Embed Size (px)
Citation preview
Presented by:
Carol Burke MSN, APRN/CNS, RNC-OB, C-EFM
Loyola University Perinatal Center
April 9, 2018
Fourth Annual Northern Illinois Perinatal, Neonatal and Pediatric Conference
Uterine Activity as a
Critical Element of EFM
Disclosures / conflict of interest
Disclosures MOD Nursing Advisory Committee AWHONN Nominating Committee and the science team for the Care of the Perioperative Patient
No financial conflict of interest No FDA “off label” pharmaceutical antibiotic treatment will be discussed Best evidence to date presented
Discuss impact of uterine activity with fetal oxygenation.
Define significance of frequency, duration intensity and
resting interval when evaluating normal and abnormal
uterine activity.
Outline documentation recommendations for uterine
activity.
With either direct or indirect monitoring the suspicion of
fetal death,
apparent fetal bradycardia, or
apparent fetal arrhythmia
Fetal monitoring technology cannot detect a difference
between a fetal and maternal signal source
requires simultaneous maternal and
fetal heart rate and/or ECG recordings.
In the absence of the fetal ECG signal (IUFD), there will usually be
no tracing. However, depending the existing maternal R wave, the
maternal heart rate may be displayed vs. from the dead or dying
fetus
A woman with a cardiac pacemaker: The transmitted maternal
pacemaker pulse may be at a higher voltage than the fetal R wave
causing the scalp electrode to record the pacemaker signal
Should palpate maternal radial pulse or apply pulse oximetry for a
minimum of 1 minute while listening to the device sounds upon
initial placement and whenever artifact is suspected.
Maternal heart rate is usually significantly lower than the mean baseline FHR throughout all stages of labor and delivery and rarely exceeds 110 beats per minute between contractions.
Maternal heart rate may be increased with chorioamnionitis, pain, anxiety, result of medications
Most ‘maternal variability’ values fall within the moderate range for FHR variability (6–25 beats per minute), and thus this difference may not be large enough to be discriminatory.
The maternal heart rate usually accelerates with uterine contractions and bearing-down efforts in stage 2.
Very similar to FHR accelerations during the latent phase of the first stage but, as labor progresses, maternal ‘accelerations’ become more frequent, have higher amplitudes, and longer duration.
Maternal cardiac output increases progressively during labor due to:
Increased venous return to the heart leading to stroke volume
Increased heart rate
Increase in catecholamine
Valsalva with pushing.
Frequency is evaluated over a minimum of 10 min
Tachysystole: > 5 spontaneous and/or stimulated uterine contractions in 10 minutes, averaged over a 30 minute window.
• Applies to spontaneous and stimulated uterine contractions.
• Even if the FHR is normal, action must be done with tachysystole
Normal : < 5 contractions in 10 minutes, averaged over a
30 minute window.
Some experts do not consider excessive uterine activity problematic unless there are corresponding changes in the fetal heart rate (FHR) pattern.
When contractions are occurring every 2 minutes or more, recovery of FSpO2 to previous baseline levels is incomplete (Clark et. al,2013)
Pit to
distress...
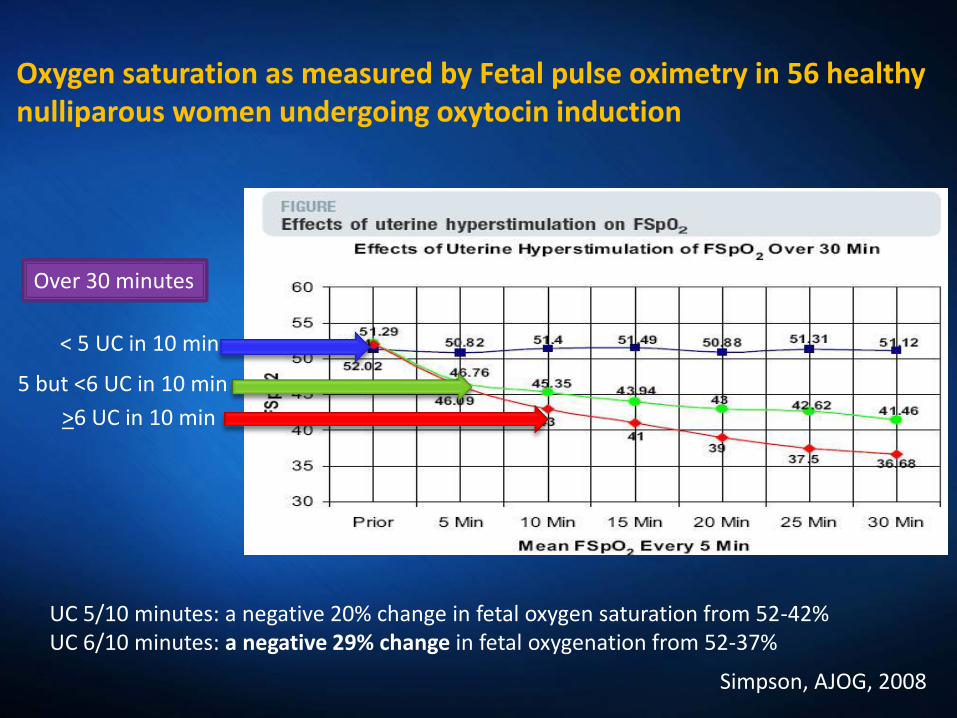
UC 5/10 minutes: a negative 20% change in fetal oxygen saturation from 52-42% UC 6/10 minutes: a negative 29% change in fetal oxygenation from 52-37%
< 5 UC in 10 min
5 but <6 UC in 10 min
>6 UC in 10 min
Over 30 minutes
Simpson, AJOG, 2008
Oxygen saturation as measured by Fetal pulse oximetry in 56 healthy nulliparous women undergoing oxytocin induction
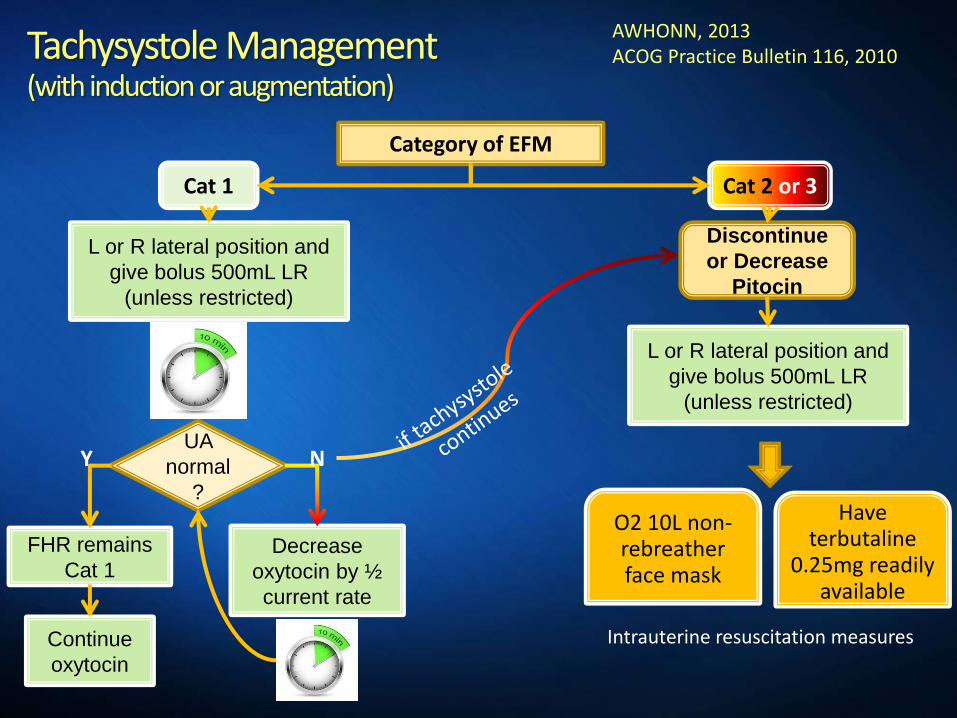
Tachysystole Management (with induction or augmentation)
Category of EFM
Cat 1
FHR remains
Cat 1 Decrease
oxytocin by ½
current rate
L or R lateral position and
give bolus 500mL LR
(unless restricted)
UA
normal
?
Cat 2 or 3
Discontinue
or Decrease
Pitocin
L or R lateral position and
give bolus 500mL LR
(unless restricted)
Continue
oxytocin
Y N
AWHONN, 2013 ACOG Practice Bulletin 116, 2010
O2 10L non-rebreather face mask
Have terbutaline
0.25mg readily available
Intrauterine resuscitation measures
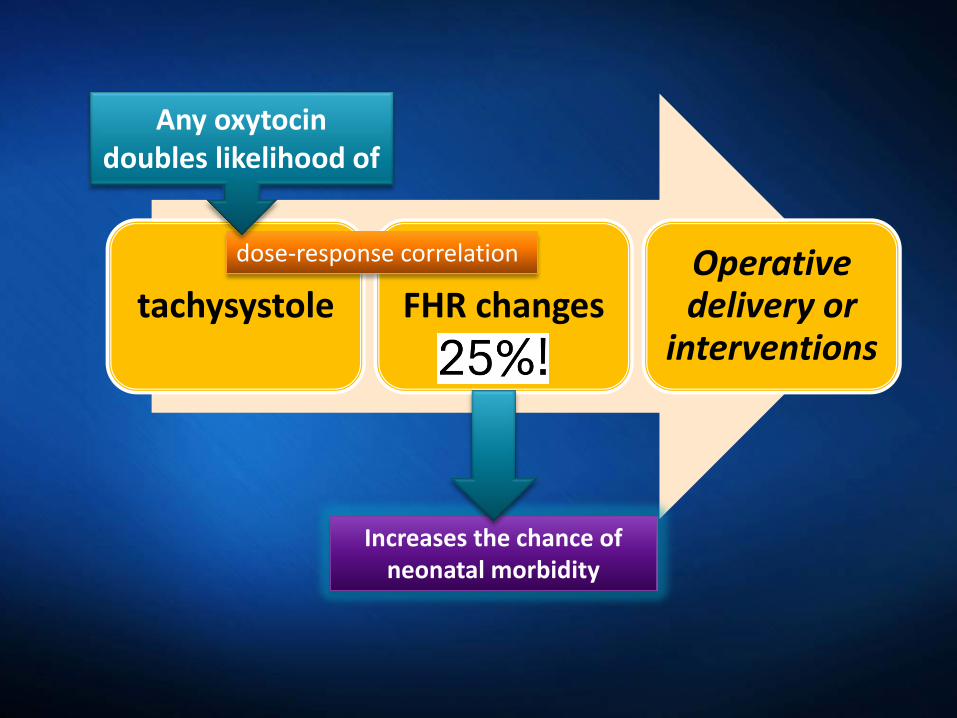
tachysystole FHR changes Operative delivery or
interventions
dose-response correlation
Increases the chance of neonatal morbidity
Any oxytocin doubles likelihood of
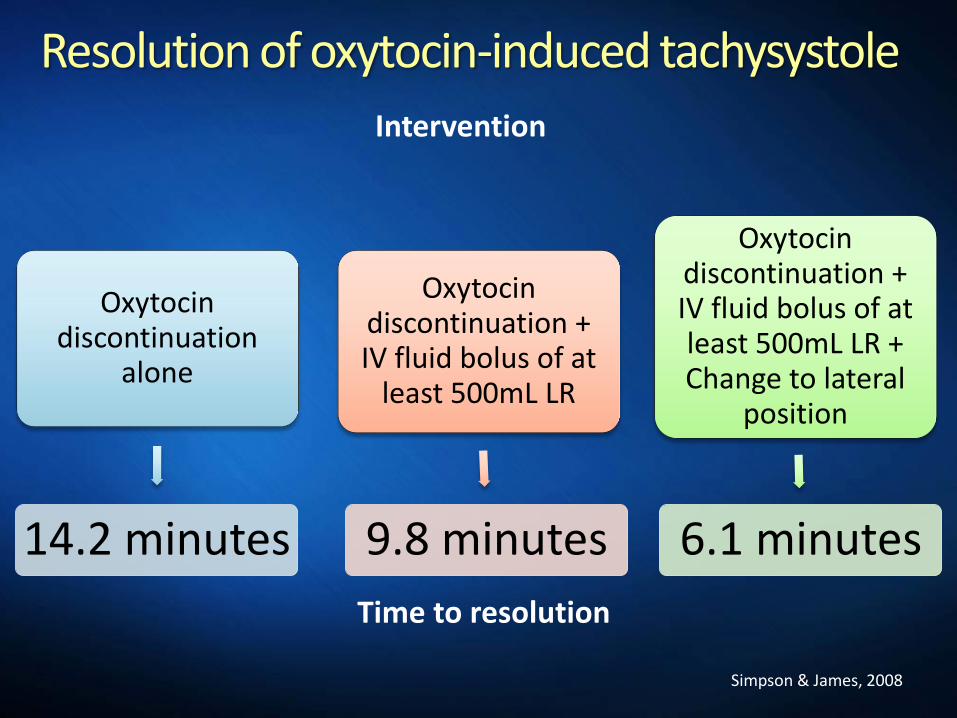
Resolution of oxytocin-induced tachysystole
Intervention
Time to resolution
Oxytocin discontinuation
alone
14.2 minutes
Oxytocin discontinuation + IV fluid bolus of at
least 500mL LR
9.8 minutes
Oxytocin discontinuation + IV fluid bolus of at least 500mL LR + Change to lateral
position
6.1 minutes
Simpson & James, 2008
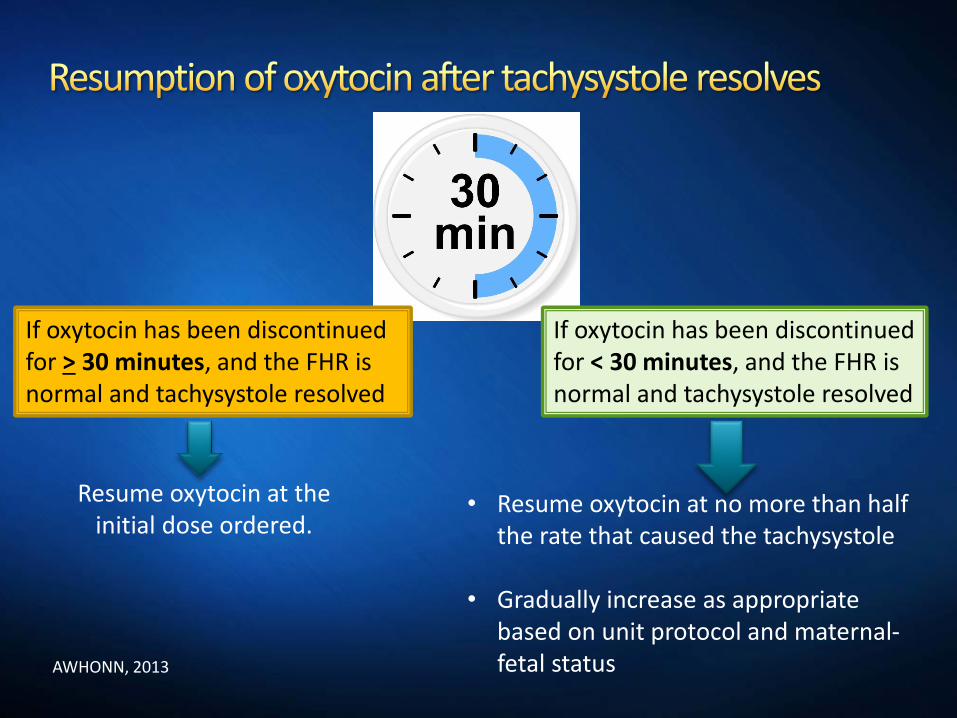
If oxytocin has been discontinued for < 30 minutes, and the FHR is normal and tachysystole resolved
• Resume oxytocin at no more than half the rate that caused the tachysystole
• Gradually increase as appropriate
based on unit protocol and maternal-fetal status
Resume oxytocin at the initial dose ordered.
If oxytocin has been discontinued for > 30 minutes, and the FHR is normal and tachysystole resolved
AWHONN, 2013
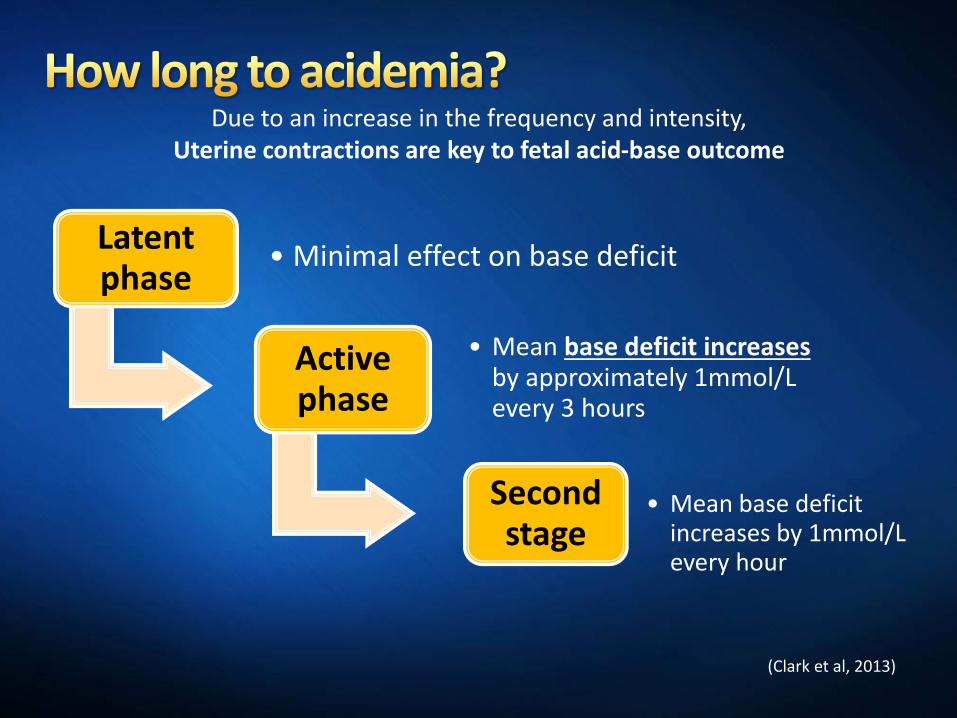
(Clark et al, 2013)
Due to an increase in the frequency and intensity, Uterine contractions are key to fetal acid-base outcome
Latent phase
• Minimal effect on base deficit
Active phase
• Mean base deficit increases by approximately 1mmol/L every 3 hours
Second stage
• Mean base deficit increases by 1mmol/L every hour
Tachysystole has a great effect on fetal-placental oxygenation
Metabolic acidemia usually does not appear suddenly, but can evolve gradually over a period of approximately 60 minutes.
Applies only to FHR tracings that are normal initially and subsequently develop minimal to absent variability with recurrent decelerations and no acute events.
(Clark et al, 2013)
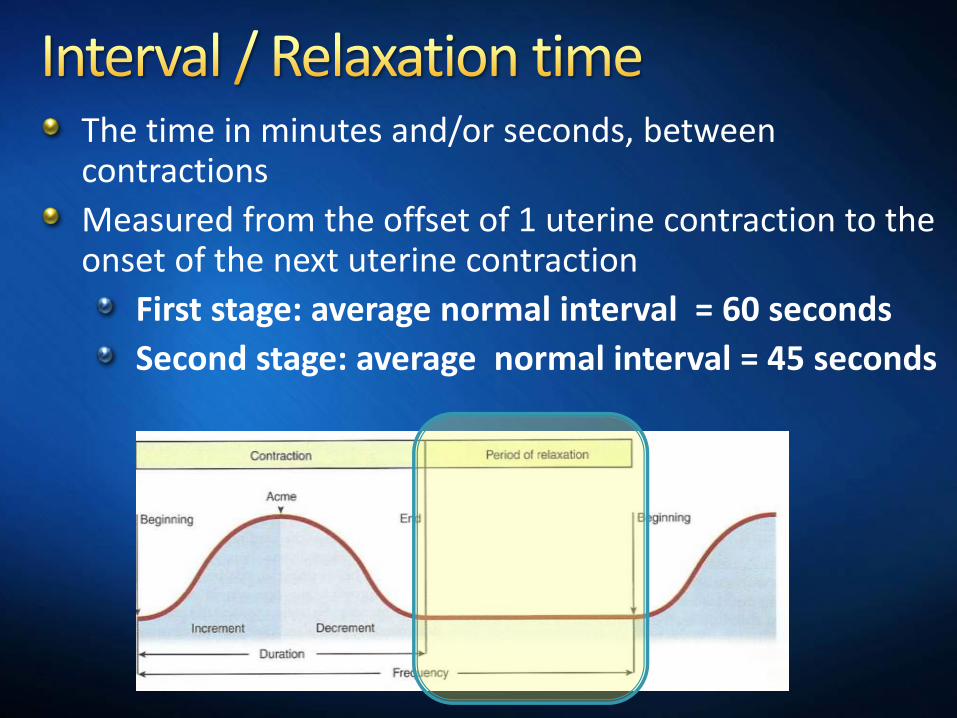
The time in minutes and/or seconds, between contractions
Measured from the offset of 1 uterine contraction to the onset of the next uterine contraction
First stage: average normal interval = 60 seconds
Second stage: average normal interval = 45 seconds
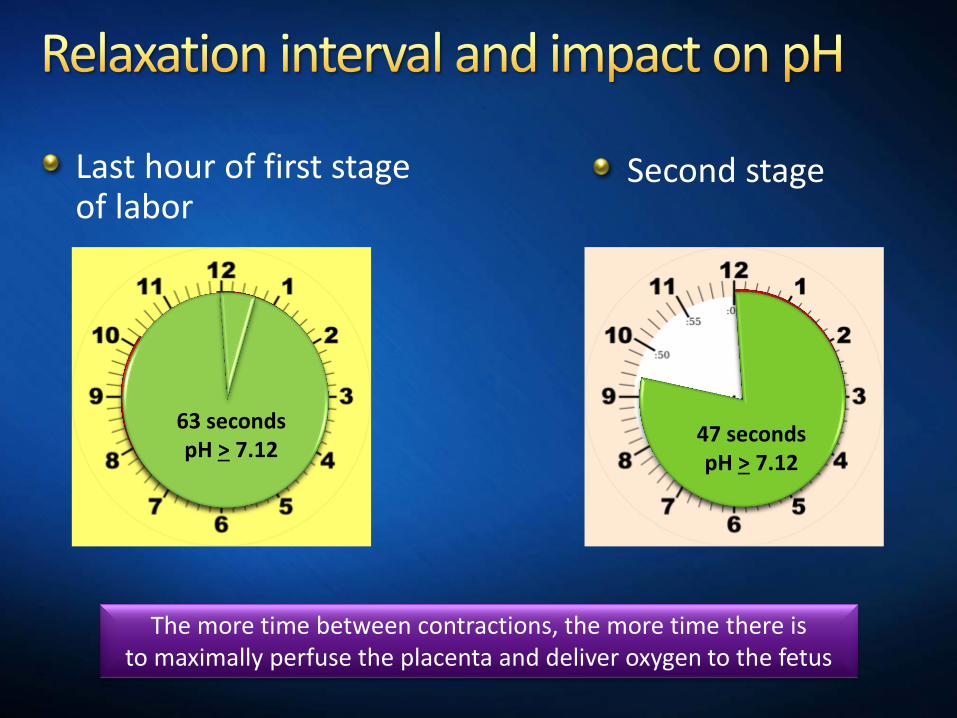
Last hour of first stage of labor
Second stage
51 seconds pH < 7.11 63 seconds pH > 7.12
36 seconds pH < 7.11
47 seconds pH > 7.12
The more time between contractions, the more time there is to maximally perfuse the placenta and deliver oxygen to the fetus
1. True
2. False
Stopping pushing temporarily or pushing with every other or every third contraction based on the fetal response can be effective at allowing the fetus to recover and maintain adequate reserves
You do not necessarily have to wait for the full 30 minutes to declare tachysystole. If the pattern is trending towards tachysystole, initial actions such as a change in position may avert this issue.
Tachysystole refers to both spontaneous and induced labor
Tachysystole, inadequate relaxation time and/or hypertonus can result in a progressive adverse effect on fetal oxygenation (ACOG & AAP, 2014).
Shortened relaxation time leads to excess constriction of the spiral arterioles reducing placental blood flow.
Measured from the baseline resting tone (AKA) High Frequency Low
amplitude
Duration < 40 seconds
NORMAL
Duration ranges from 40-90 sec. generally not exceeding 90 seconds
Uterine irritability
Abruption, infection, dehydration, stress, preeclampsia, preterm labor
Relate to underlying physiology. Narcotic administration may cause a short duration (< 20 minutes) of undulatory heart rate pattern followed by &/or preceded by a normal FHR pattern.
Transient, short duration, resolve spontaneously (usually within 20-30 min) and usually preceded and followed by a normal FHR
Following maternal administration of some opioids (e.g. butorphanol and fentanyl)
Measured from the baseline resting tone
A contraction that plateaus and does not return to normal baseline for 2 normal contraction cycles or 5 minutes
Also defined as a uterine contraction lasting >180 seconds
NORMAL
Duration ranges from 40-90 sec. generally not exceeding 90 seconds
TETANY
Normal duration 40-90 seconds
Irritability (AKA: High Frequency/Low Intensity) Uterine activity with a duration of < 40 seconds
Consider abruption before giving terbutaline
May be a precursor to labor or preterm labor or an indication of infection
Irritability is usually not associated with decreased placental oxygenation unless abruption has / is occurring
Uterine tetany – may be caused by prostaglandins, oxytocin or be spontaneous
A normal fetoplacental unit may have its uteroplacental reserve exceeded with tetanic contractions.
Intensity
Palpation: strength of the UC (mild, moderate, strong) or
IUPC: in mmHg (peak minus resting tone)
Tone
The intrauterine pressure when the uterus is not contracting
Average resting tone during labor is 10mmHg
Document as “relaxed” (meaning easily indented using palpation) or “not relaxed” (remaining firm)
Hypertonus
A resting tone exceeding 20-25 mm Hg with IUPC, or
A uterus that palpates as “not relaxed” between UC.
Associated with oxytocin, prostaglandin, CPD, and polyhydramnios or any IV bolus drug administration
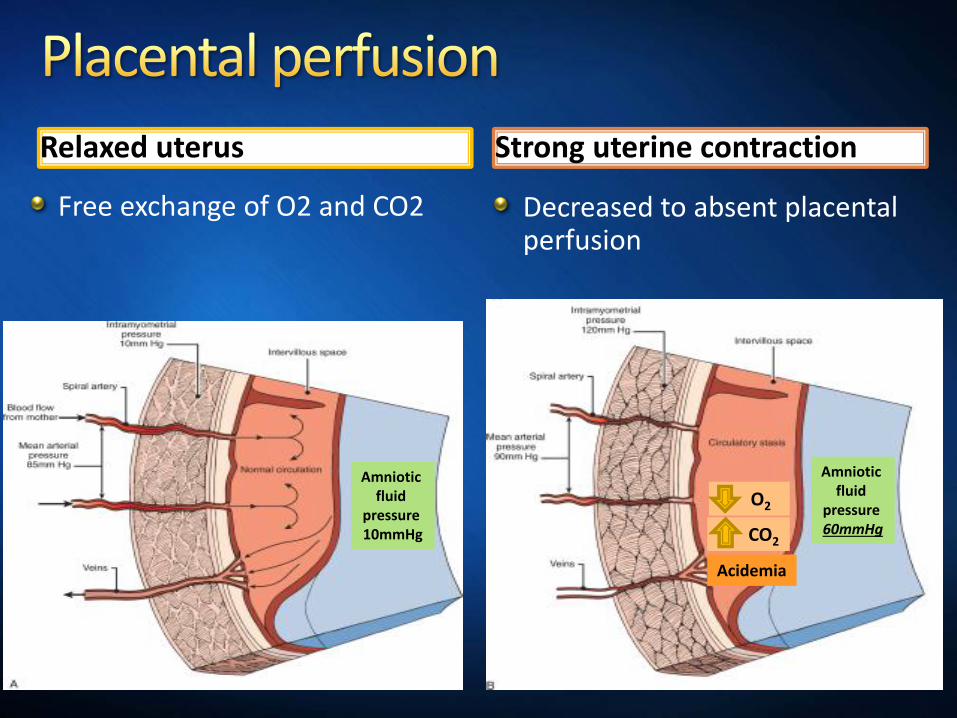
Relaxed uterus
Free exchange of O2 and CO2
Strong uterine contraction
Decreased to absent placental perfusion
Amniotic fluid
pressure 10mmHg
O2
CO2
Acidemia
Amniotic fluid
pressure 60mmHg
The spiral arterioles provide oxygen delivery to the placenta and fetus. Uterine contractions produce intermittent diminution of blood flow to the intervillous space where oxygen exchange occurs.
When fetal oxygenation is sufficiently impaired to produce fetal metabolic acidosis from anaerobic glycolysis, direct myocardial depression occurs and the FHR pattern becomes indeterminate or abnormal.
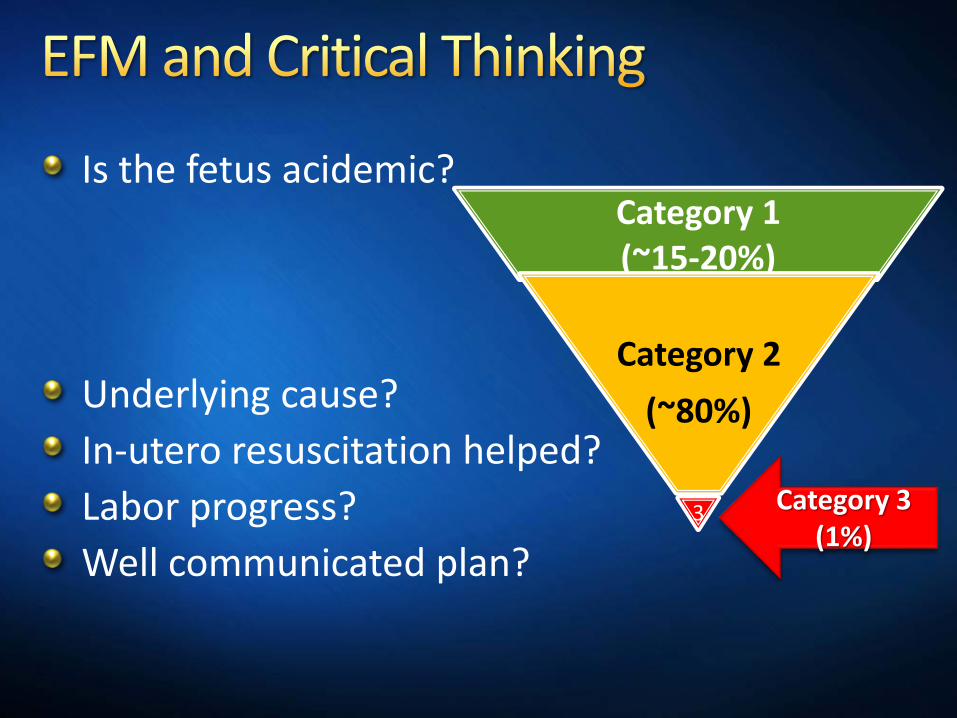
Is the fetus acidemic?
Underlying cause?
In-utero resuscitation helped?
Labor progress?
Well communicated plan?
Category 1 (~15-20%)
Category 2
(~80%)
3 Category 3 (1%)
Baseline 130
Moderate variability
No late, variable or prolonged decelerations
Does not require the presence of accelerations
Includes all FHR tracings not categorized as Category 1 or 3.
Represent about 80% of those encountered in clinical care
Multiple basic science investigations and clinical trials have been published but this body of work has primarily served to raise more questions than it has answered.
Am J Obstet Gynecol. 2013 Aug;209(2):89-97.
Category II patterns identify fetuses that may potentially be in some degree of jeopardy but are either not acidemic, or have not yet developed a degree of hypoxia/acidemia that would result in neonatal encephalopathy.
Must also avoid unnecessary intervention, and encourage vaginal delivery in women whose FHR patterns suggest minimal risk of significant deterioration prior to delivery.
Clark, et. al Am J Obstet Gynecol. 2013 Aug;209(2):89-97.
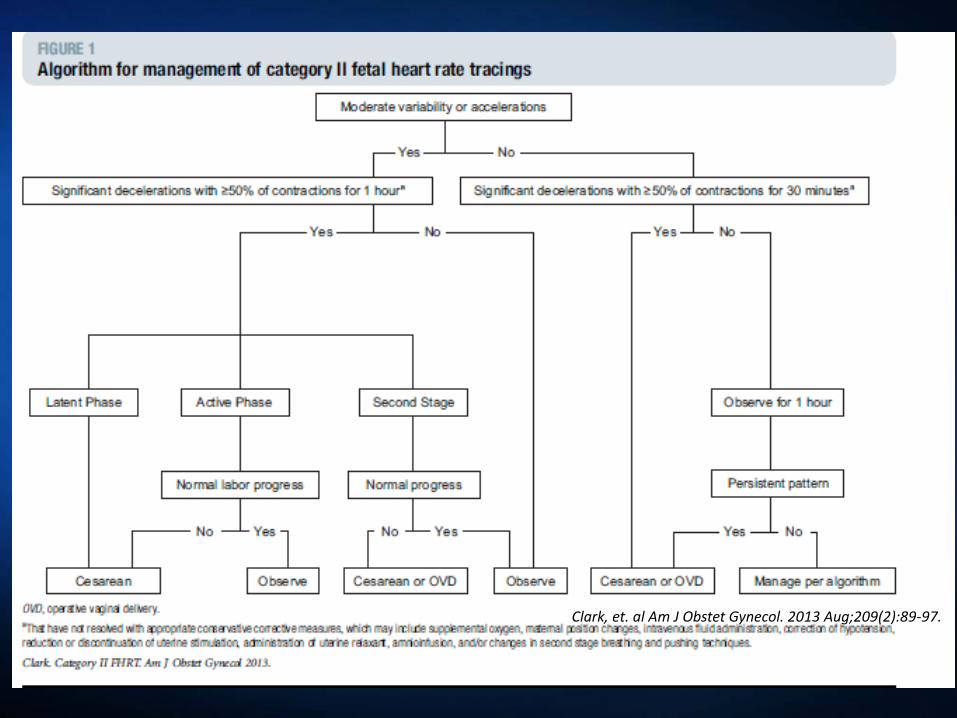
Clark, et. al Am J Obstet Gynecol. 2013 Aug;209(2):89-97.
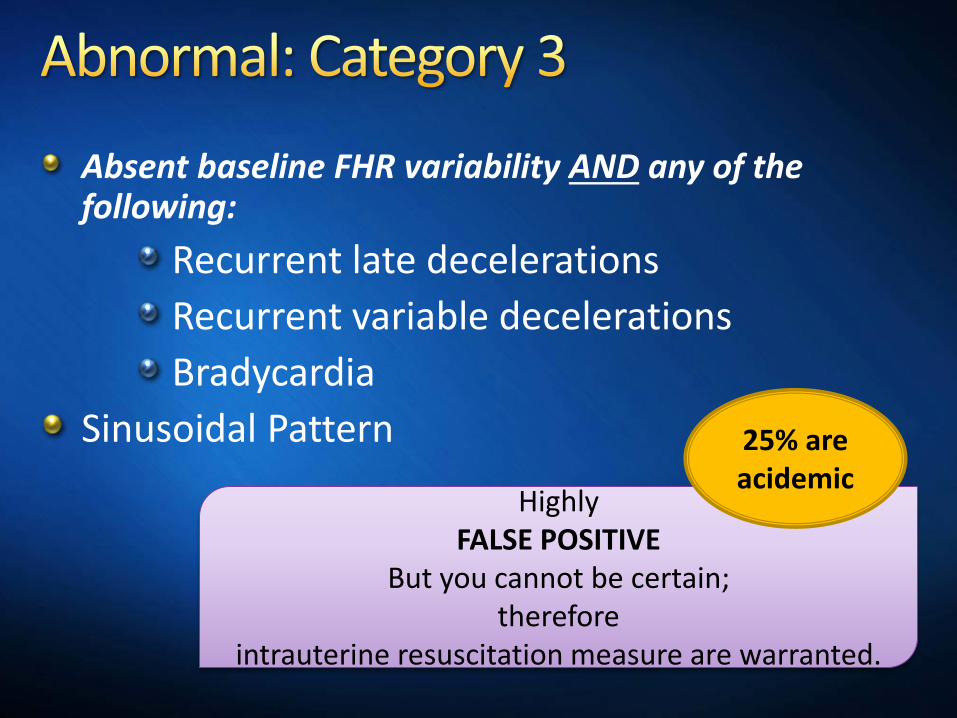
Absent baseline FHR variability AND any of the following:
Recurrent late decelerations
Recurrent variable decelerations
Bradycardia
Sinusoidal Pattern
Highly FALSE POSITIVE
But you cannot be certain; therefore
intrauterine resuscitation measure are warranted.
25% are acidemic
Reasonable management decisions simply cannot be based on the results of a test that is virtually always wrong.
The negative predictive value of intrapartum FHR monitoring is nearly 100%.
Trying to use intrapartum FHR monitoring to diagnose neurologic injury is a recipe for failure.
In contrast, relying on the presence of moderate variability or accelerations, or both, to confirm adequate fetal oxygenation allows the clinician to formulate and articulate a rational, evidence-based plan of management that reflects consensus in the literature.
(Clark et al, 2013)



![Early intrauterine development of mixed giant … · Early intrauterine development of mixed giant ... but with intrauterine death at 29 weeks [5]. Fetal . Early intrauterine development](https://img.pdfslide.net/doc/110x75/5b63022f7f8b9ade588b8aac/early-intrauterine-development-of-mixed-giant-early-intrauterine-development.jpg)