
1.20D
ays
Dru
nk/H
igh
mos
t of
day
(P90
)
Usi
ng d
aily
(P
90)
Use
d dr
ugs/
alco
hol
in p
ast 2
day
s
Nee
ds tr
eatm
ent f
orH
eroi
n
Day
s of
toba
cco
use
(P90
)
Nee
ds tr
eatm
ent f
orA
mph
etam
ines
/Met
h
Nee
ds tr
eatm
ent f
orno
n-co
mm
on D
rugs
OP
IOP
STR
LTR
CCOP

Lifetime/ Past 90 Day/ Current Interventions
-0.80
-0.30
0.20
0.70
1.20D
ays
in c
ontr
olle
d en
viro
nmen
t(P
90)
Sub
stan
ce A
buse
Tx
Inde
x(P
90)
Cur
rent
ly in
AO
D T
x
Lif
etim
e A
A C
A N
A S
Rpa
rtic
ipat
ion
CJ
Sys
tem
Ind
ex (
P90
)
Tra
inin
g A
ctiv
ity
Sca
le (
P90
)
Cur
rent
JJ
invo
lvem
ent
Cur
rent
ly in
sch
ool
Tim
es a
dmit
ted
to d
etox
Rec
ent A
rres
sts
(P90
)
OP IOPSTR LTRCCOP

Lifetime/ Past 90 Day/ Current Interventions
-0.80
-0.30
0.20
0.70
1.20
LifetimeHomeless/Runaway
Minority status Age How many peoplelive with
OP
IOP
STR
LTR
CCOP

Predicted LOC by Actual LOC
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
P_OP P_IOP P_STR P_LTR P_CCOP
CCOP
LTR
STR
IOP
OP
Predicted Level of Care
Act
ual L
evel
of
Car
e
75% correctly classifiedKappa=.51
Miss-classification includes lack of availability

Adding Text to Reflect Recommendation and Likelihood of Alternatives
• Based on the above assessment, the evaluator recommends that [NAME] be admitted to Outpatient.
• <<Distribution of placement for similar clients is: 90% OP, 5% IOP, 0% STR, 2% LTR, 1% CC_OP>>

Adding Management Tools for Clinical Supervisors and Program Planners
• Summary of requests, cell placements and individual treatment planning rates recommended, and kept vs. modified or dropped to guide program planning
• Cross tabulations of predicted vs. actual placements to identify gaps
• Running above by site, team or staff person to check for potential training issues
• Ability to customize to identify local issues or programs.
Also will be doing analysis to see if placement into expected level of care is associated with better outcomes

Next Steps and Timeline for Updating the GRRS
1. Development of a user interface
2. Expert panel to review content, rules and recommendations in late May/June
3. Testing in the summer
4. Release by end of the year!

Acknowledgment
The content of this presentations are based on treatment & research funded by the Center for Substance Abuse Treatment (CSAT), Substance Abuse and Mental Health Services Administration (SAMHSA) under contract 270-2003-00006 using data provided by CSAT adolescent treatment grantees under the Adolescent Residential Treatment (ART), Effective Adolescent Treatment (EAT), Strengthening Communities for Youth (SCY), Targeted Capacity Expansion (TCE), and Young Offender Re-entry Program (YORP) grants (TI013313, TI013309, TI013344, TI013354, TI013356, TI013305, TI013340, TI130022, TI03345, TI012208, TI013323, TI14376, TI14261, TI14189,TI14252, TI14315, TI14283, TI14267, TI14188, TI14103, TI14272, TI14090, TI14271, TI14355, TI14196, TI14214, TI14254, TI14311, TI15678, TI15670, TI15486, TI15511, TI15433, TI15479, TI15682, TI15483, TI15674, TI15467, TI15686, TI15481, TI15461, TI15475, TI15413, TI15562, TI15514, TI15672, TI15478, TI15447, TI15545, TI15671)). The opinions are those of the author and do not reflect official positions of the consortium or government. Available on line at www.chestnut.org/LI/Posters or by contacting Joan Unsicker at 720 West Chestnut, Bloomington, IL 61701, phone: (309) 827-6026, fax: (309) 829-4661, e-Mail: [email protected].













![Analisis de Fishman[1]](https://img.pdfslide.net/doc/110x75/5572138e497959fc0b9287ad/analisis-de-fishman1.jpg)